Back to Journals » Research and Reports in Urology » Volume 15
Testicular Cancer in Saudi Arabia Between 2004 and 2017
Authors Alghamdi IG ![]()
Received 25 October 2022
Accepted for publication 10 January 2023
Published 24 January 2023 Volume 2023:15 Pages 37—45
DOI https://doi.org/10.2147/RRU.S393819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Guglielmo Mantica
Ibrahim G Alghamdi
Public Health Department, College of Applied Medical Sciences, University of Al-Baha, Al-Baha, Saudi Arabia
Correspondence: Ibrahim G Alghamdi, University of AL-Baha, College of Applied Medical Sciences, Public Health Department, Prince Mohammad Bin Saud, Al-Baha, 65527, Saudi Arabia, Tel +966553777925, Email [email protected]
Objective: This study examines the epidemiology related to testicular cancer (TC) in the administrative regions of Saudi Arabia by looking at not only the percentage/ frequency of diagnosed cases, but also the crude incidence rate, age-specific incidence rate, and age-standardized incidence rate stratified by the age group, diagnosis year, and regions.
Methods: From 2004 to 2017, descriptive epidemiological research was carried out across all TC cases registered under the Saudi Cancer Registry (SCR). Descriptive statistics as well as the Kruskal–Wallis test, together with SPSS (version 20.0) were used to evaluate the data.
Results: The SCR received 1114 reports of TC diagnoses between January 2004 and December 2017. TC was diagnosed most frequently in Saudi men aged 15– 44 years. In terms of Saudi men, Jouf, Tabuk, Hail, and the Northern region reported the highest age-specific incidence rate (ASIR) of TC at 1.1 per 100,000 men. Alternatively, Baha, Jazan, and Riyadh had the lowest overall ASIR of TC (0.1 and 0.3 per 100,000 men, respectively). The ASIR of TC exceeded its previous levels by twofold. The likelihood of TC was five times higher in Jouf, Tabuk, Hail, and Northern regions than in Baha and Jazan.
Conclusion: In Saudi Arabia, the ASIRs of TC doubled between 2004 and 2017. TC was most frequently diagnosed in younger Saudi men. Jouf, Tabuk, Hail, and Northern regions of Saudi Arabia had the highest incidence of TC among Saudi men, whereas Baha, Jazan, and Riyadh had the lowest incidence.
Keywords: cancer epidemiology, testicular cancer, Saudi Cancer Registry, oncology, incidence rate
Introduction
In young men between the ages of 15 and 45, testicular cancer (TC) remains the most frequent type of cancer reported.1–4 It comprises 1% of male cancer cases and 5% of urological cancers, respectively.1 Incidence of TC has doubled over the past forty years.4 The incidence varies with ethnicity, with a higher incidence being reported in nations with higher incomes and lower incidence being seen in countries with lower incomes.1,5 As per the American Cancer Society (ACS), the total number of newly diagnosed cases of TC will be 9910 in 2022, claiming 460 lives in the USA alone.6
TC is a type of cancer that affects the testicles, which are the male reproductive organs that produce sperm and hormones. There are several subtypes of TC, including seminoma and non-seminoma. Seminoma is a type of TC that tends to grow and spread more slowly than non-seminoma. It has a survival rate of 98–99% when the diagnosis is made in nascent phases.2,7,8 The more aggressive non-seminoma tends to grow and spread more quickly than seminoma.9 There are several subtypes of non-seminoma, including teratoma, embryonal carcinoma, yolk sac tumor, and choriocarcinoma. These subtypes can behave differently and may require different treatments.10
There are several known risk factors for testicular cancer, including age (most common in men between the ages of 20 and 39 and is more likely to occur in men with a family history of the disease or who were born with cryptorchidism (undescended testicles). White men and those suffering from HIV infections are more vulnerable to TC as compared to their counterparts from other racial groups. Men who have had testicular cancer in one testicle are also at increased risk of developing cancer in the other testicle.11–13 TC may occur in men who do not have any known risk factors.13
According to the International Agency for Research on Cancer (IARC), the age-standardized incidence rate (ASIR) of this ailment in the kingdom be 0.82 per 100,000 men by 2020, with the age-standardized mortality rate (ASMR) being 0.13 per 100,000 men.14 At the same time, the ASIR of TC in Saudi men was shown to be significantly greater than in other Arabian Gulf countries. In 2020, the ASIR of TC was 0.49 in Oman and the United Arab Emirates, 0.54 in Bahrain, 0.58 in Qatar, and 0.77 in Kuwait.14
The assessment of the TC incidence rate among Saudi men was the primary goal of this study. This was accomplished by concentrating on the CIR and ASIR, which were then categorized according to the year in which they were diagnosed, the geographic region, and the age group. Thus, a decision was made to conduct observational descriptive epidemiological research by considering the temporal/geographical distribution of cases transpiring from 2004–2017 in the SCR.
