Back to Journals » Research and Reports in Tropical Medicine » Volume 13
The Burden of Typhoid Fever in Sub-Saharan Africa: A Perspective
Authors Kim CL, Cruz Espinoza LM, Vannice KS, Tadesse BT ![]() , Owusu-Dabo E, Rakotozandrindrainy R, Jani IV
, Owusu-Dabo E, Rakotozandrindrainy R, Jani IV ![]() , Teferi M, Bassiahi Soura A, Lunguya O, Steele AD
, Teferi M, Bassiahi Soura A, Lunguya O, Steele AD ![]() , Marks F
, Marks F ![]()
Received 21 December 2021
Accepted for publication 12 February 2022
Published 14 March 2022 Volume 2022:13 Pages 1—9
DOI https://doi.org/10.2147/RRTM.S282461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Cara Lynn Kim,1 Ligia Maria Cruz Espinoza,1 Kirsten S Vannice,2 Birkneh Tilahun Tadesse,1,3,4 Ellis Owusu-Dabo,5 Raphaël Rakotozandrindrainy,6 Ilesh V Jani,7 Mekonnen Teferi,8 Abdramane Bassiahi Soura,9 Octavie Lunguya,10,11 A Duncan Steele,2 Florian Marks1,6,12,13
1International Vaccine Institute, Seoul, Republic of Korea; 2Enteric and Diarrheal Diseases, Bill & Melinda Gates Foundation, Seattle, WA, USA; 3Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Institutet, Karolinska University Hospital Huddinge, Stockholm, Sweden; 4Center for Innovative Drug Development and Therapeutic Trials for Africa, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 5School of Public Health, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana; 6University of Antananarivo, Antananarivo, Madagascar; 7Instituto Nacional de Saúde (INS), Maputo Province, Mozambique; 8Armauer Hansen Research Institute, Addis Ababa, Ethiopia; 9Institut Supérieur des Sciences de la Population, Université Joseph Ki-Zerbo de Ouagadougou, Ouagadougou, Burkina Faso; 10Department of Microbiology, Institut National de Recherche Biomédicale, Kinshasa, Democratic Republic of the Congo; 11Department of Medical Biology, University Teaching Hospital of Kinshasa, Kinshasa, Democratic Republic of the Congo; 12Cambridge Institute of Therapeutic Immunology and Infectious Disease, University of Cambridge School of Clinical Medicine, Cambridge Biomedical Campus, Cambridge, UK; 13Heidelberg Institute of Global Health, University of Heidelberg, Heidelberg, Germany
Correspondence: Florian Marks, Tel +82-2-881-1133, Email [email protected]
Abstract: While typhoid fever has largely been eliminated in high-income regions which have developed modern water, sanitation, and hygiene facilities, it remains a significant public health burden resulting in morbidity and mortality among millions of individuals in resource-constrained settings. Prevention and control efforts are needed that integrate several high-impact interventions targeting facilities and infrastructure, including those addressing improvements in sanitation, access to safe water, and planned urbanization, together with parallel efforts directed at effective strategies for use of typhoid conjugate vaccines (TCV). The use of TCVs is a critical tool with the potential of having a rapid impact on typhoid fever disease burden; their introduction will also serve as an important strategy to combat evolving antimicrobial resistance to currently available typhoid fever treatments. Well-designed epidemiological surveillance studies play a critical role in establishing the need for, and monitoring the impact of, typhoid fever control and prevention strategies implemented by public health authorities. Here, we present a perspective based on a narrative review of the impact of typhoid fever on morbidity and mortality in sub-Saharan Africa and discuss ongoing surveillance activities and the role of vaccination in prevention and control efforts.
Keywords: typhoid, burden, mortality, sub-Saharan Africa, conjugate-vaccine, antimicrobial resistance
Introduction
Typhoid fever is a febrile illness caused by infection with the Gram-negative bacterium Salmonella enterica serovar Typhi (S. Typhi). There are several Salmonella enterica species: the serovar Paratyphi causes paratyphoid fever; further, there are non-typhoidal serovars, the most prevalent being serovars Enteritidis, Typhimurium, and Dublin, which cause invasive non-typhoidal salmonellosis (iNTS).1,2
Typhoid fever represents a significant public health burden, particularly in resource-constrained settings.3,4 While typhoid fever has been largely eliminated in higher-income countries with modern sanitary facilities and safe drinking water, the disease persists as a significant public health issue in many low- and middle-income countries (LMICs) worldwide.5,6 This public health issue is compounded by increasing antimicrobial resistance (AMR) and rampant economic loss due to the impact of this disease on productive members of the population.7 The World Health Organization (WHO) estimates the global burden of typhoid fever at 11–20 million cases per year, resulting in ~140,000 deaths.8
Typhoid conjugate vaccines (TCV) are highly effective and have been recommended for use in typhoid fever-endemic countries.9,10 Vaccine introduction can address the enduring problem of pediatric typhoid fever as well as the evolving problem of multi-drug resistance (MDR) in affected regions.
