Back to Journals » Journal of Inflammation Research » Volume 13
The Association Between Inflammation, Epithelial Mesenchymal Transition and Stemness in Colorectal Carcinoma
Authors Briede I ![]() , Strumfa I, Vanags A, Gardovskis J
, Strumfa I, Vanags A, Gardovskis J
Received 24 July 2019
Accepted for publication 11 November 2019
Published 8 January 2020 Volume 2020:13 Pages 15—34
DOI https://doi.org/10.2147/JIR.S224441
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Inese Briede,1 Ilze Strumfa,1 Andrejs Vanags,2 Janis Gardovskis2
1Department of Pathology, Riga Stradins University, Riga, Latvia; 2Department of Surgery, Riga Stradins University, Riga, Latvia
Correspondence: Inese Briede
Department of Pathology, Riga Stradins University, 9A Kuldigas Street, Riga LV-1007, Latvia
Tel +371 67815096
Fax +371 67471815
Email [email protected]
Background: Inflammation plays an important albeit dual role in carcinogenesis. Survival studies have highlighted the prognostic significance of peritumorous inflammation. Currently, the theoretical background allows inflammation, epithelial mesenchymal transition (EMT) and the closely associated stem cell differentiation in colorectal carcinoma (CRC) to be linked. However, there is scarce direct morphological evidence.
Purpose and methods: The aim of our study was to investigate the role of inflammation in cancer growth and invasion by analyzing the association between inflammation and known morphological prognostic features of colorectal cancer, EMT, stemness and mismatch repair (MMR) protein expression. The study was designed as a retrospective morphological and immunohistochemical assessment of 553 consecutive cases of surgically treated primary CRC.
Results: There were statistically significant associations between high-grade inflammation and lower pT (p = 0.002), absence of lymph node metastases (p < 0.001) and less frequent lymphatic (p = 0.003), venous (p = 0.017), arterial (p = 0.012), perineural (p = 0.001) and intraneural (p = 0.01) invasion. In contrast, Crohn’s like reaction (CLR) by density of lymphoid follicles in the invasive front lacked significant differences in regard to pT, pN, tumor invasion into surrounding structures (blood or lymphatic vessels, nerves), grade or necrosis (all p > 0.05). The expression of E-cadherin, CD44 and MMR proteins yielded no statistically significant associations with peritumorous inflammation by Klintrup-Mäkinen score or the density of lymphoid follicles. Nevertheless, E-cadherin levels were significantly associated with the density of eosinophils (p = 0.007).
Conclusion: High-grade peritumorous inflammation is associated with beneficial morphologic CRC features, including less frequent manifestations of invasion, and is not secondary to tissue damage and necrosis. CLR is not associated with cancer spread by pTN; this finding indirectly suggests an independent role of CLR in carcinogenesis. Further, inflammation by Klintrup-Mäkinen grade and CLR is not dependent on epithelial-mesenchymal transition and stem cell differentiation. Our study highlights the complex associations between inflammation, tumor morphology, EMT, stemness and MMR protein expression in human CRC tissues.
Keywords: colorectal carcinoma, inflammation, Klintrup-Mäkinen score, immunohistochemistry, CD44, mismatch repair proteins
Introduction
Every year, colorectal cancer is responsible for many deaths worldwide. Thus, it still ranks globally among the three deadliest cancers.1 Nowadays, there are extensive possibilities for prevention, screening or timely diagnostics of colorectal carcinoma. Fecal guaiac occult blood testing or immunochemical tests, stool DNA tests, computed tomography colonography, double-contrast barium enemas, sigmoidoscopy and colonoscopy have been implemented for screening.2,3 All positive screening results obtained by any noncolonoscopy method should be followed by timely colonoscopy.4 The guidelines for screening are available, as recently systematically reviewed by Benard et al5. Screening has been shown to reduce mortality.6 For instance, screening by fecal occult blood test reduces the relative risk of colorectal cancer mortality by 25%. Colonoscopy is associated with a 67% reduction in the incidence of colorectal cancer within the next eight years, due to its greater potential to disclose and remove adenomas.2 Based on case control and prospective cohort studies, it is also suggested that it reduces mortality by 65–88%.4 In the USA, the incidence of colorectal carcinoma in people aged 50 or older declined by 32% between 2000 and 2013 and CRC- related mortality by 34% between 2000 and 2014. These changes have been attributed to the screening and removal of adenomas.4
A wide array of treatment approaches is available, including local treatment (endoscopic or transanal excision followed by a wider resection and lymph node dissection if certain unfavorable histologic features are identified), surgery with lymph node dissection via a laparoscopic or conventional approach, irradiation, and adjuvant or systemic chemotherapy (to prevent postoperative recurrence or to treat an unresectable progressive tumor, respectively) including molecular targeted drugs. To establish a standard medical treatment of consistent quality, guidelines are issued and revised by the National Comprehensive Cancer Network (NCCN) in the USA, the European Society for Medical Oncology (ESMO) and the Japanese Society for Cancer of the Colon and Rectum.7
Extensive local spread and/or large size of the tumor, the presence of metastases in lymph nodes, mucinous differentiation, invasion into lymphatic vessels, perineural growth and peritoneal involvement all indicate an unfavorable prognosis of colorectal carcinoma.8–10 Recently, the prognostic importance of the extent of cancer necrosis has been discussed.11 These factors could show bidirectional associations with chronic inflammation, which is an important component of tumor pathogenesis, beginning from the initiation and accompanying the progression and spread.
Inflammation is increasingly recognized as an important component of carcinogenesis. In colorectal cancer, it is known to influence the risk of developing cancer. Certain inflammatory diseases, such as Crohn’s disease and ulcerative colitis, increase the risk of colorectal carcinoma. In contrast, nonsteroidal anti-inflammatory drugs, such as aspirin and selective inhibitors of cyclooxygenase-2, in epidemiological, observational and clinical studies have been shown to be effective tools for decreasing the risk of colorectal cancer, the recurrence of adenomas and the development of new tumors. Regression of existing adenomas has been reported as well.12 Hence, inflammation is known to be among the risk factors for malignant change not only in the large bowel but also in the stomach and uterine cervix.13 In an already established tumor, inflammatory reaction can either promote or suppress tumor progression. Inflammatory cells are able to produce growth factors stimulating the proliferation of neoplastic cells, to enhance angiogenesis or to degrade the connective tissue matrix that in turn facilitates invasion. Consequently, inflammation might create a microenvironment that is beneficial for tumor development. On the other hand, inflammation can induce cancer cell death.14,15 One of the main factors involved in tumor progression is the pro-inflammatory cytokine TNFα, produced by macrophages. TNFα also has a crucial role in epithelial mesenchymal transition (EMT) as it induces overexpression of the transcription factor Snail, leading to downregulation of E-cadherin and upregulation of N-cadherin,16,17 which are among the key molecules involved in EMT. In colorectal cancer, stem cell differentiation by expression of CD4418 is strongly associated with EMT19 and represents an attractive treatment target.20 However, the relation between CD44 levels and inflammation has not been extensively studied.
The response to treatment can depend on the degree of tumor heterogeneity. This is the case not only in colorectal cancer21 but also in other carcinomas22 in relation to cancer stem cells.23 With regard to colorectal cancer, the heterogeneity is more frequent in tumors exhibiting microsatellite instability (MSI) than in microsatellite-stable (MSS) carcinomas.24 Changes within the mismatch repair (MMR) protein expression via immunohistochemistry (IHC) could be the hallmark for further DNA sequencing and personalized treatment choice.
As regards colorectal carcinoma, patients featuring intense, high-grade peritumorous inflammation have better survival rates than those who have low-grade inflammation.25,26 Some studies have revealed links between decreased CD44 expression and resistance to chemotherapy27 or recurrence of colorectal cancer.28 A combined low expression of E-cadherin and CD44 is associated with decreased overall survival in patients with metastatic colorectal cancer.29 Given these prognostic trends, associations between the listed factors might be hypothesized. However, few studies have tried to assess directly the mutual relationships between inflammation, EMT, stem cell differentiation and the expression of MMR proteins in the same cohort of colorectal cancer cases.
The aim of our study was to investigate the association between peritumorous inflammation and known adverse morphological features of colorectal carcinoma, including local spread (pT), the involvement of regional lymph nodes (pN) and manifestations of invasive growth as well as the molecular landscape of EMT, cancer stem cell differentiation and the expression of MMR proteins.
Materials and Methods
Ethics Statement
The study was designed as a retrospective morphological and immunohistochemical investigation of a representative group of consecutive, surgically treated colorectal carcinoma cases. It was carried out in accordance with the Declaration of Helsinki and was approved by the Committee of Ethics of Riga Stradins University, Riga, Latvia. Considering the retrospective study design, patient consent to review their medical records and tissue sections was not required by the said institutional research board. All the patient data were treated confidentially and anonymously.
Study Group
Diagnostic histopathology reports and slides of colorectal cancer were retrieved by archive search for consecutive patients who underwent radical surgical treatment of primary invasive colorectal carcinoma in a single university hospital within a four-year period. Cases were excluded from the study on the basis of the following characteristics of the patient or tumor: 1) previous history of colorectal cancer; 2) nonsurgical treatment; 3) palliative operation; 4) tissue material limited to a biopsy; 5) tumor fragmentation during surgery precluding reliable pathological staging; 6) pTis carcinoma; 7) secondary tumor involving the large bowel; and 8) tumor of nonepithelial histogenesis. Demographic data (age and gender) were retrieved from the medical documentation.
Tissue Samples
During the initial diagnostic evaluation, the surgical pathology materials were subjected to uniform protocol-based assessment including standardized grossing and sampling. The protocol was based on the recommendations issued by the College of American Pathologists.30
The tumor location by the side of the large bowel (right vs left) was retrieved from the medical documentation. The tissues were routinely fixed in 10% neutral buffered formalin (Sigma-Aldrich, Saint Louis, USA), processed via vacuum infiltration, embedded in paraffin, cut to a thickness of 4 micrometers and stained with hematoxylin and eosin (HE). Within the frames of the current study, the retrieved diagnostic pathology slides were re-evaluated by two observers in order to reach consensus on all the investigated parameters in each case. The cancer morphology, including grading, and pTN parameters were assessed according to the World Health Organization and the Union for International Cancer Control (UICC) TNM classification.31,32 To evaluate the invasive capacity of the tumour, the presence of perineural and intraneural cancer growth and invasion into lymphatic vessels, veins and arteries were assessed as categorical binary variables.33 Cancer necrosis was analyzed as a binary variable (present versus absent) and by the extent,34 classifying the necrosis as focal (< 10% of the whole tumour), moderate (10–30%) or extensive (> 30%) in line with Richards et al, 2012.
Assessment of Inflammation
Peritumorous inflammation was assessed according to the Klintrup-Mäkinen inflammation score by identifying four groups, ie absent versus mild versus moderate versus severe inflammation, which were further redistributed into two classes, namely low-grade (absent or mild inflammation) versus high-grade (moderate or severe) inflammation.26 Inflammatory cell subpopulations were evaluated by an analogous four-tiered scale.35 The degree of Crohn’s like lymphoid reaction (CLR) was assessed as CLR density according to Väyrynen criteria, by counting CLR follicles in the invasive front of a tumor.36 Further, the CLR results were redistributed into two groups, namely low versus high CLR density, using a previously verified threshold value,36 i.e. < 0.38 versus ≥ 0.38 per mm.
Immunohistochemistry
To evaluate epithelial-mesenchymal transition, stem cell differentiation and the expression of MMR proteins, immunohistochemical visualization of E-cadherin, CD44 and the MMR proteins MSH2, MSH6, MLH1 and PMS2 was performed on whole sections from representative blocks of the tumour. For IHC, 3-micrometer thick sections were cut on electrostatic glass slides (Histobond, Marienfeld, Germany). After deparaffinization and rehydration, antigen retrieval was performed in a microwave oven (3 × 5 min) using a basic TEG (pH 9.0) buffer, followed by blocking of endogenous peroxidase (Sigma-Aldrich). The sections were incubated with primary antibodies (see Table 1 for antibody characteristics and dilution) at room temperature. Bound antibodies were detected by the enzyme-conjugated polymeric visualization system EnVision, linked with horseradish peroxidase using 3,3ʹ-diaminobenzidine as the chromogen. All IHC reagents were produced by DAKO, Glostrup, Denmark. Positive and negative quality controls were invariably performed and reacted appropriately.
