Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
The association study of high-sensitivity C-reactive protein, pentraxin 3, nitrotyrosine, and insulin dose in patients with insulin-treated type 2 diabetes mellitus
Authors Bala C ![]() , Rusu A
, Rusu A ![]() , Ciobanu DM
, Ciobanu DM ![]() , Craciun AE
, Craciun AE ![]() , Roman G
, Roman G
Received 10 January 2018
Accepted for publication 27 March 2018
Published 28 May 2018 Volume 2018:14 Pages 955—963
DOI https://doi.org/10.2147/TCRM.S162086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Cornelia Bala, Adriana Rusu, Dana Mihaela Ciobanu, Anca Elena Craciun, Gabriela Roman
Department of Diabetes and Nutrition, Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca, Romania
Purpose: The objective of this study was to examine the association between insulin dose and high-sensitivity C-reactive protein (hsCRP), nitrotyrosine, and pentraxin 3 in patients with insulin-treated type 2 diabetes.
Patients and methods: Eighty patients with type 2 diabetes treated with insulin for >6 months and with stable insulin doses (±10%) within 3 months before inclusion were enrolled in this study. Medical history, including use of insulin and insulin doses, concomitant diseases and medication, and anthropometric and routine biochemical parameters were collected for each patient. hsCRP, nitrotyrosine, and pentraxin 3 were measured in fasting conditions. Comparison analysis was performed according to the distribution in tertiles of insulin dose/kg of body weight, and linear regression adjusted for confounding factors was used to examine the associations between markers of inflammation, oxidative stress, and insulin dose.
Results: In the comparison analysis, no statistically significant difference was found between hsCRP, nitrotyrosine, and pentraxin 3 levels across tertiles of insulin dose expressed as IU/kg of body weight (p for trend >0.05 for all comparisons) except a significantly higher hsCRP level in tertile 3 compared to tertile 1 (3.9±3.6 vs 6.1±3.8 mg/dL, p=0.035). In regression analysis, after adjustment for age, gender, smoking, body mass index, glycated hemoglobin, C-peptide, metformin, antiplatelet, and statin use, only hsCRP levels were statistically significant associated with insulin dose/kg of body weight (β=0.237, p=0.043).
Conclusion: In this sample of patients with type 2 diabetes treated with insulin for >6 months, hsCRP was positively associated with insulin doses. No such association was found for pentraxin 3, a more specific marker of vascular inflammation, and for nitrotyrosine as a marker of oxidative stress.
Keywords: inflammation, oxidative stress, insulin therapy, biomarkers
Introduction
Type 2 diabetes is characterized by a progressive loss of beta-cell function during the course of the disease, and insulin therapy is recommended when non-insulin strategies fail to maintain blood glucose control.1–3
In vitro studies demonstrate that insulin exerts anti-inflammatory, anti-oxidant, anti-apoptotic, and anti-thrombotic effects which are confirmed in some, but not all, studies including patients with insulin-treated type 2 diabetes.4–10 A number of retrospective cohort or case–control studies found a positive association between insulin use and increased mortality and cardiovascular disease (CVD) events in patients with type 2 diabetes.11–14 In contrast, randomized clinical trials (RCTs) that included patients with newly diagnosed type 2 diabetes or with dysglycemia such as United Kingdom Prospective Diabetes Study or Outcome Reduction with an Initial Glargine Intervention (ORIGIN) trial did not find any excess of CVD events in patients in the insulin arms compared with non-insulin strategies.1,15 The contradictory findings of cohort studies and RCTs can be at least partially explained by numerous other factors such as background CVD risk, diabetes duration, degree of insulin resistance, insulin dose, weight gain, and hypoglycemia that may contribute to variable CVD outcomes in patients with insulin-treated type 2 diabetes.16
Several cohort and case–control studies found an association between the duration of insulin exposure or increasing insulin doses and the total and cardiovascular mortality, major cardiovascular events, and cancer.11,17,18 In a cohort of adults with type 2 diabetes from a UK database, a gradual increase in total mortality was found in patients treated with higher insulin doses when a conventional multivariable regression analysis was used, but after applying marginal structural models, no association between insulin dose and mortality could be demonstrated.19 In a recent analysis from ORIGIN trial, higher insulin doses were not associated with higher incidence of the composite outcome which included cardiovascular death, myocardial infarction, and stroke in the overall insulin-treated arm or in the subset that achieved normoglycemia.20
To explain the possible relationship between high insulin doses and negative outcomes, it was hypothesized that in obese, insulin-resistant patients with type 2 diabetes with an excessive nutrient supply, the use of high insulin doses to override insulin resistance may be deleterious.21,22 The proposed mechanism is the imbalance between phosphoinositide 3-kinase/AKT and mitogen-activated protein kinase (MAPK) insulin signaling pathways with increased signaling through the MAPK pathway, which leads to increased endothelin-1 production and inflammation, vasoconstriction, and proliferation of vascular smooth muscle cells in the endothelium.23–25 Insulin at high dose is also thought to promote oxidative stress.24 It was thus suggested that insulin may be a “bifaceted” hormone with antiatherogenic or proatherogenic actions depending on dose used for achieving blood glucose control.25
To date, very limited clinical data are available on the relationship between insulin doses and markers of inflammation and oxidative stress in patients with type 2 diabetes.26,27 The study of the association of exogenous insulin doses administered in patients with type 2 diabetes, a pro-inflammatory state, with inflammatory markers is important in the context of existing non-insulin therapies. From a practical point of view, the clarification of the relationship between inflammatory markers and higher insulin doses needed to achieve an optimal glucose control may shed light on the choice among non-insulin therapies and insulin during the natural history of type 2 diabetes with potential positive effect on the risk of CVD in this population.
