Back to Journals » Drug Design, Development and Therapy » Volume 20
The Correlation Between Neoadjuvant Chemotherapy for Ovarian Cancer and the Analgesic Effects of Remifentanil a Prospective Cohort Study
Authors Ding Y, Xing L, Paerhati H, Gao R, Gu L
Received 18 November 2025
Accepted for publication 13 March 2026
Published 1 April 2026 Volume 2026:20 582499
DOI https://doi.org/10.2147/DDDT.S582499
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Yuyan Ding,* Lingxi Xing,* Halisa Paerhati, Rong Gao, Lianbing Gu
Department of Anesthesiology, Jiangsu Cancer Hospital, Jiangsu Institute of Cancer Research, The Affiliated Cancer Hospital of Nanjing Medical University, Nanjing, 210018, China
*These authors contributed equally to this work
Correspondence: Lianbing Gu; Rong Gao, Email [email protected]; [email protected]
Background: Neoadjuvant chemotherapy (NACT) is a key therapy for ovarian cancer that reduces tumor burden but injures normal tissues, necessitating meticulous anesthesia management. However, the pharmacokinetics and pharmacodynamics of remifentanil, a commonly used anesthetic analgesic, in this context remain inadequately studied, and relevant research in this patient population remains insufficient.
Purpose: This prospective observational cohort study aimed to evaluate the effect of preoperative NACT on intraoperative remifentanil requirements in ovarian cancer patients and assess perioperative outcomes to guide its rational clinical use.
Methods: Seventy ovarian cancer patients undergoing surgery were divided into NACT (3 to 4 cycles of paclitaxel + carboplatin) and Non-NACT groups; 64 completed the study. The plasma concentration of remifentanil was titrated to maintain the intraoperative Index of Consciousness 2 (IOC2) value between 35 and 45. The primary outcome was average intraoperative remifentanil consumption; secondary outcomes included intraoperative and postoperative hemodynamic indicators, usage of vasoactive drugs, incidence of adverse events, and postoperative recovery indicators.
Results: Compared with the Non-NACT group, the NACT group had significantly higher intraoperative remifentanil consumption [11.89 ± 2.02 vs. 9.40 ± 1.81 μg·kg− 1·h− 1, p < 0.001] and target concentration adjustment frequency [3.97 (1.62) vs. 2.75 (1.32), p=0.002]. Intraoperative heart rate (HR) and mean arterial pressure (MAP) were significantly higher in the NACT group at T3, T4, and T5 (all p< 0.05). Specifically, HR at T3 [89.47 (12.00) vs. 81.56 (14.98), p=0.02], T4 [70.88 (9.20) vs. 64.53 (12.89), p=0.03], T5 [72.94 (12.86) vs. 64.31 (13.08), p=0.01]; MAP at T3 [122.80 (11.67) vs. 114.18 (12.48), p=0.01], T4 [103.16 (11.26) vs. 95.72 (8.87), p=0.01], T5 [107.27 (12.38) vs. 99.91 (10.46), p=0.01].
Conclusion: Preoperative NACT increases ovarian cancer patients’ sensitivity to intraoperative pain, leading to higher remifentanil consumption and more frequent concentration adjustments. Clinically, higher intraoperative analgesic doses are needed for adequate pain control in this population.
Keywords: ovarian cancer, NACT, opioids, remifentanil, index of consciousness 2, IOC2, intraoperative analgesia
Introduction
Ovarian cancer (OC) ranks third among malignant tumors of the female reproductive system globally while having the highest mortality rate.1 Due to subtle early symptoms, approximately 75% of patients are diagnosed at advanced stages, significantly contributing to this mortality.2 Neoadjuvant chemotherapy (NACT) refers to the administration of systemic anticancer agents prior to surgery to improve surgical conditions. According to the NCCN guidelines,3 when the Suidan score is ≥3 and primary debulking surgery (PDS) is unlikely to achieve R0 resection, the use of 3 to 4 cycles of NACT preoperatively can reduce tumor burden, improve surgical outcomes, eliminate microscopic metastases, and enhance survival rates, making it a vital part of comprehensive treatment.4,5
Currently, the paclitaxel and carboplatin regimen is the first-line NACT approach for advanced ovarian cancer.6 However, these agents can cause hepatorenal, central nervous system, and peripheral neurotoxicity,7–9 affecting their pharmacokinetics and potentially altering the metabolism of anesthetic drugs. Consequently, patients receiving NACT may have different tolerance and dosage requirements for anesthetics compared to those not undergoing chemotherapy. Most studies have focused on NACT’s impact on sedatives and neuromuscular blockers, with limited research on intraoperative analgesic sensitivity in these patients. Understanding this sensitivity is vital for optimizing perioperative recovery.
Another challenge in perioperative analgesia is the real-time, objective assessment of pain levels in patients under general anesthesia. For a long time, anesthesiologists have primarily relied on the clinical evaluation of analgesic effects based on changes in vital signs such as HR and MAP. However, the accuracy of this approach is far from sufficient. In recent years, multiple studies have indicated that the IOC2, as a novel pain assessment index, can quantify the analgesic effect.10,11 It objectively evaluates pain intensity in patients under general anesthesia, guiding the rational use of analgesic drugs to reduce perioperative adverse events. This approach shows significant advantages and promising application prospects in clinical practice.
This study aimed to evaluate the impact of NACT on the analgesic effect of remifentanil during ovarian cancer surgery. We focused on effective pain management by guiding intraoperative analgesic administration based on IOC2 monitoring and determining the average consumption of remifentanil. The findings will provide a reference for the rational and effective clinical use of remifentanil in patients who received NACT.
Methods and Materials
Study Design and Ethics
This prospective, observational, cohort clinical trial was designed, implemented, executed, and overseen by the study sponsor and steering committee. Written informed consent was obtained from all study participants before enrolment. The study was conducted in accordance with the Declaration of Helsinki and approved by the independent Institutional Ethics Committee of Jiangsu Cancer Hospital (Ethics approval number: 2024–019-01) and obtained written informed consent from all participants involved in the trial. The trial was registered at the Chinese Clinical Trial Center (Registration number: ChiCTR2400090086).
Participants
This study was a prospective observational cohort study. Inclusion criteria were as follows: preoperative biopsy pathology indicating ovarian cancer, age between 18 and 64 years, body mass index (BMI) of 18.5 to 28 kg·m−2, American Society of Anesthesiologists (ASA) classification of II to III, no significant history of cardiopulmonary disease, and laboratory tests showing no significant abnormalities in liver and renal function.
The patients were categorized into the NACT Group and the Non-NACT Group based on whether NACT was administered preoperatively. Both groups underwent surgery conducted by the same anesthesiologists and gynecologic oncologists, with similar tumor staging and comparable planned extents and degrees of resection, ensuring consistency across surgical procedures. In the NACT Group, patients received preoperative NACT with three cycles of “paclitaxel combined with carboplatin” (TC) regimen lasting 21 days per cycle. After imaging assessment and considering the Fagotti score (Peritoneal Involvement Score< 4), these patients were considered suitable for surgical intervention. In the Non-NACT Group, patients underwent surgery directly without preoperative NACT.
Exclusion criteria were as follows: declined participation; history of allergy to any medications used in this study; history of radiation therapy; chronic alcohol consumption, chronic opioids, or other analgesic use (≥ 3 months); pregnancy or lactation; severe cardiopulmonary disease or liver/kidney dysfunction; and diagnosis of mental illness or other autonomic nervous system disorders that may affect electroencephalogram (EEG) results.
Drop-out criteria were as follows: surgical duration < 2 hours or > 6 hours; severe intraoperative circulatory instability (MAP and HR fluctuations exceeding 30% of baseline); intraoperative blood loss exceeding 30% of total blood volume; postoperative endotracheal intubation and transfer to the ICU; and missing clinical data or withdrawal from the study.
