Back to Journals » Psychology Research and Behavior Management » Volume 19
The Association Between Body Image and Depression: Historical Evolution and Recent Research Progress
Received 1 January 2026
Accepted for publication 8 June 2026
Published 10 June 2026 Volume 2026:19 593127
DOI https://doi.org/10.2147/PRBM.S593127
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Yan-Min Xu,1,2 Bao-Liang Zhong1
1Department of Psychiatry, Wuhan Mental Health Center, Wuhan, Hubei, People’s Republic of China; 2Department of Psychiatry, Wuhan Hospital for Psychotherapy, Wuhan, Hubei, People’s Republic of China
Correspondence: Bao-Liang Zhong, Department of Psychiatry, Wuhan Mental Health Center, No. 89 Gongnongbing Road, Jiang’an District, Wuhan, Hubei, 430012, People’s Republic of China, Email [email protected]
Purpose: This narrative review synthesizes the historical evolution and current evidence on the association between body image and depression, with emphasis on conceptual shifts, bidirectional pathways, heterogeneity across populations, and implications for prevention and treatment.
Patients and methods: PubMed was searched using title-relevant body image terms (eg, body image, body dissatisfaction, body image disturbance) combined with depress* to capture depression-related variants. No date or language restrictions were applied. After screening, 266 records published from 1972 to 2026 were included. The search was performed on May 5, 2026.
Results: Evidence across five decades indicates that negative body image, especially body dissatisfaction, is consistently associated with depressive symptoms across cultures, developmental stages, and clinical settings. The field has evolved from early clinical observations to sociocultural and longitudinal research, and more recently to transdiagnostic, digital media, symptom network, and genetically informed approaches. Longitudinal and twin-cohort studies suggest that body dissatisfaction may prospectively predict depression, while depression may in turn exacerbate body image problems. Subjective appearance evaluation appears more strongly related to depressive outcomes than objective indices such as BMI. Proposed mechanisms include self-objectification, social comparison, cognitive biases, rumination, low self-esteem, and reduced engagement in rewarding activities. Interventions targeting body image, including CBT and dissonance-based programs, improve body image and may also reduce depressive symptoms.
Conclusion: Body image is a modifiable and clinically meaningful factor in depressive risk and maintenance. Integrating body image assessment and targeted intervention into depression prevention and care may help interrupt reciprocal cycles of dissatisfaction, shame, rumination, and withdrawal.
Keywords: body image, body dissatisfaction, depression, longitudinal studies, sociocultural models, cognitive behavioral therapy
Introduction
Depression represents one of the most significant public health challenges of the 21st century, characterized by persistent sadness, anhedonia, and functional impairment.1–4 The World Health Organization identifies depression as a leading contributor to the global burden of disease, contributing to elevated mortality rates, reduced economic productivity, and severe decrements in quality of life.5–7 Given the chronic and relapsing nature of depression, identifying modifiable risk factors is a priority for public health intervention.
Among these risk factors, body image—defined as the multidimensional construct of people’s thoughts, feelings, and perceptions regarding their physical appearance—has emerged as a critical variable.8 Historically confined within the domain of eating disorder research, body image is now recognized as a transdiagnostic factor with far-reaching implications for general mental health.9 The ubiquity of “normative discontent”, a term coined to describe the common experience of body dissatisfaction,10 underscores its potential as a lever for widespread preventative strategies.
Recent empirical evidence suggests that body image disturbance is not merely a symptom of depression but a potent precursor.11 Longitudinal data indicate that body dissatisfaction during adolescence significantly predicts the onset of major depressive episodes in adulthood, independent of other risk factors.7 Consequently, addressing body image offers a preventative avenue distinct from traditional depression treatments, potentially alleviating the disease burden by intercepting the trajectory of distress before it crystallizes into clinical psychopathology. Beyond its theoretical relevance, clarifying the role of body image in depression also carries broader clinical and public health significance: it may inform earlier identification of at-risk individuals, support prevention efforts, reduce downstream healthcare burden, and guide stigma-reduction and psychoeducational initiatives targeting harmful appearance-related norms.
While the link between body image and depression is well-established, the nature of this association is complex and evolving. Previous reviews have often focused narrowly on specific populations (eg, adolescent girls) or specific disorders (eg, eating disorders).12–14 However, the landscape of body image research has shifted dramatically with the advent of social media, the rise of the “body neutrality” movement, and the introduction of sophisticated statistical methodologies like network analysis.15,16
Furthermore, recent years have seen a proliferation of research in non-Western contexts and diverse clinical populations, challenging the universality of earlier theoretical models.17,18 A contemporary synthesis is required to integrate these disparate strands of research—ranging from genetic twin studies to digital interventions—into a cohesive narrative. This review updates the field by incorporating findings from recent studies, providing a critical analysis of the historical trajectory, current mechanistic understanding, and clinical implications of the body image-depression relationship. In response to evolving research trends, this synthesis delineates the body image-depression association across three levels of certainty: well-established empirical foundations, emerging but uncertain frontiers (eg, digital-media dynamics and network-analytic insights), and persistent understudied gaps.
This narrative review aims to clearly define and operationalize body image and related constructs within the context of mental disorders, while tracing how research on the body image-depression link has evolved from the 1970s to the present. It further synthesizes current evidence on the bidirectional and potentially causal relationships between these constructs, and examines how this association may vary by gender, across the lifespan, and within specific clinical populations. In addition, the review explores key psychological mechanisms and theoretical frameworks—such as Objectification Theory, the Tripartite Influence Model, and cognitive-behavioral accounts of appearance-related self-evaluation, shame, rumination, and avoidance—while also considering more recent network-analytic approaches that complement these models by identifying symptom-level central and bridge processes linking body image disturbance with broader affective and interpersonal psychopathology. The review further evaluates the effectiveness of interventions that target body image in reducing depressive symptoms.
Methods
This narrative review was based on a comprehensive literature search conducted exclusively in PubMed on May 5, 2026. The search strategy combined body image-related constructs with a truncated depression term to capture depression-, depressive-, and related variants. The full PubMed search string was as follows (Table 1): ((“body image” [Title/Abstract] OR “body dissatisfaction” [Title/Abstract] OR “body image disturbance” [Title/Abstract]) AND depress* [Title/Abstract]). No restrictions on publication date or language were applied.
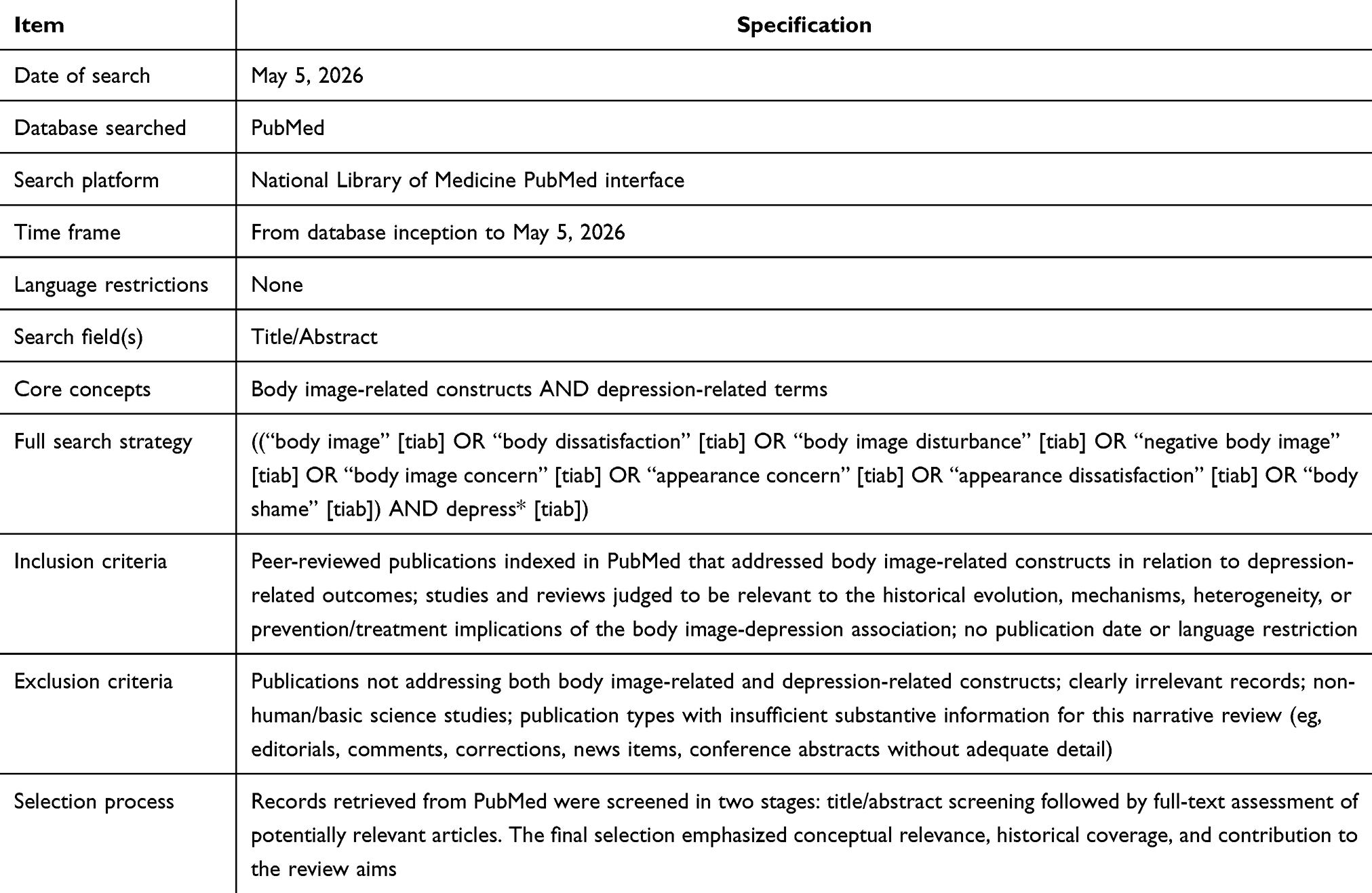 |
Table 1 Summary of the Literature Search Strategy within PubMed |
Records retrieved from PubMed were screened in two stages. First, titles and abstracts were reviewed for relevance. Publications were considered eligible if they directly addressed body image-related constructs (eg, body image, body dissatisfaction, or body image disturbance) in relation to depression-related outcomes (eg, depression, depressive symptoms, or depressive disorder), and were judged to contribute substantively to the historical development, mechanisms, population heterogeneity, or prevention/treatment implications of this association. Original studies, review articles, and other peer-reviewed papers with clear conceptual relevance were eligible for inclusion.
