Back to Journals » Clinical Ophthalmology » Volume 19
The Association Between Fundus Changes and Visual Prognosis in Central Retinal Artery Occlusion
Authors Wang H ![]() , Wei H, Dong J, Fang R, Jiang M, Chang Y, Yang R, Zhang F, Yan S, Gao Z, Zhu L, Sun H, Jin L, Li X, Zhang M
, Wei H, Dong J, Fang R, Jiang M, Chang Y, Yang R, Zhang F, Yan S, Gao Z, Zhu L, Sun H, Jin L, Li X, Zhang M
Received 21 September 2025
Accepted for publication 16 December 2025
Published 26 December 2025 Volume 2025:19 Pages 4913—4924
DOI https://doi.org/10.2147/OPTH.S568753
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Hao Wang,1– 3 Hongyu Wei,4 Jieying Dong,5 Ruizhen Fang,3 Mei Jiang,6 Yongye Chang,2 Rong Yang,2 Fen Zhang,7 Suxia Yan,2 Zhimin Gao,2 Liping Zhu,2 Huijing Sun,2 Lihui Jin,2 Xiaorong Li,1 Minglian Zhang2
1Tianjin Medical University Eye Hospital/Eye Institute, Tianjin Medical University, Tianjin, People’s Republic of China; 2Department of TCM Ophthalmology, Hebei Eye Hospital, Xingtai, Hebei, People’s Republic of China; 3North China University of Science and Technology, Tangshan, Hebei, People’s Republic of China; 4Hebei Provincial Hospital of Traditional Chinese Medicine Affiliated to Hebei University of Chinese Medicine, Shijiazhuan, Hebei, People’s Republic of China; 5Department of Pharmacy, Hebei Eye Hospital, Xingtai, Hebei, People’s Republic of China; 6Florence Nightingale Faculty of Nursing, Midwifery & Palliative Care, King’s College London, London, UK; 7Department of Ophthalmology, Xiangya Changde Hospital, Changde, Hunan, People’s Republic of China
Correspondence: Minglian Zhang, Department of TCM Ophthalmology, Hebei Eye Hospital, Xingtai, Hebei, People’s Republic of China, Email [email protected] Xiaorong Li, Tianjin Medical University Eye Hospital/Eye Institute, Tianjin Medical University, Tianjin, People’s Republic of China, Email [email protected]
Purpose: To study the association between fundus changes and visual prognosis in central retinal artery occlusion (CRAO).
Methods: A total of 222 CRAO cases hospitalized at Hebei Eye Hospital between January 2013 and December 2016 were included in this study. Fundus photographs on admission were evaluated via dual independent image review. Retinal ischemic edema and cilioretinal arteries were graded. Logistic regression analysis was performed to explore the association between fundus findings and visual prognosis in CRAO.
Results: The main fundus changes in CRAO patients on admission included retinal ischemic edema (95.0%), cherry-red spot (89.6%), retinal arterial narrowing (65.3%) and venous narrowing (53.6%), cotton-wool spots (53.6%), optic disc margin blurring (36.0%) and pallor (35.1%), retinal venous dilation (21.2%), and retinal hemorrhages (12.6%). Upon admission, retinal edema grades were grade 0 in 11 eyes (5.0%), grade 1 in 23 (10.4%), grade 2 in 80 (36.0%); and grade 3 in 108 (48.6%). Forty-seven eyes (21.1%) showed fissure-like edema, while 164 eyes (73.9%) exhibited a diffuse pattern. Chi square test showed the grade and pattern of retinal ischemic edema, the border and size of the cherry-red spot, the presence of retinal hemorrhage and cotton wool spots, macular folds and retinal arterial narrowing were all significantly associated with the time from symptom onset to presentation. Multivariate logistic regression analysis identified visual acuity at presentation, retinal ischemic grade, optic disc margin clarity, cherry-red spot size, and the presence of a cilioretinal artery supplying the macula as predictive factors for visual prognosis in CRAO.
Conclusion: The fundus changes in acute CRAO were correlated with the visual prognosis. Visual acuity at presentation, grade of retinal ischemic edema, clarity of the optic disc margin, size of the cherry-red spot, and the presence of a cilioretinal artery supplying the macula could be predictive factors for visual prognosis in CRAO.
Keywords: central retinal artery occlusion, visual prognosis, retinal ischemic edema, cherry red spot, vascular change, predictive factor
Introduction
Central retinal artery occlusion (CRAO) is an ophthalmic emergency. Approximately 90% of patients present with visual acuity (VA) worse than 20/200.1–4 A variety of therapeutic interventions are employed for CRAO, including ocular massage, intraocular pressure reduction, vasodilation, oxygen therapy, thrombolysis et al. However, none of these treatments has been validated to improve the visual prognosis of CRAO. In existing literature, once the sample size is statistically sufficient, consistently about 20%-40% of CRAO eyes ultimately achieve a VA of 20/200 or better.5–9 Even CRAO eyes without treatment or with only ocular massage achieved a VA of 20/200 or better in 29% of cases.2 Current literature suggests that VA in a subset of CRAO eyes might improve either spontaneously or following treatment, whereas another subset could suffer severe visual impairment despite undergoing the most aggressive interventions administered immediately after symptom onset. Distinguishing patients with distinct visual prognoses is of great importance. Current clinical studies on CRAO treatment often impose restrictions on the time between symptom onset and presentation, but overlook the distinguishment of patients with different visual prognosis. This could be one of the contributing factors underlying the failure of some clinical trials or the inconsistent conclusions across studies.
Research on predicting visual prognosis in CRAO is limited. Hayreh suggested that the factors influencing visual outcome include the duration of acute retinal ischemia, the cause and type of CRAO, the site of occlusion, and the presence and area of supply by a cilioretinal artery.10 Several other studies showed associations between visual prognosis and the type of CRAO,11,12 changes in fluorescein angiography,11,12 alterations in optical coherence tomography (OCT),13–16 and the “spot sign” in B-scan ultrasound.17–19 Fundus color photography is now one of the most fundamental ophthalmic examinations, providing an objective record of fundus changes. It allows for convenient and intuitive image evaluation, and the capability to magnify images dozens of times on a screen reveals subtle fundus changes with great clarity. This study aims to study the association between fundus changes and visual prognosis in CRAO and to investigate predictive factors for visual prognosis.