Clinical Presentation and Diagnosis of Typhoid Fever
Typhoid fever is a systemic infection that presents with multisystem signs and symptoms albeit without pathognomonic clinical features.4 Transmission usually occurs via the fecal-oral route, typically when an individual ingests contaminated food or water.4 S. Typhi characteristically invades the gastrointestinal tract and progresses to systemic infection.3 The risk of infection has previously been linked to factors such as exposure to contaminated water, inadequate waste management, poor hygiene conditions as well as inhabitation of urban slums.11 Clinical diagnosis is challenging because of its nonspecific and diverse symptoms that include fever, diarrhea, and abdominal pain.12
The gold standard for the diagnosis of typhoid fever is a bone-marrow culture. While this modality is highly sensitive, it is invasive and technically unfeasible in most settings.13 Thus, this disease is typically diagnosed by the more practical method of blood culture despite its limited (40–60%) sensitivity and the challenges in establishing contamination-free blood culturing in LMIC settings.14,15 While typhoid fever can usually be treated effectively with appropriate antibiotics if diagnosed accurately during the early stages of the disease, the limited resources available in most of the endemic regions often lead to delays in diagnosis and treatment, followed by empirical treatment only.16,17 New diagnostic tools with improved accuracy, including antibody-based serologic assays used to evaluate samples collected through serosurveys, are currently under development and will hopefully be available for use in field settings.18,19
Epidemiology of Typhoid Fever in Africa
S. Typhi has reportedly been cultured from patients in 42 of 57 African countries until 2018; however, this could result from limited diagnostic capacities and underreporting in the remaining 15 countries.20 Several researchers have recently estimated the incidence of disease and mortality rates at levels that are similar, if not higher, than those identified in South/Southeast Asia.20–22 Nevertheless, the results of one recent study show the high degree of heterogeneity in different settings and between countries.20 In their 2017 review, Antillón et al23 estimated the burden of typhoid fever in sub-Saharan Africa at 762 per 100,000 person-years. These findings highlight an incidence that is significantly higher than that identified in Southeast Asia, East Asia, and Oceania (estimated incidence of 108 per 100,000 person-years). This review applied a modeling approach which included factors such as population density, gross domestic product (GDP), Gini coefficients, access to improved sources of water, and sanitation as predictors of disease burden. Similarly, a 2019 comprehensive review by Marchello et al24 estimated the African incidence of typhoid fever from previous results and presented an initial pooled estimate of 112.1/100,000 person-years, with a 95% confidence interval (CI) of 46.7–203.5. After application of adjustment factors, including access to health-care facilities (ie, eligible participants not seeking care), enrollment (ie, eligible participants without blood culture data), blood culture sensitivity, and the length of the surveillance period, the revised pooled estimate of the global burden of typhoid fever increased to 134.1/100,000 person-years (95% CI, 77.9–204.8).24 The Institute for Health Metrics and Evaluation (IHME) Global Health Data Exchange provided similar estimates for 2019 at 114.8/100,000 person-years (95% CI, 73.5–171.0).25
The incidence of typhoid fever has been reported higher among children, mainly those who are older than five years of age. A systematic analysis by Stanaway et al estimated 55.9% of cases in 2017 globally occurred among children younger than 15 years (95% CI, 50.3–61.6), and 12.6% among children younger than 5 years (95% CI, 8.7–17.7).21 Another meta-analysis examining age-stratified disease occurrence reported a proportion of 0.24 (95% CI, 0.20–0.28) of pediatric enteric fever cases in Africa occurred in children under the age of five.26 While these findings emphasize the substantial burden in pediatric populations, more comprehensive data on the burden of typhoid fever in younger age groups is needed.
It is not clear if the increased incidence reported for specific regions can be attributed to an actual increase in case numbers or whether it is the result of an increase in the number of studies undertaken with extended surveillance methods and more standardized diagnostic tools, in particular blood culture. Of note, few studies have compared incidence rates in urban versus rural areas in various LMICs. Those that have been undertaken have yielded mixed results, with some reporting higher and others documenting lower incidences in rural areas.27–29 While higher incidences of typhoid fever in urban areas may be a direct result of higher population density, individuals residing in rural areas typically have more limited access to sanitation and sources of clean water. Similarly, fewer diagnostic tools of all sorts are available in rural areas compared to urban centers; this may lead to an inaccurately low calculated incidence of typhoid fever as many cases are likely to remain undiagnosed. Moreover, as there is usually a higher availability and accessibility of health-care services in urban areas, the higher incidences compared to rural areas could also be attributed to urban residents seeking health-care facilities more often when experiencing symptoms of infection. Nonetheless, given the extent of travel between urban and rural areas, the risk of exposure to typhoid fever remains ongoing in all locales.
The Typhoid Fever Surveillance in Africa Program (TSAP) that was conducted between the years 2010 and 2014 was setup in 13 sites in 10 Africa countries (Burkina Faso, Ghana, Guinea-Bissau, Senegal, Ethiopia, Sudan, Kenya, Tanzania, South Africa, and Madagascar) to determine age-stratified incidences of invasive Salmonella infections. Typhoid fever incidence estimates ranged from 0 in Sudan to 383/100,000 person-years in Burkina Faso.30 Among age groups, the highest disease burden for typhoid fever was in the 5–8 years-of-age group. The TSAP study also highlighted variations in disease patterns between rural and urban sites in Ghana and reported age-adjusted incidence rates that were two times higher in the rural versus the urban site.31 Factors contributing to this difference may include the poorer-quality sanitary and hygiene conditions in rural areas, compounded by less education and the availability of fewer typhoid interventions. However, other studies reported conflicting results, including much higher rates of typhoid fever in urban settlements.28 Further research will be needed to clarify these results. The Severe Typhoid Program in Africa (SETA) was instituted as a follow-up to TSAP. In order to assess typhoid fever severity, the SETA provided continued surveillance of four of the original ten aforementioned higher-incidence countries (Burkina Faso, Ethiopia, Ghana, and Madagascar) and included two new sites in Nigeria and the Democratic Republic of the Congo (DRC). Results from this program will provide updated information on the severity, mortality, and economic burden of typhoid disease in these African countries.32
Severity and Mortality of Typhoid Fever