Records were excluded if they did not address both body image-related and depression-related constructs, were clearly irrelevant to the review question, were non-human or basic science studies, or were publication types with insufficient substantive content for the purposes of this narrative review (eg, editorials, comments, corrections, news items, or conference abstracts without adequate information). We initially identified 3176 records in PubMed using the above search strategy. Potentially relevant full texts were then assessed for final inclusion. Because this was a narrative review rather than a systematic review, our aim was to provide broad, pragmatic coverage rather than to conduct an exhaustive multi-database search and include all eligible studies. PubMed was selected as it indexes the majority of relevant biomedical and mental health literature, sufficiently meeting the needs of this descriptive synthesis. After screening, 274 representative records published between 1972 and 2026 (Supplementary file 1), covering different eras and key thematic areas, were included in the final narrative synthesis.
Body Image and Related Concepts
Body image is a multidimensional construct encompassing perceptual, affective, cognitive, and behavioral components that interact dynamically.10 The perceptual dimension concerns the accuracy of body size estimation; While body image distortions were historically examined in eating disorders, they often emerge in depressive states when pervasive negative cognitive biases shape self-perception.19 The affective dimension captures the emotional valence attached to one’s body—such as shame, anxiety, disgust, or pride—and is most proximally linked to depressive affect, given its overlap with low self-worth, hopelessness, and heightened self-criticism.20 The cognitive dimension refers to the beliefs, assumptions, and evaluative thoughts individuals hold about their appearance, including the internalization of thinness or muscularity ideals and the extent to which self-esteem is contingent on appearance; it reflects the degree of salience and personal investment placed on appearance as a basis for identity and social value.21 Finally, the behavioral dimension includes strategies to monitor, modify, or avoid the body (eg, body checking or social avoidance), which can reinforce appearance-based threat appraisal and social withdrawal—processes that map onto core maintenance pathways in depression.22
Within this framework, several constructs require careful differentiation.23 Body dissatisfaction is the most frequently assessed predictor in research linking body image to depression and typically denotes a negative evaluation of size, weight, or shape. It operates as a chronic psychosocial stressor that reliably correlates with depressive symptoms through self-criticism and perceived social rejection.11,24 In contrast, body appreciation—rooted in positive psychology—represents an active, affirmative orientation characterized by acceptance, respect, and protective self-care; it is not simply the absence of dissatisfaction but a qualitatively distinct stance that confers resilience by supporting self-compassion and reducing appearance-based rumination.25,26 It is also essential to distinguish normative dissatisfaction from Body Dysmorphic Disorder, a severe clinical condition marked by obsessive preoccupation with perceived defects.27 Crucially, the literature consistently underscores the distinction between subjective body image and objective indices such as Body Mass Index (BMI). Depressive symptoms are more strongly predicted by perceived appearance evaluation and dissatisfaction than by actual weight status, highlighting that perception and meaning-making—rather than physiology alone—are central to understanding affective risk.28
Historical Evolution of Research on Body Image and Depression
1970s and 1980s: The Era of Clinical Correlation
During the 1970s and 1980s, research on body image and depression was largely clinically oriented and relied heavily on cross-sectional designs, with body image most often examined in the context of major medical events or severe psychopathology. Early medical-model studies focused on populations experiencing visible bodily change—such as individuals undergoing mastectomy, living with extensive burns, or adapting to other disfiguring injuries—and consistently suggested that depressive symptoms were shaped not only by pain or disability but also by disruptions to self-perception, identity, and social confidence. Conceptually, many scholars interpreted body dissatisfaction through the lens of Beck’s cognitive theory of depression, treating negative appearance-related beliefs as one manifestation of the broader “negative cognitive triad” rather than as an independent construct with its own developmental trajectory.29 At the same time, as anorexia nervosa and bulimia nervosa became increasingly visible in psychiatric research, “body image disturbance” was formalized as a core feature of eating disorders;30 however, it remained largely siloed within that literature and was only intermittently connected to depression in non–eating-disorder populations. Overall, this period positioned body image concerns primarily as a correlational clinical feature—often secondary to depression or other diagnoses—rather than as a candidate risk factor in its own right.
1990s: Sociocultural Models and Longitudinal Design
In the 1990s, the field pivoted toward understanding body dissatisfaction as a widespread phenomenon in the general population and increasingly framed it as a socioculturally patterned experience rather than a rare clinical symptom. This decade produced influential theoretical accounts that linked appearance concerns to social norms and gendered pressures, most notably Objectification Theory, which articulated how persistent surveillance and evaluation of women’s bodies could foster self-objectification, shame, and emotional distress.31 In parallel, the Tripartite Influence Model formalized peers, family, and media as key socialization agents transmitting appearance ideals, proposing that internalization of these ideals and appearance-based comparison were proximal pathways to dissatisfaction.32 Methodologically, researchers began to adopt more rigorous longitudinal designs to clarify temporal ordering, which proved consequential for theory: prospective studies in adolescents, particularly among girls, provided early evidence that body dissatisfaction could precede and predict subsequent depressive symptoms and even the onset of major depression.33 This challenged the earlier assumption that negative body evaluation was merely a byproduct of depressed mood and helped reposition body image as a potentially primary vulnerability factor, inviting greater attention to mechanisms, developmental timing, and prevention.
2000s and 2010s: Complexity, Digital Media, and Transdiagnostic Views
From the 2000s into the 2010s, research increasingly emphasized complexity—both in the lived experience of body image and in the analytic models used to study it—while cultural shifts, especially the expansion of digital media, reshaped the landscape of appearance pressures. The rise of social media introduced interactive and self-referential dynamics (eg, constant comparison to peers, curated self-presentation, “selfie” practices, and photo editing) that amplified body surveillance and appearance-based self-worth, thereby offering plausible, behaviorally specific routes to depressive symptoms beyond those observed with traditional media. At the same time, scholars began to adopt more explicitly transdiagnostic perspectives, treating body image disturbance as a mechanism relevant not only to eating disorders but also to depression and anxiety, and exploring how it could contribute to patterns of comorbidity through shared processes such as rumination, social withdrawal, and self-criticism. The empirical base also diversified: studies expanded beyond predominantly White adolescent female samples to include men (with greater attention to muscularity ideals), older adults (highlighting aging-related appearance concerns), and culturally diverse groups, prompting refinements of sociocultural models in non-Western contexts. Collectively, this era framed body image not as a narrow symptom cluster but as a broad psychosocial domain with multiple pathways to affective distress, shaped by both offline and online interpersonal environments.
2020s to Present: Network Analysis and Bio-Psychosocial Integration
In the 2020s, the literature has increasingly moved toward high-resolution models of comorbidity and a more integrated biopsychosocial account of how body image and depression intersect. Network analytic approaches have gained traction by shifting the focus from broad latent constructs to specific symptom-to-symptom connections. Importantly, this approach does not replace earlier sociocultural or cognitive-behavioral theories; rather, it helps operationalize them at a finer level by showing which concrete experiences may function as central or bridge processes linking appearance-related distress to broader psychopathology.15,34–39 For example, network studies in eating-disorder samples have identified affective symptoms, interpersonal functioning, interoceptive awareness, ineffectiveness, and drive for thinness as especially central components, while anorexia nervosa networks have highlighted depression, anxiety, interpersonal sensitivity, and ineffectiveness as key nodes linked to drive for thinness, with BMI itself appearing less central.40,41 Such findings suggest that body-image-related risk is embedded in a broader system of emotional, interpersonal, and self-evaluative processes rather than operating through a single linear pathway. Alongside these methodological advances, emerging genetically informed and developmental studies have begun to examine whether shared heritable liability and gene-environmentnterplay contribute to both body dissatisfaction and depression, complementing long-standing psychological explanations with evidence for biological vulnerability.7 Importantly, the field has also broadened beyond deficit-focused measurement toward protective and resilience-oriented constructs, including positive body image, body neutrality, and functionality appreciation, which are increasingly evaluated as intervention targets that may reduce depressive symptoms by enhancing self-compassion, reducing appearance-contingent self-worth, and supporting engagement in valued activities. Taken together, contemporary work is characterized by greater precision about mechanisms, greater attention to heterogeneity across individuals and contexts, and a stronger emphasis on translating theory into scalable prevention and treatment strategies.
