Back to Journals » Medical Devices: Evidence and Research » Volume 17
The Application Effect of Fine Management Combined with Man–Machine Fixation Mode in Reducing the Attrition Rate of Laparoscopic Instruments—A Non-Randomized, Concurrent Controlled Study
Authors Xia S, Wang X, Xu C, Bai L, Li Y
Received 15 July 2024
Accepted for publication 30 October 2024
Published 7 November 2024 Volume 2024:17 Pages 455—463
DOI https://doi.org/10.2147/MDER.S479048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shujin Xia,1 Xuelu Wang,1 Chenying Xu,1 Lina Bai,1 Yuehong Li2
1Operating Room, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Nursing Department, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal-Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China
Correspondence: Xuelu Wang; Chenying Xu, Operating Room, Shanghai Key Laboratory of Maternal Fetal Medicine, Shanghai Institute of Maternal Fetal Medicine and Gynecologic Oncology, Shanghai First Maternity and Infant Hospital, School of Medicine, Tongji University, 2699 West Gaoke Road, Pudong New Area, Shanghai, 200092, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To explore the effect of fine management combined with man-machine fixation mode in reducing the attrition rate of laparoscopic instruments.
Methods: This is a non-randomized, concurrent controlled study, from December 1, 2023, to May 1, 2024, the use of 4 laparoscopic instruments in the operating room which belongs to shanghai first maternity and infant hospital was analyzed. The instruments were divided into two groups, and the control group was managed by conventional methods. The observation group implemented with fine management combined with man-machine fixed mode. We used instrument attrition rate and physician satisfaction as outcome indicators.
Results: In this study, four laparoscopic instruments were investigated, and a total of 858 cases were used, including 429 cases in the control group (machine 1, machine 2) and 429 cases in the observation group (machine 3, machine 4). After the implementation of refined management combined with man-machine fixed mode, the observation group had significantly lower attrition rate and failure rate of laparoscopic instruments than the control group, including insufficient instrument preparation (p = 0.000), unstable light source (p = 0.012), air leakage (p = 0.000), screen color distortion (p = 0.040), and blurred visual field (p = 0.000). The satisfaction of doctors in the observation group was significantly higher than that in the control group, including preoperative preparation, process cooperation, operation proficiency, trouble solving ability, instrument debugging ability, communication and service attitude (p < 0.01).
Conclusion: The use of fine management combined with man-machine fixed mode in the management of laparoscopic instruments in the operating room can effectively reduce the incidence of instrument attrition rate, improve the efficiency of surgery, and the economic benefit of the hospital, which is worthy of popularization and application.
Keywords: management, man–machine fixed mode, laparoscopic instrument
Introduction
The successful implementation of an operation requires the effective cooperation of doctors and nurses. Medical equipment for operating room belongs to the joint management of the operating room and the equipment department. The operating room is mainly responsible for the scheduling and use of equipment. Nurses should master the manual steps, preliminary detection methods and usage precautions, which can help nurses to make adequate preparation, predict and solve possible equipment problems before surgery, so as to improve the efficiency of surgery. While if the laparoscopic management is not fine, it will lead to wrong operation, which will reduce the life of the equipment, increase the cost of the hospital, delay the operation time, and cause hidden dangers for the patients’ perioperative safety.
Laparoscopic instrument is a high-precision device integrating electronics, optics and machine.1 The minimally invasive surgery applied to gynecology has also become the preferred surgical method for patients in recent years due to its less trauma, less scar and faster recovery.2 In view of the precision construction, expensive price and high maintenance cost of endoscope equipment, it is determined that the management of the equipment must be effective and scientific. Operators can master the use and maintenance of laparoscopic equipment, detect and eliminate faults occurred during operation in time, which plays a key role in the smooth operation of the operation.3
However, during laparoscopic surgery, nurse manager occasionally hear complaints from surgeons, such as why did nurse take time to prepare equipment after the operation begins? Why the light on this screen looks so dark? Is it the cause of the fiber or the endoscope? Why cannot the nurse deal with blurry vision situation? Nursing managers decide to investigate these problems and found the following: a. Operating room laparoscopic equipment has following brands: STORZ, OLYMPUS, stryker, etc. There have some differences among each machine, and new nurses who do not often use these instruments must be not familiar with it. b. Nurses do not know who can help with these problems, until a long time later, the problem still exists. c. Nurses are even less able to anticipate and solve common problems with laparoscopic equipment. In total, the above problems show that there is a lack of an efficient laparoscopic instrument management method, and we need more detailed, more systematic, and more inherited personnel training and efficient management.