Individuals infected with S. Typhi may develop complications by the second to fourth week of illness and could progress to death if left untreated.4,33 Recent systematic reviews and meta-analyses focused on severity and mortality of typhoid fever in Africa identified an overall prevalence of complications at 37.7%22 with an overall case fatality rate (CFR) of 3.82% (95% CI, 1.97–7.26%).34 These results suggest that Africa has the highest prevalence of typhoid fever complications and mortality when compared to other WHO regions. For example, the CFR in the South-East Asian region has been estimated at 2.27% (95% CI, 0.91–5.55%).22,24,34,35 Nevertheless, it is critical to recognize the considerable variations in the burden of disease both between and within these regions.36–38
The most serious and well-characterized complication of typhoid fever is typhoid intestinal perforation (TIP). This condition is highly prevalent in Africa, with an overall incidence estimated at 7.6% of typhoid fever cases in Africa.22 This rate is higher than that reported for the Americas (1.8%), Asia (0.7%), and Oceania (0.7%) combined.22 TIP develops twice as frequently in males (66.3% of cases).22 A review of this complication published in 2017 estimated the mortality associated with TIP at 5–80% in resource-poor countries.39 The median CFR related to this complication estimated for the African region ranges from 19.5% (95% CI, 16.6–22.4%)40 to 20.0% (13.7–28.0%).22 These data can be compared to median CFRs estimated between 1.0% (0.0–8.4%)22 and 10.7% (95% CI; 8.0–13.4%)40 for the Asian region. The CFR associated with TIP among children under 18 years of age might be as high as 75%;35 this rate is significantly higher than the overall estimated CFR for typhoid fever. There are data indicating that children under five are at a higher risk of experiencing severe illness and subsequently high mortality rates.26,41,42 Similarly, Stanaway et al estimated highest mortality rates among young children; however, identifying a peak in the ages between 5 and 9 with 59.3% of global deaths occurring among children younger than 15 years of age.21
Several factors may contribute to the high rates of severity and mortality associated with typhoid fever in Africa. Recent systematic reviews point to delays in diagnosis and/or treatment as factors that are associated with both increased severity and CFR.22,43 The mean delay in the care provided for typhoid fever patients in Africa, defined as the duration of disease prior to hospitalization, has been estimated at 9.4 days.22 Results from a recent study revealed that delay in care of an average 10 days was associated with three times greater odds of developing any typhoid fever complications (Odds Ratio [OR] 3.0; 95% CI, 2.14–4.17) and the more than two times greater odds of developing TIP (OR 2.5; 95% CI, 0.43–10.80).43 A recent study focused on complications of typhoid fever specifically in Madagascar documented a substantial surge in intestinal perforations commencing at the time of onset of the Coronavirus-disease 2019 (COVID-19) pandemic, potentially as a result of delayed treatment due to general reluctance regarding visiting health-care facilities.44 Other researchers have also identified severe typhoid fever disease among individuals who began treatment later in the course of the disease.45–47 These data highlight the importance of early care and treatment for typhoid fever toward reducing morbidity and mortality. Furthermore, limited access to health services and specifically blood culture diagnostics in various settings in the African region preclude timely administration of appropriate antibiotic treatment based on pathogen susceptibility profile. This problem also contributes to poor outcomes secondary to treatment failure and the development of AMR.22,35,47 While several researchers note that the increasing AMR of S. Typhi pathologic variants is a significant factor contributing to the severity of disease,4,48,52 the relationship between the variants and severity of disease needs to be further investigated going forward.
While typhoid fever still significantly contributes to the morbidity and mortality inLMICs, socioeconomic impacts of this disease need also be considered.49 Accurate estimations for the economic costs of typhoid fever are difficult to obtain given limited data availability and the use of heterogeneous research methods; one review cited an estimated cost per typhoid fever case at $171 in Tanzania while indicating the existence of a high variation between countries considering the estimated typhoid fever incidence in LMICs.50 A primary evaluation of vaccination in LMIC settings found TCV to be cost-effective strategy in these settings.51 Further studies for assessing cost of illness are also underway in the course of the SETA study.
Increasing Antibiotic Resistance
Early diagnosis and prompt initiation of appropriate treatment are considered to be the key factors that determine disease prognosis.52 Typhoid fever responds well to treatment with antibiotics; however, the rise of MDR S. Typhi strains impairs successful treatment and may lead to a higher incidence of complications and disease severity.36,53,54 This problem is exacerbated by the frequent inappropriate use of antibiotics that contribute to the rapid development of antibiotic resistance.4,55 MDR strains, represented mainly by the H58 S. Typhi genotype, are resistant to first-line anti-typhoidal antibiotics that include chloramphenicol, ampicillin, and trimethoprim-sulfamethoxazole/co-trimoxazole. These MDR strains are also responsible for several outbreaks of typhoid fever across the African and Asian continents.56,57 Zimbabwe, a location with a substantial endemic occurrence of typhoid fever, was one of the countries affected by repeated seasonal outbreaks with a high proportion of antimicrobial-resistant strains. Most culture-confirmed isolates (88%) from this region were resistant to two or more first-line anti-typhoid drugs with increasing trends observed between 2012 and 2017.58 In response to these outbreaks, Zimbabwe carried out mass vaccination campaigns in 2019, aimed at children between the ages of 6 months and 15 years; this strategy was highly effective at reducing the incidence of typhoid fever in this age group.59 MDR strains of S. Typhi are emerging at an increasing rate in other countries across the African continent. Although reported MDR rates vary greatly between countries, the overall rate in S. Typhi isolated from countries surveyed by the TSAP was estimated at 52%.57 A study carried out in Bwamanda, DRC reported that 72.2% of S. Typhi isolates were co-resistant to ampicillin and trimethoprim-sulfamethoxazole, and an additional 33.3% were MDR.37 Another study carried out in Nairobi, Kenya, revealed a high prevalence of H58-genotype in S. Typhi cases (97%, 96/99), with 76% of the strains being also MDR.60
This increase in MDR strains of S. Typhi is particularly worrisome as this could have a profound impact on our ability to treat typhoid fever and thus result in a much higher CFR. To address this problem, current treatment strategies also include fluoroquinolones. However, recent findings have documented increases in transmission of extensively drug-resistant (XDR) S. Typhi strains, which are resistant to five classes of antibiotics: chloramphenicol, ampicillin, cotrimoxazole, fluoroquinolones, and third-generation cephalosporins.61 Pakistan experienced its largest outbreak to date with XDR-typhoid in 2018 in Hyderabad, with an increased risk of infection for children younger than 15 years of age.62 A surveillance study focused on the years 2016–2019 reported that 64% and 16% of the analyzed S. Typhi isolates from Pakistan were XDR and MDR, respectively.63 In response, Pakistan became the first country to introduce TCVs which was administered to millions of children in 2019.64 Recent studies have demonstrated that single-dose of the TCV was effective in children including against XDR-typhoid.65 This result supports their future use, notably in countries with evolving and increasing evidence of AMR.
