Back to Journals » Open Access Journal of Clinical Trials » Volume 11
The Challenges In Conducting Research Studies In Arabic Countries
Authors Sheblaq N ![]() , Al Najjar A
, Al Najjar A
Received 14 May 2019
Accepted for publication 26 September 2019
Published 7 November 2019 Volume 2019:11 Pages 57—66
DOI https://doi.org/10.2147/OAJCT.S215738
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Arthur E. Frankel
Nagham Sheblaq,1 Amal Al Najjar2
1Oncology Department, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 2Security Force Hospital, Riyadh, Saudi Arabia
Correspondence: Nagham Sheblaq
The Ministry of National Guard Health Affairs, 14611 Ar rimayah, KSA-Riyadh, Kingdom of Saudi Arabia
Tel +966553014124
Email [email protected]
Background: The fraction of patients participating in clinical research studies has been relatively low and declined further in recent years, and many barriers are facing healthcare providers in conducting such studies. Our aim in this study is to identify common barriers facing our healthcare providers to conduct clinical trials in those patients in the MENA region.
Methods: A qualitative study was carried out between July 2014 and April 2015 where the semistructured survey was conducted using Survey Monkey software to all healthcare providers who work in seven different domain areas (physicians, pharmacists, nurses, clinical research associates, clinical research coordinators, auditors, and IRB members and data entry clerks).
Results: Of 329 responders from 7 specialties, the majority [183 (55.62%)] were males and 193 (58.66%) from Saudi Arabia. Physicians and pharmacists represent the majority [155 (47.11%) and 76 (23.10%)] of the total group, respectively, and the least were nurses and auditors [5 (1.52%) in each]. The highest rate barrier reported by physicians and pharmacists was inadequate training in clinical research implementation [76 (23.1%)], while clinical research coordinator reported the same barrier in 18 (5.5%). Clinical research associates reported a lack of incentive and credit for research work in 17 (5.2%). Reviewers reported a lack of leadership support and lack of financial grant support [5 (1.5%)] for both. The top reported strength points were having an opportunity for professional development [96 (29.2)] and being in an academic institution [97 (29.5)]. Of the total participants, 200 (60.79) of the participants suggested the need for more training on research methodology.
Conclusion: This study demonstrated the barriers that face healthcare providers in the MENA region. Because of the inadequate training in clinical research implementation and the lack of designed system operating procedures for the research process, we should address to facilitate clinical research in the region.
Keywords: clinical research in Arabic countries, barriers to participating, attitude, conducting research studies
Introduction
Scientific research is the most important thing that allows the creation of new guidelines for treating patients, and the success of a country’s development efforts depends upon the degree to which its planners and program managers use and apply research for decision-making.
Medical research involving human participants has increased greatly in many developing countries during the recent decade, motivated by the need to address the high burden of diseases in these countries. The ethical conduct of research specific to developing countries has been the subject of recent discussions1–3 and has been addressed in several research ethics guidelines.4,5
Healthcare providers’ and community awareness about the need for clinical research and the manner in which it is conducted is important, as there appears to be a relationship between knowledge/awareness and willingness to participate.6
Many studies have conducted in Western countries to detect the actual barriers facing healthcare providers in the research field,7–11 but there is not enough data about the barriers faced by researchers and health service providers in the Middle East. Therefore, our aim was to gather data about points of strength and weakness on institutions, which are interested in scientific medical research on the MENA region.
Such results included in western studies, however, might not be generalizable to developing countries that incorporate different ethnicity, religions, cultures, economic, and political backgrounds.
The main objectives of this study:
- Clarify the main barriers and challenges facing healthcare providers in Arabic countries.
- Make an association and relation between common barriers among healthcare providers and the MENA region.
- Provide information about strengths in Arabic countries in the research field.
Methods
Data were collected online using Survey Monkey software and sent to all healthcare providers who work in seven different domain areas (physicians, pharmacists, nurses, clinical research associates, clinical research coordinators, auditors, and IRB members and data entry clerks).
The tool composed of five major elements:
- The socio-demographic section includes questions asking about gender, region, work area, specialty, and age.
- Questions about barriers that every participant face at his/her institution/country that affects his/her role in the research field.
- Questions about the strengths and opportunities healthcare providers have at their institution/country that affect their role in the research field.
- What type of research study the participants have at their institution?
- Every healthcare provider was asked to give Suggestions to Improve Arab Countries Research Field.
The site IRB (King Abdullah International Medical Research Center-KAIMRC) exempts the online survey review, as no harm will be encountered plus no identified information will be gathered or declared. All participants must sign electronically on the short-informed consent before proceeding into the survey.
Statistical Analysis
The collected data have been organized, tabulated, and statistically analyzed using SPSS version 19 (Statistical Package for Social Studies) created by IBM, Chicago, USA.12 The research in data analysis was based on the descriptive method, which is based on iterations and percentages.
Results
First: Demographic Characteristics
Table 1 shows some demographic characteristics, and the results in table indicates the following: the size of the respondents is 329, 183 of them are males and 146 are females, and while 72% of the respondents were from Gulf, 19.1% from North Africa and 8.5% from Levant; 55.9% work in governmental hospitals, 11.9% in university, 10.3% in academic hospitals, 5.8% in private hospitals, 5.5% in pharmaceutical companies, 2.1% in private clinics, and 8.5% in other organizations; 47.1% of the respondents were physicians, 23.1% pharmacists, and 11.2% clinical research coordinators.
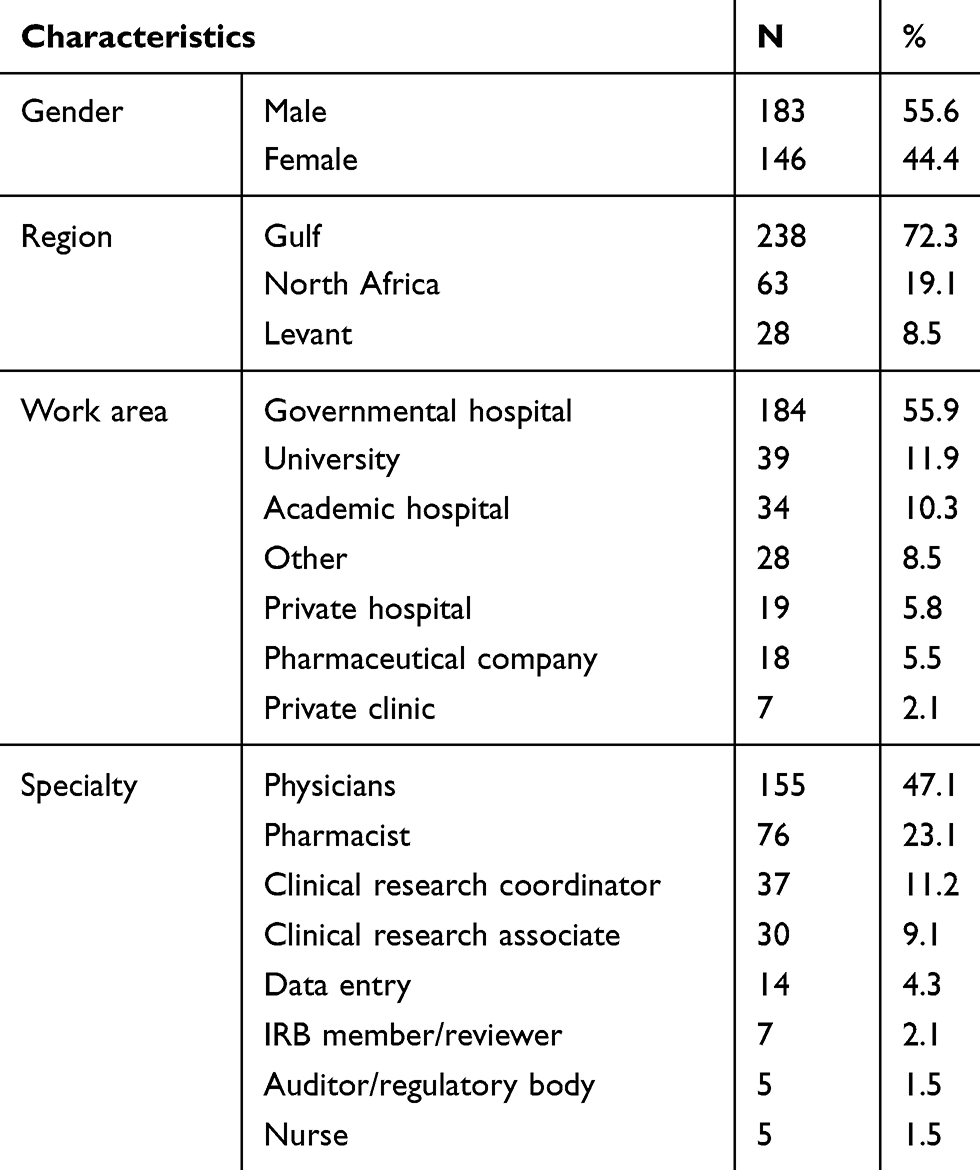 |
Table 1 Demographic Characteristics (n=329) |
Second: Barriers Affecting Roles
Barriers Affecting Physicians’ Role
The respondents indicated that 17 barriers affecting physician’s role as revealed in Table 2; the barriers affecting physician's role the most were: inadequate training in clinical research implementation (49.03%), lack of well-designed system operating procedures for local research practice (45.16%), and lack of financial/grant support (44.52%).
