Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
The association between cardiac autonomic neuropathy and diabetes control
Authors Vasheghani M ![]() , Sarvghadi F, Beyranvand MR
, Sarvghadi F, Beyranvand MR ![]()
Received 2 December 2018
Accepted for publication 5 March 2019
Published 30 April 2019 Volume 2019:12 Pages 581—587
DOI https://doi.org/10.2147/DMSO.S196729
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Maryam Vasheghani,1 Farzaneh Sarvghadi,2 Mohammad Reza Beyranvand3
1Endocrinology & Metabolism Department, School of Medicine, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 2Endocrinology & Metabolism Department, Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran; 3Interventional Cardiology, Department of Cardiology, Taleghani Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Introduction: Cardiac autonomic neuropathy (CAN) is one of major complications of diabetes mellitus (DM) that increases the risk of cardiovascular disorders, abnormal ventricular depolarization with poor prognosis as well as increased mortality and morbidity. Indeed, CAN has close relation with blood glucose level in diabetic patients. We investigated the relation of CAN with diabetes control.
Materials and methods: Totally, 115 diabetic patients (mean age 50.87±13.90 years old; 78 females) underwent study. All patients had DM and cardiac sinus rhythm. Nobody had sickness affecting cardiac rhythm and blood pressure. In addition, they did not take drugs that had effect on blood pressure, cardiac rhythm, and QT interval. Forty-six patients had tight and 69 patients had uncontrolled DM according to American Diabetes Association (ADA) criteria. The CAN was assessed based on heart rate variation during physical examination (at rest tachycardia and orthostatic hypotension) and standard Ewing’s tests (deep-breathing and laying-to-standing tests) with bedside continuous ECG recording. The P-value <0.05 is considered significant.
Results: Seventy-five patients (65.2%) had CAN. In patients with CAN, 13.9% were symptomatic and 51.3% were asymptomatic. Resting tachycardia and hypotension were found in 5.2%, 8.7% of patients, respectively. Abnormal deep-breathing and laying-to-standing tests were found in 73% and 71.3% of asymptomatic patients, respectively. CAN was more prevalence at uncontrolled DM (67.3% vs 63.7%) but the difference was not significant. The prevalence of CAN had direct association with duration of DM in both tight and uncontrolled groups (P<0.05). The mean of age, sex, and type of treatment had no association with CAN prevalence.
Conclusion: The prevalence of CAN, especially asymptomatic type, was high. Its prevalence was increased with prolonged duration of DM. But we did not find any relationship between CAN and glycemic control level.
Keywords: cardiac autonomic neuropathy, diabetes mellitus, glycemic control, diabetic autonomic neuropathy, Hb A1c, electrocardiogram
A Letter to the Editor has been received and published for this article.
A Response to Letter has been published for this article.
Background
One of the most common metabolic abnormalities with high morbidity and mortality rates around the world is diabetes mellitus (DM).1 It has chronic complications and involves various organs in body such as autonomic nervous system and cardiovascular system.1 The prevalence of cardiac autonomic neuropathy (CAN) in diabetic patients is about 10% in symptomatic cases and its prevalence reaches 100% in the asymptomatic cases with accurate methods such as radionuclide scan.2–4 The (CAN) without symptoms has high prevalence. It causes problems in sense of chest pain, changes in ischemic threshold, problems in ventricle systolic and diastolic function, increased chances of cardiac arrhythmia, changes in circadian rhythm of body blood pressure, cardiac events such as sudden death, infarction, exacerbation of silent myocardial ischemia and exercise intolerance.2–4This complication in anesthesia and surgery causes problems in insertion of tracheal tube, increased chance of pulmonary aspiration due to residual food in the stomach caused by gastroparesis, arrhythmia resistant to treatment, sudden cardiac arrest, and hypotension which is resistant to treatment. In addition, this complication has direct relationship with other diseases in diabetic patients such as small vessel disease in kidney, eye. Also, it can affect the nervous system and other organs such as digestive and genitourinary systems.5
The precise control of blood pressure, weight loss, treatment with hypotensive blood pressure anti-arrhythmic drugs, prevents the progression of these conditions.6 Also, the search for premature ventricular reperfusion, silent ischemia in patients with other risk factors for coronary artery disease prevents progression of this condition. Moreover, it will reduce the risk and complications of surgery and anesthesia before, during and after surgery. The diagnosis of autonomic neuropathy can be used to predict and diagnose other complications of diabetes such as gastroparesis which is difficult to diagnose.7
According to the lack of previous detailed investigations on this syndrome, this study aimed to identify the prevalence and relationship of cardiac autonomic neuropathy with blood glucose levels in diabetic patients.
