Back to Journals » International Journal of Women's Health » Volume 17
The Correlation Between Fetal Wellbeing and Umbilical Doppler Parameters in Pregnant Women with Gestational Hypertension
Authors Lin H, Shen M, Li D, Sun Q, Lan L
Received 26 December 2024
Accepted for publication 20 March 2025
Published 9 April 2025 Volume 2025:17 Pages 1009—1018
DOI https://doi.org/10.2147/IJWH.S514427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Hualan Lin, Meifang Shen, Dongbei Li, Qiuxia Sun, Liubing Lan
Obstetrical Department, Meizhou people’s Hospital, Meizhou City, Guangdong Province, 514000, People’s Republic of China
Correspondence: Liubing Lan, Obstetrical Department, Meizhou people’s Hospital, No. 23, Huangtang Road, Meijiang District, Meizhou City, Guangdong Province, 514000, People’s Republic of China, Email [email protected]
Objective: To investigate the role of umbilical cord blood flow parameters in evaluating intrauterine fetal hypoxia and fetal growth restriction in pregnant women with gestational hypertension.
Methods: One hundred and nine patients with gestational hypertension admitted from January 2020 to December 2023 were enrolled in this study. The peak systolic velocity/end diastolic velocity (S/D), pulse index (PI) and resistance index (RI) of cord blood were measured by ultrasound. According to the S/D, 109 cases were divided into 62 cases in the control group (S/D < 3) and 47 cases in the observation group (S/D ≥ 3), and the prognosis of pregnant women and fetuses in the two groups were compared. The ROC curves were used to analyze the effects of different parameters of umbilical blood flow on intrauterine fetal hypoxia and fetal growth restriction in pregnant women with gestational hypertension.
Results: The incidence of intrauterine fetal hypoxia, fetal growth restriction, cesarean section, and unresponsive type of non-irritation test was decreased in the control group compared with the observation group (P < 0.05). However, there was no statistical difference in the incidence of neonatal asphyxia between the two groups (P > 0.05). ROC curve analysis showed that cord blood flow RI of pregnant women with gestational hypertension had the highest sensitivity and AUC in predicting intrauterine fetal hypoxia and growth restriction, and PI had the highest specificity in predicting intrauterine fetal growth restriction. The specificity of S/D, PI and RI in predicting intrauterine hypoxia was consistent (all 80%).
Conclusion: The different parameters of umbilical blood flow in hypertensive pregnant women during pregnancy provide a good assessment of intrauterine fetal condition and can be used as clinical indicators to predict poor prognosis of intrauterine fetal hypoxia and fetal growth restriction.
Keywords: gestational hypertension, hypoxia, growth restriction, umbilical blood flow, assessment
Introduction
Gestational hypertension is defined as the development of high blood pressure (≥140/90 mmHg) after 20 weeks of gestation in a previously normotensive woman, without the presence of proteinuria. Gestational hypertension develops during pregnancy and is a relatively common clinical complication of pregnancy.1 According to the literature, the prevalence of this disease varies between countries and regions.2 In China, the incidence of gestational hypertension is high, ranging from 7.9% to 10.4%.3 Gestational hypertension can trigger an insufficient blood supply to the placenta, leading to decreased placental function, fetal hypoxia, growth restriction, intrauterine distress, and preterm delivery, thereby causing obstacles in fetal oxygen and nutrient supply and intrauterine fetal development retardation.4,5 Among them, the incidence of fetal preterm labor is higher in patients with gestational hypertension. The causes and pathogenesis of gestational hypertension are not well understood. However, hypertensive disorders of pregnancy pose a threat to the health and safety of the pregnant woman and the fetus, and are one of the major causes of adverse pregnancy outcome.6 Serious complications in pregnant women with gestational hypertension are cardiac failure, renal failure and cerebrovascular disease.7 Clinical management of gestational hypertension is mainly symptomatic to control blood pressure and terminate pregnancy if necessary.8 Studies have shown that preterm infants with gestational hypertension are significantly more likely to develop extrauterine growth retardation after birth.9–11 On the one hand, preterm infants born to hypertensive women are at higher risk of postnatal complications than preterm infants born to healthy mothers, which affects the growth and development of preterm infants to a certain extent.12,13 Under the influence of various unfavorable factors, fetal growth and development are restricted, which is clinically manifested in the reduction of placental chorionic vascular branches and the increasing resistance to blood flow in the placenta. If there is a placental circulation disorder, it can lead to fetal ischemia and hypoxia symptoms in the development process, leading to intrauterine hypoxia, neonatal asphyxia and other adverse pregnancy outcomes.14
How to monitor the condition of the fetus in pregnant women with gestational hypertension, detect intrauterine hypoxia in time, and provide timely and effective interventions and treatments have become the top priority for obstetricians and gynecologists in their clinical work. Fetal heart rate monitoring has a certain diagnostic value for intrauterine fetal conditions.15 With the progress and development of ultrasound technology, umbilical blood flow detection has also been gradually applied to prenatal examination.16 Color ultrasound monitoring of fetal umbilical artery blood flow S/D value has the advantages of non-invasive, simple and accurate, which is one of the most important parameters for detecting umbilical artery blood flow. Color ultrasound monitoring can be used to understand placental function by measuring the ratio of peak end-systolic (S) to peak end-diastolic (D) values of the umbilical artery. It can reflect the blood circulation and oxygen reserve level of the fetus in the mother during pregnancy. And the magnitude of the S/D value can reflect the presence and severity of intrauterine hypoxia in the fetus, which is closely related to the maternal outcome of pregnancy. This monitoring tool can effectively reflect the safety of the fetus in the womb and alert obstetricians and gynecologists to take timely, effective and appropriate interventions.
