Back to Journals » Clinical and Experimental Gastroenterology » Volume 12
The burden of irritable bowel syndrome and chronic constipation on health-related quality of life in black Africans: a comparison with healthy control subjects in Côte d’Ivoire, West Africa
Authors Mahassadi AK ![]() , Ebela PC, Bangoura AD, Attia AK
, Ebela PC, Bangoura AD, Attia AK
Received 29 October 2018
Accepted for publication 30 April 2019
Published 2 August 2019 Volume 2019:12 Pages 355—365
DOI https://doi.org/10.2147/CEG.S192563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wing-Kin Syn
Alassan Kouamé Mahassadi, Paulin Christian Ebela, Aboubacar Demba Bangoura, Alain Koffi Attia
Hepatology and Gastroenterology Unit, Centre Hospitalier et Universitaire de Yopougon, Abidjan, Côte d’Ivoire
Background: Although patients with irritable bowel syndrome (IBS) and chronic constipation (CC) have an impaired health-related quality of life (HRQoL), little is known in black African patients compared with control subjects. This study provided the magnitude and the influencing factors of HRQoL impairment in black African outpatients with IBS or CC compared with control subjects using the generic SF-36 questionnaire.
Materials and methods: One hundred and four consecutive black African outpatients complaining with IBS (n=72, mean age=38.9 years, female=62.5%) and CC (n=32, mean age=37.4 years, female=75%) met Rome 3 criteria were compared with 210 control subjects (mean age=37.4 years, 63.8% male). The SF-36 scores in all domains of HRQoL with the corresponding physical (PCS) and mental (MCS) composite scores between groups were compared with post hoc analysis and multivariate linear regression analysis for the assessment of the influencing factors.
Results: Overall, IBS and CC patients exhibited low SF-36 scores in the 8 domains of HRQoL in comparison with control subjects. IBS patients scored less in mental health (mean difference=−10.3, p=0.001), bodily pain (mean difference=−23.5, p≤0.0001), and social functioning domains (mean difference =−15.1, p=0.01) in comparison with CC patients. Post hoc analysis demonstrated a trend down of PCS (mean difference=−12.9, p<0.0001) and MCS (mean difference=−11.2, p=0.01) disfavoring IBS patients than those with CC in comparison with control subjects. In multivariate linear regression analysis, besides the negative impact of IBS and CC, factors influencing PCS were BMI (β=0.4; p=0.01) and comorbidities (β=−5.9; p=0.002). Those influencing MCS were the presence of remunerated activity (β=2.7, p=0.02), and patient living alone (β=9.4; p=0.04).
Conclusion: IBS and CC impact negatively on the HRQoL in black African subjects and more importantly in those with IBS than CC.
Keywords: irritable bowel syndrome, chronic constipation, quality of life, SF-36 questionnaire, black Africans
Introduction
Irritable bowel syndrome (IBS) and chronic constipation (CC) are both the most prevalent functional gastrointestinal diseases affecting, respectively, 11.2% and 14% of the individuals worldwide with geographical variations.1,2
IBS and CC are not life-threatening diseases.3 However, both impacts negatively on the health-related quality of life (HRQoL) causing high rates of care seeking behavior, direct and indirect medical costs, low productivity, and absenteeism.4–10
Various tools depicting health impairment are used to assess HRQoL in patients with functional gastrointestinal diseases.11 Among them, generic questionnaires such as the Medical Outcome Short Form quality of life (SF-36) have shown high accuracy and reliable results in Caucasian and Asian patients depicting low scores of HRQoL in patients with IBS and CC.4,5,12
The SF-36 is a psychometric evaluation of well-being in its physical and mental dimensions and comprises 36 items questioning various aspects of health status, particularly physical, psychological, and social functioning aspects.13 Besides diseases and disabilities, age, gender, body mass index, marital status, employment, and income are closely linked to health quality.14–17
The previous population-based studies markedly reported an impaired HRQoL in subjects with IBS or CC compared with healthy control subjects.4,5 Moreover, IBS and CC exerted psychological distress aggravating the impairment of HRQoL of those affected.3,18,19
IBS is subdivided into 4 symptomatic profiles and according to the stool pattern and frequency that are IBS with constipation predominant (IBS-C), IBS with diarrhea predominant (IBS-D), IBS with alternating diarrhea or constipation known as mixed IBS (IBS-M), and unclassified IBS.3
IBS and CC are prevalent in Africa and are the main reasons for seeking care amongst outpatients, while IBS-C is likely the most frequent subtype encountered in clinical practice.20–22
African subjects with IBS express more mystic beliefs regarding the chronicity and bothersomeness of their symptoms than those with CC that may hamper their health quality.23 In Nigeria, Ladep et al have reported that black Africans with IBS exhibit low scores of HRQoL and psychological distress.24 However, to our knowledge, there are no data reporting the magnitude of HRQoL impairment in black African subjects with IBS or CC compared with that of healthy control subjects.
Moreover, symptoms overlap between IBS and CC as subjects with CC may experience occasionally more severe abdominal symptoms (discomfort and bloating) than subjects with IBS-C suggesting a fluctuating score of HRQoL according to symptoms onset.25,26 Little is known about the HRQoL in black African subjects with IBS or CC and relevant influencing factors.
This study was undertaken to determine firstly, the HRQoL in black African subjects with IBS or CC, compared to that of healthy control subjects and, secondly, to assess factors associated with physical and mental dimensions impairment of HRQoL in patients with IBS and CC in African setting and the role of abdominal pain in patient with CC.
