Back to Journals » Drug Design, Development and Therapy » Volume 20
The 90% Minimum Effective Dose of Oxycodone for Thoracoscopic Lobectomy in Elderly Patients: A Double-Blind Study Using a Biased-Coin Design
Authors Li S, Pan X, Zhu Y ![]() , Liu J, Li Z, Gao X, Chai J
, Liu J, Li Z, Gao X, Chai J
Received 18 October 2025
Accepted for publication 30 January 2026
Published 19 February 2026 Volume 2026:20 560051
DOI https://doi.org/10.2147/DDDT.S560051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Si Li,1 Xuanyuan Pan,1 Youzhuang Zhu,2 Jie Liu,1 Zhichao Li,1 Xin Gao,1 Jun Chai1
1Department of Anesthesiology, Shengjing Hospital of China Medical University, Shenyang, 110122, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Hospital of Qingdao University, Qingdao, 266071, People’s Republic of China
Correspondence: Jun Chai, Department of Anesthesiology, Shengjing Hospital of China Medical University, No. 36, Sanhao St, Heping District, Shenyang, 110122, People’s Republic of China, Tel +86 24-9661568401, Email [email protected]
Purpose: Postoperative pain significantly impairs recovery in elderly patients. Oxycodone is widely used in the postoperative period due to its favorable safety profile and low risk of respiratory depression. To determine the minimum effective dose of intravenous oxycodone, administered in combination with postoperative patient-controlled intravenous analgesia, that achieves at least 90% efficacy in elderly patients undergoing video-assisted thoracoscopic surgery.
Patients and Methods: We enrolled participants aged 65 and older who underwent thoracoscopic lobectomy. Oxycodone was administered 30 minutes before the completion of the surgical procedure. The initial dose was 0.02 mg/kg. Subsequent dose adjustments were determined based on the previous patient’s response using a biased coin design. The dose interval was 0.01 mg/kg. A positive response was defined as an NRS score ≤ 3 at cough 2 hours postoperatively. The study was terminated after 45 successful responses. Secondary endpoints included postoperative pain assessed at various time points up to hospital discharge, adverse events, sedation levels, and the occurrence of chronic pain during the postoperative period.
Results: A total of sixty patients were enrolled. Among elderly patients undergoing elective VATS with multimodal analgesia, the ED90 of oxycodone was 0.104 mg/kg (95% CI: 0.095– 0.108 mg/kg). The supplementary analysis focused on patients who received at least 0.09 mg/kg of oxycodone. After adjusting for imbalanced baseline characteristics, the incidence of chronic pain in the 0.09 mg/kg dose group was significantly higher than in the 0.10 mg/kg dose group (P = 0.007).
Conclusion: For thoracoscopic lobectomy in elderly individuals aged > 65 years, the ED90 of oxycodone was 0.104 mg/kg (95% CI: 0.095– 0.108 mg/kg).
Keywords: ED90, oxycodone, elderly, chronic pain, video-assisted thoracoscopic surgery
Introduction
The incidence of lung cancer in the elderly population has been steadily increasing, accounting for 66.7% of all newly diagnosed cases.1,2 According to the World Health Organization (WHO), lung cancer is the leading cause of cancer-related mortality and a major contributor to cancer incidence worldwide, accounting for 26% of all cancer-related deaths.3 As a result, thoracoscopic lobectomy has become the preferred surgical approach for lung cancer treatment, with the number of procedures steadily increasing. However, thoracoscopic surgery is associated with significant postoperative pain. Inadequate pain control not only increases the risk of adverse events, such as postoperative pulmonary complications and delirium, but may also contribute to the development of chronic pain, thereby substantially impairing the patient’s quality of life.4
Oxycodone, an agonist of both μ and κ opioid receptors, exerts potent analgesic effects, particularly in the treatment of neuropathic and visceral pain. It has a rapid onset of action, with analgesia beginning within 2 to 3 minutes after intravenous administration and reaching peak effect at 5 minutes.5 Studies have shown that, compared to other opioid medications, low-dose oxycodone has minimal hemodynamic impact in elderly patients, demonstrating superior cardiovascular and respiratory safety.6 Furthermore, oxycodone does not induce histamine release and lacks parasympathetic inhibitory effects, thereby facilitating early recovery in postoperative patients. It is particularly well-suited for pain management during the perioperative period of thoracoscopic surgery in elderly patients.7
Additionally, studies have shown that hepatic and renal function progressively decline with advancing age in elderly patients.2,4 On this basis, age-related alterations in the pharmacokinetic and pharmacodynamic profiles of oxycodone are observed in elderly patients, which may result in increased drug sensitivity. To achieve effective perioperative analgesia while minimizing the risk of potential adverse effects, it is essential to individualize dosing strategies for elderly patients. This dose optimization holds significant clinical implications and is crucial for ensuring both the safety and therapeutic efficacy of analgesic regimens in this vulnerable population.
The Dixon up-and-down method (UDM) is widely used to estimate the median effective dose (ED50) of a drug. However, for anesthesiologists, the clinically more relevant objective is to determine the optimal effective dose (ED90). The biased coin design (BCD) for directly estimating ED90 is considered to provide superior estimation accuracy and methodological advantages, thereby enhancing its suitability for determining the optimal dose in perioperative analgesia and anesthetic interventions.8–12 Therefore, this study aims to use the statistically robust BCD to determine the ED90 of oxycodone in perioperative multimodal analgesia for patients aged 65 and older undergoing thoracoscopic lobectomy, with the goal of improving patient satisfaction and reducing the incidence of adverse events.
Materials and Methods
Study Design and Participant Methods
This double-blind, sequentially allocated trial was approved by the Ethics Committee of Shengjing Hospital, China Medical University (approval number: 2023PS023K; principal investigator: Xiaoyu Ma; approval date: 11 January 2023) and registered with the Chinese Clinical Trial Registry (ChiCTR2300071956). Written informed consent was obtained from all participants before enrollment, and the study was conducted in full accordance with the ethical principles outlined in the Declaration of Helsinki.