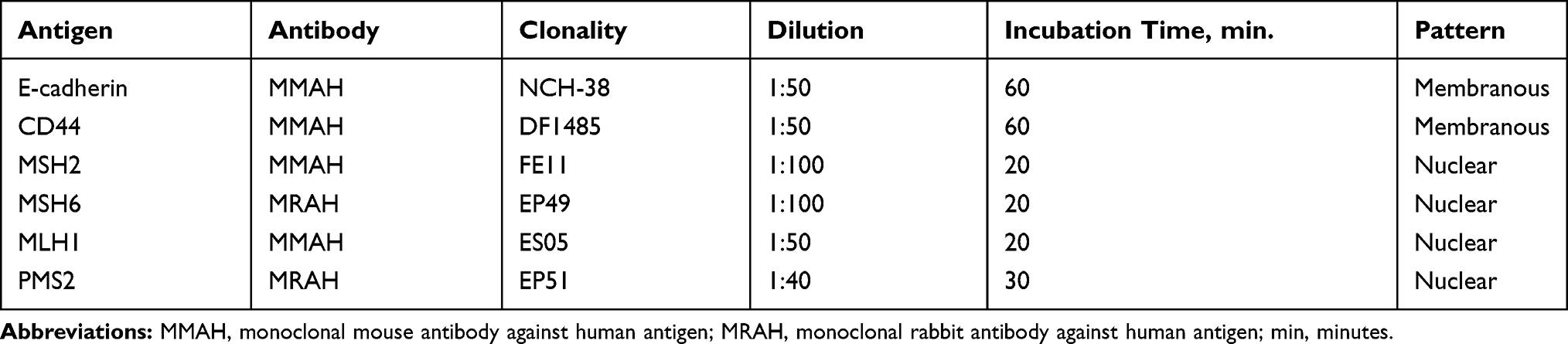 |
Table 1 Characteristics of the Primary Antibodies for Immunohistochemistry |
Quantification of Immunohistochemistry
Given the previously described cancer heterogeneity, which encompasses the immunohistochemical reactivity,21 the expression of each IHC marker was assessed both for intensity and extent. The expression intensity was evaluated on a scale ranging from 0 to 3 as follows: 0 = no expression, 1 = weak, 2 = moderate and 3 = strong expression. The relative extent (%) was measured as the fraction of cancer cells expressing the given marker with the given intensity. The final IHC score was calculated as the sum of the mathematical products of the intensity and the relative extent.
The expression of MMR proteins was evaluated both as binary variables (complete loss versus presence) and by semiquantitative scoring as described above. The MMR protein expression was reclassified then as low versus high using the median value as the cutoff threshold: 1.39 for MSH2; 1.9 for MSH6; 1.8 for PMS2; and 1.43 for MLH1.
Statistics
The statistical analysis was performed using the IBM SPSS Statistics version 22.0 statistical software package (International Business Machines Corp., Armonk, New York, USA). The assumption check of normality was performed by using the Shapiro-Wilk test. For descriptive statistics, mean ± standard deviation (SD), median ± interquartile range (IQR) and frequency were calculated as appropriate. In short, mean values were presented for normally distributed continuous variables while medians were presented for other continuous variables. Categorical data were characterized by frequency. For mean values and frequencies, 95% confidence intervals (CIs) were detected. Nonparametric methods, including the Mann–Whitney test, Spearman’s rank correlation and Pearson’s Chi-square, were used for analytical statistics. Kruskal-Wallis’s one-way analysis of variance by ranks, followed by post hoc analysis with Bonferroni correction, was applied to determine differences between three or more groups. A two-tailed p < 0.05 was considered statistically significant.
Results
The General Characteristics of the Study Group
According to the inclusion and exclusion criteria, 553 consecutive cases of surgically treated primary colorectal carcinoma were enrolled in the study (Table 2). Most of the patients were elderly: 93.0% [95% CI: 90.5–94.8] of them were older than 50. The median age was 71 (IQR, 15). The tumours were predominantly located in the left part of the large bowel, as was seen in 395 cases or 71.4% [67.5–75.0]. In regard to the morphology, adenocarcinoma was found in 88.8% [85.9–91.2], mucinous adenocarcinoma in 9.6% [7.4–12.3] and primary colorectal signet ring cell carcinoma in 1.2% [0.6–2.6] of cases. There were single cases (0.2% [0.0–1.0]) of medullary and undifferentiated carcinoma as well. When evaluating the T parameter, locally advanced tumors predominated: pT3 carcinoma represented 49.6% [45.4–53.7] and pT4 35.6% [31.7–39.7], in contrast to pT2, which was seen only in 11.9% [9.5–14.9] of all cases. In terms of grade, moderately differentiated (G2) cancers constituted 64.0% [59.9–67.9] of the study group, and high-grade (G3) carcinoma was found in 25.7% [22.2–29.5] of the cases. As for lymph node involvement, metastases in lymph nodes (pN+) were found in 40.5% [36.5–44.6] of the patients. In 56 cases (10.1% [7.9–12.9]), only tumour deposits (pN1c) were found within pericolonic or perirectal adipose tissue. The median number of retrieved lymph nodes was 11 (IQR, 8).
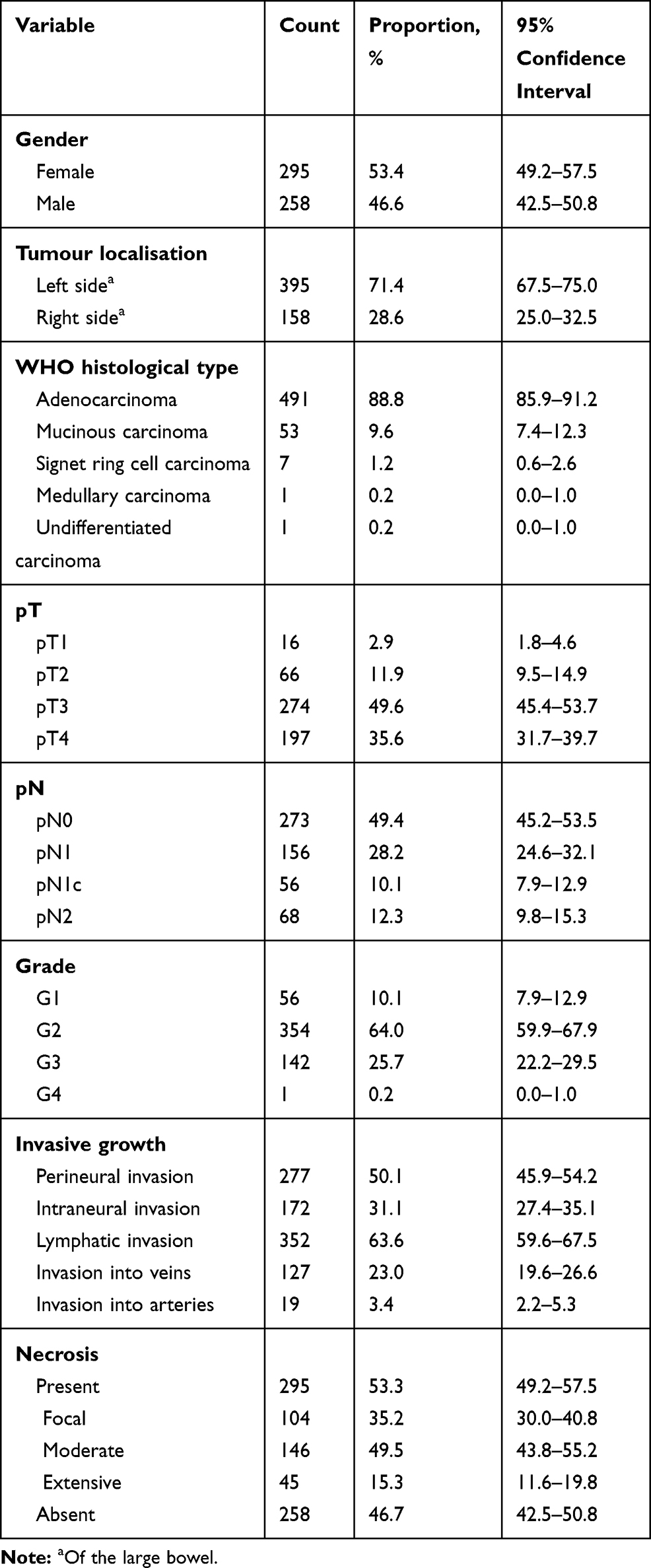 |
Table 2 Clinical and Morphological Profile of the Study Group |
In the whole study group, tumor invasion into lymphatic vessels was found in 352 cases or 63.6% [59.6–67.5], while invasion into veins was observed in 23.0% [19.6–26.6], perineural growth in 50.1% [45.9–54.2] and intraneural growth in 31.1% [27.4–35.1] of the tumors. Invasion into arteries was less frequent (3.4% [2.2–5.3]). Overall, tumor necrosis was present in 295 cases, with most of the carcinomas comprising a moderate amount of necrosis, which was present in 146 cancers representing 49.5% [43.8–55.2] of tumors exhibiting any degree of necrosis.
Pattern of the Inflammatory Reaction
Low-grade inflammation according to the redistributed Klintrup-Mäkinen score was observed in 292 cases or 52.8% [48.6–56.9] and high-grade inflammation in 261 cases or 47.2% [43.1–51.4]. These groups showed statistically significant age differences (p = 0.02). The mean age of patients presenting with low-grade inflammation was 68.1 ± 10.6 years [66.9–69.3], contrasting with 69.6 ± 11.0 years [68.2–70.9] in those characterized by high-grade peritumorous inflammation.
There were statistically significant differences (Table 3) regarding pT distribution (p = 0.002) and the status of regional lymph nodes, reflected by pN (p < 0.001) in relation to low- and high-grade inflammation. In assessing the morphological manifestations of the invasive growth, tumors surrounded by low-grade peritumorous inflammation significantly more frequently featured invasion into lymphatic vessels (p = 0.003), as well as intraarterial (p = 0.012), intravenous (p = 0.017), perineural (p = 0.001) and intraneural (p = 0.01) growth (Table 3). The degree of inflammation was not statistically significantly different between right- and left-sided colorectal carcinomas (p = 0.18), by the presence (p = 0.63) or extent (p = 0.11) of tumour necrosis or by cancer grade (p = 0.07).
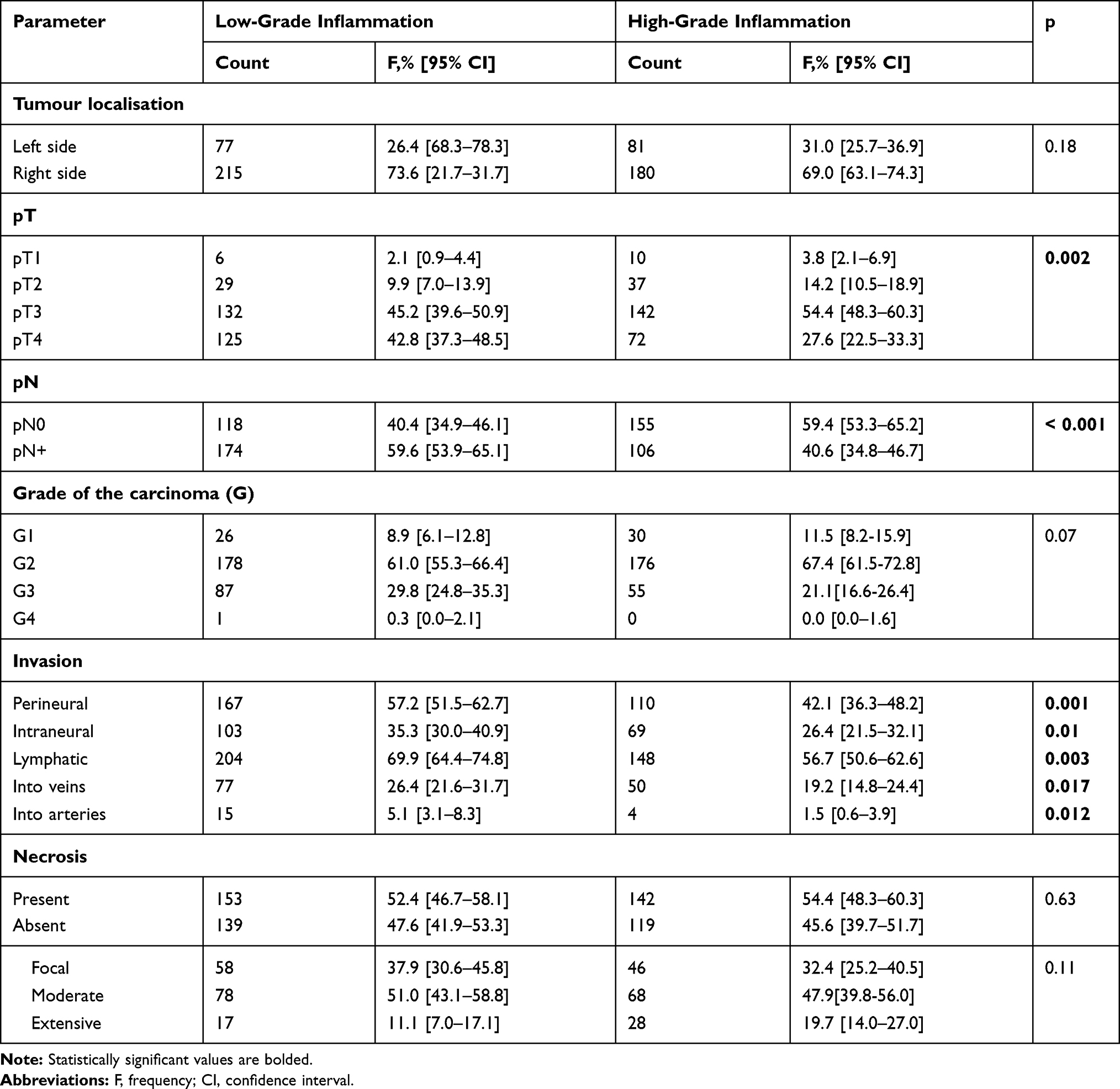 |
Table 3 Association Between Intensity of Peritumorous Inflammation by Klintrup-Makinen Grade and Morphological Features of Colorectal Carcinoma |
CLR (Figure 1) was found in 193 (34.9% [31.0–39.0]) cases. Most (85.5% [79.8–89.7]) of these tumours showed a low density of lymphoid follicles. There were no statistically significant differences in the distribution of CLR density by cancer location (right versus left side of the large bowel), pT, pN, grade, tumour invasion into surrounding structures (blood or lymphatic vessels, nerves) or necrosis (all p > 0.05). In contrast, statistically significant differences were found by assessing the presence versus the absence of CLR in regard to the manifestations of invasive growth (Table 4).