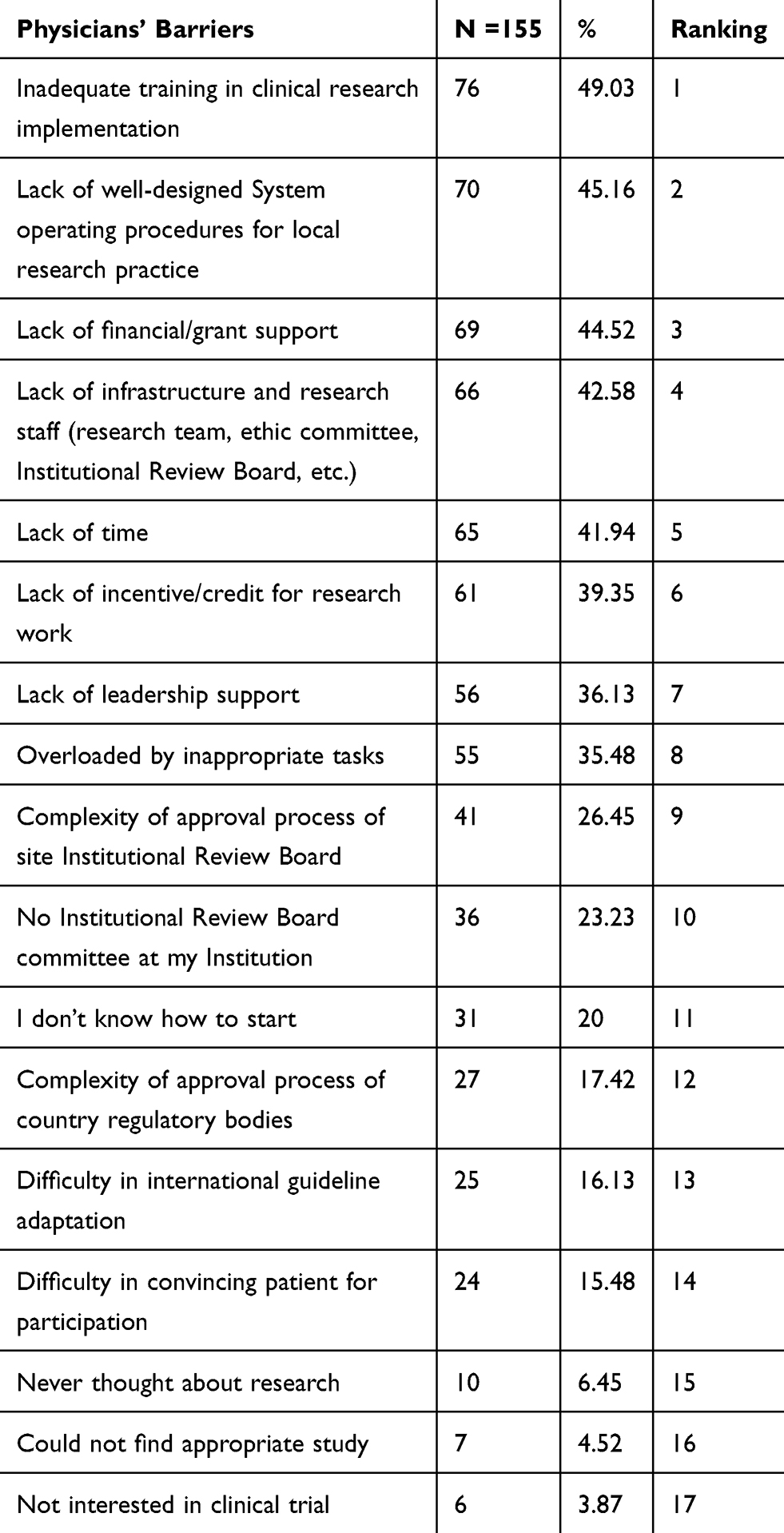 |
Table 2 Barriers Affecting Physicians’ Role |
On the other side, the barriers affecting physician’s role the least were: never thought about research (6.45%), could not find appropriate study (4.52%), and not interested in clinical trial (3.87%).
Barriers Affecting Clinical Research Associates’ (CRA) Role
The respondents indicated 13 barriers affecting clinical research associates’ (CRA) role as revealed in Table 3; the barriers affecting clinical research associates’ (CRA) role the most were: lack of incentive/credit for research work (56.67%), no enough time to be the CRF for multiple studies (53.33%), and lack of financial/grant support (50%).
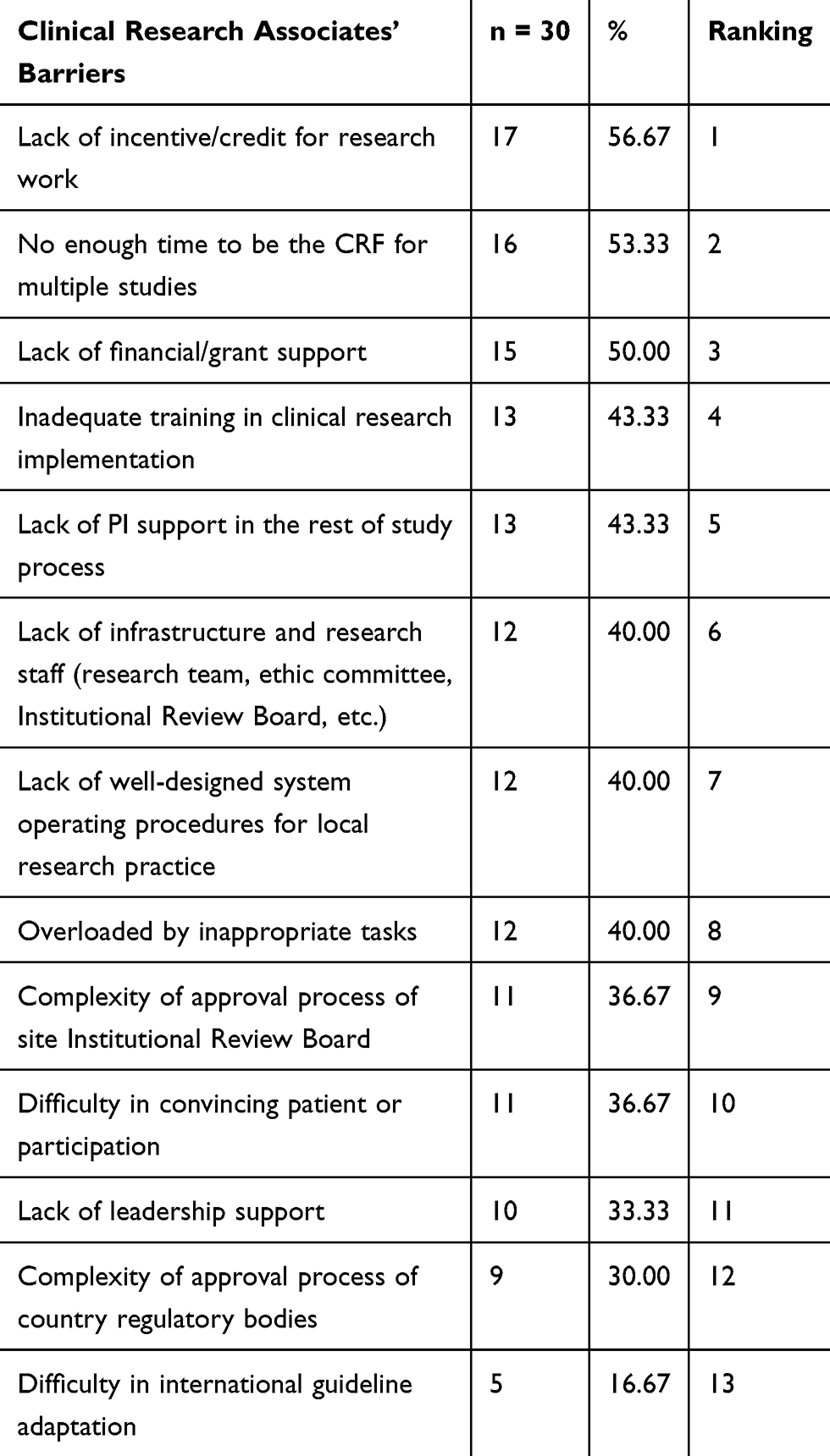 |
Table 3 Barriers Affecting Clinical Research Associates’ (CRA) Role |
On the other side, the barriers affecting clinical research associates’ (CRA) role the least were: lack of leadership support (33.33%), complexity of approval process of country regulatory bodies (30%), and difficulty in international guideline adaptation (16.67%).