Typhoid Vaccines: Recent Developments
Typhoid vaccines constitute a major tool that can be used in the global effort to prevent typhoid fever. The WHO provides guidance for the programmatic use of typhoid vaccines to control typhoid fever including recommendations to include TCV into countries’ routine immunization programs as well as targeted catch-up vaccination. It also highlights the decision-making process for countries to decide on the best vaccination strategy.10 Three typhoid vaccines are currently in use worldwide, including the newer generation TCV with the Vi-polysaccharide antigen, the unconjugated polysaccharide vaccine (Vi-PS), and a vaccine based on the administration of oral live attenuated Salmonella strain Ty21a. TCV is currently the preferred formulation because of its immunological properties, wider usage (can be administered to children ≥6 months of age), and longer-lasting protection after a single dose. The TCV formulation has overcome some of the challenges that previously hindered the success of both polysaccharide and live vaccines.66 In this formulation, the S. Typhi Vi-polysaccharide is conjugated to a protein to elicit a stronger response from the immune system.
Several TCVs have been licensed nationally;67 the Vi-TT and Vi-CRM197 formulations are WHO-prequalified for use in children as young as 6 months and are thus the first typhoid vaccines to be approved for use in children under the age of 2 years (Table 1: Overview of WHO-Prequalified Typhoid Vaccines). This approval was particularly significant because of the high proportion of young children affected by typhoid fever. The WHO recommends the administration of TCVs in typhoid fever-endemic countries to children at 9 months of age or in the second year of life as a single dose.9,10 Several additional vaccine candidates are currently in development; others have already received a national license.68
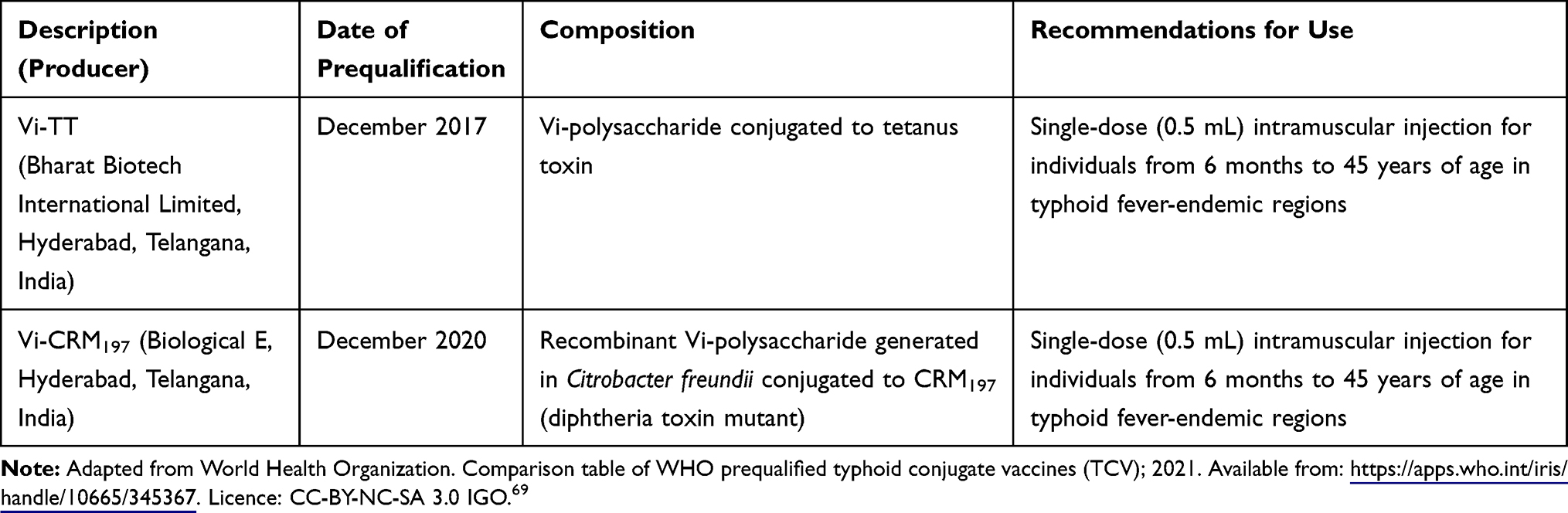 |
Table 1 Overview of WHO-Prequalified Typhoid Vaccines |
As per currently available data, the two prequalified vaccines are expected to perform comparably.69 The Typhoid Vaccine Acceleration Consortium (TyVAC) is conducting studies using the Vi-TT vaccine to evaluate efficacy (Malawi, Nepal), effectiveness (Bangladesh) and immunogenicity (Burkina Faso).66 The results from a Phase 3 trial carried out in Malawi involving 28,130 participants demonstrated both safety and 80.7% efficacy (95% CI, 64.2–89.6%) of the Vi-TT vaccine in children from 9 months to 12 years of age.70 Similar results have been reported from trials performed in Nepal and Bangladesh, with reports of 81.6% efficacy (95% CI, 58.8–91.8%) and 85.0% total vaccine protection (97.5% CI, 76.0–91.0%), respectively.71,72 New data available from the two-year follow-up of the randomized-controlled trial in Nepal revealed a protective efficacy against blood-culture confirmed typhoid fever of 79.0% (95% CI, 61.9–88.5%).73 These results were comparable to those from the interim analysis, which collectively indicate long-term vaccine protection and provide further support for its use in typhoid-endemic regions. Further, results also showed that the Vi-TT-TCV performed consistently well across different regions, populations and transmission settings with a robust safety profile.
The Typhoid Conjugate Vaccine Introduction in Africa program (THECA) has initiated a cluster-randomized trial in Ghana in 2021 and a mass vaccination campaign in the DRC in 2022 using the Vi-TT to generate information on its real-world effectiveness and impact.74 Similar evaluations of the Vi-CRM197 formulation are planned for Madagascar. It will be critical to assess vaccine efficacy and large-scale effectiveness particularly in settings with high disease burden and significant levels of AMR. However, the data currently available from Phase 3 trials and the first mass vaccinations permit optimism for the widespread application of Vi-TT, and potentially also other TCVs.