After obtaining written informed consent, we enrolled patients who underwent unilateral selective thoracoscopic lobectomy at Shengjing Hospital, China Medical University, from June to December 2023. Inclusion criteria were age > 65 years, ASA classification 1–3, and body mass index between 18.5 and 28.0 kg/m2. Exclusion criteria included asthma or other respiratory diseases; premedication use; known allergy or hypersensitivity to study medications; history of chronic pain; significant cardiopulmonary, hepatic, or renal disease; cognitive impairment; inability or unwillingness to provide informed consent; and premature discontinuation of the study protocol, including unexpected conversion from minimally invasive thoracic surgery to open thoracotomy, withdrawal of consent, or postoperative admission to the intensive care unit (ICU) for prolonged mechanical ventilation.
Randomization and Blinding
All study medications were prepared by a non-blinded investigator who was not involved in anesthesia administration, perioperative management, or data collection and analysis. Doses were independently verified by an anesthesiologist external to the study team. The allocation sequence was kept in a sealed, opaque envelope that remained with the patient and could be opened only for emergency unblinding in the event of a medical emergency. On the day of surgery, a nurse unaffiliated with patient care opened the sealed envelope containing the study group assignment, prepared the study medication outside the operating room, and diluted oxycodone with saline to a final volume of 10 mL. Data collection was managed by three independent investigators. To prevent investigators from inferring the administered oxycodone dose, they were assigned random codes (“1,” “2,” or “3”), and one investigator was randomly selected for each data collection session. If a patient was enrolled but later excluded from the analysis due to protocol deviations, the next recruited participant received the same dose assignment as the excluded patient. This approach preserved the original allocation sequence and ensured the accuracy of the ED90 estimation. In the event of unexpected serious adverse events—such as circulatory failure, impaired consciousness, or respiratory depression—that required urgent intervention, unblinding was performed by unblinded personnel. In this double-blind trial, both patients and study personnel involved in anesthesia management or data collection remained unaware of whether oxycodone was administered.
Anesthetic Procedures
Before entering the operating room, all patients received standardized instructions on patient-controlled intravenous analgesia (PCIA) and the Numeric Rating Scale (NRS) for pain assessment. They were also informed about potential postoperative discomfort to reduce preoperative anxiety. Upon entering the operating room, mean blood pressure (MBP) and heart rate (HR) were measured twice, and the averages served as baseline measurements (T0). Non-invasive blood pressure (NIBP), including systolic, diastolic, and mean arterial pressure (MAP); HR; pulse oximetry-derived oxygen saturation (SpO2); and the bispectral index (BIS) were continuously monitored, with data recorded at 5-minute intervals.
General anesthesia was induced with sufentanil (0.3 μg/kg), etomidate (0.2 mg/kg), and rocuronium bromide (0.6 mg/kg). After induction, a double-lumen endobronchial tube was inserted to facilitate lung isolation, and isolation was confirmed by fiberoptic bronchoscopy. During maintenance, patients received sevoflurane (0.8–1.5 MAC) with continuous intravenous infusions of propofol (4–6 mg/kg/h) and remifentanil (0.1–0.2 μg/kg/h) to maintain blood pressure and heart rate within ±20% of baseline and to keep the bispectral index (BIS) between 40 and 60. Intermittent rocuronium boluses were given to maintain muscle relaxation during surgery. Mechanical ventilation was managed as follows: during two-lung ventilation, tidal volume was set at 6–8 mL/kg, respiratory rate at 12 breaths/min, and positive end-expiratory pressure (PEEP) at 5 cmH2O; end-tidal carbon dioxide (EtCO2) was maintained at 35–45 mmHg, and peak airway pressure remained below 20 mmHg. During one-lung ventilation, tidal volume was reduced to 4–6 mL/kg, respiratory rate increased to 14–16 breaths/min, PEEP was maintained at 5 cmH2O, EtCO2 was controlled to ≤45 mmHg, and peak airway pressure was limited to ≤30 mmHg. Vasopressors were administered as clinically indicated, guided by continuous hemodynamic monitoring. In cases of severe bradycardia (HR <45 beats/min) or hypotension (defined as a decrease in systolic or mean arterial pressure ≥20% from baseline), atropine (0.3–0.5 mg) or ephedrine (6–10 mg) was administered at the clinician’s discretion. All patients received a standardized intraoperative infusion of Ringer’s lactate solution at 10 mL/kg/h.
All surgeries were performed by equally qualified surgeons. A predefined 10-mL dose of oxycodone was injected at the initiation of thoracic irrigation, approximately 30 minutes before the end of surgery. SBP, MAP, and HR were recorded on admission to the operating room (T0), after intubation (T1), before and after drug administration (T2 and T3), after extubation (T4), and before leaving the operating room (T5). Local infiltration analgesia was administered by a trained surgeon with 5 mL of 0.5% ropivacaine during chest closure. At the end of the procedure, patients awoke spontaneously and were extubated once extubation criteria were met. The total doses of remifentanil and propofol, blood loss, fluid transfusion, and surgery duration were recorded.
Postoperative Pain Management
The PCIA contained nalbuphine hydrochloride (0.2 mg/kg), flurbiprofen axetil (100 mg), and ramosetron hydrochloride (0.6 mg), dissolved in 100 mL of 0.9% sodium chloride solution (2 mL/hour, lockout interval 15 minutes, 0.5 mL per dose). After completing the 2-hour postoperative NRS assessment, if the NRS score was ≥4, a single PCIA bolus was administered. If rescue analgesia was required before the assessment was completed, the patient was excluded from the study.
After discontinuation of the PCIA pump, rescue analgesia (one tablet of oral Tylox) was provided if the patient’s NRS score was ≥4 or the patient actively requested analgesia. If severe adverse events such as nausea and vomiting, respiratory depression (respiratory rate <6 breaths/min or SpO2 <92% while receiving 5 L/min oxygen via nasal cannula), urinary retention, dizziness, or itching occur, the PCIA should be suspended.13,14 The PCIA pump may be restarted only once symptoms have resolved, following appropriate management by an experienced clinician.