Materials and methods
Subjects
One hundred and four consecutive outpatients complaining with IBS (n=72, mean age=38.9 years, female=62.5%) and CC (n=32, mean age=37.4 years, female=75%) met Rome 3 criteria3 and referred to the gastroenterology units of the three tertiary care university hospitals (Cocody, Yopougon, Treichville) in Abidjan, the economic capital of Côte d’Ivoire from March to September 2016 were enrolled in the study. Outpatients were eligible if they met these following criteria: age ≥15 years old, absence of concomitant organic gastrointestinal diseases, presence of reading and writing skills, and capable to complete the survey questionnaire. Outpatients with organic gastrointestinal diseases such as infectious diarrhea, fever, hepatomegaly, splenomegaly, peptic ulcer, or having low education level or difficulties for reading and understanding words written in French or refusing to participate in the study were not included. For comparison, 210 control subjects (mean age=37.4 years, 63.8% male) were recruited from 3 cities of Côte d’Ivoire (Abidjan, Grand Bassam, and Bonoua). After they have read the consent form and accepted verbally to participate in the survey, both patients and control subjects were asked to complete the questionnaire. Those aged <18 years old completed the questionnaire under parental acceptance. The Ethics committee of the Medical and Scientific Board (Direction Medicale et Scientifique) of the teaching hospital of Yopougon approved the protocol of the study, the verbal consent method, and parental acceptance before the completion of the questionnaire.
The survey questionnaire
The survey questionnaire comprised three sections retrieving social and demographic data, clinical data and items related to SF-36 questionnaire,13 and stool patterns according to the Bristol stool scale.27
In the section retrieving clinical data, subjects were asked to respond to a set of questions (Box 1)
 |
Box 1 Survey questionnaire |
The SF-36 comprised 36 items or questions depicting the impact of diseases or disabilities on the state of well-being.13 These 36 items are grouped into 8 domains that are: physical activity (AP), role of physical limitation (RPL), role of emotional limitation (REL), bodily pain (BP), general health (GH), social functioning (SF), vitality (VT), and mental health (MH). The 8 domains are aggregated into 2 composites summaries: physical (PCS) and mental (MCS). The SF-36 score of an individual varies from 0 (minimal score) to 100 (maximal score).
Methods
Administration of the questionnaire
All patients attending the gastroenterology units for symptoms belonging to functional gastrointestinal diseases at the consultation unit were asked to fill the questionnaire, after the explanation of the purpose of the survey. Control subjects were recruited in the main streets of the cities mentioned earlier using a face-to-face interview method.28 Participants read the consent form and those who gave their consent were asked to fill the questionnaire. The questionnaire was completed by participants without any interference of the surveyor. Additional explanations were given by the surveyor to those who expressed difficulties to understand the meaning of some questions without any interference in the choice of the response.
Collection of data
Social, demographic, and clinical data were retrieved for all participants included in the study comprising, age, gender, medical history, weight, height, body mass index, body mass index, marital status (widowed, married, living with partner, separated), medical history (ongoing disease or treatment), the presence of remunerated activity, stools pattern, the scores of the 8 domains of HRQoL calculated from the 36 items of SF-36 questionnaire (AP, RPL, REL, BP, GH, VT, MH), and the corresponding composites summaries: PCS and MCS.13
Definitions
IBS was defined in those experiencing abdominal pain or discomfort occurring 3 times a week during the previous non-consecutive 3 months and lasting more than 6 months with observed changes in stool pattern and frequency.3 According to bowel movement habits, IBS-C were those having symptoms of CC as stated earlier and picking out from the questionnaire the images of type 1 or 2 as frequent stool pattern exhibited during the bowel movement. Those with IBS-D were those fulfilling also IBS criteria and picking out from the questionnaire the images of type 6 and 7 as frequent stool pattern exhibited during bowel movement according to Bristol stool scale.27
CC was defined in those meeting 2 of these following Rome 3 criteria (Box 2)3
 |
Box 2 Rome 3 criteria |
CC was ascertained when the subjects picked out from the questionnaire the images stools of type 1 or 2 scales as stool pattern frequently exhibited during bowel movement.27,29
Painful CC was defined as abdominal pain or discomfort occurring in those meeting Rome 3 criteria of CC but less than 3 times a week.3,29
The non-painful CC was the absence of abdominal pain or discomfort in those meeting Rome 3 criteria of CC.3,29
The ulcer-like disease was retained in those declaring to suffer from stomach ulcer without providing its assessment by upper digestive endoscopy and in those reporting burn or epigastric pain referring to functional dyspepsia.30
Statistical analysis
Continuous variables were expressed as means and standard deviation if normally distributed, otherwise as median and range. Categorical variables were expressed as number and percentage. The calculation of the 8 domains of HRQoL was assessed using the syntax for SPSS® available on www.umcg.nl and method described by Ware et al.31,32 The internal consistency of the SF-36 questionnaire was assessed using the Cronbach’s alpha estimate.33 The mean scores of HRQoL comparison between groups were done using the analysis of variance (ANOVA) with post hoc Bonferroni multiple comparison methods and significance level set at 0.02.34 The subgroup comparison among IBS and subgroups of CC patients was computed using Kruskal Wallis (KW) for nonparametric multiple comparisons using a SAS macro published by Elliot et al.35 The absence of finite cut-off of SF-36 scores that indicates a good HRQoL,36 we decided to use multivariate linear regression analysis to determine factors affecting physical and mental dimensions of HRQoL with PCS and MCS as dependant continuous variables. The adjustment variables were age, gender, BMI, remunerated activity, marital status, ongoing disease or treatment, and duration of the disease. The independent variables of interest were CC or IBS compared with the control group and CC compared with IBS. All the analysis was computed with SPSS version 16 and SAS version 9.0 using two sides tailed tests with a significance level less than 0.05.