By determining the S/D ratios in both the gestational hypertension and control groups, we analyzed the temporal trend of S/D values throughout gestation, thereby providing insights into the hemodynamic changes associated with gestational hypertension. The aim of this study is to raise awareness of the importance of fetal umbilical artery blood flow monitoring in pregnant women with gestational hypertension. While monitoring blood pressure, the monitoring of fetal umbilical artery blood flow was emphasized. Timely assessment of fetal condition in utero reduces the incidence of adverse maternal and neonatal outcomes.
Methods
General Information About Patients
A total of 109 pregnant women with gestational hypertensive admitted from January 2020 to December 2023 who met the inclusion and exclusion criteria were selected. Based on S/D, 109 cases of gestational hypertension were categorized into the control group (S/D < 3, 62 cases) and the observation group (S/D ≥ 3, 47 cases).17 In the control group, the age range was 19–46 years (31.89 ± 5.75 years), and the gestational age ranged from 34 to 40 weeks (36.21 ± 2.28 weeks). In the observation group, the age range was 22–42 years (31.96 ± 4.85 years), and the gestational age ranged from 34 to 40 weeks (35.45 ± 3.40 weeks). The baseline table shows the comparability over the two baselines (P > 0.05) (Table 1) The study was approved by the Medical Ethics Committee of the hospital, and the patients and/or their families gave their informed consent to the study and signed the consent form.
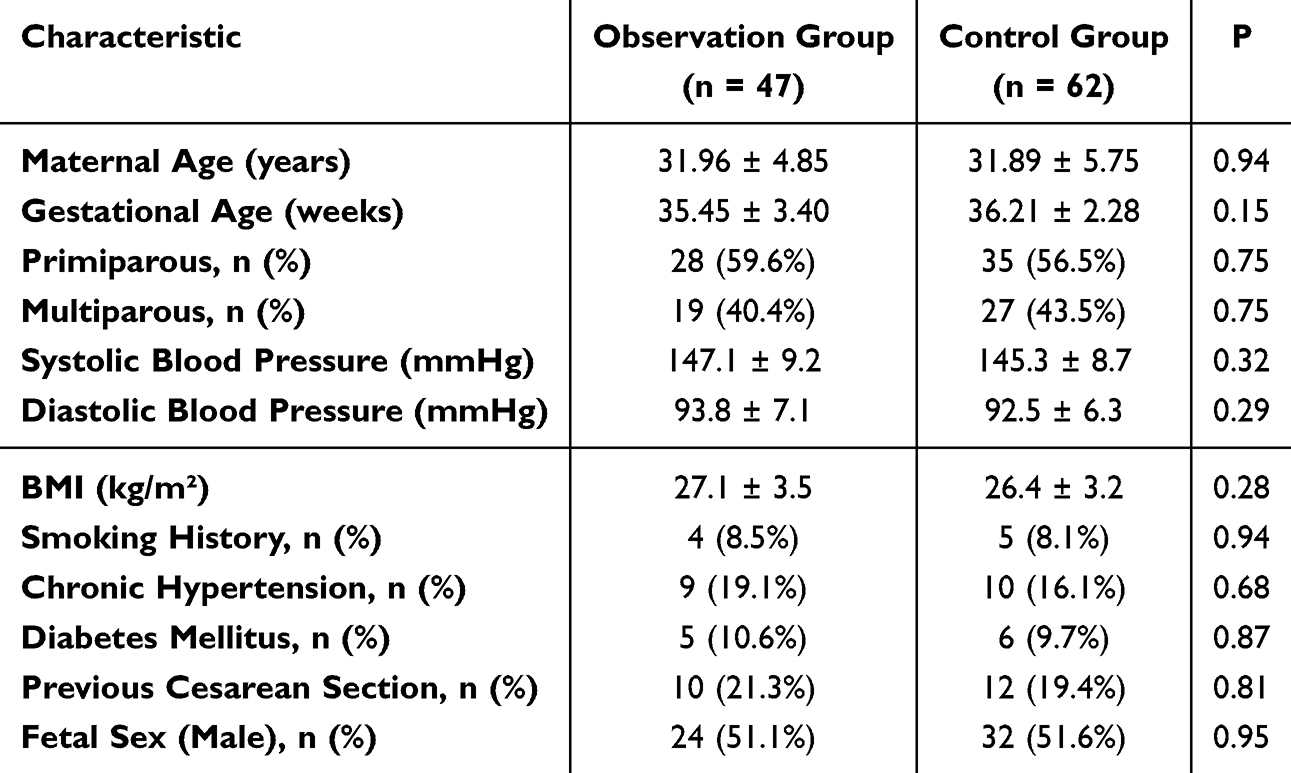 |
Table 1 Baseline Characteristic |
 |
Table 2 Comparison of Maternal and Fetal Outcomes of Gestational Hypertension with Different Umbilical Blood Flow S/D |
 |
Table 3 Comparison of Different Parameters of Umbilical Blood Flow in Intrauterine Fetus with or Without Hypoxia |
Inclusion and Exclusion Criteria
Inclusion criteria: (1) Met the diagnostic criteria for gestational hypertension, defined as a new onset of hypertension (systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg) occurring after 20 weeks of gestation. Blood pressure must be measured on at least two separate occasions, with a minimum interval of 4 hours between readings, in a woman with previously normal blood pressure, and without evidence of significant proteinuria (urine protein <300 mg in a 24-hour urine collection).; (2) All were singleton pregnancies by ultrasonography.