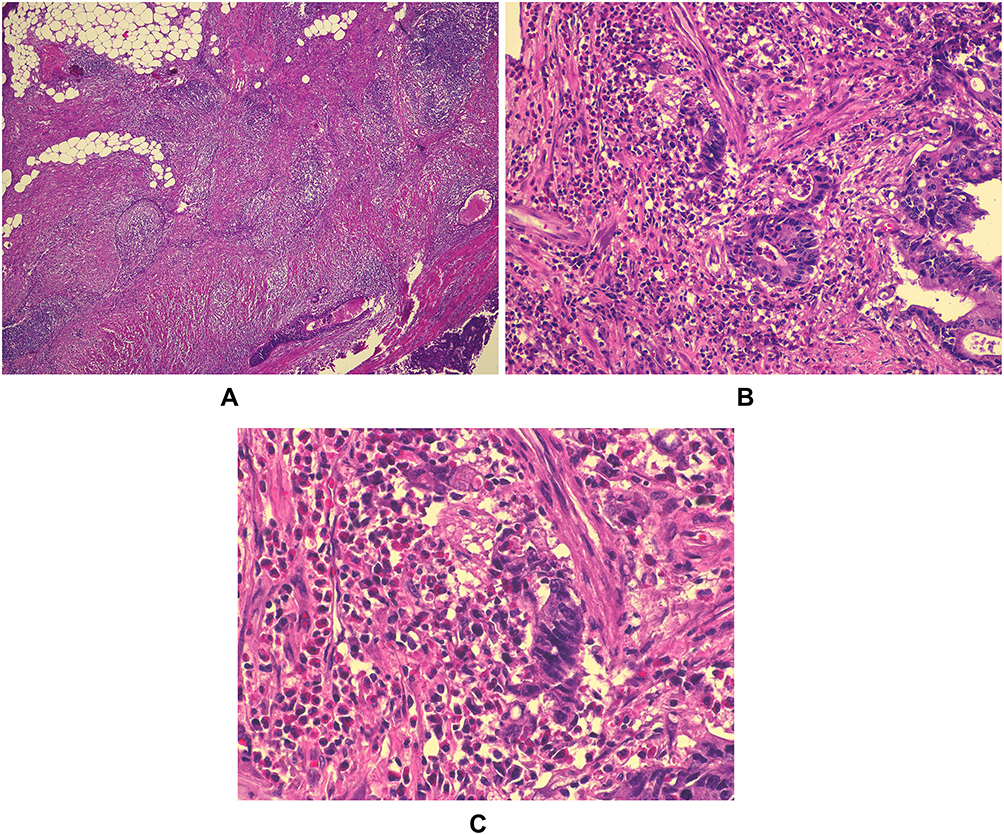 |
Figure 1 Peritumorous inflammation in a colorectal carcinoma. (A): Crohn’s like lymphoid reaction (CLR), hematoxylin-eosin (HE) staining, original magnification (OM) 40×; (B): inflammation in invasion site, HE, OM 100×; (C): mixed cellular composition in peritumorous tissue, HE, OM 400x. |
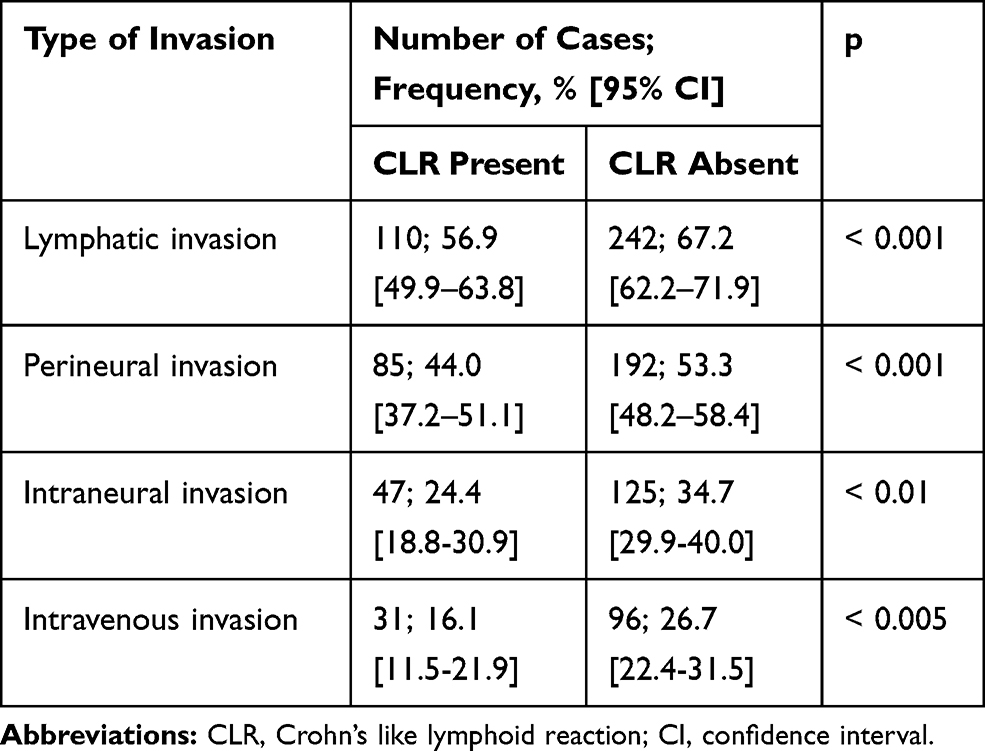 |
Table 4 Association Between Presence of CLR and Manifestations of Invasive Growth of Colorectal Carcinoma |
Inflammatory cell subpopulation analysis (Table 5) highlighted several significant associations between the density of certain tumor-infiltrating cells and the invasive capacity of the carcinoma, reflected by the manifestations of invasive growth (present versus absent). Interestingly, all the statistically significant associations involved lymphatic and perineural invasion that was linked to the density of neutrophilic leukocytes (p-values: p = 0.01 and p = 0.04, correspondingly), lymphocytes (p = 0.03 and p = 0.003) and eosinophilic leukocytes (p = 0.008 and p = 0.01). In contrast, the macrophage counts lacked any statistically significant associations (all p > 0.05).
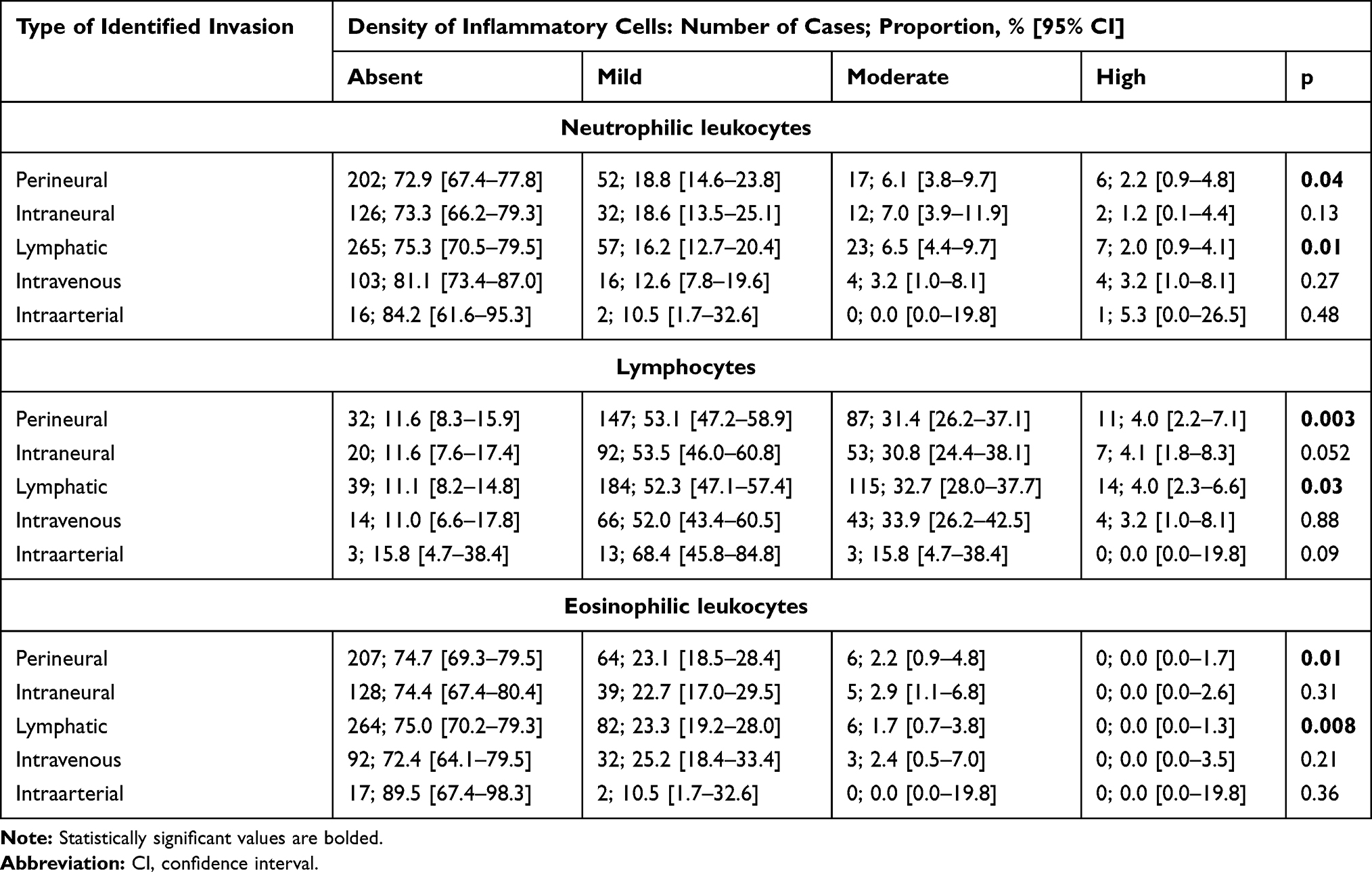 |
Table 5 Association Between Peritumorous Inflammatory Cell Density by Klintrup-Makinen Grade and Morphological Features of Colorectal Carcinoma |
EMT and Cancer Stem Cells
To assess the hypothetical relation between epithelial mesenchymal transition, tumor stemness and inflammation, immunohistochemistry was performed to detect E-cadherin and CD44 antigens (Figures 2 and 3). The overall CD44 score was 1.28 [1.16–1.41], reaching 1.24 [1.10–1.37] in adenocarcinomas and 2.00 [1.61–2.38] in mucinous carcinomas (p = 0.008). The overall E-cadherin score was 1.86 [1.78–1.94]: 1.91 [1.83–1.98] in adenocarcinoma and 1.48 [1.23–1.73] in mucinous carcinoma (p = 0.001). The CD44 expression was statistically significantly (p = 0.026) higher in pN0 carcinomas than in metastatic (pN+) tumors (Table 6). In contrast, CD44 levels did not differ by pT, grade or manifestations of invasive growth. The expression of E-cadherin showed statistically significant differences by grade, but not by pT, pN or manifestations of invasive growth. As regards inflammation, the presence of certain inflammatory cells or CLR, the only significant finding was the association between a high density of eosinophils and upregulation of E-cadherin.
