Back to Journals » Drug Design, Development and Therapy » Volume 19
The Adjunctive Effect of Quercetin on Postoperative Pain Management Following Cesarean Section: A Randomized Controlled Study
Authors Mohamed Elmokadem E, Khaled Abou El Fadl D, Bassiouny AM, Mahmoud MMAE, Samy M, El Said NO ![]()
Received 4 March 2025
Accepted for publication 7 July 2025
Published 14 July 2025 Volume 2025:19 Pages 6009—6024
DOI https://doi.org/10.2147/DDDT.S526188
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Tin Wui Wong
Eman Mohamed Elmokadem,1,* Dina Khaled Abou El Fadl,1,* Ahmed M Bassiouny,2,3 Maisa Mohamed Abd Elkhalik Mahmoud,4 Mohammed Samy,5 Nouran Omar El Said1,*
1Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, Future University in Egypt, Cairo, Egypt; 2Department of Radiodiagnosis, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Department of Radiology, Quantum Radiology, Sydney, New South Wales, Australia; 4Department of Anesthesia, El Matarya Teaching Hospital, Cairo, Egypt; 5Department of Obstetrics and Gynecology, Faculty of Medicine, Ain Shams University, Cairo, Egypt
*These authors contributed equally to this work
Correspondence: Nouran Omar El Said, Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, Future University in Egypt, 90th Street, New Cairo, Cairo, 12311, Egypt, Tel +201006526452, Email [email protected]
Purpose: Post-cesarean section pain management remains a crucial challenge in obstetric care, with implications for maternal recovery, mother-child bonding, and long-term health outcomes. Quercetin, a naturally occurring flavonoid with anti-inflammatory and antioxidant properties, has shown promising analgesic effects in preclinical studies but has limited clinical evidence for acute pain management. This study aimed to assess the efficacy of preoperative Quercetin administration on acute post-operative pain following cesarean section.
Patients and Methods: In this prospective, double-blinded, randomized controlled trial, 80 patients undergoing elective cesarean section under spinal anaesthesia were randomly allocated to receive either 500 mg oral Quercetin (n=40) or matching placebo (n=40) one hour before surgery. The primary outcome was postoperative pain intensity assessed using a 10 cm Visual Analog Scale (VAS) at 2, 6, 12, and 24 hours after surgery. Secondary outcomes included time to first analgesic request, total morphine consumption, incidence of postoperative nausea and vomiting, time to physical activity initiation, functional activity, patient satisfaction, and adverse effects.
Results: The Quercetin group demonstrated significantly lower VAS scores at all measured time points (p< 0.001) and delayed time to first analgesic request (3.9± 1.3 vs 2.73± 0.78 hours, p< 0.001) compared to the placebo group. Additionally, patients receiving Quercetin initiated physical activity significantly earlier (15.2± 1.9 vs 19.03± 2.66 hours, p< 0.001) and reported higher satisfaction levels on postoperative day 2 (p=0.042). However, total morphine consumption, functional activity, incidence of nausea and vomiting, and hospital length of stay were comparable between groups, with no significant differences in adverse effects.
Conclusion: Preoperative administration of 500 mg Quercetin significantly reduced postoperative pain and delayed the need for rescue analgesia following cesarean section, allowing for earlier mobilization without increasing adverse effects. These findings suggest Quercetin may serve as a safe, effective adjunct in multimodal pain management protocols for cesarean delivery.
Clinical Trial Registration: NCT06650891 (2024– 10-21).
Keywords: quercetin, post-cesarean pain, analgesia, flavonoid, postoperative pain management
Introduction
The rate of Cesarean section (C-section) has been increasing over the past decades and now exceeds 32% of births.1 C-section can cause moderate-to-severe postoperative pain in a large percentage of women.2 Effective postoperative pain management is crucial yet challenging, as insufficient pain control can impact a mother’s ability to care for her newborn and impair mother‐child bonding.3 Inadequate postoperative pain management risks chronic pain, increased opioid consumption, impaired recovery, and postpartum depression,4–6 while causing immobility-related complications,7 and economic burdens through extended hospitalizations and readmissions.8,9
Thus, providing adequate pain relief following cesarean delivery is essential to ensure better health outcomes and overall patient satisfaction.3
Oral, intramuscular and intravenous analgesics have been traditionally used to manage acute postoperative pain.10 Opioids, particularly when injected, have been effective in relieving acute pain.11,12 Nevertheless, opioid use is accompanied by dose-related side effects such as respiratory depression, nausea, vomiting, urinary retention, itching, drowsiness, and postoperative ileus.13,14
While opioids are essential for managing pain after surgery, their risk of addiction and fatal overdose means each patient’s risk factors for substance abuse must be carefully assessed before prescribing these medications.15
Consequently, it is crucial to explore compounds that can enhance the analgesic effects of opioids, improving pain control while reducing opioid consumption.16
Natural medicinal plant compounds show promise as safer pain management alternatives with fewer side effects than traditional medications.17 Flavonoids are a significant class of natural products categorized as secondary plant metabolites with polyphenolic structures.18 Commonly found in fruits, vegetables, and natural beverages, they encompass several classes including flavones, flavanones, isoflavones, flavonols, flavanonols, flavan-3-ols, and anthocyanidins.19
Quercetin (3,3′,4′,5,7-pentahydroxyflavone), a flavonoid and polyphenol, is abundantly present in various plants and fruits, including capers, cranberries, figs, red onions, asparagus, radish leaves, walnuts, broccoli, and coriander. This compound possesses distinctive properties that improve physical and mental performance while reducing the risk of infection.20
Quercetin has garnered significant attention from researchers due to its wide range of beneficial properties, including its ability to combat inflammation, neutralize harmful free radicals, regulate blood sugar levels, inhibit cancer cell growth, and protect heart function. Additionally, research suggests quercetin may safeguard liver and brain health, prevent excessive blood clotting, fight bacterial infections, and assist in weight management.21,22
Rising evidence shows Quercetin has antinociceptive effects in various rodent models of chronic pain, including inflammatory, neuropathic, and cancer pain23–25 Anjaneyulu et al first demonstrated that chronic Quercetin treatment significantly effectively reduced both heat hypersensitivity and cold allodynia induced by streptozotocin.26
In chronic constriction injury (CCI)-induced neuropathic pain, Civi et al found Quercetin’s analgesic effect superior to gabapentin and morphine27 Moreover, Quercetin dose-dependently alleviated thermal hyperalgesia and mechanical allodynia in neuropathic pain associated with paclitaxel use by stabilizing mast cell membranes, preventing excessive histamine release, and blocking protein kinase C epsilon type (PKCε) and transient receptor potential vanilloid-1 (TRPV1) activation.28
Kaur et al revealed that co-administering low doses of Quercetin with clonidine (α2-agonist) produces synergistic analgesic effects by modulating adrenergic pathways.29
The sigma-1 receptor is critical in chronic pain generation and maintenance.3,30,31 And Espinosa-Juarez et al demonstrated that sigma-1 receptor antagonists potentiated Quercetin’s antinociceptive effect in CCI-induced neuropathic pain.32
Literature indicates Quercetin exerts analgesic effects by suppressing neuroinflammation and oxidative stress while modulating synaptic plasticity, GABAergic, and opioidergic systems.33
For cancer pain, Quercetin showed good analgesic activity in Ehrlich tumor-induced hyperalgesia by inhibiting interleukin −1 (IL-1β) and tumor necrosis factor-α (TNF-α) production.34 Li et al demonstrated that chronic Quercetin treatment ameliorated bone cancer pain by suppressing peripheral and central sensitization.35
Additionally, Quercetin may prevent excess bleeding, decrease inflammation, initiate early fibrinolysis, and prevent adhesions after gynecological surgery in female Wistar Hannover rats,36 while also inhibiting fibroblast proliferation and reducing surgery-induced epidural fibrosis.37
As its safety is well established, Quercetin has great potential for clinical use in pain treatment. However, there are limited clinical studies on the effect of Quercetin on acute or chronic pain. Only one study reported that 500 mg Quercetin daily supplementation for 8 weeks resulted in improvements in clinical symptoms, disease activity, high-sensitivity tumor necrosis factor-α (hs-TNFα), and health assessment questionnaire in women with rheumatoid arthritis.38
Therefore, the current study is designed to assess the efficacy of preoperative Quercetin administration in acute post-operative pain following cesarean section.