Neuromonitoring Methods
The level of analgesia was continuously recorded using the proprietary analgesia index IOC2 (Index of Consciousness 2, also known as qNOX) with the Angel-6000D Multi-parameter Anesthesia Monitor (Shenzhen Weihaokang Medical Technology Co., Ltd., Guangdong, China). IOC2 was utilized in this study to evaluate patients’ responses to noxious stimuli and to assess analgesic depth. In the European market, IOC2 is referred to as qNOX (CONOX monitor, Fresenius Kabi/Quantium Medical).
The IOC2 scale ranges from 0 to 99, with values between 50 and 99 indicating suboptimal intraoperative analgesia, while values between 0 and 30 signify excessive analgesia.11 Zhao et al demonstrated that maintaining an IOC2 within 35–45 provides the optimal depth of analgesia, minimizing anesthetic-induced suppression of endocrine function to the greatest extent. To minimize bias between the experimental and control groups, IOC2 values were maintained within the 35–45 range for both groups.
Anaesthetic Procedures
All patients received total intravenous anesthesia following routine preoperative fasting for 8 hours and nil by mouth for liquids for 4 hours. No analgesics were administered preoperatively. Upon arrival in the operating room, standard monitoring was initiated, including 5-lead electrocardiography, pulse oximetry, non-invasive automated blood pressure measurement, and neuromuscular monitoring. Under local anesthesia, radial artery catheterization was performed for invasive blood pressure (IBP) monitoring. A cerebral depth-of-anesthesia monitor (IOC) was attached for continuous recording of IOC1 and IOC2.
Anesthesia was induced and maintained using target-controlled infusion (TCI). Propofol was administered using the Marsh model, and remifentanil was delivered using the Minto model. Induction was performed with a plasma target concentration (Cp) of 4 µg·mL−1 for propofol and 5 ng·mL−1 for remifentanil, along with an intravenous bolus of rocuronium 0.6 mg·kg−1. Following induction, tracheal intubation was performed when the train-of-four (TOF) count reached 0 and IOC2 was below 45, to avoid stress responses related to tracheal intubation.
Following successful intubation, mechanical ventilation was initiated in pressure-controlled volume-guaranteed (PCV‑VG) mode: tidal volume 8–10 mL·kg−1, FiO2 60%, respiratory rate 12–16 breaths/min, I:E ratio 1:2, and PETCO2 maintained between 35 and 45 mmHg. During the procedure, the propofol Cp was adjusted between 2 and 5 µg·mL−1 to maintain IOC1 within 40–60. After intubation, the remifentanil Cp was titrated to 4 ng·mL−1. When IOC2 exceeded 45 for 1 minute, the Cp was increased by 0.5 ng·mL−1; conversely, when IOC2 fell below 35 for 1 minute, the Cp was decreased by 0.5 ng·mL−1. If IOC2 increased by more than 10 within 1 minute, the Cp was further increased by 0.5 ng·mL−1. The remifentanil Cp was maintained between 2 and 6 ng·mL−1 to keep IOC2 within 35–45. The maintenance infusion dose of rocuronium was 0.6–1.0 mg·kg−1·h−1. Intraoperatively, MAP and HR were maintained within 20% of baseline values. When IOC1 stabilized between 40 and 60 and IOC2 between 35 and 45, a persistent HR below 50 beats per minute warranted intravenous administration of 0.5 mg atropine. If MAP fell below 80% of baseline, 5 mg ephedrine or 30–60 μg phenylephrine was administered intravenously. Intraoperative temperature management was implemented to maintain nasopharyngeal temperature ≥ 36°C. Given the visceral pain associated with ovarian cancer resection, all patients received 10 mg oxycodone upon abdominal closure. Propofol and remifentanil TCI were discontinued at the end of surgery. To prevent postoperative nausea and vomiting, 4 mg ondansetron was administered at the end of surgery.
After surgery, all patients were transferred to the post-anesthesia care unit (PACU) and connected to a patient-controlled intravenous analgesia (PCIA) pump. Extubation was performed when spontaneous ventilation was fully restored, consciousness was regained, and the TOF ratio was greater than 0.9. The PCIA formulation consisted of sufentanil 2.5 μg·kg−1 diluted in normal saline to a total volume of 100 mL. The background infusion rate was set at 1.0 mL·h−1, with a bolus dose of 1.0 mL per demand and a lockout interval of 15 minutes. The PCIA regimen was adjusted to maintain a Visual Analogue Scale (VAS) score ≤ 3. Rescue analgesia with flurbiprofen axetil 50 mg intravenously was administered for a VAS score ≥ 4, with a maximum daily dose not exceeding 100 mg. For postoperative nausea or vomiting, ondansetron 2 mg was administered intravenously as needed.
Outcome Measures
The primary outcome was the average intraoperative dose of remifentanil.
Secondary outcomes included intraoperative and postoperative indicators. The intraoperative observational indicators comprised MAP and HR at defined time points: on entering the operating room (T1), prior to anesthetic induction (T2), at tracheal intubation (T3), 1 minute after intubation (T4), and at the end of surgery (T5). Additional intraoperative indicators included other anesthetic drug doses, the frequency of vasoactive drug administration, the incidence of intraoperative adverse events (such as hypotension and bradycardia), and the number of adjustments made to the remifentanil plasma target concentration based on IOC2.
Postoperative observational variables included time to extubation, duration of PACU stay, and VAS scores at rest and during movement at 24, 48, and 72 h after surgery. In addition, cumulative consumption of analgesics and antiemetics at 24, 48, and 72 h postoperatively was recorded. Other recorded variables included effective and total presses of the PCIA pump, total 72-hour analgesic consumption, time to first flatus, and total hospital stay.
The average intraoperative dose of remifentanil (μg·kg−1·h−1) was calculated by dividing the total remifentanil consumption dose (μg) by the weight of patients (kg) and the total duration of infusion (h).
Regarding intraoperative adverse events, intraoperative hypotension was defined as MAP< 65mmHg or IBP exceed 20% of the baseline, and intraoperative bradycardia is defined as a sinus HR below 50 beats per minute.12,13
Statistical Analysis
In the pilot study of this study, under IOC2 monitoring, patients receiving NACT exhibited an average intraoperative remifentanil consumption of (10.66±1.58) μg·kg−1·h−1, while Non-NACT patients had an average consumption of (9.56±1.12) μg·kg−1·h−1. Sample size estimation was conducted using PASS software, setting the significance level at α = 0.05 and 1 - β = 0.85. The calculations indicated that a minimum of 30 patients per group was required. Taking into account a 15% dropout rate, a final total of 35 patients per group was included, resulting in 70 patients overall.
All data were analyzed using SPSS version 24.0 (IBM, Armonk, NY, USA). Independent samples t-test was used for intergroup comparisons of normally distributed continuous variables, while the Mann–Whitney U-test was applied for non-normally distributed data. Categorical variables were compared using the chi-square test or Fisher’s exact test. Normally distributed data are presented as mean ± standard deviation, whereas categorical variables are reported as frequencies (percentages). Non-normally distributed data are expressed as median and interquartile range [M (IQR)]. P<0.05 was considered statistically significant.
Results
Patient Population
The CONSORT flow diagram for participant inclusion was presented in Figure 1.
 |
Figure 1 Flow diagram of the participants’ inclusion in the study. |
Characteristics Baseline
In this study, an initial cohort of 70 patients met the inclusion criteria. However, patients were subsequently excluded for the following reasons: During the study period, one patient had an operation duration exceeding 6 hours, while two patients had an operation duration of less than 2 hours. One patient was transferred to the ICU postoperatively with an endotracheal tube in place. Additionally, two patients experienced blood loss exceeding 15% of their total blood volume. Ultimately, 64 patients were included in the final analysis, with 32 patients in the NACT group and 32 patients in the Non-NACT Group.
