Back to Journals » Patient Preference and Adherence » Volume 13
The association of angiotensin receptor blocker-based combination therapy with persistence and adherence in newly treated, uncomplicated hypertensive patients
Authors Ah YM ![]() , Shin J, Lee JY
, Shin J, Lee JY ![]()
Received 21 November 2018
Accepted for publication 10 January 2019
Published 31 January 2019 Volume 2019:13 Pages 241—248
DOI https://doi.org/10.2147/PPA.S195423
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Young-Mi Ah,1 Jaekyu Shin,2 Ju-Yeun Lee3
1College of Pharmacy, Yeungnam University, Gyeongsangbuk-do, Republic of Korea; 2Department of Clinical Pharmacy, School of Pharmacy, University of California San Francisco, San Francisco, CA, USA; 3College of Pharmacy and Research Institute of Pharmaceutical Sciences, Seoul National University, Seoul, Republic of Korea
Purpose: We compared treatment adherence and persistence during treatment with an angiotensin receptor blocker (ARB)-based single pill combination (SPC) and free equivalent combination (FEC) and between SPCs of an ARB with a thiazide diuretic (TD) and an ARB with a calcium channel blocker (CCB) as initial treatment in uncomplicated hypertensive patients who received pre-packaged medications from the pharmacy.
Patients and methods: Uncomplicated hypertensive patients who started combination treatment consisting of ARB and either TD or CCB were identified from a Korean national claims database. We used propensity score matching to construct two pairs of cohorts: SPC and FEC cohorts (20,175 patients per cohort) and SPC cohorts of ARB + TD and ARB + CCB (45,253 patients per cohort). We compared adherence measured via the medication possession ratio as well as overall 1-year and initial treatment persistence.
Results: Compared with the FEC cohort, the SPC cohort had significantly higher medication adherence (OR 1.31, 95% CI 1.25–1.37), overall persistence (HR 1.33, 95% CI 1.28–1.38), and initial treatment persistence (HR 1.61, 95% CI 1.56–1.64). Neither the rate of medication adherence nor the rate of treatment persistence differed significantly between the ARB + TD and ARB + CCB cohorts. However, the ARB + CCB cohort had a significantly higher rate of initial treatment persistence than did the ARB + TD cohort (HR 1.12, 95% CI 1.10–1.14).
Conclusion: Our data suggest that, compared with FEC therapy, initiating an ARB-based SPC therapy may increase adherence and persistence in patients with uncomplicated hypertension who also receive pre-packaged medication from the pharmacy. Although using an ARB + CCB SPC may improve initial treatment persistence, it does not increase adherence or overall persistence when compared with an ARB + TD SPC.
Keywords: single pill combination, persistence, adherence, hypertension, angiotensin receptor blocker
Introduction
According to the National Health and Nutrition Examination Survey (2011–2014), only 53.0% of patients with hypertension in the US meet their blood pressure (BP) goal.1 Since uncontrolled hypertension increases the risk of adverse cardiovascular events,2 barriers to controlling hypertension should be removed. One such barrier is medication adherence.3 Medication adherence is particularly important because controlling hypertension usually requires multiple antihypertensive agents. For example, in various high-risk populations, 2–4 antihypertensive agents were needed to properly control BP.4 In addition, just 40% of patients who achieved their target BP after 5 years of follow-up remained on monotherapy in The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial.5 In fact, a combination regimen with multiple antihypertensive agents may control BP better with a lower probability of adverse drug events and treatment discontinuation.6 Since guidelines for treating hypertension, such as those in 2018 European Society of Cardiology/European Society of Hypertension and the 2017 American College of Cardiology/American Heart Association, recommend combination regimens for most patients with hypertension, preferably in single pill combinations (SPCs), their use has steadily increased as the initial choice for treating hypertension.7,8
Combination regimens have one major disadvantage, that is, low medication adherence.9 Two strategies commonly used to increase adherence in patients taking combination regimen are the use of a medication organizer and SPCs. Tools to help patients organize medications, such as pillboxes, blister packs, or packaging with a calendar feature, have been shown to improve medication adherence.10–12 SPCs have also been demonstrated to improve medication adherence and clinical outcomes in patients with hypertension when compared to free equivalent combination (FEC).13–15 However, whether SPCs increase medication adherence when compared to FECs in patients with uncomplicated hypertension who also receive a medication organizer is unknown.