Postoperative Follow-Up
Postoperatively, NRS and RASS scores were assessed at 2, 6, 12, and 24 hours after the patient returned to the ward, during both rest and coughing. Adverse events occurring within 72 hours of the first dose—including nausea, vomiting, dizziness, respiratory depression, and delirium—were recorded.15–18 The use and frequency of rescue analgesics were also documented. Key postoperative clinical milestones, such as time to ambulation, time to drain removal, and length of hospital stay (from surgery completion to discharge), were meticulously recorded.
All patients were followed up via telephone questionnaire to collect their NRS scores and Brief Pain Inventory (BPI) results.
Biased-Coin Design
The biased-coin up-and-down sequential design was used to assess the minimum effective dose of oxycodone required to produce effective analgesia in 90% of patients. This statistical method has been widely applied in clinical research. Postoperative NRS scores > 3 during coughing at 2 hours post-surgery were classified as negative responses, whereas NRS scores ≤3 were classified as positive responses.19 Based on previous studies conducted by other investigators, the initial oxycodone dose was set at 0.02 mg/kg.20,21 The dose for the next patient is determined by the analgesic response of the previous patient, following the classic Dixon’s up-and-down sequential design but with modified allocation probabilities. If the previous patient exhibits a negative response, the oxycodone dose for the next patient is increased by 0.01 mg/kg. If the response is positive (ie, effective analgesia), the next patient is randomized to receive either a dose 0.01 mg/kg lower than the previous one, with a probability of 0.11, or the same dose, with a probability of 0.89 (1 − ß).
Patients excluded due to protocol deviations or removed after enrollment were not included in the analysis and therefore did not affect the estimation of ED90. Dose allocation was implemented using Microsoft Excel (Microsoft Corp., Redmond, WA, USA).
Outcomes
The primary objective was to determine the ED90 of intravenously administered oxycodone in elderly patients, given 30 minutes before the completion of thoracoscopic lobectomy, that achieves a 90% effective analgesic response.
Secondary outcomes included the incidence of acute pain during hospitalization, the incidence of chronic pain at 1 and 3 months postoperatively, perioperative hemodynamic changes, RASS scores within 24 hours postoperatively, opioid-related adverse events within 3 days postoperatively (including itching, nausea, and respiratory depression), surgical duration (defined as the time from skin incision to procedure completion), time to first ambulation, time to drain removal, length of postoperative hospital stay, dosage and frequency of rescue analgesics, and intraoperative propofol and remifentanil consumption.
Statistical Analysis
Due to the inherent characteristics of the biased-coin design, including non-independent dose allocation and an unknown distribution, traditional sample size calculation methods are no longer applicable. To estimate the ED90, at least 45 patients (the smallest multiple of 9 greater than 40) who exhibited positive pain responses were required. To determine the minimum effective dose for 90% of patients, we used the R software developed by Pace and Stylianou. This software enabled us to obtain the isotonic regression estimator μ3 by applying the pool-adjacent-violators algorithm (PAVA) and to derive a bias-corrected 95% confidence interval through bootstrapping.22,23 Statistical analysis was performed using dedicated software, R version 4.0.5 (ISBN; http://www.Rproject.org).
The exploratory endpoint supplementary analysis was limited to doses administered to at least 10 participants. Continuous variables were assessed for normality using the Kolmogorov–Smirnov test. Data were presented as mean ± standard deviation (SD), median (interquartile range), or frequency (%), as appropriate. Differences in continuous variables across the three dose groups were evaluated with the Kruskal–Wallis test. Categorical data were compared with the chi-squared test or Fisher’s exact test. Repeated-measures data (NRS and BPI scores at various time points) were analyzed with generalized estimating equations (GEE). Because baseline characteristics (age, gender, preoperative diagnosis, surgical side, comorbidities, and smoking status) differed between groups, we conducted a sensitivity analysis using logistic regression to model pain occurrence and linear regression to model NRS scores, adjusting for potential bias from imbalanced covariates. If key model assumptions (homoscedasticity or Gaussian distribution in linear models) were not met, data transformations and/or alternative generalized linear models were applied as appropriate, adjusting for baseline scores and including the aforementioned variables as covariates. Perioperative hemodynamic differences were analyzed with repeated-measures analysis of covariance (ANCOVA), with baseline measurements included as covariates. Statistical analysis was performed using SPSS version 26 (SPSS Inc., Chicago, Illinois, USA), and P-values <0.05 were considered statistically significant.
Results
A total of 60 patients completed the study; four were excluded, including three who underwent conversion to open thoracotomy during surgery and one who refused follow-up midway through the study (Figure 1). All patients completed telephone follow-up at 1 and 3 months postoperatively, with no loss to follow-up.
 |
Figure 1 Flow chart of the study. |
The study sample included 26 male patients (43.3%). The mean age was 69.92 ± 3.81 years, with a mean body weight of 65 ± 13 kg and a mean height of 164.93 ± 7.83 cm, yielding a mean BMI of 23.51 ± 2.50 kg/m2 (Table 1).
