Back to Journals » Drug Design, Development and Therapy » Volume 9
The association of CXCR4 expression with clinicopathological significance and potential drug target in prostate cancer: a meta-analysis and literature review
Received 9 February 2015
Accepted for publication 10 March 2015
Published 7 September 2015 Volume 2015:9 Pages 5115—5122
DOI https://doi.org/10.2147/DDDT.S82475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Shu-Feng Zhou
Qi Chen, Tie Zhong
Department of Urology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xian, Shaanxi Province, People’s Republic of China
Abstract: CXCR4/CXCL12 axis plays an important role in tumor growth, angiogenesis, metastasis, and therapeutic resistance. The aim of this study is to perform a meta-analysis and literature review to evaluate the association of CXCR4 expression with clinicopathological significance and prognosis in patients with prostate cancer (PCa). A detailed literature search was made in Medline, EMBASE, Web of Science, and Google Scholar for related research publications. The data were extracted and assessed independently. Analysis of pooled data was performed using Review Manager 5.2. Odds ratio (OR) with corresponding confidence intervals were calculated and summarized. The meta-analysis included a total of eleven studies and 630 patients. The rate of CXCR4 protein expression in PCa was significantly higher than in nonmalignant prostate tissues (OR =35.71, P<0.00001). The expression of CXCR4 protein was not significantly associated with Gleason score (P=0.73). However, the frequency of CXCR4 protein expression was significantly higher in T3–4 stage than in T1–2 stage of PCa (OR =2.35, P=0.001). The expression of CXCR4 protein was significantly associated with the presence of lymph node and bone metastasis of PCa: for lymph node metastasis positive versus negative, OR was 5.07 and P=0.0003, and for bone metastasis positive versus negative, OR was 7.03 and P=0.003. Cancer-specific survival of patients with PCa was significantly associated with CXCR4 protein expression, and the pooled Hazard ratio was 0.24 and P=0.002. In conclusion, the high expression of CXCR4 protein is a diagnostic biomarker of PCa, and it is significantly associated with T stages. The increased expression of CXCR4 protein is significantly associated with lymph nodes or bone metastasis, and CXCR4 is a poor prognosis predictor for patients with PCa. Taken together, our findings indicate that CXCR4 could be a target not only for the development of therapeutic intervention but also for the noninvasive monitoring of PCa progression.
Keywords: prostate cancer, CXCR4, CXCL12, prognosis, metastasis
Introduction
Prostate cancer (PCa) is the most common cancer in men and the second leading cause of cancer-related death among men in developed countries.1 The most common cause of mortality in PCa is not the primary tumor growth but rather the spread of the cancer to other organs, predominantly to bone.2 Therefore, understanding the molecular mechanism of the metastatic pathway would be crucial in elucidating the mechanisms of PCa progression and developing new therapy strategy.3
Chemokines, small proinflammatory chemoattractant cytokines that bind to specific G-protein coupled seven-span transmembrane receptors,4 are major regulators of cell trafficking and adhesion,5–7 survival,8,9 proliferation,10 and gene transcription.11 Chemokine receptor 4 (CXCR4) is an alpha-chemokine receptor specific for stromal-derived-factor-1 (SDF-1, now renamed CXCL12), a molecule endowed with potent chemotactic activity for lymphocytes.12 CXCR4 had gained tremendous attention over the past decade ever since it was found to be upregulated in a wide variety of cancer types and contributed to the tumor growth, angiogenesis, metastasis, and therapeutic resistance.13–16 Recent advances in the field of cancer biology has also pointed to the critical role that CXCR4 and its ligand CXCL12 play in cancer stem cell renewal and the metastasis of various types of cancer, including PCa.17,18 However, the clinical relevance of the expression of CXCR4 in PCa remains controversial, and the association between CXCR4 expression and clinicopathological features is inconclusive due to the relatively small number of tested samples in each study. Lee et al performed a meta-analysis and reported increased CXCR4 expression in PCa is associated with the presence of metastasis but not associated with T stages of PCa.19 We performed a meta-analysis to investigate not only the association between CXCR4 expression and clinicopathological features but also the precise relationship of CXCR4 expression to prognosis in patients with PCa in the present study.
Methods
Selection criteria and study search
We conducted a literature search for relevant articles without any language restrictions by using PubMed (January 1966–January 2015), Web of Science (January 1945–January 2015), and EMBASE (January 1980–January 2015). The keywords “Chemokine receptor 4” or “CXCR4” and “prostate cancer” or “prostate carcinoma” were used for searching the relative articles. There were 157 articles identified from PubMed, 342 articles from Web of Science, and 462 articles from EMBASE. A total of 842 articles were identified from Google Scholar. Only the first 300 of the articles were screened because the rest of them were not related to the present study. A total of 1,261 articles were screened by article titles and abstracts. A manual search of the reference lists from the included articles was also conducted to identify other potential publications.