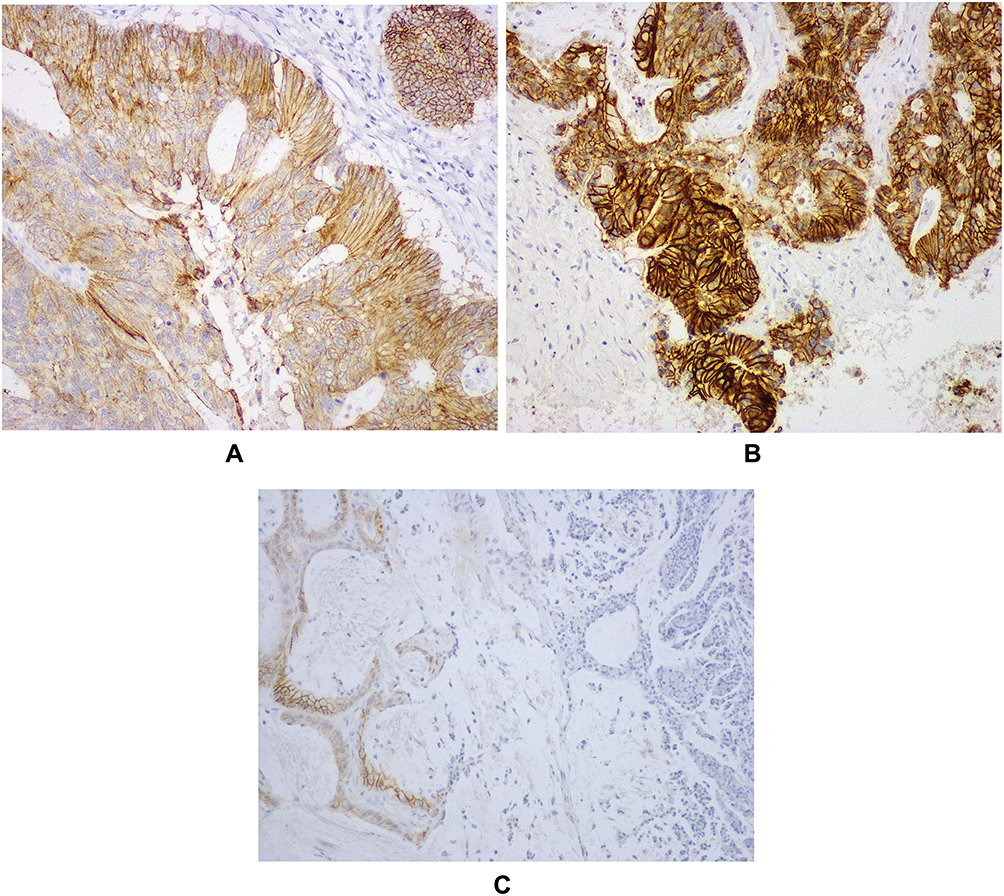 |
Figure 2 E-cadherin expression in CRC. (A): moderate E-cadherin expression, OM 200×; (B): strong expression, OM 200×; (C): weak expression, OM 200×. |
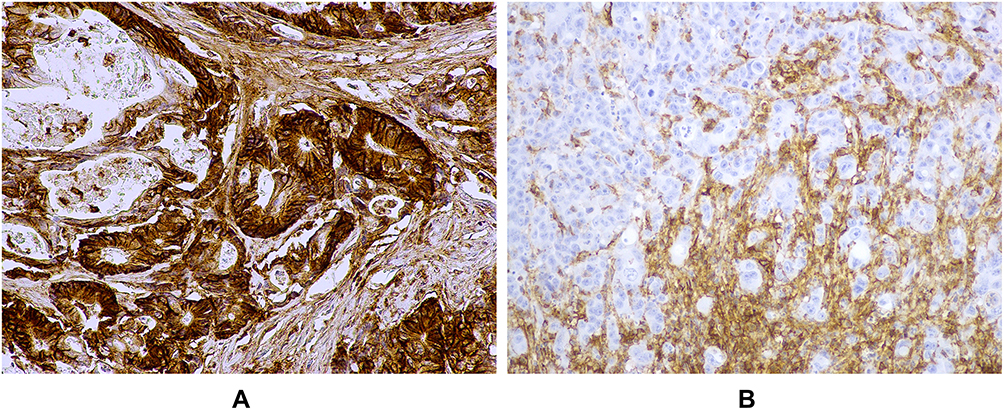 |
Figure 3 CD44 expression in CRC. (A): intense CD44 expression, OM 100×; (B): no CD44 expression in tumor parenchyma, compared with surrounding stromal tissue, OM 200×. |
MMR Protein Analysis
To see whether inflammation has any association with mismatch repair status, IHC analysis of MMR proteins, namely MSH2, MSH6, MLH1 and PMS2, was performed. A complete loss of MSH2, MSH6, PMS2 and MLH1 was found in 0.8% [0.0–4.9], 4.8% [2.0–10.4], 8.9% [4.9–15.3] and 3.2% [1.0–8.3] of cases, respectively (Figure 4). Stratifying the cases into high versus low level of MMR proteins, the Mann–Whitney test showed a statistically significant difference in E-cadherin level by MSH2 and PMS2. CD44 only showed a significant difference by PMS2 expression (Table 7). There was no significant association between the grade of peritumorous inflammation according to the Klintrup-Mäkinen score and the expression of MMR proteins (Table 8), although individual cell analysis showed that an increased density of tumor-infiltrating lymphocytes is associated with MSH6 expression, ranging from 1.66 [1.46–1.86] in cases with mild lymphocytic infiltration to 1.93 [1.74–2.11] in carcinomas showing a moderate to high amount of lymphocytes.
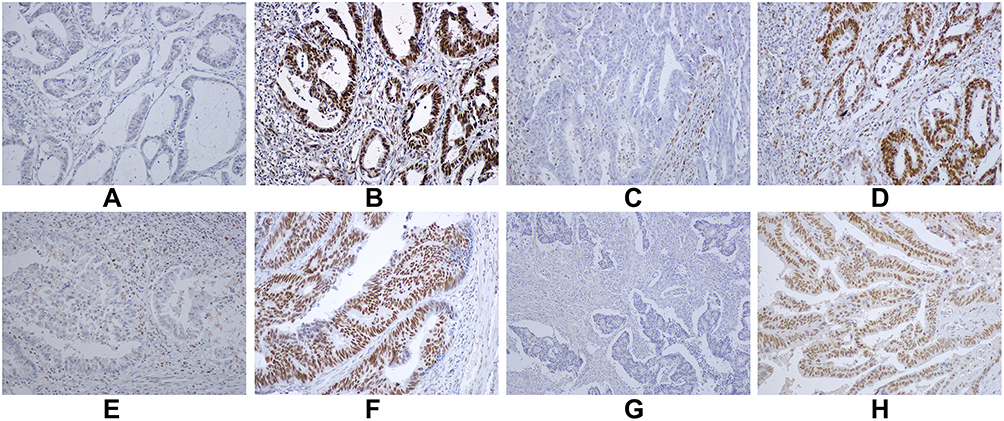 |
Figure 4 MMR protein expression in CRC. (A,B): MSH2: no nuclear expression (A); strong nuclear expression (B); (C,D): MSH6: no nuclear expression (C); strong nuclear expression (D); (E,F): MLH1: no nuclear expression (E); strong nuclear expression (F); (G,H): PMS2: no nuclear expression (G); strong nuclear expression (H). |
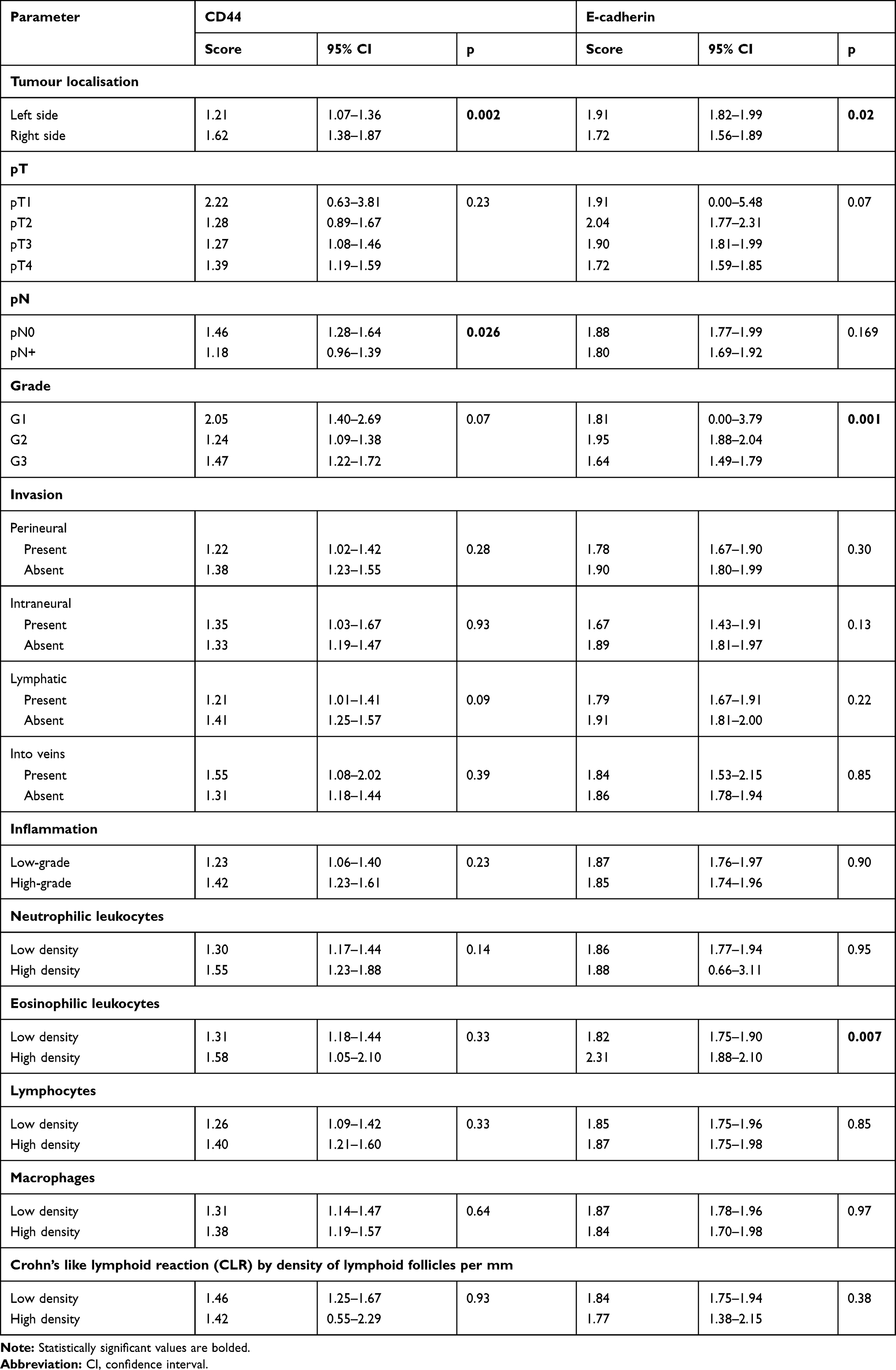 |
Table 6 CD44 and E-Cadherin Expression in Regard to Morphological Features of Colorectal Carcinoma |
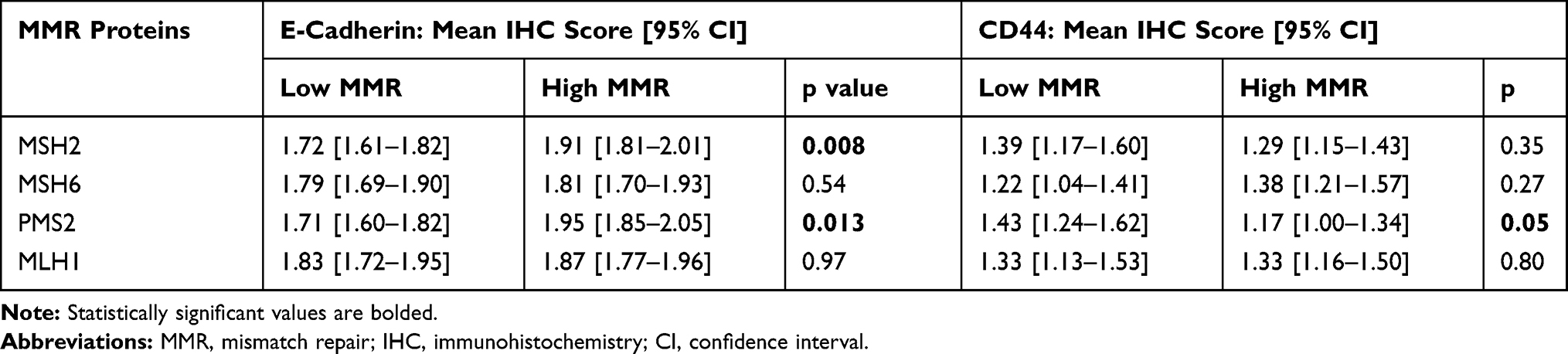 |
Table 7 E-Cadherin and CD44 Levels in Regard to Mismatch Repair Protein Expression in Colorectal Carcinoma |
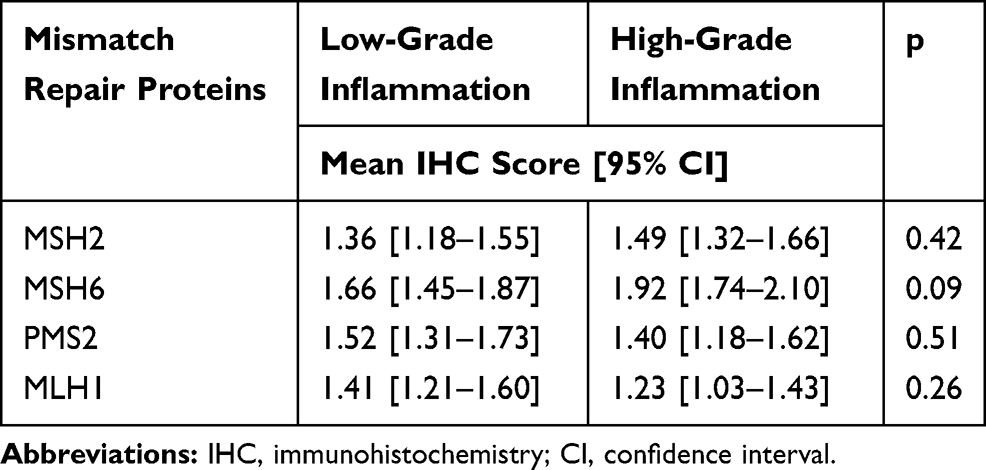 |
Table 8 Mismatch Repair Protein Expression in Regard to Klintrup-Makinen Grade of Peritumorous Inflammation |
Discussion
Colorectal carcinoma is among the most frequent malignant tumors worldwide, ranking third by incidence and fourth by mortality.6 It accounts for 9.7% of the global cancer burden.7 The geographic variations are significant: the incidence rates differ tenfold, with the highest occurring in Europe, North America and, in particular, Australia and New Zealand, the later two having age-standardized incidences of 44.8 and 32.2/100,000 males and females, respectively.6
There are beneficial epidemiological trends, such as declining mortality and increasing five-year survival rates in many countries. For instance, in the USA, the five-year survival rate (across all stages) has improved from 50.6% to 65.4% for colon cancer and from 48.1% to 67.7% in the case of rectal cancer since the mid-70s. The mortality rates have decreased in the USA, Australia and New Zealand, and the majority of western Europe, as well as in some other countries.6 Nevertheless, colorectal cancer still carries significant mortality, accounting for 8.5% of oncological death cases.7 The overall five-year survival rate is 64.9%, ranging from 90% in early cases to 70.4% if the tumour has spread to regional lymph nodes, and only 12.5% if distant metastases are present.6 Therefore both additional prognostic markers and treatment strategies are needed. Inflammation has been targeted for both these directions.
The prognostic role of local and systemic inflammation represents a hot topic in colorectal carcinoma research. Markers of systemic inflammation, e.g. Glasgow prognostic score or neutrophil-to-lymphocyte ratio in peripheral blood, have prognostic and predictive value in colorectal cancer.37 Similarly, the prognostic value of inflammation within the tumor microenvironment has been identified.38
Immunotherapy of colorectal cancer is developing in several directions, including checkpoint blockade, adoptive cell transfer and vaccination. Thus, anti-PD1 treatment has been approved by the Food and Drug Administration for microsatellite-unstable colorectal carcinomas. As most metastatic colorectal cancer cases are microsatellite-stable and the possibilities of immunotherapy are still limited in such tumors, it has been advised to intensify the research of the complex tumor microenvironment in association with microsatellite status.39
As the first target of our study, we aimed to assess the inflammation in a large group of 553 consecutive, surgically treated primary colorectal carcinomas. Colorectal cancer is classically seen in aged people. In accordance with this, most of our patients were diagnosed with the tumor after the age of 50. The proportion of younger patients varies from 0.8% to 15% in different populations, even reaching 36% in Iran.40,41 In the current study, it was 7.0%. Incidence rates in younger adults have been increasing in the USA despite the declining incidence and mortality in those aged 55 or older. Thus, 20–29% of colorectal cancer cases in the USA are diagnosed in patients younger than 55, and this worrisome tendency is associated with either a lack of screening in those younger than 50 or lower adherence to screening, delayed diagnosis and more frequent presence of distant metastases at the time of the first diagnosis.4 Although colorectal cancer is known to be more frequent in males,6 our study shows a slight predominance of females, constituting 53.4% [ 49.2–57.5 %]. This can be explained by the study design. In order to ensure complete evaluation of such morphological traits as the deepest invasion, the status of regional lymph nodes, morphological manifestations of invasive growth and the characteristics of peritumorous inflammation, we had to limit our study to surgically treated cases. Thus, patients who were not suitable for surgery because of advanced local tumour spread, the presence of distant metastases or serious other (e.g. cardiovascular) diseases were also not eligible for the study. Considering the low compatibility with colorectal cancer screening in our population (as discussed later), it is likely that males might have a tendency to approach a doctor with a more advanced tumor. A higher occurrence of cardiovascular diseases in males is also a well-known phenomenon.42
Our cohort is characterized by a remarkable predominance of locally advanced tumors: pT3 carcinoma represented 49.6% [45.4–53.7] and pT4 35.6% [31.7–39.7], but pT2 only 11.9% [9.5–14.9] of all cases. In parallel with this, we observed a high rate of perineural and lymphatic invasion, in contrast to previous studies in other countries.43 These data likely reflect the overall increased proportion of advanced cancer cases in the population, paralleling the reported low compliance (only 9.6% in 2013) with the population-based colorectal cancer screening in Latvia.44 In other European countries, the participation rates in screening programs for colorectal cancer range from 77 to 80% in Germany,45 68.2% in the Netherlands, 19.9% in Croatia and 22.7% in the Czech Republic. The acceptable minimum participation rate is 45% but the desired target is more than 65%, thus screening in our population cannot be considered efficient.3