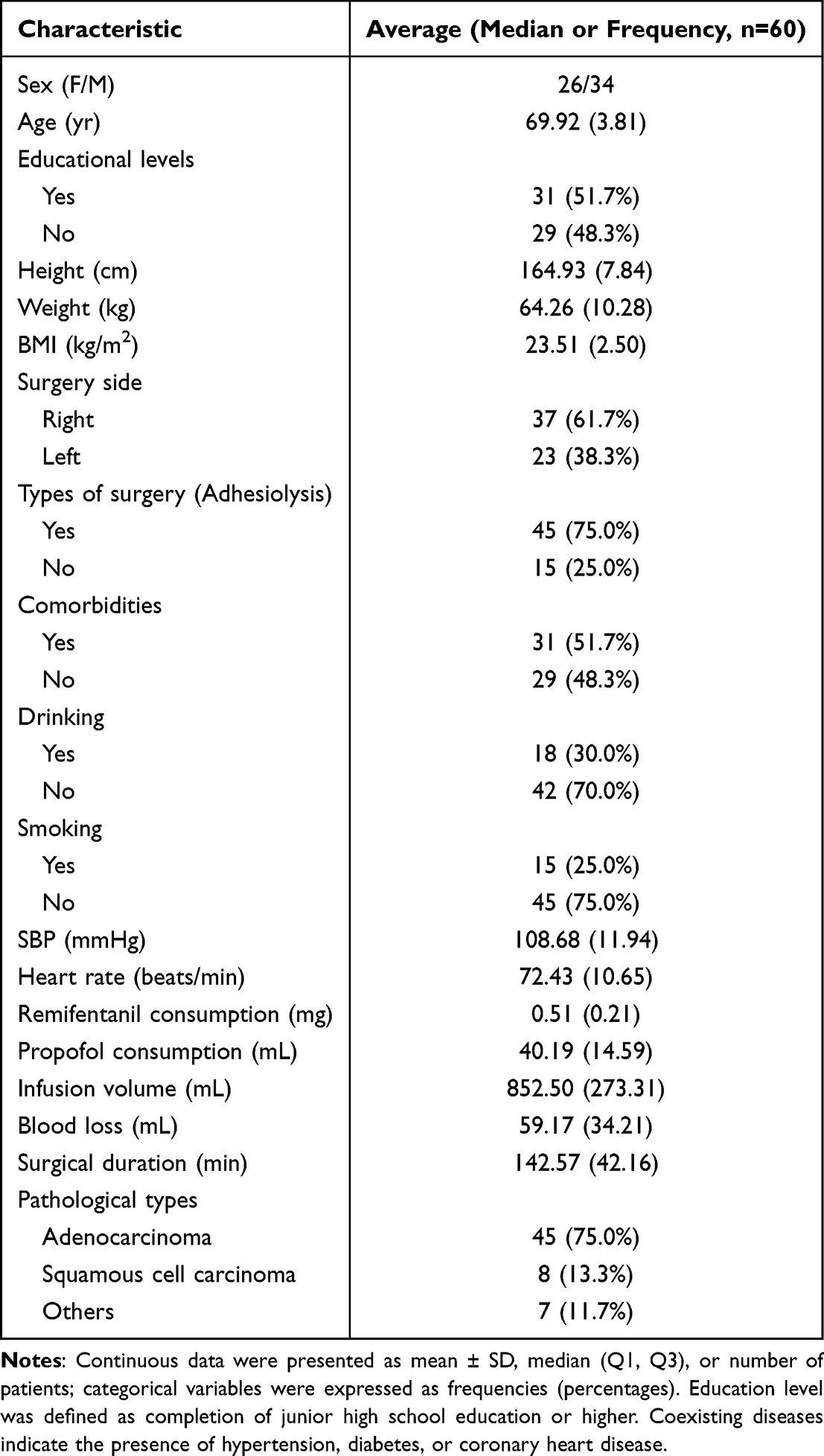 |
Table 1 Patient Demographics |
Table 2 presents the observed response rates according to oxycodone dose. Fifteen patients (25.0%) had inadequate postoperative analgesia, and eight required supplemental oral analgesics. Among the doses examined, the 0.10 mg/kg group had the largest number of patients, 24, and 87.5% of them met the established criteria for analgesic efficacy.
 |
Table 2 Pain Relief Observed After Oxycodone Administration |
The ED90 of oxycodone, determined by isotonic regression, was 0.104 mg/kg, with a 95% confidence interval of 0.095–0.108 mg/kg (Figure 2).
 |
Figure 2 Sequences of successes (total circles) and failures (empty circles) in the 60 consecutive patients. The x-axis represents the subject sequence number, indicating the chronological order of participant enrollment in the BCD. The y-axis shows the range of oxycodone doses administered, spanning from 0.02 to 0.11 mg/kg. The horizontal line indicates the model-estimated optimal oxycodone dose corresponding to the ED90 (ie, the dose predicted to produce effective analgesia in 90% of participants); error bars represent the 95% CI around this estimate. |
The supplementary analysis was limited to dose groups with at least 10 participants. Patients were categorized into three dose-based subgroups: Group A (0.09 mg/kg), Group B (0.10 mg/kg), and Group C (0.11 mg/kg). Preoperative baseline characteristics were generally comparable across groups, except for sex (P = 0.020), age (P < 0.001), height (P = 0.002), surgical side (P = 0.025), comorbidities (P < 0.001), and smoking history (P = 0.021), which showed statistically significant differences. There were no significant differences in BMI among groups (P = 0.867); therefore, height was excluded from the sensitivity analysis (Table 3).
 |
Table 3 Preoperative Comparison |
Repeated-measures analysis of variance was conducted on perioperative hemodynamic parameters and postoperative sedation levels, and no statistically significant time effects or time-by-group interaction effects were observed for any of the measured variables. Among these parameters, MAP was significantly lower in Group A than in Groups B and C at the time of administration (P < 0.001). In contrast, heart rate and RASS sedation scores did not differ significantly across the three groups at any time point (P > 0.05). GEE was used to assess within- and between-group differences in NRS pain scores, and the timing of assessment significantly affected all measured outcomes. However, after adjusting for baseline characteristics, the differences in NRS scores during coughing at various time points were not statistically significant among groups A, B, and C (P > 0.05, Figure 3). The static NRS scores showed a significant interaction effect (P < 0.001). However, there were no differences in the interventions among the groups at any time (P > 0.05).
 |
Figure 3 NRS scores at cough and rest at various time points. The time points t1, t2, t3, t4, t5, t6, and t7 correspond to the immediate postoperative period, 2 hours, 6 hours, 12 hours, 24 hours, 72 hours, and just before discharge, respectively. |
Participants were followed up by telephone to assess the incidence of postoperative chronic pain. To assess the robustness of the results, a sensitivity analysis was performed on dynamic NRS pain scores across different time points and subgroups. The incidence of pain in group A was 2.514 times higher than that in group B (P = 0.007), and the incidence of pain was lower at three months postoperatively compared with one month postoperatively (B = 0.986, P = 0.001). The physiological and emotional disturbances associated with pain were evaluated. Results showed that BPI scores were consistently low across all groups, with no statistically significant differences among groups (P > 0.05). Furthermore, BPI scores at 3 months postoperatively were significantly lower than those at 1 month postoperatively, indicating a highly significant reduction (P < 0.001) (Figure 4).
 |
Figure 4 Three groups of post-discharge BPI and dynamic NRS scores. ΔAfter adjusting for baseline factors, a significant difference was observed between the 0.09 mg/kg and 0.10 mg/kg groups (P < 0.05). |
A post hoc analysis of NRS scores was also conducted during the three-month period following surgical intervention. Preoperative complications and diagnoses were associated with variations in static NRS scores. After adjusting for baseline characteristics, a statistically significant difference between groups emerged (Wald = 7.469, P = 0.024). Specifically, group B had a 0.607 lower pain score than group A (P = 0.007). The pain score was 0.735 lower at three months post-surgery than at one month post-surgery (Wald = 55.029, P < 0.001) (Table 4).