We included studies that met the following criteria: 1) The association between CXCR4 protein expression and the clinicopathological features of PCa and 2) the association of CXCR4 protein expression and prognosis in patients with PCa. After screening by article titles and abstracts, 20 relevant articles were included for full-text review. The following exclusion criteria were used: 1) investigating the association between CXCR4 mRNA expression and clinicopathological significance, 2) utilizing the same population or overlapping database, and 3) the studies utilized cell lines or mice. Eleven articles were eligible for inclusion in this meta-analysis. The detailed information of eleven relevant articles is listed in Table 1.
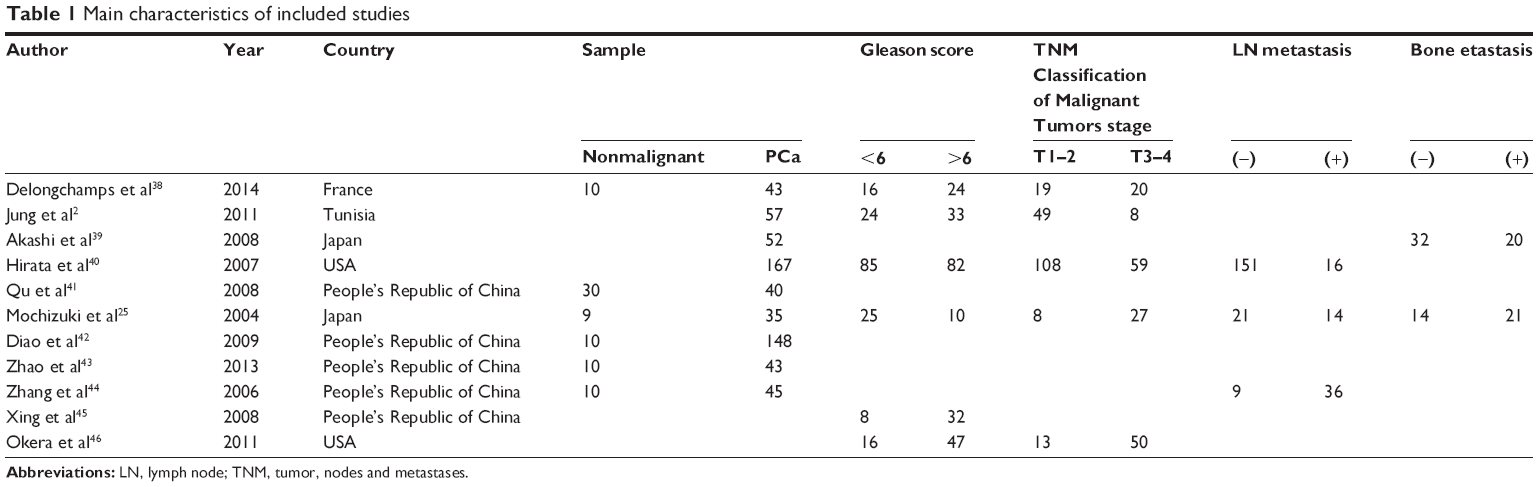 | Table 1 Main characteristics of included studies |
Data extraction and study assessment
Two reviewers (QC and TZ) independently extracted data from selected studies using a standardized data extraction form. Any disagreement was discussed and reached a consensus for all issues. The following items were collected from each study: first author’s name, year of publication, geographical location, sample size of different histologic categories of PCa, T stage, Gleason score, lymph node and bone metastasis status, and prognosis in patients with PCa.
Statistics analysis
Odds ratios (ORs) with its 95% confidence intervals (CIs) were calculated. Heterogeneity among studies was estimated using the Cochran’s Q statistic and I2 tests. A fixed effect model was used for I2<50%, while a random effect model was used for I2>50%. The analysis was performed to compare the frequency of CXCR4 protein expression between PCa and nonmalignant prostate tissue. In addition, we evaluated the rate of CXCR4 protein positive immunolabeling of tumor tissue in different T stages, Gleason score, different lymph node, and bone metastasis status. The immunostaining was scored according to the intensity of positive staining. Negative staining was no staining or weak staining, while positive staining was moderate or strong staining. All P-values were two-sided. Funnel plots were used for the detection of publication bias. All analyses were performed using Review Manager 5.2 (Cochrane Collaboration, Software Update, Oxford, UK).
Results
Eleven relevant articles were included for full review and meta-analysis (Figure 1). The following items were collected from each study: first author’s name, year of publication, number of patients with PC, benign prostate hyperplasia, para tumor tissue or normal prostate tissue, T stages, Gleason score, and prognosis (Table 1).