Materials and methods
This study was a descriptive cross-sectional study which was performed on diabetic patients who referred to internal medicine or endocrine clinic of Loghman Hakim General Hospital, Tehran, Iran. All patients who referred to the two clinics during one year were entered into the study according to inclusion and exclusion criteria. Inclusion criteria: diabetic patients who have cardiac sinus rhythm and stable vital sign; exclusion criteria: presence of any symptoms of anemia, hypoxia, hypovolemia, sepsis, renal failure and other diseases that affect heart rhythm and orthostatic hypotension; Patients who take medications that affect cardiac rhythm, QT intervals and blood pressure eg: calcium channel blockers and beta receptors, except angiotensin converting enzyme inhibitors and angiotensin receptor blocking agent; anti-arrhythmic drugs and triangular antidepressants, phenothiazine
This research has been reviewed at the Ethics Committee of the Medicine Faculty of Shahid Beheshti University of Medical Sciences and has been approved in accordance with the Helsinki Statement. This research has been designed and implemented according to the recommendations of this committee.
After obtaining written consent, patients were interviewed and examined by an internal medicine resident. The first clinical exam was performed in a fasting state and other evaluations were conducted from 09:00 to 16:00, at least 2 hours after waking up.8,9 Weight was measured with a digital scale with 100 g accuracy with minimum clothes and height were measured with a metal stadiometer with a precision of 0.5 cm in standard standing position without shoes. Blood pressure was measured after 15 minutes of rest with a standard mercurial sphygmometer from the right hand in the sitting position. Then, 10 cc of venous blood was taken from the patient after 12 hours of fasting. All specimens were stored in Vacutainer’s single-use test tubes (KIMO brand, Italy) at −20 °C and tests were done at the end of each week. Blood glucose, total cholesterol, triglyceride, high and low density lipoprotein cholesterol were measured by enzymatic flowmetery (Random Kit, UK).
A questionnaire containing demographic information was completed. Then the blood pressure and heart rate of the right hand examined in lying down (15 minutes rest) and standing positions. Later on, the continuous electrocardiogram (ECG) was taken from each individual in two modes:4,10,11
- The patient breathed deeply 6 times per minute, and the ECG was taken continuously for 1 minute in supine position. The time of inspiration and expiration was marked on the ECG tape.
- The ECG was taken continuously for 1 minute in standing position.
The RR intervals were calculated based on the continuous ECG tape.
Body mass index (BMI) was calculated by dividing the weight (kg) by height (m).2
Diagnosis of diabetes was based on American Diabetes Association criteria.12 The patients were divided into two groups, patients with tight controlled DM for at least 1 year (HbA1c <7%, BS 2 hours post prandial <180 mg/dl, FBS <130 mg/dl) and uncontrolled DM (without one of the above criteria).
The CAN was diagnosed based on standard Ewing’s tests.4 There are five bed side tests for cardiovascular reflexes and patients scored based on 0 to 5. The definite CAN was diagnosed based on at least two abnormal tests.
The patients who had orthostatic hypotension or at rest tachycardia were considered symptomatic CAN.4
Ewing’s tests for diagnosis of CAN:4
Statistical analysis
All information recorded in the questionnaire. Independent t-test was used to compare the quantitative variables. Chi-squared test was used for qualitative variables. Simple regression analysis was used to determine the relation of blood glucose level with each quantitative parameters of CAN. SPSS Version 13.1 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis and P<0.05 was considered as a significant level of difference.
Result
During 1 year, 128 patients were examined, 8 patients were excluded from the study despite repeated follow-up because of incomplete tests and 5 patients were excluded due to incomplete ECGs. Finally, the data of 115 patients were analyzed. The mean ±SD age of the patients was 50.87±13.99 years (14–78 years). Of these, 32.2% were male and 67.8% were female. The mean ±SD duration of diabetes was 77.43±77.22 months (0 at least in newly diagnosed individuals and maximum 384 months). In these patients, 40% had tightly controlled DM and 60% had uncontrolled DM. In diabetic patients 61.7% received oral glucose-lowering tablets, 24.3% insulin, 2.6% combined treatments, 3.5% had only diet and 7.8% were not treated. There were no significant differences in age and sex in both groups (P=1 and P=0.16, respectively). The basic characteristics of the participants are listed in Table 1.