Methods
Study Design and Participants
This retrospective study was conducted at Hebei eye Hospital, Hebei Province, China. The medical records of inpatients diagnosed with CRAO between January 2013 and December 2016 were reviewed. CRAO was diagnosed via characteristic clinical features including sudden visual loss in one eye, ischemic retinal whitening, cherry-red spot in the macula, delayed filling of the retinal vessels and prolonged retinal arteriovenous circulation on fundus fluorescein angiography (FFA), thickening and hyperreflectivity in inner retina layers in optical coherence tomography (OCT). Patients with other ocular diseases such as retinal vein occlusion, macular degeneration, glaucoma, optic neuropathy, proliferative diabetic retinopathy were excluded. A total of 252 consecutive CRAO patients were screened; 222 had clear 45° posterior pole color photographs and were included in this study. All participants received conservative treatment, including oxygen therapy, sublingual nitroglycerin, retrobulbar atropine injection, intravenous vasodilators, and oral aspirin. Demographic data, medical histories, best corrected visual acuity (BCVA), ocular findings, treatment regimens, and clinical courses were collected. The final VA was defined as the BCVA at the last follow-up. All patient data were de-identified and anonymized prior to analysis to ensure confidentiality.
Fundus color photographs upon admission were performed by Topcon TRC-NW6S. Two ophthalmologists (HW/RY) experienced in retinal diseases independently evaluated the fundus photographs of enrolled CRAO patients. The inter-rater and intra-rater reliability was quantified, with all Kappa coefficients (for categorical variables) and intraclass correlation coefficients (for continuous variables) between 0.6 to 0.95. When interpretation discrepancies arose, a senior attending physician (MLZ) served as the final arbitrator. To evaluate the severity of retinal ischemic edema, we established a grading system for edema based on representative reference images derived from a large series of CRAO fundus photographs. Grading was performed by comparing the CRAO fundus photograph with these reference images.
Retinal ischemic edema was graded as (see Figure 1):
 |
Figure 1 Reference images of retinal ischemic edema. (a) Grade 0: No macular opacity, the retina appears clear and translucent; (b) Grade 1: Mild macular edema, the retina is slight haze, resembling a thin mist obscuring retinal details; (c) Grade 2: Medium macular opacity, the retina presents diffuse haze, through which the Orange-tinted choroidal background remains partially visible; (d) Grade 3: Severe macular opacity, where the macular and perimacular areas exhibit whitish-gray opacity, completely obscuring the underlying orange choroidal background. |
Grade 0: No macular opacity, the retina appears clear and translucent;
Grade 1: Mild macular edema, the retina is slight haze, resembling a thin mist obscuring retinal details;
Grade 2: Medium macular opacity, the retina presents diffuse haze, through which the orange-tinted choroidal background remains partially visible.
Grade 3: Severe macular opacity, where the macular and perimacular areas exhibit whitish-gray opacity, completely obscuring the underlying orange choroidal background.
Cilioretinal artery may affect visual acuity in eyes with CRAO. Therefore, we grade cilioretinal artery by its perfusion territory area (see Figure 2).
 |
Figure 2 Grading of cilioretinal artery. (a) Grade 1: Perfusion territory ≤1 disc area (DA); (b) Grade 2: Perfusion territory between Grades 1 and 3; (c) Grade 3: Perfusion extends nasal to the fovea, supplying retina nasal to the fovea without reaching temporal fovea; (d) Grade 4: Perfusion extends to or beyond the temporal side of the fovea. |
Grade 1: Perfusion territory ≤1 disc area (DA).
Grade 2: Perfusion territory between Grade 1 and 3.
Grade 3: Perfusion extends nasal to the fovea, supplying retina nasal to the fovea without reaching temporal fovea.
Grade 4: Perfusion extends to or beyond the temporal side of the fovea.
Statistical Analysis
Clinical data of CRAO patients was input into computer using Epidata 3.1 software. Statistical analyses were performed using SPSS 18.0. Fundus changes in the CRAO eyes with final VA < 20/200 were compared against those in eyes with final VA ≥20/200. Categorical variables were described using frequencies and percentages, and compared using Pearson’s chi-square test or Fisher’s exact test. Continuous variables were presented as mean ± standard deviation or median, and compared using the t-test or Mann–Whitney U-test. A two-sided p-value of < 0.05 was considered statistically significant.
Binary logistic regression analysis was performed to investigate the relationship between fundus changes and visual prognosis in CRAO and to identify predictive factors for visual outcome. To ensure a more homogeneous sample, cases were excluded if they met either of the following criteria: (1) symptom onset exceeded 1 week, or (2) hospitalization duration was < 1 week (except for patients with a BCVA ≥ 20/60 at discharge). The dependent variable was defined as follows: Y = 0 for a final BCVA ≥ 0.1, and Y = 1 for a final BCVA < 0.1. Predictor variables with a significance of p < 0.05 from univariate analyses were entered into the multivariate logistic regression model to identify independent factors associated with the visual prognosis.
Results
Demographic data, medical histories, visual acuity, interval between symptom onset and admission, follow-up time of the 222 participants were shown in Table 1.