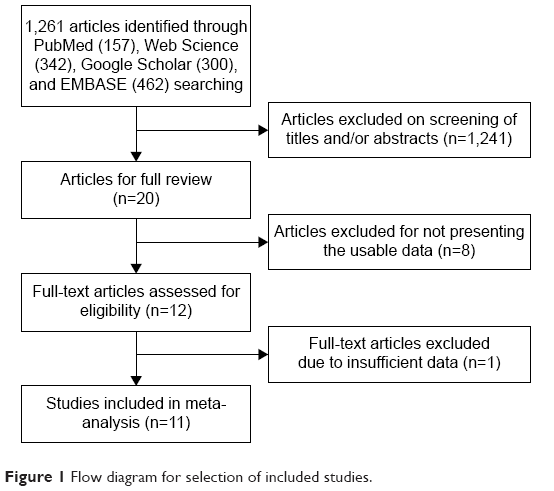 | Figure 1 Flow diagram for selection of included studies. |
The rate of CXCR4 protein expression in PC was significantly higher than in nonmalignant prostate tissues: OR was 35.71 with 95% CI =15.58–81.84, test for overall effect z=8.45, P<0.00001, and I2=14% (Figure 2). The expression of CXCR4 protein was not associated with Gleason score: OR was 1.19, 95% CI =0.43–3.27, test for overall effect z=0.34, P=0.73, and I2=60% (Figure 3). However, the frequency of CXCR4 protein expression was significantly higher in T3–4 stage than in T1–2 stage of PCa: OR was 2.35, 95% CI =1.40–3.96, test for overall effect z=3.21, P=0.001, and I2=29% (Figure 4). The CXCR4 protein expression was significantly associated with the presence of lymph node or bone metastasis of PCa; for lymph node metastasis positive versus negative, OR was 5.07, with 95% CI =2.11–12.17, test for overall effect z=3.63, P=0.0003, and I2=0% (Figure 5), and for bone metastasis positive versus negative, OR was 7.03, with 95% CI =1.98–24.93, test for overall effect z=3.02, P=0.003, I2=0% (Figure 6). Cancer-specific survival of patients with PCa was significantly associated with CXCR4 protein expression, and the pooled HR was 0.24 with 95% CI =0.10–0.61, test for overall effect z=3.03, P=0.002, I2=20% (Figure 7).
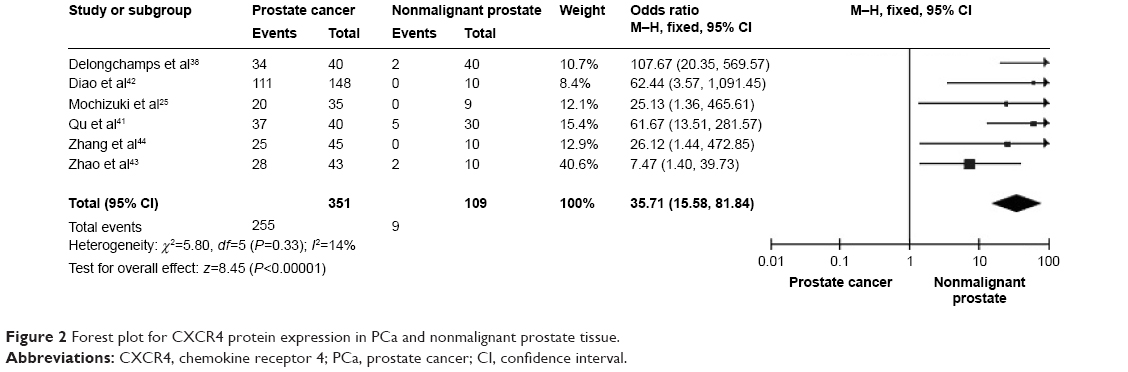 | Figure 2 Forest plot for CXCR4 protein expression in PCa and nonmalignant prostate tissue. |
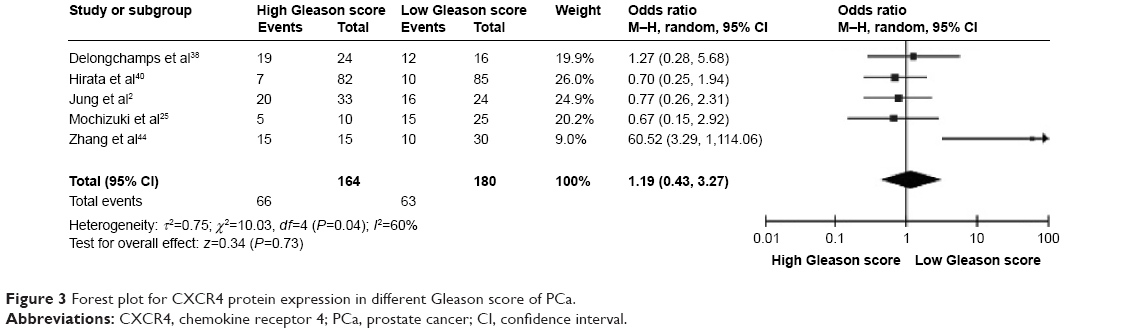 | Figure 3 Forest plot for CXCR4 protein expression in different Gleason score of PCa. |