Results
The characteristic description of enrollment
CC and IBS were found in women in 62.5% and 75%, respectively. Globally, 93 (89.4%) experienced abdominal pain or discomfort occurring more than 3 times a week in 41 (39.4%) patients, lasting more than 5 years in 55 (63.5%) patients. Irregular bowel movements were reported by 25 (24%) patients and 96 (37.5%) declared having less than 3 stools evacuations per week, mostly of type 1 (39.4%) and type 2 (20.2%) according to the Bristol stool scale. In addition to IBS or CC, 25 (29.8%) patients declared comorbidities (diabetes: 2 patients, arterial hypertension: 6 patients, ulcer-like pain: 23 patients). In contrast with the result of Rome 3 criteria, 54 (51.4%) and 50 (48.1) of interviewed patients self-reported having, respectively, IBS and CC. Baseline characteristics are depicted in Table 1. Based upon Rome 3 criteria, IBS-C was seen in 42 (58.3%) and diarrhea-predominant IBS in only 1 (14.4%) among patients with IBS. The remaining IBS patients (40.1%) were considered as having unclassified IBS (Table 1).
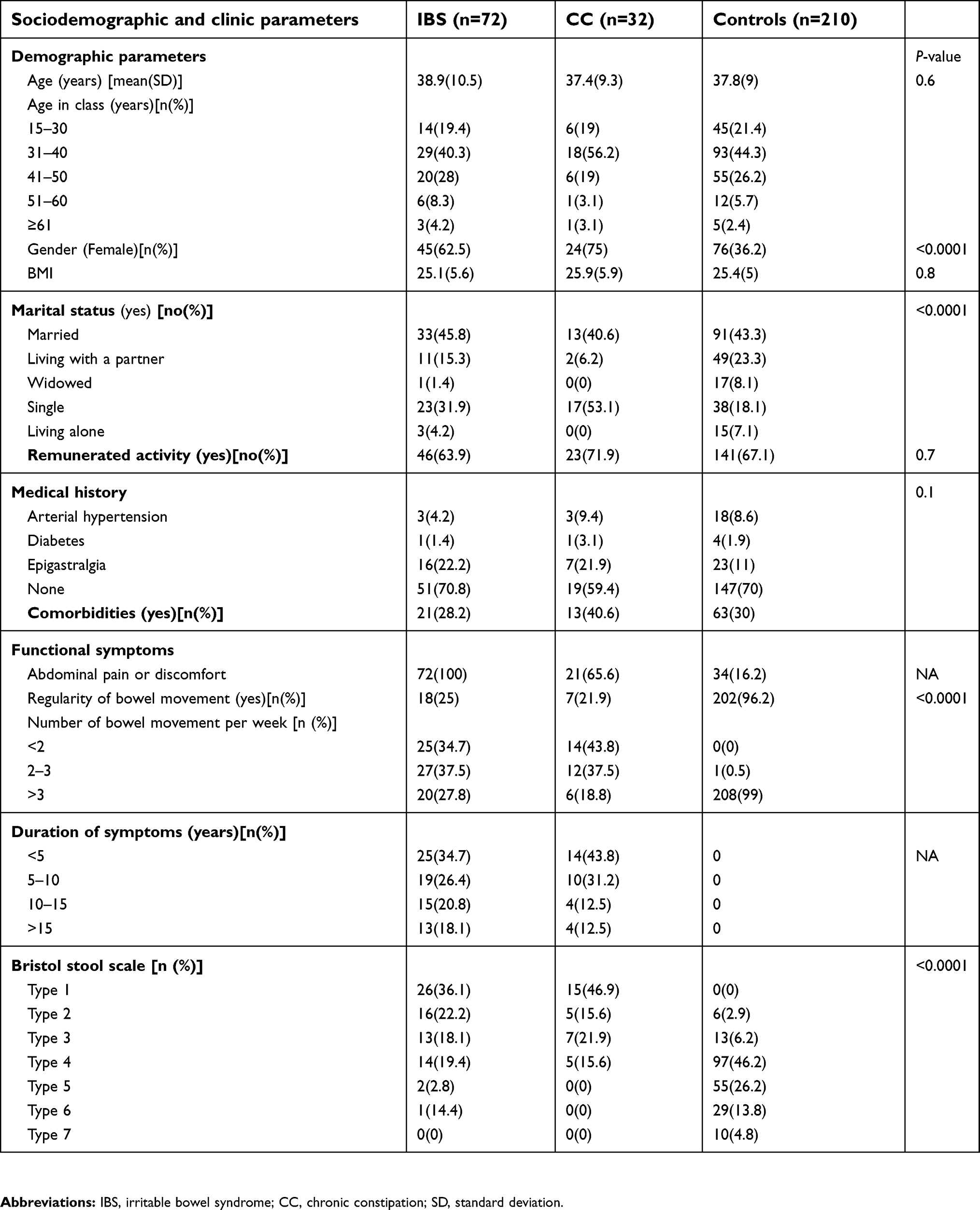 |
Table 1 Baseline characteristics at inclusion |
Distribution of SF-36 scores in the population of the study
As shown in Table 2, patients with IBS or CC obtained low SF-36 scores in the 8 domains compared to that of control subjects. More importantly, IBS patients had significantly lower SF-36 scores in 6 domains in comparison with CC patients except for PF and VT. Overall, PCS and MCS were profoundly low in IBS patients (mean differences of – 30.9 and –23.6, respectively) than that of CC patients (mean differences of −18 and −12, respectively) in comparison with control subjects. Overall, the internal consistency of the SF-36 questionnaire in our study was high with a Cronbach’s alpha estimate of 0.87. Within the subgroups, the Cronbach’s alpha estimates were 0.84, 0.81, and 0.76 in IBS, CC, and control groups, respectively.
 |
Table 2 Mean scores of SF-36 questionnaire items and differences comparison between groups |
There were any significant differences of the median or mean values of SF-36 scores adjusted with gender (Table 3) and age (Figure 1) within all subgroups of subjects with IBS, CC, or control groups.