Combination regimens including an angiotensin receptor blocker (ARB) with either a thiazide diuretic (TD) or a dihydropyridine calcium channel blocker (CCB) are widely used. Given the difference in side effect profiles, these two combination regimens may have different adherence rates. One study showed that an SPC of ARB with hydrochlorothiazide significantly improved adherence compared with the diuretic monotherapy.16 However, SPCs of ARB with TD have not been compared with SPCs of ARB with CCB for medication adherence.
In Korea, standard pharmacy practice is to dispense medications in a pre-packaged format according to their administration time (eg, morning, lunch, evening, and bedtime). This practice applies to all outpatient pharmacies, including community pharmacies. Therefore, the present study has two main aims. We used nationwide insurance claims data to compare medication adherence and persistence between ARB-based SPC and FEC as initial treatment for patients with uncomplicated hypertension who also received pre-packaged medications from the pharmacy. We also evaluated medication adherence and persistence between SPCs of an ARB with TD and an ARB with CCB in the same population.
Patients and methods
In this retrospective study, we used a national claims database provided by the Health Insurance Review and Assessment Service (HIRA), which covers the entire Korean population.
Cohort selection
This study included adult patients (≥18 years old) who had an ICD-10 code of hypertension (I10, I11, I12, I13, or I15) and started combination regimen consisting of an ARB and either a TD or CCB in 2012. The first date of a prescription for the study medication in 2012 was considered to be the index date. Patients were excluded if they had an ICD-10 code for the following diagnoses: cardiovascular disease, cerebrovascular disease, peripheral vascular disease, renal disease, diabetes mellitus, or pregnancy. Patients were also excluded if they received a prescription of an antihypertensive medication during the year preceding the index date, received an antihypertensive medication for less than 7 days, or were hospitalized for >7 days after the index date. Depending on the type of initial treatment for hypertension, patients were grouped into SPC or FEC cohorts. In addition, the SPC cohort was divided into ARB + TD and ARB + CCB cohorts.
Study variables
The primary outcomes of the study were medication adherence and persistence for 1 year after the index date. Medication possession ratio (MPR) was used to measure medication adherence. MPR was calculated by summing days covered by antihypertensive prescriptions over 1 year from the index date divided by 365 days. We truncated MPR to 1.0 and categorized patients as fully adherent (MPR ≥0.8), intermediate (MPR 0.4–0.79), or low (MPR <0.4).17 Medication persistence was defined as receiving prescriptions for antihypertensive medications with a gap of no more than 60 days between medication supplies. The proportion of persistent patients was calculated overall, at 6 months, and at 1 year.
Potential confounders were age; sex; comorbid diseases such as dementia, depression, and dyslipidemia; Charlson Comorbidity Index (CCI) score; and insurance type. Data on confounders were obtained from the national claims database.
Statistical analyses
The descriptive statistics used were mean, SD, median, and range. Student’s t-test and chi-squared test were used to compare baseline characteristics between groups. To reduce the effects of confounding factors, the cohorts were selected by 1:1 matching using propensity scores calculated with age, sex, and CCI. Multivariable logistic regression analysis adjusted for potential confounders was used to compare medication adherence between cohorts. Multivariable Cox proportional hazard regression analysis adjusted for potential confounders was used to compare treatment persistence between cohorts. We used SAS 9.3 (SAS Institute Inc., Cary, NC, USA) and considered a P-value <0.05 to be statistically significant.
Ethics approval and informed consent
This study was approved by the Seoul National University Institutional Review Board (P01-201406-SB-03 – 02). Institutional Review Board waived informed consents because only de-identified information was used.