The objective of the study presented here was to examine the association between insulin dose and high-sensitivity C-reactive protein (hsCRP), nitrotyrosine, and pentraxin 3 in patients with type 2 diabetes treated with insulin for >6 months.
Patients and methods
Study design and participants
This was an observational cross-sectional study performed between July and November 2017 at Diabetes Center, Emergency County Clinical Hospital Cluj-Napoca, Romania (trial registration ACTRN12616001542482). Consecutive adult patients with type 2 diabetes presenting for a regular appointment were invited to participate. Patients were enrolled if they were treated with insulin alone or in association with other hypoglycemic agents for at least 6 months and with stable insulin dose (±10%) within 3 months before study inclusion. These 3 and 6 months time periods were chosen to limit the effect on inflammatory markers of glycemic variations during the titration period and of potential further changes of glycated hemoglobin (HbA1c) if steady-state effect of hypoglycemic agents used was not achieved. Exclusion criteria included type 1 diabetes, specific forms of diabetes, gestational diabetes, pregnancy and lactation, acute infections (respiratory, genitourinary, and others), acute episodes within 3 months prior to study inclusion that based on clinical judgment might have impaired glycemic control (eg cardiovascular events and surgical interventions), severe liver or kidney diseases (alanine aminotransferase [ALAT]/aspartate aminotransferase [ASAT] levels >3 × upper normal limit; estimated glomerular filtration rate [eGFR] <30 mL/min/1.73 m2), chronic inflammatory diseases, cancers with the exception of those declared cured for more than 5 years before inclusion, use of anti-inflammatory (except acetylsalicylic acid <300 mg/day) or immunosuppressive drugs within 3 months before study inclusion. Eighty patients fulfilling inclusion criteria and without exclusion criteria were enrolled and included in the analysis. The study was approved by the Institutional Ethics Committee of “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania, and was conducted according to the International Conference on Harmonization Good Clinical Practice Guidelines and the Declaration of Helsinki. All patients provided written informed consent before any study procedure.
Data collection
Detailed medical history (diabetes duration and therapy, concomitant diseases, and therapy), age, gender, results of anthropometrical measurements (weight, height, and waist circumference) and blood pressure values were collected by patient interviews, clinical examination, and from medical files. The presence of chronic complications of diabetes (diabetic retinopathy and diabetic peripheral neuropathy) was assessed by eye fundoscopy and foot examination. Height, weight, and waist circumference were measured in the morning, in fasting condition, with patients wearing light clothes and no shoes. Body mass index (BMI) was calculated as weight (kg)/height2 (m). Insulin dose/kg body weight was calculated as total dose of insulin in the previous day/weight (kg). Blood pressure was measured in sitting position after 5 minutes of rest. Hypertension was defined as a systolic blood pressure of ≥140 mmHg, a diastolic blood pressure ≥90 mmHg, and/or use of antihypertensive therapy. Dyslipidemia was diagnosed if low-density lipoprotein (LDL) cholesterol was ≥100 mg/dL and/or triglycerides ≥150 mg/dL and/or high-density lipoprotein (HDL) cholesterol <40 mg/dL in men and <50 mg/dL in women and/or use of statins or fibrates. Peripheral arterial disease was considered as present if ankle-brachial index performed as study procedure was <0.9.
Laboratory assessments
Fasting blood samples were collected for plasma glucose, HbA1c, total, LDL, and HDL cholesterol, triglycerides, creatinine, ASAT, ALAT, C-peptide, hsCRP, nitrotyrosine, and pentraxin 3. Biochemical measurements (plasma glucose, total, LDL, and HDL cholesterol, triglycerides, creatinine, ASAT, and ALAT) were performed on the day of collection by using routine enzymatic methods. HbA1c was determined by using ion-exchange chromatography. Samples for the assessment of C-peptide, hsCRP, nitrotyrosine, and pentraxin 3 were centrifuged on the same day and frozen until assessment by commercially available ELISA sandwich test, according to manufacturers’ instructions (Wuhan Fine Biological Technology, Wuhan, China for C-peptide; Hycult Biotech, Plymouth Meeting, PA, USA for hsCRP, nitrotyrosine and pentraxin 3). Urinary albumin excretion and urinary creatinine were assessed in a spot urine sample by using commercially available immunoturbidimetric methods. eGFR was calculated by using Chronic Kidney Disease Epidemiology Collaboration formula available online at http://www.qxmd.com/calculate-online/nephrology/ckd-epi-egfr.
Statistical analysis
Sample size calculation was performed with DSS calculator available at https://www.dssresearch.com. It was calculated that a sample of 80 patients, with at least 25 patients in each group of the 3 tertiles of insulin dose/kg of body weight would be required to detect a difference in the hsCRP levels among groups of 0.5 mg/dL with a statistical power of 97.1% and an alpha criterion of significance of 5%.