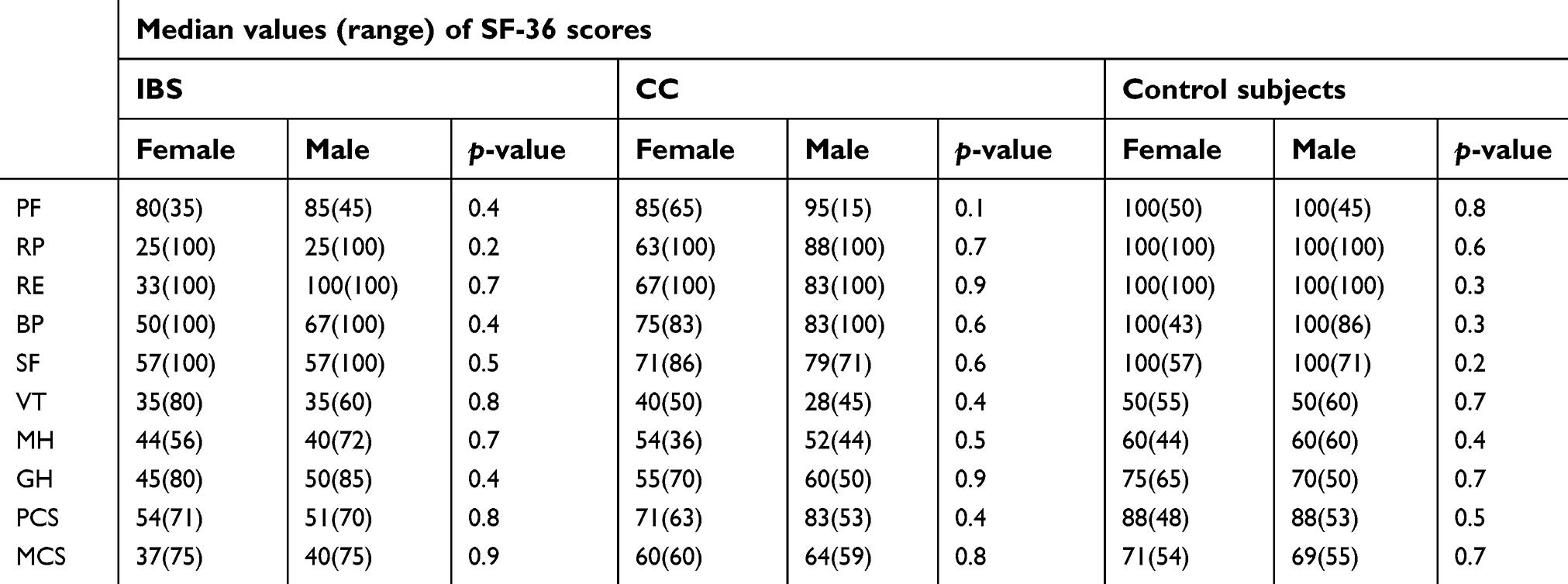 |
Table 3 Distribution of the scores of SF-36 questionnaire according to the gender within the subgroup of subjects with irritable bowel syndrome, chronic constipation, or control subjects |
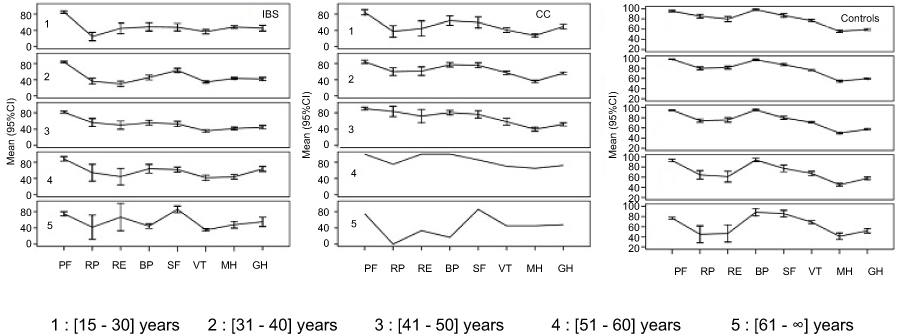 |
Figure 1 Distribution and trend of means scores of SF-36questionnaire items adjusted to age within all subgroups. Lines were smoothed because of the presence of one subject in the belonging age class. Abbreviations: IBS, irritable bowel syndrome; CC, chronic constipation; Ct, controls; PF, physical functioning; RP, role of physical; RE, role of emotional; BP, bodily pain; SF, social functioning; GH, general health; VT, vitality; MH, mental health; PCS, physical composite score; MCS, mental composite score. |
Post Hoc comparisons of the SF-36 scores
Post hoc analysis demonstrated that IBS patients had low PCS (mean difference=−12.9, p=0.01) and MCS (mean difference=−11.2, p=0.02) compared with CC patients. There was a trend down of PCS and MCS disfavoring IBS patients compared with CC patients and control subjects (Figure 2). IBS patients scored less in MH domain (mean difference=−10.3, p=0.001), BP domain (mean difference=−23.5, p≤0.0001), and SF domain (mean difference =−15.1, p=0.01) in comparison with CC patients (Table 2).