Fine management is an efficient, economical and scientific management method from rough to fine and from shallow to deep by adopting the management mode of program,4 in order to achieve efficient cooperation among various departments.5 In this study, the concept of fine management combined with the man-machine fixed mode was integrated into laparoscopic management in the operating room, so as to test the practical effectiveness of this method in reducing the loss of laparoscopic equipment and promoting successful operation in the clinic.
Methods
Study Design and Sample
In order to better simulate the actual clinical situation and quickly evaluate the effectiveness of the intervention method, we chose a non-randomized concurrent controlled study as the research method, and compared the differences between the observation group and the control group without randomly assigning subjects. From December 1, 2023, to May 1, 2024, 4 laparoscopic instruments in the operating room which belongs to Shanghai first maternity and infant hospital were analyzed. The research objects were 4 laparoscopic instruments purchased at similar time and with the same brand. The four instruments were divided into two groups, the innovation of “fine management combined with human-machine fixed mode” was applied to the observation group (No.3 and No.4), the impacts of this method on the study were evaluated, and the results will be compared to control group (No.1 and No.2).
Management Method
The control group implemented routine management mode, including random use of the machine in the operating room, check the operation of the machine before use, register after use; The observation group implements fine management combined with man-machine fixed mode, and the specific measures are as follows:
To Establish an Operating Room Laparoscopic Management Group
We set up 4 groups according to the study, each group consisted of 5–6 members, the team leader is operating room nurse manager, team members including two laparoscopic nurse, one laparoscopic company engineer, one oncology surgery nurse and one laparoscopic gynecologist. The specialist group is responsible for clarifying the responsibilities of personnel at all levels, developing the use system of laparoscopic instruments, training team members to master the working principle and use of laparoscopic instruments, regular assessment, and holding group meetings for continuous quality improvement. The team focused on enhancing the scientific management awareness of the specialist members on the high-precision instruments, reducing the failure and damage to the instruments caused by improper operation, and improving the initiative and accuracy of the cooperation of the specialist nurses in endoscopic surgery.
Formulate the Responsibilities of the Laparoscopic Management Team Members
Each member of the operating room laparoscopic management group has his or her own division of responsibilities, as shown in Table 1. After each person completes his/her duties, the head nurse is responsible for holding a brainstorming meeting every month, and adopts the bottom-up and step-by-step feedback mode. The nurse is responsible for reporting the operating habits of different groups of doctors in laparoscopic surgery, common faults encountered during surgery, and problems that cannot be solved in the table engineers, doctors and head nurse discuss the problems from the perspectives of equipment, medical and management, and jointly determine the improvement plan. The head nurse is responsible for supervising the continuous improvement of quality, so as to ensure that each specialist nurse is in accordance with the standard and standardized implementation.