Results
We identified 126,679 uncomplicated hypertensive patients who started treatment with either ARB + TD or ARB + CCB. More than 80% of the patients used an SPC regimen (Figure 1). Of these patients, 56% used an ARB + TD. After propensity score matching, SPC and FEC cohorts had 20,175 patients each. We also selected 45,253 patients for each of the ARB + TD and ARB + CCB cohorts (Figure 1).
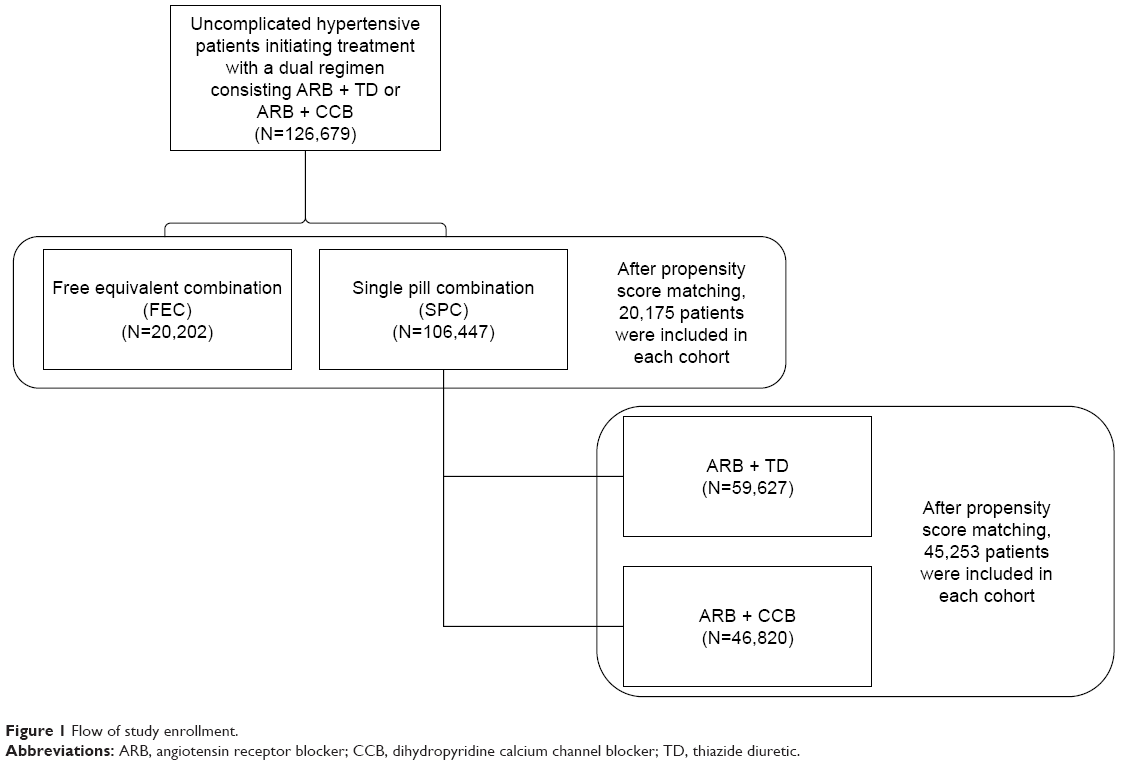 | Figure 1 Flow of study enrollment. |
SPC versus FEC
Table 1 shows the baseline characteristics of each cohort. The overall mean age was 56.1 years and 58.8% were male. The prevalence of comorbid disease states did not differ significantly between cohorts. However, a significantly lower percentage of the SPC cohort had medical aid insurance than did the FEC cohort (4.8% vs 5.5%; P=0.01). Also, the SPC cohort had a higher prevalence of ARB + TD use than did the FEC cohort (56.3% vs 15.2%; P<0.01).