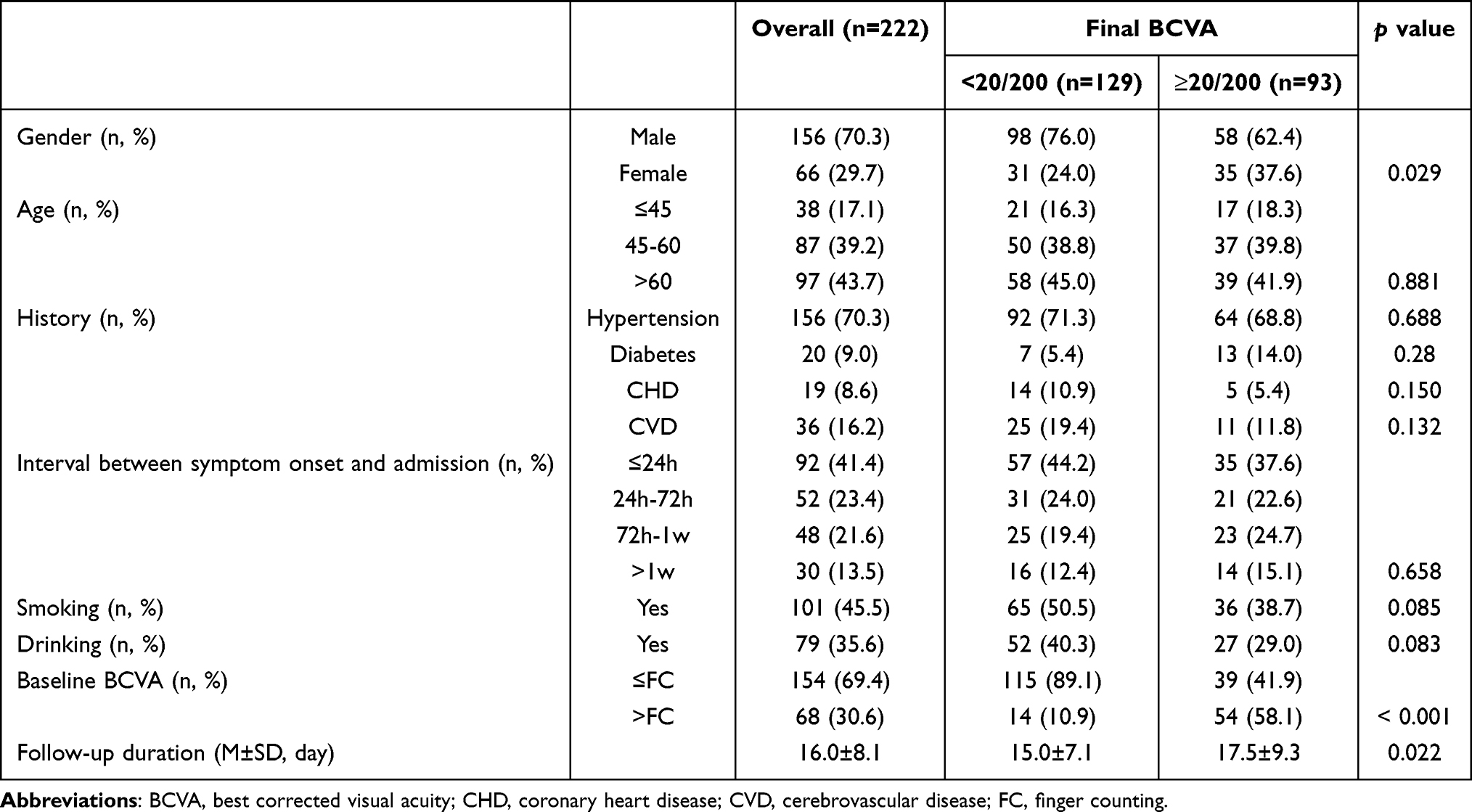 |
Table 1 Demographic and Clinical Characteristics of the 222 CRAO Participants |
Fundus Changes in CRAO
The principal fundus findings at presentation in CRAO included retinal ischemic edema, cherry-red spot, retinal arterial/venous narrowing, and the optic disc margin blurring. Additional changes may be present but these constitute the core features (see Table 2).
 |
Table 2 Fundus Changes in CRAO |
Optic Disc Changes in CRAO
Upon presentation, optic disc changes were observed in 125 of 222 eyes (56.3%), primarily manifesting as disc pallor and disc margin blurring. Disc pallor was present in 78 eyes (35.1%). Disc pallor should not be interpreted as optic nerve atrophy; the pallor reflects optic disc hypoperfusion with a diminished reddish hue compared with the fellow normal eye (see Figure 3a and b). Disc margin blurring occurred in 80 eyes (36.0), accompanied by notable peripapillary retinal whitish edema without elevation of the optic disc or the surrounding retina. In some cases, the disc-margin blur was concentrated at the superior and inferior parts, with relatively distinct nasal and temporal margins. The concomitant presence of disc pallor and margin blurring was observed in 33 eyes (14.9%) (see Figure 3c and d).
 |
Figure 3 Fundus findings of CRAO. (a) Normal fundus; (b) Disc pallor, arterial and venous narrowing, macular diffused edema, well-defined and punched-out cherry red spot; (c) Disc palor and margin blurring, retinal arterial narrowing and venous dilation; (d) Disc pallor, margin blurring, vascular flow interruption and cotton-wool spots; (e) Macular fissure-like edema, dilated retinal vein, and cherry red spot with indistinct border; (f) Diffused macular edema with folds; (g) Hemorrhage on the surface of disc adjacent to the cilioretinal artery. |
Vascular Changes in CRAO
Upon admission, retinal vascular alterations were present in 181 eyes (81.5%), of which 145 eyes (65.3%) exhibited retinal arterial narrowing (See Figure 3e) and 119 eyes (53.6%) showed retinal venous narrowing. Approximately half of the CRAO eyes had concurrent arterial and venous narrowing (110/222, 49.5%) (See Figure 3b, d and f). Retinal vascular narrowing was most readily observed in the large branch vessels of the peripapillary region and those located superior and inferior to the macula. Affected vessels demonstrated not only a reduction in diameter but also irregularities in caliber. Retinal venous dilation, a frequently overlooked sign in CRAO, was present in 47 eyes (21.2%) in this cohort. The dilation was characterized by an increase in venous diameter and a reduced tapering of the lumen upon successive branching compared to normal retinal veins (see Figure 3c and e). Both retinal venous narrowing and dilation were correlated with the final visual outcome (χ2=4.587, p=0.032; χ2=4.416, p=0.036). Eyes with venous narrowing had a poorer visual prognosis, whereas those exhibiting venous dilation were associated with a more favorable visual outcome. Other vessel-associated changes, such as intravascular emboli, vascular flow interruption (see Figure 3d), and vascular sheathing, were less frequently encountered in this case series (see Table 2).
A cilioretinal artery was present in 69 eyes (31.1%) in this case series, all of which arose from the temporal side of the optic disc. The majority of the cilioretinal arteries supplied the papillomacular bundle or the areas immediately above and below it. Twenty-five eyes (25/69, 36.2%) had patent cilioretinal arteries reaching or even extending temporal to the macula. The cilioretinal arteries were graded into four levels according to the area they supplied (see Figure 2). The grade of the cilioretinal artery showed a significant correlation with visual outcome (χ2 = 18.046, p = 0.001; see Table 2).