Exclusion criteria: (1) Ultrasonographic detection of fetal malformations; (2) Patients in active labor at the time of examination; (3) Patients presenting with severe hypertensive complications (eg, severe headache, visual disturbances, HELLP syndrome, or eclampsia) that could affect hemodynamic measurements; (4) Patients with additional systemic diseases (eg, renal, hepatic, or cardiovascular disorders) that might influence pregnancy outcomes or confound umbilical blood flow assessment (Figure 1).
 |
Figure 1 Inclusion and Exclusion Flowchart. |
Examination Methods
Umbilical cord blood flow test: Cord blood flow was measured in late pregnancy in both groups. GE Voluson E10 4-dimensional color ultrasound machine (manufactured by GE Healthcare, Milwaukee, WI, USA; produced in 2014) was used, with the probe frequency set at 3.5 MHz. The pregnant women emptied their bladders and lay down in a flat position. The probe was placed on the abdomen to examine the development of fetal organs. At the same time, the sonogram of umbilical artery blood flow is probed on the ventral side of the fetus, and the waveform is frozen when a typical and stable waveform appears. The S/D, pulse index (PI) and resistance index (RI) of cord blood flow were recorded by the same spectrogram with more than five peaks and valleys, and the average value was taken for three consecutive measurements.
Fetal heart rate monitoring: Fetal heart rate monitoring was performed in both groups using an MFM-CNSF200 fetal heart rate monitor manufactured by Edan Instruments, Inc. (Shenzhen, China). The MFM-CNSF200 is a multi-function obstetric monitor designed specifically for simultaneous recording of fetal heart rate and maternal uterine contractions. Key specifications include: Model: MFM-CNSF200; Channels: 3-channel monitoring; Sampling Frequency: 4 hz with a resolution of 2 ms; Display: 8-inch full-color LCD for clear visualization; Data Storage & Transfer: Built-in storage (1 GB capacity) with USB connectivity for data export and subsequent analysis; Production Year: 2017. This monitor meets international quality and safety standards, ensuring reliable performance in clinical obstetric applications. The pregnant women were placed in a semi-recumbent position and underwent the non-stimulation test (NST) for 20 min, which was extended to 40 min in case of abnormality.