Statistical analysis was performed by using IBM® SPSS® Statistics version 20.0 (IBM Corporation, Armonk, NY, USA). Distribution of all quantitative variables was tested by using Kolmogorov–Smirnov tests, skewness, and kurtosis. Data were presented as number (proportions) for qualitative variables and as mean and standard deviation or median (quartile 1; quartile 3) for continuous variables, according to their distribution. Patients were divided in three groups according to tertiles of insulin dose/kg of body weight and assessed parameters were compared between these groups by using Student’s t-test, chi-square test, analysis of variance, and Kruskal–Wallis tests. The association between inflammatory markers (hsCRP, nitrotyrosine, and pentraxin 3) and insulin dose/kg of body weight was tested by using unadjusted and adjusted linear regression analyses. Factors used for the adjustment of linear regression model were those known to influence inflammatory and oxidative stress markers (age, gender, smoking, BMI, HbA1c, C-peptide, metformin, antiplatelet use, and statin use). Because nitrotyrosine had a non-Gaussian distribution, it was logarithmically transformed for the inclusion in the linear regression analysis as dependent variable. A two-sided p-value ≤0.05 was considered statistically significant.
Results
Mean age of the study participants was 63.8 years, mean BMI 32.5 kg/m2, and mean waist circumference 113.7 cm. Diabetes duration was 12.9 years and mean HbA1c 8.4%; 25.7% had diabetic retinopathy and 63.7% had diabetic peripheral neuropathy. All were treated with insulin (median dose/kg body weight 0.7 IU; minimum 0.18 IU/kg body weight; maximum 2.35 IU/kg of body weight) and 66.3% had metformin, 5.0% sulfonylurea, and 8.8% incretins associated with insulin therapy. Hypertension was present in 86.3% of the sample, dyslipidemia in 78.8%, and coronary heart disease (CHD) in 30.0%. As concomitant therapy, 48.8% were using statins, 20.0% fibrates, 31.3% angiotensin-converting enzyme inhibitors (ACEIs), 21.3% angiotensin-receptor blockers (ARBs), and 27.5% antiplatelet drugs (Table 1).
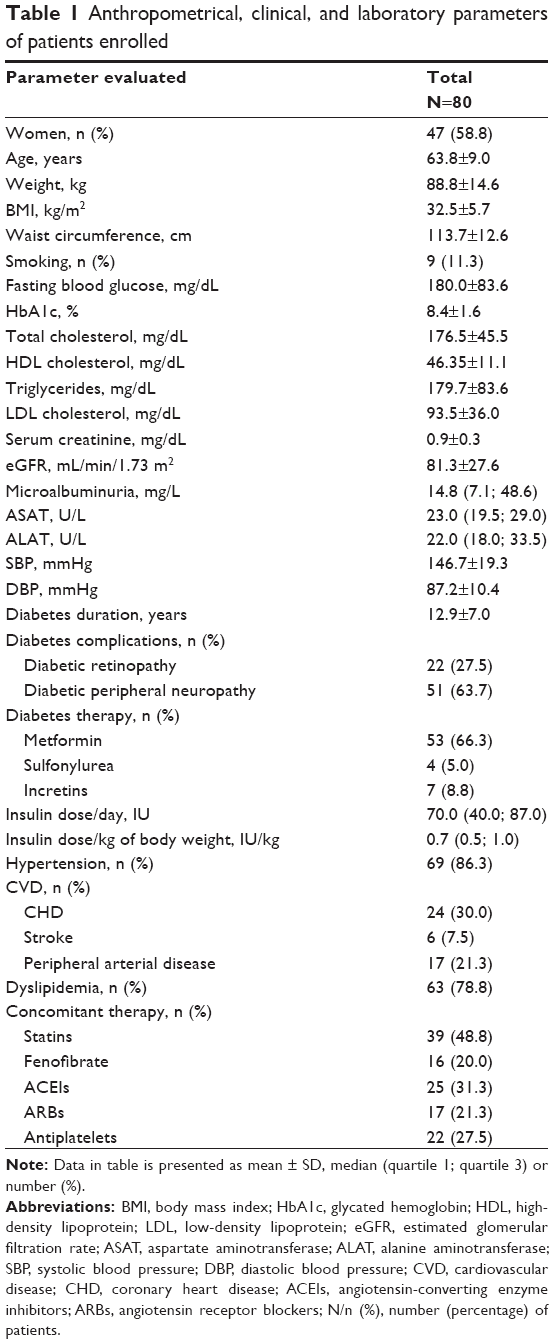 | Table 1 Anthropometrical, clinical, and laboratory parameters of patients enrolled |
Patients were divided into three groups according to tertiles of insulin dose/kg of body weight: group 1 – tertile 1 (0.18–0.57 IU/kg of body weight); group 2 – tertile 2 (0.58–0.89 IU/kg of body weight); group 3 – tertile 3 (0.90–2.35 IU/kg of body weight). Patients in the 3rd tertile had a significantly higher insulin dose/day (median 93.0 IU in tertile 3 vs 70.0 IU in tertile 2 and 31.0 IU in tertile 1, p<0.001). Also, those in the 3rd tertile of insulin dose/kg of body weight had a significantly higher frequency of arterial hypertension (96.3% vs 88.9% vs 73.1%, p=0.044) and CHD (44.4% vs 37.0% vs 7.7%, p=0.009) compared with those in the 1st and 2nd tertiles. No statistical significant differences between tertiles of insulin dose/kg of body weight were observed for age, BMI, smoking, diabetes duration, diabetes therapy, frequency of stroke and peripheral arterial disease, HbA1c, and other laboratory parameters evaluated. A statistically significant higher proportion of patients in the 2nd tertile of insulin dose/kg of body weight were using fibrates as compared to the other tertiles. The use of statins, ACEIs, ARBs, and antiplatelet drugs was similar in all tertiles of insulin dose/kg of body weight (Table 2).