Demographics and surgical characteristics of the two groups were compared. No significant differences were observed between the NACT group and the Non-NACT group in terms of age, height, weight, ASA classification, patients’ preexisting comorbidities, patients’ preoperative blood pressure, heart rate, preoperative 24-hour VAS score, preoperative medication use, tumor stage and surgical site (Tables 1 and 2).
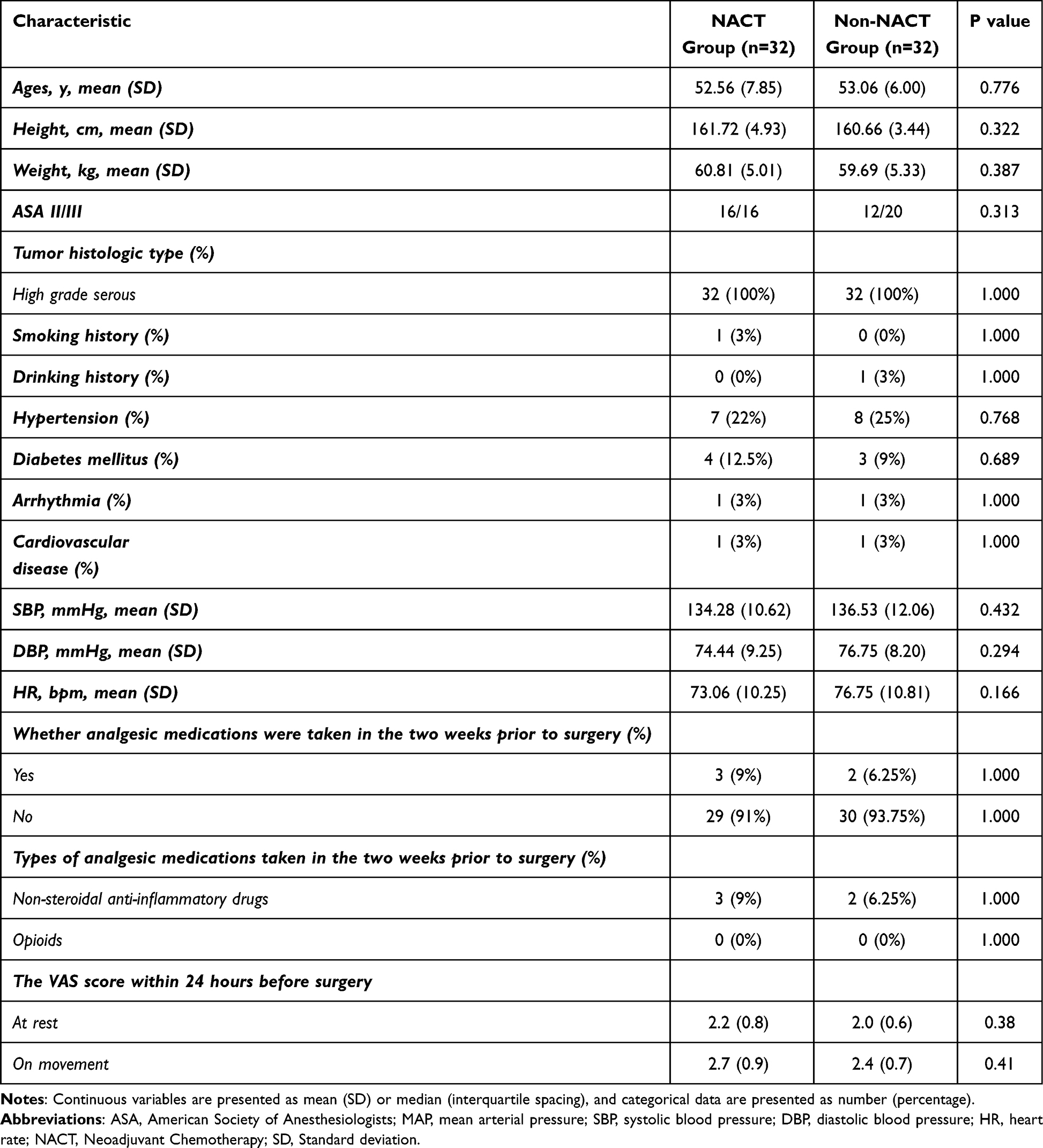 |
Table 1 Characteristics Baseline |
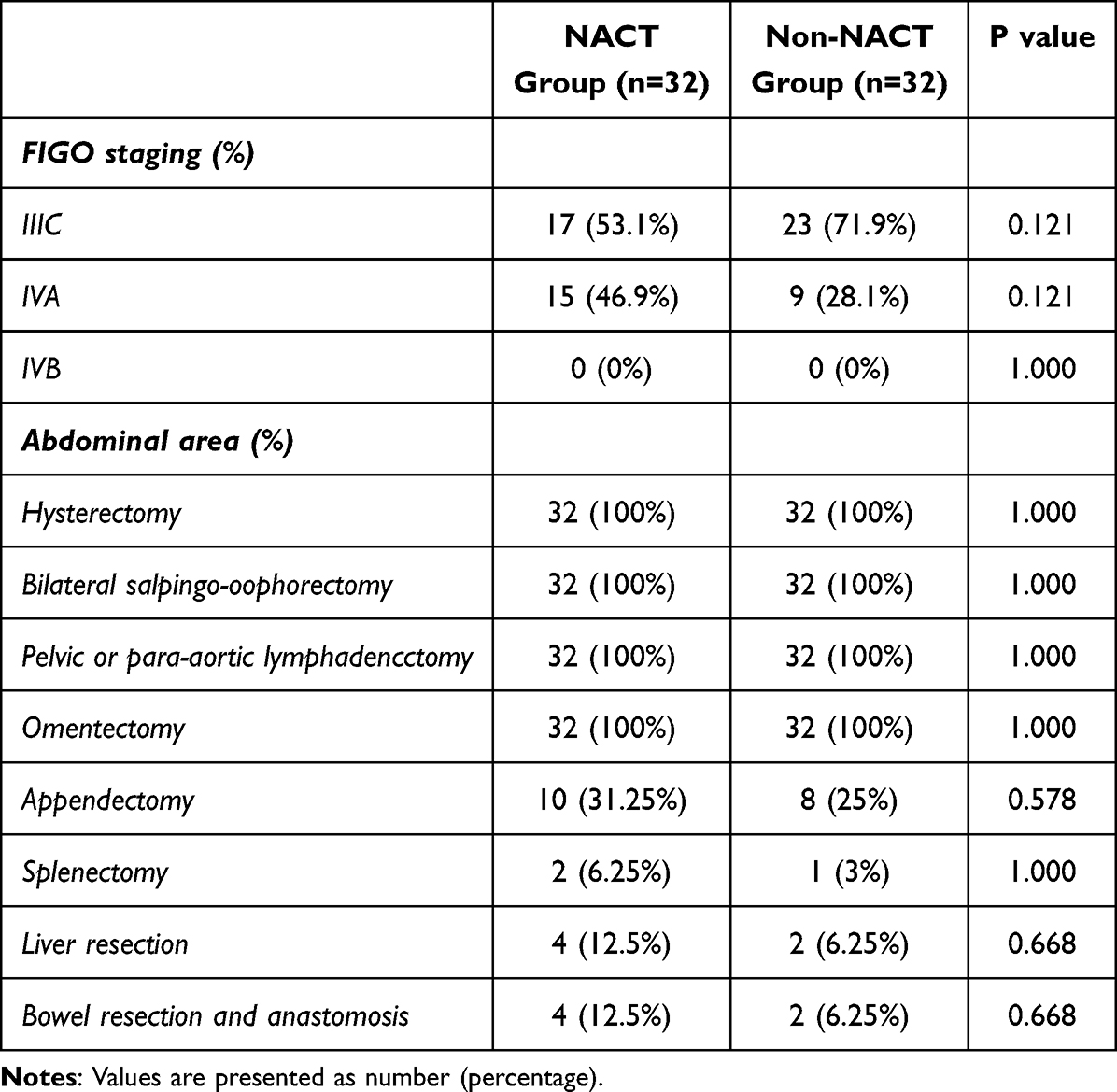 |
Table 2 Tumor Staging and Extent of Tumor Resection |
Primary Outcome Measure
The average intraoperative dose of remifentanil in the NACT group was (11.89±2.02) μg·kg−1·h−1, compared with (9.40±1.81) μg·kg−1·h−1 in the Non-NACT group (P < 0.001).