Observation Indicators
The prognosis of pregnant women and fetuses in the control and observation groups was compared. According to whether the fetus was hypoxic or not, 109 cases were divided into the group of hypoxic fetus and normal fetus. The 109 cases of gestational hypertension were divided into the fetal growth restriction group and the normal fetal growth group according to whether the fetal growth was restricted or not. Different parameters of umbilical blood flow (S/D, PI, RI) were observed and compared between the intrauterine fetal hypoxia group and the intrauterine fetal normal group, as well as between the fetal growth-restricted group and the fetal growth-normal group, respectively. The predictive value of different parameters of umbilical cord blood flow in hypertensive pregnant women during pregnancy on intrauterine fetal hypoxia and fetal growth restriction and their correlation with poor fetal prognosis were analyzed.
The fetal prognosis was as follows:
(1) Intrauterine fetal hypoxia: a. Fetal heart rate (FHR) < 120/min or > 160/min; b. There was variable deceleration, late deceleration, abnormal oxytocin provocation test or uterine stress test on fetal heart monitoring; c. Acidosis was present, when fetal scalp blood gas analysis showed a pH of less than 7.20, a partial pressure of arterial oxygen of less than 10 mmHg, and a partial pressure of arterial carbon dioxide of more than 60 mmHg; d. The Apgar score of neonates was ≤7 at 1 min after birth. The presence of any of the above was defined as intrauterine fetal hypoxia. (2) Fetal growth restriction: a. Maternal uterine height and abdominal circumference <10th percentile by 3 weeks continuous measurement; b. Fetal abdominal circumference and head circumference <10th percentile by ultrasound; c. The mean values of fetal biparietal diameter and femoral length were less than 2 standard deviations. Fetal growth restriction is defined as any of the above. (3) Diagnostic criteria for fetal heart rate monitoring: NST reactive is defined as a baseline fetal heart rate of 120–160/min, fine variant amplitude of >6 beats per minute, or ≥3 fetal movements in 20 min, accompanied by acceleration of the fetal heart rate with an amplitude of ≥15/min and a duration of ≥15s. NST unresponsive is defined as a 40-min period of fetal heart rate monitoring with no fetal movement or no acceleration of the fetal heart rate in the case of fetal movement, accompanied by the disappearance of the long variant of the baseline fetal heart rate. NST non-responsive indicates abnormal fetal heart rate monitoring. The presence of intrauterine fetal hypoxia, fetal growth restriction, or neonatal asphyxia was considered a poor prognosis for the fetus.
Statistical Methods
SPSS 27.0 was used to analyze all the data. Enumeration data were compared by χ2 test and expressed as rate (%). The measurement data were analyzed by independent sample t test and expressed as ( ). Receiver operating characteristic (ROC) curve was used to analyze the predictive value of umbilical blood flow parameters in pregnant women with gestational hypertension for intrauterine fetal hypoxia and growth restriction.
). Receiver operating characteristic (ROC) curve was used to analyze the predictive value of umbilical blood flow parameters in pregnant women with gestational hypertension for intrauterine fetal hypoxia and growth restriction.
Results
Comparison of Maternal and Fetal Outcomes
Table 2 shows the maternal and fetal outcomes in the two groups. Compared with the observation group, the incidence of intrauterine fetal hypoxia, fetal growth restriction, cesarean section and NST non-response was significantly decreased in the control group (P < 0. 05). This result indicated that abnormal S/D value implied intrauterine hypoxia and growth restriction.
Intrauterine Fetal Hypoxia and Umbilical Blood Flow Parameters
Table 3 and Figure 2 demonstrate the results of cord blood flow parameters for both groups. S/D, PI and RI of umbilical blood flow in intrauterine fetal hypoxia group were significantly higher than those in intrauterine fetal normal group (P < 0. 01). High S/D, PI and RI suggested intrauterine hypoxia.
 |
Figure 2 Comparison of S/D (A), PI (B), and RI (C) between intrauterine hypoxic and non-hypoxic fetuses. |
Results of Pathological Features
S/D, PI and RI of umbilical blood flow in the intrauterine fetal growth restriction group were significantly higher than those in the normal intrauterine fetal growth group (Table 4 and Figure 3, P < 0.05). High S/D, PI and RI may indicate fetal growth restriction.