The intensity of peritumorous inflammation showed a statistically significant association with both the depth of local invasion and the status of regional lymph nodes. Low-grade inflammation was frequently observed in pT4 cases, but it was significantly less common in pT3 carcinomas: 63.5% [56.5–69.9] versus 48.2% [42.3–54.1]. Previously, an association between high-grade inflammation and T1-2 (as opposed to T3-4) had been reported.34 Thus, the Klintrup-Mäkinen grade is shown to have distinct associations with the full scope of pT, from the earliest pT parameters to the advanced cases predominating in our study. Similarly, only 40.4% [34.9–46.1] of patients featuring low-grade inflammation were free of tumor metastases in the lymph nodes (pN0), in contrast to 59.4% [53.3–65.2] in those presenting with high-grade peritumorous inflammation. Our findings are in accordance with Richards et al (2012), who also reported a significant difference (p = 0.0039) between the grade of inflammation in pN0 and pN+.34
As pT and pN are the strongest prognostic factors, our results showing a statistically significant association between high-intensity inflammation and a less extensive cancer spread indirectly confirm the previously described association between high-grade inflammation according to the Klintrup-Mäkinen score and beneficial cancer-specific or overall survival. However, the tendency toward a lower intensity of inflammation in advanced cases also indicates that peritumorous inflammation is not a simple secondary phenomenon related to the extent of tissue damage and/or compromised intestinal motility. Although necrosis is a classic inciting factor of inflammatory reaction, there was no association between cancer necrosis and high-grade peritumorous inflammation. In addition, cases presenting with intense inflammation significantly less frequently featured specific manifestations of the higher invasive capacity of the tumour, including perineural and intraneural growth and invasion into lymphatic vessels, veins and arteries. Thus, high-grade peritumorous inflammation is associated with beneficial morphologic features of colorectal carcinoma and is not secondary to tissue damage and necrosis.
The development of lymphoid aggregates along the invasive front of colorectal cancer was first described by Graham and Appelman as early as in 1990.46 Since the initial report, significant progress has been made regarding both the pathogenetic understanding and the evaluation methods. The considered phenomenon was initially described as a Crohn’s disease-like reaction. Later, Väyrynen et al proceeded with a detailed immunohistochemical evaluation of the cellular composition of these lymphoid aggregates. As there was no evidence of granulomas, which represent the hallmark of Crohn’s disease, the researchers suggested the term “colorectal cancer-associated lymphoid reaction”.36 Initially, qualitative criteria were used for analysis: the CLR was scored as 0 (absent Crohn’s disease-like reaction: no or a single lymphoid aggregate along the whole invasive front in all tumor slides) versus 1 (occasional lymphoid aggregates with rare or absent germinal centres) versus 2 (numerous lymphoid aggregates with germinal centres) as described by Graham and Appelman (1990). Later, Väyrynen et al reported on a quantitative assessment, which showed excellent intra- and inter-observer agreement. Although both approaches were useful for showing the association between a high CLR count and longer survival,36,46 in our study, we followed the recommendations for computer-assisted quantitative evaluation36 given the high accuracy and low observer-related variability.
The association between CLR count and TNM parameters is still controversial. Initially, Graham and Appelman observed that CLR was associated with transmural invasion (in contrast to cancer limited to the intestinal wall) but lower incidence of metastases in regional lymph nodes. In addition, there was an association with right-sided location in the context with transmural growth,46 suggesting an impact of MMR-deficient tumors. Using a quantitative approach analogously to the current study, Väyrynen et al identified a significant association between CLR count and pT in a retrospective cohort of 418 patients,36 but a trend was only observed in a prospective cohort comprising 117 patients.36 We did not find significant associations with pT and pN. The lack of association with grade and pN is in accordance with previous studies.36 This conclusion indirectly indicates that CLR density can be an independent variable to be included in morphological protocols and algorithms of computed-based whole-slide analysis.
Interestingly, the mere presence or absence of CLR46 did show statistically significant associations with the morphological manifestations of invasive growth. Cancers not surrounded by any CLR significantly more frequently displayed lymphatic (p < 0.001), perineural (p < 0.001), intraneural (p < 0.01) and intravenous (p < 0.005) invasion. Thus, the prognostically important threshold identified by Väyrynen et al through ROC analysis of survival may be more related to the outcome of the disease than to a particular morphological profile of the tumor, thereby again suggesting indirectly an independent protective role of immune and inflammatory reaction that is not simply proportional to tumor burden.
Immunoscore,47,48 using the densities of CD3-positive and CD8-positive lymphocytes, has been advised for evaluating the status of the local immune system in colorectal cancer. However, the availability of computer-based immunohistochemical assessment has been questioned.34,35 There is a strong trend of achieving most tumor microenvironment characteristics in routine slides stained by hematoxylin-eosin.34,38 In the near future, the same slides might serve as the basis for computer-based assessment complementing whole-slide scanning.49 Therefore we decided to evaluate the cellular composition of the inflammatory infiltrate on the hematoxylin-eosin basis. In addition, IHC, e.g. for CD68, can be less specific than expected34 due to background or cross-reactivity issues. The possibility of counting cells reliably in HE slides was shown by Richards et al, who reported reasonable inter-observer variabilities, reaching 0.92 for lymphocytes, 0.80 for plasmatic cells and 0.92 for eosinophils.34 In addition to the classically tested relations with pTNM,35 we also evaluated the association with the manifestations of invasive growth.