Barriers Affecting Clinical Research Coordinators’ (CRC) Role
The respondents indicated 14 barriers affecting clinical research coordinators’ (CRC) role as revealed in Table 4; the barriers affecting clinical research coordinators’ (CRC) role the most were: inadequate training in clinical research implementation (48.65%), complexity of approval process of site Institutional Review Board (37.84%), and lack of well-designed system operating procedures for local research practice (37.84%).
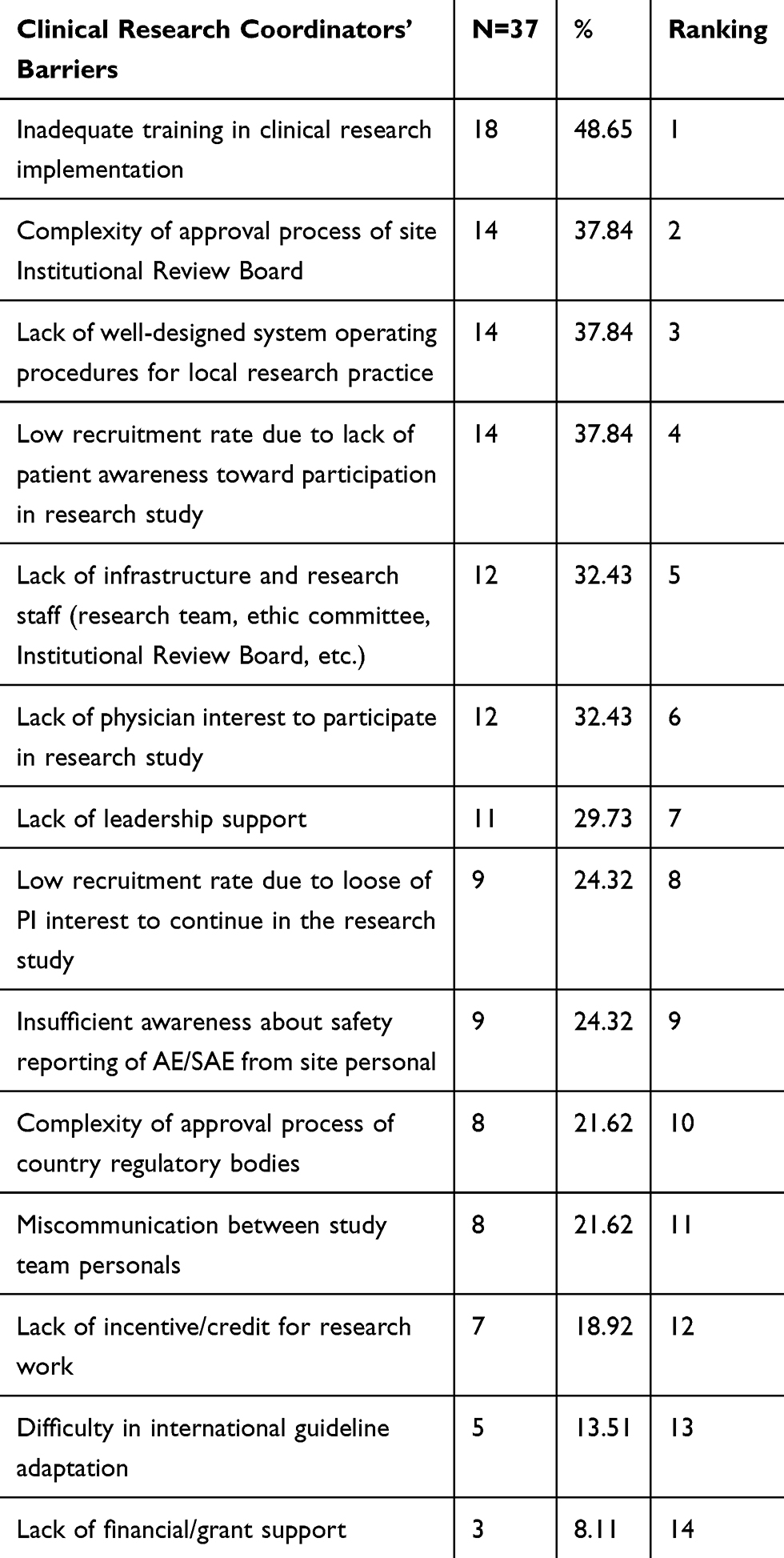 |
Table 4 Barriers Affecting Clinical Research Coordinators’ (CRC) Role |
On the other side, the barriers affecting clinical research coordinators’ (CRC) role the least were: lack of incentive/credit for research work (18.92%), difficulty in international guideline adaptation (13.51%), and lack of financial/grant support (8.11%).
Barriers Affecting IRB Members’ Role
The respondents indicated 11 barriers affecting IRB members’ role as revealed in Table 5; the barriers affecting IRB members’ role the most were: lack of leadership support (71.43%), lack of financial/grant support (71.43%), and lack of incentive/credit for research work (57.14%).
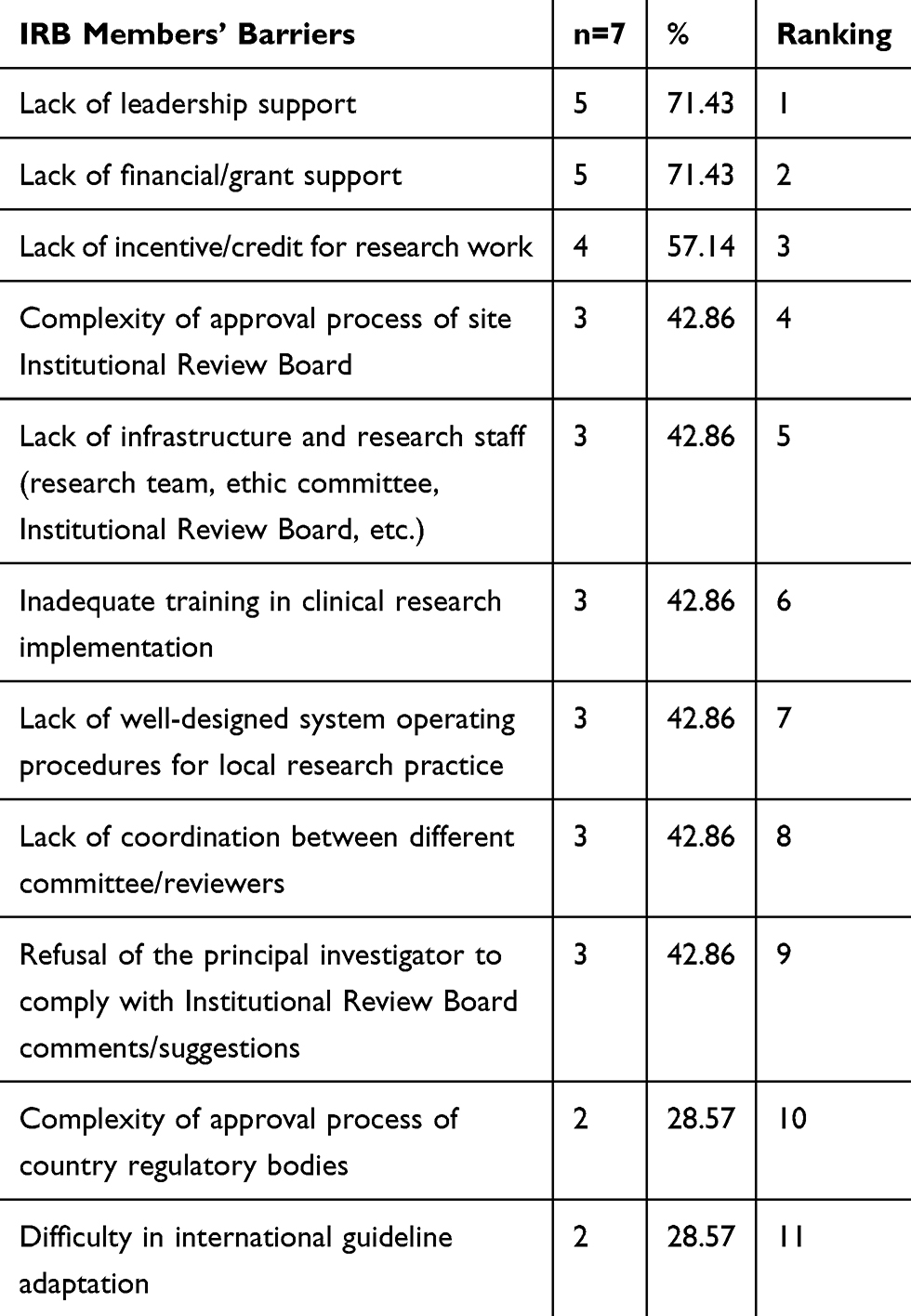 |
Table 5 Barriers Affecting IRB Members’ Role |
On the other side, the barriers Affecting IRB members’ role the least were: refusal of the principal investigator to comply with Institutional Review Board comments/suggestions (42.86%), complexity of approval process of country regulatory bodies (28.57%), and difficulty in international guideline adaptation (28.57%).