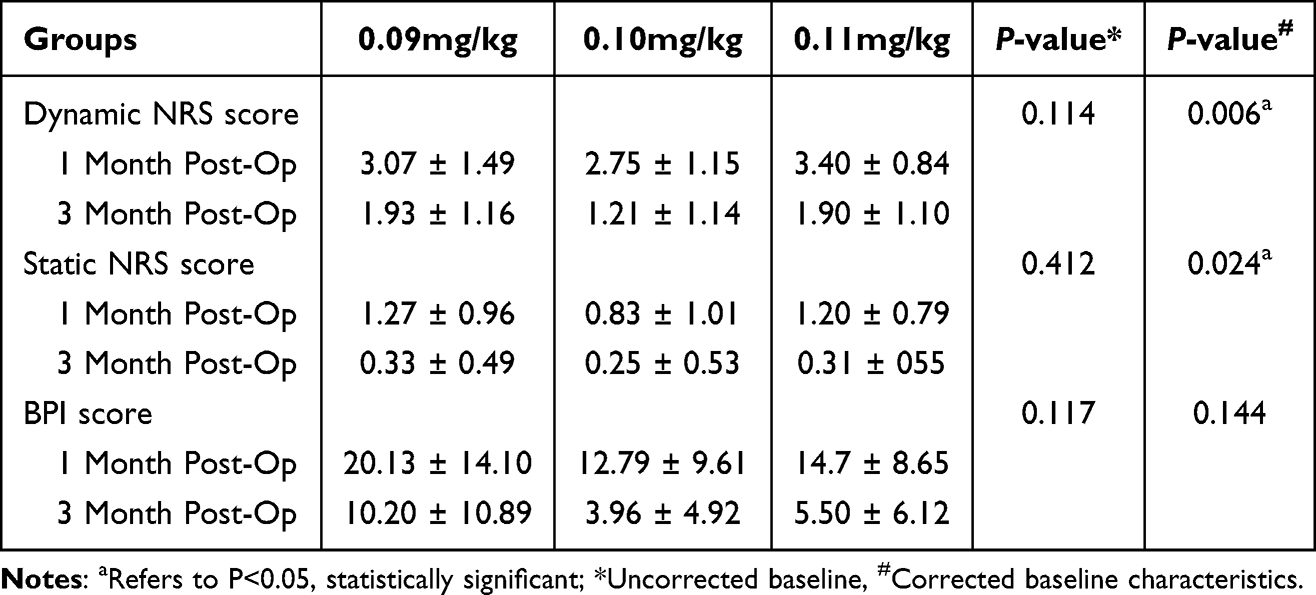 |
Table 4 Comparison of NRS and BPI Scores for Chronic Pain in Three Groups |
Figure 5 illustrates the prevalence of side effects, with no significant differences in the incidence of adverse reactions observed across dose groups (P = 0.291). Constipation was the most common adverse reaction and increased gradually with escalating oxycodone dose across subjects (33.3%, 37.5%, and 70.0%, respectively), showing a statistically significant difference among the three groups (P = 0.038). No patients experienced respiratory depression or other serious adverse events.
 |
Figure 5 Incidence of adverse reactions within 72 hours after surgery. |
Discussion
As the population ages, the number of elderly patients with lung cancer continues to rise, and the proportion undergoing thoracoscopic lobectomy has steadily increased. For these patients, adequate pain management is essential. Inadequate pain relief significantly increases the risk of postoperative pulmonary complications and delirium and may lead to chronic pain, substantially impairing quality of life. However, excessive use of analgesics may also result in opioid-related adverse effects.
Currently, oxycodone is considered more suitable than morphine for postoperative pain management in elderly patients due to its favorable pharmacokinetic profile. However, given the age-related physiological changes in this population, there is an urgent need for pharmacological studies specifically targeting elderly patients to determine the optimal analgesic dose of oxycodone, thereby enabling precise dosing to reduce inadequate pain relief and minimize the occurrence of adverse effects.
This study uses a biased-coin design to determine the optimal effective dose (ED90) of a single intravenous oxycodone dose in elderly patients undergoing thoracoscopic lobectomy, as part of a multimodal perioperative analgesic regimen. Additionally, this study examines factors associated with perioperative acute pain in elderly patients and conducts an exploratory analysis of the incidence of postoperative chronic pain.
Clinicians often refer to a drug’s ED90 to guide dosing. Most studies still use the Dixon up-and-down method to determine the ED50 and then extrapolate it to the ED90. However, this simple extrapolation from the dose-response curve is limited in its ability to accurately reflect the true ED90 of the drug.24 The biased-coin design improves upon the traditional sequential method by adjusting randomization probabilities to converge toward the dose near the ED90, enabling a more intuitive and accurate determination of the drug’s ED90.25
We employed the isotonic regression estimator to derive the ED90 for a single intravenous dose of oxycodone on the dose-response curve. This estimator enables accurate estimation of the effect dose at any quantile along the curve under conditions of low bias and low variance, and has increasingly become a widely adopted approach for determining optimal drug dosing in clinical anesthesia research.8 Additionally, compared to traditional discrete dose-response designs or randomized controlled trials, this method significantly reduces the number of participants required, enabling accurate estimation of the drug’s 90% effective dose with a minimal sample size, while maintaining estimation precision.26
Our study determined the optimal intravenous dose of oxycodone to be 0.104 mg/kg, with a 95% confidence interval of 0.095 to 0.108 mg/kg. An interesting observation emerged from this study: although the ED90 of oxycodone was determined to be 0.104 mg/kg through rigorous statistical analysis, two patients achieved satisfactory analgesia following administration of only 0.02 mg/kg. These individuals reported no pain during hospitalization and did not develop chronic pain during the postoperative follow-up period. The potential factors contributing to the satisfactory analgesia observed in these two patients are as follows. First, both individuals were male. Existing reviews indicate significant sex-based differences in brain structures and functional connectivity involved in pain processing, with females generally exhibiting more widespread neural responses to pain stimuli. This suggests that males may exhibit greater analgesic sensitivity and higher metabolic efficiency when oxycodone is administered, thereby requiring lower doses.27 Second, the pharmacokinetics of oxycodone are influenced by CYP2D6 gene polymorphisms, and carriers of the rapid-metabolizer allele typically demonstrate enhanced analgesic effects. However, genetic testing was not conducted in this study; therefore, the aforementioned speculation requires further validation through targeted research.