The density of eosinophils (p = 0.008), neutrophils (p = 0.01) and lymphocytes (p = 0.03) showed statistically significant associations with cancer invasion into lymphatic vessels. Perineural growth was associated with the same cellular players: lymphocytes (p = 0.003), eosinophils (p = 0.01) and neutrophils (p = 0.04). Thus, the densities of particular inflammatory cells, evaluated in regard to the pattern of tumor growth, cluster in a distinct morphological syndrome of lymphatic and perineural invasion. These morphological manifestations of infiltrative growth are remarkable as the most sensitive markers of invasion due to the thin tissue layer subjected to damage. However, they are also the most frequent among the morphological signs of cancer invasion, thereby increasing the power of statistical analysis. Our study might be more capable of detecting the associations between the density of neutrophils, eosinophils and lymphocytes and the pattern of tumor invasion because the present cohort is characterized by a predominance of advanced tumors and hence a high frequency of manifestations of invasive growth. Although further research is clearly necessary to test both the reported findings and the intra- and inter-observer variability, we strongly suggest that evaluation of the inflammatory infiltrate should be included in the routine diagnostic evaluation of colorectal cancer tissues, in order to gain experience and obtain data for further computer-based analysis.
Previously, high numbers of stromal eosinophils in colorectal cancer have been reported to show an association with a lower tumor stage and better overall and cancer-specific five-year survival, as reflected by hazard ratios for death of 0.61 (95% CI: 0.36–1.02; p = 0.02) and 0.48 (95% CI: 0.24–0.93; p = 0.01), respectively.50 Further, a higher density of peritumoral eosinophils was significantly associated with lower T, N and G, the absence of vascular invasion, and longer progression-free and cancer-specific survival.51
The previous findings on neutrophilic leukocytes infiltrating colorectal carcinoma are more controversial.52 High counts of intratumoral neutrophils correlated with a higher pT, pM and stage. This was also an independent adverse prognostic factor.53 Neutrophil infiltration in cancer cells has been demonstrated as being an independent predictor of lymph node metastasis.54 In contrast, a Swedish research team from Umeå University found that neutrophil infiltration in the tumor front was a favorable prognostic factor in early colorectal carcinoma.55 These controversies might be explained by the duality of neutrophils comprising both a tumor-suppressive N1 subpopulation and tumor-supportive N2 neutrophils.52 The N1 versus N2 phenotype of tumor-infiltrating neutrophils depends on the signals encountered in the cancer microenvironment,52 which might be stage-dependent.
The CD44 protein is a transmembrane adhesion molecule. It is involved in the cell-cell or cell-matrix interaction, as well as in cell migration. CD44 is one of the markers for identifying cancer stem cells, characterized by self-renewing, clonogenicity, metastatic spread and resistance to chemotherapy.56 Multiple morphological studies and reviews57 have been devoted to the CD44 expression in colorectal cancer, although they have led to controversial findings. When analyzing 174 patients, more frequent expression was found in G1 and G2 carcinomas (75.8% versus 44.4% in G3; p = 0.037), pN0 (85.7% versus 66.3% in pN+; p = 0.004) and cases lacking lymphatic invasion (88.6% versus 69.2%; p = 0.011). There was no association with pT (p = 0.826).58 In contrast, the authors of a recent meta-analysis concluded that CD44 overexpression in colorectal carcinoma is an unfavorable prognostic factor that predicts a high grade and metastases in lymph nodes and distant sites.59 Hong et al reported on 162 immunohistochemically investigated colorectal cancer cases. This team did not find statistically significant associations between pT (p = 0.578), pTNM stage (p = 0.711), G (p = 0.144) or age (p = 0.690). Nevertheless, they observed a stronger expression in primary carcinoma than in paired lymph node metastasis, characterized by p < 0.001. A loss of CD44 was an independent prognostic factor for cancer-free (p = 0.028) but not overall (p = 0.107) survival.28 In 60 patients, a positive expression of CD44 was associated with histological type, but not pT, pN, M, pTNM stage or G. No association with perineural or lymphovascular invasion was found.60 In mRNA and protein assessment, no differences in CD44 levels were seen by age (p = 0.500), grade (p= 0.026), pT (p = 0.613), lymphovascular (p = 0.422) or perineural (p = 0.734) invasion.61 After preoperative chemoradiotherapy, high levels of CD44 protein in rectal cancer were associated with ypN0 (p = 0.009) but not with age (p = 0.734), ypT (p = 0.666), grade and histological type (p = 0.515), or lymphatic (p = 0.078) or vascular (p = 0.077) invasion.62 In a National Cancer Institute study, there was no association between CD44 and overall survival, grade and histological type, cancer stage and lymph node status.63 In rectal cancer, CD44 did not correlate with age, pT, lymph node metastasis, or lymphatic and blood vessel invasion.64
In our study, we confirmed a significant association between CD44 expression and pN (p = 0.026), as well as with tumor histogenesis (p = 0.008). A statistically significantly higher expression was found in right-sided carcinomas (p = 0.002), paralleling and expanding the observations of more frequent (p = 0.02) expression in colonic adenocarcinomas than in rectal tumours.60 CD44 levels also showed a significant association with the expression of PMS2 protein (p = 0.05).
Malignant tumor progression is closely associated with inflammatory processes, and interaction between pro- and anti-inflammatory cytokines and it has been previously described by different authors. In CRC pathogenesis, as well as in other malignancies, the role of chronic inflammation has been widely discussed. Within blood tests, elevated levels of interleukin-6 (IL-6), interleukin-17 (IL-17), TNF and other cytokines are associated with cancerogenesis.37 Tumor-associated macrophages (TAMs) are one of the sources of cytokines, and their released IL-10 levels increase in patients with CRC, especially in advanced stages.65 Yan et al found a correlation between a high TAM count in gastric cancer and its progression, related to EMT.66 IL-4, one of the anti-inflammatory cytokines produced by T cells, inhibits the expression of E-cadherin and carcinoembryonic antigen (CEA), and its levels are increased in patients with CRC compared to healthy patients.67 Interleukin-8 levels, as described by Kantola et al, increase in patients with CRC, especially in poorly differentiated carcinomas.68
Chen et al, found a relation between high NLR (neutrophil/lymphocyte ratio) and elevated cytokine levels, while lower NLR was associated with lower levels of cytokines.69
Within our study, we found that high-grade inflammation, consisting of high amounts of granulocytes and lymphocytes, is associated with more frequent involvement of anatomical structures, such as lymph vessels and nerves. However, further analysis of monocyte-related changes and the NLR rates within blood should be done.
The authors of several studies exploring inflammatory pathways have identified mechanisms of CD44 upregulation by inflammatory cells and/or the relevant mediators. TNF-beta, produced by activated lymphocytes, induces NF-kappaB activation and EMT (including upregulation of vimentin and downregulation of E-cadherin) and enhances stemness by CD44 expression in colorectal cancer.70 Macrophages that were polarized to M1 state via infection by commensal microorganisms, such as Enterococcus faecalis, activated the Wnt/beta-catenin pathway and upregulated CD44 in murine colonic epithelium. The effect was partially mediated via TNF-alpha.71 In turn, colon adenocarcinoma overexpressing CD44 recruits tumour-associated macrophages.72 Reciprocal interactions between tumor-associated macrophages and CD44-expressing malignant cells promote tumorigenicity in colorectal cancer.73 Crosstalk between stromal fibroblasts and colorectal cancer cells also promotes EMT and CD44 expression.74 The crosstalk between fibroblasts and colorectal carcinoma is also evidenced under the conditions of chemotherapy when it involves interleukin IL-17A messaging to maintain CD44-positive cancer stem cells.75 Nonsteroidal anti-inflammatory drugs suppress CD44-expressing stem cells of colorectal carcinoma via COX-2 inhibition. This effect was evident in cell culture as well as in an in vivo mouse xenograft model.76 Despite these multiple observations linking CD44 and inflammation in colorectal carcinoma, we did not find any significant associations in surgical material. CD44 levels were not related to the grade of inflammation according to the Klintrup-Mäkinen score, cellular components of peritumoral inflammation or the presence of CLR. Thus, the upregulation/loss of CD44 seems to be influenced by a complex network of molecular events, and therefore morphological evaluation of whole tissues represents an important supplement to in vitro and experimental animal studies.
In colorectal cancer, there is a close association between CD44 and EMT, characterized by a loss of epithelial markers, such as E-cadherin, and the development of mesenchymal traits in the tumor cells. EMT leads to enrichment with CD44-positive cancer stem cells.77 Snail, a known activator of EMT, induces CD44expressing cell differentiation.78 CD44 is a canonical target of the Wnt cascade. In turn, CD44 regulates Wnt signalling through a positive feedback loop.79 However, in a large immunohistochemical study from Seoul comprising 174 patients, the loss of E-cadherin was associated with the loss of CD44,58 thereby highlighting once again the complexity of molecular networks in cancer tissues as opposed to in vitro experiments.
E-cadherin is a calcium-dependent epithelial transmembrane glycoprotein supporting epithelial layer integrity and polarity. The loss of E-cadherin, or displacement of it apart from the cell membrane, weakens intercellular adhesion and facilitates cell migration and invasion.56,58 However, E-cadherin may have dual functions in colorectal cancer. Downregulation of E-cadherin is known to develop within epithelial mesenchymal transition associated with higher invasive and metastatic potential of cancer cells and, consequently, a worse outcome. Thus, an immunohistochemical loss of E-cadherin was associated with shorter cancer-free (p = 0.002) and overall survival (p = 0.007) in 286 cases of colorectal cancer.80 In contrast, E-cadherin positivity in colorectal cancer stem cells is associated with a higher growth potential in vivo than seen in the E-cadherin negative subpopulation of cancer stem cells.81 Combined assessment of E-cadherin and CD44 in colorectal cancer has been shown to have a higher prognostic value than isolated evaluation of single markers.29,82 The pathways of EMT induction and stemness differ by MSI status. Twist1 induced EMT and CD44 via AKT/GSK-3beta/beta-catenin and AKT/NF-kappaB pathways in MSS cells, while only the beta-catenin pathway was activated in MSI colorectal cancer cells.83 In contrast, Park et al reported that CD44 expression did not differ by MSI status.84
Several morphological studies have been devoted to E-cadherin expression in colorectal cancer. When analyzing 174 patients, the expression was statistically significantly more frequent (p = 0.007) in G1 and G2 carcinomas (78.2% versus 33.3% in G3). There was no association between pT (p = 0.697), pN (p = 0.456) and lymphatic invasion (p = 0.710) as reported by Seo et al (2015).58 In our study, we also found significant associations between E-cadherin score and cancer grade, but not spread, as reflected by pT and pN. There was a statistically significant link (p = 0.007) between the level of E-cadherin and the density of eosinophils. Interestingly, a protective association (p = 0.003) has been reported between an increased eosinophil blood count and a decreased risk of colorectal cancer, with hazard ratios of 1.0, 0.70 [0.50–0.98] and 0.58 [ 0.40–0.83] across the tertiles of absolute eosinophil count.85 A protective role has also been ascribed to stromal eosinophils in colorectal carcinoma.50 Thus, upregulation of E-cadherin is associated with beneficial tumor features, possibly including the recruitment of eosinophils as one of the mechanisms.
Previously, it has been shown that MLH1 and MSH2 immunohistochemistry has acceptable sensitivity and specificity for high MSI status: 92.3% and 100%, respectively.86 Therefore this approach has been applied in other studies.35 Here, we extended the IHC for MMR proteins with MSH6 and PMS284 that might be implicated in at least 10–15% of pedigrees affected by Lynch syndrome,87 which is known to occur in Latvia as well.88 The levels of certain MMR proteins showed associations with the molecular characteristics of colorectal cancer. Thus, a higher mean score of E-cadherin was significantly associated with the presence of MSH2 (p = 0.008) and PMS2 (p = 0.014), while a lower expression of CD44 was significantly associated with PMS2 (p = 0.05). The expression of MMR proteins did not differ between cases featuring a high versus a low intensity of inflammation according to two-tiered Klintrup-Mäkinen grading.
The key strengths of the current study include the representative in-depth analysis and the high relevance to human pathology as the full complexity of pathogenetic networks is displayed in the affected tissues. The evaluation of inflammation and malignancy as well as of morphology and immunophenotype was carried out using an integrated approach.