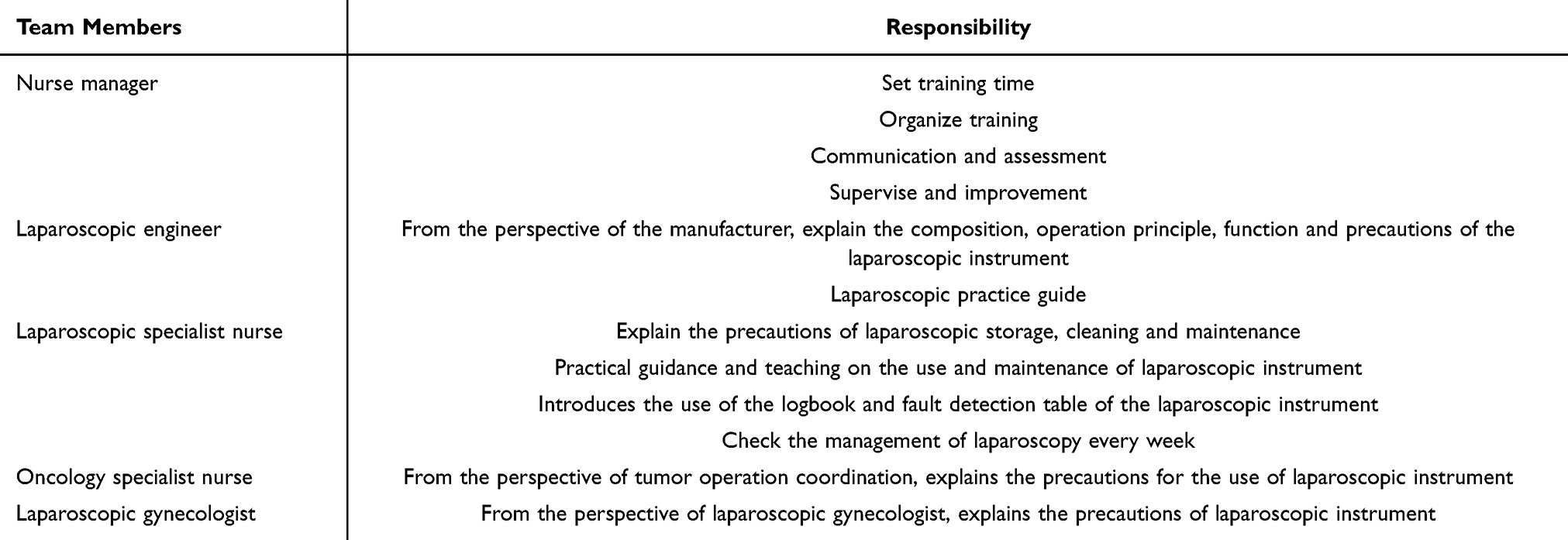 |
Table 1 Responsibility of the Laparoscopic Management Team Members |
Laparoscopic Instruments Management Implementation Method
Preparation of Laparoscopic Instruments Before Operation
The day before operation, the doctor and nurse manager in the operating room determined the next day’s laparoscopic operation number, and the nurse manager coordinated the arrangement of laparoscopic instrument. The machine is numbered in a fixed man-machine mode, and the doctor group and manager are indicated on the machine, and the machine is placed at a fixed place. The commonly used machine is placed in the operating room to avoid frequent movement. Before the operation, the team checked the integrity of the machine, tightened the connection interface, connected the power supply of the device, and the socket was independent and reliably grounded. The light source and the pneumoperitoneum button are placed at 0 points, so as not to suddenly turn on the cold light source brightness is too large and damage the bulb.
Detection and Elimination of Common Faults During the Operation
At the beginning of the operation, make sure that the instrument vent is free of debris. Connect the camera, cold light source, pneumoperitoneum machine and flushing suction system in turn and ensure that the interface of each line is firm when the hand washing nurse connects. When the circulating nurse delivers the camera and cold light source, one hand should hold the head end, and the other hand should hold the flexible cable to avoid bending and head-end collision. Pneumoperitoneum and cold light source systems should gradually be adjusted from low to high gear. Based on the clinical operation feedback, the camera system and inflatable equipment of laparoscope are more prone to failure. Therefore, this study conducted the use management and effect evaluation for the above two parts. In case of instrument failure during use, the power supply, voltage regulator, and connection of each component should be eliminated one by one according to Table 2. Laparoscopic instrument failure detection table and the effectiveness of each accessory should be checked. If it cannot be solved, the equipment should be changed. For the faulty equipment, register in time, and contact the manufacturer technicians to visit or send them to the production factory for maintenance after surgery.