Intraoperative Datas
There were no significant differences in anesthesia time, operation time, blood loss, urine output, fluid infusion volume, and other intraoperative data between the two groups (P > 0.05). The results showed that the number of Cp adjustments based on IOC2 in the NACT group was significantly higher than that in the Non-NACT group (P = 0.002). These data were presented in Table 3.
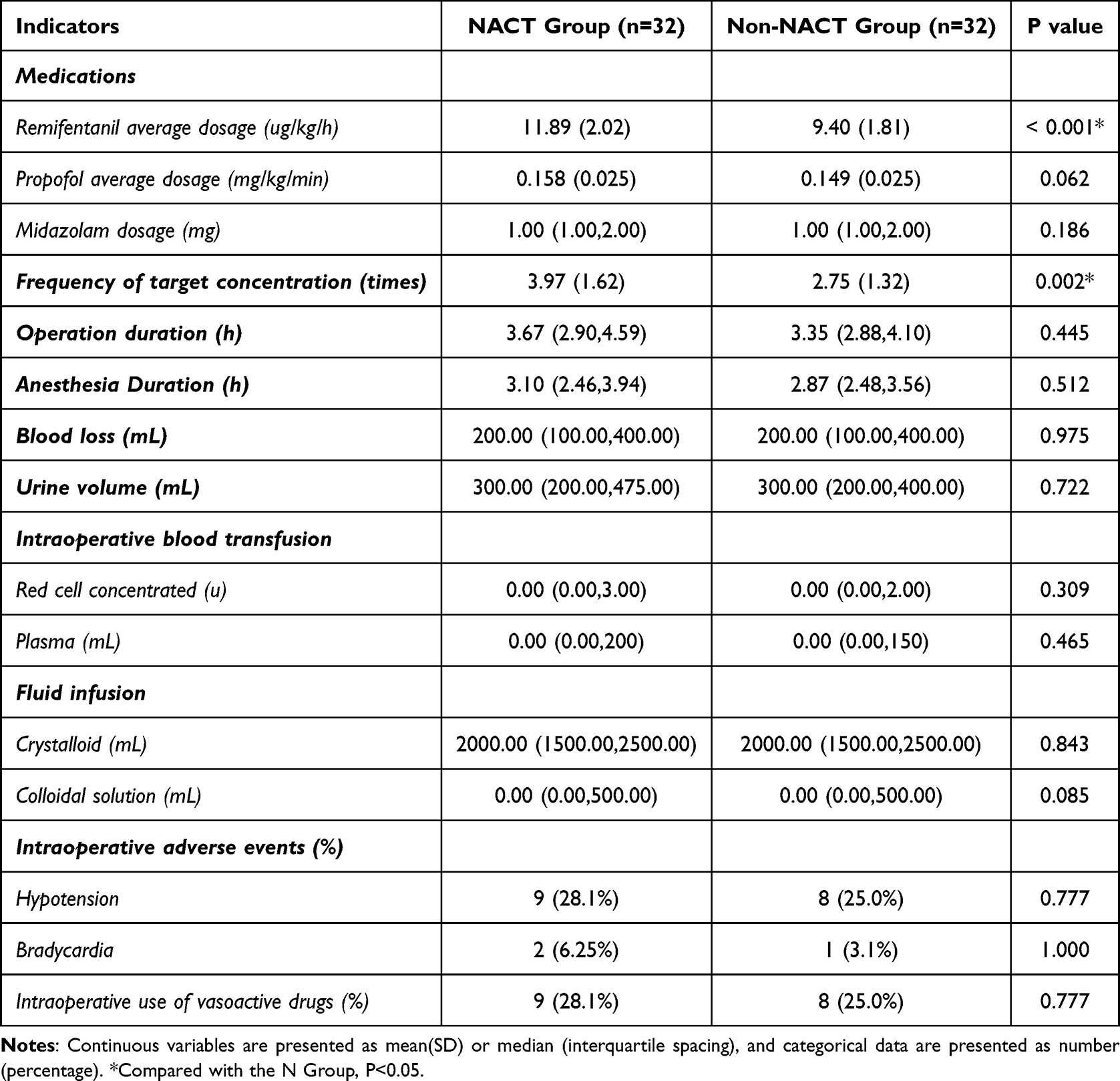 |
Table 3 Basic Information of Patients During the Surgery |
At three key time points—tracheal intubation (T3), 1 minute after intubation (T4), and the end of surgery (T5)—this study demonstrated that the MAP and HR levels in the NACT group (N Group) were significantly higher than those in the Non-NACT group (C Group) (P < 0.05). At baseline time points, namely entry to the operating room (T1) and pre-intubation after induction of anesthesia (T2), no statistically significant differences in MAP and HR levels were observed between N Group and C Group (P > 0.05). These results were shown in Table 4, Figures 2 and 3.