Barriers Affecting Auditors/Regulatory Body’s Role
The respondents indicated 11 barriers affecting auditors/regulatory body’s role as revealed in Table 6; the barriers affecting auditors/regulatory body’s role the most were: lack of infrastructure and research staff (research team, ethic committee, Institutional Review Board, etc.) (60%), inadequate training in clinical research implementation (60%), and lack of financial/grant support (40%).
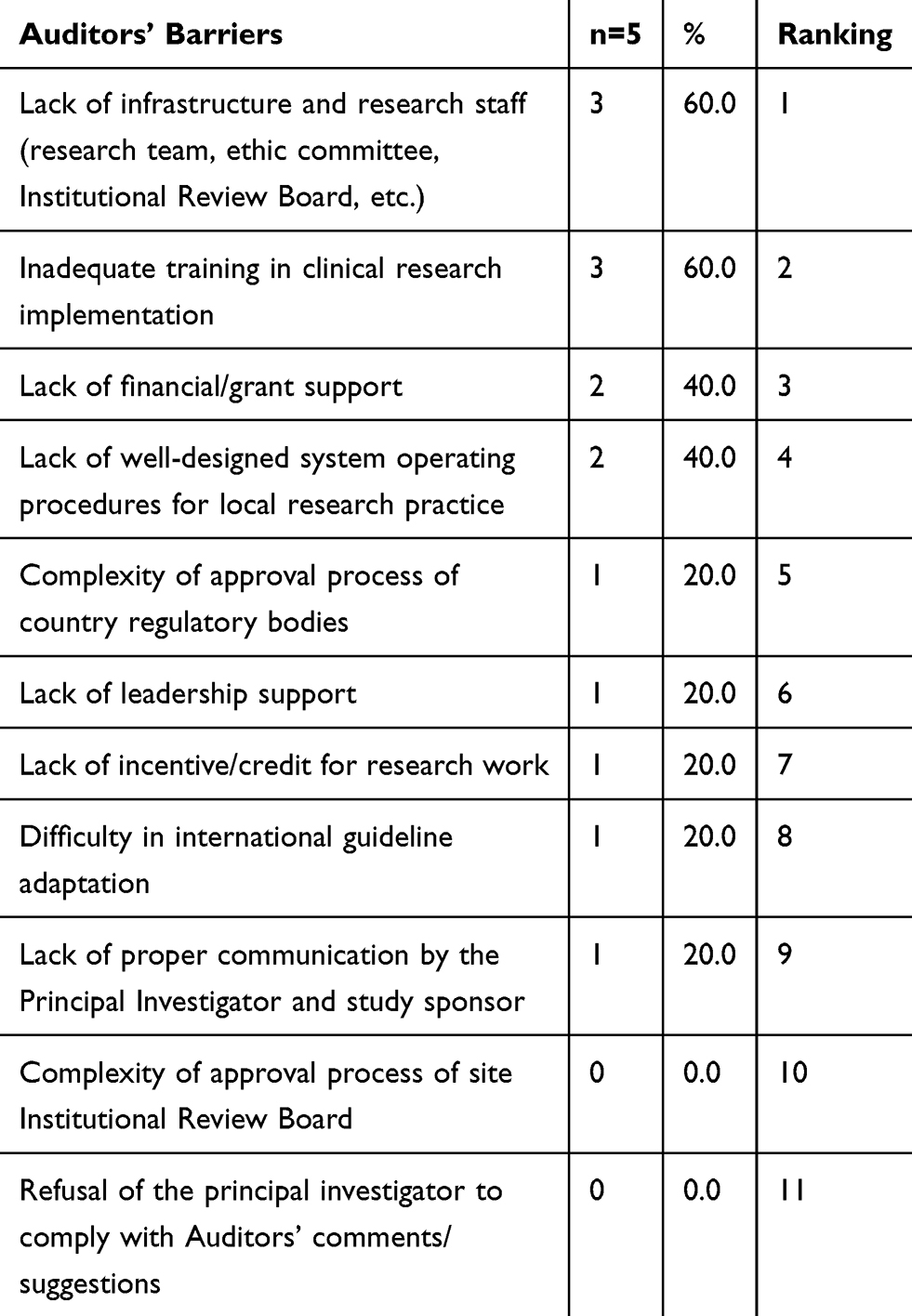 |
Table 6 Barriers Affecting Auditors/Regulatory Body’s Role |
On the other side, the barriers affecting auditors/regulatory body’s role the least were: lack of proper communication by the principal investigator and study sponsor (20%), complexity of approval process of site Institutional Review Board (0%), and refusal of the principal investigator to comply with auditors’ comments/suggestions (0%).
Barriers Affecting Pharmacists’ Role
The respondents indicated 15 barriers affecting Pharmacists’ role as revealed in Table 7; the barriers affecting pharmacists’ role the most were: inadequate training in clinical research implementation (42.11%), complexity of approval process of site Institutional Review Board (39.47%), and lack of financial/grant support (36.84%).