Recent Research Progress: The Bidirectional Relationship
Body Image as a Predictor of Depression
A growing body of longitudinal evidence indicates that negative body image—particularly body dissatisfaction—prospectively predicts increases in depressive symptoms, supporting the view that appearance-related self-evaluation can function as an antecedent risk factor rather than merely a correlate of low mood. Genetically informed designs, including large twin-cohort studies, further suggest that this association reflects both shared heritable liability and environmentally mediated pathways, consistent with a developmental process in which early body dissatisfaction heightens vulnerability to later depression.7 Importantly, research repeatedly shows that subjective body evaluation is more strongly tied to depressive outcomes than objective indices such as BMI: individuals who perceive themselves as unattractive or overweight report higher depressive symptoms regardless of measured weight status, underscoring the primacy of appraisal and self-meaning over physiology.28 Mechanistically, the prospective link is frequently explained by downstream processes such as reduced global self-esteem and increased rumination; negative body-related evaluations may generalize into broader self-criticism and hopelessness, thereby amplifying depressive affect and creating a cognitive–affective pathway from body dissatisfaction to depression.
Depression as a Predictor of Negative Body Image
Conversely, depression may actively shape and worsen body image through mood-congruent cognitive processing and depression-related behavioral changes, even in the absence of substantial physical transformation. Depressive states are characterized by attentional and interpretive biases that preferentially amplify negative appearance cues—such as fixating on perceived flaws, discounting positive feedback, and construing ambiguous social signals as appearance-related criticism—thereby fostering a more globally negative body evaluation. In parallel, behavioral sequelae of depression (eg, anhedonia-driven inactivity, disrupted sleep, diminished self-care, and changes in appetite or eating patterns) can produce bodily sensations of lethargy or “heaviness” and, for some individuals, weight change, both of which may be interpreted as confirming negative self-beliefs. Population-based cohort analyses further illustrate that while higher BMI can be associated with later depressive symptoms, this relationship is often partially mediated by the emergence or intensification of body dissatisfaction, highlighting how objective physical states may become psychologically consequential primarily when filtered through negative self-perception.42
The Reciprocal Cycle Between Body Image and Depression
Taken together, these pathways converge into a reciprocal, self-reinforcing cycle in which body dissatisfaction and depression mutually exacerbate one another over time. Negative body image can erode self-worth, increase self-focused attention, and promote avoidance of social and rewarding activities, thereby intensifying isolation and reducing access to protective interpersonal experiences—core conditions that maintain depressive symptoms. Depression, in turn, deepens negative self-schemata and depletes cognitive and emotional resources needed to resist sociocultural appearance pressures, making individuals more susceptible to comparison, self-objectification, and escalating dissatisfaction. Recent symptom-level approaches, including network analyses, provide a useful framework for clarifying these dynamics by identifying central and potentially bridging processes that connect body image disturbance to depressive symptom clusters.15,36–38 Such work suggests that body-image-related distress may be linked to depression not only through broad mediators such as self-esteem or rumination, but also through more specific symptom-level pathways involving affective distress, interpersonal sensitivity, shame, ineffectiveness, and avoidance. This extends traditional reciprocal or mediation-based accounts by showing which concrete symptom constellations may sustain the linkage over time and therefore represent more precise intervention targets.
Body Image-Depression Link: Demographic and Population Differences
Gender Differences
Gender shapes both the content of body image concerns and the pathways through which they relate to depression. Across many contexts, women and girls tend to report higher levels of body dissatisfaction alongside higher rates of depressive symptoms, a pattern often attributed to persistent sociocultural pressures surrounding the thin ideal, appearance-based social evaluation, and heightened self-objectification.31 In this framework, body image becomes a salient domain for self-worth, such that dissatisfaction more readily generalizes into global self-criticism, shame, and hopelessness—core affective and cognitive features of depression. At the same time, a growing literature highlights that men’s body image concerns are substantial, though historically underrecognized because they are less likely to be framed as “dissatisfaction with thinness” and more likely to center on muscularity, leanness, and strength (eg, the drive for muscularity or concerns consistent with muscle dysmorphia). When studies measure male-relevant domains—such as muscular dissatisfaction or perceived lack of size/definition—the association between negative body image and depression often appears comparable in magnitude to that observed in females.24 However, men may be less likely to present these concerns explicitly, instead expressing distress through somatic complaints, performance/fitness preoccupations, or functional impairment, which can obscure the role of body image in depressive vulnerability and maintenance.
Adolescents vs Adults
Developmental stage is another key moderator of the body image-depression link, with adolescence widely regarded as a period of heightened sensitivity.43,44 Puberty introduces rapid, highly visible bodily changes while peer dynamics and media exposure intensify appearance-based comparison, making body image unusually central to identity formation and social belonging. Cognitive-developmental factors—such as increased self-consciousness and sensitivity to perceived judgment—can amplify the emotional impact of perceived appearance shortcomings, thereby strengthening the pathway from dissatisfaction to depressive symptoms through mechanisms like rumination, social withdrawal, and diminished self-esteem. Yet body image concerns are not confined to youth: in adulthood and midlife, shifting roles, changing social expectations, and age-related physical transitions (eg, pregnancy, menopause, changes in weight distribution, skin elasticity, or perceived vitality) can reactivate or reshape appearance concerns, sometimes producing clinically meaningful distress and depressive symptoms. In later life, the focus may increasingly shift from aesthetics to body functionality—what the body can do rather than how it looks—such that functional decline, disability, or illness-related limitations can become central to body-related self-evaluation and, in turn, contribute to depression through loss of autonomy, reduced activity engagement, and altered self-identity.
Clinical and Specific Populations
Clinical contexts often intensify the body image-depression association by introducing rapid or uncontrollable bodily changes and by amplifying the social meaning attached to appearance. In perinatal populations, pregnancy and the postpartum period can involve marked changes in weight, shape, and physical comfort, and body dissatisfaction during this time has been consistently linked to perinatal depressive symptoms—particularly when “feeling fat”, concerns about weight retention, and perceived pressure to rapidly “return” to a pre-pregnancy body heighten shame and self-criticism.45 In oncology, especially breast cancer, body image can become a critical psychological “bridge” connecting depressive symptoms to broader quality-of-life outcomes, given that surgery, scarring, and treatment-related changes (eg, hair loss) may directly challenge femininity, sexuality, and embodied identity;9 these effects can be especially pronounced when the affected body part is tightly bound to cultural meanings of gender and attractiveness. Other conditions with visible phenotypic features, such as polycystic ovary syndrome (PCOS), may elevate depression risk through chronic appearance-related triggers (eg, hirsutism, acne, alopecia, weight gain), which can sustain social anxiety, stigma sensitivity, and depressive rumination while undermining positive body evaluation.46 Finally, sexual- and gender-minority populations—particularly transgender and non-binary individuals—often report elevated body dissatisfaction and depression, reflecting not only body-related distress that may be intertwined with gender dysphoria but also the additive burden of minority stress, discrimination, and harassment, which can intensify appearance-based vigilance and erode protective factors such as self-compassion and social support.47
Psychosocial Mechanisms and Theoretical Models Underlying the Body Image-Depression Relationship
Objectification Theory
Objectification Theory, proposed by Fredrickson and Roberts, offers a foundational account of why body image concerns may be especially consequential for depression in gendered social contexts.31 The theory argues that in cultures where women’s bodies are routinely scrutinized and evaluated, many girls and women learn to adopt an observer’s perspective on their own appearance, a process termed self-objectification.48 This internalized external gaze promotes habitual body surveillance—ongoing monitoring of how one looks rather than how one feels or what one can do—which can consume attentional resources and heighten vulnerability to negative affect. Because culturally prescribed ideals are often narrow and unattainable, surveillance frequently culminates in body shame, appearance anxiety, and a sense of failure that can generalize into broader self-devaluation.49 From this perspective, depressive symptoms emerge not simply from dissatisfaction per se, but from the chronic experience of the body as a site of judgment and social threat, which undermines perceived agency and self-efficacy.50 Recent empirical work has further suggested that positive body image may buffer these processes, yet high levels of self-objectification remain directly associated with depressive affect through pathways involving shame, helplessness, and reduced psychological resources for emotion regulation.51
The Tripartite Influence Model
The Tripartite Influence Model conceptualizes body image disturbance as a socially transmitted phenomenon shaped primarily by peers, parents, and media, and it has become one of the most widely used frameworks for explaining how appearance pressures translate into internal distress.52 In this model, sociocultural influences exert their effects largely through two proximal mechanisms: internalization of appearance ideals (eg, thinness, leanness, muscularity) and appearance-based social comparison.53 Once individuals adopt these standards as personal benchmarks, everyday exposure to idealized bodies—whether through interpersonal comments, family norms, or algorithm-driven media feeds—creates repeated opportunities for upward comparison and perceived inadequacy.54 Integrating this model with depression research has clarified a plausible sequence in which comparison and internalization predict body dissatisfaction, which then erodes self-esteem and increases rumination, thereby elevating depressive symptoms. Importantly, cross-cultural findings generally support the model’s basic architecture while indicating that the relative weight of each influence can vary by social ecology: for example, in more collectivist contexts, family norms and parental commentary may play a particularly strong role in shaping internalization, whereas in more individualist contexts, peer dynamics and media exposure may dominate.55 This flexibility has helped the model remain useful as appearance pressures evolve—from traditional advertising to highly interactive social media environments.