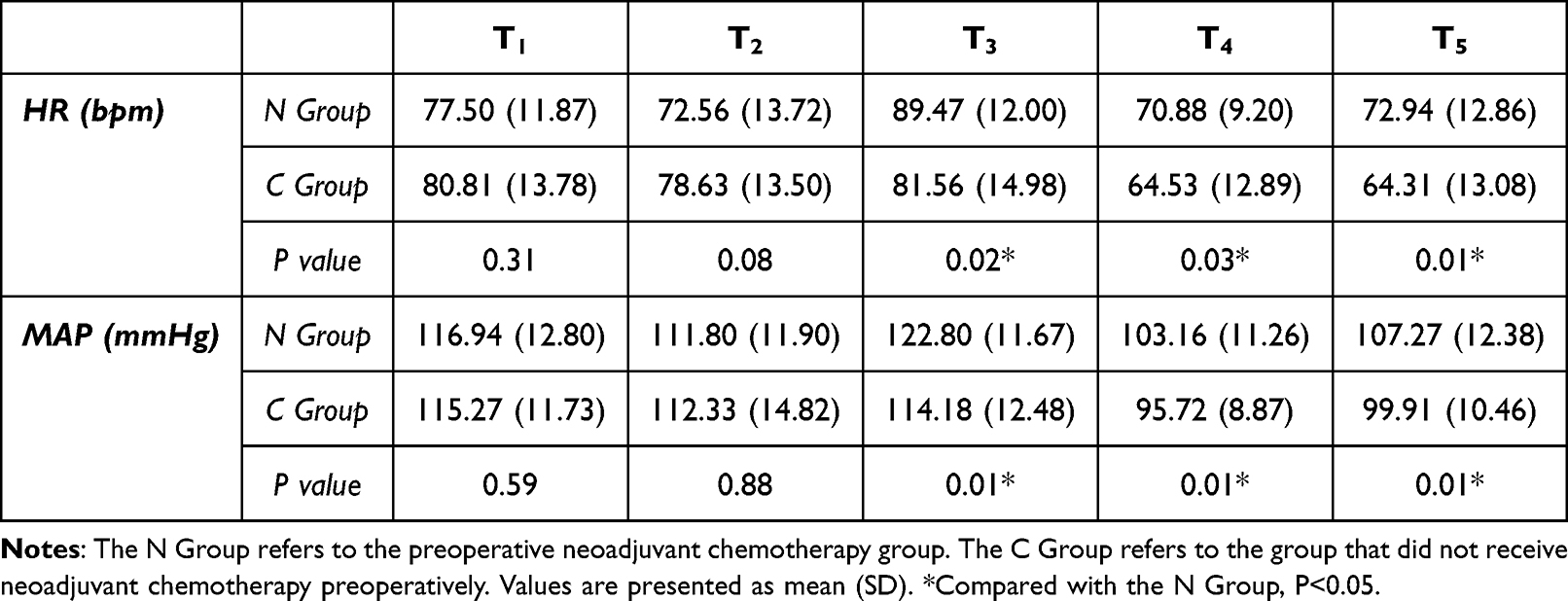 |
Table 4 MAP and HR at Different Time Points During the Procedure |
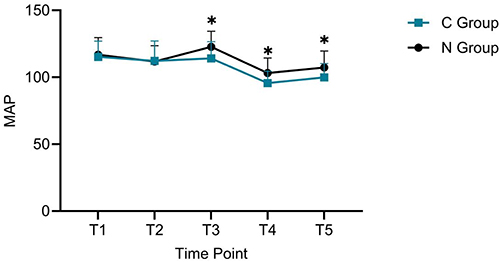 |
Figure 2 MAP at different time points during the surgery. Notes: T1, On entering the operating room; T2, Prior to anesthetic induction; T3, At tracheal intubation; T4, One-minute post-intubation; T5, At the end of surgery. *Compared with the N Group, P<0.05. |
 |
Figure 3 HR at different time points during the surgery. Notes: T1, On entering the operating room; T2, Prior to anesthetic induction; T3, At tracheal intubation; T4, One-minute post-intubation; T5, At the end of surgery. *Compared with the N Group, P<0.05. |
Postoperative Indicators
After surgery, no statistically significant differences were observed between the NACT group and the Non-NACT group in terms of extubation time, awakening time, and the use of rescue antiemetics and analgesics in patients in the PACU (P > 0.05). Please refer to Table 5.
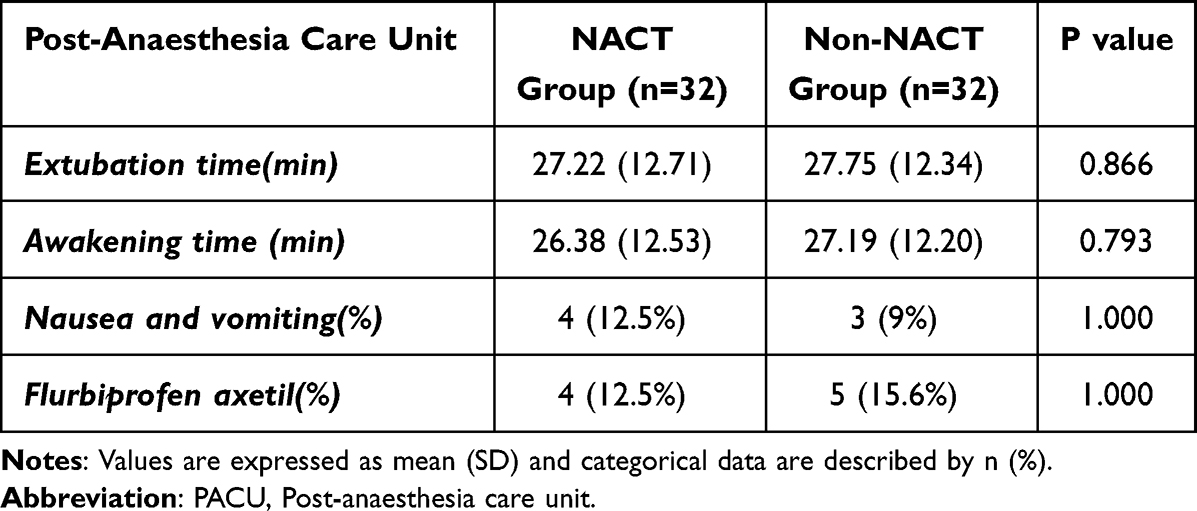 |
Table 5 The Indicators for Patients Entering the PACU Postoperatively |
On postoperative days 1, 2, and 3, there were no statistically significant differences between the NACT group and the Non-NACT group in VAS scores at rest and during activity (coughing), as well as in the use of rescue antiemetics and analgesics (P > 0.05). Refer to Table 6.
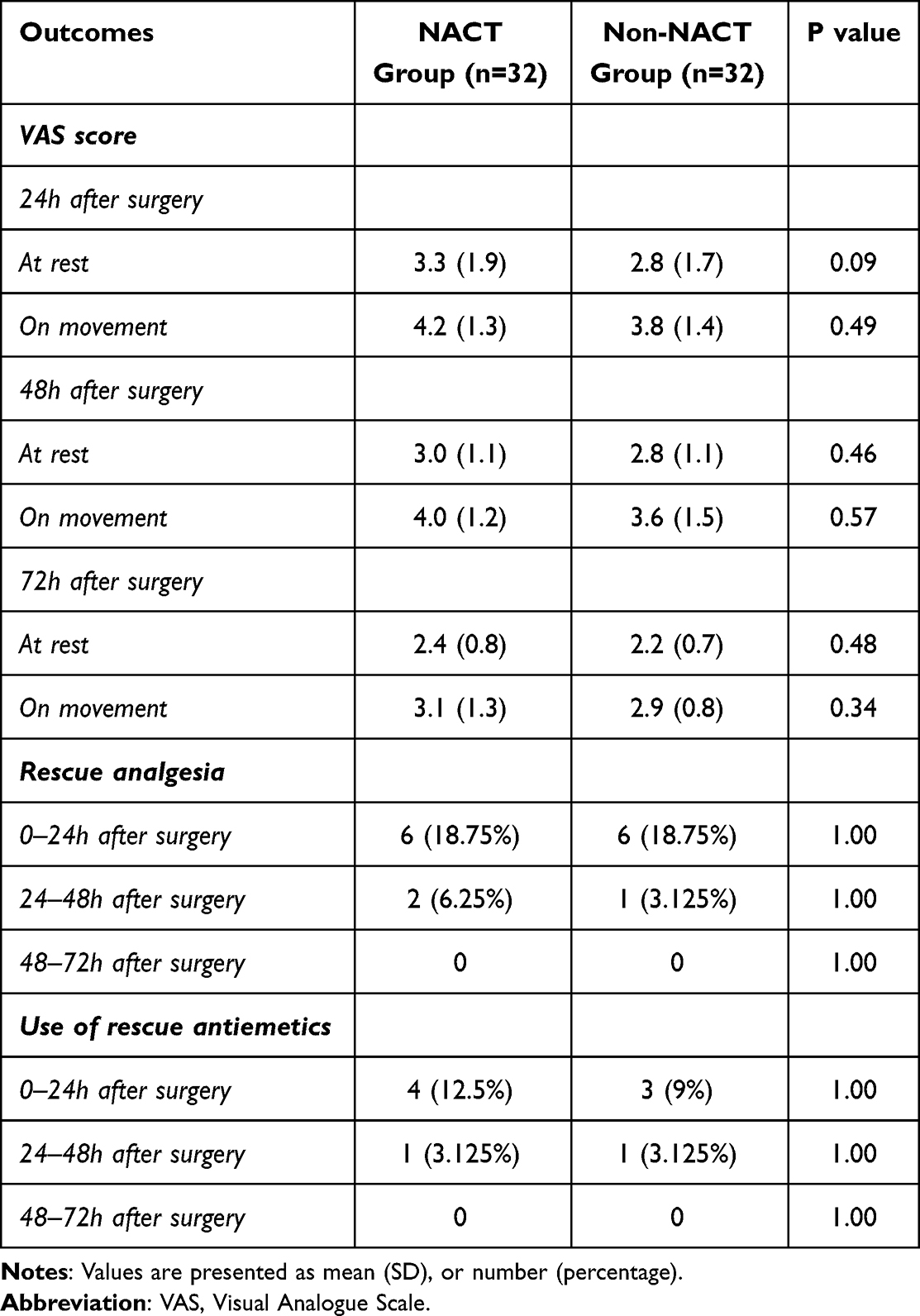 |
Table 6 Indicators Within Three days Postoperatively |
Additionally, compared with the Non-NACT group, the NACT group showed statistically significant differences in effective press counts, total press counts, and PCIA usage within 72 hours (P < 0.05). There were no statistically significant differences between the two groups in the time to first flatus or total hospital stay (P > 0.05). Refer to Table 7.