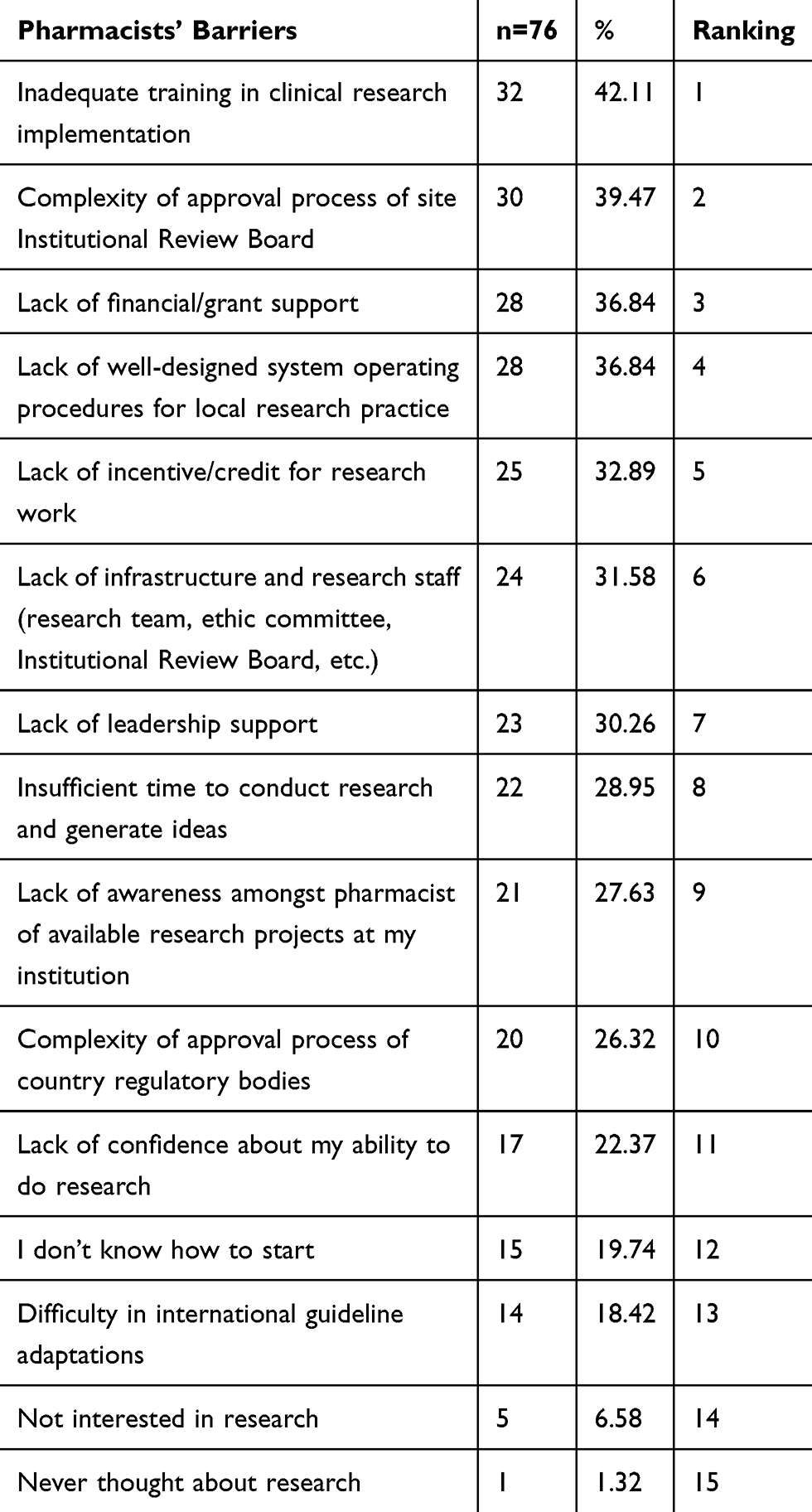 |
Table 7 Barriers Affecting Pharmacists’ Role |
On the other side, the barriers affecting pharmacists’ role the least were: difficulty in international guideline adaptations (18.42%), not interested in research (6.58%), never thought about research (1.32%).
Barriers Affecting Data Entry Clerks’ Role
The respondents indicated 12 barriers affecting data entry clerks’ role as revealed in Table 8; the barriers affecting data entry clerks’ role the most were: lack of leadership support (50%), lack of incentive/credit for research work (42.86%), and inadequate training in clinical research implementation (35.71%).
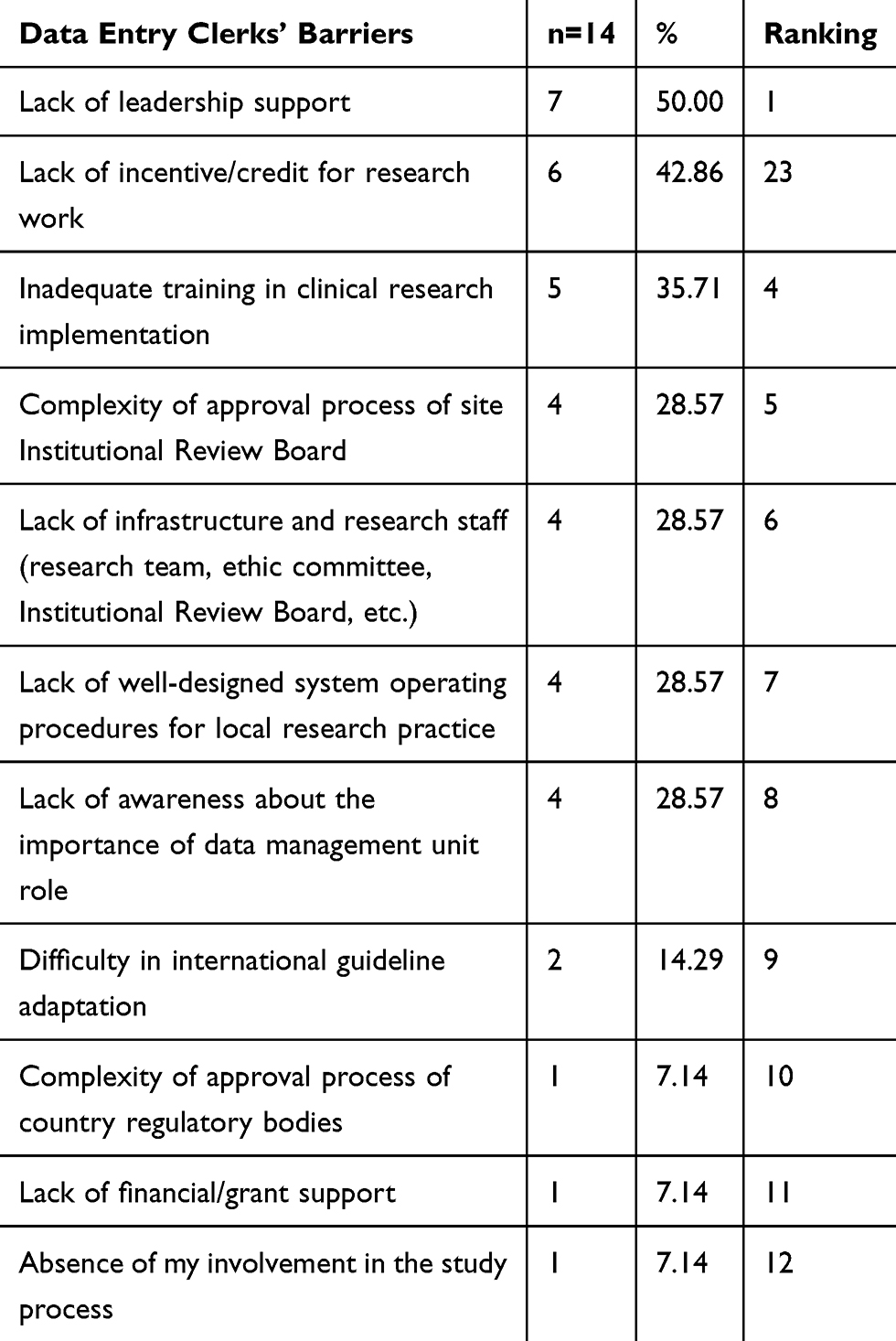 |
Table 8 Barriers Affecting Data Entry Clerks’ Role |
On the other side, the barriers affecting data entry clerks’ role the least were: complexity of approval process of country regulatory bodies (7.14%), lack of financial/grant support (7.14%), and absence of my involvement in the study process (7.14).
Barriers Affecting Nurses’ Role
The respondents indicated 13 barriers affecting nurses’ role as revealed in Table 9; the barriers affecting nurses’ role the most were: inadequate training in clinical research implementation (60%), overloaded by inappropriate tasks (60%), and lack of time (60%).