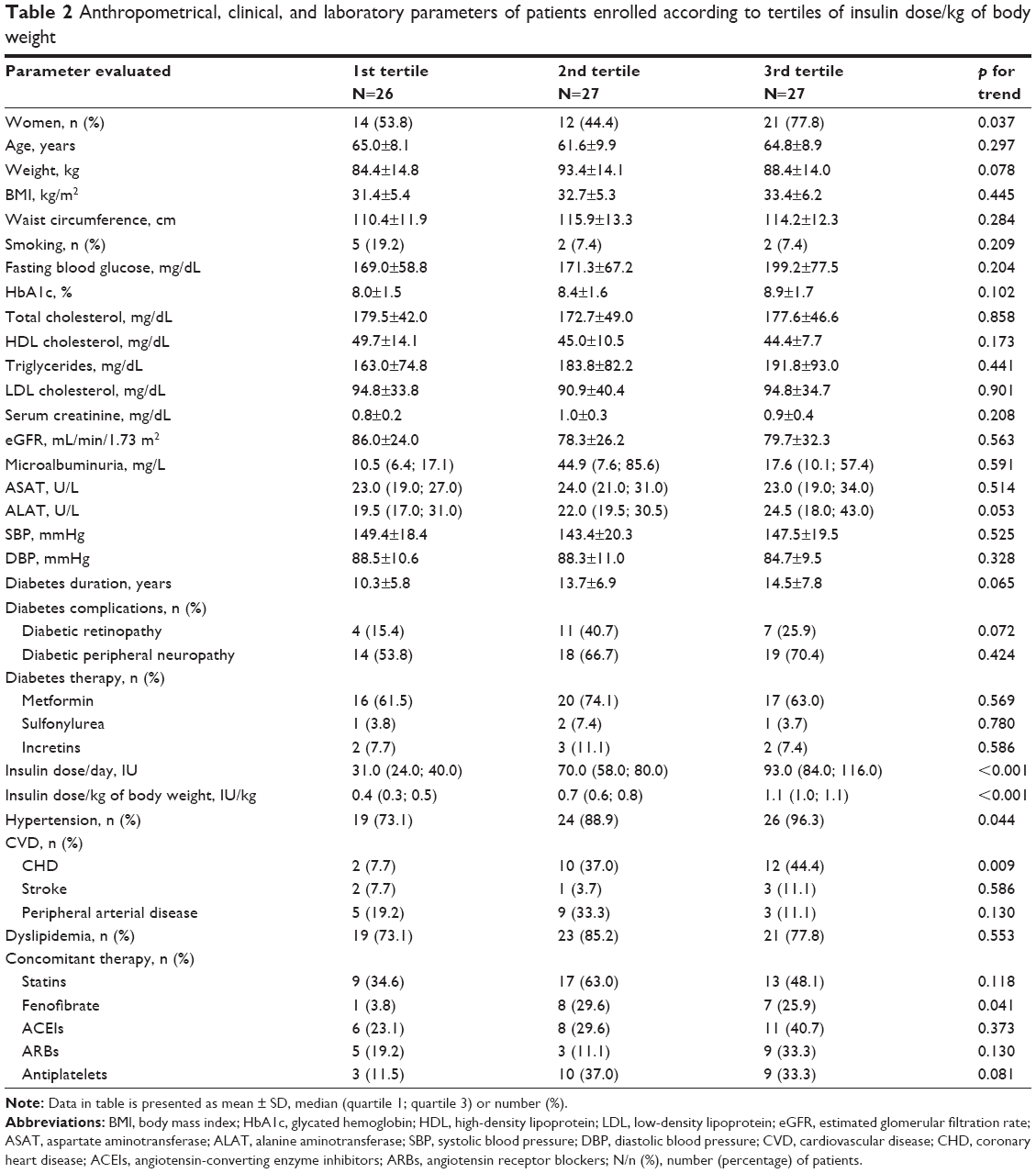 | Table 2 Anthropometrical, clinical, and laboratory parameters of patients enrolled according to tertiles of insulin dose/kg of body weight |
Fasting C-peptide levels ranged between 0.10 and 2.56 ng/mL. Median levels of C-peptide were similar in all tertiles of insulin dose/kg of body weight. Mean level of hsCRP was 4.9 mg/dL, increasing from 3.9 mg/L in the 1st tertile to 4.7 mg/dL in the 2nd tertile and 6.1 mg/dL in the 3rd tertile, with no statistical difference between the groups (p for trend =0.102). hsCRP was significantly higher in the 3rd tertile as compared to the values in the 1st tertile of insulin dose (p=0.035). For nitrotyrosine, although the levels were higher in the 2nd and the 3rd tertile of insulin dose as compared to the 1st tertile, the difference was not statistically significant (p for trend =0.412). Pentraxin 3 levels were similar in all tertiles of insulin dose/kg of body weight. No statistically significant difference was observed between the 1st and 3rd tertiles of insulin dose for nitrotyrosine and pentraxin 3 levels (Table 3).