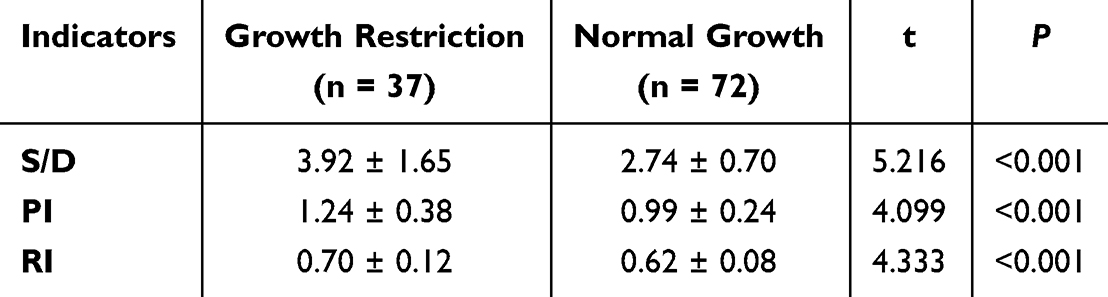 |
Table 4 Comparison of Cord Blood Flow Parameters in Fetuses with or Without Growth Restriction |
 |
Figure 3 Comparison of S/D (A), PI (B), and RI (C) between fetal growth restriction and normal fetal growth. ***P < 0.001. |
Effect of Umbilical Blood Flow Parameters on Fetal Hypoxia
ROC curve analysis showed that RI of cord blood flow in pregnant women with gestational hypertension had the highest sensitivity in evaluating intrauterine fetal hypoxia. The specificity of S/D, PI and RI in predicting intrauterine hypoxia was consistent (all 80%). And RI had the highest area under the curve (AUC, 0.881) in predicting intrauterine fetal hypoxia (Table 5 and Figure 4).
 |
Table 5 Evaluation of Fetal Hypoxia by Different Parameters of Umbilical Blood Flow |
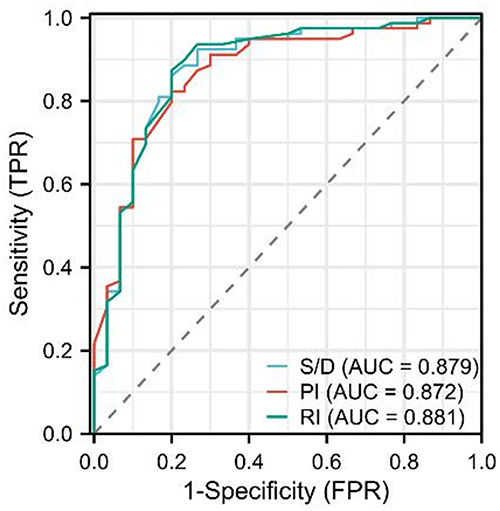 |
Figure 4 ROC curve of different parameters of umbilical blood flow for fetal hypoxia. |
Effect of Cord Blood Flow Parameters on Fetal Growth Restriction
ROC curve analysis showed that RI, S/D, and PI all demonstrated strong sensitivity values, and RI was the best (94.44%) and AUC (0.719) in predicting fetal growth restriction, and PI had the highest specificity (59.46%) in predicting fetal growth restriction (Table 6 and Figure 5).
 |
Table 6 Evaluation of Fetal Growth Restriction by Different Parameters of Umbilical Blood Flow |
 |
Figure 5 ROC curve of parameters of umbilical blood flow for fetal growth restriction. |
Discussion
Hypertension in pregnancy is one of the major causes of adverse maternal and infant outcomes.18 The pathology is characterized by spasm of small arteries throughout the body, increased vascular permeability, and plasma exudation leading to hypercoagulability of the blood.19 In addition, atherosclerosis of the blood vessels at the myometrium and meconium reduces the effective exchange area, resulting in impaired fetal-placental circulation, which seriously affects the normal development of the fetus.20 The impaired circulation between the mother and the fetus is manifested by changes in hemodynamic parameters. Fetal umbilical blood flow analysis is currently considered a safe method of evaluating placental function, nutrition, metabolism and blood supply.21 Therefore, blood flow-related parameters can be measured to reflect intrauterine fetal development in order to intervene in advance and improve pregnancy outcomes.