Materials and Methods
Study Design and Setting
This prospective, double-blinded, randomized controlled trial was conducted in accordance with the Declaration of Helsinki. The study took place at the obstetrics and gynecology unit of Al Matareya Teaching Hospital in Cairo, Egypt.
Ethical Considerations
The study protocol was approved by the Research Ethics Committee of the General Organization for Teaching Hospitals and Institutes (HM000184) and the Research Ethics Committee for Experimental and Clinical Studies, Faculty of Pharmacy, Future University in Egypt (RFC-PH-3/2024) and registered on clinicalTrials.gov (NCT06650891). Written informed consent was obtained from all participants during preoperative appointments before enrollment.
Study Population
The study included pregnant females aged over 18 years with American Society of Anesthesiologists (ASA) physical status I–II, who underwent elective major cesarean section under spinal anesthesia at full-term gestational age. Exclusion criteria comprised a history of seizures, pre-eclampsia or eclampsia, hypertension, use of narcotic analgesics within 24 hours prior to surgery, or medications known to induce neuropathy (eg, amiodarone, metronidazole, phenytoin, colchicine) or interact with the study intervention (eg, fluoroquinolones, loratadine, fexofenadine, alvimopan, armodafinil). Additionally, patients with prolonged cesarean section duration (>90 minutes), increased incision size, intraoperative complications, failed spinal anesthesia requiring conversion to general anesthesia, or contraindications to spinal anesthesia were excluded.
Intervention and Randomization
Participants were randomly allocated to one of two groups using a computer-generated random number sequence. The Quercetin group received 500 mg of oral Quercetin (NOW Foods Egypt) one hour before surgery, while the control group received a matching placebo. All participants, caregivers, and outcome assessors were blinded to group assignments.
Before spinal anesthesia, patients received a 1000 mL crystalloid preload (0.9% normal saline or Ringer’s solution) to minimize hypotension risk. Spinal anesthesia was administered with a 22G or 20G Quincke needle using a midline or paramedian approach, with the bevel oriented laterally. A mixture of 10 mg (2 mL) of 0.5% hyperbaric bupivacaine and 25 μg (0.5 mL) of fentanyl was injected intrathecally at the L4/L5 interspace.
Intraoperative monitoring included continuous electrocardiography (ECG), non-invasive blood pressure (NIBP), peripheral oxygen saturation (SpO2), and end-tidal carbon dioxide (EtCO2). Vital signs were recorded every five minutes for 45 minutes after the block and continuously throughout the procedure.
Postoperative analgesia was initiated with 75 mg intramuscular diclofenac sodium at peritoneal closure, while 4 mg ondansetron hydrochloride was administered after abdominal closure to prevent nausea and vomiting. Patients were monitored in the recovery area for two hours before being transferred to the obstetrics department.
A standard postoperative analgesic strategy was administered to the patients, which included acetaminophen 1 g orally 4 times a day.
Rescue Analgesia Protocol
Patient-controlled analgesia (PCA) with morphine (1 mg/mL) was initiated upon arrival in the post-anesthesia care unit (PACU). The PCA pump (CareVis PCA Pump, Promecon Medical Supplies, Hamburg, Germany) was programmed to deliver a 5 mg bolus dose with a 20-minute lockout interval and a maximum dose of 40 mg within a 4-hour period. Patients were instructed to self-administer a bolus as needed for pain relief. The time to the first rescue analgesia request was recorded.
Outcome Measures and Follow-Up
Preoperative data were collected, including baseline and demographic patient characteristics such as age, gestational age, ASA physical status, surgery duration, and medical history.
Primary Outcome
Postoperative Pain
Postoperative pain intensity was assessed using a 10 cm Visual Analog Scale (VAS) at 2, 6, 12, and 24 hours following surgery. The VAS ranged from 0 cm (no pain) to 10 cm (worst imaginable pain), and scores were assessed by a qualified assessor blinded to the study groups.
Secondary Outcomes
Secondary outcomes included the following:
- Postoperative Nausea and Vomiting (PONV): The occurrence of postoperative nausea and vomiting was monitored at 2, 6, 12, and 24 hours post-surgery.
- Postoperative Symptoms: The incidence of any post-operative symptoms such as pruritus, headache, and backache was recorded. The need for antiemetic medication was also documented for each patient.
- Postoperative Analgesia Assessment: The time to the first request for analgesia was measured in hours from the completion of surgery to the administration of the first rescue analgesic dose. In addition, opioid consumption within 24 hours postoperatively was monitored and recorded for each group.
- Physical and Functional Activity Assessment: The time to initiation of physical activity was recorded. Also, functional activity was assessed by evaluating the patients’ ability to sit with or without assistance, stand with or without assistance, and walk with or without assistance at 24 hours post-surgery.
- Patient Satisfaction Assessment: Patient satisfaction was evaluated on days 1, 2, and 3 postoperatively using a structured questionnaire, with responses categorized into five levels: extremely unsatisfied, unsatisfied, mildly satisfied, satisfied, and extremely satisfied.
- Hospital Length of Stay and Medication Safety: The length of the hospital stay, from admission to discharge, was recorded. Medication safety was assessed by documenting any side effects, including headache and other adverse reactions.