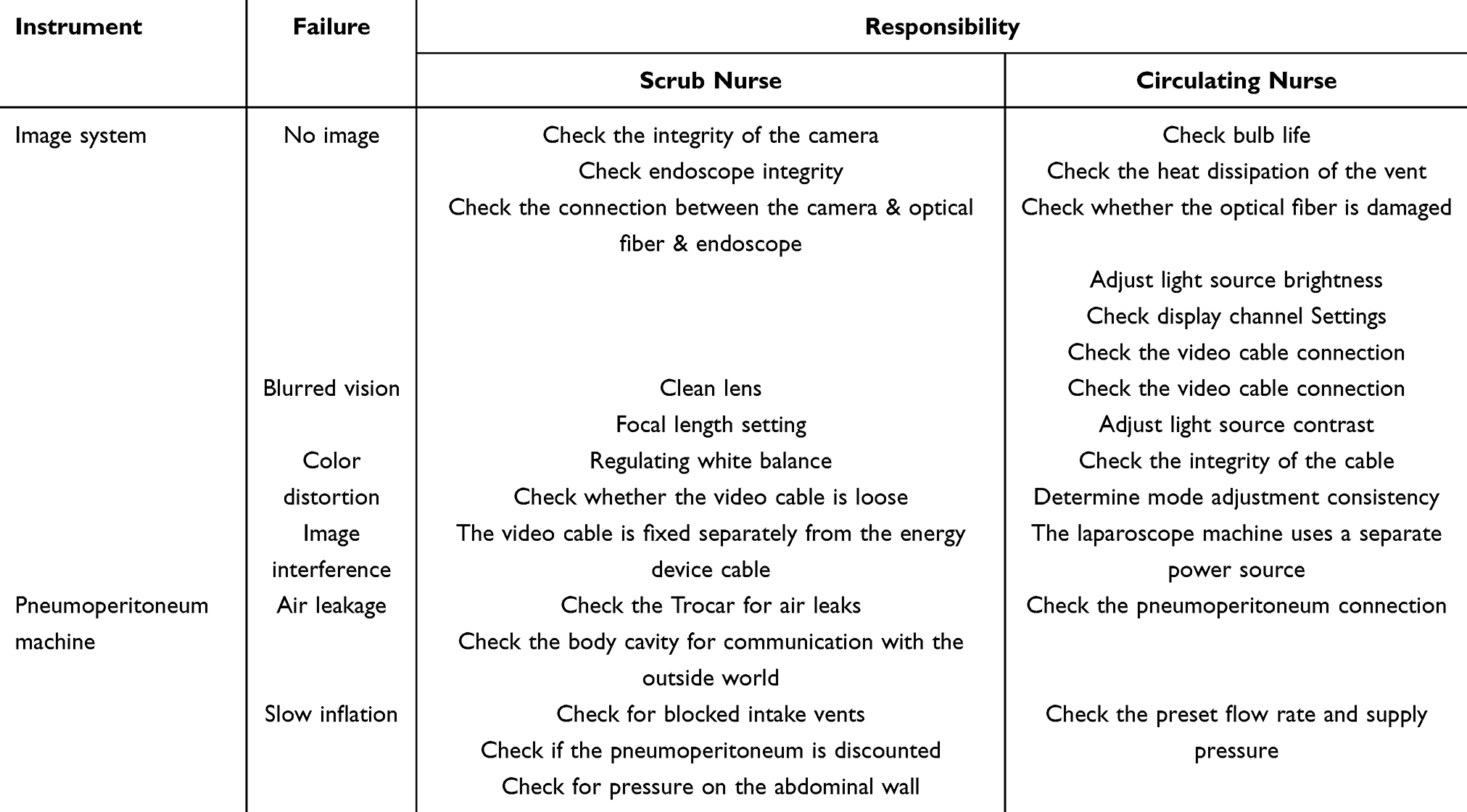 |
Table 2 Laparoscopic Instrument Failure Detection Table |
Instrument Maintenance After Operation
a. After the operation, the output strength should be turned to the lowest point before the device is deactivated and then turned off. b. Avoid bending the light cable. c. All kinds of pipelines cannot be folded after cleaning with 75% alcohol gauze and should be hung in a fixed position with a coil diameter of more than 10cm. d. The surface of the laparoscopic instrument should be cleaned with 75% alcohol gauze and dried in a ventilated place. It should be stored in a fixed position and should not be moved at will during non-working hours. e. Establish a log book for the use of each instrument to record the name of the operation, the time of use, operation status and failure of the instrument. The team leader of the specialist is responsible for checking the performance and use of the equipment every week, and the nurse manager should check every month.