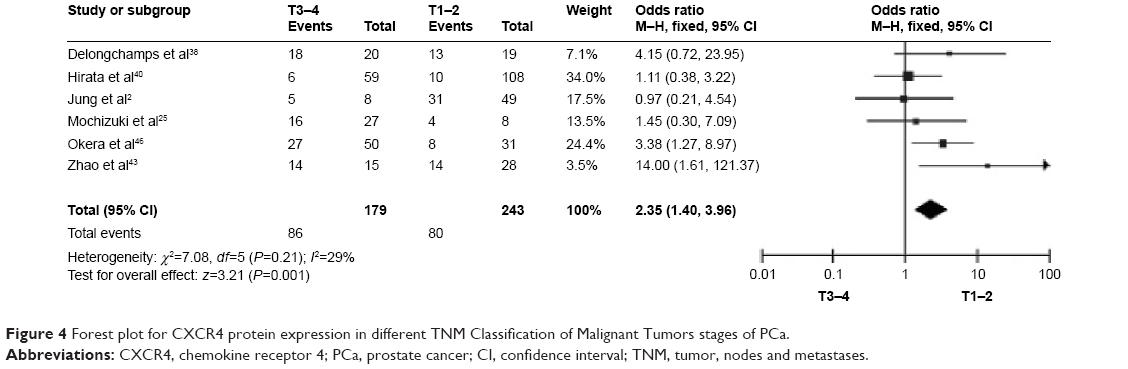 | Figure 4 Forest plot for CXCR4 protein expression in different TNM Classification of Malignant Tumors stages of PCa. |
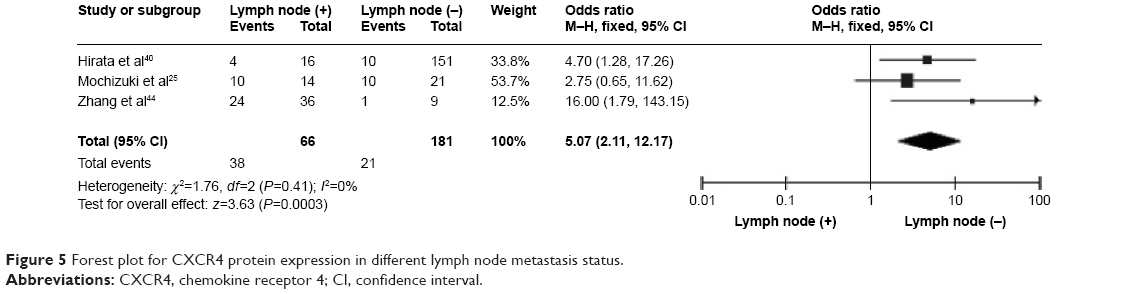 | Figure 5 Forest plot for CXCR4 protein expression in different lymph node metastasis status. |
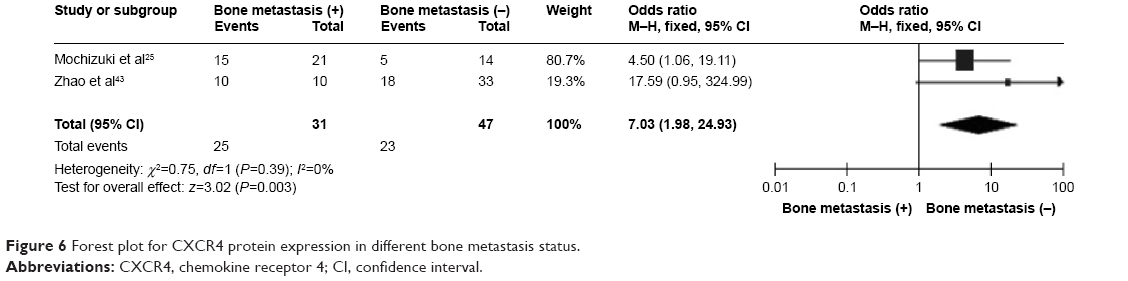 | Figure 6 Forest plot for CXCR4 protein expression in different bone metastasis status. |
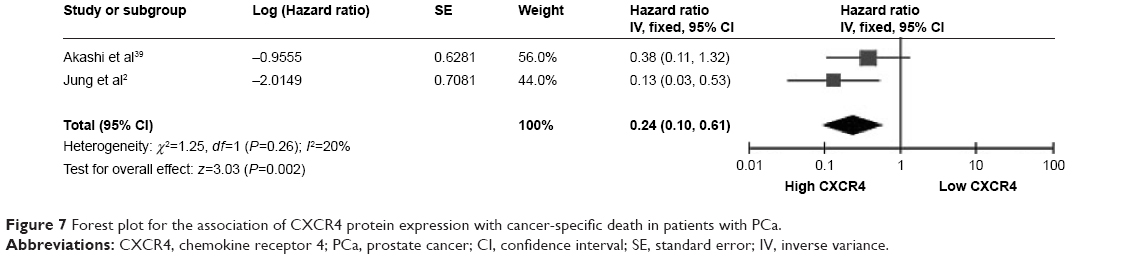 | Figure 7 Forest plot for the association of CXCR4 protein expression with cancer-specific death in patients with PCa. |
Methodological quality of included articles was assessed using the Newcastle Ottawa Quality Assessment Scale. This scale was used to allocate a maximum of nine points for the quality of selection, comparability, exposure, and outcomes for study participants. The NOS scores ranged from 0 to 9, and a score ≥7 indicates a good quality. Of the studies, seven scored eight points, two scored seven points, and two scored six points. Hence, the studies were of a relatively high quality (data not shown). A sensitivity analysis, in which one study was removed at a time, was conducted to assess the result stability. The pooled HR was not significantly changed, indicating the stability of our analyses. The funnel plots were largely symmetric (Figure 8), suggesting there were no publication biases in the meta-analysis of CXCR4 protein expression and clinicopathological features.