Cognitive and Attentional Biases
A complementary mechanistic account focuses on shared information-processing vulnerabilities in body image disturbance and depression, emphasizing how biased cognition can maintain both negative appearance evaluation and depressed mood.56 Individuals with elevated body dissatisfaction often show attentional bias toward perceived bodily flaws, alongside heightened attention to appearance ideals in others, which reinforces maladaptive self-schemata and makes negative self-evaluations more salient and “evidence-based” in the moment.57 In parallel, interpretation bias can lead ambiguous social cues—glances, whispers, delayed replies, neutral feedback—to be construed as appearance-related criticism, strengthening shame and promoting the ruminative self-focus characteristic of depressive states.58 These biases can operate automatically, shaping perception before deliberate reflection occurs, and may therefore be resistant to change through insight alone. Experimental paradigms (including eye-tracking and cognitive bias modification approaches) support the idea that biased attention and interpretation contribute to persistence of distress by repeatedly confirming negative beliefs and narrowing the person’s perceived options for coping.59 Clinically, this framework helps explain why some individuals remain distressed despite objective reassurance and why interventions that directly target attentional deployment, interpretation styles, and rumination may be particularly relevant in comorbid presentations.60
Psychological Network Findings on Symptom-Level Body Image-Depression Association
Network analysis is best understood as complementary to—rather than a replacement for—sociocultural and cognitive-behavioral models of the body image-depression relationship. Sociocultural frameworks such as Objectification Theory and the Tripartite Influence Model primarily explain where vulnerability comes from: repeated exposure to appearance ideals, social comparison, and body surveillance creates risk for body dissatisfaction and emotional distress. Cognitive-behavioral accounts, in turn, explain how this vulnerability is maintained through maladaptive appearance-related beliefs, shame, rumination, attentional and interpretive biases, avoidance, and low perceived effectiveness. Traditional vulnerability or mediation frameworks have been highly informative, but they typically model these associations at the level of broad constructs and along relatively linear pathways—for example, sociocultural pressure or ideal internalization leading to body dissatisfaction, which then contributes to low self-esteem, rumination, or depressive symptoms.
Network-analytic findings add a different level of explanation by examining how specific symptoms or experiences directly activate and reinforce one another. In eating-disorder samples, network studies have shown that central nodes include not only eating-disorder-specific features such as drive for thinness, but also affective symptoms, interpersonal functioning, interoceptive awareness, and ineffectiveness.40 In anorexia nervosa specifically, depression, anxiety, interpersonal sensitivity, and ineffectiveness appear to occupy especially central positions and are strongly connected with drive for thinness, whereas BMI itself is less central.41 These findings help integrate network analysis with existing theories: drive for thinness maps closely onto sociocultural accounts of ideal internalization, whereas ineffectiveness, interoceptive difficulties, affective distress, and interpersonal sensitivity align with cognitive-behavioral maintenance processes. Importantly, the network perspective suggests that body-image-related psychopathology is maintained not simply because one broad risk factor statistically predicts another, but because specific nodes belonging to body image, mood, and interpersonal systems may mutually reinforce one another within the same network.
Evidence from adjacent body-image-related conditions extends this point. A network perspective on body dysmorphic disorder and major depressive disorder illustrates how appearance-focused psychopathology and depressive psychopathology can be examined within a shared comorbidity structure,61 while network intervention analyses of cognitive-behavioral treatment for body dysmorphic disorder suggest that symptom change may unfold through identifiable pathways over time rather than through a single undifferentiated mediator.62 Community and nonclinical network studies similarly indicate that negative body image is embedded in wider systems involving self-objectification, self-consciousness, interoceptive sensibility, and even paranoia-like ideation, and network comparisons in pregnant versus non-pregnant women suggest that body dissatisfaction may differ not only in severity but also in structural organization and influential components across contexts.36–38
In this way, network analysis refines and extends existing theories rather than displacing them. Sociocultural models specify distal inputs, cognitive-behavioral models specify proximal maintenance processes, and network approaches specify how these processes may be organized into dynamic symptom-to-symptom systems that help explain comorbidity, heterogeneity across populations, and potentially more precise intervention targets. At the same time, especially in cross-sectional studies, central nodes and edges should be interpreted as clinically meaningful hypotheses rather than definitive causal pathways.
Neurobiological Correlates of Body-Related Stress
Beyond psychosocial pathways, emerging evidence suggests that body image-related distress acts as a chronic stressor that triggers neurobiological dysregulation.63 High levels of body dissatisfaction and perceived weight stigma are associated with overactivation of the hypothalamic-pituitary-adrenal (HPA) axis, leading to prolonged cortisol elevation, which impairs mood-regulating brain regions.64 Furthermore, systemic inflammation has been identified as a potential biological mediator; pro-inflammatory markers such as C-reactive protein and interleukin-6 appear to partially mediate the link between body-related distress and depressive symptoms,65 suggesting that the “internalization” of societal ideals has measurable physiological costs. These findings align with a holistic biopsychosocial model, where cognitive appraisals of the body are translated into affective risk through integrated neuroendocrine and immune pathways.
To provide a comprehensive overview of these pathways, Figure 1 illustrates an integrative mechanistic map of the body image-depression association. Distal sociocultural pressures from peers, family, and digital media are conceptualized as operating through Objectification Theory, the Tripartite Influence Model, and cognitive-attentional accounts to shape body image across perceptual, affective, cognitive, and behavioral domains. Disturbance in these domains may, in turn, contribute to depression and other psychopathology through psychosocial mechanisms (eg, low self-esteem, rumination, shame, perfectionism, and maladaptive coping) and neurobiological mechanisms (eg, HPA axis dysregulation and inflammatory activation). The figure further emphasizes bidirectionality, showing that depressive states can reinforce negative body image through mood-congruent processing, generalized negative self-appraisal, and behavioral withdrawal.