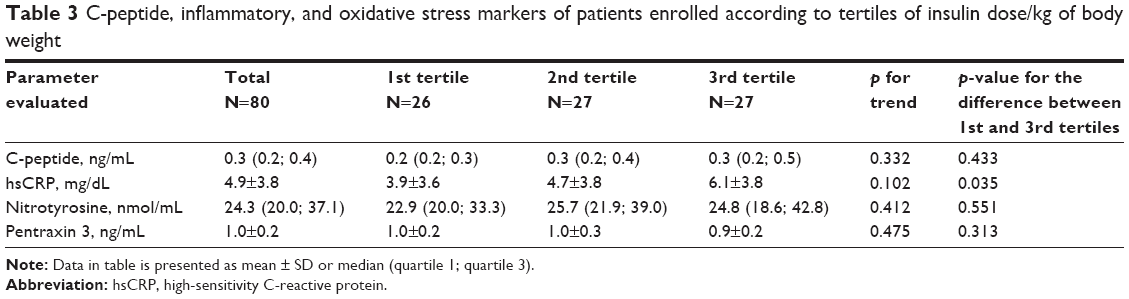 | Table 3 C-peptide, inflammatory, and oxidative stress markers of patients enrolled according to tertiles of insulin dose/kg of body weight |
Of the inflammatory and oxidative stress parameters evaluated, in the unadjusted model, only hsCRP was associated with insulin dose/kg of body weight (β=0.242, p=0.030). After adjustment for age, gender, smoking, BMI, HbA1c, C-peptide, metformin, antiplatelet, and statin use, hsCRP levels associated with insulin dose/kg of body weight remained statistically significant (β=0.237, p=0.043). Nitrotyrosine and pentraxin 3 levels were not associated with insulin dose/kg of body weight after adjustment for the above-mentioned parameters (p>0.05 for all; Table 4).
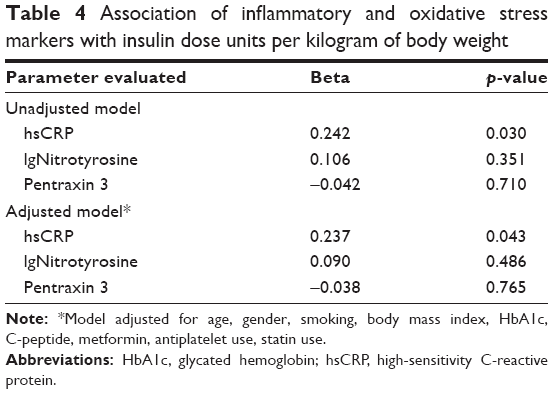 | Table 4 Association of inflammatory and oxidative stress markers with insulin dose units per kilogram of body weight |
Discussion
This study tested the hypothesis that higher insulin doses are associated with increased inflammation and oxidative stress in type 2 diabetes patients treated with insulin for >6 months and in those using stable insulin doses (±10%) during the last 3 months. In comparison analysis, we did not find statistically different levels of hsCRP, nitrotyrosine, and pentraxin 3 across tertiles of insulin dose expressed as IU/kg of body weight except a significantly higher hsCRP level in tertile 3 compared to tertile 1. In linear regression analysis, a statistically significant positive association was found between insulin dose and hsCRP levels after adjustment for age, gender, smoking, BMI, HbA1c, C-peptide, metformin, antiplatelet, and statin use. No association was found between nitrotyrosine and pentraxin 3 levels and insulin dose.
The role of inflammation and oxidative stress in promoting atherosclerosis is well-recognized in individuals with or without diabetes.27,28 In patients with type 2 diabetes, both the processes are under the influence of numerous factors: chronic hyperglycemia reflected by higher HbA1c levels, glucose variability, obesity and insulin resistance, renal disease, or smoking.29–31 Higher levels of C-peptide seem to play a role in CVD risk in patients with type 2 diabetes independently of other known CVD risk factors.32 Drugs commonly used for concomitant morbidities in type 2 diabetes were also shown to exhibit anti-inflammatory effects, and this was proven especially for statins, ACEIs, ARBs, aspirin, and to a lesser extent for fenofibrate.33–36 Antihyperglycemic agents, unless contraindicated, are frequently used in combination with insulin and potentially modify levels of low-grade inflammation. The best well-proven effect on inflammation and oxidative stress is attributed to metformin and pioglitazone, but reports on anti-inflammatory effect of the newer class of incretins are also available.37,38 In the present study we did not account for all possible factors mentioned above that might have interfered in the relationship between markers of inflammation, oxidative stress and insulin doses. Because of the small sample size, only age, gender, smoking, BMI, HbA1c, C-peptide, metformin, anti-platelet and statin use were used for adjustment in the regression analysis.