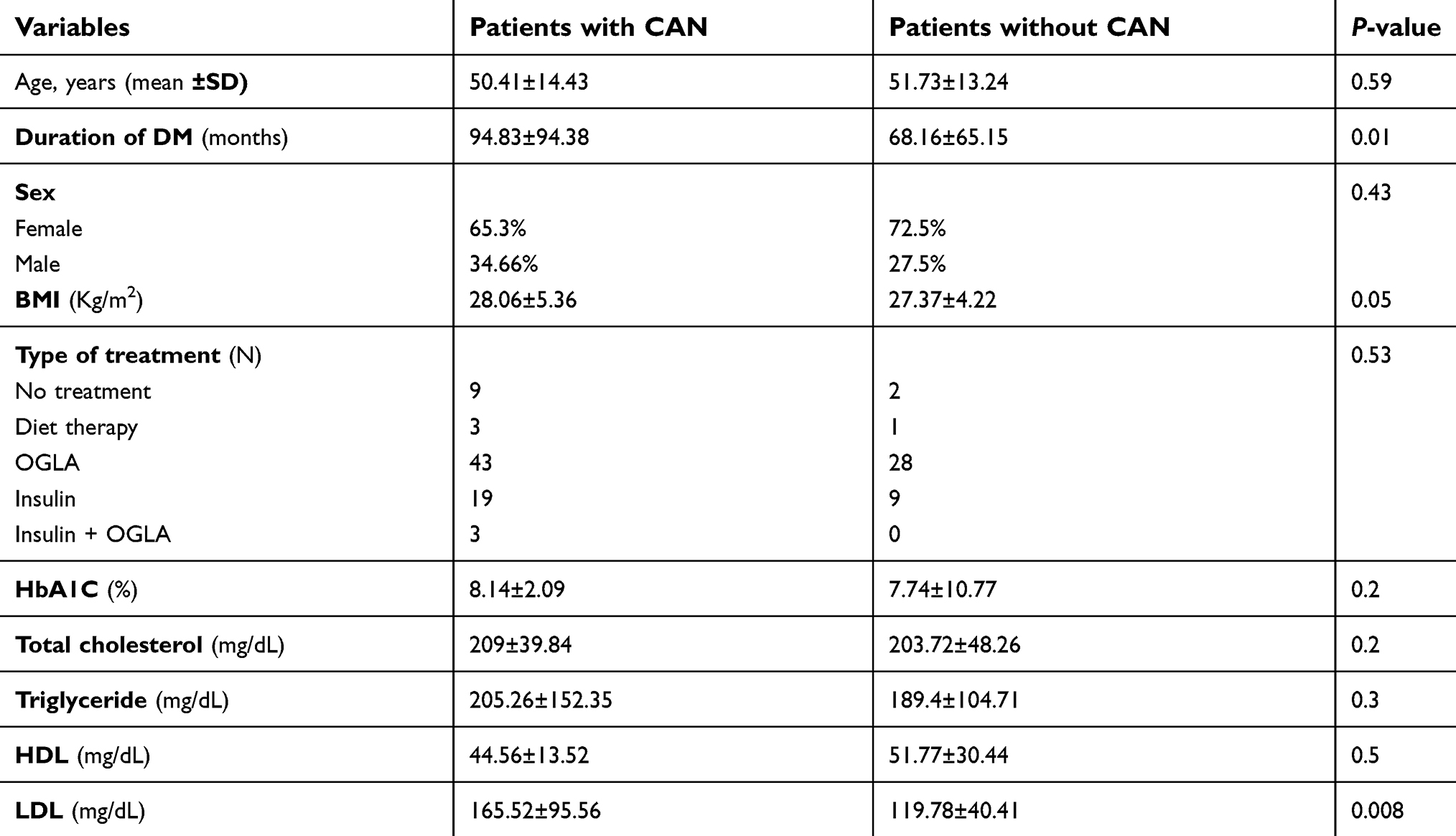 | Table 1 Characteristic of the study subjects in patients with and without CAN |
In total, 65.2% patients had CAN and 34.8% had no CAN. Sixteen patients (13.9%) had symptomatic CAN (with resting tachycardia or orthostatic hypotension ), and 59 patients (51.3%) had asymptomatic CAN. (5.2% at rest tachycardia; 8.7% orthostatic hypotension; 73% abnormal breathing test; 71.3% abnormal lying-to-standing test). Patients with and without CAN had no significant difference in age and sex (P=0.59 and P=0.43, respectively).