Ethical Considerations
This study has passed the review and approval of the Ethics Committee of Shanghai First Maternity and Infant Health Hospital, with the ethics number KS24244.
Measurements/Instruments
General Information Questionnaire
The name of operation, number of operation cases, group of laparoscopy doctors, group of laparoscopy nurses, machine using time, attrition site and attrition number.
Laparoscopic Instruments Attrition Survey Form
Instrument preparation is inadequate, soft fiber break, fiber converter loss, unstable light source, air leakage, low inflation pressure, color distortion, blurred vision, no image, visual field interference.
Doctor Satisfaction Rate
According to the purpose of the study, the doctor satisfaction scale was developed by ourselves, including (1) Preoperative laparoscopic instrument preparation, (2) operation coordination, (3) operation proficient, (4) trouble clearing situation, (5) Instrument debugging, (6) effective communication, (7) attitude, (8) overall satisfaction. Evaluation scale (1–5 points): very dissatisfied, dissatisfied, average, satisfied, very satisfied, doctor satisfaction = (very satisfied + satisfied)/total cases × 100%.
Data Analysis
SPSS22.0 was used for statistical analysis of the test data. Percentage was used for general instrument use, non-parametric rank test was used for fault analysis, and independent sample T-test was used for doctor satisfaction. p < 0.05 showed that there was a statistical difference between the control group and the observation group.
Results
Results of General Survey of Instrument Using Phenomenon