An exploratory analysis was conducted across the three dose groups with the largest number of participants to evaluate the clinical benefits of the optimal dose compared to adjacent doses. There were no significant differences among the three oxycodone dose groups in postoperative recovery outcomes, including RASS sedation scores, time to first ambulation, length of hospital stay, and pain incidence. Further analysis of NRS scores from the postoperative period to discharge was conducted. The results showed that 93.3% of patients had a resting NRS score below 4 at discharge, indicating that most patients achieved effective analgesia. After adjusting for baseline imbalances among the three groups, generalized estimating equations were employed to analyze intergroup differences in acute pain and related influencing factors. The results revealed no statistically significant differences in postoperative acute pain scores.
Postoperative chronic pain is defined as pain lasting more than 3 months and not attributable to other causes, such as infection, malignancy, or pre-existing pain conditions. According to the Acute to Chronic Pain Signature (A2CPS) initiative by the National Institutes of Health (NIH), 10% to 70% of patients develop chronic pain after surgery. Pain is one of the strongest predictors of the transition from acute to chronic pain. Across diverse populations, acute postoperative pain reliably predicts the development of chronic postsurgical pain, with robust effect sizes observed for pain at rest, pain during movement, widespread pain, and pain at multiple sites. Additionally, elderly patients often have multiple comorbidities and may require long-term use of various analgesics, thereby increasing the risk of drug tolerance and misuse. Due to the potential injury to the pleura and intercostal nerves caused by thoracoscopic surgery, inadequate postoperative pain management in elderly patients increases the risk of developing chronic pain. Based on these factors, we conducted a long-term follow-up of the subjects to investigate the incidence of chronic pain and evaluate the advantage of the optimal-dose group in reducing the risk of chronic pain development compared with the other two groups.
After excluding baseline (T0) data and adjusting for potential confounding patient characteristics that could influence pain scores, the results showed that the incidence of chronic pain in the optimal-dose group was significantly lower than in the adjacent lower-dose group. Post hoc analysis revealed a significant correlation between chronic pain scores and both the presence of preoperative comorbidities and postoperative complications. A recent meta-analysis showed that the incidence of chronic pain three months after thoracic surgery ranged from 20.0% to 71.4% across 24 studies involving 2400 patients.28 In contrast, 80.6% of the patients in our study experienced only mild pain (NRS < 4) at three months postoperatively, and the pain incidence was significantly lower at three months than at one month (B = 0.986, P = 0.001). In our study, the incidence of chronic postoperative pain was 10%, and cough-induced pain intensity was 1.8 ± 1.3 on the NRS. The results of the prospective study by Bayman et al were notably higher than those of our study: the incidence of chronic pain at three months postoperatively was 29%, and the NRS score during coughing was 2.8 ± 2.2.29 This difference may be attributed to the inclusion of elderly patients in our study population, who typically exhibit reduced pain sensitivity and higher pain thresholds. More importantly, the oxycodone dose administered in our study was close to the optimal effective dose.
Among the 60 patients included in this study, 28 (46.7%) did not experience any opioid-related adverse effects. The incidence of constipation increased with higher oxycodone doses, which is consistent with previous literature, indicating a clear dose-response relationship for this adverse effect. In contrast, no dose-dependent association was observed for other opioid-related adverse effects.30 The incidence of constipation was higher than that of other adverse effects, which may be attributed to the following factors: First, oxycodone’s pharmacological properties determine its mechanism of action. Exogenous opioids bind to μ-opioid receptors in the intestine, impairing gastrointestinal motility and secretory function, thereby causing constipation.31 Hunold et al reported that the incidence of opioid-induced constipation in elderly patients (≥65 years) within one week after emergency department discharge was 21%, compared to 3% in those receiving nonsteroidal anti-inflammatory drugs (NSAIDs).32 Second, elderly patients are at higher risk for constipation. Epidemiological data show that the prevalence of constipation increases with advancing age.33 With aging, neurodegenerative changes in the central nervous system may lead to gastrointestinal motility disorders and hormonal imbalances.
This study followed a rigorous experimental design and implementation protocol, utilizing a standardized multimodal analgesia regimen that combines intraoperative preemptive analgesia, postoperative regional blocks, and PCIA. Compared with the Dixon up-and-down method, the biased-coin up-and-down sequential method provides a more accurate estimate of the optimal analgesic dose (ED90) for a single intravenous dose of oxycodone in elderly patients, thereby ensuring effective analgesia while reducing the incidence of adverse effects. Additionally, this study further explored the impact of acute pain relief on chronic postoperative pain and the potential benefits of optimal analgesic dosing in reducing its incidence.
This study has the following limitations: First, as a single-center design, it may be influenced by site-specific practices, since clinical prescribing patterns can vary across medical centers, limiting the external generalizability of the findings. Second, genetic testing for CYP2D6 polymorphisms was not performed. Although previous studies have shown that this genetic polymorphism can influence the pharmacokinetics of oxycodone, no significant differences in clinical analgesic effects have been observed.34 Additionally, while the biased-coin design can be used to estimate the optimal drug dose, the “optimal” dose derived from this method may not be applicable to all patients. On the one hand, there is individual variability in patients’ analgesic responses; on the other hand, even without accounting for individual factors, the ED90 dose suggests that approximately 10% of patients may not achieve effective analgesia, leading to “ineffective” responses.