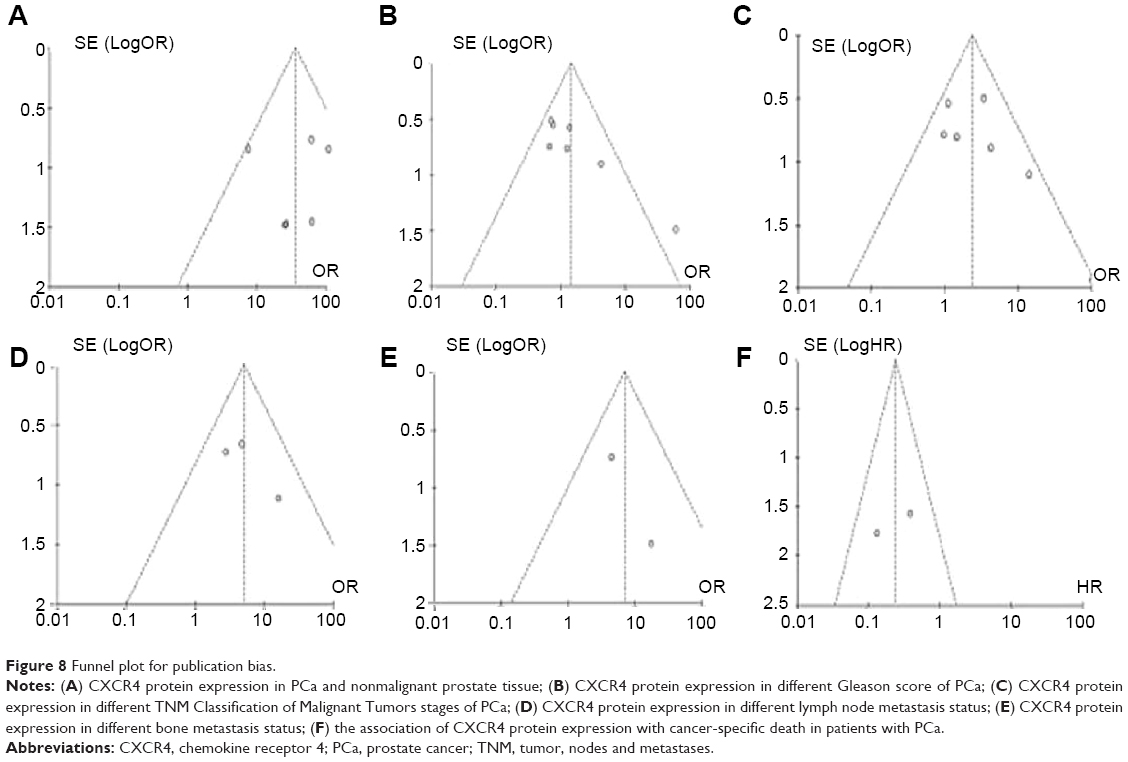 | Figure 8 Funnel plot for publication bias. |
Discussion
Serum prostate-specific antigen measurements have been used for effective screening, early detection of PCa, prediction of tumor invasion, prognosis, selection of treatment modality, and monitoring of treatment response. However, there were some limitations for the application of prostate-specific antigen in various clinical settings.20 Many PCa identified by prostate-specific antigen screening were indolent at presentation and could be appropriately managed with active surveillance. However, some of them were biologically aggressive and were appropriate targets for the immediate treatment. Molecular biomarker could be applied as a more accurate assay to discriminate indolent and aggressive tumors at diagnosis and optimize clinical strategy.17 CXCR4, a unique receptor that exclusively interacts with the endogenous ligand CXCL12,12 had been reported in at least 23 epithelial, mesenchymal, and hematopoietic tumors, suggesting its importance of this ligand/receptor axis in tumor initial, aggressiveness, and metastasis.13–15,21–23 In addition, numerous studies have experimentally demonstrated the role of SDF-1/CXCR4 axis in PCa. Several studies have shown higher expression of CXCR4 protein in PCa; however, the clinical relevance of CXCR expression in PCa remains inconsistent. We pooled six studies and compared the pooled rate of CXCR4 protein expression in PCa and nonmalignant prostate tissue including normal prostate tissue, benign prostate hyperplasia, and para PCa tissue. Our data showed the frequency of CXCR4 protein expression in PCa was 35 times higher than in nonmalignant prostate tissue, suggesting that CXCR4 expression could be a diagnostic biomarker for PCa. Our result also showed CXCR4 protein expression was associated with T stage; the rate of CXCR4 protein expression was significantly higher in T3–4 stages than in T1–2 stages. Several studies investigated the association between CXCR4 expression and T stages and reported controversial results due to small tested samples.2,19,24,25 Because CXCR4 expression was significantly higher in PCa than in nonmalignant prostate tissue, CXCR4-targeted imaging could be used for the diagnosis of PCa and monitoring cancer treatment. A few of peptide and small molecular CXCR4 antagonists including AMD3100, Ac-TZ14011, and CPCR4 have been developed and utilized as CXCR4-targeted SPECT or PET imaging probes.17 Recently, a technetium-99m labeled AMD3100 analog (CXCR4-specific antagonist) was reported and evaluated in mouse model bearing PC-3 xenograft. The tracer was significantly uptaken not only in tumor but also in lung, liver, spleen, bone, and kidney. However, SPECT images showed the specific accumulation of (99mTc) O2-AMD3100 in PCa xenograft, when the nonspecific uptake was significantly blocked with excess unlabeled AMD3100. Further studies are needed for the diagnosis in human with CXCR4-targeted antagonists.