There was no significant difference between the two groups in terms of controlling diabetes (tightly controlled or uncontrolled DM) and type of treatment with CAN (P=0.68 and P=0.53, respectively).The mean ±SD duration of diabetes in people with CAN was higher than those without CAN, (P=0.01). (Table 2)
 | Table 2 Frequency of CAN in terms of diabetes control in subjects |
Discussion
In summary, the data of 115 diabetic patients with mean age of 50 years, which were 67.8% female, were studied. In these diabetic patients 40% had tightly controlled and 60% had uncontrolled DM at least for 1 year. About two thirds of patients had CAN. The number of asymptomatic patients was almost four times symptomatic individuals. Generally, the average age was lower in those with CAN. There were more male, and patients with tightly controlled DM in this group, but these differences were not significant. Duration of diabetes was longer in people with CAN, and this relationship was significant. There was no significant difference in age and sex in the two groups.
Neuropathy is the most prevalent complication of DM,13 and our study based on cardiovascular reflexes (Ewing’s tests), showed that CAN has a high prevalence (65.2%), which is often asymptomatic (51.3%). As reported in large studies, the incidence of CAN in diabetic patients can range from 17–90% in patients. For example, in patients with type 1 diabetes, an incidence of 27.5% and in patients with type 2 diabetes was 73%.14 The prevalence of CAN in this study was consistent with the overall incidence of CAN in other studies, like 68% in the review of Mendivil in the US in 2016.15
In this study, the incidence of symptomatic CAN was 13.9% on the basis of orthostatic hypotension and resting tachycardia. Symptomatic CAN sometimes has a high prevalence on the basis of the above criteria. The prevalence of this symptom in diabetics is 10% and increases with age to 16–20% which is consistent with our results.16,17 In one study, postural hypotension had a prevalence of around 46%.18,19
CAN prevalence increases with the duration of the disease. In this study, the duration of diabetes in people with CAN was higher than those without CAN, which is consistent with some previous studies. In many studies such as Andrei and Amorin study, there was a direct relationship between the incidence of neuropathy and the duration of diabetes. Of course, depending on the type of diabetes, this relationship sometimes varies. In type 2 diabetes, This complication occurred earlier than type 1 diabetes.20
If we use more diagnostic criteria and more precise instruments, the prevalence is higher.
The prevalence of CAN in precise methods such as MIBG scan and PET scan is high.20–22 We used a short-term continuous ECG. Its accuracy is less than 24-hour Holter monitoring of heart rate and blood pressure but is acceptable, noninvasive, and simple and can be done at the patient’s bedside. Its sensitivity is 93–100% and specificity 69–75% in different studies. Though all interviews and examinations have been performed by the researcher herself, she is an assistant in the Internal Medicine Department. Moreover, the disadvantage of these tests is that they require the patient’s cooperation or active participation, and are operator dependent.23 Even the newly published studies also used ECGs less than 10 seconds long and had similar results. In very short duration continuous ECG like 10 -second duration, you cannot measure frequency amplitude but you can measure time domain.24
Heart rate variability (HRV) decreases with age. Of course, in some studies, the relationship between HRV and age is U-shaped, that is, the heart rate rises from birth to age 20 and then decreases slightly until about 40 years. After that, it reaches the Plato level and rises again from about 75 years of age.25 In our study, no significant difference was seen between the two groups in terms of age and age groups at baseline characteristics. This eliminates the difference between the two groups and prevents the results from being altered due to age differences. The mean ±SD age for CAN patients was lower than those without CAN, but this was not statistically significant. Other studies have shown that CAN is not related to age.26 Although most studies showed a positive relationship between age and CAN prevalence. Part of this difference can be due to the age composition of the population studied. For example, in our study, 15% of people were aged less than 40 years old and 9% of those were aged over 70 years old.