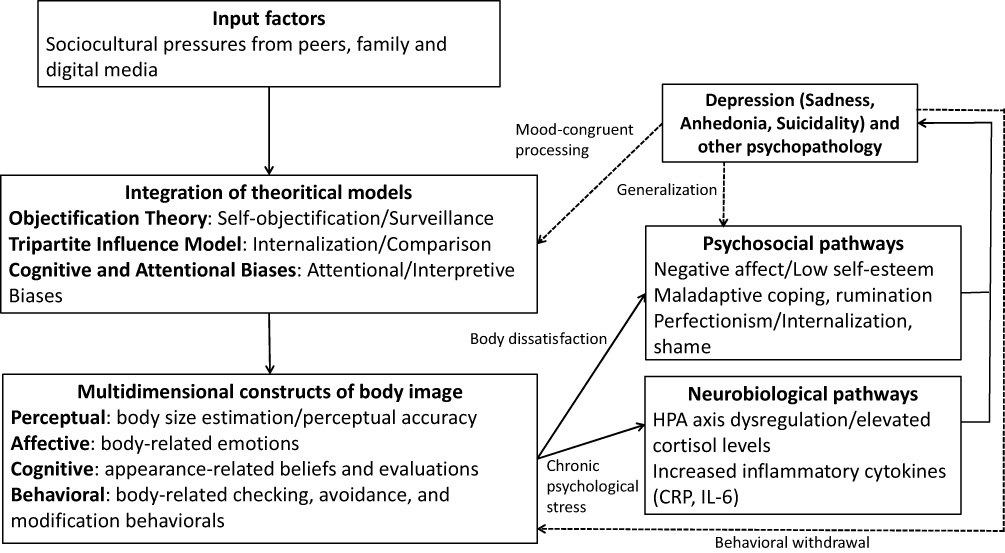 |
Figure 1 Integrative framework of psychosocial and neurobiological pathways linking body image and depression. Abbreviations: HPA, Hypothalamic-Pituitary-Adrenal; CRP, C-reactive protein; IL-6, Interleukin-6. |
Interventions Targeting Body Image as a Viable Strategy for Preventing or Reducing Depression
Cognitive Behavioral Therapy (CBT)
Cognitive Behavioral Therapy (CBT) remains the most established, empirically supported intervention for body image disturbance and is increasingly recognized for its utility in reducing comorbid depressive symptoms.66,67 Conceptually, CBT targets the maladaptive cognitive appraisals that link appearance to self-worth (eg, rigid, conditional beliefs such as “If I do not look a certain way, I am unacceptable”) and the behavioral strategies that maintain distress, including body checking, reassurance seeking, avoidance, and appearance-focused safety behaviors.68 By identifying, testing, and restructuring distorted appearance-related thoughts, CBT reduces the salience of appearance as a primary determinant of value and interrupts reinforcement cycles that perpetuate shame and anxiety.69 This cognitive and behavioral shift is particularly relevant for depression because it attenuates self-criticism, rumination, and withdrawal—core maintenance processes in depressive disorders—thereby improving mood not only indirectly through enhanced functioning but also directly through reduced negative self-evaluation.70 In clinical and medical populations where appearance concerns are intertwined with chronic symptoms or visible phenotypic changes, CBT’s structured, skills-based approach can provide patients with concrete tools to challenge hopeless interpretations, restore agency, and increase engagement in rewarding activities, which together support broader affective improvement.71
Cognitive Dissonance–Based Interventions
Cognitive dissonance–based interventions, exemplified by programs such as the Body Project, represent a prevention-oriented strategy that has demonstrated meaningful benefits for body dissatisfaction and, importantly, downstream improvements in depressive symptoms.72 These interventions deliberately create dissonance by asking participants to actively critique culturally prescribed appearance ideals—through exercises such as writing persuasive arguments against the thin ideal, role-playing resistance to diet culture, or advising younger peers about the harms of appearance-based norms.73 Because individuals experience discomfort when their public advocacy conflicts with privately internalized ideals, they are motivated to resolve the inconsistency by reducing internalization of those ideals and weakening appearance-contingent self-worth.73 Although originally designed to reduce eating-disorder risk, a consistent finding across the broader evidence base is that decreasing ideal internalization also reduces chronic experiences of perceived failure, shame, and social comparison—psychological conditions that commonly feed depressive affect.72 As a result, dissonance-based approaches can yield “secondary” antidepressant effects by removing a pervasive, socially reinforced source of self-discrepancy and by promoting more flexible, values-consistent self-evaluation.74
Body Neutrality and Functionality Appreciation
More recent intervention approaches reflect a conceptual shift from “body positivity” (emphasizing liking or loving one’s appearance) toward “body neutrality” and functionality appreciation, which prioritize what the body does over how it looks.75 In this framework, the therapeutic goal is not to convince individuals to adopt uniformly positive feelings about appearance, but to decouple self-worth from aesthetic evaluation and to expand identity beyond the visual body.76 Functionality-focused exercises encourage attention to embodied capacities (eg, strength, mobility, sensory experience, caregiving, creativity) and foster gratitude and respect for the body as an instrument for living rather than as an object for appraisal.75 This reorientation has particular relevance for depression because it can reduce appearance-based rumination and shift attentional resources toward personally meaningful activities, supporting behavioral activation and a more stable sense of self.77 Clinically, body neutrality may be especially appropriate for individuals facing aging-related changes, chronic illness, disability, or treatment-related disfigurement, for whom an expectation of “loving” appearance may feel unattainable or inauthentic.71 By offering a realistic, compassionate alternative to appearance-centric self-evaluation, functionality-based interventions may strengthen resilience to unavoidable bodily change and thereby reduce vulnerability to hopelessness and depressive symptom escalation.75
Cognitive Bias Modification (CBM)
Cognitive Bias Modification (CBM) applies a mechanistic, neurocognitive lens to intervention by attempting to retrain automatic attentional, interpretive, or perceptual processes that contribute to body image disturbance and depressive vulnerability.78 Delivered through brief, computerized tasks, CBM is designed to shift rapid, habitual processing patterns—such as over-attending to perceived flaws, interpreting ambiguity as criticism, or using overly strict perceptual categories for weight and attractiveness—before reflective cognition has a chance to intervene.78 Early evidence suggests that such training can successfully alter targeted biases (for example, adjusting perceptual thresholds for what is classified as “fat” versus “thin”), supporting the feasibility of modifying automatic processing.74 However, short-term changes in bias do not always translate immediately into measurable reductions in depressive symptoms, implying that symptom improvement may require greater training intensity, longer follow-up windows, or integration with broader psychotherapeutic elements such as cognitive restructuring, emotion regulation skills, and behavioral activation.78 From a clinical translation perspective, CBM is promising as an adjunctive tool: it may be most effective when embedded within multimodal interventions that address both fast, automatic processes and slower, meaning-based belief systems that jointly sustain body-related distress and depressed mood.78
Discussion
Synthesis of Findings
Across the literature reviewed, body image emerges as a central construct in the psychopathology of depression rather than a peripheral correlate. Evidence accumulated over several decades indicates that the association between body image disturbance—most consistently operationalized as body dissatisfaction—and depressive symptoms is robust across cultural settings, evident across developmental stages, and relevant in transdiagnostic contexts beyond eating disorders. Importantly, the evidentiary base has progressed from largely cross-sectional demonstrations of correlation to more methodologically rigorous longitudinal, genetically informed, and symptom-level analytic approaches, strengthening the inference that body image can function as a meaningful vulnerability factor within depressive trajectories. One of the most consistent insights is that subjective appraisal carries greater predictive weight than objective anthropometric indices such as BMI: it is the perceived experience of being flawed, unattractive, or unacceptable—and the meaning attached to that perception—rather than objective body size per se, that most strongly forecasts depressive outcomes. Our synthesis further highlights that this subjective distress is not biologically silent; it is increasingly linked to HPA axis dysregulation and low-grade systemic inflammation, providing a physiological basis for the observed psychological vulnerability.
To clarify the current state of the field, our findings can be categorized into three levels of evidence. Well-established facts include the longitudinal predictive power of body dissatisfaction for adult depression and the primacy of subjective appearance evaluation over objective BMI. Emerging but uncertain areas include the complex impact of digital-media behaviors—such as curated self-presentation and photo editing—and the clinical utility of symptom-level network analysis in identifying “bridge” symptoms like self-hatred or worthlessness. Finally, understudied domains persist regarding male-specific muscularity ideals, the applicability of sociocultural models in non-Western contexts, and the unique appearance-related distress in palliative or oncology care settings.
Consistency and Divergence
The field shows substantial convergence on several core findings, particularly the role of body dissatisfaction as a prospective risk factor for depression and the central mediating role of self-esteem in translating appearance-related evaluations into broader affective disturbance.79 Patterns observed in specific contexts—such as body image functioning as a “bridge” process shaping quality of life in breast cancer, or the predictive value of “feeling fat” during the perinatal period—align with the broader proposition that body-related distress undermines psychological resilience by amplifying shame, self-criticism, and withdrawal. At the same time, meaningful divergences remain. Gender-related findings are not fully uniform: although some studies suggest comparable associations when male-relevant domains (eg, muscularity dissatisfaction) are adequately measured, other work indicates that pathways may differ in content and mechanism (thinness- versus muscularity-centered standards, or different patterns of social comparison). Intervention evidence also varies by modality; CBT has relatively consistent support, whereas mechanistic approaches such as CBM show more mixed outcomes, especially in translating bias change into symptom reduction. Finally, the role of BMI is nuanced: while subjective body image generally predicts depression more strongly, extreme BMI values may contribute independent biological burdens and stigma-related stressors, implying a complex interaction in which physiology and perception jointly shape risk.
Critical Evaluation
Methodologically, recent work has strengthened the field by incorporating large-scale longitudinal cohorts, twin designs, and network analytic models, each of which adds inferential clarity about temporal ordering, shared liabilities, and symptom-level interconnections that earlier decades could not resolve. These advances support more precise hypotheses about causality and identify plausible intervention targets (eg, bridge symptoms such as worthlessness or self-hatred). Nonetheless, important limitations persist. Crucially, the widespread reliance on single-source self-report scales across both body image and mood assessments may introduce common method bias, leading to a spurious inflation of the shared-method variance.80 This risk is particularly salient in clinical samples, where mood-congruent reporting biases can cause individuals to rate both their appearance and their emotional state more negatively, thereby overestimating the substantive link between the two constructs. Future research should prioritize multi-informant assessments or clinician-rated interviews to triangulate these findings. Conceptual heterogeneity also complicates synthesis: “body image” is operationalized variously as weight/shape satisfaction, appearance evaluation, self-objectification, or functionality appreciation, which can obscure whether different components exert distinct effects on depression. Most existing network studies in this area remain cross-sectional, so central nodes and bridge connections should be interpreted as theoretically and clinically informative hypotheses rather than as definitive evidence of causal priority. Moreover, treating body image as a single omnibus variable may mask differential impacts of specific concerns (eg, facial dissatisfaction versus weight dissatisfaction) and differential mechanisms (eg, shame versus avoidance). Cultural representativeness remains another constraint: despite growing contributions from non-Western settings, much of the evidence base is still concentrated in Western and industrialized populations, and the applicability of dominant sociocultural models in rural, indigenous, or highly diverse cultural ecologies remains insufficiently tested.81 Cultural context may shape both the content of body ideals and the social meaning attached to appearance, such that the strength, expression, and mechanisms of the body image-depression relationship may differ across collectivist and individualistic settings.