In addition, we found that CXCR4 protein expression was significantly associated with the presence of lymph node or bone metastasis. The frequency of CXCR4 protein expression was significantly higher in PCa with lymph node or bone metastasis than in PCa without metastasis. Recent studies showed that CXCL12 mRNA was preferentially expressed in lymph nodes and bone marrow.23 CXCL12 was constitutively produced by osteoblasts, fibroblasts, and endothelia cells in bone marrow.24 PCa cells with overexpressed CXCR4 protein migrated to lymph nodes and bone marrow by an interaction between CXCR4 and CXCL12 in the pathway.25 Moreover, previous evidence showed increased CXCR4 expression in cancer-associated fibroblasts, which play an important role in tumor growth, angiogenesis, and metastasis.26–28 Taken together, our findings suggest that increased CXCR4 expression is a useful tool in predicting the presence of metastasis in PCa.
Androgen deprivation treatment is the most effective intervention for advanced PCa with metastasis. Although approximately 80% patients initially respond to this treatment, they eventually become unresponsive to androgen deprivation.29,30 Considering the critical role that CXCR4 and its ligand CXCL12 play in cancer development and metastasis of PCa, there is currently growing interest in the discovery and development of antagonists and imaging probes for therapeutic targeting and noninvasive monitoring of CXCR4 expression. Numerous agents, including peptide, small-molecule-based, and antibody-based treatment, and imaging probes have been developed to monitor CXCR4 expression and therapeutic resistance in past two decades. Lower molecular weight peptide analogs including T22, TW70, and T134 have been developed to reduce their cytotoxicity since 1992.31,32 Later Tamamura et al developed T140, a high-affinity 14 amino acid cyclic structural analog, which is essential for the development of various peptide analogs such as CVX15 and Ac-TZ14011. The efficacy of T140 and its analogs has been demonstrated in vitro and in vivo by reducing tumor growth and metastasis in chronic leukemia, multiple myeloma, breast cancer, melanoma, and pancreatic cancer mouse models.33 Darash-Yahana et al reported that CXCR4 inhibitory antibodies blocked CXCR4-dependent vascularization and tumor growth.22 Additionally, AMD3100, a CXCR4-specific antagonist, was utilized on human PCa PC-3 cells and xenograft model, which has lower expression of proliferation marker Ki67 and anti-apoptptic maker Bcl-2 compared with control tumors in vivo.34 Moreover, anti-CXCR4 antibodies and peptide analogs have been found to disrupt tumor-stromal interaction in breast cancer models and reduce the extent of metastasis as well as intraosseous growth in mouse xenograft models of PCa.35–37 Taken together, the inhibition of interaction of CXCR4 and CXCL12 could contribute to not only the therapeutic intervention but also the noninvasive monitoring of disease progression in patients with PCa. Further investigations are required for future clinical development of diagnosis and management of PCa.
We investigated the relationship between CXCR4 expression and cancer-specific death, indicating CXCR4 expression was strongly associated with prognosis in patients with PCa. The finding indicated CXCR4 expression is a poor prognosis predictor, which is consistent with previous studies. Finally, our study selected all the published articles written in English and Chinese and did not include some relevant articles written in other languages or unpublished papers that may result in certain publication bias. Therefore, the result should be interpreted carefully.