There is a difference in HRV between men and women, although the difference between the two sexes decreases with age. The mechanism of making the difference between the two sexes is not precisely defined, but factors such as genetics, sex hormones, and underlying differences in cardiovascular parameters such as differences in baseline blood pressure are considered effective.27–29 In our study like the Verona Newly Diagnosed Type 2 Diabetes Study (VNDS),29 patients with CAN (either with precise control, or uncontrolled DM), the number of females has been higher than males, but this difference was not significant.
The prevalence of CAN was 53.8% in uncontrolled and 46.2% in patients with tightly controlled DM, but this difference was not statistically significant. The controlling of diabetes can prevent or delay the onset of microvascular complications and the cumulative incidence of diabetic neuropathy has a direct relationship with HbA1c level.30 These differences can be due to several reasons that may affect the results such as criteria for tight control diabetes, duration of diabetes , metabolic memory, sample size, and diagnostic method for CAN.
We selected patients with HbA1c <7%, BS 2 hours post prandial <180 mg/dL, FBS <130 mg/dL for at least 1 year as tightly controlled DM.
First, different criteria have been used to define precise control of diabetes in various studies.31
Second, because HbA1c only shows the status of the last 3 months, and unfortunately most of our patients lack regular and valid medical history to determine the long-term status of diabetes control. The above criterion only indicates proper glucose control over the past year and does not indicates long-term control of DM in patients.
Third, the metabolic memory may also affect the results.32
The sample number of our study is low with shorter follow-up period compared to large studies and was conducted only in a single center.
We have used physical examination (pulse rate and blood pressure measurement in supine and standing positions) and continuous ECG for CAN diagnosis. At each stage of the diagnostic tests, a continuous ECG was taken for at least 1 minute.
Although the continuous ECG has a lower diagnostic accuracy than the 24-hour Holter monitoring, it is an easy, accessible, available and inexpensive test which can be done at the patient’s bedside. This test has an appropriate sensitivity and specificity for the diagnosis of autonomic neuropathy. Several studies have shown the acceptable sensitivity and specificity of these tests, even when they are performed at a shorter time than 24 hours (for 10 seconds to 20 minutes).29,33,34
We used five tests for CAN diagnosis in all participants but other studies used two tests for suspicious participants who have had dizziness in standing, diarrhea at nights and incomplete bladder emptying.34–36
We did not evaluate other risk factors of neuropathy like hypertension, smoking, etc.37 These factors may have affected our results.
This study had some limitation. First, this study had small sample size. Second a tightly controlled criterion for DM was considered for the 1 year, while long-term blood glucose control was unclear. Third, we did not evaluate other risk factors of neuropathy.
This study has several strengths. First, the examinations and diagnostic procedures were performed by a single person who increases the internal validity of tests. Second, all tests were performed throughout the day to eliminate circadian changes in heart rate variability and blood pressure. Third, we used five tests for CAN diagnosis. Forth, in this research we used a cheap, accessible, easy and affordable tool at the patient’s bedside. In remote and deprived areas that do not have access to advanced facilities such as cardiac Holter monitoring, all physicians and technicians can easily apply this technique and interpret its results.
In conclusion, this study showed CAN has high prevalence, especially asymptomatic CAN and its prevalence is increased with prolongation of disease. We did not find any relationship between CAN and glycemic control level. Because of the cross-sectional study it was not apparent how much time DM was controlled and we could not clarify long-term glycemic control. Cardio vascular reflexes (Ewing’s Test) seem to be the primary technique in evaluation of CAN due to its low cost, easy use at the patient's bedside with good interindividual reproducibility. Finally, the prevalence of CAN in different studies varies depending on the definition, diagnostic criteria, population of the study, diagnostic methods, duration of the disease, stage of disease, and so on.
Ethics approval and consent to participate
This research has been reviewed at the Ethics Committee of the Faculty of Medicine of Shahid Beheshti University of Medical Sciences and has been approved in accordance with the Helsinki Statement. This research has been designed and implemented according to the recommendations of this committee.
Consent for publication
The research subjects were interviewed and examined after obtaining written consent.
Availability of data and material
The data are available from the authors upon reasonable request.
Acknowledgments
The authors thank the colleagues of the Endocrine and Heart clinics who helped them with this research. They are also grateful to the patients who collaborated on this project. They appreciate Dr. Habib Emami, epidemiologist, who helped in data reanalysis and manuscript edition.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Polonsky KS, Burant CF. Chapter 31, type 2 diabetes mellitus. In: Williams Textbook of Endocrinology.