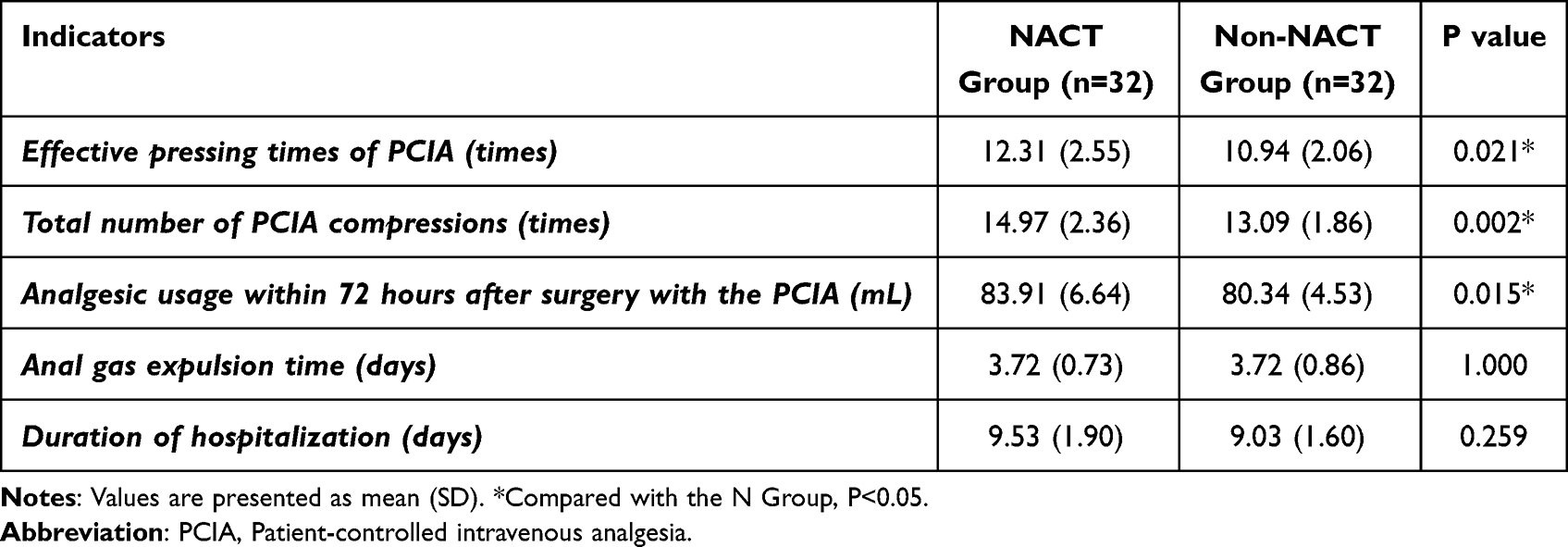 |
Table 7 Usage of the PCIA Pump and Related Indicators for Postoperative Recovery |
Discussion
NACT is pivotal in the management of ovarian cancer, aiming to reduce tumor size and enhance surgical outcomes.1,14 However, its application may influence the pharmacokinetics and pharmacodynamics of general anesthetics, thereby affecting intraoperative depth of anesthesia, recovery, and perioperative analgesia. Studies have shown that NACT can increase patient sensitivity to inhalational anesthetics, reduce the minimum alveolar concentration for blocking adrenergic responses (MAC-BAR) of sevoflurane, and alter its efficacy.15 Additionally, NACT has been found to enhance the sedative effects of propofol during induction and prolong its duration of action during surgery.16 Furthermore, abnormalities in voltage-gated Na+ channel function induced by NACT can lead to changes in neuromuscular excitability, thereby affecting muscle relaxation and the dosage required for muscle relaxants.17,18 Current research on the effects of NACT on intraoperative anesthetic agents has primarily focused on sedatives and neuromuscular relaxants, while studies examining its impact on analgesics remain limited. However, adequate analgesia is an essential component of the perioperative period. Chemotherapeutic agents, as cytotoxic stimuli, affect the neuro-immuno-endocrine system, causing damage to nociceptive Aδ and C fibers through mechanisms such as mitochondrial dysfunction, increased oxidative stress, and neuroinflammatory responses, ultimately leading to heightened pain sensitivity.19,20 Wang et al21 demonstrated that neoadjuvant PD-1 inhibitor therapy increases perioperative opioid consumption and postoperative pain in non-small-cell lung cancer (NSCLC) patients, while Sarkar et al reported a higher neuropathy risk (elevated movement-related VAS scores) in patients receiving NACT.22
Remifentanil is a potent, ultra-short-acting synthetic opioid analgesic primarily used for intraoperative anesthesia maintenance. Unlike conventional analgesics that undergo hepatic and renal metabolism, remifentanil is primarily hydrolyzed by non-specific esterases in plasma and tissues. This metabolic feature endows remifentanil with a rapid degradation profile (short context-sensitive half-time) and enhanced controllability, making it more suitable than other analgesics for observing differences in analgesic dosing among diverse patient populations. In clinical practice, we observed that patients undergoing NACT required a higher remifentanil dosage compared with those who did not receive NACT. Notably, previous studies have rarely focused on the impact of NACT on remifentanil efficacy in patients with ovarian cancer. Our study demonstrates that patients who received preoperative NACT required a significantly higher remifentanil dosage compared with those who did not undergo preoperative NACT. This finding suggests that NACT may affect the analgesic efficacy of remifentanil. A comprehensive understanding of the impact of NACT on remifentanil is crucial for anesthesiologists to achieve more effective intraoperative pain management and reduce postoperative complications.
Although relevant literature is scarce, indirect evidence suggests that preoperative NACT agents (eg, paclitaxel, carboplatin) for ovarian cancer are closely associated with the development of neuropathic pain.23 Specifically, these chemotherapeutic agents upregulate perioperative inflammatory cytokines, including IL-1, IL-6, IL-8, TNF-α, and IL-β, which in turn activate transient receptor potential ankyrin 1 (TRPA1)—a polymodal, non-selective cation-permeable channel expressed in nociceptors and implicated in chemotherapy-induced peripheral neuropathy as well as other painful neuropathic conditions—thereby enhancing TRPA1-mediated signaling. Concurrently, NACT agents induce “calcium overload” through distinct mechanisms: paclitaxel inhibits microtubule depolymerization to block mitosis,24 carboplatin disrupts endoplasmic reticulum calcium pump function and reduces mitochondrial calcium uptake,25 and paclitaxel further activates mitochondrial permeability transition pores, leading to rapid mitochondrial depolarization and disrupted Ca2⁺ release from both mitochondria and the endoplasmic reticulum, which ultimately contributes to neuronal damage.26 This abnormal elevation in intracellular calcium concentrations alters presynaptic membrane potential by inhibiting calcium-dependent potassium channels and activating calcium-dependent sodium channels, impairing opioid receptor signal transduction.