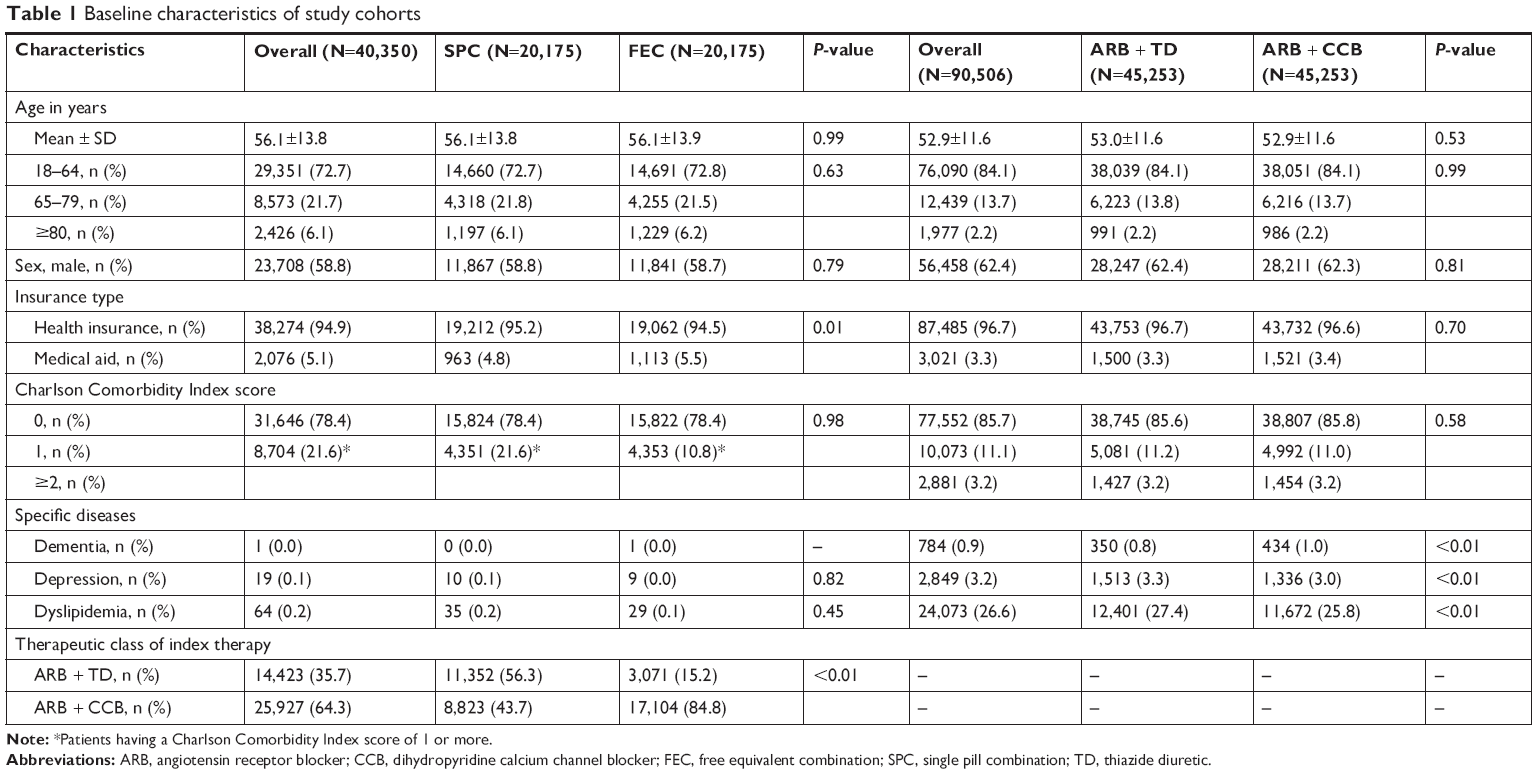 | Table 1 Baseline characteristics of study cohorts |
Table 2 compares medication adherence and persistence between cohorts. About two-thirds of the entire population were fully adherent. Compared with the FEC cohort, the SPC cohort had a significantly higher proportion of patients with full or intermediate adherence. In addition, the SPC cohort had significantly higher rates of medication adherence (0.8±0.3 vs 0.7±0.3; P<0.01), overall persistence (66.4% vs 59.2%; P<0.01), and initial treatment persistence (41.9% vs 34.4%; P<0.01). Furthermore, the SPC cohort had a longer duration of overall persistence (285.5±120.5 days vs 262.6±130.5 days, P<0.01) and initial treatment persistence (228.9±129.4 days vs 175.1±151.1 days, P<0.01) than did the FEC cohort.