Theoretical and Practical Implications
Theoretically, the findings are best understood through a complementary rather than competitive framework. Sociocultural models explain the distal origins of body image-related risk by specifying how appearance ideals, social evaluation, and objectifying environments generate chronic vulnerability. Cognitive-behavioral models explain the proximal processes through which this vulnerability is maintained, including maladaptive self-evaluation, attentional bias, shame, rumination, avoidance, and reduced perceived effectiveness. Network-analytic findings extend these earlier frameworks by moving from broad vulnerability or mediation pathways to a more fine-grained, symptom-level account of how body image disturbance becomes linked with depression and other forms of psychopathology in practice. In particular, network studies suggest that eating-disorder-specific features such as drive for thinness may co-occur with central affective, interpersonal, and self-evaluative processes, while broader body-image networks in community and special populations indicate that negative body image is embedded in wider systems involving self-objectification, interoceptive sensibility, self-consciousness, and context-specific body-related concerns. This helps explain why similar appearance pressures may lead to different forms of distress across individuals and contexts, and why treatment may need to target not only body dissatisfaction itself but also the symptom-level processes through which it is connected to mood and functioning.
Rather than treating body image as an ancillary concern, contemporary models imply that appearance-based self-evaluation can shape core depressive mechanisms, including self-criticism, rumination, shame, social withdrawal, and reduced engagement in rewarding activities. Practically, this perspective argues for a more explicit incorporation of body image into both assessment and intervention. In clinical settings, routine screening for body dissatisfaction and appearance-contingent self-worth is warranted among depressed patients even when eating disorder symptoms are absent, because unaddressed body-related distress may perpetuate low self-esteem and avoidance. Specifically, clinicians should implement standardized protocols such as administering the Body Image States Scale to capture momentary evaluative distress or the Body Image Disturbance Questionnaire to screen for clinical severity.82,83 These tools should ideally be integrated into the initial psychiatric intake for all patients presenting with mood disorder symptoms, enabling early identification of appearance-related triggers that may otherwise be overlooked in traditional depression assessments. Actionable integration involves establishing clear referral pathways to body-image-focused CBT when a patient scores above established clinical cut-offs.84 Treatment planning may benefit from moving beyond symptom reduction alone toward strengthening protective constructs such as body appreciation, body neutrality, and functionality-based self-concepts, particularly for populations facing unavoidable bodily change (eg, illness, aging, postpartum transitions). At the public health level, school- and community-based prevention programs may be reframed to treat body image not only as an eating-disorder concern but also as a primary prevention target for depression, especially during sensitive developmental windows.
Future Research Directions
Several priorities follow from the current evidence base and its limitations. First, greater mechanistic precision is needed to capture the micro-temporal dynamics through which body image and mood influence one another; ecological momentary assessment designs could clarify how daily fluctuations in body confidence, comparison exposure, and rumination precipitate near-term changes in depressive affect and behavior. Second, improving generalizability requires systematic inclusion of diverse populations, including male-specific measurement domains (muscularity/leanness concerns), gender-diverse individuals, and broader representation from non-Western and under-studied cultural contexts to test the cultural boundary conditions of prevailing models. Third, scalable digital interventions deserve rigorous evaluation, particularly app-based or social-media–focused programs that target comparison, self-objectification, and appearance-ideal internalization while promoting neutrality or functionality appreciation; these approaches may offer practical reach if efficacy and engagement can be demonstrated. Fourth, to address persistent gaps in causal inference, future research must prioritize longitudinal designs and experimental manipulations. While existing evidence supports a strong association, multi-wave prospective studies with extended follow-up periods are essential to definitively establish temporal precedence and clarify the long-term trajectories of the bidirectional link. Furthermore, randomized controlled trials that specifically manipulate body image (eg, through targeted psychological interventions) are needed to test whether improving appearance-related self-evaluation directly reduces depressive symptoms, thereby moving beyond descriptive correlation toward mechanistic causation.74 Finally, future work should more directly integrate neurobiological evidence by examining neural correlates of body image distortion and self-referential processing in depressed versus non-depressed individuals (eg, salience and threat circuitry), with the goal of identifying objective markers of distress and clarifying how biological vulnerability interacts with sociocognitive mechanisms over development.
Conclusion
The association between body image and depression extends beyond simple comorbidity. Evidence from longitudinal, experimental, and genetically informed studies suggests that body dissatisfaction is a significant psychological stressor that can precede and intensify depressive symptoms. This influence appears to operate through several overlapping mechanisms, including shame and self-criticism, self-objectification and body surveillance, and repetitive negative thinking such as rumination. Together, these processes undermine self-esteem, reduce social and rewarding engagement, and narrow a person’s sense of agency. Importantly, the literature indicates that subjective body evaluation often predicts depressive outcomes more strongly than objective indices such as BMI, suggesting that perceived appearance flaws and their implications for self-worth are more consequential than physical characteristics alone.
Depression, in turn, can further worsen body image by biasing attention and interpretation toward negative appearance-related information and by encouraging behavioral patterns such as reduced activity, diminished self-care, and disrupted eating or sleep. Symptom-level and network approaches support this reciprocal relationship, highlighting bridge symptoms such as worthlessness and self-hatred that connect body image disturbance to broader depressive syndromes. These findings have important clinical implications: body image should be routinely assessed in depression care, and interventions should focus not on changing the body itself but on modifying maladaptive appraisals, reducing appearance-contingent self-worth, and strengthening body appreciation, body neutrality, and functionality-focused self-concepts. Viewing body image as a modifiable risk factor may help interrupt this cycle and broaden prevention and treatment strategies for depression across diverse populations.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used Doubao 1.67.3 Pro exclusively to refine language fluency, enhance readability, and correct grammatical inaccuracies. No AI-generated content was incorporated into the manuscript at any stage of the writing process. The conceptual framework, methodological design, data interpretation, and scholarly conclusions remain entirely original to the authors. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
Funding
This work was supported by the 2025 Wuhan Natural Science Foundation Exploration Plan Municipal Medical Institutions Clinical Research Key Project (2025020701020282, PI: Xu YM) and the Young Top Talent Programme in Public Health from Health Commission of Hubei Province (grant number: EWEITONG[2021]74, PI: Zhong BL). The funding source listed had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the paper for publication.
Disclosure
Bao-Liang Zhong is an associate editor in the journal of Psychology Research and Behavior Management. The authors reports no other conflicts of interest in this work.
References
1. Luo W, Zhong BL. The relationship between childhood abuse, personality, and depression: a narrative review. Alpha Psychiatry. 2025;26(4):45405. doi:10.31083/AP45405
2. Zhong BL, Ruan YF, Xu YM, Chen WC, Liu LF. Prevalence and recognition of depressive disorders among Chinese older adults receiving primary care: a multi-center cross-sectional study. J Affect Disord. 2020;260:26–17. doi:10.1016/j.jad.2019.09.011
3. Xu YM, Hu CJ, Zhong BL. Family dynamics and depression among children: an integrative review of theoretical models and attachment-based interventions. Psychol Res Behav Manag. 2025;18:2259–2272. doi:10.2147/PRBM.S559551
4. Hu X, Guo C. Temporal trends and cohort variations of gender-specific major depressive disorders incidence in China: analysis based on the age-period-cohort-interaction model. Gen Psychiatr. 2024;37(4):e101479. doi:10.1136/gpsych-2023-101479
5. Amiri S, Khan MAB. Trends in prevalence and burden of depressive disorders in Iran at national and subnational levels: estimates based on sex and age groups. Gen Psychiatr. 2025;38(3):e102016. doi:10.1136/gpsych-2024-102016
6. Liu J, Ning W, Zhang N, Zhu B, Mao Y. Estimation of the global disease burden of depression and anxiety between 1990 and 2044: an analysis of the global burden of disease study 2019. Healthcare. 2024;12(17):1721. doi:10.3390/healthcare12171721
7. Costantini I, Eley TC, Pingault JB, et al. Longitudinal associations between adolescent body dissatisfaction, eating disorder and depressive symptoms, and BMI: a UK twin cohort study. Lancet Psychiatry. 2026;13(1):37–46. doi:10.1016/S2215-0366(25)00333-5
8. Rodgers RF, Laveway K, Campos P, de Carvalho PHB. Body image as a global mental health concern. Glob Ment Health. 2023;10:e9. doi:10.1017/gmh.2023.2
9. Rotella L, Aloi M, Carbone EA, et al. Body image: a bridge between depression and quality of life in women with cancer. Psychooncology. 2025;34(11):e70328. doi:10.1002/pon.70328