As emerging AMR remains a global concern for the treatment of typhoid fever as well as numerous other infectious diseases, vaccines are increasingly recognized as a potential solution. This point has received particular support from the findings of a study carried out in Pakistan that showed that Vi-TT was highly effective in combating an outbreak of XDR-typhoid fever (ie, 97% effectiveness against XDR-S. Typhi).65 Vaccination campaigns carried out in endemic areas might limit not only the incidence but also the spread of typhoid fever, thereby reducing the need for antibiotics and the development of AMR.
Gavi, the Vaccine Alliance, pledged its support toward the introduction of TCV in designated countries starting in 2019.75 Several countries have since applied for Gavi support with vaccine introductions planned for 2022.76 Rollout of the TCV in sub-Saharan Africa has started and continued throughout the COVID-19 pandemic. In April 2021, Liberia became the first country in sub-Saharan Africa (and the second country globally after Pakistan) to introduce TCV in a program aimed at vaccinating more than one million children. This was followed by a similar program in Zimbabwe later that same year.77 Malawi has recently received approval of their application to Gavi and plans to introduce TCV in the near future.78
Data from ongoing and future trials will also help elucidate the optimal use of TCV, including efforts to assess the local burden of disease, design and implementation of national vaccination strategies throughout Africa, as well as duration of protection exhibited through a single dose of TCV.76
While the development of typhoid fever vaccines has far progressed, the development of paratyphoid and iNTS vaccines are a decade behind. While there are currently no licensed vaccines available for either, there are several promising vaccine candidates of different compositions in the pipeline, with clinical trials ongoing.77,79,80 Further investment and research efforts are needed to accelerate developments.
Conclusion and the Way Forward
Numerous studies carried out over the last decade that focused on typhoid fever specifically in Africa have improved our understanding of the epidemiology of the disease and the population at risk. Findings from these studies showed the higher incidence of disease as well as its increased severity and mortality in the region. They have provided insight into factors with the potential to contribute to these severe outcomes, including limited access to healthcare and delays in diagnosis and treatment. Ongoing multi-site surveillance programs that include more countries than any study performed previously are designed to collect a wide range of data with a systematic focus on disease severity, mortality, and complications, thus circumventing one of the major limitations of previous studies. The findings from these systematic investigations will provide a more accurate description of disease severity and mortality and will thus serve to guide vaccine introduction strategies in African countries. However, it may be important to expand surveillance to include more rural areas and to determine the feasibility of environmental surveillance and serological assays (vide infra) to achieve an improved understanding of the spatiotemporal distribution of the disease. Both methods are currently under evaluation as an addition to ongoing surveillance programs. If successful, such tools could become powerful and low-cost methodologies to support the incidence assessments of S. Typhi infection and the impact of vaccination strategies introduced in many endemic countries.81 Additionally, as there is often a limited awareness and knowledge on infectious diseases in affected populations, another aspect to be considered is the education and community engagement in these respective populations, which could result in increased awareness and participation, as well as improved overall collaboration.82,83
Future efforts might also focus on improving diagnostic strategies for use under field conditions and remote settings. Other efforts might be directed toward effective treatment options, to provide care as early as possible to achieve better outcomes. Simultaneously, preventive measures should be introduced, primarily vaccination with prequalified TCV-vaccines in highly affected regions. This would help provide sustained protection against typhoid fever in the short term. Widespread vaccination will also limit the spread of MDR and XDR strains. Finally, efforts to improve water, sanitation, and health infrastructure in Africa should be developed and accomplished as long-term goals towards the global UN Sustainable Development Goals.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Basnyat B, Qamar FN, Rupali P, Ahmed T, Parry CM. Clinical update: Enteric Fever. BMJ. 2021;372:n437. doi:10.1136/BMJ.N437
2. Haselbeck AH, Panzner U, Im J, Baker S, Meyer CG, Marks F. Current perspectives on invasive nontyphoidal Salmonella disease. Curr Opin Infect Dis. 2017;30(5):498. doi:10.1097/QCO.0000000000000398
3. Dougan G, Baker S. Salmonella enterica serovar Typhi and the pathogenesis of typhoid fever. Annu Rev Microbiol. 2014;68:317–336. doi:10.1146/ANNUREV-MICRO-091313-103739
4. Crump J, Sjöund-Karlsson M, Gordon M, Parry C. Epidemiology, clinical presentation, laboratory diagnosis, antimicrobial resistance, and antimicrobial management of invasive Salmonella infections. Clin Microbiol Rev. 2015;28(4):901–937. doi:10.1128/CMR.00002-15
5. Cutler D, Miller G. The role of public health improvements in health advances: the twentieth-century United States. Demography. 2005;42(1):1–22. doi:10.1353/DEM.2005.0002
6. World Health Organization. Typhoid and other invasive salmonellosis. Vaccine-preventable diseases, surveillance standards; 2018. Available from: https://www.who.int/immunization/monitoring_surveillance/burden/vpd/WHO_SurveillanceVaccinePreventable_21_Typhoid_R1.pdf?ua=1.
7. John J, Van Aaart C, Grassly N. The burden of typhoid and paratyphoid in India: systematic review and meta-analysis. PLoS Negl Trop Dis. 2016;10(4):e0004616. doi:10.1371/JOURNAL.PNTD.0004616