Additionally, the dorsal root ganglion (DRG)—a primary center for nociceptive signaling critical to the onset and maintenance of acute and chronic neuropathic pain27—undergoes morphological changes in neuron nuclei following NACT exposure, resulting in reduced opioid receptor expression; recent studies28,29 have further shown that increased methylation of the μ-opioid receptor gene (Oprm1) promoter, coupled with recruitment of epigenetic regulators such as methyl-CpG binding protein 2 (MeCP2) and histone deacetylase 1 (HDAC1), modulates promoter acetylation status to downregulate neuronal μ-opioid receptor expression.
Moreover, multiple studies29,30 have identified Sigma-1 receptor activation as a key driver of neuropathic pain, which inhibits endogenous opioid analgesia and promotes mechanical allodynia and pathological pain, with platinum-based NACT agents potentially enhancing this inhibitory effect to reduce patient sensitivity to opioids.31 Furthermore, inflammatory mediator secretion induced by NACT directly or indirectly activates pain receptors linked to mechanical allodynia and thermal hyperalgesia, leading to pain sensitization.
Collectively, these interconnected mechanisms—TRPA1 activation, calcium homeostasis disruption, impaired opioid receptor signaling, reduced opioid responsiveness, and disrupted endogenous analgesic pathways—diminish the analgesic efficacy of opioids, thereby increasing the requirement for analgesic medications during surgery and the postoperative period. Notably, further basic research is needed to clarify the specific correlation between ovarian cancer NACT agents and Sigma-1 receptors, as existing investigations have focused primarily on oxaliplatin.
Statistical analysis of the secondary outcomes indicated that MAP and HR in the experimental group were significantly higher at T3, T4, and T5 compared with the control group (P < 0.05). These time points—tracheal intubation (T3), 1 minute after intubation (T4), and the end of surgery (T5)—represent major perioperative nociceptive stimuli. The observed differences in MAP and HR suggest that patients receiving NACT exhibit increased sensitivity to painful stimuli, leading to a higher demand for analgesics.
Although we adjusted the remifentanil dosage when IOC2 exceeded 45, baseline analgesia inadequacy (eg, reduced opioid receptor availability28) may have influenced the observed outcomes. The frequency of adjustments to the plasma target concentration based on IOC2 in the experimental group was significantly higher than in the control group, further indicating that NACT patients are more sensitive to analgesic interventions, resulting in more frequent adjustments.
Postoperative data from this study indicate that NACT increased the effective button presses, total presses, and usage of the PCIA pump within 72 hours in ovarian cancer patients, without significantly increasing pain-related adverse effects. Various inflammatory responses, neural remodeling, and reductions in opioid receptor expression caused by NACT may enhance pain perception, thereby resulting in a greater requirement for analgesics to manage postoperative pain. However, there were no significant differences in postoperative VAS scores between the two groups, likely due to the increased use of the PCIA pump in patients receiving NACT, which may have reduced overall postoperative pain intensity. This study found no significant differences in the intraoperative doses of propofol and benzodiazepines, while remifentanil consumption differed significantly. This finding indicates that NACT has a more pronounced impact on analgesic needs than on sedative requirements.
In our study, we selected IOC2 (qNOX) as a quantitative measure to monitor analgesia levels in patients under general anesthesia. Unlike analgesia monitoring techniques such as the analgesia nociception index (ANI)32 and skin conductance (SC),33 which rely on peripheral vasoconstriction and cardiac autonomic activity, IOC2 calculates the amplitudes of theta and delta frequency bands in EEG signals. This method is less affected by vasoactive medications and heart rate fluctuations. Previous studies10,34,35 have indicated that IOC2 can reflect patients’ sensitivity to nociceptive stimuli in an unconscious state, offering advantages such as non-invasiveness, real-time monitoring, continuous assessment, and quantification. The real-time adjustment of remifentanil dosage through IOC2 monitoring allows for more effective intraoperative pain management while minimizing interference from different analgesic effects. No statistically significant differences were observed in postoperative outcomes between the groups; however, prompt intraoperative adjustments based on IOC2 improved postoperative recovery quality. Additionally, adjusting the propofol target concentration using IOC1 showed no significant differences in extubation and awakening times, indicating its efficacy in monitoring intraoperative depth of consciousness.
This study has some limitations. (1) Pain perception is subjective and influenced by factors like age, psychological state, and emotions; these were not considered in the analysis, which may impact VAS scores. (2) The study lacked long-term follow-up, necessitating further research on the impact of NACT on long-term sensitivity to postoperative pain. (3) Considering the interaction between propofol and remifentanil, lower doses of propofol may increase the demand for remifentanil. Although we adjusted the propofol dosage to achieve an appropriate anesthetic depth for the surgery (ie, maintaining the IOC1 value within the range of 40–60), this adjustment may still introduce a potential bias in the intraoperative average consumption of remifentanil.
Conclusion
In ovarian cancer patients undergoing NACT, the average intraoperative dose of remifentanil was significantly increased by approximately 26.49%. This finding suggests that NACT may reduce the analgesic efficacy of remifentanil, indicating that clinicians should appropriately increase the dosage of remifentanil to alleviate intraoperative nociceptive stimuli. Furthermore, analgesic requirements within 72 hours postoperatively were also elevated in patients who received NACT, highlighting the necessity of enhanced postoperative pain management in this patient population. This goal can be achieved by optimizing the parameters of postoperative analgesia pumps, adopting multimodal analgesic strategies, or performing nerve blocks. However, careful consideration is essential to avoid potential complications associated with excessive analgesia.
Data Sharing Statement
The datasets supporting the conclusions of this article are included within the article. Deidentified individual participant data will be provided. The data supporting this study are available from the corresponding author (Lianbing Gu, [email protected]) upon reasonable request.
Consent for Publication
All authors have approved the manuscript and consent to its publication in Drug Design, Development and Therapy. The authors also confirm that the manuscript is free from any conflicts of interest and that no individuals’ privacy rights are violated in this work.
Acknowledgments
The authors are immensely grateful to the patients in the study. We also thank the physicians of the Department of Anesthesiology and the Department of Gynecologic Surgery of Jiangsu Cancer Hospital for their support in the execution of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Qunfeng Project of Jiangsu Cancer Hospital [DFXK202503].
Disclosure
The authors report no conflicts of interest in this work.
References
1. González-Martín A, Harter P, Leary A, et al; ESMO Guidelines Committee. Electronic address: [email protected]. Newly diagnosed and relapsed epithelial ovarian cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann Oncol. 2023;34(10):833–14. doi:10.1016/j.annonc.2023.07.011
2. Jokhadze N, Das A, Dizon DS. Global cancer statistics: a healthy population relies on population health. CA Cancer J Clin. 2024;74(3):224–226. doi:10.3322/caac.21838
3. Armstrong DK, Alvarez RD, Backes FJ, et al. NCCN guidelines® insights: ovarian cancer, version 3.2022. J Natl Compr Canc Netw. 2022;20(9):972–980. doi:10.6004/jnccn.2022.0047
4. Sambasivan S. Epithelial ovarian cancer: review article. Cancer Treat Res Commun. 2022;33:100629. doi:10.1016/j.ctarc.2022.100629
5. Wright AA, Bohlke K, Armstrong DK, et al. Neoadjuvant chemotherapy for newly diagnosed, advanced ovarian cancer: society of gynecologic oncology and American society of clinical oncology clinical practice guideline. Gynecol Oncol. 2016;143(1):3–15. doi:10.1016/j.ygyno.2016.05.022
6. First-line chemotherapy for newly diagnosed epithelial ovarian cancer. Chin J Pract Gynecol Obstetr. 2021;37(6):613–616.