Materials and Methods
This study aimed to carry out a descriptive (retrospective observational) epidemiological analysis of each case of TC tracked in the kingdom from January 2004 to December 2017. This study obviated the need for ethical clearance due to the abundant availability of information on TC rates in Saudi Arabia for researchers. Data for this study was provided by a population-based cancer registry developed by Saudi Arabia’s Ministry of Health in 1992. It was in 2004 that the most accurate report on cancer, in general, was published in Saudi Arabia.
Since 2001, the SCR has issued publications outlining the epidemiological pattern of cancer in Saudi Arabia. Accordingly, 13 regions spanning 2004–2017 are able to access extensive reports, including the CIR, the percentage/ frequency of cases, as well as the ASIR. These reports were utilized to carry out crucial data gathering on the entire information extracted by SCR.
To analyse the data, we used SPSS (Statistical Package for the Social Sciences) version 20.0. The overall number and percentage, the age-specific incidence rate, the crude incidence rate (CIR), and the age-standardised incidence rate (ASIR) were stratified by geographical region, age group, and year of diagnosis and were computed for the epidemiological data assessment. We also employed the Kruskal–Wallis test for evaluating TC’s CIR as well as ASIR in varied areas of the kingdom.
Results
Between January 2004 and December 2017, the SCR received 1114 TC cases. In 2004, there were 44 TC cases (1.3% of all cancer cases), as shown in Figure 1. In 2010, this figure had risen to 78, accounting for 1.7% of all cancer cases. Between 2011 and 2014, the annual number of TC cases fluctuated between 80 and 98, accounting for 1.6% to 1.8% of all cancer cases. Furthermore, the SCR recorded the largest number of TC cases among Saudi men between 2015 and 2017, ranging between 102 and 124, representing 1.9 to 2.1% of total cancer cases. During the study period, however, the overall annual number and percentage of TC cases among Saudi men were 80 (1.6% of all cancer cases).
 |
Figure 1 Testicular cancer cases among Saudi men (number and percentage) between 2004 and 2017. |
Using SCR data, the average number and percentage of TC incidences observed from 2004 to 2017 across Saudi men in terms of age group were deduced for ages 0 to 4 years, 5 to 9 years, 10 to 14 years, 15 to 19 years, 20 to 24 years, and more than 75 years. From 2004–2017, the highest incidence of TC was seen in Saudi men aged 25–29 (18 cases per year, 22.5%, and CIR 2.0 per 100,000 men), followed by those aged 20–24 (14.1 cases per year, 17.1%, and CIR 1.5 per 100,000 men) and those aged 30–34 (12.0 cases per year, 15.7%, and CIR 1.6 per 100,000 men). However, from 2004 to 2017, the overall annual incidence of TC among Saudi men aged 15 to 44 reached 80.8% of the total number of cases (Figures 1 and 2).