Statistical Analysis
Statistical analysis was done by SPSS version 28 (IBM Co., Armonk, NY, USA). Numerical data were presented as the mean and standard deviation (SD) and analyzed using independent samples t-test or as the median and interquartile range (IQR) and analyzed using Mann Whitney-test. Categorical data were presented as the frequency and percentage and analyzed using Chi-square test or exact test, as appropriate. Time to first analgesic request was analyzed using Kaplan Meier curve with Log rank test. A two tailed P value < 0.05 was considered statistically significant.
The sample size was calculated using G*Power 3.1, with a type-1 error (α) of 5% and power of 90%. Based on a previous study which reported a mean time to first opioid request of 3.53 ± 1.51 hours in the intervention group and 2.03 ± 1.73 hours in the placebo group, a minimum of 26 participants per group (52 total) was required.39 To account for potential dropouts and enhance power in detecting clinically relevant differences between groups, 40 participants were enrolled in each group (80 total).
Results
Patient recruitment was conducted at the obstetrics unit from November 2024 to February 2025. A total of 138 patients were initially screened for eligibility. Of these, 80 eligible patients were randomly allocated in a 1:1 ratio to either the Quercetin group (n=40) or the placebo group (n=40). All randomized patients completed the study protocol and were included in the final analysis, with no dropouts in either group (Figure 1).
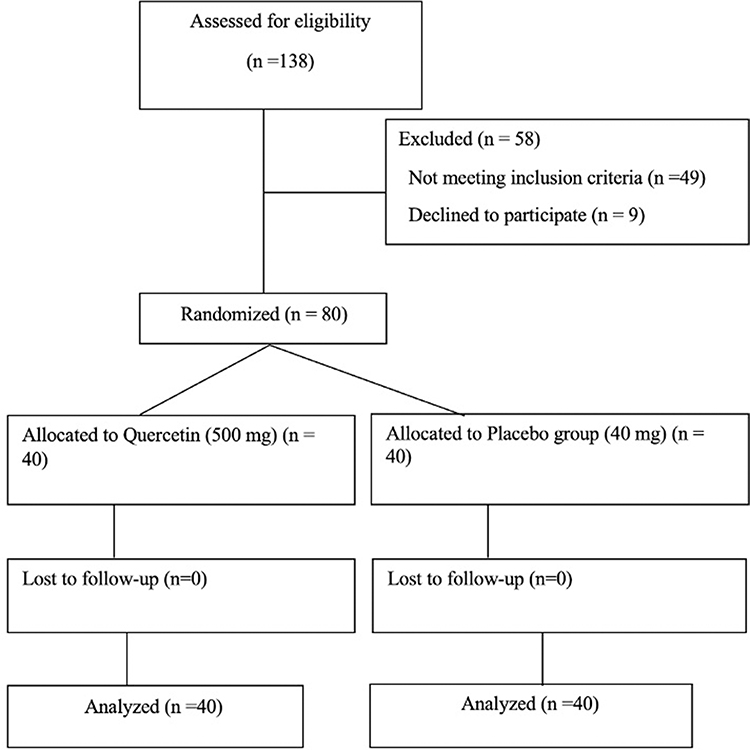 |
Figure 1 CONSORT flowchart. |
Baseline and Demographic Characteristics
As shown in Table 1, there was no statistically significant difference between the two studied groups in terms of age, gestational age, ASA physical status, duration of surgery and medical history.
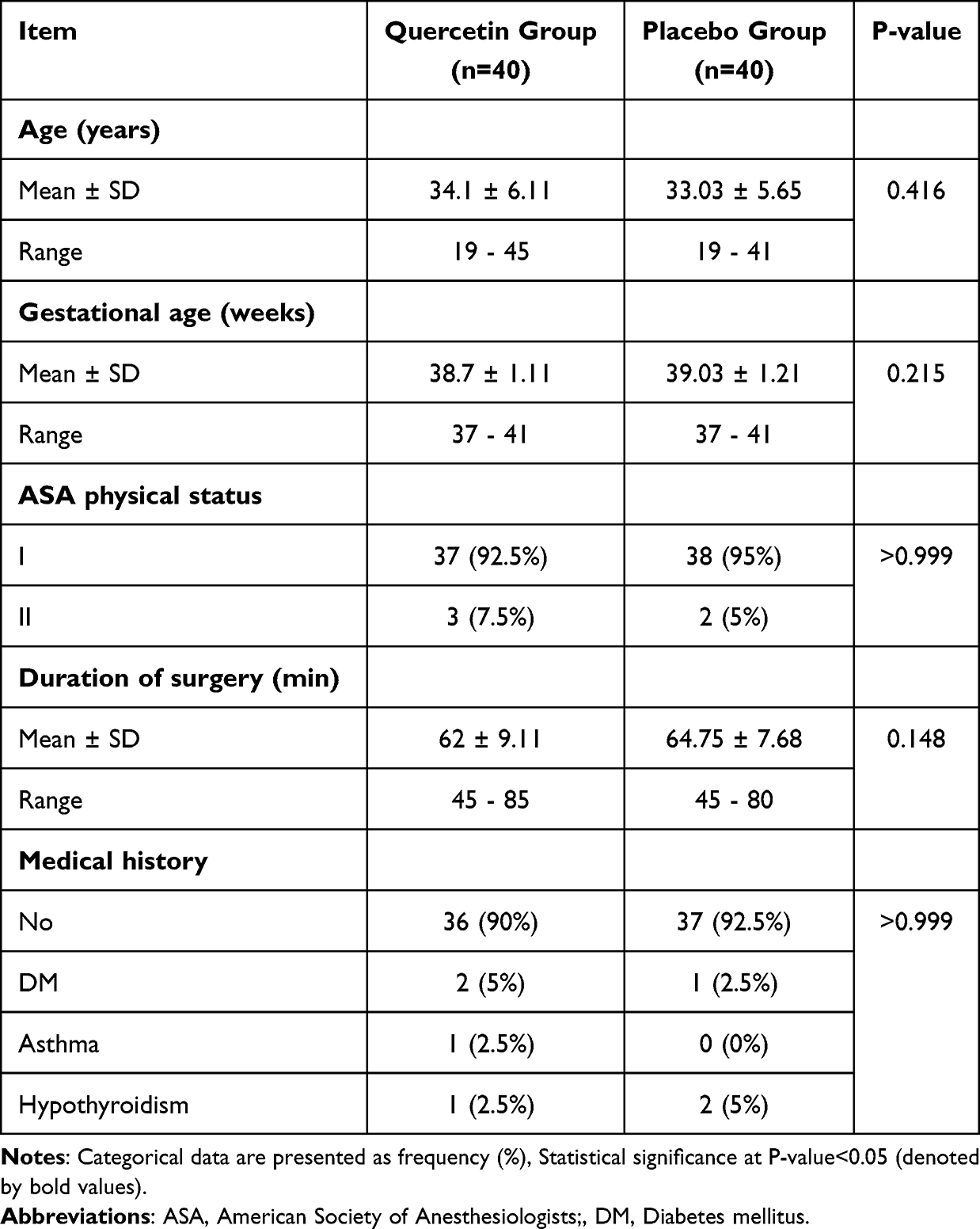 |
Table 1 Baseline Characteristics of the Studied Groups |
Postoperative Pain, PONV, and Postoperative Symptoms
VAS was significantly lower in Quercetin group than placebo (P<0.001) after 2 hours, 6 hours, 12 hours and 24 hours postoperatively. The percentage of patients who suffered nausea was 12.5% in Quercetin group vs 17.5% in placebo group after 2 hours, 12.5% vs 15% after 6 hours, 7.5% vs 10% after 12 hours and 5% vs 7.5% after 24 hours while that of patients who suffered vomiting was 5% vs 7.5% after 2 hours and 0% vs 2.5% after 6 hours, and those differences were not statistically significant. Moreover, the incidence of pruritus, headache and backache was respectively 5% in Quercetin group vs 7.5% in placebo group, 17.5% vs 17.5% and 25% vs 27.5%, with no statistically significant differences. Furthermore, the percentage of patients who were prescribed antiemetics was insignificantly different between the two groups [Table 2, Figures 2 and 3].