Many biomarkers can be used to assess low-grade inflammation and oxidative stress. In the present study, hsCRP and pentraxin 3 were chosen as markers of inflammation and nitrotyrosine for the assessment of oxidative stress. hsCRP is an acute-phase reactant and the most extensively studied systemic inflammatory biomarker in relation to CVD in observational and interventional studies.39 Pentraxin 3 is a long pentraxin belonging to the same family of pentraxins, which also includes two short pentraxins – CRP and serum amyloid P-component. Although CRP is produced primarily in liver, pentraxin 3 is released locally by vascular endothelial cells, smooth muscle cells, and macrophages as a response to vascular injuries and is considered a more specific marker of vascular inflammation.40 Its value as marker of atherosclerotic risk was demonstrated, among other studies, by the Multi-Ethnic Study of Atherosclerosis in which pentraxin 3 was associated with the incident CHD events and other markers of CV risk and subclinical atherosclerosis independent of CRP and conventional CVD risk factors.41
Nitrotyrosine is the result of the nitration of protein tyrosine residues in the presence of peroxynitrite, which is a potent oxidant produced by the reaction between superoxide ion and nitric oxide.42 Nitrotyrosine was used as a marker of oxidative stress in numerous studies and in various clinical conditions known to be associated with increased oxidative stress.43
The relationship between insulin and markers of inflammation or oxidative stress was examined in a limited number of studies and most of them evaluated the changes in metabolic markers following insulin initiation in type 2 diabetes. In two short-term (2–8 weeks) uncontrolled studies and one RCT with metformin as comparator, initiation of insulin treatment was shown to significantly decrease hsCRP, tumor necrosis factor-alpha, and interleukin (IL)-6 as compared to baseline and metformin, respectively.6–8 In other two studies, one observational and one having a randomized 2×2 factorial design with placebo/metformin and open-label glargine, no effects on hsCRP, leukocyte adhesion molecules, IL-6, and soluble tumor necrosis factor receptor 2 were seen compared to baseline or between study groups.9,10 In another study which included 43 insulin-naive patients, oxidative stress evaluated with urinary 8-iso-prostaglandin F2α was decreased only in the detemir group and not in the group assigned to three-time insulin aspart despite a greater improvement in plasma glucose seen in the aspart group. The authors speculated that, among other explanations, this finding could be attributed to the different doses of insulin (26.0±10.7 U/day for aspart and 13.7±4.9 U/day for detemir).44
Only two other studies that examined the relationship between inflammation or oxidative stress and insulin doses in patients with type 2 diabetes were found in the literature.26,27 In a group of 170 patients with type 2 diabetes of which 64 had a BMI <30.0 kg/m2 (non-obese group) and 106 had a BMI ≥30.0 kg/m2 (obese group), with 23% and 39% using insulin in non-obese and obese groups, respectively, and who were followed for 1 year after discharge from an intensive cardiac risk management clinic, there was a significant direct association between log CRP and both insulin use and daily dose for non-obese participants but not for obese participants.26 It should be mentioned that this is a retrospective analysis of an interventional study aiming to achieve and maintain strict glycemic, lipid, and blood pressure targets. At the 1-year follow-up, both the groups had mean HbA1c levels <7%, no significant weight changes as compared to baseline, and insulin doses used were small (9 IU/day in the non-obese and 28 IU/day in the obese group). No data on duration of diabetes or C-peptide levels were collected; therefore, the interpretation of the different results in non-obese and obese patients is challenging.
In the present study, a positive association between hsCRP and insulin dose in the overall study group was found, and this association remained significant after multivariate adjustment for several potential confounders, including BMI and C-peptide. The enrolled participants had a mean BMI similar to those in the obese group from the abovementioned study, with a mean diabetes duration of 12.9 years and a median C-peptide of 0.3 ng/mL showing a significantly diminished residual beta-cell function. Insulin doses were much larger (median insulin dose in the overall group was 70.0 U/day) and mean HbA1c was 8.4%. Therefore, this study group could be more typical for a type 2 diabetes population with longer exposure to insulin treatment.
Although hsCRP and pentraxin 3 are both markers of subclinical inflammation, the lack of association between pentraxin 3 and insulin doses observed could suggest that higher insulin doses do not increase the inflammation of the vascular wall, and this in turn may not be deleterious for vascular complications of diabetes. To prove this hypothesis, the measurement of pentraxin 3 in vascular endothelial cells could be more conclusive, but such a measurement in vivo would be technically challenging.
In an observational study of 122 persons with type 2 diabetes, the subgroup treated with a combination of metformin and insulin at a dose of <0.4 IU/kg had the lowest level of 24-h urinary excretion rates of 8-iso-prostaglandin F2α, a marker of oxidative stress, compared with the subgroups treated with either metformin and insulin at a dose of ≥0.4 IU/kg or oral hypoglycemic agents. Mean insulin doses ranged from 0.2 IU/kg/day in the group with <0.4 IU/kg to 0.47 IU/kg in basal insulin and 0.8 IU/kg in basal-bolus insulin from the group with ≥0.4 UI/kg.27 In the present study, no association between insulin doses and nitrotyrosine as marker of oxidative stress was observed. Mean doses of insulin used in patients enrolled in this research were higher than those in the study by Monnier et al,27 in which only patients using a mean insulin dose of 0.2 IU/kg/day had a decreased oxidative stress. Several limitations of the study should be acknowledged. The number of patients included is relatively small, which limited the number of factors for which adjustments were made in the regression analysis. Second, patients using low insulin doses were underrepresented as already in the first tertile median insulin dose was 0.4 IU/kg/day. Also, the cross-sectional design does not allow establishing causality between insulin doses, inflammation, and oxidative stress.