 |
Figure 2 Incidence rate (Overall Age Specific) of testicular cancer cases among Saudi men from 2004 to 2017. |
Figure 3, shows that the CIRs of TC cases among men in Saudi Arabia, stratified by year of diagnosis and per 100,000 men, doubled between 2004 and 2017. The SCR observed the maximum CIR in 2016 and 2017 at 1.2 per 100,000 men. However, the annual overall CIR of TC among Saudi men was 0.8 (95% CI: 0.7 to 1.0) per 100,000 men. The overall CIRs for TC in Jouf, Tabuk, Hail, and Northern regions were the highest, at 1.2 per 100,000 men. There are statistically significant differences between these areas and other regions of Saudi Arabia, according to the Kruskal–Wallis test for non-normally distributed data χ2 (12, N=181) =62.082, P < 0.001). On the other hand, Figure 4 shows that Baha, Jazan, and Riyadh, showed the lowest overall CIRs of TC at 0.1, 0.3, and 0.4 per 100,000 men, respectively.
 |
Figure 3 Incidence rate (Crude) of testicular cancer cases among Saudi men from 2004 to 2017. |
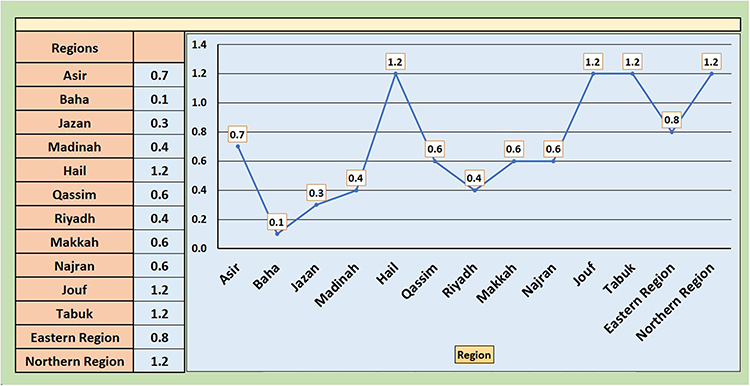 |
Figure 4 Incidence rate (Overall Crude) of testicular cancer cases among Saudi men by region from 2004 to 2017. |
As shown in Figure 5, the number of TC cases increased twofold from 2004 to 2017. For 2004, the estimated ASIR stood at 0.6 per 100,000 men, and 2016 and 2017 witnessed the highest ASIR noted by the SCR (1.1 per 100,000 men). Meanwhile, the yearly total TC ASIR among men in Saudi Arabia stood at 0.8 per 100,000 men. The overall TC ASIR stratified by regions in Saudi Arabia between 2004 and 2017 is shown in Figure 6. The ASIR for TC was 1.1 per 100,000 men in Jouf, Tabuk, Hail, and Northern regions. The Kruskal–Wallis test found a statistically significant difference between these locations and the rest of Saudi Arabia χ2 (12, N=181) =60.623, P < 0.001). In comparison, Baha, Jazan, and Riyadh have the lowest overall ASIR of TC at 0.1, 0.2, and 0.3 per 100,000 men, respectively.
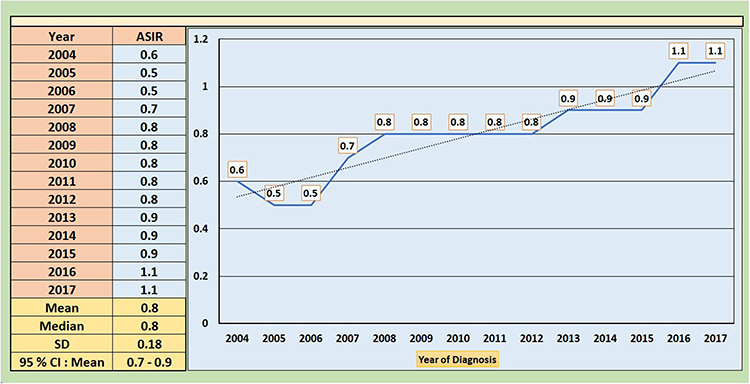 |
Figure 5 Incidence rate (age-standardised) of testicular cancer cases among Saudi men from 2004 to 2017. |
 |
Figure 6 Incidence rate (Overall Age-Standardised) of testicular cancer cases among Saudi men by region from 2004 to 2017. |
Discussion
As per the PubMed database, this descriptive epidemiological study is the first of its kind that examines both the temporal and spatial distribution of TC in Saudi men residing across administrate areas. This research is unique in that it examines both the existing pattern of the ailment and its importance in the country.