 |
Table 2 Postoperative Parameters of the Studied Groups |
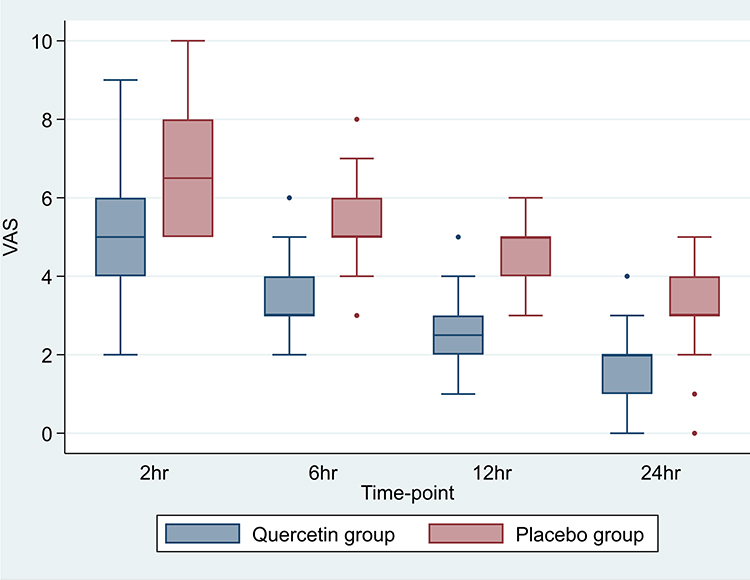 |
Figure 2 Comparison of VAS scores in the studied groups. |
 |
Figure 3 The incidence of nausea and vomiting in the studied group. |
Postoperative Analgesia
Analgesic request was significantly delayed in Quercetin group than placebo, with a mean of 3.9 ± 1.3 vs 2.73 ± 0.78 hours (P<0.001). The result of Log rank test was consistent with that of unpaired t-test (P<0.001), with hazard ratio of 0.22 (95% CI: 0.11 to 0.42) for Quercetin group as shown in Figure 4
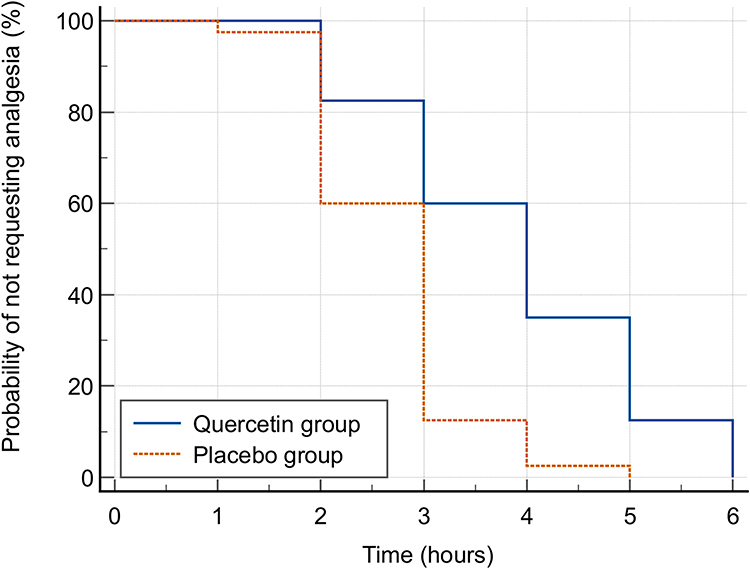 |
Figure 4 Kaplan-Meier curve analysis for time to first analgesic request. |
The mean morphine intake in 24 hours was 58.3 ± 6.48 mg in Quercetin group vs 58.9 ± 6.2 mg in placebo group, denoting no statistically significant difference [Table 3 and Figure 5].
 |
Table 3 Analgesic Intake of the Studied Groups |
 |
Figure 5 Morphine intake during 24 hrs. |
Physical & Functional Activity and Patient Satisfaction
Start of physical activity was significantly earlier in Quercetin group than placebo (P<0.001) with a mean of 15.2 ± 1.9 vs 19.03 ± 2.66 hours. As regards to functional activity reported after 24 hours, it was comparable between both groups, with 20% of Quercetin group vs 22.5% of placebo group being able to sit without assistance, 30% vs 37.5% being able to stand with assistance and 20% vs 15% being able to stand without assistance [Table 4].