In this study, four laparoscopic instruments were investigated. The control group (No. 1 machine, No. 2 machine) and observation group (No. 3 machine, No. 4 machine) used a total of 858 cases of operation. There were 429 cases in control group, including 262 cases in machine 1 and 167 cases in machine 2. Observation group 429 cases, including No. 3 machine 277 cases, No. 4 machine 152 cases. The control group was randomly used, machine 1 was used for medical group A, B, C, D and group A, B, C, D and E, and machine 2 was used for medical group C, D and E and group A, B, C, D and E. The observation group was in fixed man-machine mode, machine No. 3 was used by group E and group F, and machine No. 4 was used by group G and group F. For details, see Table 3 Survey on the use of laparoscopic instruments.
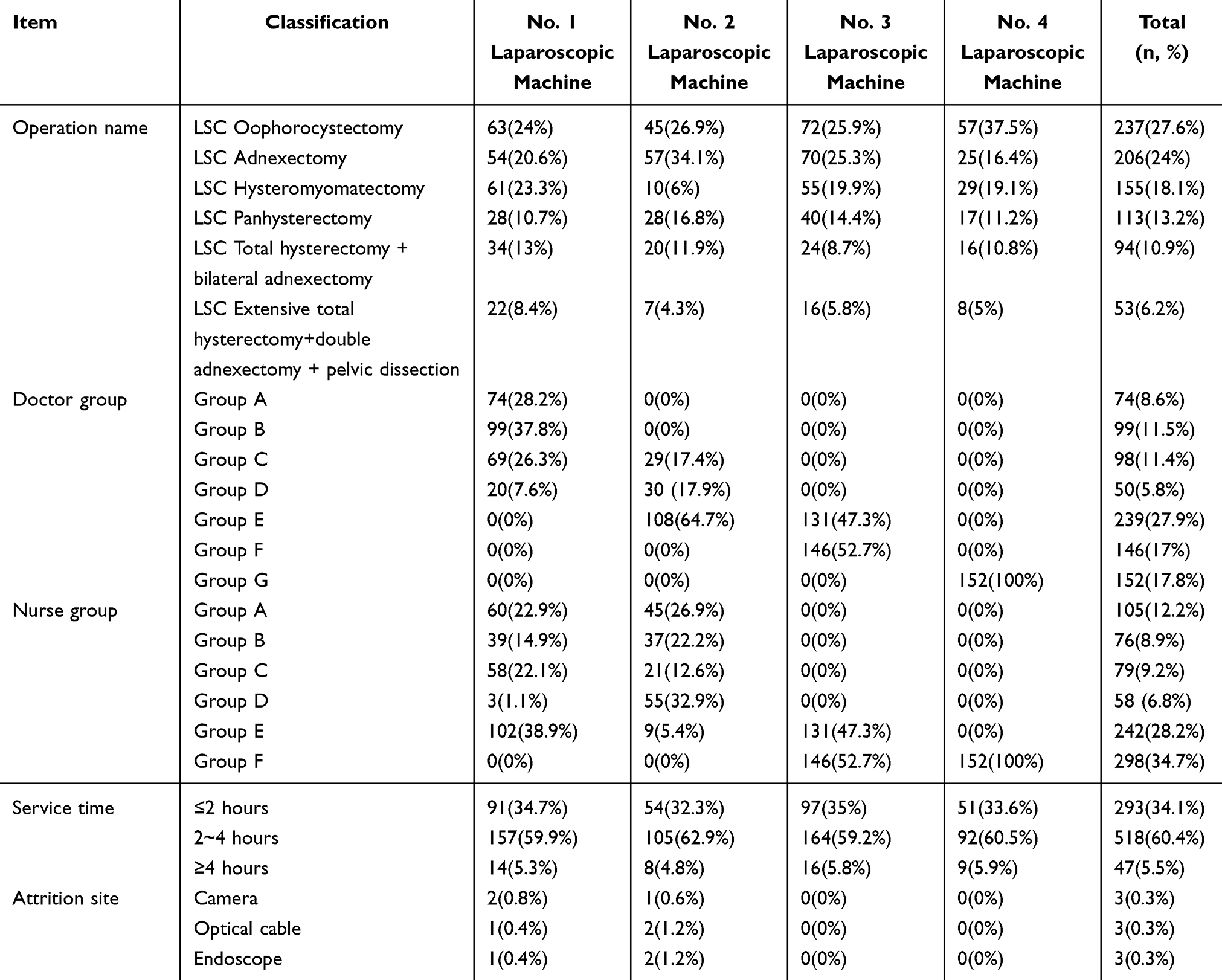 |
Table 3 Survey on the Use of Laparoscopic Instruments (n, %) |
Laparoscopic Instrument Attrition Situation
The incidence of insufficient instrument preparation, optical fiber breakage, optical fiber converter loss, unstable light source, air leakage, color distortion, blurred field of vision, and no image in the control group was higher than that in the observation group implementing fine management combined with human-machine fixed mode, and the differences in inadequate instrument preparation, unstable light source, air leakage, color distortion, and blurred field of vision were statistically significant (p < 0.05). See Table 4 Laparoscopic instrument attrition situation.
 |
Table 4 Laparoscopic Instrument Attrition Situation (n, %) |
Evaluation of Doctors’ Satisfaction Rate
The observation group that implemented refined management combined with fixed man-machine mode had higher performance than the control group in preoperative preparation, operation cooperation, operation proficiency, trouble clearing, instrument debugging, effective communication, service attitude and overall satisfaction, with statistical significance (p < 0.01), as shown in Table 5 Evaluation of doctor satisfaction rate.