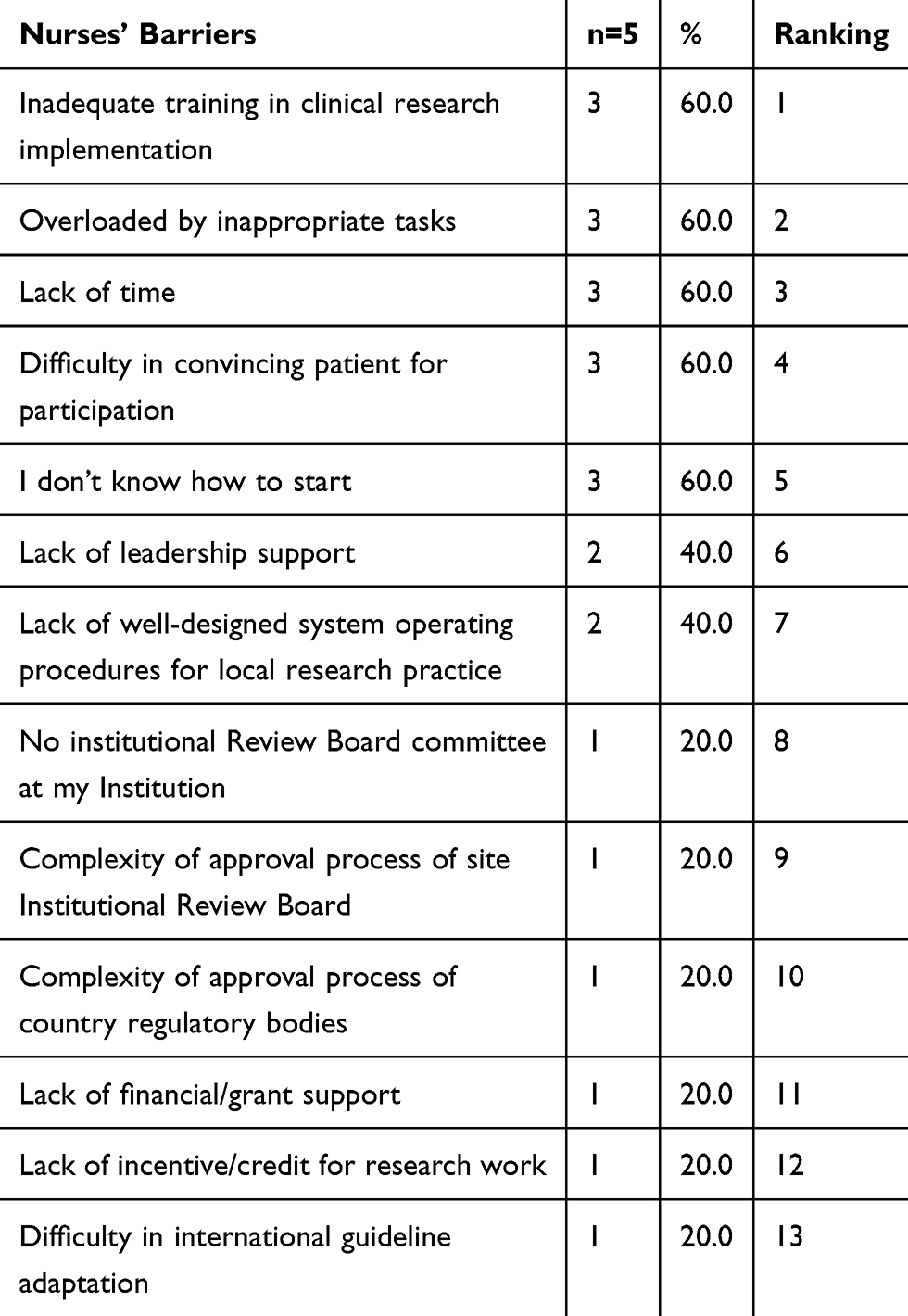 |
Table 9 Barriers Affecting Nurses’ Role |
On the other side the barriers affecting nurses’ role the least were: lack of financial/grant support (20%), lack of incentive/credit for research work (20%), and difficulty in international guideline adaptation (20%).
Common Barriers Among All Specialties
Table 10 reveals the common barriers among all specialties; it is clear from the table that among the barriers training ranks first (45.6%) followed by system operating procedures (40.4%), infrastructure (37.7%), financial support (37.4%), incentives (36.8%), leadership support (34.3%), approval process – IRB (31.3%), approval regulatory body (20.7%), and International Guidelines Adaptation (16.4%).
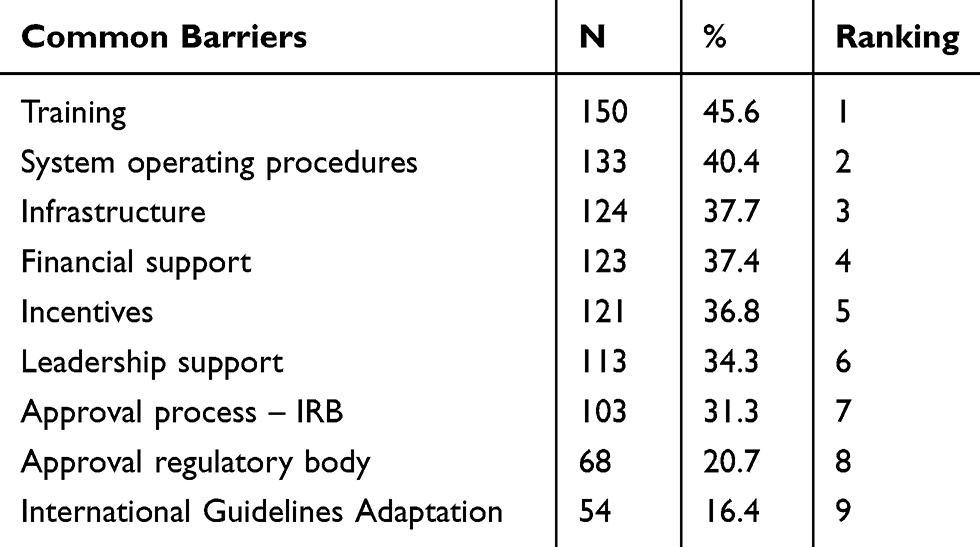 |
Table 10 Common Barriers Among All Specialties |
Table 11 reveals the regions that have most common barriers: Gulf has the most common barriers in approval process _IRB; North Africa has the most common barriers in financial, approval process _ regulatory, and International Guidelines Adaptation; and Levant has the most common barriers in training, operating system, infrastructure, incentives, and leadership.
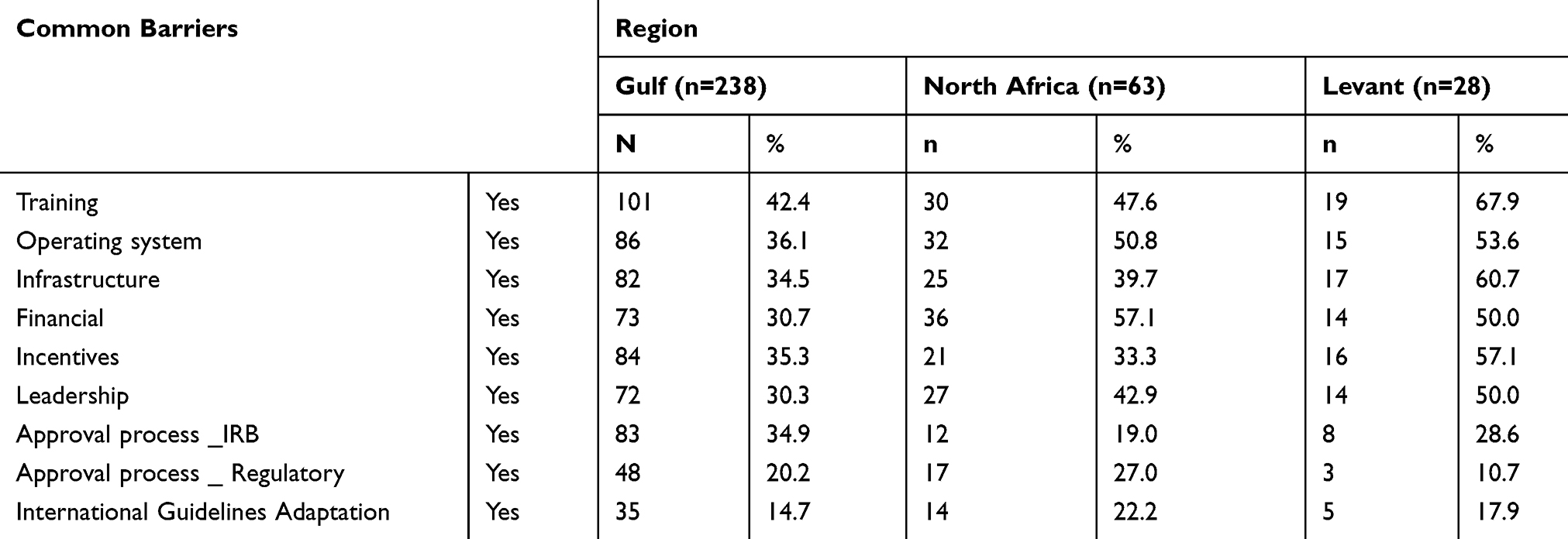 |
Table 11 Region And Common Barriers |
Third: Overall Strengths/Opportunities Exist In Institutions
Table 12 reveals the overall strengths/opportunities that exist in institutions; there are 9 overall strengths/opportunities that exist in institutions which are: being in an academic institution, opportunity for professional development, presence of well-trained support staff, availability of funding, being in a research institution, training in the research field at my institution, requirement by institution, awards/recognition, and financial incentive, with 29.8%, 29.2%, 25.5%, 21.9%, 21.6%, 18.8%, 17.6%, 16.4%, and 11.9%, respectively.