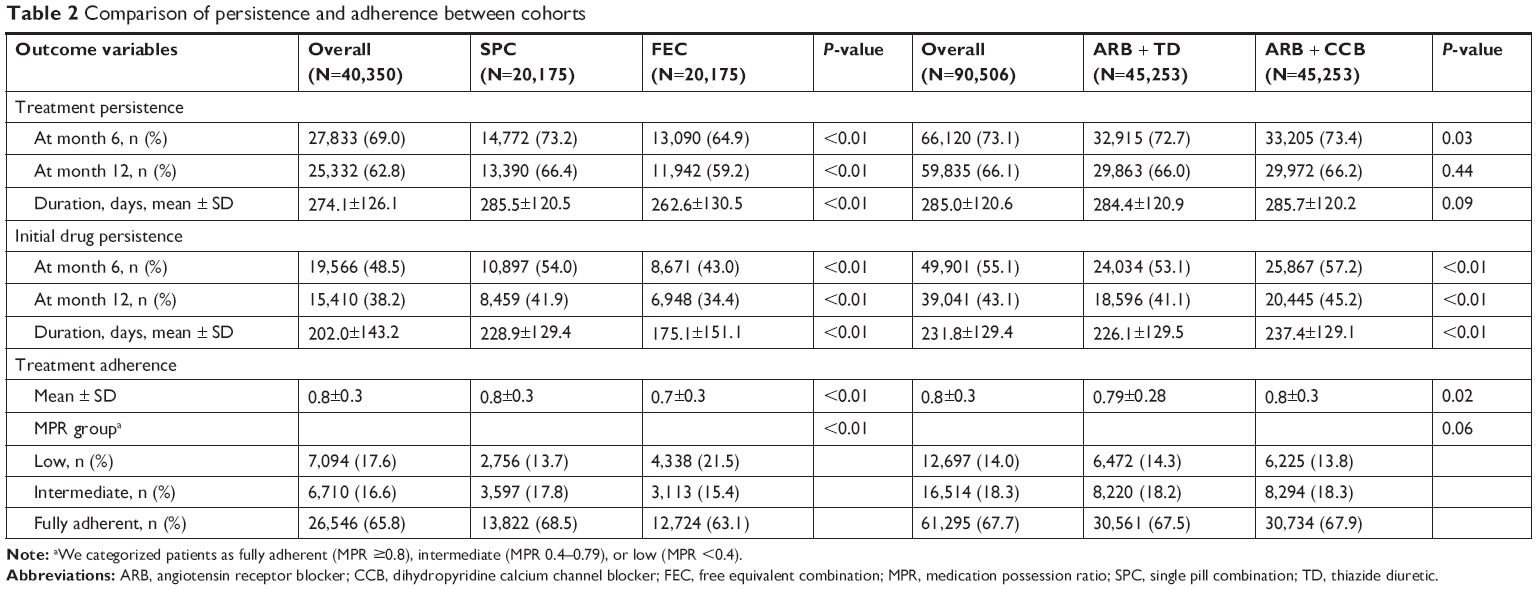 | Table 2 Comparison of persistence and adherence between cohorts |
Table 3 shows the likelihood of medication adherence and persistence between the SPC and FEC cohorts after adjusting for potential confounders. The use of SPCs was significantly associated with a 30% higher medication adherence (OR 1.31, 95% CI 1.25–1.37), a 33% higher overall treatment persistence (HR 1.33, 95% CI 1.28–1.38), and a 61% higher initial treatment persistence (HR 1.61, 95% CI 1.56–1.64) than was for the use of FECs.
 | Table 3 Comparison of 1-year treatment persistence, initial treatment persistence, and adherence |
ARB + TD versus ARB + CCB as SPC
Overall, the only baseline characteristics that differed significantly between the two cohorts were dementia, depression, and dyslipidemia (Table 1). Dementia was significantly more prevalent in the ARB + CCB cohort, whereas depression and dyslipidemia were more common in the ARB + TD cohort.