Our findings suggest that TC is most predominantly reported in Saudi men aged 15 to 44 years old. The overall ASIR of TC among Saudi men from 2004 to 2017 suggests that the disease peaked between the ages of 25 and 29. This finding is in consonance with previous studies that observed the highest prevalence of TC among young adult males aged 15 to 40.3,15 There is a dearth of enough evidence to suggest that high levels of testosterone in young adults could be attributed to a heightened risk TC, but some studies suggest that men with TC may have lower testosterone levels during treatment cycle and returns to normal level following the completion of chemotherapy. However, the relationship between testosterone levels and testicular cancer is not fully understood and more research is needed to confirm this potential association. It is also worth considering that testosterone levels can vary significantly among individuals and may be influenced by factors such as age, diet, and lifestyle.16,17 It is also uncommon for TC cases to occur in males under the age of 15. The exact reason for this is not fully understood, but it may be because testicular cancer tends to occur in males who have reached puberty when the testicles begin to produce testosterone and other hormones.18,19
In Saudi Arabia, the ASIR of TC among Saudi men doubled between 2004 and 2017. Similarly, the rate of TC cases has been increasing in many Western countries over the past several decades, with a twofold increase being observed since the 1960s. It is important to note that the incidence of testicular cancer may vary widely among different populations and may be influenced by a variety of factors such as genetics, lifestyle, and environmental exposures.20 In the United States, the age-adjusted incidence rates of TC have climbed moderately over the past several years, while the age-adjusted death rate has remained low and consistent from 2004 to 2019. (Figure 7).6 However, with proper treatment, the prognosis is favorable, with a cure rate of >90% and a five-year survival rate of >95%.21,22 It is important to note that the fear of COVID-19 may also affect the diagnosis and treatment of testicular cancer. According to Cieri et al, patients may avoid seeking medical evaluation due to the pandemic, leading to lower rates of routine disease management and hospitalizations for acute and severe conditions, including cancer. This may increase the risk of morbidity and potentially severe complications, as well as higher rates of mortality for testicular cancer patients.23
 |
Figure 7 Trend line of testicular cancer in the USA from 2004 to 2019. |
Saudi men in the regions of Jouf, Tabuk, Hail, and Northern reported the most ASIRs from 2004 to 2017, indicating that Saudi men residing in these areas may be highly exposed to TC risk factors. Consequently, the Saudi Arabian government, represented by the Ministry of Health, may focus its epidemiological studies on these regions. In contrast, Saudi men in Baha and Jazan were least susceptible to TC, indicating that they were more exposed to protective factors against TC than men in other locations. However, the probability of TC was five times higher in Jouf, Tabuk, Hail, and Northern areas than in Baha and Jazan.