10. Cash TF, Smolak L. Body Image: A Handbook of Science, Practice, and Prevention.
11. Sharpe H, Patalay P, Choo TH, et al. Bidirectional associations between body dissatisfaction and depressive symptoms from adolescence through early adulthood. Dev Psychopathol. 2018;30(4):1447–1458. doi:10.1017/S0954579417001663
12. Cheng Y, Chen Y, Barnhart WR, et al. Improving body image in female Chinese social media users with eating disorder symptoms: a randomized controlled trial of two online self-guided single-session interventions. J Eat Disord. 2025;14(1):37. doi:10.1186/s40337-025-01497-3
13. Prnjak K, Jukic I, Mitchison D, Griffiths S, Hay P. Body image as a multidimensional concept: a systematic review of body image facets in eating disorders and muscle dysmorphia. Body Image. 2022;42:347–360. doi:10.1016/j.bodyim.2022.07.006
14. Wang Y, Chen Y, Lu C, et al. The psychological factors mediating/moderating the association between body-image disturbance and depression: a systematic review. Psych J. 2024;13(4):527–540. doi:10.1002/pchj.754
15. Mullarkey MC, Marchetti I, Beevers CG. Using network analysis to identify central symptoms of adolescent depression. J Clin Child Adolesc Psychol. 2019;48(4):656–668. doi:10.1080/15374416.2018.1437735
16. Smith AC, Ahuvia I, Ito S, Schleider JL. Project Body Neutrality: piloting a digital single-session intervention for adolescent body image and depression. Int J Eat Disord. 2023;56(8):1554–1569. doi:10.1002/eat.23976
17. Kakar V, Fardouly J, Rapee RM, Guo M, Arman S, Niazi E. Exploring the tripartite influence model of body image and disordered eating among adolescent girls living in Australia, China, India, and Iran. Body Image. 2023;47:101633. doi:10.1016/j.bodyim.2023.101633
18. Abdoli M, Scotto Rosato M, Desousa A, Cotrufo P. Cultural differences in body image: a systematic review. Soc Sci. 2024;13(6):305. doi:10.3390/socsci13060305
19. Brokjob LG, Cornelissen PL, Gumancik J, McCarty K, Tovee MJ, Cornelissen KK. Evidence for a specific distortion in perceptual body image in eating disorders: a replication and extension. PLoS One. 2024;19(11):e0313619. doi:10.1371/journal.pone.0313619
20. Sick K, Pila E, Nesbitt A, Sabiston CM. Does self-compassion buffer the detrimental effect of body shame on depressive symptoms? Body Image. 2020;34:175–183. doi:10.1016/j.bodyim.2020.05.012
21. Crocker J, Luhtanen RK, Cooper ML, Bouvrette A. Contingencies of self-worth in college students: theory and measurement. J Pers Soc Psychol. 2003;85(5):894–908. doi:10.1037/0022-3514.85.5.894
22. Hofschroer V, Vivell MB, Vocks S, Hartmann AS. Short-term functions and long-term consequences of body checking as a transdiagnostic phenomenon across eating disorders, body dysmorphic disorder, and illness anxiety disorder: a systematic review. J Eat Disord. 2025;13(1):281. doi:10.1186/s40337-025-01462-0
23. Cash TF. Body image: past, present, and future. Body Image. 2004;1(1):1–5. doi:10.1016/S1740-1445(03)00011-1
24. Bornioli A, Lewis-Smith H, Slater A, Bray I. Body dissatisfaction predicts the onset of depression among adolescent females and males: a prospective study. J Epidemiol Community Health. 2020;
25. Tylka TL, Wood-Barcalow NL. What is and what is not positive body image? Conceptual foundations and construct definition. Body Image. 2015;14:118–129. doi:10.1016/j.bodyim.2015.04.001
26. Hevron H, Weinbach N. Self-compassion and cognitive reappraisal restore female adolescents’ body satisfaction and appreciation after appearance-related rumination. Body Image. 2024;51:101779. doi:10.1016/j.bodyim.2024.101779
27. Noles SW, Cash TF, Winstead BA. Body image, physical attractiveness, and depression. J Consult Clin Psychol. 1985;53(1):88–94. doi:10.1037//0022-006x.53.1.88
28. Plesea-Condratovici C, Dionisie V, Moroianu LA, Serban PS, Plesea-Condratovici V, Arbune M. Perception versus actual weight: body image dissatisfaction as a stronger correlate of anxiety and depression than BMI among romanian health sciences students. Healthcare. 2025;13(23):3118. doi:10.3390/healthcare13233118
29. Beck AT. Cognitive Therapy and the Emotional Disorders. International Universities Press; 1976.
30. He Q, Zheng H, Zhang J, et al. Association between the frontoparietal network, clinical symptoms and treatment response in individuals with untreated anorexia nervosa. Gen Psychiatr. 2024;37(3):e101389. doi:10.1136/gpsych-2023-101389
31. Fredrickson BL, Roberts T-A. Objectification theory: toward understanding women’s lived experiences and mental health risks. Psychol Women Q. 1997;21(2):173–206. doi:10.1111/j.1471-6402.1997.tb00108.x
32. Thompson JK, Heinberg LJ, Altabe M, Tantleff-Dunn S. Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance. American Psychological Association; 1999.
33. Stice E, Bearman SK. Body-image and eating disturbances prospectively predict increases in depressive symptoms in adolescent girls: a growth curve analysis. Dev Psychol. 2001;37(5):597–607. doi:10.1037//0012-1649.37.5.597
34. Borsboom D, Cramer AO. Network analysis: an integrative approach to the structure of psychopathology. Annu Rev Clin Psychol. 2013;9:91–121. doi:10.1146/annurev-clinpsy-050212-185608
35. Zhong BL, Yuan MD, Li F, Sun P. The psychological network of loneliness symptoms among Chinese residents during the COVID-19 outbreak. Psychol Res Behav Manag. 2023;16:3767–3776. doi:10.2147/PRBM.S424565
36. Piwinska J, Bagrowska P, Gaweda L. Body image and paranoia-findings from a large-scale community sample using network analysis. J Clin Psychol. 2026. doi:10.1002/jclp.70141
37. Zhang N, Yang HX. A network analysis of body image concern, interoceptive sensibility, self-consciousness, and self-objectification. J Clin Psychol. 2024;80(11):2247–2267. doi:10.1002/jclp.23734
38. Fuller-Tyszkiewicz M, Broadbent J, Richardson B, Watson B, Klas A, Skouteris H. A network analysis comparison of central determinants of body dissatisfaction among pregnant and non-pregnant women. Body Image. 2020;32:111–120. doi:10.1016/j.bodyim.2019.12.001
39. Zheng M, Chen P, Zhang L, et al. Prevalence and network structure of depression and its association with quality of life among older stroke survivors: findings from a national survey in China. Gen Psychiatr. 2025;38(2):e101838. doi:10.1136/gpsych-2024-101838
40. Solmi M, Collantoni E, Meneguzzo P, Degortes D, Tenconi E, Favaro A. Network analysis of specific psychopathology and psychiatric symptoms in patients with eating disorders. Int J Eat Disord. 2018;51(7):680–692. doi:10.1002/eat.22884
41. Solmi M, Collantoni E, Meneguzzo P, Tenconi E, Favaro A. Network analysis of specific psychopathology and psychiatric symptoms in patients with anorexia nervosa. Eur Eat Disord Rev. 2019;27(1):24–33. doi:10.1002/erv.2633
42. Blundell E, De Stavola BL, Kellock MD, et al. Longitudinal pathways between childhood BMI, body dissatisfaction, and adolescent depression: an observational study using the UK Millenium Cohort Study. Lancet Psychiatry. 2024;11(1):47–55. doi:10.1016/S2215-0366(23)00365-6
43. Han ZY, Ye ZY, Zhong BL. School bullying and mental health among adolescents: a narrative review. Transl Pediatr. 2025;14(3):463–472. doi:10.21037/tp-2024-512
44. Ye ZY, Han ZY, Zhong BL. Secure base and mental health in children: a narrative review. Transl Pediatr. 2024;13(9):1608–1616. doi:10.21037/tp-24-191
45. He J, Chen X, Luo B. The association between body image and depressive symptoms in pregnant and postpartum women: a meta-analysis. Front Public Health. 2025;13:1655639. doi:10.3389/fpubh.2025.1655639
46. Jannink TI, Bordewijk EM, Lehmann V, Hoek A, Goddijn M, van Wely M. Patient characteristics associated with symptoms of anxiety, depression, and reduced body appreciation in women with polycystic ovary syndrome. Hum Reprod. 2025;40(12):2360–2368. doi:10.1093/humrep/deaf214
47. Bates J, Maalin N, Thornborrow T. Aspects of body image as moderators and mediators in the relationship between minority stress and depression among diverse LGBTQIA+ identities. Body Image. 2025;55:101975. doi:10.1016/j.bodyim.2025.101975
48. Moradi B, Huang Y-P. Objectification theory and psychology of women: a decade of advances and future directions. Psychol Women Q. 2008;32(4):377–398. doi:10.1111/j.1471-6402.2008.00452.x