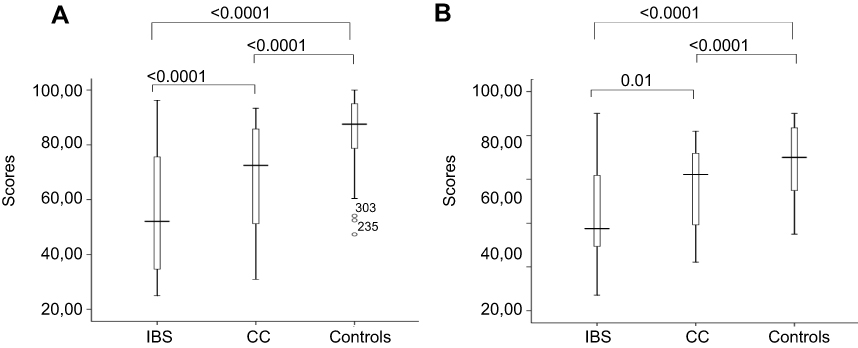 |
Figure 2 Box plots depicting the distribution and trends of physical (A) and mental (B) composite scores between patients with irritable bowel syndrome, chronic constipation, and control subjects. The box represents the interquartile range; the top and the bottom of the box are, respectively, the 25th and 75th percentile. The line across the box is the median. The lower and upper values are indicated by the whiskers. Stars and circles represent the outliers and extreme values. Abbreviations: IBS, irritable bowel syndrome; CC, chronic constipation. |
Influence of abdominal pain on HRQoL in patients with CC compared with IBS patients
Among the 32 patients with CC, 21 (65.6%) complained about abdominal pain. There were no differences between age and gender between groups. As shown in Figure 2, the overall comparison of the median score values of PCS (p=0.01) and MCS (p=0.03) was significantly different between IBS patients and subgroups of patients with no pain and painful CC. The post hoc analysis showed that IBS patients exhibited significant impairment of HRQoL both on its physical (median values of PCS: 52.1 vs 72.5, KW post hoc test=2.76, DF=2, p<0.05) and mental (median value of MCS: 37.5 vs 62.7, KW post hoc test=2.91, DF=2, p<0.05) dimensions than those with painful CC. In contrast, patients with no painful CC have a similar pattern of PCS (72.5 vs 52.1; p=ns) and MCS (53 vs 37.5; p=ns) in comparison with IBS patients (Figure 3).
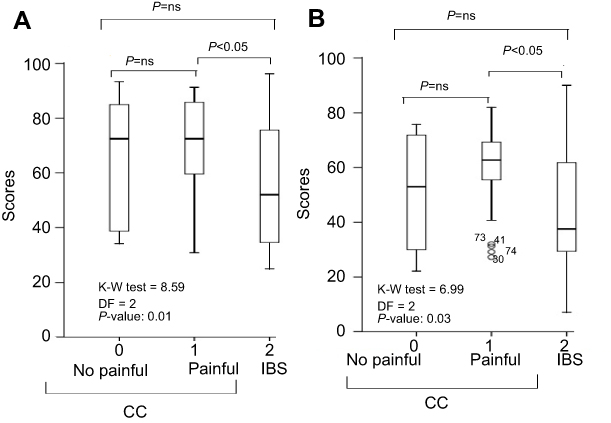 |
Figure 3 Box plots depicting the distribution, comparison, and trends of physical (A) and mental (B) composite summaries between subjects with no painful chronic constipation (0), painful chronic constipation (1) and irritable bowel syndrome (2). The box represents the interquartile range; the top and the bottom of the box are, respectively, the 25th and 75th percentile. The line across the box is the median. The lower and upper values are indicated by the whiskers. Stars and circles represent outliers and extreme values. SE: standard error, Q = calculated statistic, Q(0.05): the critical value of tabled Q statistic =2.39. KW = Kruskal Wallis test. Abbreviations: IBS, irritable bowel syndrome; CC, chronic constipation. |
Factors influencing the HRQoL between CC and IBS patients compared with control subjects
Influencing factors of HRQoL in comparison with control subjects
In multivariate analysis using control subjects, factors lowering PCS were comorbidities (β=−5.9, 95% IC=−9.7, −2.1, p=0.02), IBS (β=−30.1, 95% IC=−34, −26.2, p<0.0001), and CC (β=−17.3, 95% IC=−22.8, −11.9, p<0.0001) and the enhancing factor was BMI (β=0.4, 95% IC=0.1, 0.7, p=0.02).
For MCS, the lowering factors were IBS (β= −23.3, 95% IC= −27.9, −18.7, p<0.0001) and CC (β=−11.8, 95% IC=−18.3, −5.3, p=0.0004) and the enhancing factors were remunerated activity (β=2.7, 95% IC=0.4−5.1, p=0.02) and patient living alone (β=9.4, 95% IC=0.6, 18.3, p=0.04).
Factors influencing the HRQoL in the subgroup of patients with IBS or CC
Both BMI and a remunerated activity remained the enhancing factors of HRQoL when comparing IBS and CC patients. The duration of symptoms did not appear as a lowering factor (Table 4).
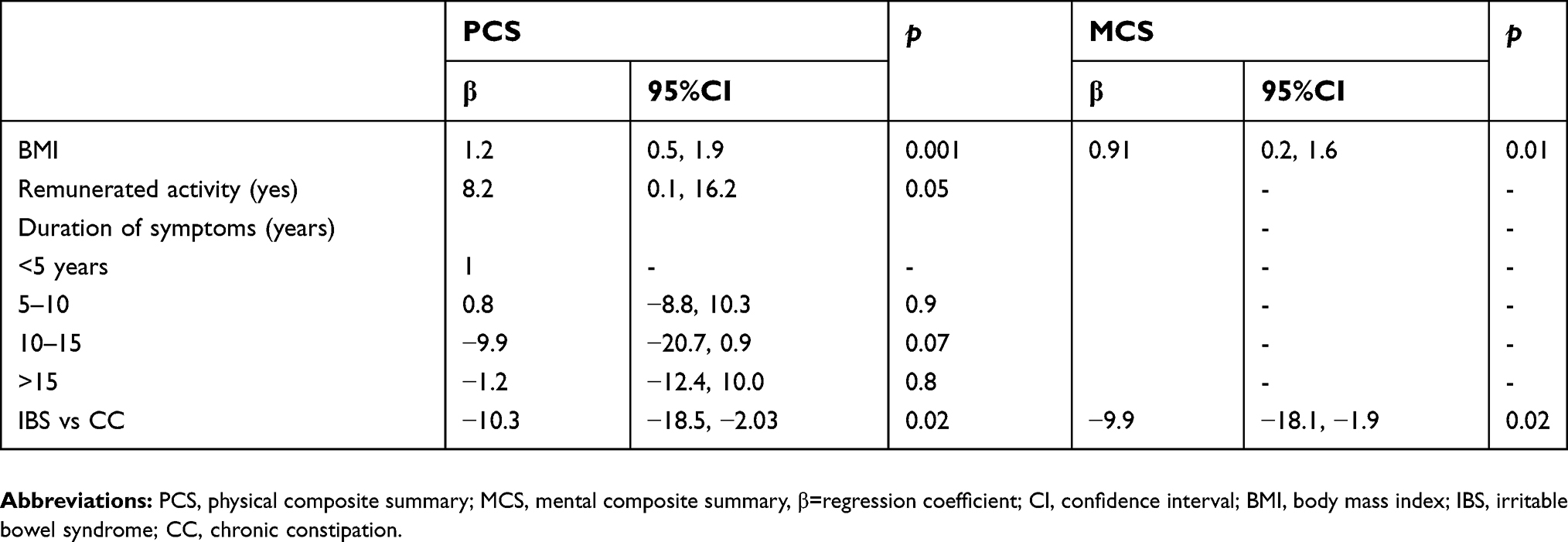 |
Table 4 Predictive factors affecting physical and mental composite summaries of the SF-36 scores in subjects with irritable bowel syndrome compared with those with chronic constipation: multivariate regression analysis |
Discussion
We have demonstrated in this study that black African patients with IBS and CC exhibit low HRQoL in comparison with control subjects. The mean differences of SF-36 scores in all dimensions of HRQoL were significantly lower in IBS patients than in CC patients in comparison with controls. Moreover, IBS patients have a profound impairment of HRQoL in comparison with CC patients. Painful constipation did not seem to reduce HRQoL in comparison with IBS. Besides CC and IBS, factors affecting HRQoL were BMI, marital status, and the presence of remunerated activity.