2. Vinik AI, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007;115(3):387–397. doi:10.1161/CIRCULATIONAHA.106.634949
3. Vinik AI, Erbas T. Diabetic autonomic neuropathy. Handb Clin Neurol. 2013;117:279–294. doi:10.1016/B978-0-444-53491-0.00022-5
4. Vinik AL, Erbas T. Recognizing and treating diabetic autonomic neuropothy. Cleve Clin J Med. 2001;68(11):
5. Fleisher LA, Mythen M. Chapter 39, anesthetic implications of concurrent diseases. In: Miller’s Anesthesia.
6. Somers VK. Chapter 89, Cardiovascular manifestations of autonomic disorders. In: Elsevier & Saunders, Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine.
7. Asakawa H, Onishi M, Hayashi I, Fukuda A, Tokunaga K. Comparison between coefficient of R-R interval variation and gastric emptying in type 2 diabetes mellitus patients. J Gastroenterol Hepatol. 2005;20(9):1358–1364. doi:10.1111/j.1440-1746.2005.04025.x
8. Boudreau P, Yeh WH, Dumont GA, Boivin DB. Circadian variation of heart rate variability across sleep stages. Sleep. 2013;36(12):1919–1928. doi:10.5665/sleep.3230
9. Corino VD, Platonov PG, Enger S, Tveit A, Ulimoen SR. Circadian variation of variability and irregularity of heart rate in patients with permanent atrial fibrillation: relation to symptoms and rate control drugs. Am J Physiol Heart Circ Physiol. 2015;309(12):H2152–7. doi:10.1152/ajpheart.00300.2015
10. Dimple KN, Singh H, Sandhu PK, Kaur S, Arora A. Heart rate variability as an early index of autonomic neuropathy in diabetics. Pak J Physiol. 2015;11(4):12–16.
11. Flynn AC, Jelinek HF, Smith M. Heart rate variability analysis: a useful assessment tool for diabetes associated cardiac dysfunction in rural and remote areas. Aust J Rural Health. 2005;13(2):77–82. doi:10.1111/j.1440-1854.2005.00658.x
12.
13. Maffi P, Secchi A. The burden of diabetes: emerging. Data Dev Ophthalmol. 2017;60:1–5. doi:10.1159/000459641
14. Bissinger A. Cardiac autonomic neuropathy: why should cardiologists care about that? J Diabetes Res. 2017;2017:5374176. doi:10.1155/2017/5374176
15. Mendivil CO, Kattah W, Orduz A, Tique C, Cárdenas JL, Patiño JE. Neuropad for the detection of cardiovascular autonomic neuropathy in patients with type 2 diabetes. J Diabetes Complications. 2016;30(1):93–98. doi:10.1016/j.jdiacomp.2015.10.004. Witte DR, Tesfaye S, Chaturvedi N, Eaton SE, Kempler P, Fuller JH; EURODIAB Prospective Complications Study Group. Risk factors for cardiac autonomic neuropathy in type 1 diabetes mellitus. Diabetologia. 2005 Jan;48(1):164-71. PMID: 15619072; doi: 10.1007/s00125-004-1617-y.