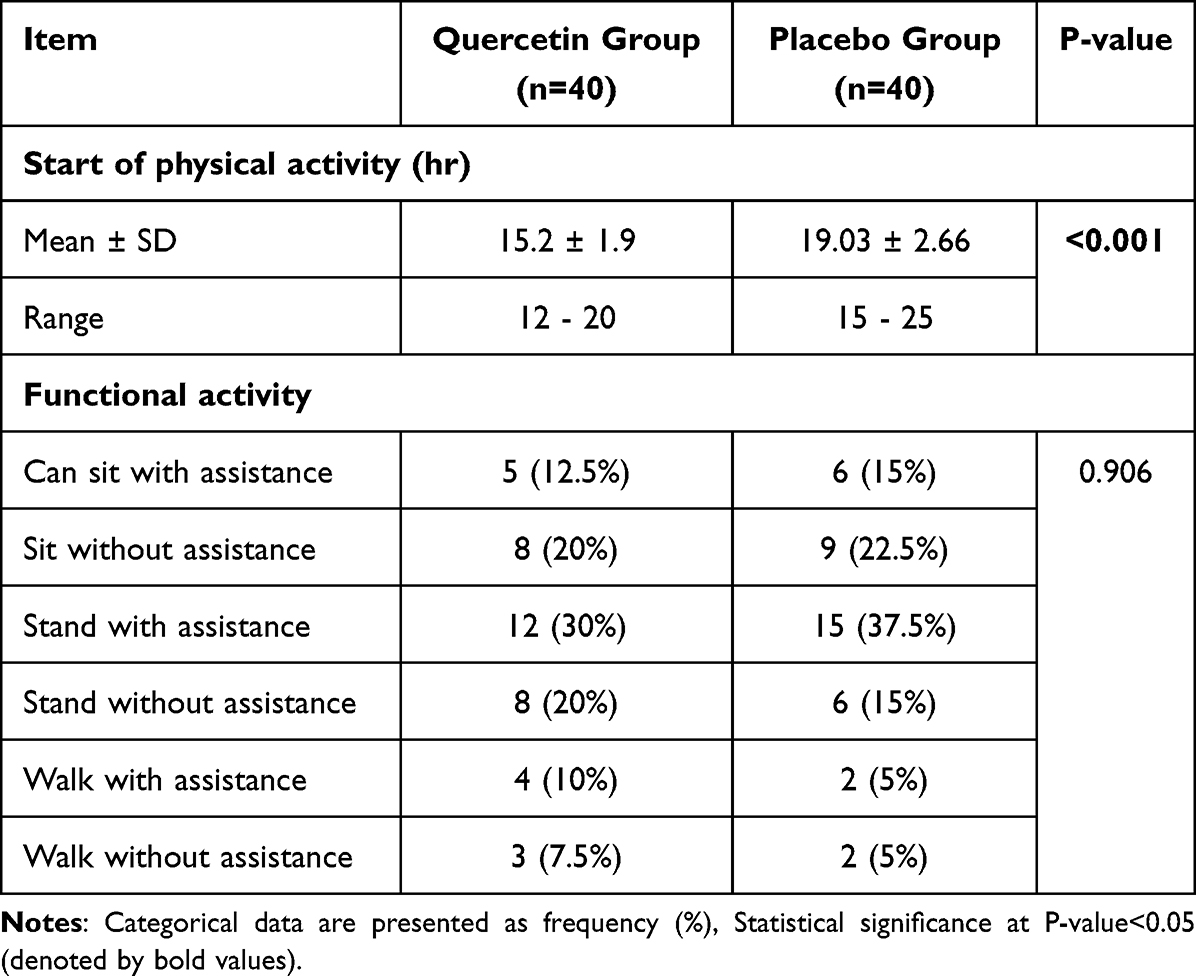 |
Table 4 Physical and Functional Activity of the Studied Groups |
Patient satisfaction was similar between both groups at day 1 postoperatively. On the other hand, satisfaction level was significantly higher in Quercetin group than placebo after 2 days (P=0.042), with 20% vs 45% being satisfied and 60% vs 45% being extremely satisfied. After 3 days, the satisfaction was comparable between both groups, with 72.5% of Quercetin group vs 57.5% of placebo group being extremely satisfied [Table 5 and Figure 6].
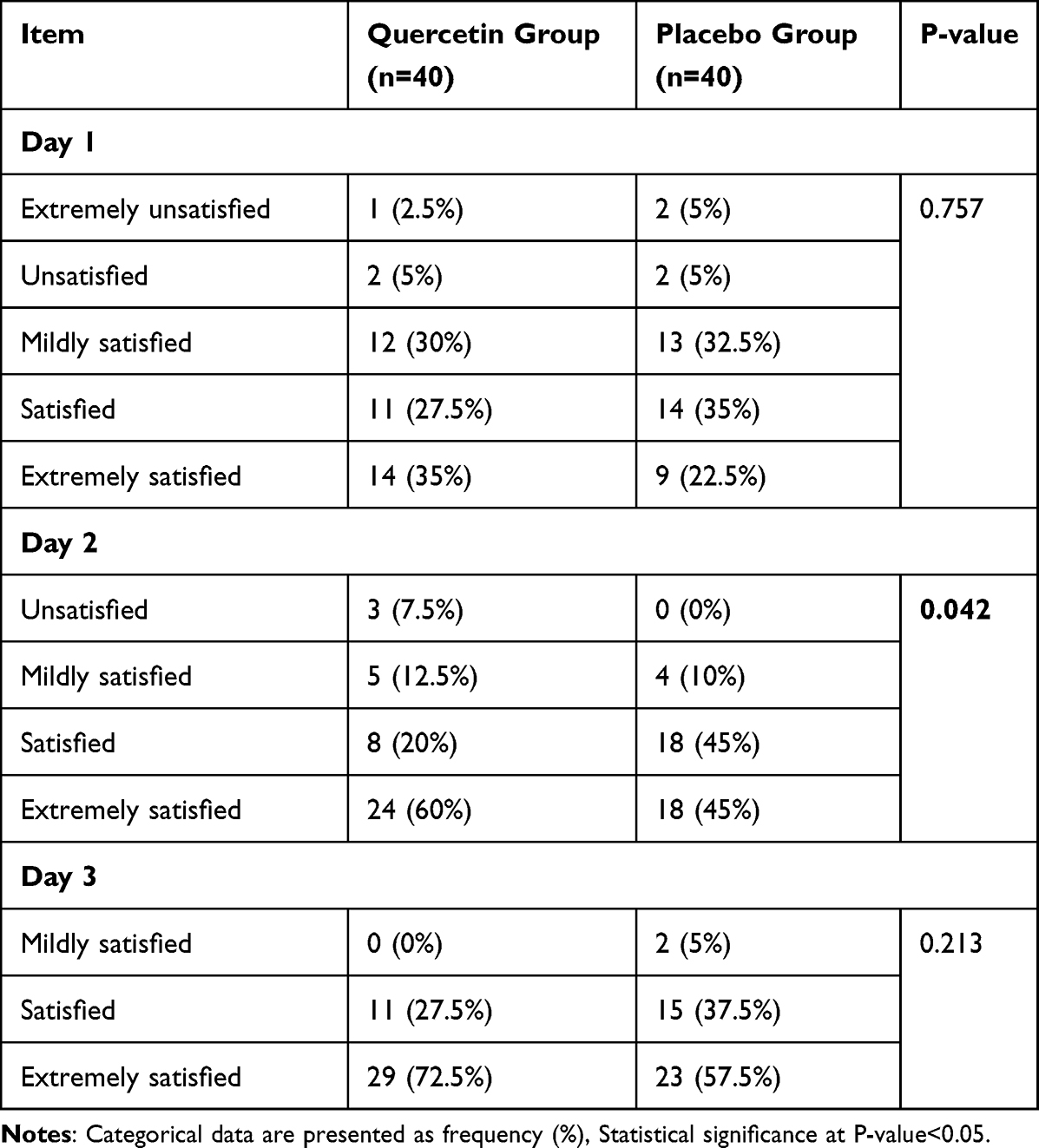 |
Table 5 Patient Satisfaction in the Studied Groups |
 |
Figure 6 Patient satisfaction level. |
Hospital Length of Stay and Medication Safety
As demonstrated in Table 6, hospital stay was comparable in both the Quercetin and placebo groups (P=1). Noteworthy, 17.5% of each group had headaches, and epigastric symptoms were similar in both groups as side effects of medications.