The proportion of fully adherent patients did not differ significantly between cohorts (Table 2). Approximately, two-thirds of patients in both cohorts were persistent with overall treatment. However, the ARB + CCB cohort had a significantly higher rate of persistence with initial treatment than did the ARB + TD cohort (45.2% vs 41.1%, P<0.001).
After adjusting for potential confounders, neither the medication adherence rate nor overall persistence rate differed significantly between ARB + TD cohort and ARB+CCB cohort (Table 3). However, the use of ARB + CCB SPC was significantly associated with a 12% higher rate of persistence with initial treatment than was ARB + TD SPC (HR 1.12, 95% CI 1.10–1.14) (Table 3).
Discussion
This study had the following main findings. The use of ARB-based SPCs was associated with significant increases in the medication adherence rate by 31%, overall treatment persistence by 33%, and initial treatment persistence by 61% in patients with uncomplicated hypertension when compared with ARB-based FEC. These increased rates of medication adherence and persistence were observed in patients who also received pre-packaged medications format from pharmacies. The rates of medication adherence and persistence with overall treatment did not differ between the ARB + TD and ARB + CCB SPC cohorts, although the rate of persistence with initial treatment was higher in the ARB + CCB SPC cohort.
Our data are consistent with results of previous studies reporting that the use of SPCs may improve medication adherence when compared with FECs. In a meta-analysis, the use of SPCs increased MPR by ~8% in treatment-naïve patients.13 Although one study reported no significant differences in the risk of treatment discontinuation between the use of SPC and FEC in newly treated hypertension patients,6 other studies have shown a lower discontinuation rate with the use of SPC. For example, in a study of patients initiating ARB + CCB to treat hypertension, the use of SPC decreased the rate of discontinuing initial treatment by 34%.18 In addition, valsartan-amlodipine SPC had a continuation rate up to 35% higher than that of FEC.19 Furthermore, patients initiating SPC therapy of ARB + TD had higher adherence and treatment persistence than did FEC users in a Taiwan population-based study.15 Recent studies have reported that patients treated with SPC had a higher adherence rate as well as better clinical outcomes such as a lower rate of death or hospitalizations due to adverse cardiovascular events than patients following FEC regimen.20,21 Based on these favorable findings, recent guidelines have encouraged the use of SPC for most patients with hypertension,7,8 even though SPC is associated with high cost and difficulty in dose titration of the individual components.22 Since generic SPC are becoming more affordable, however, the cost issue is gradually being resolved.
Our study population received medications in a pre-packaged format. In a meta-analysis on the effects of pre-packaging medications with a calendar feature on medication adherence, six of the ten included trials reported improved medication adherence with pre-packaging.12 Thus, our data suggest that using an ARB-based SPC may increase medication adherence and persistence even further in patients with uncomplicated hypertension who also receive pre-packaged medications.
In a previous study using a HIRA sample in 2009, the use of SPCs was associated with a higher medication adherence in patients with hypertension when compared with the use of FECs. Our study differed from that study in that ours included only incident users, whereas the previous study also included prevalent users. In addition, the previous study included patients with complications from hypertension and measured outcomes with only 1-year sample data.23
In our study, >80% of subjects received an ARB-based SPC as initial therapy and both ARB + CCB and ARB + TD combinations were used almost equally in the SPC cohort. This result is related to the introduction of various SPCs in the Korean pharmaceutical market. As of December 2013, 627 two-drug SPCs were approved to treat hypertension, many of which were generic. The majority of currently available SPCs in Korea are ARB based (91.5%).