Retinal Changes in CRAO
The pathological changes secondary to acute ischemia and hypoxia represent the most direct evidence for diagnosing CRAO. Retinal alterations induced by CRAO included retinal ischemic edema, cherry-red spot, cotton-wool spots, and retinal hemorrhages, among others.
Retinal whitish edema secondary to acute ischemia was the most prominent fundoscopic finding in CRAO. Among the patients in this series, varying degrees of retinal whitish edema were observed in 211 eyes (95.0%), while 11 eyes (5.0%) showed no retinal edema at presentation (see Table 2). The retinal ischemic edema caused by CRAO was predominantly located in the posterior pole, particularly involving the macula and the surrounding retina. The edema appeared as a diffuse whitish opacity in the majority of affected eyes (see Figure 3b and f); however, in 22.3% (47/211) of eyes, a relatively normal-colored narrow band was preserved along the retinal arteries, resulting in a “fissure-like” pattern of edema (see Figure 3e). Table 2 summarizes the grading of retinal ischemic edema. In 34 of these cases (15.3%), pronounced retinal swelling in the macular region led to radial macular folds centered on the fovea (see Figure 3f).
A cherry-red spot was present in 199 eyes (89.6%) in this cohort. Eyes without a cherry-red spot typically exhibited milder retinal ischemic edema or harbored a large cilioretinal artery supplying the macular region. The cherry-red spot usually had an indistinct border, with a color transition zone between the spot and the surrounding whitish, edematous retina (see Figure 3c and e). However, in 32 eyes (16.1%), the cherry-red spot was well-defined and punched-out (see Figure 3b and f). The size of the cherry-red spot also varied. In 61 eyes (30.7%), the vertical diameter of the spot was ≤ 1/3 of optic disc diameter. The size of the cherry-red spot was correlated with the final BCVA (χ2 = 23.69, *p* < 0.001): Eyes with a spot vertical diameter ≤ 1/3 optic disc diameter had a worse visual outcome.
Cotton-wool spots-also a manifestation of acute retinal ischemia (see Figure 3e), were observed in 119 eyes (53.6%) at presentation. These spots were predominantly distributed around the optic disc and near the superior and inferior vascular arcades. No correlation was found between the final BCVA and the presence of cotton-wool spots (χ2 = 0.738, p = 0.390).
Retinal hemorrhages unrelated to diabetic retinopathy were observed in 28 eyes (12.6%). These hemorrhages were exclusively distributed around the optic disc or near the retinal vascular arcades (see Figure 3g), presenting as focal, patchy, or flame-shaped lesions located in the superficial retinal layers. Retinal hemorrhages were adjacent to the distribution of the cilioretinal artery present in 14 of these 28 eyes (50%). Pearson’s chi-square analysis revealed a significant correlation between the presence of retinal hemorrhages and the presence of cilioretinal artery (χ2 = 5.35, p = 0.021). However, no significant correlation was found between retinal hemorrhages and final BCVA (χ2 = 3.062, p = 0.080).
Relationship Between Fundus Changes and Time Since CRAO Onset