 |
Table 5 Doctor Satisfaction Rate (Mean ± Standard Deviation) |
Discussion
Fine Management Combined with Man-Machine Fixed Mode is Conducive to Reducing the Loss of Laparoscopic Instruments
The results of the study showed that after the intervention, there were significant differences in the aspects of “insufficient preparation of laparoscopic surgical instruments, unstable light source, air leakage, color distortion and blurred vision”. For “Insufficient preparation of laparoscopic surgical instruments” part. The endoscopic management specialist team in the operating room includes doctors, nurses, equipment engineers and management personnel. The training knowledge covers endoscopic surgery methods, preparation of tumor surgical instruments and precautions for the use of equipment. The multidisciplinary team helps nurses form diversified thinking, understand the common faults in operation and their requirements for nursing cooperation from the perspective of doctors, understand the composition, operation principle and precautions in operation of the instrument from the perspective of equipment repair engineers, and cover the knowledge blind area and strengthen the knowledge weakness through systematic learning and timely feedback, so as to effectively achieve comprehensive preparation. In terms of “unstable light source and air leakage” part, it indicates that the man-machine fixed mode of this study effectively solves this problem. Its advantage is that the fixed combination of personnel and machine enables medical personnel to master the characteristics and use methods of the machine. If an unstable light source or damaged optical cable occurs, the manager will also timely find the cause and effectively reduce the incidence of failure.6 In terms of “color distortion and blurred vision” part, this is related to the use of the lens and optical cable, usually the nurse does the preparation work, the doctor links the lens and optical cable, but the new doctor does not know the habits of the surgeon, resulting in frequent adjustment during the operation, bending the optical cable, and the camera adjustment failure. However, fine management can effectively solve this problem. Nurses know the habits of the operator, are familiar with the members of the medical team, and master the method of using the machine. Before the operation, nurses will assemble the equipment in advance, predict the failure and solve the problem according to the “Fault detection table of the laparoscopic instrument in the operating Room” and the “Log book of the use of the laparoscopic instrument”. In addition, the long-term man-machine fixed mode will make the operator have a sense of responsibility, cherish the endoscope machine more, and take the initiative to find the cause of failure, record and give feedback in time, which not only improves the subjective initiative of the operator but also indirectly improves the economic benefits of the hospital.7 Finally, medical operators can promote the smooth implementation of endoscopic surgery, shorten operation time, improve patient safety, and improve surgical efficiency when they are familiar with the machine and able to deal with sudden failures with ease.8
Fine Management Combined with Fixed Man-Machine Model is Helpful to Improve Doctor Satisfaction
The results showed that after the implementation of fine management combined with man-machine fixed mode, the scores of the observation group in “preoperative preparation, process cooperation, operation proficiency, trouble solving, instrument debugging, timely communication and service attitude” were significantly higher than those of the control group. There were significant improvements in surgical process coordination proficiency, endoscopic equipment operation proficiency, emergency fault handling ability and nurses’ service attitude. The significance of fine management is that the manager provides a set of quantifiable, standardized and easy to implement operating standards, so as to make each department fine and efficient continuous operation, to improve the efficiency of the hospital as the core, to promote patient satisfaction as the goal of the detailed management concept. The concept connotation is the attention to details. According to the concept, this study starts with every detail of instrument management, use and trouble solving, quantifies the responsibility to the person, optimizes and integrates the existing training resources of the hospital, improves the technical content of laparoscopic cooperation of specialist nurses, and improves the surgical cooperation service.9 Laparoscopic instrument is the most valuable and precise instrument among the existing surgical instruments in our hospital. The implementation of fine management combined with man-machine fixed mode helps nurses to quickly and comprehensively grasp the key points of surgical coordination, improve the quality of surgical coordination, and thus improve doctors’ satisfaction. Doctors’ satisfaction and nurses’ satisfaction are mutually promoting. Through the cooperation of competent endoscopic surgery, specialist nurses can effectively predict and solve instrument failures in operation, so as to find a sense of professional belonging in nursing work. Long-term, stable and high-quality cooperation will make nurses recognized and respected by doctors, which is not only conducive to enhancing nurses’ professional identity. It also helps to shape the nursing brand of the operating room.
The Management Mode of Laparoscopic Instruments in the Operating Room Needs to Be Continuously Refined
First of all, laparoscopic instruments are sophisticated in design, complex in structure, expensive and easily damaged, which makes their management relatively difficult. Fine management can ensure the correct use and maintenance of the instrument, extend its service life, reduce the loss rate, and thus save the operating costs of the hospital. In addition, the smooth operation and surgical quality of laparoscopic surgery are directly affected by the performance of laparoscopic instruments. Fine management can ensure that the instrument is in good working condition before the operation and avoid damage during the operation, so as to ensure the smooth operation and the safety of patients. Thirdly, China’s Ministry of Health issued the “Endoscopic Cleaning and disinfection Technical Operating standards”, and laparoscopic and other endoscopic instruments must undergo strict cleaning, disinfection and sterilization treatment to ensure the safety of surgery and aseptic operation.10 This requires the operating room must establish a complete set of laparoscopic instrument management system, the use of instruments, cleaning, disinfection, sterilization, storage and maintenance of the links for fine management. The refined management of laparoscopic instruments in the operating room in this study is also in line with the requirements of national industry standards and is an important measure to ensure the quality of surgery and patient safety.