To the best of our knowledge, based on a search of PubMed, there are no preceding studies that directly assess the correlations between inflammation, EMT, stem cell differentiation and MMR protein expression in the tissues of colorectal carcinoma. Despite the experimental evidence that provides the theoretical background to link these processes, we found no statistically significant associations in surgical material that indirectly point to a complex, balanced network of cellular and molecular interactions. When elaborating and planning innovative molecular-based or anti-inflammatory treatment options, this complexity must be accounted for.
In order to ensure representative data, the enrolled cohort was of an appropriate size, comprising 553 patients subjected to surgical treatment for primary colorectal carcinoma. Further, as consecutive cases were studied, the tissues represent the full, intricate landscape of events in a cancer microenvironment. The analysis of inflammation, morphological features and immunophenotype of carcinoma was performed in whole-tissue sections that reflect cancer heterogeneity more completely than biopsies or tissue microarrays. The tissue-based assessment of colorectal carcinoma has an advantage over in vitro or animal studies as our approach shows the result of the cellular and molecular interplay in cancer-related inflammation. To ensure accuracy, which is the mainstay of all scientific studies, elaborate, protocol-based morphological evaluation was accomplished by two experienced pathologists in line with WHO and UICC recommendations.
In conclusion, here we present an extensive, detailed study of inflammation in association with morphological and immunohistochemical features of colorectal carcinoma. We have shown that high-grade peritumorous inflammation is associated with beneficial morphologic features of colorectal carcinoma and is not secondary to tissue damage and necrosis.
The densities of particular inflammatory cells, including neutrophils, eosinophils and lymphocytes, in cancer tissues cluster in a distinct morphological syndrome of lymphatic and perineural invasion, confirmed by statistically significant associations. These morphological manifestations of infiltrative growth are remarkable as the most sensitive markers of invasion due to the thin tissue layer subjected to damage. However, those are also the most frequent among the morphological signs of cancer invasion, thereby increasing the power of statistical analysis. Our study might have a greater ability to detect these associations because the present cohort is characterized by a predominance of advanced tumours and hence a high frequency of manifestations of invasive growth.
The complete absence of CLR is statistically significantly associated with more frequent manifestations of invasive growth, including lymphatic, perineural, intraneural and intravenous invasion. However, the CLR density is not related to cancer spread by pTN. These findings indirectly indicate an independent protective role of immune reaction that is not simply proportional to tumor burden. Thus, we suggest that peritumorous inflammation according to Klintrup-Mäkinen score and CLR density should be included in morphological protocols and algorithms of computed-based whole-slide analysis for routine evaluation of surgical materials.
Further, inflammation according to Klintrup-Mäkinen grade and CLR are not dependent on the expression of E-cadherin, CD44 and MMR proteins. Our study highlights the complex associations between inflammation, tumour morphology, EMT, stem cell differentiation and MMR protein expression in surgical tissue material.
Conclusions
High-grade peritumorous inflammation according to Klintrup-Mäkinen score is associated with beneficial morphological features of colorectal carcinoma, including a lower pT, and less frequent lymph node metastases and manifestations of invasive growth. Although necrosis is a classic inciting factor of inflammatory reaction, there was no association between cancer necrosis and high-grade inflammation. Thus, peritumorous inflammation is not secondary to tissue damage (by tumor burden and/or invasive growth) and necrosis.
The densities of particular inflammatory cells, including neutrophils, eosinophils and lymphocytes, cluster in a distinct morphological syndrome of lymphatic and perineural invasion, confirmed by statistically significant associations. These morphological manifestations of infiltrative growth are remarkable as the most frequent and also most sensitive markers of invasion due to the thin tissue layer subjected to damage. Our study might have a greater ability to detect these associations because the present cohort is characterized by a predominance of advanced tumors and hence a high frequency of manifestations of invasive growth.
The complete absence of CLR is statistically significantly associated with more frequent manifestations of invasive growth, including lymphatic, perineural, intraneural and intravenous invasion. However, Crohn’s disease-like lymphoid reaction is not linked to cancer spread by pTN. These findings indicate an independent protective role of inflammatory and immune reaction that is not simply proportional to tumor load. Therefore we suggest that evaluation of peritumorous inflammation by Klintrup-Mäkinen score and CLR should be included in morphological protocols and algorithms of computer-based whole-slide analysis.
Further, inflammation according to Klintrup-Mäkinen grade and CLR density in surgical tissue material is not associated with the expression of E-cadherin, CD44 and MMR proteins. Our study highlights the complex associations between inflammation, tumor morphology, EMT, stem cell differentiation and MMR protein expression in surgical tissue material.
Acknowledgements
The present work was carried out within the frame of a scientific project supported by Riga Stradins University.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marley A, Nan H. Epidemiology of colorectal cancer. Int J Mol Epidemiol Genet. 2016;7(3):105−114.
2. Torre L, Bray F, Siegel R, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87−108. doi:10.3322/caac.21262
3. Navarro M, Nicolas A, Ferrandez A, Lanas A. Colorectal cancer population screening programs worldwide in 2016: an update. World J Gastroenterol. 2017;23(20):3632−3642. doi:10.3748/wjg.v23.i20.3632
4. Smith R, Andrews K, Brooks D, et al. Cancer screening in the United States, 2018: a review of current American Cancer Society guidelines and current issues in cancer screening. CA Cancer J Clin. 2018;68(4):297−316. doi:10.3322/caac.21446
5. Benard F, Barkun A, Martel M, von Renteln D. Systematic review of colorectal cancer screening guidelines for average-risk adults: summarizing the current global recommendations. World J Gastroenterol. 2018;24(1):124−138. doi:10.3748/wjg.v24.i1.124
6. Favoriti P, Carbone G, Greco M, Pirozzi F, Pirozzi R, Corcione F. Worldwide burden of colorectal cancer: a review. Updates Surg. 2016;68(1):7−11. doi:10.1007/s13304-016-0359-y
7. Shinagawa T, Tanaka T, Nozawa H, et al. Comparison of the guidelines for colorectal cancer in Japan, the USA and Europe. Ann Gastroenterol Surg. 2017;2(1):6−12.
8. Marzouk O, Schofield J. Review of histopathological and molecular prognostic features in colorectal cancer. Cancers. 2011;3(2):2767−2810. doi:10.3390/cancers3022767
9. De Divitiis C, Nasti G, Montano M, Fisichella R, Iaffaioli R, Berretta M. Prognostic and predictive response factors in colorectal cancer patients: between hope and reality. World J Gastroenterol. 2014;20(41):15049−15059. doi:10.3748/wjg.v20.i41.15049
10. Saha S, Shaik M, Johnston G, et al. Tumor size predicts long-term survival in colon cancer: an analysis of the National Cancer Data Base. Am J Surg. 2015;209(3):570−574.
11. Vayrynen S, Vayrynen J, Klintrup K, et al. Clinical impact and network of determinants of tumour necrosis in colorectal cancer. Br J Cancer. 2016;114(12):
12. Kraus S, Sion D, Arber N. Can we select patients for colorectal cancer prevention with aspirin? Curr Pharm Des. 2015;21(35):5127−5134. doi:10.2174/1381612821666150915111000
13. Okada F. Inflammation-related carcinogenesis: current findings in epidemiological trends, causes and mechanisms. Yonago Acta Med. 2014;57(2):65−72.
14. Hanahan D, Coussens L. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. 2012;21(3):309−322. doi:10.1016/j.ccr.2012.02.022
15. Galdiero M, Garlanda C, Jaillon S, Marone G, Mantovani A. Tumor associated macrophages and neutrophils in tumor progression. J Cell Physiol. 2013;228(7):1404−1412. doi:10.1002/jcp.24260
16. Wang H, Wang H, Zhou B, et al. Epithelial−mesenchymal transition (EMT) induced by TNF-alpha requires AKT/GSK-3beta-mediated stabilization of snail in colorectal cancer. PLoS One. 2013;8(2):e56664. doi:10.1371/journal.pone.0056664
17. Zhang Z, Xu J, Liu B, et al. Ponicidin inhibits pro-inflammatory cytokine TNF-alpha-induced epithelial-mesenchymal transition and metastasis of colorectal cancer cells via suppressing the AKT/GSK-3beta/Snail pathway. Inflammopharmacology. 2019;27(3):627−638. doi:10.1007/s10787-018-0534-5
18. Mukohyama J, Shimono Y, Minami H, Kakeji Y, Suzuki A. Roles of microRNAs and RNA-binding proteins in the regulation of colorectal cancer stem cells. Cancers. 2017;9(10):143. doi:10.3390/cancers9100143
19. Fabregat I, Malfettone A, Soukupova J. New insights into the crossroads between EMT and stemness in the context of cancer. J Clin Med. 2016;5(3):37. doi:10.3390/jcm5030037
20. Xu J, Zhang Y, Xu J, et al. Reversing tumor stemness via orally targeted nanoparticles achieves efficient colon cancer treatment. Biomaterials. 2019;216:119247. doi:10.1016/j.biomaterials.2019.119247
21. Zlatian O, Comanescu M, Rosu A, et al. Histochemical and immunohistochemical evidence of tumor heterogeneity in colorectal cancer. Roman J Morphol Embryol. 2015;56(1):175−181.
22. Prince M, Sivanandan R, Kaczorowski A, et al. Identification of a subpopulation of cells with cancer stem cell properties in head and neck squamous cell carcinoma. Proc Natl Acad Sci U S A. 2007;104(3):973−978. doi:10.1073/pnas.0610117104
23. Papi A, Orlandi M. Role of nuclear receptors in breast cancer stem cells. World. J Stem Cells. 2016;8(3):62−72.
24. De Smedt L, Lemahieu J, Palmans S, et al. Microsatellite instable vs stable colon carcinomas: analysis of tumour heterogeneity, inflammation and angiogenesis. Br J Cancer. 2015;113(3):500−509. doi:10.1038/bjc.2015.213
25. Shibutani M, Maeda K, Nagahara H, et al. The peripheral monocyte count is associated with the density of tumor-associated macrophages in the tumor microenvironment of colorectal cancer: a retrospective study. BMC Cancer. 2017;17(1):404. doi:10.1186/s12885-017-3395-1
26. Klintrup K, Makinen J, Kauppila S, et al. Inflammation and prognosis in colorectal cancer. Eur J Cancer. 2005;41(17):2645−2654. doi:10.1016/j.ejca.2005.07.017
27. Ngan C, Yamamoto H, Seshimo I, et al. A multivariate analysis of adhesion molecules expression in assessment of colorectal cancer. J Surg Oncol. 2007;95(8):652−662. doi:10.1002/(ISSN)1096-9098
28. Hong I, Hong S, Chang Y, et al. Expression of the cancer stem cell markers CD44 and CD133 in colorectal cancer: an immunohistochemical staining analysis. Ann Coloproctol. 2015;31(3):84−91. doi:10.3393/ac.2015.31.3.84
29. Iseki Y, Shibutani M, Maeda K, Nagahara H, Ikeya T, Hirakawa K. Significance of E-cadherin and CD44 expression in patients with unresectable metastatic colorectal cancer. Oncol Lett. 2017;14(1):1025−1034. doi:10.3892/ol.2017.6269
30. Washington M, Berlin J, Branton P, et al. Protocol for the examination of specimens from patients with primary carcinomas of the colon and rectum. Arch Pathol Lab Med. 2008;132(7):1182−1193.
31. Brierley JD, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours. Oxford (UK): Wiley-Blackwell; 2016.
32. Bosman FTCF, Hruban RH, Theise ND. WHO Classification of Tumours of the Digestive System. Lyon: International Agency for Research on Cancer; 2010.