 |
Table 6 Hospital Stay and Medication Side Effects in the Studied Groups |
Discussion
Quercetin has demonstrated promising anti-nociceptive properties in chronic pain and shown potential benefits in post-surgical recovery through its anti-inflammatory and fibrinolytic effects in various animal models. While clinical evidence is currently limited to one study showing improved outcomes in rheumatoid arthritis patients, Quercetin’s well-established safety profile makes it a promising candidate as an adjuvant analgesic for post-operative pain management.38
This randomized controlled trial evaluated the efficacy of Quercetin for post-operative pain management and recovery outcomes following cesarean section. Our findings demonstrate that Quercetin administration significantly improved post-operative pain control with a favorable safety profile.
The most notable finding was the significant reduction in post-operative pain scores across all time points in the Quercetin group. VAS scores were lower at 2, 6, 12, and 24 hours post-operation compared to the placebo group. This analgesic effect was further evidenced by the significantly delayed time to the first analgesic request in the Quercetin group (3.9 hours versus 2.73 hours, p<0.001), suggesting that Quercetin reduced the likelihood of early analgesic requirement. These findings may be explained by previous literature reports demonstrating Quercetin’s anti-inflammatory and analgesic properties, potentially mediated by inhibiting pro-inflammatory cytokines and oxidative stress pathways. Furthermore, animal studies indicate the impact of Quercetin on the modulation of the opioid system to potentiate morphine’s analgesic effects.26
Similarly, a study compared the analgesic efficacy of different Melatonin doses (5 mg vs 10 mg) against placebo in post-cesarean pain management. They reported that a higher dose of Melatonin (10 mg) provides more effective post-surgical pain control compared to a lower dose (5 mg) or placebo and prolonged time before requiring pain medication. The 10 mg Melatonin dose demonstrated significant pain control at all time points (6, 12, and 24 hours post-surgery), while the 5 mg Melatonin dose only showed significantly better pain control than placebo at 6 and 12 hours, indicating a dose-dependent analgesic effect of Melatonin.39
Another clinical study investigated the analgesic efficacy of preoperative melatonin and vitamin C in major abdominal surgery. The research demonstrated that both melatonin (6 mg) and vitamin C (2 g), administered orally one hour before surgery, significantly improved postoperative pain management compared to placebo. Both interventions showed comparable efficacy in reducing pain scores.40
Quercetin shares similar mechanisms with Melatonin and Vitamin C in postoperative pain management due to their common antioxidant properties. All three reduce pro-inflammatory cytokines and oxidative stress while increasing endogenous antioxidant defenses. Despite acting through different pathways (Quercetin and Melatonin via receptor-mediated mechanisms, Vitamin C by direct antioxidant effects), they demonstrate comparable efficacy as adjuvant analgesics in postoperative pain protocols.41–44
Interestingly, unlike previous studies with Vitamin C and Melatonin, which demonstrated reduced postoperative morphine consumption, our investigation found that Quercetin, while effectively lowering pain scores and delayed analgesic request time, did not significantly decrease total morphine consumption over 24 hours compared to placebo (58.3 mg versus 58.9 mg, p=0.673). This may be attributed to the fact that our protocol allowed unrestricted access to morphine through PCA, allowing patients to manage pain proactively. This approach, despite prioritizing patient comfort, may have led patients to use morphine before severe pain occurred, possibly masking the true differences in opioid needs between the groups. Future studies might benefit from implementing a different analgesic regimen to better elucidate Quercetin’s opioid-sparing effects. Additionally, the single 500mg dose of Quercetin may have been insufficient to significantly reduce the opioid needs after cesarean. Like Melatonin, which showed better results at higher doses, Quercetin might require multiple or higher doses to reduce morphine use.39 Nevertheless, the improved pain scores with unchanged morphine consumption suggest Quercetin may boost the effectiveness of standard pain treatment rather than directly reducing opioid needs. Higher doses may be investigated in future trials.
A particularly promising finding was the significantly earlier initiation of physical activity in the Quercetin group (15.2 hours versus 19.03 hours, p<0.001). This accelerated mobilization could be attributed to better pain control in the early postoperative period. However, this advantage did not translate into differences in functional activity or hospital length of stay. This suggests that while Quercetin may facilitate earlier mobilization, other factors may play more dominant roles in determining functional recovery and discharge timing. The return of normal physiological functions like bowel movements and achievement of mobility goals as well as the development of postpartum complications, play crucial roles in determining hospital stay duration45,46. Similar to our Quercetin findings, both 5mg and 10mg doses of Melatonin significantly reduced time to physical movement compared to placebo.39
Patient satisfaction data revealed an interesting temporal pattern. While satisfaction was comparable between groups on day 1, the Quercetin group reported significantly higher satisfaction on day 2, with 80% of patients being satisfied or extremely satisfied compared to 90% in the placebo group (p=0.042). This difference normalized by day 3, suggesting that Quercetin’s greatest impact on patient experience may occur during the intermediate postoperative period.
Regarding safety, the incidence of PONV was comparable between groups, with no significant differences in antiemetic requirements. This may be attributed to the comparable opioid use by patients from both groups. Other post-operative symptoms, including pruritus, headache, and backache, occurred at similar rates in both groups. The comparable incidence of medication-related headaches and epigastric discomfort in both groups suggests that Quercetin is safe with minimal adverse effects like those associated with standard post-operative care.47,48
Study Limitations
Despite the promising findings of this study, several limitations should be acknowledged, the use of a single dose of Quercetin suggests that higher doses may be necessary to observe significant effects on secondary outcomes. Additionally, the small sample size may limit the generalizability of the findings. The study population was restricted to patients undergoing cesarean sections, which may not reflect outcomes in other surgical procedures. Furthermore, the short follow-up period also restricted the assessment of long-term effects.
To address these limitations, future research should include larger, more diverse patient populations and evaluate the impact of different dosing regimens. Extending the follow-up period would help determine whether the observed benefits persist beyond the immediate postoperative phase.