7. Coleridge SL, Bryant A, Kehoe S, Morrison J. Neoadjuvant chemotherapy before surgery versus surgery followed by chemotherapy for initial treatment in advanced ovarian epithelial cancer. Cochrane Database Syst Rev. 2021;7(7):CD005343. doi:10.1002/14651858.CD005343.pub6
8. Loizzi V, Leone L, Camporeale A, et al. Neoadjuvant chemotherapy in advanced ovarian cancer: a single-institution experience and a review of the literature. Oncology. 2016;91(4):211–216. doi:10.1159/000447743
9. Zhao D, Wu LY, Wang XB, et al. Role of neoadjuvant chemotherapy in the management of advanced ovarian cancer. Asian Pac J Cancer Prev. 2015;16(6):2369–2373. doi:10.7314/APJCP.2015.16.6.2369
10. Wang X, Zhang S, Wang C, et al. Real-time evaluation of the independent analgesic efficacy of dexmedetomidine. BMC Anesthesiol. 2023;23(1):68. doi:10.1186/s12871-023-02022-2
11. Zhao J, Kang Z, Xie W, Lin H, Liu Y. Effects of depth of anesthesia monitored by IoC on patients undergoing laparoscopic radical resection of colorectal cancer. MolTher Methods Clin Dev. 2020;18:304–311. doi:10.1016/j.omtm.2020.05.032
12. Saugel B, Fletcher N, Gan TJ, Grocott MPW, Myles PS, Sessler DI. PeriOperative quality initiative XI (POQI XI) workgroup members. perioperative quality initiative (POQI) international consensus statement on perioperative arterial pressure management. Br J Anaesth. 2024;133(2):264–276. doi:10.1016/j.bja.2024.04.046
13. Kusumoto FM, Schoenfeld MH, Barrett C. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a Report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart rhyth. Circulation. 2019;140(8):E382–E482. doi:10.1161/CIR.0000000000000628
14. Vergote I, Coens C, Nankivell M, et al; EORTC; MRC CHORUS study investigators. Neoadjuvant chemotherapy versus debulking surgery in advanced tubo-ovarian cancers: pooled analysis of individual patient data from the EORTC 55971 and CHORUS trials. Lancet Oncol. 2018;19(12):1680–1687. doi:10.1016/S1470-2045(18)30566-7
15. Wang Q, Zheng H, He Z, Zhang M. Determination of the minimum alveolar concentration of sevoflurane in patients diagnosed as gastric carcinoma and treated with neoadjuvant chemotherapy. J Clin Anesthesiol. 2018;34(3):238–240.
16. Yong F, Jia H, Wang H, Li C, Du W. Effect of neoadjuvant chemotherapy for ovarian cancer on sedative potency of propofol and oxycodone for anesthesia induction. Chinese Journal of Anesthesiol. 2019;39(1):71–73.
17. Park SB, Lin CS, Krishnan AV, Goldstein D, Friedlander ML, Kiernan MC. Dose effects of oxaliplatin on persistent and transient Na+ conductances and the development of neurotoxicity. PLoS One. 2011;6(4):e18469. doi:10.1371/journal.pone.0018469
18. Wang T, Li X, Ma F. Effect of neoadjuvant chemotherapy on the rocuronium muscle relaxation in breast cancer patients. J Clin Anesthesiol. 2020;36(11):1091–1095.
19. Cheng XL, Liu HQ, Wang Q, Huo JG, Wang XN, Cao P. Chemotherapy-induced peripheral neurotoxicity and complementary and alternative medicines: progress and perspective. Front Pharmacol. 2015;6:234. doi:10.3389/fphar.2015.00234
20. Kanat O, Ertas H, Caner B. Platinum-induced neurotoxicity: a review of possible mechanisms. World J Clin Oncol. 2017;8(4):329–335. doi:10.5306/wjco.v8.i4.329
21. Wang K, Er J, Zhang Y, et al. Increased opioid consumption in neoadjuvant immunotherapy plus chemotherapy for patients with non-small-cell lung cancer: a multicenter, prospective cohort study. CNS Neurosci Ther. 2024;30(8):e14893. doi:10.1111/cns.14893
22. Sarkar S, Pal R, Mahata S, et al. Evaluation of numerical rating scale and neuropathic pain symptom inventory pain scores in advanced ovarian carcinoma patients undergoing surgery and first-line chemotherapy. J Clin Trans Res. 2022;8(1):54–60.
23. Marcotti A, Fernández-Trillo J, González A, et al. TRPA1 modulation by Sigma-1 receptor prevents oxaliplatin-induced painful peripheral neuropathy. Brain. 2023;146(2):475–491. doi:10.1093/brain/awac273
24. Moustafa-Kamal M, Kucharski TJ, El-Assaad W, et al. The mTORC1/S6K/PDCD4/eIF4A axis determines outcome of mitotic arrest. Cell Rep. 2020;33(1):108230. doi:10.1016/j.celrep.2020.108230
25. Guo Y, Jin S, Yuan H, et al. DNA-unresponsive platinum(II) complex induces ERS-mediated mitophagy in cancer cells. J Med Chem. 2022;65(1):520–530. doi:10.1021/acs.jmedchem.1c01690
26. Management TR. Expert consensus on standardized management of taxane-related peripheral neuropathy. Chin J Oncol. 2020;42(3):170–179. doi:10.3760/cma.j.cn112152-20200203-00062
27. Eldridge S, Guo L, Hamre J. A comparative review of chemotherapy-induced peripheral neuropathy in in vivo and in vitro models. Toxicol Pathol. 2020;48(1):190–201. doi:10.1177/0192623319861937
28. Sun N, Yu L, Gao Y, et al. MeCP2 epigenetic silencing of oprm1 gene in primary sensory neurons under neuropathic pain conditions. Front Neurosci. 2021;15:743207. doi:10.3389/fnins.2021.743207
29. Ruiz-Cantero MC, Cortés-Montero E, Jain A, et al. The sigma-1 receptor curtails endogenous opioid analgesia during sensitization of TRPV1 nociceptors. Br J Pharmacol. 2023;180(8):1148–1167. doi:10.1111/bph.16003
30. Bruna J, Videla S, Argyriou AA, et al. Efficacy of a novel sigma-1 receptor antagonist for oxaliplatin-induced neuropathy: a randomized, double-blind, placebo-controlled phase iia clinical trial. Neurotherapeutics. 2018;15(1):178–189. doi:10.1007/s13311-017-0572-5
31. Desforges AD, Hebert CM, Spence AL, et al. Treatment and diagnosis of chemotherapy-induced peripheral neuropathy: an update. Biomed Pharmacother. 2022;147:112671. doi:10.1016/j.biopha.2022.112671
32. Hickey A, O’Gara Á, Lavelle A. Analgesia nociception index for intra-operative remifentanil dose and pain after gynaecological laparotomy. Anaesthesia. 2023;78(10):1304. doi:10.1111/anae.16065
33. Hu J, Harrold J, Squires JE, Modanloo S, Harrison D. The validity of skin conductance for assessing acute pain in mechanically ventilated infants: a cross-sectional observational study. Eur J Pain. 2021;25(9):1994–2006. doi:10.1002/ejp.1816
34. Wang XH, Zhang SY, Huang Y, et al. Multimodal analgesia with sevoflurane provides enhanced intraoperative analgesic effects in percutaneous nephrolithotomy: a randomized, blinded clinical trial. Pain Physician. 2022;25(3):283–291.
35. Cao S, Kan M, Jia Y, Wang C, Wang T. Index of Consciousness monitoring may effectively predict and prevent circulatory stress induced by endotracheal intubation under general anesthesia: a prospective randomized controlled trial. BMC Anesthesiol. 2024;24(1):316. doi:10.1186/s12871-024-02701-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.