IBS and CC are known to impair HRQoL in several clinical studies from the western and Asian countries. Both IBS and CC patients exhibit lower SF-36 scores in all domains of HRQoL in comparison with US normative data and elsewhere, similar to our findings in Ivorian patients with IBS and CC.4,5,12,37
However, the magnitude of HRQoL impairment may differ between IBS and CC patients regarding the 8 domains of the SF-36 questionnaire in comparison with healthy subjects.38,39 In the study of Ruiz-Lopez, IBS-C and CC patients exhibit similar scores in the domains of physical functioning, role of physical limitation, role of emotional limitation, and general health except for vitality.38 Meanwhile in the study of Zhao et al, in Chinese patients using Rome 2 criteria, only mental health was significantly lower in IBS-C patients compared with CC patients.39 We have found similar results of the mean SF-36 scores on physical functioning and vitality domains between IBS and CC patients and low scores for other domains, particularly role of emotional limitation, social functioning, general health, and mental health. Moreover, in our study, the HRQoL was more profoundly affected in IBS patients with a disfavoring trend down of physical and mental composite scores. Similar patterns of HRQoL have been described in German subjects with IBS-C compared with those having functional constipation.40 However, in the study of Wong et al, in the United States, using the same profile of subjects and the SF-12 questionnaire, only the mental composite score was affected in IBS-C patients in comparison with subjects with functional constipation (48.9 vs 52.4, p<0.001).41
This discrepancy suggests different patterns of HRQoL. In Côte D’Ivoire, IBS and CC may alter both physical and mental dimensions of state of well-being and, more importantly in IBS subjects that may lead to anxiety and depression as reported in Nigerian IBS subjects.18,19,24 We have previously reported in Côte d’Ivoire that IBS subjects expressed mystic beliefs than those with CC.23 The valuable explanation is that, in Africa, the disease perception is surrounded by mysticism leading to psychological distress owing to the chronicity and bothersomeness of the underlying disease.4–10,42
IBS patients seeking care exhibit more severe symptoms and a high degree of anxiety compared with non-consulters and display low scores in physical functioning and role of physical functioning.43 In this study, physical functioning and vitality scores were lower compared with that of control subjects, but similar between IBS and CC patients, suggesting the existence of other factors that could motivate IBS and CC patients to seek care in an African setting.
Painful and no painful CC patients in our study have similar physical and mental composite scores of the SF-36 questionnaire. Painful constipation symptoms did not seem to alter the HRQoL of those with CC in comparison with IBS patients, probably due to the infrequent onset of pain during the course of constipation, even though, painful CC and IBS-C subjects have more symptoms of constipation than those with no painful constipation.3,29 However, the clinical spectrum of CC and IBS marked by the overlap of their symptoms may explain the same results of physical and mental composite scores of SF-36 questionnaire between non-painful constipation and IBS patients in our study.3,29
It was not surprising to find out that comorbidities were factors associated with physical dimension impairment of HRQoL. Diseases and disabilities are common sources of health quality impairment in human being.44 The beneficial effect of BMI on the physical component of HRQoL may be attributed to the mean value within the normal range of this variable in our study and closely linked to a better HRQoL in comparison with underweight or overweight subject.45 A remunerated activity may provide subsidies that promote a better well-being.14 Moreover, even though marriage status enhances good quality of life, the absence of marriage constraints in the African context may explain probably the favorable mental well-being of those living alone in our study.46,47
The main limitation of our study was the absence of finite characterization of the defecation pattern (straining, anal blockage, digital maneuver) exhibited by patients.3,48 IBS and painful CC are considered by some authors as two entities of the same disease that do not stabilize over time, which can lead to misclassification of patients due to the symptoms overlapping.40,41,49 Finally, the absence of cultural adaptation of the SF-36 questionnaire into local languages limits the generalizability of our results to nonliterate subjects in Côte d’Ivoire.50
However, our study provided new insights into the HRQoL in black African patients with IBS and CC. Finally, the results of HRQoL in patients with IBS and CC were globally in the line of previous reports confirming the reproducibility of the SF-36 questionnaire, whatever the environment and type of patients.4,5,12
In conclusion, IBS and CC impact negatively on the HRQoL in black African subjects in Côte d’Ivoire and more importantly in those with IBS-C. The assessment of HRQOL may be used to distinguish between IBS-C subjects and those with painful CC in order to motivate the use of the more psychological treatment in the former in an African setting.51
Acknowledgments
We want to thank Mr Gadafi Iddrisu Balali, Department of Theoretical and Applied Biology, Kwame Nkrumah University of Science and Technology, Kumasi Ghana, for having corrected the English translation of the manuscript.