Conclusion
In conclusion, this study highlights the potential of Quercetin in reducing postoperative pain and prolonging the request for analgesia, suggesting its role as a complementary, safe approach to pain management. The findings support its efficacy, paving the way for further research to optimize dosing and explore its broader clinical applications.
Abbreviations
C-section, Cesarean section; VAS Visual Analog Scale; CCI, chronic constriction injury; PKCε, protein kinase C epsilon type; TRPV1, transient receptor potential vanilloid-1; IL-1β, interleukin −1; TNF-α, tumor necrosis factor-α; hs-TNFα, high-sensitivity tumor necrosis factor-α; ASA American Society of Anesthesiologists; ECG, electrocardiography; NIBP, non-invasive blood pressure; SpO2, peripheral oxygen saturation; EtCO2, end-tidal carbon dioxide; PCA, Patient-controlled analgesia; PACU, post-anesthesia care unit; PONV, Postoperative Nausea and Vomiting.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Research Ethics Committee of the General Organization for Teaching Hospitals and Institutes (HM000184) and the Research Ethics Committee for Experimental and Clinical Studies, Faculty of Pharmacy, Future University in Egypt (RFC-PH-3/2024).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research and/or authorship of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Betran AP, Ye J, Moller A-B, Souza JP, Zhang J. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health. 2021;6(6):e005671. doi:10.1136/bmjgh-2021-005671
2. Granot M, Lowenstein L, Yarnitsky D, Tamir A, Zimmer EZ. Postcesarean section pain prediction by preoperative experimental pain assessment. Anesthesiology. 2003;98(6):1422–1426. doi:10.1097/00000542-200306000-00018
3. Aryafar M, Bozorgmehr R, Gholami F, Farazmehr K, Alizadeh R. A randomized double-blind clinical trial evaluating the effect of elastic stocking on hemodynamic changes and dose use of ephedrine for elective cesarean surgery under spinal anesthesia. Int J Surg Open. 2020;27:58–63. doi:10.1016/j.ijso.2020.10.019
4. Shen D, Hasegawa-Moriyama M, Ishida K, Fuseya S, Tanaka S, Kawamata M. Acute postoperative pain is correlated with the early onset of postpartum depression after cesarean section: a retrospective cohort study. J Anesth. 2020;34(4):607–612. doi:10.1007/s00540-020-02789-5
5. Sutton CD, Carvalho B. Optimal pain management after cesarean delivery. Anesthesiol Clin. 2017;35(1):107–124. doi:10.1016/j.anclin.2016.09.010
6. Komatsu R, Ando K, Flood PD. Factors associated with persistent pain after childbirth: a narrative review. Br J Anaesth. 2020;124(3):e117–e130. doi:10.1016/j.bja.2019.12.037
7. Pillitteri A. Maternal_Child_Health_Nursing. In: Maternal & Child Health Nursing: Care of the Childbearing & Childrearing Family,
8. Gadsden J, Hart S, Santos AC. Post-cesarean delivery analgesia. Anesth Analg. 2005;101(5S):S62–S69. doi:10.1213/01.ANE.0000177100.08599.C8
9. Twersky R, Fishman D, Homel P. What happens after discharge? Return hospital visits after ambulatory surgery. Anesth Analg. 1997;84(2):319–324. doi:10.1097/00000539-199702000-00014
10. Puntillo F, Giglio M, Varrassi G. The routes of administration for acute postoperative pain medication. Pain Ther. 2021;10(2):909–925. doi:10.1007/s40122-021-00286-5
11. Unlugenc H, Vardar MA, Tetiker S. A comparative study of the analgesic effect of patient-controlled morphine, pethidine, and tramadol for postoperative pain management after abdominal hysterectomy. Anesth Analg. 2008;106(1):309–312. doi:10.1213/01.ane.0000287815.32869.2a
12. Habibi MR, Masoomi S, Godazandeh GA, Emadi SA, Akhbari P, Nooraee SM. The effect of magnesium sulphate on postoperative pain and opioid consumption in inguinal hernia surgery. J Mazandaran Univ Med Sci. 2012;21(86):168–173.
13. Tramer MR, Schneider J, Marti RA, Rifat K. Role of magnesium sulfate in postoperative analgesia. Anesthesiology. 1996;84(2):340–347. doi:10.1097/00000542-199602000-00011
14. Alizadeh R, Aghsaeifard Z, Abbasvandi F, Hazrati E. Evaluation of clinical and non-clinical parameters among partial and total mastectomy patients. Int J Surg Open. 2020;27:130–135. doi:10.1016/j.ijso.2020.11.007
15. Santa Cruz Mercado LA, Liu R, Bharadwaj KM, et al. Association of intraoperative opioid administration with postoperative pain and opioid use. JAMA Surg. 2023;158(8):854. doi:10.1001/jamasurg.2023.2009
16. Alizadeh R, Aghsaeifard Z, Alavi N, Abbasvandi F, Khanigarabadi A. A cross-sectional study on the postoperative analgesic-associated side effects and clinical parameters following partial mastectomy. Int J Surg Open. 2020;27:114–118. doi:10.1016/j.ijso.2020.10.018
17. Duran P, Loya‐López S, Ran D, et al. The natural product argentatin C attenuates postoperative pain via inhibition of voltage‐gated sodium and T‐type voltage‐gated calcium channels. Br J Pharmacol. 2023;180(9):1267–1285. doi:10.1111/bph.15974
18. Panche AN, Diwan AD, Chandra SR. Flavonoids: an overview. J Nutr Sci. 2016;
19. Ferraz CR, Carvalho TT, Manchope MF, et al. Therapeutic potential of flavonoids in pain and inflammation: mechanisms of action, pre-clinical and clinical data, and pharmaceutical development. Molecules. 2020;25(3):762. doi:10.3390/molecules25030762
20. Zhao L, Wang H, Du X. The therapeutic use of quercetin in ophthalmology: recent applications. Biomed. Pharmacother. 2021;137:111371. doi:10.1016/j.biopha.2021.111371
21. Soofiyani SR, Hosseini K, Forouhandeh H, et al. Quercetin as a novel therapeutic approach for lymphoma. Oxid Med Cell Longev. 2021;2021(1). doi:10.1155/2021/3157867
22. Abo-EL-Sooud K, Abd-Elhakim YM, Hashem MMM, El-Metwally AE, Hassan BA, El-Nour HHM. Ameliorative effects of quercetin against hepatic toxicity of oral sub-chronic co-exposure to aluminum oxide nanoparticles and lead-acetate in male rats. Naunyn Schmiedebergs Arch Pharmacol. 2023;396(4):737–747. doi:10.1007/s00210-022-02351-y
23. Grewal AK, Singh TG, Sharma D, et al. Mechanistic insights and perspectives involved in neuroprotective action of quercetin. Biomed. Pharmacother. 2021;140:111729. doi:10.1016/j.biopha.2021.111729
24. Ghafouri-Fard S, Shabestari FA, Vaezi S, et al. Emerging impact of quercetin in the treatment of prostate cancer. Biomed. Pharmacother. 2021;138:111548. doi:10.1016/j.biopha.2021.111548
25. Narenjkar J, Roghani M, Alambeygi H, Sedaghati F. The effect of the flavonoid quercetin on pain sensation in diabetic rats. Basic Clin Neurosci. 2011;2.