Conclusion
The optimal intraoperative intravenous single dose of oxycodone for achieving the effective dose for elderly patients undergoing elective thoracoscopic lobectomy was 0.104 mg/kg (95% CI: 0.095–0.108 mg/kg). In the exploratory analysis, patients receiving this dose had a lower incidence of postoperative adverse effects and a reduced incidence of chronic pain during follow-up.
Abbreviations
ASA, American Society of Anesthesiologists; A2CPS: Acute to Chronic Pain Signature; ANCOVA, analysis of covariance; BPI, Brief Pain Inventory; ED90, the 90% minimum effective dose; GEE, generalized estimating equations; ICU, intensive care unit; MAC, minimal alveolar concentration; NIH: National Institutes of Health; NRS, numerical rating scale; PACU, post-anesthesia care unit; PAVA, pool adjacent violators algorithm; PCIA, patient-controlled intravenous analgesia; PEEP, positive end-expiratory pressure; PONV, postoperative nausea and vomiting; SD, standard deviation; SpO2, pulse-derived oxygen saturation; UDM, The Dixon Up-Down Method; VATS, video-assisted thoracoscopic surgery; WHO, World Health Organization.
Data Sharing Statement
All the data in the manuscript are available upon reasonable request from the corresponding author.
Acknowledgments
Assistance with the study: The authors would like to thank Professor Shanyan Gao of the Department of Epidemiology at Shengjing Hospital of China Medical University for her valuable contributions to the statistical analysis. We also gratefully acknowledge the medical and nursing staff for their role in patient care and for collecting and reporting the protocol-required data throughout the trial.
Funding
This study was supported by the Key Research and Development Program of Liaoning Province (2020JH2/10300129).
Disclosure
The authors report no conflicts of interest in this study.
References
1. Lim E, Harris RA, McKeon HE, et al. Impact of video-assisted thoracoscopic lobectomy versus open lobectomy for lung cancer on recovery assessed using self-reported physical function: VIOLET RCT. Health Technol Assess. 2022;26(48):1–13. doi:10.3310/THBQ1793
2. Luciani C, Scacchi A, Vaschetti R, et al. The uniportal VATS in the treatment of stage II pleural empyema: a safe and effective approach for adults and elderly patients-a single-center experience and literature review. World J Emerg Surg. 2022;17(1):46. doi:10.1186/s13017-022-00438-8
3. Castillo M. An overview of perioperative considerations in elderly patients for thoracic surgery: demographics, risk/benefit, and resource planning. Current Opinion Anaesthesiol. 2018;31(1):1–5. doi:10.1097/aco.0000000000000535
4. Petersen RH, Gjeraa K, Jensen K, Møller LB, Hansen HJ, Konge L. Assessment of competence in video-assisted thoracoscopic surgery lobectomy: a Danish nationwide study. J Thoracic Cardiovasc Surg. 2018;156(4):1717–1722. doi:10.1016/j.jtcvs.2018.04.046
5. Zhu Y, Xie K, Yuan J, et al. Efficacy of oxycodone in intravenous patient-controlled analgesia with different infusion modes after laparoscopic radical surgery of cervical cancer a prospective, randomized, double-blind study. Medicine. 2019;98(34):e16810. doi:10.1097/md.0000000000016810
6. Dinges HC, Otto S, Stay DK, et al. Side effect rates of opioids in equianalgesic doses via intravenous patient-controlled analgesia: a systematic review and network meta-analysis. Anesthesia Analg. 2019;129(4):1153–1162. doi:10.1213/ane.0000000000003887
7. Zhao H, Xin L, Feng Y. The effect of preoperative erector spinae plane vs. paravertebral blocks on patient-controlled oxycodone consumption after video-assisted thoracic surgery: a prospective randomized, blinded, non-inferiority study. J Clin Anesth. 2020;62:109737. doi:10.1016/j.jclinane.2020.109737
8. Wu B, Shan J, Zhou Q, Wang L. Determination of the ED(95) of a single bolus dose of dexmedetomidine for adequate sedation in obese or nonobese children and adolescents. Br J Anaesth. 2021;126(3):684–691. doi:10.1016/j.bja.2020.11.037
9. Olutoye OA, Yu X, Govindan K, et al. The effect of obesity on the ED(95) of propofol for loss of consciousness in children and adolescents. Anesthesia Analg. 2012;115(1):147–153. doi:10.1213/ANE.0b013e318256858f
10. Shatalin D, Arzola C, Downey K, Ye XY, Carvalho JCA. L’administration programmee de bolus periduraux pour l’analgesie du travail obstetrical pendant le premier stade du travail: une etude de repartition sequentielle pour determiner le temps d’intervalle optimal entre des bolus d’un volume fixe de 2,5 mL de bupivacaine 0,25 % plus 8 mug.mL(−1) de fentanyl [Programmed intermittent epidural bolus for labour analgesia during first stage of labour: a sequential allocation trial to determine the effective interval time between boluses of a fixed volume of 2.5 mL of bupivacaine 0.25% plus fentanyl 8 microg.mL(-1)]. Can J Anaesthesia. 2021;68(5):653–660. doi:10.1007/s12630-021-01922-6
11. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
12. Sviggum HP, Arendt KW, Jacob AK, et al. Intrathecal hydromorphone and morphine for postcesarean delivery analgesia: determination of the ED90 using a sequential allocation biased-coin method. Anesthesia Analg. 2016;123(3):690–697. doi:10.1213/ane.0000000000001229
13. Kim DH, Oh YJ, Lee JG, Ha D, Chang YJ, Kwak HJ. Efficacy of ultrasound-guided serratus plane block on postoperative quality of recovery and analgesia after video-assisted thoracic surgery: a randomized, triple-blind, placebo-controlled study. Anesthesia Analg. 2018;126(4):1353–1361. doi:10.1213/ane.0000000000002779