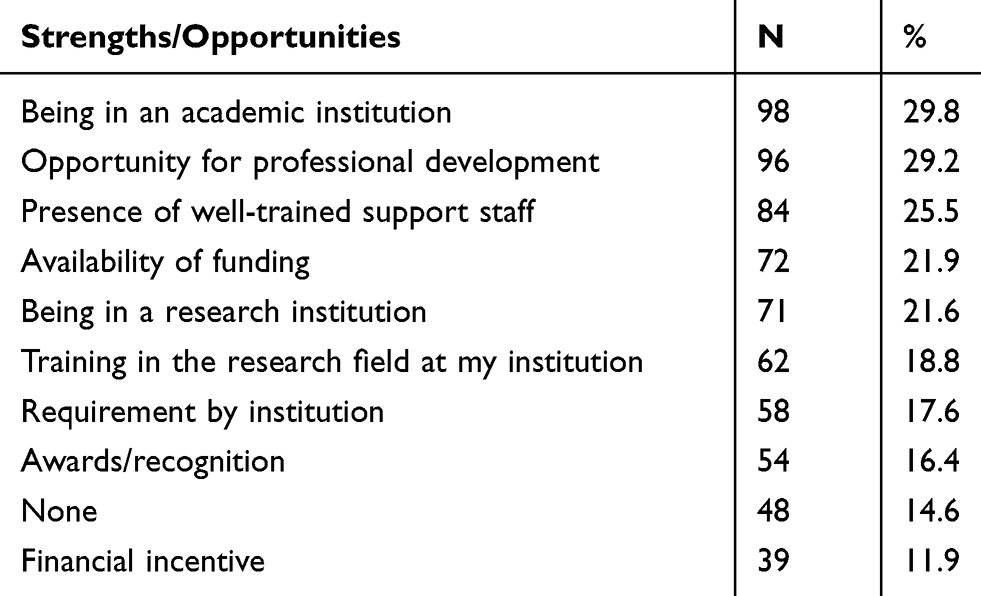 |
Table 12 Overall Strengths/Opportunities That Exist In Institutions |
Table 13 reveals the regions that have more strengths/opportunities: Gulf has more strengths/opportunities in presence of well-trained support staff, training in the research field at my institution, availability of funding, requirement by institution, being in the research institution, financial incentive, and awards/recognition; North Africa has more strength/opportunities in being in an academic institution; and Levant has more strengths/opportunities in opportunity for professional development.
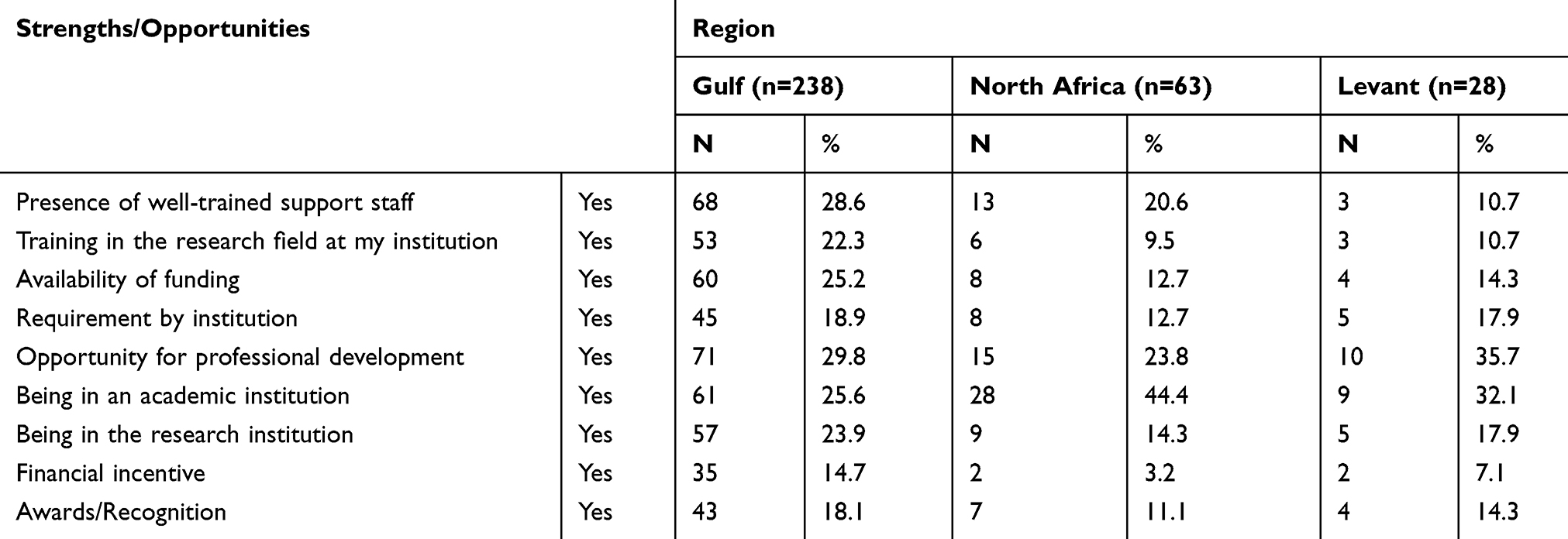 |
Table 13 Region And Strengths/Opportunities |
Fourth: Suggestions To Improve Arab Countries Research Field
Table 14 reveals suggestions to improve Arab Countries Research Field; there are 7 suggestions which are: increase training workshop about research for all medical health staff, increase awareness and interest in the importance of research, the critical need for infrastructure to support research, improve communication/collaboration among institution and universities, database/website for the available research project for the interested healthcare provider to participate, provide adequate compensation for time (ie, funds or replacement for their work), and exchange national/international expertise to reach a well-defined national research guidelines, with 60.8%, 56.8%, 56.5%, 56.5%, 54.1%, 53.5%, and 52.9%, respectively.
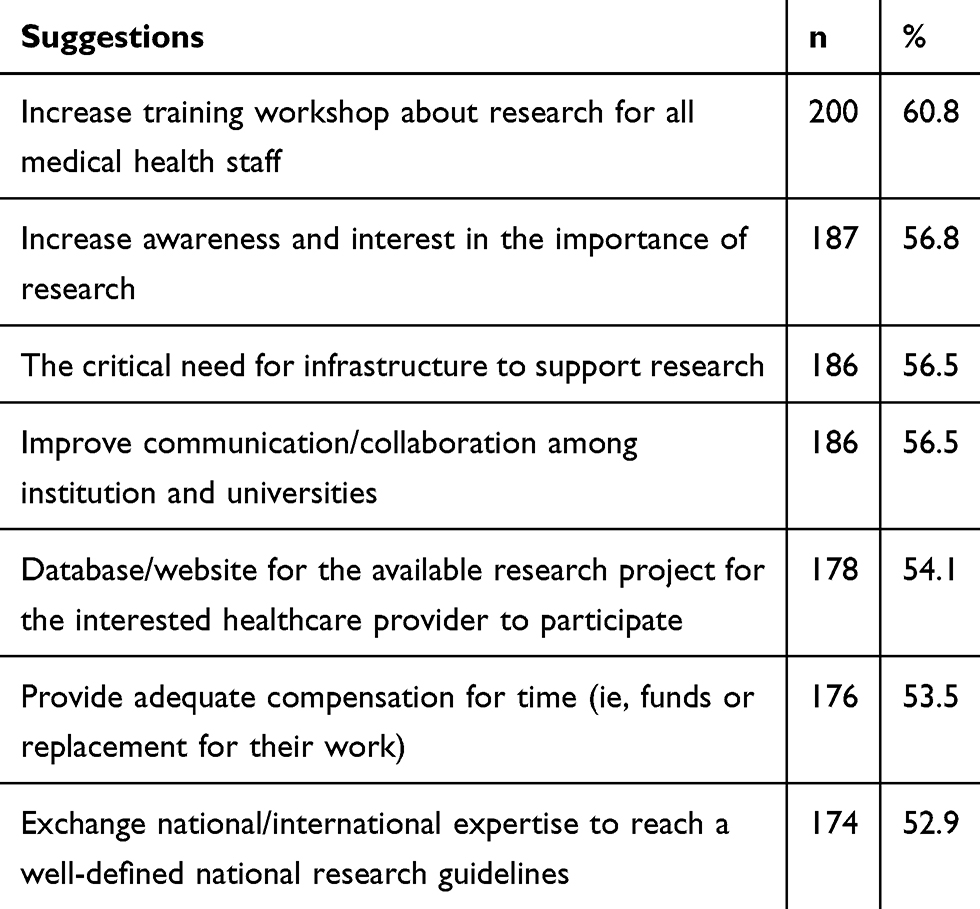 |
Table 14 Suggestions To Improve Arab Countries Research Field |
Discussion
This study reveals several important data regarding the challenges and barriers facing healthcare providers in the MENA region that might be applicable to individuals in other developing countries.