Limitations
First, this study was a single-center study that only explored the use of four laparoscopic instruments. The effectiveness of this method in the management of other equipment is not verified. Second, the observational indicators in this study were the attrition rate of laparoscopic instrument and the doctor satisfaction rate, which were not comprehensive enough. Third,the problems in this study originated from clinical practice. In order to better simulate the actual clinical situation and quickly evaluate the effectiveness of the intervention method, we chose this non-randomized concurrent controlled study method. However, this method has certain limitations. The study subjects were not randomly assigned to the observation group and the control group but were grouped according to the factors of near purchase and the same brand, which exists selection bias and confounding factors, may affect the accuracy of the results to a certain extent. Also, this is an innovation for our department and our hospital, but there is less innovation in nursing management methods, which is also our limitation. The above are the areas we need to improve next time.
Conclusion
The application effect of fine management combined with man-machine fixed mode in reducing the loss rate of laparoscopic instruments is remarkable, which not only improves the management efficiency and service life of laparoscopic instruments but also further guarantees the surgical quality and patient safety. Through the implementation of fine management of laparoscopic instruments, we have established a laparoscopic instrument management system and operation process, including instrument configuration list, card management, registration and so on. At the same time, combined with the man-machine fixed mode, the laparoscopic instrument is fixed with a specific surgical doctor and nurse, ensuring that each user has a deep understanding of the performance and operation requirements of the instrument, thereby reducing the damage caused by improper operation. This is the innovation in the instrument management program of our operating room department, and we will update the information and continuously refine the management in the future. In summary, the application of fine management combined with man-machine fixed mode in reducing the loss rate of laparoscopic instruments has significant advantages and effects, and is worthy of widespread promotion and application in operating room management. In the future, we will continue to improve and optimize this management mode to provide more powerful support for the safe and efficient operation of the operating room.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has no fund assistance.
Disclosure
Shujin Xia and Lina Bai are co-first authors for this study. The authors declare that they have no competing interests in this work.
References
1. White EJ, McMahon M, Walsh MT. et al. A study of laparoscopic instrument use during colorectal surgery. Appl Ergon. 2019;78:301–308. doi:10.1016/j.apergo.2018.02.010
2. de Lion Botero Couto Lopes C, Uchikawa Graziano K, Pinto TDJA. Terezinha de Jesus Andreoli Pinto. Evaluation of single-use reprocessed laparoscopic instrument sterilization. Rev Lat Am Enfermagem. 2011;19(2):370–377. doi:10.1590/s0104-11692011000200020
3. Guoling M. Problems and Countermeasures in the use of laparoscopic instruments. China Medical Device Information. 2019;2019(15):35–36.
4. Meinong Z, Xiaoling L, Qunai H, et al. Application of refined nursing quality management based on goal orientation in surgical ward. Journal of Nursing. 2019;26(10):11–13.
5. Kono E, Taniguchi K, Lee S-W, Ohdaira T, Uchiyama K. Laparoscopic instrument for female surgeons: an innovative model for endoscopic purse-string suture. Minim Invasive Ther Allied Technol. 2022;31(4):642–645. doi:10.1080/13645706.2020.1851724
6. Yang Qiong GUY, Min XU. Application analysis of detail management measures in operating room instrument management. Journal of Traditional Chinese Medicine Management. 2018;26(3):107–109.
7. Bannon R, Gohil R, Manickavasagam J. Laparoscopic instrument use in laryngeal surgery: transoral resection of a supraglottic haemangioma. J Laryngol Otol. 2017;131(9):823–826. doi:10.1017/S0022215117001438
8. Xiaoping L, Yan J, Binfei L, et al. Practice and effect evaluation of link management in improving operating efficiency of operating room. Journal of Nursing. 2018;25(22):21–24.
9. Yinghui H. Application of Diversified Teaching in Cultivating Students’ Clinical thinking Ability. Nursing Research. 2014;2014(34):4325–4327.
10. China’s Ministry of Health. Endoscopic Cleaning and disinfection Technical Operating standards. 2004. [EB/OL][Reference date 2024-10-22][No. 100].
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.