Conclusion
In this sample of patients with type 2 diabetes treated with insulin for >6 months, hsCRP was positively associated with insulin doses after adjustment for parameters known to influence the level of inflammatory and oxidative stress markers. No such association was found for pentraxin 3, a more specific marker of vascular inflammation, and for nitrotyrosine as marker of oxidative stress. The relevance of these findings for the clinical practice remains to be established. This study adds to the knowledge regarding the relationship between insulin dose and precursors of atherosclerotic disease, but further studies are needed to fully characterize this relationship which is of clear interest for the routine care of patients with diabetes. If the association between higher exogenous insulin doses and inflammatory markers is confirmed in larger populations, this may influence the choice of hypoglycemic agents in patients with important insulin resistance in which high insulin doses are required to achieve an optimal glucose control and may finally have a positive consequence on cardiovascular risk of these patients.
Acknowledgment
This work was supported by an internal grant financed by the “Iuliu Haţieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania (4944/5/8.3.2016).
Author contributions
CB had substantial contributions to conception and design, acquisition, and interpretation of data and drafted the article. AR contributed to acquisition, analysis, and interpretation of data and drafted the article. DMC and AEC contributed to data acquisition and interpretation and revised the draft critically for important intellectual content. GR contributed to conception and design and revised the draft critically for important intellectual content. All the authors approved the final version to be published and accept to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
CB declares speaker fees, sponsorships, and consultancy fees from AstraZeneca, Sanofi, Eli Lilly, Servier, Merck Sharpe&Dhome, Meda Pharmaceuticals, Novartis, Amgen, Unilever, and Danone. DMC received speaker fees from AstraZeneca and Sanofi. AEC declares speaker fees from Sanofi and Eli Lilly. GR declares speaker fees from AstraZeneca, Sanofi, Eli Lilly, NovoNordisk, Servier, Merck Sharpe&Dhome, Mylan, and Berlin Chemie, and consultancy fees from Sanofi and Eli Lilly. AR reports no conflicts of interest in this work.
References
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–853. | ||
Ferrannini E, Gastaldelli A, Miyazaki Y, Matsuda M, Mari A, DeFronzo RA. Betacell function in subjects spanning the range from normal glucose tolerance to overt diabetes: a new analysis. J Clin Endocrinol Metab. 2005;90:493–500. | ||
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the study of Diabetes (EASD). Diabetes Care. 2012;35:1364–1379. | ||
Dandona P, Chaudhuri A, Ghanim H, Mohanty P. Insulin as an anti-inflammatory and antiatherogenic modulator. J Am Coll Cardiol. 2009;53(5 Suppl):S14–S20. | ||
Yan H, Ma Y, Li Y, et al. Insulin inhibits inflammation and promotes atherosclerotic plaque stability via PI3K-Akt pathway activation. Immunol Lett. 2015;170:7–14. | ||
Takebayashi K, Aso Y, Inukai T. Initiation of insulin therapy reduces serum concentrations of high-sensitivity C-reactive protein in patients with type 2 diabetes. Metabolism. 2004;53:693–699. | ||
Bogdanski P, Pupek-Musialik D, Dytfeld J, et al. Influence of insulin therapy on expression of chemokinereceptor CCR5 and selected inflammatory markers in patients with type 2 diabetes mellitus. Int J Clin Pharmacol Ther. 2007;45:563–567. | ||
Mao XM, Liu H, Tao XJ, Yin GP, Li Q, Wang SK. Independent anti-inflammatory effect of insulin in newly diagnosed type 2 diabetes. Diabetes Metab Res Rev. 2009;25:435–441. | ||
Aviles-Santa L, Salinas K, Adams-Huet B, Raskin P. Insulin therapy, glycemic control, and cardiovascular risk factors in young Latin Americans with type 2 diabetes mellitus. J Investig Med. 2006;54:20–31. | ||
Pradhan AD, Everett BM, Cook NR, Rifai N, Ridker PM. Effects of initiating insulin and metformin on glycemic control and inflammatory biomarkers among patients with type 2 diabetes: the LANCET randomized trial. JAMA. 2009;302:1186–1194. | ||
Gamble JM, Simpson SH, Eurich DT, Majumdar SR, Johnson JA. Insulin use and increased risk of mortality in type 2 diabetes: a cohort study. Diabetes Obes Metab. 2010;12:47–53. | ||
Currie CJ, Poole CD, Evans M, Peters JR, Morgan CL. Mortality and other important diabetes-related outcomes with insulin vs other antihyperglycemic therapies in type 2 diabetes. J Clin Endocrinol Metab. 2013;98:668–677. | ||
Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet. 2010;375:481–489. | ||
Colayco DC, Niu F, McCombs JS, Cheetham TC. A1C and cardiovascular outcomes in type 2 diabetes: a nested case-control study. Diabetes Care. 2011;34:77–83. | ||
ORIGIN Trial Investigators, Gerstein HC, Bosch J, Dagenais GR, et al. Basal insulin and cardiovascular and other outcomes in dysglycemia. N Engl J Med. 2012;367:319–328. | ||