33. Fleming M, Ravula S, Tatishchev S, Wang H. Colorectal carcinoma: pathologic aspects. J Gastrointest Oncol. 2012;3(3):153−173. doi:10.3978/j.issn.2078-6891.2012.005
34. Richards C, Roxburgh C, Anderson J, et al. Prognostic value of tumour necrosis and host inflammatory responses in colorectal cancer. Br J Surg. 2012;99(2):287−294. doi:10.1002/bjs.v99.2
35. Vayrynen J, Tuomisto A, Klintrup K, Makela J, Karttunen T, Makinen M. Detailed analysis of inflammatory cell infiltration in colorectal cancer. Br J Cancer. 2013;109(7):1839−1847. doi:10.1038/bjc.2013.508
36. Vayrynen J, Sajanti S, Klintrup K, et al. Characteristics and significance of colorectal cancer associated lymphoid reaction. Int J Cancer. 2014;134(9):2126−2135. doi:10.1002/ijc.28533
37. Rossi S, Basso M, Strippoli A, et al. Are markers of systemic inflammation good prognostic indicators in colorectal cancer? Clin Colorectal Cancer. 2017;16(4):264−274. doi:10.1016/j.clcc.2017.03.015
38. Park J, McMillan D, Powell A, et al. Evaluation of a tumor microenvironment-based prognostic score in primary operable colorectal cancer. Clin Cancer Res. 2015;21(4):882−888. doi:10.1158/1078-0432.CCR-14-1686
39. Kather J, Halama N, Jaeger D. Genomics and emerging biomarkers for immunotherapy of colorectal cancer. Semin Cancer Biol. 2018;52:189−197. doi:10.1016/j.semcancer.2018.02.010
40. Campos F. Colorectal cancer in young adults: a difficult challenge. World J Gastroenterol. 2017;23(28):5041−5044. doi:10.3748/wjg.v23.i28.5041
41. Dolatkhah R, Somi M, Kermani I, et al. Increased colorectal cancer incidence in Iran: a systematic review and meta-analysis. BMC Public Health. 2015;15:997. doi:10.1186/s12889-015-2342-9
42. Khan S, Andrews K, Jennings G, Sampson A, Chin-Dusting J. Y chromosome, hypertension and cardiovascular disease: is inflammation the answer? Int J Mol Sci. 2019;20(12):2892. doi:10.3390/ijms20122892
43. Liebig C, Ayala G, Wilks J, et al. Perineural invasion is an independent predictor of outcome in colorectal cancer. J Cli Oncol. 2009;27(31):5131−5137. doi:10.1200/JCO.2009.22.4949
44. Santare D, Kojalo I, Huttunen T, et al. Improving uptake of screening for colorectal cancer: a study on invitation strategies and different test kit use. Eur J Gastroenterol Hepatol. 2015;27(5):536−543. doi:10.1097/MEG.0000000000000314
45. Guo F, Chen C, Schottker B, Holleczek B, Hoffmeister M, Brenner H. Changes in colorectal cancer screening use after introduction of alternative screening offer in Germany: prospective cohort study. Int J Cancer. 2019. doi:10.1002/ijc.32566
46. Graham D, Appelman H. Crohn’s-like lymphoid reaction and colorectal carcinoma: a potential histologic prognosticator. Mod Pathol. 1990;3:332−335.
47. Galon J, Pages F, Marincola F, et al. Cancer classification using the immunoscore: a worldwide task force. J Transl Med. 2012;10:205. doi:10.1186/1479-5876-10-205
48. Guo G, Wang Y, Zhou Y, et al. Immune cell concentrations among the primary tumor microenvironment in colorectal cancer patients predicted by clinicopathologic characteristics and blood indexes. J Immunother Cancer. 2019;7(1):179. doi:10.1186/s40425-019-0656-3
49. Forrest R, Guthrie G, Orange C, Horgan P, McMillan D, Roxburgh C. Comparison of visual and automated assessment of tumour inflammatory infiltrates in patients with colorectal cancer. Eur J Cancer. 2014;50(3):544−552. doi:10.1016/j.ejca.2013.11.003
50. Prizment A, Vierkant R, Smyrk T, et al. Tumor eosinophil infiltration and improved survival of colorectal cancer patients: iowa women’s health study. Mod Pathol. 2016;29(5):516−527. doi:10.1038/modpathol.2016.42
51. Harbaum L, Pollheimer M, Kornprat P, Lindtner R, Bokemeyer C, Langner C. Peritumoral eosinophils predict recurrence in colorectal cancer. Mod Pathol. 2015;28(3):403−413. doi:10.1038/modpathol.2014.104
52. Mizuno R, Kawada K, Itatani Y, Ogawa R, Kiyasu Y, Sakai Y. The role of tumor-associated neutrophils in colorectal cancer. Int J Mol Sci. 2019;20(3):529. doi:10.3390/ijms20030529
53. Rao H, Chen J, Li M, et al. Increased intratumoral neutrophil in colorectal carcinomas correlates closely with malignant phenotype and predicts patients’ adverse prognosis. PLoS One. 2012;7(1):e30806. doi:10.1371/journal.pone.0030806
54. Akishima-Fukasawa Y, Ishikawa Y, Akasaka Y, et al. Histopathological predictors of regional lymph node metastasis at the invasive front in early colorectal cancer. Histopathology. 2011;59(3):470−481. doi:10.1111/j.1365-2559.2011.03964.x
55. Wikberg M, Ling A, Li X, Oberg A, Edin S, Palmqvist R. Neutrophil infiltration is a favorable prognostic factor in early stages of colon cancer. Hum Pathol. 2017;68:193−202.
56. Simtniece Z, Vanags A, Strumfa I, et al. Morphological and immunohistochemical profile of pancreatic neuroendocrine neoplasms. Pol J Pathol. 2015;66(2):176−194.
57. Cherciu I, Barbalan A, Pirici D, Margaritescu C, Saftoiu A. Stem cells, colorectal cancer and cancer stem cell markers correlations. Curr Health Sci J. 2014;40(3):153−161.
58. Seo K, Kim M, Kim J. Prognostic implications of adhesion molecule expression in colorectal cancer. Int J Clin Exp Pathol. 2015;8(4):4148−4157.
59. Wang Z, Tang Y, Xie L, et al. The prognostic and clinical value of CD44 in colorectal cancer: a meta-analysis. Front Oncol. 2019;9:309. doi:10.3389/fonc.2019.00309
60. Ismaiel N, Sharaf W, Helmy D, Zaki M, Badawi M, Soliman A. Detection of cancer stem cells in colorectal cancer: histopathological and immunohistochemical study. Open Access Maced J Med Sci. 2016;4(4):543−547. doi:10.3889/oamjms.2016.126
61. Jing F, Kim H, Kim C, Kim Y, Lee J, Kim H. Colon cancer stem cell markers CD44 and CD133 in patients with colorectal cancer and synchronous hepatic metastases. Int J Oncol. 2015;46(4):1582−1588. doi:10.3892/ijo.2015.2844
62. Saigusa S, Inoue Y, Tanaka K, et al. Clinical significance of LGR5 and CD44 expression in locally advanced rectal cancer after preoperative chemoradiotherapy. Int J Oncol. 2012;41(5):1643−1652. doi:10.3892/ijo.2012.1598
63. Langan R, Mullinax J, Ray S, et al. A pilot study assessing the potential role of non-CD133 colorectal cancer stem cells as biomarkers. J Cancer. 2012;3:231−240. doi:10.7150/jca.4542
64. Nagata T, Sakakura C, Komiyama S, et al. Expression of cancer stem cell markers CD133 and CD44 in locoregional recurrence of rectal cancer. Anticancer Res. 2011;31(2):495−500.
65. Szylberg L, Janiczek M, Popiel A, Marszalek A. Large bowel genetic background and inflammatory processes in carcinogenesis: systematic review. Adv Clin Exp Med. 2015;24(4):555−561. doi:10.17219/acem/31239
66. Yan Y, Zhang J, Li JH, et al. High tumor-associated macrophages infiltration is associated with poor prognosis and may contribute to the phenomenon of epithelial-mesenchymal transition in gastric cancer. Onco Targets Ther. 2016;9:3975−3983.
67. Kanai T, Watanabe M, Hayashi A, et al. Regulatory effect of interleukin-4 and interleukin-13 on colon cancer cell adhesion. Br J Cancer. 2000;82:1717−1723.
68. Kantola T, Klintrup K, Väyrynen J, et al. Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma. Br J Cancer. 2012;107(10):1729−1736. doi:10.1038/bjc.2012.456
69. Chen ZY, Raghav K, Lieu CH, et al. Cytokine profile and prognostic significance of high neutrophil-lymphocyte ratio in colorectal cancer. Br J Cancer. 2015;112(6):1088−1097. doi:10.1038/bjc.2015.61
70. Buhrmann C, Yazdi M, Popper B, et al. Resveratrol chemosensitizes TNF-beta-induced survival of 5-FU-treated colorectal cancer cells. Nutrients. 2018;10(7):888. doi:10.3390/nu10070888
71. Wang X, Yang Y, Huycke M. Commensal-infected macrophages induce dedifferentiation and reprogramming of epithelial cells during colorectal carcinogenesis. Oncotarget. 2017;8(60):102176−102190.
72. Xu H, Zhang Y, Pena M, Pirisi L, Creek K. Six1 promotes colorectal cancer growth and metastasis by stimulating angiogenesis and recruiting tumor-associated macrophages. Carcinogenesis. 2017;38(3):281−292. doi:10.1093/carcin/bgw121
73. Rao G, Wang H, Li B, et al. Reciprocal interactions between tumor-associated macrophages and CD44-positive cancer cells via osteopontin/CD44 promote tumorigenicity in colorectal cancer. Clin Cancer Res. 2013;19(4):785−797. doi:10.1158/1078-0432.CCR-12-2788
74. Buhrmann C, Kraehe P, Lueders C, Shayan P, Goel A, Shakibaei M. Curcumin suppresses crosstalk between colon cancer stem cells and stromal fibroblasts in the tumor microenvironment: potential role of EMT. PLoS One. 2014;9(9):e107514. doi:10.1371/journal.pone.0107514
75. Lotti F, Jarrar A, Pai R, et al. Chemotherapy activates cancer-associated fibroblasts to maintain colorectal cancer-initiating cells by IL-17A. J Exp Med. 2013;210(13):2851−2872. doi:10.1084/jem.20131195
76. Moon C, Kwon J, Kim J, et al. Nonsteroidal anti-inflammatory drugs suppress cancer stem cells via inhibiting PTGS2 (cyclooxygenase 2) and NOTCH/HES1 and activating PPARG in colorectal cancer. Int J Cancer. 2014;134(3):519−529. doi:10.1002/ijc.28381
77. Ye J, Wu D, Shen J, et al. Enrichment of colorectal cancer stem cells through epithelial-mesenchymal transition via CDH1 knockdown. Mol Med Rep. 2012;6(3):507−512.
78. Hwang W, Yang M, Tsai M, et al. SNAIL regulates interleukin-8 expression, stem cell-like activity, and tumorigenicity of human colorectal carcinoma cells. Gastroenterology. 2011;141(1):279−291. doi:10.1053/j.gastro.2011.04.008
79. Orian-Rousseau V, Schmitt M. CD44 regulates Wnt signaling at the level of LRP6. Mol Cell Oncol. 2015;2(3):e995046. doi:10.4161/23723556.2014.995046
80. Choi J, Bae J, Kang M, et al. Expression of epithelial-mesenchymal transition and cancer stem cell markers in colorectal adenocarcinoma: clinicopathological significance. Oncol Rep. 2017;38(3):1695–1705. doi:10.3892/or.2017.5790
81. Tamura S, Isobe T, Ariyama H, et al. Ecadherin regulates proliferation of colorectal cancer stem cells through NANOG. Oncol Rep. 2018;40(2):693−703. doi:10.3892/or.2018.6578
82. Qu J, Jiang Y, Liu H, et al. Prognostic value of E-cadherin-, CD44-, and MSH2-associated nomograms in patients with stage II and III colorectal cancer. Transl Oncol. 2017;10(2):121−131. doi:10.1016/j.tranon.2016.12.005
83. Oh B, Kim S, Lee Y, et al. Twist1-induced epithelial-mesenchymal transition according to microsatellite instability status in colon cancer cells. Oncotarget. 2016;7(35):57066−57076. doi:10.18632/oncotarget.v7i35
84. Park J, Kwon J, Oh S, et al. Differential expression of CD133 based on microsatellite instability status in human colorectal cancer. Mol Carcinogen. 2014;53(Suppl 1):1−10. doi:10.1002/mc.21971
85. Prizment A, Anderson K, Visvanathan K, Folsom A. Inverse association of eosinophil count with colorectal cancer incidence: atherosclerosis risk in communities study. Cancer Epidemiol Biomarkers Prev. 2011;20(9):1861−1864.
86. Lindor N, Burgart L, Leontovich O, et al. Immunohistochemistry versus microsatellite instability testing in phenotyping colorectal tumors. J Clin Oncol. 2002;20(4):1043−1048. doi:10.1200/JCO.20.4.1043
87. Peltomaki P. Deficient DNA mismatch repair: a common etiologic factor for colon cancer. Hum Mol Genet. 2001;10(7):735−740. doi:10.1093/hmg/10.7.735
88. Vanags A, Strumfa I, Gardovskis A, et al. Population screening for hereditary and familial cancer syndromes in Valka district of Latvia. Hered Cancer Clin Pract. 2010;8(1):8. doi:10.1186/1897-4287-8-8
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.