26. Anjaneyulu M, Chopra K. Quercetin attenuates thermal hyperalgesia and cold allodynia in STZ-induced diabetic rats. Indian J Exp Biol. 2004;42(8):766–769.
27. Çivi S, Emmez G, Dere ÜA, Börcek AÖ, Emmez H. Effects of quercetin on chronic constriction nerve injury in an experimental rat model. Acta Neurochir. 2016;158(5):959–965. doi:10.1007/s00701-016-2761-0
28. Gao W, Zan Y, Wang ZJJ, Hu XY, Huang F. Quercetin ameliorates paclitaxel-induced neuropathic pain by stabilizing mast cells, and subsequently blocking PKCε-dependent activation of TRPV1. Acta Pharmacol Sin. 2016;37(9):1166–1177. doi:10.1038/aps.2016.58
29. Kaur R, Singh D, Chopra K. Participation of α 2 receptors in the antinociceptive activity of quercetin. J Med Food. 2005;8(4):529–532. doi:10.1089/jmf.2005.8.529
30. Choi SR, Han HJ, Beitz AJ, Lee JH. Intrathecal interleukin-1β decreases sigma-1 receptor expression in spinal astrocytes in a murine model of neuropathic pain. Biomed. Pharmacother. 2021;144:112272. doi:10.1016/j.biopha.2021.112272
31. Ruiz-Cantero MC, González-Cano R, Tejada MÁ, et al. Sigma-1 receptor: a drug target for the modulation of neuroimmune and neuroglial interactions during chronic pain. Pharmacol Res. 2021;163:105339. doi:10.1016/j.phrs.2020.105339
32. Espinosa‐Juárez JV, Jaramillo‐Morales OA, Déciga‐Campos M, Moreno‐Rocha LA, López‐Muñoz FJ. Sigma‐1 receptor antagonist potentiates the antinociceptive effect of quercetin in neuropathic pain induced by chronic constriction injury. Drug Dev Res. 2021;82(2):267–277. doi:10.1002/ddr.21750
33. Liu C, Liu DQ, Tian YK, et al. The emerging role of quercetin in the treatment of chronic pain. Curr Neuropharmacol. 2022;20(12):2346–2353. doi:10.2174/1570159X20666220812122437
34. Calixto-Campos C, Corrêa MP, Carvalho TT, et al. Quercetin reduces Ehrlich tumor-induced cancer pain in mice. Anal Cell Pathol. 2015;2015:1–18. doi:10.1155/2015/285708
35. Li Z, Zhang J, Ren X, Liu Q, Yang X. The mechanism of quercetin in regulating osteoclast activation and the PAR2/TRPV1 signaling pathway in the treatment of bone cancer pain. Int J Clin Exp Pathol. 2018;11(11):5149–5156.
36. Güney G, Kaya C, Oto G, Yıldırım S, Özdemir H, Tokmak A. Effects of quercetin and surgicel for preventing adhesions after gynecological surgery: a rat uterine horn model. J Obstetrics Gynaecol Res. 2017;43(1):179–184. doi:10.1111/jog.13185
37. Cao Y, Chen H, Sun Y, Fan Z, Cheng H. Quercetin inhibits fibroblasts proliferation and reduces surgery-induced epidural fibrosis via the autophagy-mediated PI3K/Akt/mTOR pathway. Bioengineered. 2022;13(4):9973–9986. doi:10.1080/21655979.2022.2062530
38. Javadi F, Ahmadzadeh A, Eghtesadi S, et al. The effect of quercetin on inflammatory factors and clinical symptoms in women with rheumatoid arthritis: a double-blind, randomized controlled trial. J Am Coll Nutr. 2017;36(1):9–15. doi:10.1080/07315724.2016.1140093
39. Kiabi FH, Emadi SA, Jamkhaneh AE, Aezzi G, Ahmadi NS. Effects of preoperative melatonin on postoperative pain following cesarean section: a randomized clinical trial. Ann Med Surg. 2021;66. doi:10.1016/j.amsu.2021.102345
40. Laflı Tunay D, Türkeün Ilgınel M, Ünlügenç H, Tunay M, Karacaer F, Biricik E. Comparison of the effects of preoperative melatonin or vitamin C administration on postoperative analgesia. Bosn J Basic Med Sci. 2019. doi:10.17305/bjbms.2019.4379
41. Rebec GV, Christopher Pierce R. A vitamin as neuromodulator: ascorbate release into the extracellular fluid of the brain regulates dopaminergic and glutamatergic transmission. Prog Neurobiol. 1994;43(6):537–565. doi:10.1016/0301-0082(94)90052-3
42. Lu R, Kallenborn-Gerhardt W, Geisslinger G, Schmidtko A. Additive antinociceptive effects of a combination of vitamin C and vitamin E after peripheral nerve injury. PLoS One. 2011;6(12):e29240. doi:10.1371/journal.pone.0029240
43. Chen WW, Zhang X, Huang WJ. Pain control by melatonin: physiological and pharmacological effects. Exp Ther Med. 2016;12(4):1963–1968. doi:10.3892/etm.2016.3565
44. El-Shenawy SM, Abdel -salam OME, Baiuomy AR, EL-Batan S, Arbid MS. Studies on the anti-inflammatory and anti-nociceptive effects of melatonin in the rat. Pharmacol Res. 2002;46(3):235–243. doi:10.1016/S1043-6618(02)00094-4
45. Blumenfeld Y, El-Sayed Y, Lyell D, Nelson L, Butwick A. Risk factors for prolonged postpartum length of stay following cesarean delivery. Am J Perinatol. 2015;32(09):825–832. doi:10.1055/s-0034-1543953
46. Van Otterloo L, Connelly C, Gould J, Abreo A, Main E. Mothers at risk. J Perinatal Neonatal Nurs. 2018;32(4):303–314. doi:10.1097/JPN.0000000000000342
47. Han MK, Barreto TA, Martinez FJ, Comstock AT, Sajjan US. Randomised clinical trial to determine the safety of quercetin supplementation in patients with chronic obstructive pulmonary disease. BMJ Open Respir Res. 2020;7(1):e000392. doi:10.1136/bmjresp-2018-000392
48. Andres S, Pevny S, Ziegenhagen R, et al. Safety aspects of the use of quercetin as a dietary supplement. Mol Nutr Food Res. 2018;62(1). doi:10.1002/mnfr.201700447
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.