As shown in Table 3, a significant correlation existed between the time since symptom onset and funduscopic findings at presentation. The grade (χ2 = 15.6, p < 0.001) and pattern (χ2 = 39.1, p < 0.001) of retinal ischemic edema, the border (χ2 = 7.89, p = 0.019) and size (χ2 = 11.92, p = 0.003) of the cherry-red spot, the presence of retinal hemorrhage (χ2 = 7.16, p = 0.028), cotton wool spots (χ2 = 8.47, p = 0.014), macular folds (χ2 = 15.10, p = 0.001) and retinal arterial narrowing (χ2 = 6.07, p = 0.048) were all significantly correlated with the time from symptom onset to presentation.
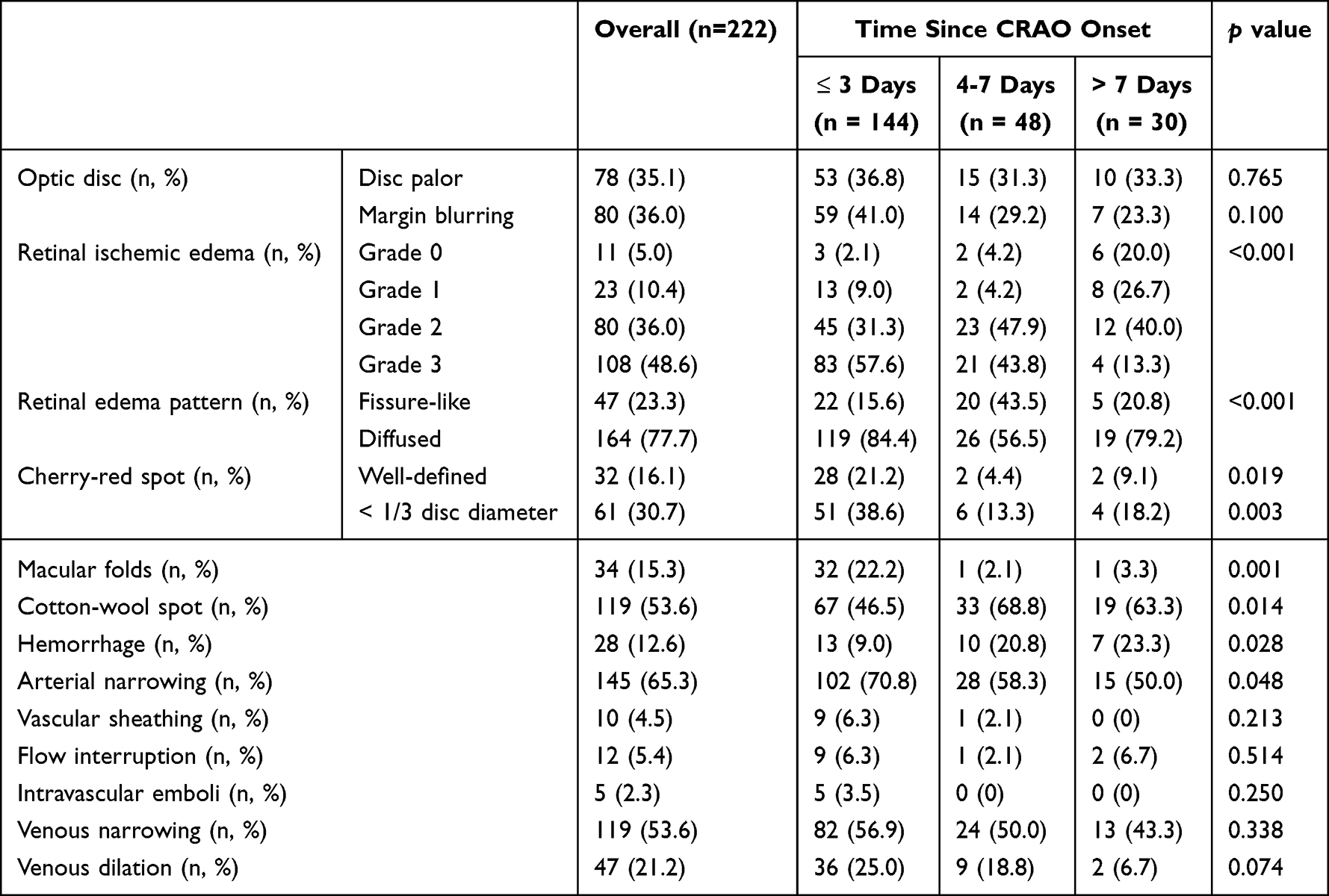 |
Table 3 The Correlation Between Fundus Changes and Time Since CRAO Onset |
In patients presenting within 3 days of symptom onset, macular ischemic edema was more severe and predominantly diffuse. Additionally, macular folds, retinal arterial narrowing, and well defined cherry-red spots < 1/3 disc diameter were more common. By contrast, patients who presented after 3 days exhibited less severe retinal ischemic edema, with a higher proportion of the fissure-like pattern. The prevalence of retinal arterial narrowing and macular folds was significantly reduced, while the incidence of cotton-wool spots and retinal hemorrhages increased.
The Relationship Between Fundus Changes and Visual Prognosis in CRAO
Tltally177 patients were included in the regression analysis. Of these, 79 had a final BCVA ≥20/200, and 98 had a final BCVA < 20/200. Chi-square tests revealed that the following factors were correlated with final BCVA: BCVA at presentation, grade of retinal ischemic edema, presence of macular folds, size of the cherry-red spot, clarity of the optic disc margin, presence of a cilioretinal artery supplying the macula, and retinal venous narrowing. These significant factors were incorporated into the logistic regression model. Multivariate logistic regression analysis revealed that BCVA at presentation, grade of retinal ischemic edema, clarity of the optic disc margin, diameter of the cherry-red spot, and the presence of a cilioretinal artery supplying the macula were significant factors affecting visual prognosis in CRAO. These factors can thus independently serve as predictive factors. A better initial BCVA, milder retinal ischemic edema, or the presence of a cilioretinal artery supplying the macula predicted a more favorable visual outcome. Conversely, an indistinct optic disc margin or a cherry-red spot diameter ≤ 1/3 of the optic disc diameter predicted a poor visual prognosis in CRAO. The results of the analysis are presented in Table 4.
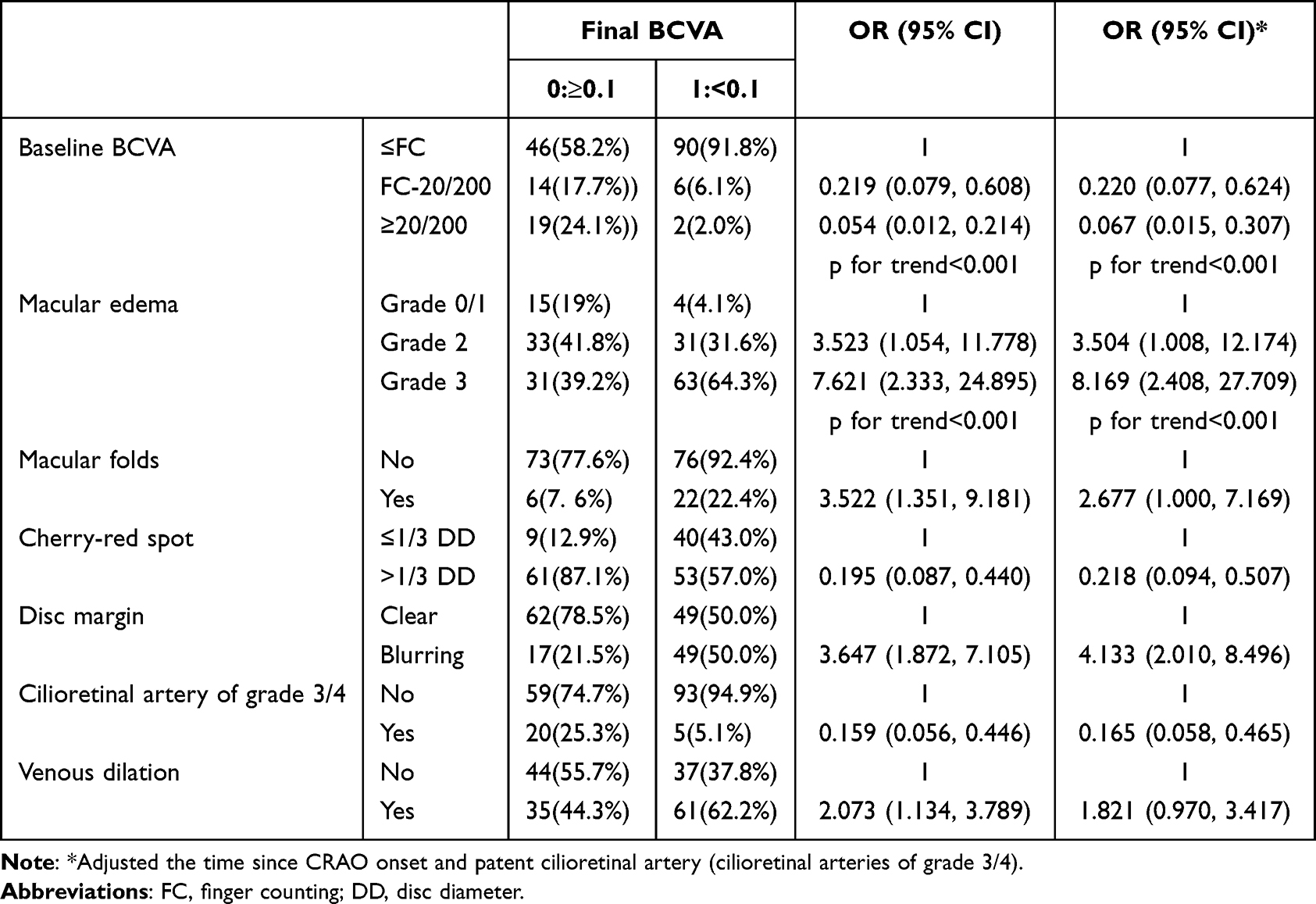 |
Table 4 Logistic Regression Analysis of Factors Associated with Visual Prognosis in CRAO |
Discussion
The retinal pathological changes constitute the most direct evidence for diagnosing CRAO and serve as a critical basis for assessing the severity of the condition. By reviewing the fundus photographs of 222 CRAO patients at admission, this study found that the main funduscopic changes upon presentation included retinal ischemic edema, cherry-red spot, retinal arterial and/or venous narrowing, blurring of the optic disc margin, and cotton-wool spots. Other less common alterations included retinal hemorrhages, venous dilation, and macular folds. Logistic regression analysis identified BCVA at presentation, the grade of retinal ischemic edema, clarity of the optic disc margin, size of the cherry-red spot, presence of macular folds, and a cilioretinal artery supplying the macula as factors influencing the final visual outcome in CRAO. These factors can therefore serve as independent predictors for visual prognosis in CRAO.