8. World Health Organization. Typhoid; 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/typhoid.
9. Bentsi-Enchill AD, Hombach J. Revised global typhoid vaccination policy. Clin Infect Dis. 2019;68(Suppl 1):S31. doi:10.1093/CID/CIY927
10. World Health Organization. Typhoid vaccines: WHO position paper, March 2018 - recommendations. Vaccine. 2019;37(2):214–216. doi:10.1016/J.VACCINE.2018.04.022
11. Uzoka F-ME, Akwaowo C, Nwafor-Okoli C, et al. Risk factors for some tropical diseases in an African country. BMC Public Health. 2021;21(1):2261. doi:10.1186/S12889-021-12286-3
12. Mweu E, English M. Typhoid fever in children in Africa. Trop Med Int Health. 2008;13(4):532–540. doi:10.1111/J.1365-3156.2008.02031.X
13. Wain J, Hosoglu S. The laboratory diagnosis of enteric fever. J Infect Dev Ctries. 2008;2(06):421–425. doi:10.3855/jidc.155
14. Parry CM, Wijedoru L, Arjyal A, Baker S. The utility of diagnostic tests for enteric fever in endemic locations. Expert Rev Anti Infect Ther. 2011;9(6):711–725. doi:10.1586/ERI.11.47
15. Mogasale V, Ramani E, Mogasale V, Park J. What proportion of Salmonella Typhi cases are detected by blood culture? A systematic literature review. Ann Clin Microbiol Antimicrob. 2016;15(1). doi:10.1186/S12941-016-0147-Z
16. Dougan G. Typhoid in Africa and vaccine deployment. Lancet Glob Heal. 2017;5(3):e236–e237. doi:10.1016/S2214-109X(17)30045-1
17. Parry CM, Wijedoru L, Arjyal A, Baker S. The utility of diagnostic tests for enteric fever in endemic locations. Expert Rev Anti Infect Ther. 2014;9(6):711–725. doi:10.1586/ERI.11.47
18. Andrews JR, Khanam F, Rahman N, et al. Plasma immunoglobulin a responses against 2 Salmonella Typhi antigens identify patients with typhoid fever. Clin Infect Dis. 2019;68(6):949–955. doi:10.1093/CID/CIY578
19. Najib MA, Mustaffa KMF, Ong EBB, et al. Performance of immunodiagnostic tests for typhoid fever: a systematic review and meta-analysis. Pathog. 2021;10(9):1184. doi:10.3390/PATHOGENS10091184
20. Kim J-H, Im J, Parajulee P, et al. A systematic review of typhoid fever occurrence in Africa. Clin Infect Dis. 2019;69(Suppl 6):S492–S498. doi:10.1093/CID/CIZ525
21. Stanaway JD, Reiner RC, Blacker BF, et al. The global burden of typhoid and paratyphoid fevers: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Infect Dis. 2019;19(4):369–381. doi:10.1016/S1473-3099(18)30685-6
22. Marchello CS, Birkhold M, Crump JA. Complications and mortality of typhoid fever: a global systematic review and meta-analysis. J Infect. 2020;81(6):902–910. doi:10.1016/J.JINF.2020.10.030
23. Antillón M, Warren JL, Crawford FW, et al. The burden of typhoid fever in low- and middle-income countries: a meta-regression approach. PLoS Negl Trop Dis. 2017;11(2):e0005376. doi:10.1371/JOURNAL.PNTD.0005376
24. Marchello CS, Hong CY, Crump JA. Global typhoid fever incidence: a systematic review and meta-analysis. Clin Infect Dis. 2019;68(Suppl 2):S105–S116. doi:10.1093/CID/CIY1094
25. GBD results tool | gHDx. Available from: http://ghdx.healthdata.org/gbd-results-tool. Accessed November 7, 2021.
26. Britto C, Pollard AJ, Voysey M, Blohmke CJ. An appraisal of the clinical features of pediatric enteric fever: systematic review and meta-analysis of the age-stratified disease occurrence. Clin Infect Dis. 2017;64(11):1604–1611. doi:10.1093/CID/CIX229
27. Andrews JR, Vaidya K, Bern C, et al. High rates of enteric fever diagnosis and lower burden of culture-confirmed disease in peri-urban and rural Nepal. J Infect Dis. 2018;218(Suppl 4):S214–S221. doi:10.1093/INFDIS/JIX221
28. Breiman RF, Cosmas L, Njuguna H, et al. Population-based incidence of typhoid fever in an urban informal settlement and a rural area in Kenya: implications for typhoid vaccine use in Africa. PLoS One. 2012;7(1):e29119. doi:10.1371/JOURNAL.PONE.0029119
29. Gibani MM, Britto C, Pollard AJ. Typhoid and paratyphoid fever: a call to action. Curr Opin Infect Dis. 2018;31(5):440–448. doi:10.1097/QCO.0000000000000479
30. Marks F, Kalckreuth V, Aaby P, et al. Incidence of invasive Salmonella disease in sub-Saharan Africa: a multicentre population-based surveillance study. Lancet Glob Heal. 2017;5(3):e310–e323. doi:10.1016/S2214-109X(17)30022-0
31. Cruz Espinoza L, Nichols C, Adu-Sarkodie Y, et al. Variations of invasive Salmonella infections by population size in Asante Akim North Municipal, Ghana. Clin Infect Dis. 2016;62(Suppl 1):s17–s22. doi:10.1093/CID/CIV787
32. Park SE, Toy T, Cruz Espinoza LM, et al. The Severe Typhoid Fever in Africa program: study design and methodology to assess disease severity, host immunity, and carriage associated with invasive salmonellosis. Clin Infect Dis. 2019;69(Suppl 6):S422–S434. doi:10.1093/CID/CIZ715
33. Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid Fever. N Engl J Med. 2002;347(22):1770–1782. doi:10.1056/NEJMRA020201
34. Pieters Z, Saad NJ, Antillón M, Pitzer VE, Bilcke J. Case fatality rate of enteric fever in endemic countries: a systematic review and meta-analysis. Clin Infect Dis. 2018;67(4):628–638. doi:10.1093/CID/CIY190
35. Birkhold M, Coulibaly Y, Coulibaly O, et al. Morbidity and mortality of typhoid intestinal perforation among children in Sub-Saharan Africa 1995–2019: a scoping review. World J Surg. 2020;44(9):2892. doi:10.1007/S00268-020-05567-2