Conclusion
In conclusion, the high expression of CXCR4 is a diagnostic biomarker of PCa, and it is significantly associated with T stages. The increased expression of CXCR4 protein is significantly associated with the presence of lymph nodes or bone metastasis, and CXCR4 is a poor prognosis predictor for patients with PCa. Taken together, our findings indicate that CXCR4 could be a target not only for the development of therapeutic intervention of advanced PCa but also for the noninvasive monitoring of progression in patients with PCa.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. | ||
Jung SJ, Kim CI, Park CH, et al. Correlation between chemokine receptor CXCR4 expression and prognostic factors in patients with prostate cancer. Korean J Urol. 2011;52:607–611. | ||
Goto Y, Kurozumi A, Enokida H, Ichikawa T, Seki N. Functional significance of aberrantly expressed microRNAs in prostate cancer. Int J Urol. 2015;22(3):242–252. | ||
Berson JF, Long D, Doranz BJ, Rucker J, Jirik FR, Doms RW. A seven-transmembrane domain receptor involved in fusion and entry of T-cell-tropic human immunodeficiency virus type 1 strains. J Virol. 1996;70:6288–6295. | ||
Zlotnik A, Yoshie O. Chemokines: a new classification system and their role in immunity. Immunity. 2000;12:121–127. | ||
Butcher EC, Williams M, Youngman K, Rott L, Briskin M. Lymphocyte trafficking and regional immunity. Adv Immunol. 1999;72:209–253. | ||
Zhang XF, Wang JF, Matczak E, Proper JA, Groopman JE. Janus kinase 2 is involved in stromal cell-derived factor-1alpha-induced tyrosine phosphorylation of focal adhesion proteins and migration of hematopoietic progenitor cells. Blood. 2001;97:3342–3348. | ||
Ward SG. T lymphocytes on the move: chemokines, PI 3-kinase and beyond. Trends Immunol. 2006;27:80–87. | ||
Mellado M, Rodriguez-Frade JM, Manes S, Martinez AC. Chemokine signaling and functional responses: the role of receptor dimerization and TK pathway activation. Annu Rev Immunol. 2001;19:397–421. | ||
Mo W, Chen J, Patel A, et al. CXCR4/CXCL12 mediate autocrine cell- cycle progression in NF1-associated malignant peripheral nerve sheath tumors. Cell. 2013;152:1077–1090. | ||
Vlahakis SR, Villasis-Keever A, Gomez T, Vanegas M, Vlahakis N, Paya CV. G protein-coupled chemokine receptors induce both survival and apoptotic signaling pathways. J Immunol. 2002;169:5546–5554. | ||
Oberlin E, Amara A, Bachelerie F, et al. The CXC chemokine SDF-1 is the ligand for LESTR/fusin and prevents infection by T-cell-line-adapted HIV-1. Nature. 1996;382:833–835. | ||
Furusato B, Mohamed A, Uhlen M, Rhim JS. CXCR4 and cancer. Pathol Int. 2010;60:497–505. | ||
Zlotnik A. New insights on the role of CXCR4 in cancer metastasis. J Pathol. 2008;215:211–213. | ||
Vandercappellen J, Van Damme J, Struyf S. The role of CXC chemokines and their receptors in cancer. Cancer Lett. 2008;267:226–244. | ||
Don-Salu-Hewage AS, Chan SY, McAndrews KM, et al. Cysteine (C)-x-C receptor 4 undergoes transportin 1-dependent nuclear localization and remains functional at the nucleus of metastatic prostate cancer cells. PLoS One. 2013;8:e57194. | ||
Chatterjee S, Behnam Azad B, Nimmagadda S. The intricate role of CXCR4 in cancer. Adv Cancer Res. 2014;124:31–82. | ||
Gladson CL, Welch DR. New insights into the role of CXCR4 in prostate cancer metastasis. Cancer Biol Ther. 2008;7:1849–1851. | ||
Lee JY, Kang DH, Chung DY, et al. Meta-analysis of the relationship between CXCR4 expression and metastasis in prostate cancer. World J Mens Health. 2014;32:167–175. | ||
Canfield SE, Kibel AS, Kemeter MJ, Febbo PG, Lawrence HJ, Moul JW. A guide for clinicians in the evaluation of emerging molecular diagnostics for newly diagnosed prostate cancer. Rev Urol. 2014;16:172–180. | ||
Balkwill F. The significance of cancer cell expression of the chemokine receptor CXCR4. Semin Cancer Biol. 2004;14:171–179. | ||
Darash-Yahana M, Pikarsky E, Abramovitch R, et al. Role of high expression levels of CXCR4 in tumor growth, vascularization, and metastasis. FASEB J. 2004;18:1240–1242. | ||
Müller A, Homey B, Soto H, et al. Involvement of chemokine receptors in breast cancer metastasis. Nature. 2001;410:50–56. | ||
Ponomaryov T, Peled A, Petit I, et al. Induction of the chemokine stromal-derived factor-1 following DNA damage improves human stem cell function. J Clin Invest. 2000;106:1331–1339. | ||