Retinal Ischemic Edema and Cherry-Red Spot in CRAO
The most prominent funduscopic finding in CRAO is retinal ischemic edema. Acute ischemia results in retinal intracellular edema and coagulative necrosis, manifesting as grayish-white opacification upon ophthalmoscopic examination or fundus photography. The macula has the highest cellular density, and exhibits the most pronounced grayish-white opacification in CRAO, whereas the peripheral retina-with lower cellular density and thinner structure-shows minimal morphological changes.20 The central foveola contains only photoreceptors and is primarily nourished by the choroid. It remains transparent in CRAO, making the underlying color of the choroid and retinal pigment epithelium visible, and presenting the “cherry-red spot”. Cherry-red spot sometimes is absent in CRAO.21 Hayreh reported a noticeable cherry-red spot appeared within 20 minutes after the central retinal artery was blocked in animal CRAO models.22 In this study, the severity of retinal ischemic edema was graded by comparison with standard photographs. Lower-grade edema often coexisted with a poorly defined cherry-red spot. Severe retinal ischemia can lead to significant tissue swelling, which leads to macular folds. This swelling compresses the cherry-red spot, reducing its size and sharpening its borders. Both the grade of retinal edema and the morphology of the cherry-red spot can serve as indicators for assessing CRAO severity.
In some CRAO cases, a narrow peri-artery retinal band with relatively normal color can be observed, resulting in a “fissure-like” pattern of edema. This indicates that residual blood flow within the retinal artery may support the immediate perivascular avascular zone, thereby preventing the development of ischemic edema in this area or facilitating its resolution. This study found that the presence of fissure-like edema was associated with the time since symptom onset. The proportion of eyes with fissure-like edema was only 15.6% among those presenting within 72 hours of onset. This proportion nearly doubled in patients presenting at 4–7 days. Concurrently, the proportion of eyes with diffuse edema decreased by one-third. This finding suggests the recovery of retinal blood flow during CRAO.
Disc Changes in CRAO
Disc pallor and margin blurring are the primary alterations of the optic disc in CRAO, and they may occur in isolation or coexist.
In animal models of CRAO, Hayreh observed that disc pallor could occur as early as 7 minutes after the CRAO onset.22 Among patients presenting within 1 week of CRAO onset, 27.2% exhibited optic disc pallor. In the present study, a higher proportion (35.1%) of eyes with CRAO showed optic disc pallor upon presentation. Statistical analysis revealed that disc pallor was correlated with retinal arterial narrowing, venous narrowing, and venous dilation (χ2 = 19.77, 32.39, 6.686, respectively; p < 0.001, < 0.001, = 0.01, respectively). Disc pallor was more common in eyes with retinal arterial/venous narrowing, while less frequently observed in eyes with retinal venous dilation. Based on these findings, we propose that disc pallor in CRAO should be attributable to optic disc circulatory disturbance, rather than edema of the superficial nerve fiber layer.20
It has been reported that 16.9% of CRAO patients presenting within 1 week of symptom onset exhibited optic disc edema.20 In the present study, optic disc margin blurring was observed in 36.0% of eyes with CRAO, with the superior and inferior disc poles being most prominently involved. This margin blurring often coexisted with other signs of severe retinal ischemia, such as retinal arterial narrowing and disrupted blood flow, and correlated with the grade of macular edema. Typically, CRAO does not induce optic disc swelling or elevation, unless complicated by anterior ischemic optic neuropathy (AION) or other optic nerve disorders. Instead, it presents solely as disc margin blurring, which arises from edema of the retinal nerve fiber layer (RNFL) rather than from primary optic disc pathology. Therefore, using the term “optic disc edema” to describe this sign may be misleading. We recommend the more precise description “blurring of the optic disc margin” to avoid conceptual ambiguity.
Retinal Vascular Changes in CRAO
Retinal arterial alterations are crucial diagnostic evidence for CRAO, primarily including arterial narrowing, blood flow disruption, and intravascular emboli. In the present study, complete interruption of retinal blood flow was rare; instead, residual blood flow persisted within the arteries in most cases. Arterial narrowing was observed in 65.3% of eyes at presentation—a proportion significantly higher than that reported in Hayreh’s study.20 This discrepancy may be explained by the timing of patient presentation: the majority of patients in our cohort were evaluated within 1 week of symptom onset. Given the time-dependent progression of fundus manifestations in CRAO, retinal arterial narrowing is more pronounced during the disease early stage. Retinal arterial emboli were identified in only 2.3% of eyes with CRAO in this series, all of which were bright, yellowish cholesterol emboli. By contrast, Hayreh reported a detection rate of emboli as high as 69%.20 This substantial discrepancy may be attributed to two key factors. First, our embolus assessment relied solely on fundus photographs that likely missed emboli located in the peripheral retina. Second, Hayreh’s embolus diagnosis was based on repeated evaluations conducted over multiple follow-up visits, —an approach that better captured the temporal and spatial multifocality of embolic distribution within the retinal vasculature.