36. Feasey NA, Gaskell K, Wong V, et al. Rapid emergence of multidrug resistant, H58-lineage Salmonella Typhi in Blantyre, Malawi. PLoS Negl Trop Dis. 2015;9(4):e0003748. doi:10.1371/JOURNAL.PNTD.0003748
37. Phoba M, De Boeck H, Ifeka B, et al. Epidemic increase in Salmonella bloodstream infection in children, Bwamanda, the Democratic Republic of Congo. Eur J Clin Microbiol Infect Dis. 2014;33(1):79–87. doi:10.1007/S10096-013-1931-8
38. Breiman R. The rapidly re-emerging burden of endemic typhoid fever in the 21st Century: a preventable by-product of massive urbanization in the developing world? Int J Infect Dis. 2014;21:54. doi:10.1016/J.IJID.2014.03.531
39. Contini S. Typhoid intestinal perforation in developing countries: still unavoidable deaths? World J Gastroenterol. 2017;23(11):1925–1931. doi:10.3748/WJG.V23.I11.1925
40. Mogasale V, Desai SN, Mogasale VV, Park JK, Leon Ochiai R, Wierzba TF. Case fatality rate and length of hospital stay among patients with typhoid intestinal perforation in developing countries: a systematic literature review. PLoS One. 2014;9(4):e93784. doi:10.1371/JOURNAL.PONE.0093784
41. Butler T, Islam A, Kabir I, Jones P. Patterns of morbidity and mortality in typhoid fever dependent on age and gender: review of 552 hospitalized patients with diarrhea. Rev Infect Dis. 1991;13(1):85–90. doi:10.1093/CLINIDS/13.1.85
42. Azmatullah A, Qamar FN, Thaver D, Zaidi AKM, Bhutta ZA. Systematic review of the global epidemiology, clinical and laboratory profile of enteric fever. J Glob Health. 2015;5(2). doi:10.7189/JOGH.05.020407
43. Cruz Espinoza LM, McCreedy E, Holm M, et al. Occurrence of typhoid fever complications and their relation to duration of illness preceding hospitalization: a systematic literature review and meta-analysis. Clin Infect Dis. 2019;69(Suppl 6):S435–S448. doi:10.1093/CID/CIZ477
44. Jeon HJ, Marks F, Sugimoto J, et al. Surge of typhoid intestinal perforations as possible result of COVID-19–associated delays in seeking care, Madagascar. Emerg Infect Dis. 2021;27(12):3163–3165. doi:10.3201/EID2712.210516
45. Keddy KH, Smith AM, Sooka A, et al. The burden of typhoid fever in South Africa: the potential impact of selected interventions. Am J Trop Med Hyg. 2018;99(3 Suppl):55. doi:10.4269/AJTMH.18-0182
46. Bulage L, Masiira B, Ario AR, et al. Modifiable risk factors for typhoid intestinal perforations during a large outbreak of typhoid fever, Kampala Uganda, 2015. BMC Infect Dis. 2017;17(1). doi:10.1186/S12879-017-2720-2
47. Chalya P, Mabula J, Koy M, et al. Typhoid intestinal perforations at a University teaching hospital in Northwestern Tanzania: a surgical experience of 104 cases in a resource-limited setting. World J Emerg Surg. 2012;7(1):4. doi:10.1186/1749-7922-7-4
48. Parry CM, Thompson C, Vinh H, et al. Risk factors for the development of severe typhoid fever in Vietnam. BMC Infect Dis. 2014;14(1):1–9. doi:10.1186/1471-2334-14-73
49. Kaljee LM, Pach A, Garrett D, Bajracharya D, Karki K, Khan I. Social and economic burden associated with typhoid fever in Kathmandu and surrounding areas: a Qualitative Study. J Infect Dis. 2018;218(suppl_4):S243–S249. doi:10.1093/INFDIS/JIX122
50. Luthra K, Watts E, Debellut F, Pecenka C, Bar-Zeev N, Constenla D. A review of the economic evidence of typhoid fever and typhoid vaccines. Clin Infect Dis. 2019;68(Suppl 2):S83–S95. doi:10.1093/cid/ciy1122
51. Antillón M, Bilcke J, Paltiel AD, Pitzer VE. Cost-effectiveness analysis of typhoid conjugate vaccines in five endemic low- and middle-income settings. Vaccine. 2017;35(27):3506. doi:10.1016/J.VACCINE.2017.05.001
52. Bhutta ZA. Current concepts in the diagnosis and treatment of typhoid fever. BMJ Br Med J. 2006;333(7558):78. doi:10.1136/BMJ.333.7558.78
53. Argimón S, Yeats CA, Goater RJ, et al. A global resource for genomic predictions of antimicrobial resistance and surveillance of Salmonella Typhi at pathogenwatch. Nat Commun. 2021;12(1):1–12. doi:10.1038/s41467-021-23091-2
54. Azhar AB, Khalid A, Shah S. The implications of extensive drug-resistant typhoid fever: a Case Report. Cureus. 2019;11(6). doi:10.7759/CUREUS.5032
55. Mather RG, Hopkins H, Parry CM, Dittrich S. Redefining typhoid diagnosis: what would an improved test need to look like? BMJ Glob Heal. 2019;4(5). doi:10.1136/BMJGH-2019-001831
56. Rowe B, Ward LR, Threlfall EJ. Multidrug-resistant Salmonella Typhi: a worldwide epidemic. Clin Infect Dis. 1997;24(Suppl 1):S106–S109. doi:10.1093/clinids/24.Supplement_1.S106
57. Park SE, Pham DT, Boinett C, et al. The phylogeography and incidence of multi-drug resistant typhoid fever in sub-Saharan Africa. Nat Commun. 2018;9(1):1–10. doi:10.1038/s41467-018-07370-z
58. Mashe T, Gudza-Mugabe M, Tarupiwa A, et al. Laboratory characterisation of Salmonella enterica serotype Typhi isolates from Zimbabwe, 2009–2017. BMC Infect Dis. 2019;19(1):1–9. doi:10.1186/S12879-019-4114-0
59. Olaru ID, Mtapuri-Zinyowera S, Feasey N, Ferrand RA, Kranzer K. Typhoid Vi-conjugate vaccine for outbreak control in Zimbabwe. Lancet Infect Dis. 2019;19(9):930. doi:10.1016/S1473-3099(19)30425-6