Disclosure
Dr Alassan Kouamé Mahassadi reports personal fees and non-financial support from Genix Pharma and Sanofi, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012;10(7):712–721.e4. doi:10.1016/j.cgh.2012.02.029
2. Suares NC, Ford AC. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: systematic review and meta-analysis. Am J Gastroenterol. 2011;106:1582–1591. doi:10.1038/ajg.2011.164
3. Longstreth GF, Grant Thompson W, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterol. 2006;130:1480–1491. doi:10.1053/j.gastro.2005.11.061
4. Gralnek JM, Hays RD, Kilbourne A, Naliboff B, Mayer EA. The impact of irritable bowel syndrome on health-related quality of life. Gastroenterol. 2000;119:654–660. doi:10.1053/gast.2000.16484
5. Wald A, Scarpignato C, Kamm AM, et al. The burden of constipation on quality of life: results of a multinational survey. Aliment Pharmacol Ther. 2007;26:227–236. doi:10.1111/j.1365-2036.2007.03376.x
6. Talley NJ, Gabriel SE, Harmsen WS, Zinsmeister AR, Evans RW. Medical costs in community subjects with irritable bowel syndrome. Gastroenterol. 1995;109:1738–1741. doi:10.1016/0016-5085(95)90738-6
7. Nyrop KA, Palsson OS, Levy RL, et al. Cost of health care for irritable bowel syndrome, chronic constipation, functional diarrhoea and functional abdominal pain. Alim Pharm Ther. 2007;26:237–248. doi:10.1111/apt.2007.26.issue-2
8. Heidelbaugh JJ, Stelwagon M, Miller SA, Shea EP, Chey W. The spectrum of constipation-Predominant irritable bowel syndrome and chronic idiopathic constipation: US survey assessing symptoms, care seeking, and disease burden. Am J Gastroenterol. 2015;110:580–587. doi:10.1038/ajg.2015.67
9. Lee V, Guthrie E, Robison A, et al. Functional bowel disorders in primary care: factors associated with health-related quality of life and doctor consultation. J Psych Res. 2008;64:129–138. doi:10.1016/j.jpsychores.2007.09.004
10. Nellesen D, Yee K, Chawla A, Lewis BE, Carson RT. A systematic review of the economic and humanistic burden of illness in irritable bowel syndrome and chronic constipation. J Manag Care Pharm. 2013;19(9):755–764. doi:10.18553/jmcp.2013.19.9.755
11. Wong R, Drossman DA. Quality of life measures in irritable bowel syndrome. Expert Rev Gastroenterol. 2010;4(3):277–284. doi:10.1586/egh.10.19
12. Jeong JJ, Choi M-G, Cho Y-S, et al. Chronic gastrointestinal symptoms and quality of life n the Korean population. World J Gastroenterol. 2008;14(41):6388–6394. doi:10.3748/wjg.14.6388
13. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). Conceptual framework and item selection. Med Care. 1992;30(6):473–483.
14. Hemingway H, Nicholson A, Marmot M, Roberts R, Marmot M. The impact of socioeconomic status on health functioning as assessed by the SF-36 questionnaire: the whitehall II study. Am J Public Health. 1997;87:1484–1490. doi:10.2105/ajph.87.9.1484
15. Doll HA, Petersen SEK, Stewart-Brown L. Obesity and physical and emotional well-being: association between body mass index, chronic illness, and the physical and mental components of the SF-36 questionnaire. Obes Res. 2000;8(2):160–170. doi:10.1038/oby.2000.17
16. Kyu-Tae H, Eun-Cheol P, Jae-Hyun K, Sun J, Sohee P. Is marital status associated with quality of life? Health Qual Outcomes. 2014;12:109. doi:10.1186/s12955-014-0109-0
17. Hilka TK, Abulfathi A, Rosenkranz B, Bennett B, Schwenkglenks M, Sinanovic E. Health-related quality of life and its association with medication adherence, active pulmonary tuberculosis-A systematic review of global literature with focus on South Africa. Health Qual Life Outcomes. 2016;14:42. doi:10.1186/s12955-016-0442-6
18. Lee S, Wu J, Ma YL, Tsang A, Guo W-J, Sung J. Irritable bowel syndrome is strongly associated with generalized anxiety disorder: a community study. Aliment Pharmacol Ther. 2009;30:643–651. doi:10.1111/j.1365-2036.2009.04074.x
19. Cheng C, Chan AO, Hui WM, Lam SK. Coping strategies, illness perception, anxiety and depression of patients with idiopathic constipation: a population-based study. Alim Pharm Ther. 2003;18:319–326. doi:10.1046/j.1365-2036.2003.01663.x
20. Okeke EN, Ladep NG, Adah S, Bpwatda P, Agaba EI, Malu AO. Prevalence of irritable bowel syndrome: a community survey in an African population. Ann Afr Med. 2009;8(3):177–180. doi:10.4103/1596-3519.57241
21. Obonna GC, Arowolo AO, Agbakwuru A. Experience with colonoscopy in riverine southwestern Nigeria. J West Afr Coll Surg. 2012;2(2):63–73.