Retinal vein alterations primarily include venous narrowing and venous dilation. Venous narrowing in CRAO often coexists with arterial narrowing, whereas retinal venous dilation is a frequently overlooked sign. In the present study, this sign was observed in 47 eyes (21.2%). Venous dilation was characterized not only by an increase in venous diameter but also by a reduced tapering of the venous lumen upon branching, resulting in a diminished caliber difference between the major venous trunk and its tributaries. Retinal venous dilation may indicate either partial retinal reperfusion or impaired vascular autoregulation.
Other Retinal Changes in CRAO
Retinal hemorrhage can also occur in CRAO. In this study, 28 eyes (12.6%) exhibited retinal hemorrhages. These hemorrhages were focal, patchy, or flame-shaped, exclusively, and distributed near the optic disc, around the retinal vascular arcades, or adjacent to the perfusion area of a cilioretinal artery. All these regions have relatively better blood supply. It has been proposed that these superficial flame-shaped or patchy hemorrhages are related to arterial perfusion pressure. Retinal ischemia may impair the blood-retinal barrier, which becomes susceptible to rupture under intraluminal perfusion pressure.23 Compared to deeper capillary networks, the superficial capillaries are subjected to greater perfusion pressure, which may explain why hemorrhages in CRAO often appear flame-shaped or patchy. Retinal hemorrhages were more prevalent in CRAO cases presenting beyond 3 days of symptom onset. This finding suggests that incomplete retinal reperfusion occurring at a certain time point following retinal artery occlusion under ischemic conditions.
Predictive Factors for Visual Prognosis in CRAO
A review of the existing literature reveals that some patients with CRAO may achieve visual improvement even in the absence of treatment, whereas some others would suffer from persistent severe visual impairment, despite receiving the most aggressive interventions administered immediately after symptom onset. Previous studies on CRAO often selected participants based primarily on factors such as time since symptom onset and the presence of a cilioretinal artery, without comprehensively evaluating the overall retinal condition to predict visual prognosis. This approach may introduce selection bias and confounding factors, thereby influencing the research outcomes. Therefore, to some extent, predicting the potential for visual recovery and carefully selecting appropriate CRAO cases—before initiating clinical studies—are more critical than the choice of interventional treatment itself.
Research on visual prognosis prediction in CRAO remains relatively limited. Hayreh,2 Schmidt11 and Ahn24 all found that CRAO classification was associated with visual prognosis. Since the classification is primarily based on findings from funduscopy and fluorescein angiography (FFA), their work indirectly supports a link between funduscopic or FFA changes and CRAO visual prognosis. Hadanny et al found that the presence of a cherry-red spot was correlated with visual prognosis of CRAO; those with a cherry-red spot had poorer vision, while conversely, the visual prognosis was better in its absence.6 Gong et al categorized CRAO into three types based on angiographic findings: hypoperfusion, exudative, and mixed. They demonstrated that this angiographic classification correlated with the degree of visual impairment, with the exudative type exhibiting a more favorable visual prognosis than the hypoperfusion or mixed types.12 Alterations on optical coherence tomography (OCT) in eyes with CRAO also correlate with visual prognosis. Specifically, the retinal thickness shows a positive correlation with logMAR visual acuity.13–16 Furthermore, Chen et al demonstrated that final logMAR visual acuity was mildly or moderately correlated with retinal thickness and strongly correlated with the optical intensity of photoreceptor/retinal pigment epithelium and optical intensity ratio.16 On B-scan ultrasonography, a “spot sign” posterior to the optic disc in CRAO indicates an embolus and is often associated with a poor visual prognosis.18,19
Visual acuity and fundoscopic findings are the most readily available clinical data for CRAO patients at presentation. These findings not only reflect the degree of retinal ischemia, but also provide information on current retinal function and circulatory status, thereby assisting clinicians in assessing disease severity and predicting visual prognosis. Identifying predictive factors from these parameters holds significant clinical value. This study focused on pathological changes in posterior pole fundus photographs of CRAO patients. Logistic regression analysis revealed that BCVA at presentation, the grade of retinal ischemic edema, the size of the cherry-red spot, presence of a patent cilioretinal artery and the clarity of the optic disc margin were all associated with visual outcome, and could serve as independent predictive factors for visual prognosis in CRAO. A better initial BCVA, milder retinal ischemic edema, or the presence of a cilioretinal artery supplying the macula predicted a more favorable visual outcome. By contrast, an indistinct optic disc margin or a cherry-red spot with a diameter ≤ 1/3 of the optic disc diameter indicated a poor visual prognosis.
Conclusion
Common funduscopic changes in acute CRAO include retinal ischemic edema, cherry-red spot, retinal arterial and/or venous narrowing, blurring of the optic disc margin, and cotton-wool spots, as well as other less frequent alterations such as retinal hemorrhages, venous dilation, and macular folds. The fundus changes in acute CRAO were correlated with the visual prognosis. Visual acuity at presentation, grade of retinal ischemic edema, clarity of the optic disc margin, size of the cherry-red spot, and the presence of a cilioretinal artery supplying the macula could be predictive factors for visual prognosis in CRAO.
Data Sharing Statement
The de-identified data used to support the findings of this study are available from the corresponding author (Prof. Minglian Zhang, email: [email protected]; Prof. Xiaorong Li, [email protected]) on reasonable request.