60. Kariuki S, Dyson ZA, Mbae C, et al. Multiple introductions of multidrug-resistant typhoid associated with acute infection and asymptomatic carriage, Kenya. Elife. 2021;10. doi:10.7554/ELIFE.67852
61. Klemm EJ, Shakoor S, Page AJ, et al. Emergence of an extensively drug-resistant Salmonella enterica serovar Typhi clone harboring a promiscuous plasmid encoding resistance to fluoroquinolones and third-generation cephalosporins. MBio. 2018;9(1). doi:10.1128/mBio.00105-18
62. Qamar FN, Yousafzai MT, Khalid M, et al. Outbreak investigation of ceftriaxone-resistant Salmonella enterica serotype Typhi and its risk factors among the general population in Hyderabad, Pakistan: a matched case-control study. Lancet Infect Dis. 2018;18(12):1368–1376. doi:10.1016/S1473-3099(18)30483-3
63. Qamar FN, Yousafzai MT, Dehraj IF, et al. Antimicrobial resistance in typhoidal Salmonella: surveillance for enteric fever in Asia project, 2016–2019. Clin Infect Dis. 2020;71(Suppl3):S276–S284. doi:10.1093/CID/CIAA1323
64. Aslam F, Yue Y, Aziz M. Introduction of typhoid vaccine in the expanded immunization program of Pakistan. Hum Vaccin Immunother. 2021;17(7):2132. doi:10.1080/21645515.2020.1869496
65. Yousafzai MT, Karim S, Qureshi S, et al. Effectiveness of typhoid conjugate vaccine against culture-confirmed Salmonella enterica serotype Typhi in an extensively drug-resistant outbreak setting of Hyderabad, Pakistan: a cohort study. Lancet Glob Heal. 2021;9(8):e1154–e1162. doi:10.1016/S2214-109X(21)00255-2
66. Neuzil KM, Pollard AJ, Marfin AA. Introduction of typhoid conjugate vaccines in Africa and Asia. Clin Infect Dis. 2019;68(Suppl 1):S27. doi:10.1093/CID/CIY878
67. Sahastrabuddhe S, Saluja T. Overview of the typhoid conjugate vaccine pipeline: current status and future plans. Clin Infect Dis. 2019;68(Suppl 1):S22–S26. doi:10.1093/CID/CIY884
68. Syed KA, Saluja T, Cho H, et al. Review on the recent advances on typhoid vaccine development and challenges ahead. Clin Infect Dis. 2020;71(Suppl 2):S141–S150. doi:10.1093/CID/CIAA504
69. World Health Organization. Comparison table of WHO-prequalified typhoid conjugate vaccines (TCV); 2021. Available from: https://apps.who.int/iris/handle/10665/345367.
70. Patel PD, Patel P, Liang Y, et al. Safety and efficacy of a typhoid conjugate vaccine in Malawian children. N Engl J Med. 2021;385(12):1104–1115. doi:10.1056/NEJMOA2035916
71. Shakya M, Colin-Jones R, Theiss-Nyland K, et al. Phase 3 efficacy analysis of a typhoid conjugate vaccine trial in Nepal. N Engl J Med. 2019;381(23):2209–2218. doi:10.1056/NEJMOA1905047
72. Qadri F, Khanam F, Liu X, et al. Protection by vaccination of children against typhoid fever with a Vi-tetanus toxoid conjugate vaccine in urban Bangladesh: a cluster-randomised trial. Lancet. 2021;398(10301):675–684. doi:10.1016/S0140-6736(21)01124-7
73. Shakya M, Voysey M, Theiss-Nyland K, et al. Efficacy of typhoid conjugate vaccine in Nepal: final results of a phase 3, randomised, controlled trial. Lancet Glob Heal. 2021;9(11):e1561. doi:10.1016/S2214-109X(21)00346-6
74. Haselbeck AH, Tadesse BT, Park J, et al. Evaluation of Typhoid Conjugate Vaccine Effectiveness in Ghana (TyVEGHA) using a cluster-randomized controlled Phase IV trial: trial design and population baseline characteristics. Vaccines. 2021;9(3):281. doi:10.3390/VACCINES9030281
75. Soble A, Patel Z, Sosler S, Hampton L, Johnson H. Gavi support for typhoid conjugate vaccines: moving from global investments to country introduction. Clin Infect Dis. 2020;71(Suppl 2):S160–S164. doi:10.1093/CID/CIAA342
76. Carey ME, Diaz ZI, Broadstock M, Bailey R, Bentsi-Enchill AD, Larson HJ. Toward Control? The prospects and challenges of typhoid conjugate vaccine introduction. Clin Infect Dis. 2019;69(Suppl 5):S408–S411. doi:10.1093/CID/CIZ483
77. Shakya M, Neuzil KM, Pollard AJ. Prospects of future typhoid and paratyphoid vaccines in endemic countries. J Infect Dis. 2021;224(Supplement_7):S770–S774. doi:10.1093/INFDIS/JIAB393
78. International Vaccine Access Center (IVAC). Johns Hopkins Bloomberg School of Public Health. VIEW-hub. Available from: https://view-hub.org/.
79. Balasubramanian R, Im J, Lee JS, et al. The global burden and epidemiology of invasive non-typhoidal Salmonella infections. Hum Vaccin Immunother. 2019;15(6):1421–1426. doi:10.1080/21645515.2018.1504717
80. Martin LB, Simon R, MacLennan CA, Tennant SM, Sahastrabuddhe S, Khan MI. Status of paratyphoid fever vaccine research and development. Vaccine. 2016;34(26):2900–2902. doi:10.1016/J.VACCINE.2016.03.106
81. Uzzell CB, Troman CM, Rigby J, et al. Environmental surveillance for Salmonella Typhi as a tool to estimate the incidence of typhoid fever in low-income populations. medRxiv. 2021. doi:10.1101/2021.05.21.21257547
82. Marotta C, Nacareia U, Estevez AS, et al. Mozambican adolescents and youths during the COVID-19 pandemic: knowledge and awareness gaps in the provinces of sofala and tete. Healthc. 2021;9(3). doi:10.3390/HEALTHCARE9030321
83. Henley P, Igihozo G, Wotton L. One Health approaches require community engagement, education, and international collaborations—a lesson from Rwanda. Nat Med. 2021;27(6):947–948. doi:10.1038/s41591-021-01350-5
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.