Seven specialties of healthcare providers were included in our study and we have mentioned the barriers facing every category in the respective tables.
Many barriers facing healthcare providers in conducting research detected previously in many studies conducted in western countries.
A study conducted by Eva Hummers-Pradier et al 200813 identified barriers to general practitioners (GPs’) participation in primary healthcare research. Nearly all respondents (88/96) considered general practice research to be important, but 58% had not previously participated in research projects and 56% would not do so in the future. Some GPs expressed concerns about recruiting their own patients for the study. Some doctors complained of not being sufficiently recognized as a partner or not having a voice in the research process.
A study conducted by Suzanne Bakken et al 2009 detected barriers, enablers, and incentives for research participation. The survey and qualitative data of this study indicated a strong interest in clinical research among current and potential Practice-Based Research Network “PBRN” members if it was relevant to improving quality of care in their practice or community. They also identified important perceived barriers (lack of time, inadequate training in research methods, lack of collaborators and support staff, institutional review board hurdles, and community distrust of research) and the necessary requirements for overcoming barriers to conducting research in busy clinical settings, which included collaborators, mentors, research support staff, and a trusting patient–clinician relationship.14
Hiroaki Yanagawa et al conducted a study in Japan about nurse awareness of clinical research. The authors found that that clinical nurses have only limited knowledge of clinical research and the importance to have chances to make nurses aware of clinical research-related issues is suggested to establish an extended research team.15
Those suggestions given by these study participants may help to remove the barriers facing conduction of clinical research studies in Arabic countries especially as there are many fears from the public to participate in clinical trials as conducted in a study by Susan S Khalil et al 2007, which detected attitudes, understanding, and concerns regarding medical research amongst Egyptians. All individuals valued the importance of medical research; however, most would not participate in research that involved more than minimal risk. Individuals were comfortable with studies involving surveys and blood sampling, but many viewed drug trials as being too risky. So trying to remove the barriers may help to increase the trust of the public people to participate in any kind of research studies.16
Another study of Giselle Corbie-Smith et al about attitudes and beliefs of African Americans toward participation in Medical Research found that African-American participants described distrust of the medical community as a prominent barrier to participation in clinical research. Participants described real and perceived examples of exploitation to support their distrust of researchers. The goal of the consent process, to inform patients of risks and benefits to facilitate self-determination, was misinterpreted by these participants. Understanding the importance of interpersonal trust within the clinical relationship may prove to be a significant factor in enhancing participation in clinical trials.17 Therefore, there is a great need to remove the barriers facing all researchers to facilitate working and improvement in the research field.
In addition, the suggestions included in our study may help to increase scientific research publications in Arabic countries, due to decreased capacity to absorb scientific knowledge in Arabic countries because of bad research infrastructure, leading to low levels of scientific output. A study of the comparative performance of the world’s major science-producing countries found that researchers in eight countries – led by the USA, the UK, Germany, and Japan – produce almost 85% of the world’s most cited publications, while another 163 countries, mostly developing countries, account for less than 2.5%.18
According to our study, we found that retrospective and observational studies were the most common type of research studies conducted in the MENA region. Which selected by 44.7% of participants followed by basic research, which selected by 30.1% of this study participants, the question here is why there are no clinical trials and more study types to be conducted in our Arabic countries?
We suggested conducting more studies with larger sample size for each specialty of the seven specialties included in our study and to get more data about the barriers and challenges to conducting clinical scientific research in every Arabic country separately as every country has its conditions.
We faced many limitations to collect the sample for this study through internet, but once collected, the participants showed a good general understanding of the concept of research and the importance of scientific research work to advance medical progress and so they agreed to complete our online questionnaire.
Conclusions
This study demonstrated the barriers faced by healthcare providers in the MENA region. Inadequate training in clinical research implementation and the lack of designed system operating procedures for the research process should be addressed to facilitate clinical research in this region. In addition, this study provided a good association between Arabic regions included and barriers faced by healthcare providers in conducting research and so this study could be a good reference for authorities to improve the clinical research in Arabic countries especially every country has its conditions.
Many suggestions given by the participants to improve research field such as increasing training workshop about research for all medical health staff categories to improve research field and increasing awareness and interest about the importance of research are very important. This study provides a good association between Arabic regions included and barriers facing healthcare providers in conducting research so this study could be a good reference for authorities to improve the clinical research in Arabic countries.
There is also a great need for providing a database/website for the available research project for the interested healthcare provider to participate. Authorities responsible for the development of scientific research should provide infrastructure to support research and improve communication/collaboration among institutions and universities.
Acknowledgments
The authors would like to thank all the healthcare providers who participated in the research. We would like also to thank also all administrative persons who facilitate the condition of the work.
The authors also would like to thank Mr. Mohamed Al Khayat and Mr. Ahmed Qudaimat, clinical research coordinators, for their help in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bhutta ZA. Ethics in international health research: a perspective from the developing world. Bull World Health Organ. 2002;80:114–120.
2. Shapiro HT, Meslin EM. Ethical issues in the design and conduct of clinical trials in developing countries. Mass Med Soc. 2001.
3. Benatar SR. Reflections, and recommendations on research ethics in developing countries. Soc Sci Med. 2002;54(7):1131–1141. doi:10.1016/S0277-9536(01)00327-6
4. Vallotton MB. Council for international organizations of medical sciences perspectives: protecting persons through international ethics guidelines. Int J Integr Care. 2010;10(5). doi:10.5334/ijic.478
5. Willis L. Nuffield Council on Bioethics. The ethics of research related to healthcare in developing countries. Med Conflict Survival. 2003;19(1):74.
6. Tallon D, Chard J, Dieppe P. Relation between agendas of the research community and the research consumer. Lancet. 2000;355(9220):2037–2040. doi:10.1016/S0140-6736(00)02351-5
7. Ridda I, Lindley R, MacIntyre RC. The challenges of clinical trials in the exclusion zone: the case of the frail elderly. Australas J Ageing. 2008;27(2):61–66. doi:10.1111/j.1741-6612.2008.00288.x
8. Ferrari A, Montello M, Budd T, Bleyer A. The challenges of clinical trials for adolescents and young adults with cancer. Pediatr Blood Cancer. 2008;50(S5):1101–1104. doi:10.1002/(ISSN)1545-5017
9. Somkin CP, Altschuler A, Ackerson L, et al. Organizational barriers to physician participation in cancer clinical trials. Am J Manag Care. 2005;11(7):413–421.
10. Murillo H, Reece EA, Snyderman R, Sung NS. Meeting the challenges facing clinical research: solutions proposed by leaders of medical specialty and clinical research societies. Acad Med. 2006;81(2):107–112. doi:10.1097/00001888-200602000-00002
11. Stening BW, Zhang MY. Methodological challenges confronted when conducting management research in China. Int J Cross Cult Manage. 2007;7(1):121–142. doi:10.1177/1470595807075179
12. Nie NH, Bent DH, Hull CH. SPSS: Statistical Package for the Social Sciences. Vol. 227. New York: McGraw-Hill; 1975.
13. Hummers-Pradier E, Scheidt-Nave C, Martin H, Heinemann S, Kochen MM, Himmel W. Simply no time? Barriers to GPs’ participation in primary health care research. Fam Pract. 2008;25(2):105–112. doi:10.1093/fampra/cmn015
14. Bakken S, Lantigua RA, Busacca LV, Bigger JT. Barriers, enablers, and incentives for research participation: a report from the Ambulatory Care Research Network (ACRN). J Am Board Family Med. 2009;22(4):436–445. doi:10.3122/jabfm.2009.04.090017
15. Yanagawa H, Takai S, Yoshimaru M, Miyamoto T, Katashima R, Kida K. Nurse awareness of clinical research: a survey in a Japanese University Hospital. BMC Med Res Methodol. 2014;14(1):85. doi:10.1186/1471-2288-14-85
16. Khalil SS, Silverman HJ, Raafat M, El-Kamary S, El-Setouhy M. Attitudes, understanding, and concerns regarding medical research amongst Egyptians: a qualitative pilot study. BMC Med Ethics. 2007;8(1):9. doi:10.1186/1472-6939-8-9
17. Corbie-Smith G, Thomas SB, Williams MV, Moody-Ayers S. Attitudes and beliefs of African Americans toward participation in medical research. J Gen Intern Med. 1999;14(9):537–546. doi:10.1046/j.1525-1497.1999.07048.x
18. King DA. The scientific impact of nations. Nature. 2004;430(6997):311–316. doi:10.1038/430311a
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.