In Saudi Arabia, the ASIR for TC among Saudi men was estimated to be 0.82 per 100,000 men in 2020. The rate is considerably higher than those of other Arabian Gulf nations. Saudi Arabia and Kuwait had the highest ASIR of TC among men in the Arabian Gulf, with rates of 0.82 and 0.77 per 100,000 men, respectively; these rates were about 1.6 times higher than those of other Arabian Gulf nations (Figure 8).14 Furthermore, for the same year, the ASMR of TC in Saudi Arabia was detected at a rate of 0.13 per 100,000 men, which was higher when compared with those in other nations in the Arab Gulf. However, the United Arab Emirates and Oman had the lowest ASMR of TC among men in 2020, at 0.02 and 0.08 per 100,000 men, respectively, while Qatar did not report any TC-related deaths. Compared to other world countries, the overall ASIR of TC in Saudi Arabia is extremely low compared to Norway (11.8 per 100,000 men), Denmark (10.4, per 100,000 men), Germany (10.0, per 100,000 men), and France (9.0, per 100,000 men); these rates were 11 to 15 times higher than in Saudi Arabia (Figure 9).14
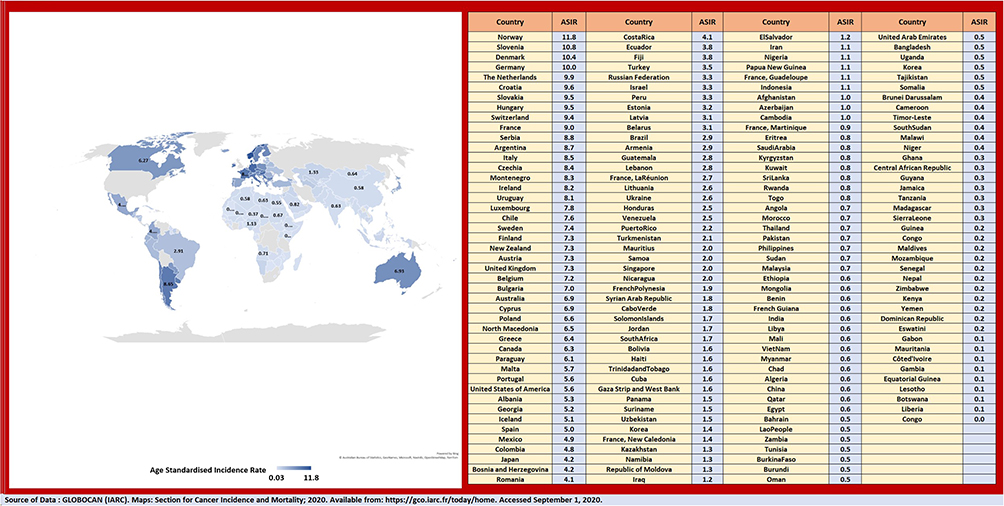 |
Figure 8 Incidence rate (age-standardised) of testicular cancer among men (World) in 2020. |
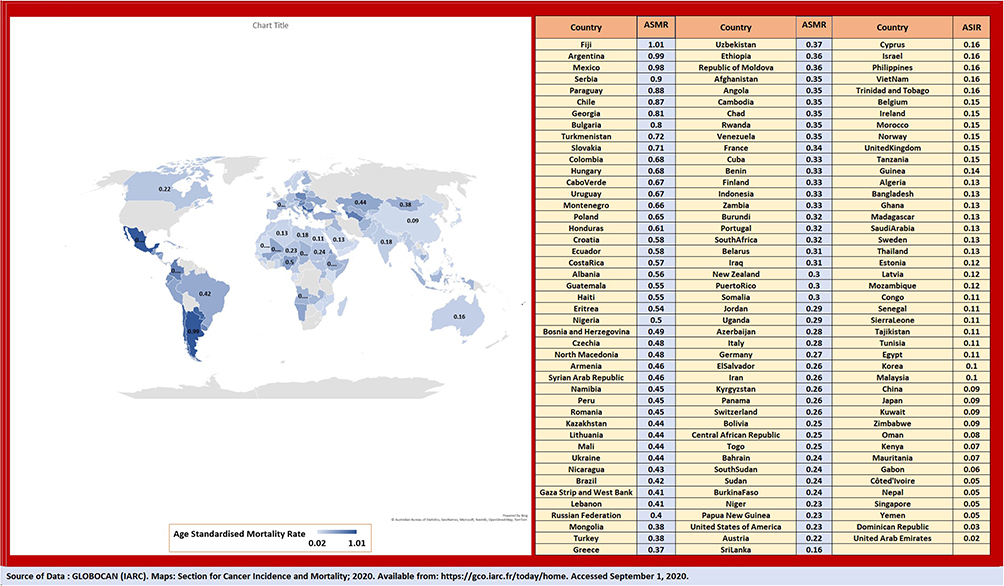 |
Figure 9 Mortality rate (age-standardised) of testicular cancer among men (World) in 2020. |
Our research investigates the actual distribution of TC in Saudi Arabia. It helps other researchers in generating a fresh hypothesis regarding the potential risk-protective factors of TC among Saudi men residing in different localities. However, descriptive epidemiological studies have several strengths, including the ability to provide a broad overview of the distribution and determinants of a health outcome in a population, the ability to be conducted quickly and inexpensively, the ability to identify areas for further research or support the development of public health policies and interventions, and the ability to track the effectiveness of interventions or monitor changes in the prevalence or incidence of a health outcome over time. In addition, descriptive epidemiological studies also suffer from several limitations, including the inability to identify cause-and-effect relationships between risk factors and health outcomes, the potential for bias such as sampling or reporting bias, the inability to fully control for confounders, and the potential for limited generalizability to other populations.24,25 However, the average death rates of TC in various regions of Saudi Arabia could not be determined in this research since the SCR reports lacked information on the number of TC-related deaths.