Our data also suggest that using an ARB + CCB SPC may improve the rate of persistence with initial treatment compared with using an ARB + TD SPC, although they did not differ in medication adherence or overall persistence. Significantly fewer subjects discontinued initial treatment in the ARB + CCB cohort (HR 0.89, 95% CI 0.88–0.91), which might be due to differences in the incidence of adverse drug events and medication tolerance between CCB and TD groups. In a study that investigated reasons for treatment modification in patients with hypertension, the most common reason was side effects.24 Another study comparing between TD and CCBs found that TD had a higher incidence of adverse events.25 In addition, using a CCB with an ARB reduced the rate of dose-dependent adverse drug events related to CCB.26
In our study, patients receiving ARB + TD using a SPC were more numerous than those using FEC and the opposite was true for ARB + CCB. These findings are observed not only in our study cohort but also in the total population from the national claims database provided by HIRA before propensity score matching. Although selection bias may not be completely excluded, these findings may be explained, in part, by the fact that SPC of ARB + TD was introduced earlier and more widely available on the Korean market than that of ARB + CCBs at the time this study was conducted.
We acknowledge the following limitations of our study. We were not able to investigate clinical outcomes due to the relatively short-term follow-up and the unavailability of clinical data, such as BP, in the claims data. As we used only prescription claims to estimate persistence and adherence, we were not able to assess whether patients had actually taken medications. However, this method has been widely adopted to assess medication adherence and persistence.27–29 We compared medication adherence and persistence between ARB-based SPC and FEC in patients who also received pre-packaged medications (medication organizer) from the pharmacy. As dispensing medications in a pre-packaged format is a standard practice in Korea, we could not evaluate the effect of a SPC in patients without a medication organizer. So, the study results in favor of SPC might be more pronounced in patients who were not provided with a medication organizer.
We were also unable to determine the reasons for the discontinuation of treatment, such as lack of efficacy or development of an adverse drug event, because of the unavailability of this type of data in the claims data.
Conclusion
Our data suggest that using an SPC may improve medication adherence and persistence in patients with uncomplicated hypertension who also receive a medication organizer, such as pre-packaged medications. Clinicians may consider using a SPC to improve medication adherence even if patients are using a medication organizer. In addition, our data may indicate that either ARB + CCB SPC or ARB + TD SPC can be considered as an initial treatment for uncomplicated hypertension, as the two combinations did not differ in the adherence or overall persistence rate.
Data availability
The data could not be shared because the access to raw data of the Korean HIRA service is regulated by the Rules for Data Exploration and Utilization of the HIRA.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Yoon SS, Carroll MD, Fryar CD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS Data Brief. 2015(220):1–8. | ||
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. | ||
Elliott WJ. What factors contribute to the inadequate control of elevated blood pressure? J Clin Hypertens. 2008;10(s1):20–26. | ||
Haller H. Effective management of hypertension with dihydropyridine calcium channel blocker-based combination therapy in patients at high cardiovascular risk. Int J Clin Pract. 2008;62(5):781–790. | ||
Cushman WC, Ford CE, Cutler JA, et al; ALLHAT Collaborative Research Group. Success and predictors of blood pressure control in diverse North American settings: the antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). J Clin Hypertens. 2002;4(6):393–404. | ||
Corrao G, Parodi A, Zambon A, et al. Reduced discontinuation of antihypertensive treatment by two-drug combination as first step. Evidence from daily life practice. J Hypertens. 2010;28(7):1584–1590. | ||
Williams B, Mancia G, Spiering W, et al; ESC Scientific Document Group. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. | ||
Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. Hypertension. 2018;71(6):e13–e115. | ||
Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. | ||
Nochowitz B, Shapiro NL, Nutescu EA, Cavallari LH. Effect of a warfarin adherence aid on anticoagulation control in an inner-city anticoagulation clinic population. Ann Pharmacother. 2009;43(7):1165–1172. | ||
Huang HY, Maguire MG, Miller ER 3rd, Appel LJ. Impact of pill organizers and blister packs on adherence to pill taking in two vitamin supplementation trials. Am J Epidemiol. 2000;152(8):780–787. | ||
Zedler BK, Kakad P, Colilla S, Murrelle L, Shah NR. Does packaging with a calendar feature improve adherence to self-administered medication for long-term use? A systematic review. Clin Ther. 2011;33(1):62–73. | ||
Sherrill B, Halpern M, Khan S, Zhang J, Panjabi S. Single-pill vs free-equivalent combination therapies for hypertension: a meta-analysis of health care costs and adherence. J Clin Hypertens (Greenwich). 2011;13(12):898–909. | ||
Machnicki G, Ong SH, Chen W, Wei ZJ, Kahler KH. Comparison of amlodipine/valsartan/hydrochlorothiazide single pill combination and free combination: adherence, persistence, healthcare utilization and costs. Curr Med Res Opin. 2015;31(12):2287–2296. | ||
Hsu CI, Hsiao FY, Wu FL, Shen LJ. Adherence and medication utilisation patterns of fixed-dose and free combination of angiotensin receptor blocker/thiazide diuretics among newly diagnosed hypertensive patients: a population-based cohort study. Int J Clin Pract. 2015;69(7):729–737. | ||
Patel BV, Remigio-Baker RA, Thiebaud P, Preblick R, Plauschinat C. Improved persistence and adherence to diuretic Fixed-dose combination therapy compared to diuretic monotherapy. BMC Fam Pract. 2008;9(1):61. | ||
Rasmussen JN, Chong A, Alter DA. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarction. JAMA. 2007;297(2):177–186. | ||
Zeng F, Patel BV, Andrews L, Frech-Tamas F, Rudolph AE. Adherence and persistence of single-pill ARB/CCB combination therapy compared to multiple-pill ARB/CCB regimens. Curr Med Res Opin. 2010;26(12):2877–2887. | ||
Brixner DI, Jackson KC 2nd, Sheng X, Nelson RE, Keskinaslan A. Assessment of adherence, persistence, and costs among valsartan and hydrochlorothiazide retrospective cohorts in free-and fixed-dose combinations. Curr Med Res Opin. 2008;24(9):2597–2607. | ||
Ho CT, Tung YC, Chou SH, et al. Clinical outcomes in hypertensive patients treated with a single-pill Fixed-dose combination of renin-angiotensin system inhibitor and thiazide diuretic. J Clin Hypertens (Greenwich). 2018;20(12):1731–1738. | ||
Verma AA, Khuu W, Tadrous M, Gomes T, Mamdani MM. Fixed-dose combination antihypertensive medications, adherence, and clinical outcomes: a population-based retrospective cohort study. PLoS Med. 2018;15(6):e1002584. | ||
Dipette DJ, Skeete J, Ridley E, et al. Fixed-dose combination pharmacologic therapy to improve Hypertension control worldwide: clinical perspective and policy implications. J Clin Hypertens. 2019;21(1):4–15. | ||
Min JY, Min KB, Hong JM, Kim EG, Yang BM. Compliance and persistence of free-combination antihypertensive therapy versus single-pill combination in Korean hypertensive patients. Int J Cardiol. 2013;168(4):4576–4577. | ||
Lip GY, Beevers DG. Doctors, nurses, pharmacists and patients – the rational evaluation and choice in hypertension (REACH) survey of hypertension care delivery. Blood Press Suppl. 1997;1:6–10. | ||
Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose combination treatment with blood pressure lowering drugs: analysis of 354 randomised trials. BMJ. 2003;326(7404):1427. | ||
Parati G. Optimization of hypertension management: the role of angiotensin receptor blocker-calcium channel blocker combinations. J Cardiovasc Pharmacol. 2009;53(5):352–358. | ||
Mancia G, Zambon A, Merlino L, Corrao G, Corrao G. Factors involved in the discontinuation of antihypertensive drug therapy: an analysis from real life data. J Hypertens. 2014;32(8):1708–1715. | ||
Grimmsmann T, Himmel W. Persistence of antihypertensive drug use in German primary care: a follow-up study based on pharmacy claims data. Eur J Clin Pharmacol. 2014;70(3):295–301. | ||
Selmer R, Blix HS, Landmark K, Reikvam A. Choice of initial antihypertensive drugs and persistence of drug use: a 4-year follow-up of 78,453 incident users. Eur J Clin Pharmacol. 2012;68(10):1435–1442. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.