22. Onyekwere CA, Asiyanbi A, Obi J. IBS in Nigeria; is there a decline in prevalence? Gut. 2012;61:A297. doi:10.1136/gutjnl-2012-302514d.2
23. Ndri-Yoman T, Mahassadi AK, Toure A, et al. Black African patients with irritable bowel syndrome expressed mystic belief than those with chronic constipation. J Afr Hepatol Gastroenterol. 2010;4:103–109. doi:10.1007/s12157-010-0168-8
24. Ladep NG, Obindo TJ, Audu MD, Okeke EN, Malu AO. Depression in patients with irritable bowel syndrome in Jos Nigeria. World J Gastroenterol. 2006;12(48):7844–7847. doi:10.3748/wjg.v12.i48.7844
25. Talley NJ, Zinsmeister AR, Van Dyke C, Melton LJ. Epidemiology of colonic symptoms and the irritable bowel syndrome. Gastroenterol. 1991;101:927–934. doi:10.1016/0016-5085(91)90717-Y
26. Talley NJ, Weaver AL, Zinsmeister AR, Melton JLIII. Functional constipation and outlet delay: a population-based study. Gastroenterol. 1993;105:781–790. doi:10.1016/0016-5085(93)90896-K
27. Minguez Perez M. The bristol scale- A useful system to assess stool form? Rev Esp Enferm Dig. 2009;101(5):305–311.
28. Mathers N, Fox N, Hunn A. Surveys and Questionnaires. The NIHR RDS for the East Midlands/Yorkshire & the Humber. Nottingham: NIHR RDS; 2007.
29. Rey E, Balboa A, Mearin F. Chronic constipation, irritable bowel syndrome with constipation and constipation with pain/discomfort: similarities and differences. Am J Gastroenterol. 2014;109:876–884. doi:10.1038/ajg.2014.18
30. Tack J, Talley NJ, Camilleri M, et al. Functional gastroduodenal disorders. Gastroenterol. 2006;130:1466–1479. doi:10.1053/j.gastro.2005.11.059
31. Anonymous. Syntax file rand-36 V2. Available from: https://www.umcg.nl/SiteCollectionDocuments/research/institutes/SHARE/assessment%20tools/syntax_file_rand-6_v2_withoutaggregatescores.pdf. Accessed July 1, 2016.
32. Ware JE. SF-36 Health Survey. Manual and Interpretation Guide. Boston, Massachusets: The Health Institute, New England Medical Center; 1993.
33. Dennick R, Tavakol M. Making sense of cronbach’s alpha. Int J Med Edu. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
34. McHugh ML. Multiple comparison analysis testing in ANOVA. Bioch Med. 2011;21(3):203–209. doi:10.11613/BM.2011.029
35. Elliott AC, Hynan LS. A SAS(®) macro implementation of a multiple Kruskal-Wallis analysis. Comput Methods Programs Biomed. 2011;102(1):75–80. doi:10.1016/j.cmpb.2010.11.002
36. Lins L, Carvalho FM, SF-36 total score as a single measure of health-related quality of life: a scoping review. SAGE Open Med. 2016;4. 2050312116671725. doi:10.1177/2050312116671725
37. Jamali R, Jamali A, Poorrahnama M, et al. Evaluation of health-related quality of life in irritable bowel syndrome patients. Health Qual Life Outcomes. 2012;10:12. doi:10.1186/1477-7525-10-12
38. Ruiz-Lopez MC, Coss-Adame E. Quality of life in patients with different constipation subtypes based on the Rome III criteria. Revis Gastroenterol Mexico. 2015;80(1):13–20.
39. Zhao Y-F, Ma X-Q, Wang R, Yan X-Y, Zou D-W, He I. Epidemiology of functional constipation and comparison with constipation-predominant irritable bowel syndrome: the systematic investigation of gastrointestinal diseases in China (SILC). Aliment Pharmacol Ther. 2011;34:1020–1029. doi:10.1111/j.1365-2036.2011.04809.x
40. Enck P, Leinert J, Smid M, Thorsten K, Schwille-Kiuntke J. Functional constipation and constipation-predominant IBS in general constipation: data from the GECCO study. Gastroenterol Res Prac. 2016;9:1–9. Article ID:3186016.
41. Wong RK, Palsson OS, Turner MJ, et al. Inability of the Rome III criteria to distinguish functional constipation from constipation subtype irritable bowel syndrome. Am J Gastroenterol. 2010;105(10):2228–2234. doi:10.1038/ajg.2010.200
42. White P. The concept of diseases and health care in African traditional religion in Ghana. Theol Studies. 2015;71(3):7. doi:10.4102/hts.v71i3.2762
43. Ringström G, Abrahamsson H, Strid H, Simrén M. Why do subjects with irritable bowel syndrome seek health care for their symptoms. Scand J Gastroenterol. 2007;42(10):1192–1203. doi:10.1080/00365520701320455
44. Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu AL, Maltais D. Multimorbidity and quality of life in primary care: a systematic review. Health Qual Life Outcomes. 2004;4:51. doi:10.1186/1477-7525-2-51
45. Doll HA, Petersen S, Stewart-Brown SL. Well-being: associations between body mass index, chronic illness, and the physical and mental components of the SF-36 questionnaire. Obes Res. 2000;8(2):165–170. doi:10.1038/oby.2000.17
46. Diener E, Gohm CL, Suh E, Oishi S. Similarity of the relation between marital status and subjective well-being across cultures. J Cross-Cultural Psychol. 2000;31(4):419–436. doi:10.1177/0022022100031004001
47. Draper P. African marriage systems: perspectives from evolutionary ecology. Ethol Sociobiol. 1989;10(1):145–169. doi:10.1016/0162-3095(89)90017-4
48. Rao SS, Vellema T, Kempf J, Stessman M. Symptoms, stool patterns and quality of life in patients with dyssynergic defecation. Gastroenterology. 2000;118(4):A127. doi:10.1016/S0016-5085(00)82586-X
49. Siah K, Wong RK, Whitehead WE. Chronic constipation and constipation-predominant IBS: separate and distinct disorders or a spectrum of disease? Gastroenterol Hepatol. 2016;12(3):171–178.
50. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417–1432.
51. Palsson OS, Drossman DA. Psychiatric and psychological dysfunction in irritable bowel syndrome and the role of psychological treatments. Gastroenterol Clin N Am. 2005;34:281–303. doi:10.1016/j.gtc.2005.02.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.