Conclusion
This study revealed a double increase in the Saudi men’s ASIRs of TC from 2004 to 2017. The highest overall ASIRs were observed in Jouf, Tabuk, Hail, and Northern regions while the lowest rates were seen in Baha, Jazan, and Riyadh. Among the Arabian Gulf countries, Saudi Arabia has the highest TC ASIR. TC was more prevalent among younger Saudi men.
Ethical Approval Statement
The Department of National Health Registries in the Ministry of Health, Saudi Arabia, was established as part of the national center of health information. They have responsibilities over the existing registries and setting standards for creating of new registries. The by-law of disease registries was approved by Saudi Health Council resolution No. (66/7) dated 13/9/1434 H. The Saudi Cancer Registry is one of the ongoing national registries that offers unrestricted access to its data. The National Health Records Administration has made available to academics annual reports including comprehensive data on all forms of cancer in the Kingdom of Saudi Arabia. These reports and data can be accessed on the National Health Records Administration website by any researcher interested in scientific publishing in the field of oncology, without condition, restriction, or formal consent. The Department of National Health Records has declared that all cancer reports in the Kingdom of Saudi Arabia are available to researchers in universities and scientific research centers, and has encouraged them to analyze these reports and contribute to scientific publishing without limitation. The data on the prevalence of testicular cancer in Saudi Arabia are publicly available and widely accessible through the Saudi Cancer reports; thus, no ethical approval was required for this descriptive epidemiological observational study. In addition, the guidelines outlined in the Declaration of Helsinki were followed. The author declares that the paper does not raise any ethical concern. The data regarding Testicular cancer incidence in Saudi Arabia are publicly available and easily accessible through the Saudi Cancer reports; therefore, no ethical approval was required for this observational descriptive epidemiological study. All reports can be directly downloaded from the National Health Information Centre’s website, available from: https://nhic.gov.sa/en/eServices/Pages/TumorRegistration.aspx
Disclosure
The author reports no conflicts of interest in this work.
References
1. Cassell A, Jalloh M, Ndoye M, et al. Review of testicular tumor: diagnostic approach and management outcome in Africa. Res Rep Urol. 2020;12:35–42. PMID: 32110551; PMCID: PMC7035899. doi:10.2147/RRU.S242398
2. Stephenson A, Eggener SE, Bass EB, et al. Diagnosis and treatment of early stage testicular cancer: AUA guideline. J Urol. 2019;20:10–97.
3. Park JS, Kim J, Elghiaty A, Ham WS. Recent global trends in testicular cancer incidence and mortality. Medicine. 2018;97(37):e12390. doi:10.1097/MD.0000000000012390
4. Gaddam SJ, Chesnut GT. Testicle cancer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
5. Albers P, Albrecht W, Algaba FC, et al. EAU Guidelines on Testicular Cancer. EAU; 2017.
6. American Cancer Society. Key statistics about Testicular cancer; 2022. Available from https://seer.cancer.gov/statfacts/html/testis.html.