Ultrasound detection of fetal umbilical blood flow is a noninvasive and reproducible examination, which is widely used in prenatal examination.22 It can reflect the umbilical hemodynamic correlation and characteristics of fetal-placental circulatory resistance. Umbilical blood flow ultrasonography significantly improves the detection rate of intrauterine fetal abnormalities and provides objective indicators of fetal growth in utero.23 The umbilical cord is the link between the placenta and the fetus. In order to meet the needs of the growing fetus for more oxygen and nutrients, the resistance to blood flow in the umbilical artery decreases with gestational age.24 The establishment of utero-placental circulation is associated with pregnancy-induced hypercoagulability, platelets and their release of bioactive substances, and production of angiogenic factors by inflammatory cells.25 Hypercoagulability during pregnancy prevents women from miscarrying, reduces labor bleeding, and protects placental function. Hypercoagulability at the utero-placental interface contributes to placental hemostasis, but it may also make the placenta more susceptible to vascular complications.26 Low-pressure blood flow between the villi can trigger fibrin deposition in the placental micro vessel, resulting in microinfarcts. Stasis and hypoperfusion of the uteroplacental circulation may also lead to further thrombus formation in the umbilical vessels and fetal circulation. Abnormalities in coagulation may affect utero-placental circulation, and inadequate perfusion of terminal blood causes abnormal chorionic villus development and increased oxygen free radicals, leading to abnormal activation of inflammation and endothelial cell dysfunction in the maternal circulation. To a certain extent, S/D value can reflect the state of the uterus-placenta circulation, the changes in the general circulation of the fetus and the level of the oxygen reserve of the fetus in the maternal circulation and the intrauterine condition.17 In normal pregnancy, the placenta matures gradually with the increase in gestational weeks. Chorionic vessels thicken and increase, placental vascular resistance decreases, umbilical blood flow S/D decreases, and blood flow increases to ensure blood supply for normal fetal growth.27 The structure of placental chorionic vasculature changes as the disease progresses in pregnant women with gestational hypertension. Decreased number of small arteries, deposition of fibrous material, and atherosclerosis reduce blood flow between the fetus and the placenta, inhibit fetal growth and development, affect peak diastolic flow velocity in the umbilical artery, and lead to an abnormal increase in S/D. In this study, we grouped pregnant women with gestational hypertension according to umbilical blood flow S/D and found that the incidence of intrauterine fetal hypoxia, fetal growth restriction, cesarean section, and NST unresponsiveness were lower in the control group than in the observation group.
Abnormal increase in umbilical blood flow S/D may indicate fetal hypoxia or growth restriction, and early intervention is needed.28 In addition, PI and RI of cord blood flow are also effective indicators for evaluating fetal-placental circulation and intrauterine fetal development. In this study, S/D, PI and RI of umbilical blood flow in the intrauterine fetal hypoxia group were higher than those in the intrauterine fetal normal group, indicating that umbilical blood flow parameters have certain value in evaluating the poor prognosis of fetus, which is consistent with the report of Hidaka.29 The higher S/D, RI and PI of umbilical blood flow, the greater vascular resistance, the less blood flow, and the more serious intrauterine hypoxia, which can cause adverse effects on fetal development and health. ROC curve analysis showed that the AUC of S/D, PI and RI of cord blood flow in predicting intrauterine fetal hypoxia was 0.879, 0.872 and 0.881, respectively, and the sensitivity was 86.08%, 82.28% and 87.34%, respectively, indicating that different parameters of cord blood flow had high accuracy in predicting intrauterine fetal hypoxia. This study also found that the S/D, PI and RI of umbilical blood flow in the fetal growth restriction group were higher than those in the normal fetal growth group. The AUC of umbilical blood flow S/D, PI and RI in predicting fetal growth restriction was 0.715, 0.697 and 0.719, respectively, and the sensitivity was 93.06%, 80.56% and 94.44%, respectively. It is suggested that umbilical cord blood flow parameters also have high value in the evaluation of fetal growth restriction. Previous studies have found that umbilical blood flow S/D is associated with fetal growth restriction and also with blood concentration in response to increased umbilical artery resistance. Fan pointed out that in patients with fetal growth restriction, the placental blood flow circulation ratio was abnormally increased, the umbilical artery end-diastolic blood flow was decreased, and the umbilical artery S/D, RI, and PI values were significantly increased.30
In conclusion, the changes of fetal umbilical cord blood flow in pregnant women with gestational hypertension are closely related to the severity of the disease, which has certain value in predicting fetal adverse outcomes such as hypoxia and growth restriction, and can provide objective evidence for the evaluation of the condition and pregnancy outcome of pregnant women with gestational hypertension. However, there are still some shortcomings in this study, such as the sample size of the included studies is small, and the adverse outcomes of pregnant women with different severity of gestational hypertension are not further analyzed, which will reduce the credibility of the study to a certain extent. In the future, large sample size studies are still needed to provide evidence.