Ethics
This study was conducted with approval by the Hebei eye Hospital Institutional Review Board (ethics approval number: 2024KY42), which waived the requirement for individual informed consent due to the retrospective nature of the research. All procedures adhered to the tenets of the Declaration of Helsinki. All patient data were de-identified and anonymized prior to analysis to ensure confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Hebei Provincial Key R&D Program - TCM Innovation Special Project (No.23377712D), Xingtai city Innovation Capacity Enhancement Program (No.2023ZZ106) and High-Level Key Discipline in Traditional Chinese Medicine Construction and Development Project launched by the National Administration of Traditional Chinese Medicine (No.zyyzdxk-2023017).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Rumelt S, Dorenboim Y, Rehany U. Aggressive systematic treatment for central retinal artery occlusion. Am J Ophthalmol. 1999;128(6):733–738. doi:10.1016/S0002-9394(99)00359-1
2. Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140(3):376–391. doi:10.1016/j.ajo.2005.03.038
3. Takai Y, Tanito M, Matsuoka Y, et al. Systemic prostaglandin E1 to treat acute central retinal artery occlusion. Invest Ophthalmol Vis Sci. 2013;54(4):3065–3071. doi:10.1167/iovs.12-11445
4. Shah R, Zheng X, Patel AP, et al. Central retinal artery occlusion: visual outcomes from a large northern california cohort. Ophthalmol Retina. 2024;8(6):566–570. doi:10.1016/j.oret.2023.12.007
5. Richard G, Lerche RC, Knospe V, et al. Treatment of retinal arterial occlusion with local fibrinolysis using recombinant tissue plasminogen activator. Ophthalmology. 1999;106(4):768–773. doi:10.1016/S0161-6420(99)90165-3
6. Hadanny A, Maliar A, Fishlev G, et al. Reversibility of retinal ischemia due to central retinal artery occlusion by hyperbaric oxygen. Clin Ophthalmol. 2017;11:115–125. doi:10.2147/OPTH.S121307
7. Runsheng W, Peilin L, Yaping Z, et al. Intravenous thrombolysis with urokinase for central retinal artery occlusion in 115 patients. Chin J Ocular Fundus Dis. 2012;28(5):466–471.
8. Préterre C, Gaultier A, Obadia M, et al. Intravenous alteplase versus oral aspirin for acute central retinal artery occlusion within 4·5 h of severe vision loss (THEIA): a multicentre, double-dummy, patient-blinded and assessor-blinded, randomised, controlled, Phase 3 trial. Lancet Neurol. 2025;24(11):909–919. doi:10.1016/S1474-4422(25)00308-4
9. Schumacher M, Schmidt D, Jurklies B, et al. Central retinal artery occlusion: local intra-arterial fibrinolysis versus conservative treatment, a multicenter randomized trial. Ophthalmology. 2010;117(7):1367–75.e1. doi:10.1016/j.ophtha.2010.03.061
10. Hayreh SS. Central retinal artery occlusion. Indian J Ophthalmol. 2018;66(12):1684–1694. doi:10.4103/ijo.IJO_1446_18
11. Schmidt DP, Schulte-Monting J, Schumacher M. Prognosis of central retinal artery occlusion: local intraarterial fibrinolysis versus conservative treatment. AJNR Am J Neuroradiol. 2002;23(8):1301–1307.
12. Gong H, Song Q, Wang L. Manifestations of central retinal artery occlusion revealed by fundus fluorescein angiography are associated with the degree of visual loss. Exp Ther Med. 2016;11(6):2420–2424. doi:10.3892/etm.2016.3175
13. Ikeda F, Kishi S. Inner neural retina loss in central retinal artery occlusion. Jpn J Ophthalmol. 2010;54(5):423–429. doi:10.1007/s10384-010-0841-x
14. Chen SN, Hwang JF, Chen YT. Macular thickness measurements in central retinal artery occlusion by optical coherence tomography. Retina. 2011;31(4):730–737. doi:10.1097/IAE.0b013e3181f2a15c
15. Ahn SJ, Woo SJ, Park KH, et al. Retinal and choroidal changes and visual outcome in central retinal artery occlusion: an optical coherence tomography study. Am J Ophthalmol. 2015;159(4):667–676. doi:10.1016/j.ajo.2015.01.001
16. Chen H, Xia H, Qiu Z, et al. Correlation of optical intensity on optical coherence tomography and visual outcome in central retinal artery occlusion. Retina. 2016;36(10):1964–1970. doi:10.1097/IAE.0000000000001017
17. Schnieder M, Fischer-Wedi SV, Bemme S, et al. The retrobulbar spot sign and prominent middle limiting membrane as prognostic markers in non-arteritic retinal artery occlusion. J Clin Med. 2021;10(2):338. doi:10.3390/jcm10020338
18. Ertl M, Altmann M, Torka E, et al. The retrobulbar “spot sign” as a discriminator between vasculitic and thrombo-embolic affections of the retinal blood supply. Ultraschall Med. 2012;33(7):E263–7. doi:10.1055/s-0032-1312925
19. Nedelmann M, Tanislav C, Kaps M. A traveling “spot sign” in recurrent amaurosis fugax and central retinal artery occlusion. J Stroke Cerebrovasc Dis. 2014;23(9):e421–2. doi:10.1016/j.jstrokecerebrovasdis.2014.05.001
20. Hayreh SS, Zimmerman MB. Fundus changes in central retinal artery occlusion. Retina. 2007;27(3):276–289. doi:10.1097/01.iae.0000238095.97104.9b
21. Fan W, Huang Y, Zhao Y, et al. Central retinal artery occlusion without cherry-red spots. BMC Ophthalmol. 2023;23(1):434. doi:10.1186/s12886-023-03176-w
22. Hayreh SS, Weingeist TA. Experimental occlusion of the central artery of the retina. I. Ophthalmoscopic and fluorescein fundus angiographic studies. Br J Ophthalmol. 1980;64(12):896–912. doi:10.1136/bjo.64.12.896
23. Hayreh SS, Van Heuven WA, Hayreh MS. Experimental retinal vascular occlusion. I. Pathogenesis of central retinal vein occlusion. Arch Ophthalmol. 1978;96(2):311–323. doi:10.1001/archopht.1978.03910050179015
24. Ahn SJ, Kim JM, Hong JH, et al. Efficacy and safety of intra-arterial thrombolysis in central retinal artery occlusion. Invest Ophthalmol Vis Sci. 2013;54(12):7746–7755. doi:10.1167/iovs.13-12952
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.