Mochizuki H, Matsubara A, Teishima J, et al. Interaction of ligand-receptor system between stromal-cell-derived factor-1 and CXC chemokine receptor 4 in human prostate cancer: a possible predictor of metastasis. Biochem Biophys Res Commun. 2004;320:656–663. | ||
Eck SM, Cote AL, Winkelman WD, Brinckerhoff CE. CXCR4 and matrix metalloproteinase-1 are elevated in breast carcinoma-associated fibroblasts and in normal mammary fibroblasts exposed to factors secreted by breast cancer cells. Mol Cancer Res. 2009;7:1033–1044. | ||
Kojima Y, Acar A, Eaton EN, et al. Autocrine TGF-beta and stromal cell-derived factor-1 (SDF-1) signaling drives the evolution of tumor-promoting mammary stromal myofibroblasts. Proc Natl Acad Sci U S A. 2010;107:20009–20014. | ||
Orimo A, Gupta PB, Sgroi DC, et al. Stromal fibroblasts present in invasive human breast carcinomas promote tumor growth and angiogenesis through elevated SDF-1/CXCL12 secretion. Cell. 2005; 121:335–348. | ||
Leuprolide versus diethylstilbestrol for metastatic prostate cancer. The Leuprolide Study Group. N Engl J Med. 1984;311:1281–1286. | ||
Gittes RF. Carcinoma of the prostate. N Engl J Med. 1991;324:236–245. | ||
Nakashima H, Masuda M, Murakami T, et al. Anti-human immunodeficiency virus activity of a novel synthetic peptide, T22 ([Tyr-5,12, Lys-7]polyphemusin II): a possible inhibitor of virus-cell fusion. Antimicrob Agents Chemother. 1992;36:1249–1255. | ||
Tamamura H, Arakaki R, Funakoshi H, et al. Effective lowly cytotoxic analogs of an HIV-cell fusion inhibitor, T22 ([Tyr5,12, Lys7]-polyphemusin II). Bioorg Med Chem. 1998;6:231–238. | ||
Burger JA, Peled A. CXCR4 antagonists: targeting the microenvironment in leukemia and other cancers. Leukemia. 2009;23:43–52. | ||
Cho KS, Yoon SJ, Lee JY, et al. Inhibition of tumor growth and histopathological changes following treatment with a chemokine receptor CXCR4 antagonist in a prostate cancer xenograft model. Oncol Lett. 2013;6:933–938. | ||
Porvasnik S, Sakamoto N, Kusmartsev S, et al. Effects of CXCR4 antagonist CTCE-9908 on prostate tumor growth. Prostate. 2009;69:1460–1469. | ||
Sun YX, Schneider A, Jung Y, et al. Skeletal localization and neutralization of the SDF-1(CXCL12)/CXCR4 axis blocks prostate cancer metastasis and growth in osseous sites in vivo. J Bone Miner Res. 2005; 20:318–329. | ||
Muller G, Lipp M. Signal transduction by the chemokine receptor CXCR5: structural requirements for G protein activation analyzed by chimeric CXCR1/CXCR5 molecules. Biol Chem. 2001;382:1387–1397. | ||
Delongchamps NB, Beuvon F, Mathieu JR, et al. CXCR4 is highly expressed at the tumor front but not in the center of prostate cancers. World J Urol. 2015;33:281–287. | ||
Akashi T, Koizumi K, Tsuneyama K, Saiki I, Takano Y, Fuse H. Chemokine receptor CXCR4 expression and prognosis in patients with metastatic prostate cancer. Cancer Sci. 2008;99:539–542. | ||
Hirata H, Hinoda Y, Kikuno N, et al. CXCL12 G801A polymorphism is a risk factor for sporadic prostate cancer susceptibility. Clin Cancer Res. 2007;13:5056–5062. | ||
Qu F, Xing YF, Xiao YJ, Xiao CG, Guo HQ. CXCR4 combined with P504S or P63 in differential diagnosis of benign and malignant prostatic diseases. Zhonghua Nan Ke Xue. 2008;14:4. | ||
Diao X, Chen Z, Ye M, et al. CXCR4 and SDF-1 expression and its clinical significance in prostate cancer. J Prac Med. 2009;10:3. | ||
Zhao L, Guo L, Liu J, Gao W. Prostate cancer CXCR4, VEGF expression and significance. Changrong Kang trip carrying heavy ion regeneration (heavy particles) in the treatment of cancerous tumors. 2013;4:32–35. | ||
Zhang R, Wang D, Wang J, Guo M, Qiu L, Guo B. Expression of chemokine receptor CXCR4 in human prostatic carcinoma tissues. Acad J Sec Mil Med Univ. 2006;27:4. | ||
Xing Y, Liu M, Du Y, et al. Tumor cell-specific blockade of CXCR4/SDF-1 interactions in prostate cancer cells by hTERT promoter induced CXCR4 knockdown: a possible metastasis preventing and minimizing approach. Cancer Biol Ther. 2008;7:1839–1848. | ||
Okera M, Bae K, Bernstein E, et al. Evaluation of nuclear factor kappaB and chemokine receptor CXCR4 co-expression in patients with prostate cancer in the Radiation Therapy Oncology Group (RTOG) 8610. BJU Int. 2011;108:E51–E58. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.