Conclusion
In pregnant women with gestational hypertension, elevated umbilical cord blood flow parameters, specifically S/D, RI, and PI, are indicative of fetal hypoxia and growth restriction. Our findings underscore the importance of early and comprehensive monitoring of these indices as critical indicators of adverse intrauterine conditions. Early identification of abnormal values can facilitate timely clinical intervention, thereby potentially improving fetal outcomes through proactive management or, when necessary, timely termination of the pregnancy.
Data Sharing Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Meizhou People's Hospital (Meizhou City Ethics Review 2020-C-137). Informed consent was obtained from all the participants. All methods were carried out in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Wang W, Fan D, Wang J, et al. Association between hypertensive disorders complicating pregnancy and risk of placenta accreta: a meta-analysis and systematic review. Hypertens Preg. 2018;37(3):168–174. doi:10.1080/10641955.2018.1498880
2. Yuriah S, Kartini F. Factors affecting with the prevalence of hypertension in pregnancy: scoping review. Hypertension. 2022;7:3.
3. Li F, Qin J, Zhang S, Chen L. Prevalence of hypertensive disorders in pregnancy in China: a systematic review and meta-analysis. Preg Hypertension. 2021;24:13–21. doi:10.1016/j.preghy.2021.02.001
4. Soobryan N, Kumar A, Moodley J, Mackraj I. The role and expression of pro/antiangiogenic factors and microRNAs in gestational hypertension and pre-eclampsia. Eur J Obstet Gynecol Reprod Biol. 2023;290:38–42. doi:10.1016/j.ejogrb.2023.09.012
5. Ozkan D, Ibanoglu MC, Adar K, et al. Efficacy of blood parameters in predicting the severity of gestational hypertension and preeclampsia. J Obstetrics Gynaecol. 2023;43(1):2144175. doi:10.1080/01443615.2022.2144175
6. Saumtally ZN, Chapman L, Perry H, Thilaganathan B, Khalil A. Cardiovascular function in women after experiencing a hypertensive disorder in pregnancy. Ultrasound Obstetrics Gynecol. 2017;50(S1):169. doi:10.1002/uog.18045
7. Clark SL, Saade GA, Tolcher MC, et al. Gestational hypertension and “severe” disease: time for a change. Am J Obstet Gynecol. 2023;228(5):547–552. doi:10.1016/j.ajog.2022.11.1280
8. Mayne SL, Yellayi D, Pool LR, Grobman WA, Kershaw KN. Racial residential segregation and hypertensive disorder of pregnancy among women in Chicago: analysis of electronic health record data. Am J Hypertens. 2018;31(11):1221–1227. doi:10.1093/ajh/hpy112
9. Grover S, Brandt JS, Ananth CV. Risks of preterm delivery and small for gestational age births associated with chronic hypertension. Ame J Obstetrics Gynecol. 2023;228(1):S578. doi:10.1016/j.ajog.2022.11.980
10. An H, Jin M, Li Z, et al. Impact of gestational hypertension and pre-eclampsia on preterm birth in China: a large prospective cohort study. BMJ Open. 2022;12(9):e058068. doi:10.1136/bmjopen-2021-058068
11. Liu C, Lu J, Liu C, Liu C, Liu C, Liu C. Analysis of extrauterine growth retardation and related risk factors in 132 premature infants. Pakistan J Med Sci. 2022;38(6):1644. doi:10.12669/pjms.38.6.5864
12. Nzelu D, Dumitrascu-Biris D, Hunt KF, Cordina M, Kametas NA. Pregnancy outcomes in women with previous gestational hypertension: a cohort study to guide counselling and management. Pregnancy Hypertens. 2018;12:194–200. doi:10.1016/j.preghy.2017.10.011
13. Darmstadt GL, Al Jaifi NH, Ariff S, et al. Research priorities for care of preterm or low birth weight infants: health policy. eClinicalMedicine. 2023;63. doi:10.1016/j.eclinm.2023.102126.