Ferrannini E, DeFronzo RA. Impact of glucose-lowering drugs on cardiovascular disease in type 2 diabetes. Eur Heart J. 2015;36:2288–2296. | ||
Holden SE, Jenkins-Jones S, Morgan CL, Schernthaner G, Currie CJ. Glucose-lowering with exogenous insulin monotherapy in type 2 diabetes: dose association with all-cause mortality, cardiovascular events and cancer. Diabetes Obes Metab. 2015;17:350–362. | ||
Stoekenbroek RM, Rensing KL, Bernelot Moens SJ, et al. High daily insulin exposure in patients with type 2 diabetes is associated with increased risk of cardiovascular events. Atherosclerosis. 2015;240:318–323. | ||
Gamble JM, Chibrikov E, Twells LK, et al. Association of insulin dosage with mortality or major adverse cardiovascular events: a retrospective cohort study. Lancet Diabetes Endocrinol. 2017;5:43–52. | ||
Gerstein HC, Ferrannini E, Riddle MC, et al; ORIGIN Trial Investigators. Insulin resistance and cardiovascular outcomes in the ORIGIN trial. Diabetes Obes Metab. 2018;20:564–570. | ||
Nolan CJ, Ruderman NB, Kahn SE, Pedersen O, Prentki M. Insulin resistance as a physiological defense against metabolic stress: implications for the management of subsets of type 2 diabetes. Diabetes. 2015;64:673–686. | ||
Bittencourt MS, Hajjar LA. Insulin therapy in insulin resistance: could it be part of a lethal pathway? Atherosclerosis. 2015;240:400–401. | ||
Cao W, Ning J, Yang X, Liu Z. Excess exposure to insulin is the primary cause of insulin resistance and its associated atherosclerosis. Curr Mol Pharmacol. 2011;4:154–166. | ||
Le Marchand-Brustel Y. Molecular mechanisms of insulin action in normal and insulin-resistant states. Exp Clin Endocrinol Diabetes. 1999;107:126–132. | ||
Monnier L, Hanefeld M, Schnell O, Colette C, Owens D. Insulin and atherosclerosis: how are they related? Diabetes Metab. 2013;39:111–117. | ||
Khatana SA, Taveira TH, Dooley AG, Wu WC. The association between C-reactive protein levels and insulin therapy in obese vs nonobese veterans with type 2 diabetes mellitus. J Clin Hypertens (Greenwich). 2010;12:462–468. | ||
Monnier L, Colette C, Michel F, Cristol JP, Owens DR. Insulin therapy has a complex relationship with measure of oxidative stress in type 2 diabetes: a case for further study. Diabetes Metab Res Rev. 2011;27:348–353. | ||
Szuszkiewicz-Garcia MM, Davidson JA. Cardiovascular disease in diabetes mellitus: risk factors and medical therapy. Endocrinol Metab Clin North Am. 2014;43:25–40. | ||
Hameed I, Masoodi SR, Mir SA, Nabi M, Ghazanfar K, Ganai BA. Type 2 diabetes mellitus: from a metabolic disorder to an inflammatory condition. World J Diabetes. 2015;6:598–612. | ||
Yang H, Jin X, Kei Lam CW, Yan SK. Oxidative stress and diabetes mellitus. Clin Chem Lab Med. 2011;49:1773–1782. | ||
Gluhovschi C, Gluhovschi G, Petrica L, et al. Urinary biomarkers in the assessment of early diabetic nephropathy. J Diabetes Res. 2016;2016:4626125. | ||
Wang L, Lin P, Ma A, et al. C-peptide is independently associated with an increased risk of coronary artery disease in T2DM subjects: a cross-sectional study. PLoS One. 2015;10(6):e0127112. | ||
Antonopoulos AS, Margaritis M, Lee R, Channon K, Antoniades C. Statins as anti-inflammatory agents in atherogenesis: molecular mechanisms and lessons from the recent clinical trials. Curr Pharm Des. 2012;18:1519–1530. | ||
Pacurari M, Kafoury R, Tchounwou PB, Ndebele K. The renin-angiotensin-aldosterone system in vascular inflammation and remodeling. Int J Inflam. 2014;2014:689360. | ||
Ridker PM, Cushman M, Stampfer MP, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997;336:973–979. | ||
Nita C, Bala C, Porojan M, Hancu N. Fenofibrate improves endothelial function and plasma myeloperoxidase in patients with type 2 diabetes mellitus: an open-label interventional study. Diabetol Metab Syndr. 2014;6:30. | ||
Nesti L, Natali A. Metformin effects on the heart and the cardiovascular system: a review of experimental and clinical data. Nutr Metab Cardiovasc Dis. 2017;27:657–669. | ||
Scheen AJ, Esser N, Paquot N. Antidiabetic agents: potential anti-inflammatory activity beyond glucose control. Diabetes Metab. 2015;41:183–194. | ||
Ridker PM. A Test in context: high-sensitivity C-reactive protein. J Am Coll Cardiol. 2016;67:712–723. | ||
Mantovani A, Garlanda C, Bottazzi B, et al. The long pentraxin PTX3 in vascular pathology. Vascul Pharmacol. 2006;45:326–330. | ||
Jenny NS, Blumenthal RS, Kronmal RA, Rotter JI, Siscovick DS, Psaty BM. Associations of pentraxin 3 with cardiovascular disease: the multi-ethnic study of atherosclerosis. J Thromb Haemost. 2014;12:999–1005. | ||
Beckman JS, Koppenol WH. Nitric oxide, superoxide, and peroxynitrite: the good, the bad, and ugly. Am J Physiol. 1996;271:1424–1437. | ||
Davies MJ, Fu S, Wang H, Dean RT. Stable markers of oxidant damage to proteins and their application in the study of human disease. Free Radic Biol Med. 1999;27:1151–1163. | ||
Naruse R, Takebayashi K, Morita K, Aso Y, Inukai T. Comparison of effects of insulin aspart three times a day versus insulin detemir once a day on oxidative stress in patients with type 2 diabetes. Endocr J. 2011;58:1055–1063. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.