49. Saunders JF, Nutter S, Waugh R, Hayden KA. Testing body-related components of objectification theory: a meta-analysis of the relations between body shame, self-objectification, and body dissatisfaction. Body Image. 2024;50:101738. doi:10.1016/j.bodyim.2024.101738
50. Grabe S, Hyde JS, Lindberg SM. Body objectification and depression in adolescents: the role of gender, shame, and rumination. Psychol Women Q. 2007;31(2):164–175. doi:10.1111/j.1471-6402.2007.00350.x
51. Baek SU, Yoon JH. Association of objective body shape and perceived body image with depressive symptoms in men and women. Psychiatry Clin Neurosci. 2025;79(8):458–465. doi:10.1111/pcn.13836
52. van den Berg P, Thompson JK, Obremski-Brandon K, Coovert M. The Tripartite Influence model of body image and eating disturbance: a covariance structure modeling investigation testing the mediational role of appearance comparison. J Psychosom Res. 2002;53(5):1007–1020. doi:10.1016/s0022-3999(02)00499-3
53. Keery H, van den Berg P, Thompson JK. An evaluation of the Tripartite Influence Model of body dissatisfaction and eating disturbance with adolescent girls. Body Image. 2004;1(3):237–251. doi:10.1016/j.bodyim.2004.03.001
54. Roberts SR, Maheux AJ, Hunt RA, Ladd BA, Choukas-Bradley S. Incorporating social media and muscular ideal internalization into the tripartite influence model of body image: towards a modern understanding of adolescent girls’ body dissatisfaction. Body Image. 2022;41:239–247. doi:10.1016/j.bodyim.2022.03.002
55. Zheng Q, Chen M, Hu J, Zhou T, Wang P. Appearance comparison, body appreciation, and adolescent depressive symptoms: roles of gender, age, and body-mass index. Psychol Res Behav Manag. 2024;17:3473–3484. doi:10.2147/PRBM.S483375
56. Rodgers RF, DuBois RH. Cognitive biases to appearance-related stimuli in body dissatisfaction: a systematic review. Clin Psychol Rev. 2016;46:1–11. doi:10.1016/j.cpr.2016.04.006
57. Everaert J, Podina IR, Koster EHW. A comprehensive meta-analysis of interpretation biases in depression. Clin Psychol Rev. 2017;58:33–48. doi:10.1016/j.cpr.2017.09.005
58. Mathews A, MacLeod C. Cognitive vulnerability to emotional disorders. Annu Rev Clin Psychol. 2005;1:167–195. doi:10.1146/annurev.clinpsy.1.102803.143916
59. Glombitza E, Cornelissen PL, Tovee MJ, Legenbauer T. Effect of cognitive bias modification training on body image dissatisfaction in adolescents with anorexia nervosa or depression-a pilot feasibility randomized controlled crossover study. Front Psychol. 2025;16:1655064. doi:10.3389/fpsyg.2025.1655064
60. Xia HS, Li YX, Zhang QY, et al. Attention bias modification for depression: a systematic review and meta-analysis. Front Psychiatry. 2023;14:1098610. doi:10.3389/fpsyt.2023.1098610
61. Summers BJ, Aalbers G, Jones PJ, McNally RJ, Phillips KA, Wilhelm S. A network perspective on body dysmorphic disorder and major depressive disorder. J Affect Disord. 2020;262:165–173. doi:10.1016/j.jad.2019.11.011
62. Bernstein EE, Phillips KA, Greenberg JL, Curtiss J, Hoeppner SS, Wilhelm S. Mechanisms of cognitive-behavioral therapy effects on symptoms of body dysmorphic disorder: a network intervention analysis. Psychol Med. 2023;53(6):2531–2539. doi:10.1017/S0033291721004451
63. Sabik NJ, Lupis SB, Geiger AM, Wolf JM. Are body perceptions and perceived appearance judgments by others linked to stress and depressive symptoms? J Appl Behav Res. 2019;24:e12131. doi:10.1111/jabr.12131
64. Lamarche L, Ozimok B, Gammage KL, Muir C. Men respond too: the effects of a social-evaluative body image threat on shame and cortisol in university men. Am J Mens Health. 2017;11(6):1791–1803. doi:10.1177/1557988317723406
65. Steptoe A, Frank P. Obesity and psychological distress. Philos Trans R Soc Lond B Biol Sci. 2023;378(1888):20220225. doi:10.1098/rstb.2022.0225
66. Amirshahi M, Saremi AA, Nouri R, Karbalaee MH, Hosseini Sadat R. Comparing the effectiveness of emotion-focused and cognitive-behavioral therapies on body image, anxiety, and depression in women with PCOS. J Educ Health Promot. 2024;13:230. doi:10.4103/jehp.jehp_687_23
67. Sun Y, Park S, Malik A, et al. Pregnancy stressors and postpartum symptoms of depression and anxiety: the moderating role of a cognitive-behavioural therapy (CBT) intervention. Gen Psychiatr. 2024;37(1):e101136. doi:10.1136/gpsych-2023-101136
68. Patel TA, Summers BJ, Cougle JR. The scientific status of safety behaviors in body dysmorphic disorder. J Obsessive Compuls Relat Disord. 2024;43:100911. doi:10.1016/j.jocrd.2024.100911
69. Lewis-Smith H, Diedrichs PC, Halliwell E. Cognitive-behavioral roots of body image therapy and prevention. Body Image. 2019;31:309–320. doi:10.1016/j.bodyim.2019.08.009
70. Graboyes EM, Kistner-Griffin E, Hill EG, et al. Mechanism underlying a brief cognitive behavioral treatment for head and neck cancer survivors with body image distress. Support Care Cancer. 2023;32(1):32. doi:10.1007/s00520-023-08248-7
71. Zhao W, Chong YY, Chien WT. Effectiveness of cognitive-based interventions for improving body image of patients having breast cancer: a systematic review and meta-analysis. Asia Pac J Oncol Nurs. 2023;10(4):100213. doi:10.1016/j.apjon.2023.100213
72. Stice E, Marti CN, Shaw H, Rohde P. Meta-analytic review of dissonance-based eating disorder prevention programs: intervention, participant, and facilitator features that predict larger effects. Clin Psychol Rev. 2019;70:91–107. doi:10.1016/j.cpr.2019.04.004
73. Stice E, Becker CB, Yokum S. Eating disorder prevention: current evidence-base and future directions. Int J Eat Disord. 2013;46(5):478–485. doi:10.1002/eat.22105
74. Ahuvia I, Jans L, Schleider J. Secondary effects of body dissatisfaction interventions on adolescent depressive symptoms: a meta-analysis. Int J Eat Disord. 2022;55(2):231–246. doi:10.1002/eat.23659
75. Linardon J, Messer M, Tylka TL. Functionality appreciation and its correlates: systematic review and meta-analysis. Body Image. 2023;45:65–72. doi:10.1016/j.bodyim.2023.02.002
76. Mulgrew KE, Hinz A. What is body neutrality and how is it different to existing body image concepts? An analysis of experts and general community responses. Body Image. 2024;51:101780. doi:10.1016/j.bodyim.2024.101780
77. Alleva JM, Diedrichs PC, Halliwell E, et al. More than my RA: a randomized trial investigating body image improvement among women with rheumatoid arthritis using a functionality-focused intervention program. J Consult Clin Psychol. 2018;86(8):666–676. doi:10.1037/ccp0000317
78. Cristea IA, Kok RN, Cuijpers P. Efficacy of cognitive bias modification interventions in anxiety and depression: meta-analysis. Br J Psychiatry. 2015;206(1):7–16. doi:10.1192/bjp.bp.114.146761
79. Paxton SJ, Neumark-Sztainer D, Hannan PJ, Eisenberg ME. Body dissatisfaction prospectively predicts depressive mood and low self-esteem in adolescent girls and boys. J Clin Child Adolesc Psychol. 2006;35(4):539–549. doi:10.1207/s15374424jccp3504_5
80. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
81. Akinyemi O, Ekundayo OK, Fasokun M, et al. Body image, obesity, and sexual coercion: impacts on depression among students at a Nigerian university. PLoS One. 2025;20(6):e0319308. doi:10.1371/journal.pone.0319308
82. Cash TF, Fleming EC, Alindogan J, Steadman L, Whitehead A. Beyond body image as a trait: the development and validation of the body image states scale. Eat Disord. 2002;10(2):103–113. doi:10.1080/10640260290081678
83. Cash TF, Phillips KA, Santos MT, Hrabosky JI. Measuring “negative body image”: validation of the body image disturbance questionnaire in a nonclinical population. Body Image. 2004;1(4):363–372. doi:10.1016/j.bodyim.2004.10.001
84. Chopra D, De La Garza R, Lacourt TE. Clinical relevance of a body image scale cut point of 10 as an indicator of psychological distress in cancer patients: results from a psychiatric oncology clinic. Support Care Cancer. 2021;29(1):231–237. doi:10.1007/s00520-020-05491-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Body Image and Negative Emotions in Chinese Deaf and Hard-of-Hearing College Students: The Mediating Role of Core Self-Evaluation and the Moderating Role of Self-Compassion
Bu X, Zhang Y, Zeng T, Zhou L, Ma H, Du Y
Psychology Research and Behavior Management 2025, 18:759-768
Published Date: 31 March 2025