14. Khalil A, Beune I, Hecher K, et al. Consensus definition and essential reporting parameters of selective fetal growth restriction in twin pregnancy: a Delphi procedure. Ultrasound Obstet Gynecol. 2019;53(1):47–54. doi:10.1002/uog.19013
15. Wang J, Ma J, Hong S, et al. Signal quality index for the fetal heart rates: development and improvements for fetal monitoring. Expert Systems Appl. 2023;213. doi:10.1016/j.eswa.2022.119244.
16. Stampalija T, Monasta L, Barbieri M, et al. Late-term fetuses with reduced umbilical vein blood flow volume: an under-recognized population at increased risk of growth restriction. Eur J Obstet Gynecol Reprod Biol. 2022;272:182–187. doi:10.1016/j.ejogrb.2022.03.032
17. Netam SB, Singh A, Mandle H, et al. Best color Doppler indices in prediction of fetal hypoxia in IUGR fetuses. Int J Med Res Rev. 2015;3(9):1012–1019. doi:10.17511/ijmrr.2015.i9.187
18. Mussarat N, J. B Jr, Martin J, et al. Masked pregnancy-associated hypertension as a predictor of adverse outcomes. Ame J Obstetrics Gynecology MFM. 2023;5(7):100976. doi:10.1016/j.ajogmf.2023.100976
19. Prinja P, Nelson-Piercy C. Hypertension in pregnancy. Medicine. 2018;46(12):743–746. doi:10.1016/j.mpmed.2018.09.010
20. Liang Z, Wang L. Expression and clinical significance of lncRNA NORAD in patients with gestational hypertension. Ginekologia Polska. 2023;94(6):429–434. doi:10.5603/GP.a2022.0016
21. Kuckian P, Mahendru AA. Doppler ultrasound in obstetrics. Obstetrics Gynaecol Reprod Med. 2021;31(12):327–334. doi:10.1016/j.ogrm.2021.10.001
22. Song QY, Wen J, Luo H. Prenatal ultrasound findings regarding obstruction to blood flow and an umbilical artery varix caused by umbilical cord torsion. Eur J Obstet Gynecol Reprod Biol. 2022;269:144–146. doi:10.1016/j.ejogrb.2021.12.014
23. Cahill LS, Stortz G, Ravi Chandran A, et al. Wave reflections in the umbilical artery measured by Doppler ultrasound as a novel predictor of placental pathology. EBioMedicine. 2021;67:103326. doi:10.1016/j.ebiom.2021.103326
24. Song X, Liu C, Wang J, Yang X, Li M. Current perspectives on umbilical cord abnormalities including blood flow parameters based on ultrasound observations. Mol Cell Biomechanics. 2022;19(4):209–219. doi:10.32604/mcb.2022.026082
25. Dugalic S. Pathophysiology of Asphyxia in Pregnancy. In: Asphyxia in Neonates. CRC Press; 2024:17–38.
26. Jurisic A, Jurisic Z, Lefkou E, Pombo J, Girardi G. Pravastatin and-L-arginine combination improves umbilical artery blood flow and neonatal outcomes in dichorionic twin pregnancies through an nitric oxide-dependent vasorelaxant effect. Vascul Pharmacol. 2018;110:64–70. doi:10.1016/j.vph.2018.06.001
27. Dai W, Xu Y, Ma X-W, Zhang L, Zhu M-J. Ultrasonic characteristics and clinical significance of umbilical cord blood flow in acute fetal distress. J Acute Dis. 2016;5(6):483–487. doi:10.1016/j.joad.2016.07.003
28. Hidaka N, Sato Y, Kido S, Fujita Y, Kato K. Ductus venosus Doppler and the postnatal outcomes of growth restricted fetuses with absent end-diastolic blood flow in the umbilical arteries. Taiwan J Obstet Gynecol. 2017;56(5):642–647. doi:10.1016/j.tjog.2017.08.012
29. Fan H, Li L, Hao C. Clinical significance of three-dimensional power Doppler combined with two-dimensional Doppler ultrasonography for evaluating fetal growth restriction. J maternal-Fetal Neonatal Med. 2024;37(1):2322610. doi:10.1080/14767058.2024.2322610
30. Farsetti D, Pometti F, Tiralongo GM, et al. Distinction between SGA and FGR by means of fetal umbilical vein flow and maternal hemodynamics. J Maternal-Fetal Neonatal Med. 2022;35(25):6593–6599. doi:10.1080/14767058.2021.1918091
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.