14. Park MH, Kim JA, Ahn HJ, Yang MK, Son HJ, Seong BG. A randomised trial of serratus anterior plane block for analgesia after thoracoscopic surgery. Anaesthesia. 2018;73(10):1260–1264. doi:10.1111/anae.14424
15. Fu Z, Zhang Y, Zhou Y, et al. A comparison of paravertebral block, erector spinae plane block and the combination of erector spinae plane block and paravertebral block for post-operative analgesia after video-assisted thoracoscopic surgery: a randomised controlled trial. J Minim Access Surg. 2022;18(2):241–247. doi:10.4103/jmas.JMAS_277_20
16. Hill SE, Keller RA, Stafford-Smith M, et al. Efficacy of single-dose, multilevel paravertebral nerve blockade for analgesia after thoracoscopic procedures. Anesthesiology. 2006;104(5):1047–1053. doi:10.1097/00000542-200605000-00022
17. Konstantatos AH, Howard W, Story D, Mok LY, Boyd D, Chan MT. A randomised controlled trial of peri-operative pregabalin vs. placebo for video-assisted thoracoscopic surgery. Anaesthesia. 2016;71(2):192–197. doi:10.1111/anae.13292
18. Song JW, Park EY, Lee JG, Park YS, Kang BC, Shim YH. The effect of combining dexamethasone with ondansetron for nausea and vomiting associated with fentanyl-based intravenous patient-controlled analgesia. Anaesthesia. 2011;66(4):263–267. doi:10.1111/j.1365-2044.2011.06648.x
19. Hu B, Li L, Wang H, et al. Determining the minimum effective concentration of ropivacaine in epidural anesthesia for tolerable pain in transforaminal percutaneous endoscopic lumbar discectomy to avoid nerve injury: a double-blind study using a biased-coin design. Drug Des Devel Ther. 2022;16:315–323. doi:10.2147/DDDT.S334605
20. Yu W, Wu X, Liu L, et al. The median effective dose of one intravenous bolus of oxycodone for postoperative analgesia after myomectomy and hysterectomy with local ropivacaine wound infiltration: an Up-Down Dose-Finding Study. Anesthesia Analg. 2020;131(5):1599–1606. doi:10.1213/ane.0000000000005011
21. Shi L, Liu L, He Y, Yang Y, Ni H, Hussein AF. Comparison of a small dose of oxycodone and sufentanil for the prevention of sufentanil-induced cough during general anesthesia induction: a prospective randomized controlled trial. Comput Math Methods Med. 2022;2022:7924643. doi:10.1155/2022/7924643
22. Taha AM, Abd-Elmaksoud AM. Ropivacaine in ultrasound-guided femoral nerve block: what is the minimal effective anaesthetic concentration (EC90)? Anaesthesia. 2014;69(7):678–682. doi:10.1111/anae.12607
23. Gao W, Chen Y, Wang W, et al. The 90% minimum effective volume and concentration of ropivacaine for ultrasound-guided median nerve block in children aged 1–3 years: a biased-coin design up-and-down sequential allocation trial. J Clin Anesth. 2022;79:110754. doi:10.1016/j.jclinane.2022.110754
24. Kewlani A, Bhatia N, Makkar JK, Kumar V. Median effective volume of 0.5% ropivacaine for ultrasound-guided costoclavicular block. Anesthesiology. 2021;134(4):617–625. doi:10.1097/aln.0000000000003731
25. Wesselink EJ, Koopman SJ, Vegt RV, et al. ED90 of spinal 2-chloroprocaine 1% in ambulatory knee arthroscopy up to 45 min: a randomized biased-coin- up-and-down sequential allocation trial. Reg Anesth Pain Med. 2022;47(4):212–216. doi:10.1136/rapm-2021-103089
26. Lavoie A, McCarthy RJ, Wong CA. The ED90 of prophylactic oxytocin infusion after delivery of the placenta during cesarean delivery in laboring compared with nonlaboring women: an up-down sequential allocation dose-response study. Anesthesia Analg. 2015;121(1):159–164. doi:10.1213/ane.0000000000000781
27. Kinnunen M, Piirainen P, Kokki H, Lammi P, Kokki M. Updated clinical pharmacokinetics and pharmacodynamics of oxycodone. Clin Pharmacokinet. 2019;58(6):705–725. doi:10.1007/s40262-018-00731-3
28. Wang L, Yang M, Meng W. Prevalence and characteristics of persistent postoperative pain after thoracic surgery: a systematic review and meta-analysis. Anesthesia Analg. 2023;137(1):48–57. doi:10.1213/ane.0000000000006452
29. Bayman EO, Parekh KR, Keech J, Selte A, Brennan TJ. A prospective study of chronic pain after thoracic surgery. Anesthesiology. 2017;126(5):938–951. doi:10.1097/ALN.0000000000001576
30. Daoust R, Paquet J, Cournoyer A, et al. Side effects from opioids used for acute pain after emergency department discharge. Am J Emergency Med. 2020;38(4):695–701. doi:10.1016/j.ajem.2019.06.001
31. Leng X, Zhang F, Yao S, et al. Prolonged-Release (PR) oxycodone/naloxone improves bowel function compared with oxycodone PR and provides effective analgesia in chinese patients with non-malignant pain: a randomized, double-blind trial. Adv Ther. 2020;37(3):1188–1202. doi:10.1007/s12325-020-01244-x
32. Hunold KM, Esserman DA, Isaacs CG, et al. Side effects from oral opioids in older adults during the first week of treatment for acute musculoskeletal pain. Acad Emergency Med. 2013;20(9):872–879. doi:10.1111/acem.12212
33. Liu X, Zhao D, Zhao S, Li Z, Wang Y, Qin X. Deciphering the correlations between aging and constipation by metabolomics and network pharmacology. Aging. 2021;13(3):3798–3818. doi:10.18632/aging.202340
34. Cajanus K, Neuvonen M, Koskela O, et al. Analgesic plasma concentrations of oxycodone after surgery for breast cancer-which factors matter? Clin Pharmacol Ther. 2018;103(4):653–662. doi:10.1002/cpt.771
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.