16. Pop-Busui R, Low PA, Waberski BH, et al. Effects of prior intensive insulin therapy on cardiac autonomic nervous system function in type 1 diabetes mellitus: the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications study (DCCT/EDIC). Circulation. 2009;119(22):2886–2893. doi:10.1161/CIRCULATIONAHA.108.837369
17. Jaiswal M, Divers J, Urbina EM, et al. Cardiovascular autonomic neuropathy in adolescents and young adults with type 1 and type 2 diabetes: the SEARCH for diabetes in youth cohort study. Pediatr Diabetes. 2018;19(4):680–689. doi:10.1111/pedi.12633
18. Oduwole OA, Adeniyi OF, Esezebor CI, Ekure E, Fajolu IB, Renner JK. Postural hypotension in type 1 diabetes: the influence of glycemic control and duration of illness. Niger J Clin Pract. 2014;17(2):140–144. doi:10.4103/1119-3077.127421
19. Andrei CB, Amorin RP. Diabetic neuropathy prevalence and its associated risk factors in two representative groups of type 1 and type 2 diabetes mellitus patients from Bihor county. Maedica (Buchar). 2018;13(3):229–234. doi:10.26574/maedica.2018.13.3.229
20. Fisher VL, Tahrani AA. Cardiac autonomic neuropathy in patients with diabetes mellitus: current perspectives. Diabetes Metab Syndr Obes. 2017;10:419–434. doi:10.2147/DMSO.S129797
21. Pappachan JM, Sebastian J, Bino BC, et al. Cardiac autonomic neuropathy in diabetes mellitus: prevalence, risk factors and utility of corrected QT interval in the ECG for its diagnosis. Postgrad Med J. 2008;84(990):205–210. doi:10.1136/pgmj.2007.064048
22. Tannus LR, Drummond KR, Clemente EL, da Matta Mde F, Gomes MB,
23. Jacobson AF, Senior R, Cerqueira MD, et al. ADMIRE-HF Investigators. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55(20):2212–2221. doi:10.1016/j.jacc.2010.01.014
24. Van Den Berg ME, Rijnbeek PR, Niemeijer MN, et al. Normal values of corrected heart-rate variability in 10-second electrocardiograms for all ages. Front Physiol. 2018;9:424. doi:10.3389/fphys.2018.00424
25. Hayano J, Ohashi K, Yoshida Y, et al. Increase in random component of heart rate variability coinciding with developmental and degenerative stages of life. Physiol Meas. 2018;39(5):054004. doi:10.1088/1361-6579/aac007
26. Röhling M, Strom A, Bönhof GJ, Roden M, Ziegler D. Cardiorespiratory fitness and cardiac autonomic function in diabetes. Curr Diab Rep. 2017;17(12):125. doi:10.1007/s11892-017-0959-z
27. Voss A, Schroeder R, Heitmann A, Peters A, Perz S. Short-term HRV–influence of gender and age in healthy subjects. PLoS One. 2015;10(3):e0118308. doi:10.1371/journal.pone.0118308
28. Paniccia M, Verweel L, Thomas S, et al. Heart rate variability in healthy non-concussed youth athletes: exploring the effect of age, sex, and concussion-like symptoms. Front Neurol. 2018;8:753. doi:10.3389/fneur.2017.00753
29. Zoppini G, Cacciatori V, Raimondo D, et al. Prevalence of cardiovascular autonomic neuropathy in a cohort of patients with newly diagnosed type 2 diabetes: the Verona Newly Diagnosed Type 2 Diabetes Study (VNDS). Diabetes Care. 2015;38(8):1487–1493. doi:10.2337/dc15-0081
30. Moţăţăianu A, Maier S, Bajko Z, Voidazan S, Bălaşa R, Stoian A. Cardiac autonomic neuropathy in type 1 and type 2 diabetes patients. BMC Neurol. 2018;18(1):126. doi:10.1186/s12883-018-1125-1
31. Nathan DM,
32. Misra A, Bloomgarden Z. Metabolic memory: evolving concepts. J Diabetes. 2018;10(3):186–187. doi:10.1111/1753-0407.12622
33. Sacre JW, Jellis CL, Marwick TH, Coombes JS. Reliability of heart rate variability in patients with type 2 diabetes mellitus. Diabet Med. 2012;29(7):e33–e40. doi:10.1111/j.1464-5491.2011.03557.x
34. Imam MH, Karmakar CK, Khandoker AH, Jelinek HF, Palaniswami M. Heart rate independent QT variability component can detect subclinical cardiac autonomic neuropathy in diabetes. Conf Proc IEEE Eng Med Biol Soc. 2016;2016:928–931. doi:10.1109/EMBC.2016.7590853
35. Vinik AI, Nevoret ML, Casellini C, Parson H. Diabetic neuropathy. Endocrinol Metab Clin North Am. 2013;42(4):747–787. doi:10.1016/j.ecl.2013.06.001
36. Schnell O, Cappuccio F, Genovese S, Standl E, Valensi P, Ceriello A. Type 1 diabetes and cardiovascular disease. Cardiovasc Diabetol. 2013;12:156. doi:10.1186/1475-2840-12-156
37. Serhiyenko VA, Serhiyenko AA. Cardiac autonomic neuropathy: risk factors, diagnosis and treatment. World J Diabetes. 2018;9(1):1–24. doi:10.4239/wjd.v9.i1.1
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.