7. Cedeno JD, Light DE, Leslie SW. Testicular Seminoma. StatPearls. 2020;105(2):123–134.
8. Ouguellit S, Loriot Y. Tumeurs germinales de stade I [Stage 1 germ-cell tumour]. Bull Cancer. 2019;106(10):887–895. French. doi:10.1016/j.bulcan.2019.03.010
9. National Cancer Institute. Testicular cancer treatment (PDQ®)–patient version; 2021. Available from: https://www.cancer.gov/types/testicular/patient/testicular-treatment-pdq.
10. Khan O, Protheroe A. Testis cancer. Postgrad Med J. 2007;83(984):624–632. doi:10.1136/pgmj.2007.057992
11. Cancer.net. Testicular cancer: what is testicular cancer?; 2020. Available from: https://www.cancer.net/cancer-types/testicular-cancer/what-is-testicular-cancer.
12. Mayo Clinic. Testicular cancer: diagnosis and treatment; 2021. Available from https://www.mayoclinic.org/diseases-conditions/testicular-cancer/diagnosis-treatment/drc-20353443.
13. GLOBOCAN (IARC). Maps: section for cancer incidence and mortality; 2020. Available from: https://gco.iarc.fr/today/home.
14. Chia VM, Quraishi SM, Devesa SS, et al. International trends in the incidence of testicular cancer 1973–2002. Cancer Epidemiol Biomarkers Prev. 2010;19:1151–1159. doi:10.1158/1055-9965.EPI-10-0031
15. Xu P, Choi E, White K, Yafi FA. Low testosterone in male cancer patients and survivors. Sex Med Rev. 2021;9(1):133–142. doi:10.1016/j.sxmr.2020.03.004
16. Sarfraz M, Ashraf Y, Sajid S, Ashraf M. Testosterone level in testicular cancer patients after chemotherapy. West Indian Med J. 2016. doi:10.7727/wimj.2016.060
17. Hayes-Lattin B, Nichols CR. Testicular cancer: a prototypic tumor of young adults. Semin Oncol. 2009;36(5):432–438. PMID: 19835738; PMCID: PMC2796329. doi:10.1053/j.seminoncol.2009.07.006
18. Urology Care Foundation. Testicular cancer in children: symptoms, diagnosis & treatment. Available from: https://www.urologyhealth.org/urology-a-z/t/testicular-cancer-in-children.
19. Shanmugalingam T, Soultati A, Chowdhury S, Rudman S, Van Hemelrijck M. Global incidence and outcome of testicular cancer. Clin Epidemiol. 2013;5:417–427. PMID: 24204171; PMCID: PMC3804606. doi:10.2147/CLEP.S34430
20. Smith ZL, Werntz RP, Eggener SE. Testicular cancer: epidemiology, diagnosis, and management. Med Clin North Am. 2018;102(2):251–264. doi:10.1016/j.mcna.2017.10.003
21. Baird DC, Meyers GJ, Hu JS. Testicular cancer: diagnosis and treatment. Am Fam Physician. 2018;97(4):261–268.
22. Cieri M, Contieri R, De Carlo C, et al. Delayed diagnosis of a testicular mass during COVID-19 pandemic in Lombardy: a case report. Res Rep Urol. 2021;13:41–44. doi:10.2147/rru.s297880
23. Rakesh A, Priya R. Study designs: part 2 – descriptive studies. Perspect Clin Res. 2019;10(1):34–36. doi:10.4103/picr.PICR_154_18
24. Centers for Disease Control and Prevention. Epidemiology 101: descriptive studies; 2019. Available from: https://www.cdc.gov/csels/dsepd/ss1978/lesson1/section5.html.
25. Nauman M, Leslie SW. Nonseminomatous testicular tumors. StatPearls. 2020;105(2):123–134.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.