Back to Journals » International Medical Case Reports Journal » Volume 15
Temporary Vitelliform Regression After Intravitreal Ranibizumab Injection for Macular Neovascularization Complicating Best Disease
Authors Fayed A
Received 27 July 2022
Accepted for publication 3 October 2022
Published 18 October 2022 Volume 2022:15 Pages 593—598
DOI https://doi.org/10.2147/IMCRJ.S383541
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alaa Fayed1,2
1Department of Ophthalmology, Kasr Al-Ainy School of Medicine, Cairo University, Giza, Egypt; 2Watany Research and Development Center, Watany Eye Hospital, Cairo, Egypt
Correspondence: Alaa Fayed, Department of Ophthalmology, Kasr Al-Ainy School of Medicine, Kasr Al-Ainy St, Giza, Egypt, Email [email protected]
Background: In this report, we present a case of a 12-year-old boy with Best vitelliform macular dystrophy (BVMD) complicated by macular neovascularization (MNV) and treated with two intravitreal ranibizumab injections. We document an unusual temporary regression of his vitelliform deposits and describe a 2-year follow-up course through multimodal imaging.
Case Presentation: A 12-year-old boy complaining of metamorphopsia presented with bilateral yellowish subfoveal deposits, suggestive of BVMD, which was confirmed by fundus autofluorescence and electrooculography. The left eye showed an inferior juxtafoveal complicating MNV, for which the patient was treated with two intravitreal ranibizumab injections. In addition to demonstrating a remarkable response to injection, both clinically and through various multimodal imaging modalities, optical coherence tomography (OCT) showed a surprising temporary resolution of the subfoveal hypopreflective space denoting a regression in the lipofuscin deposits accumulating at the RPE and the subfoveal space. Within 2 months, there was a subsequent build-up of the subfoveal space and lipofuscin reaccumulation through serial imaging despite the clear regression of the MNV. The patient remained stable over a course of 2 years.
Conclusion: Our findings cast light on a rather unusual response to intravitreal anti-VEGF injections that has not been previously reported in literature in the form of a temporary disappearance of the subfoveal vitelliform deposits, which later began to reaccumulate. This process may reflect a temporary relief of the RPE dysfunction or decreased photoreceptor damage with regression of the complicating MNV, leading to decreased vitelliform deposition. Adding to other reports, our findings also provide a 2-year-long follow-up with serial multimodal documentation of the response to injection and suggest a favorable long-term prognosis for intravitreal anti-VEGF injections in eyes with BVMD presenting with early complicating MNVs.
Keywords: Best, lipofuscin, macular neovascularization, ranibizumab, VEGF, vitelliform
Introduction
Best vitelliform macular dystrophy (BVMD) is an autosomal dominant genetic disorder with variable clinical presentations, ranging from accidental discovery on routine clinical examination to affection of central vision through various complications, most notably macular neovascular membranes (MNV) and outer retinal atrophic changes in late cases.1 Several case reports have identified intravitreal anti-vascular endothelial growth factor (VEGF) agents as a potentially favorable management option for BVMD cases presenting with complicating MNVs.2,3 That said, there are no long-term studies that have been conducted to explore the long-term consequences of anti-VEGF agents on disease progression or vitelliform deposition.
Case Presentation
A healthy 12-year-old boy presented to our clinic with abnormal vision of the left eye, described by the patient as “seeing a squiggly line”, which was evident on Amsler grid testing. A review of his family history confirmed no significant known ophthalmological disorders or relevant information. On examination, his best corrected visual acuity was 20/20 in both eyes, and the intraocular pressure was recorded as 14 and 13 mmHg in the right and left eyes, respectively. The anterior segments, pupillary light reflexes and extraocular motility examination were all unremarkable.
Fundus examination revealed bilateral elevated maculae with yellow subfoveal deposits, giving off the characteristic “egg yolk” appearance of the vitelliform stage of Best vitelliform macular dystrophy (BVMD). On close inspection of the left macula, a darkish lesion was identified inferior to the fovea, consistent with retinal pigmentary changes suggestive of a possible complicating macular neovascularization (MNV). Fundus autofluorescence showed a circular ring of hyperautofluorescence surrounding the fovea, consistent with lipofuscin accumulation at the diseased RPE. The dark inferior juxtafoveal examination seen on fundus examination coincided with a tiny hypoautofluorescent spot seen in the left eye.
Optical coherence tomography (OCT) revealed bilateral subfoveal optically hyporeflective spaces and thickening of the cone outer segments. The left eye revealed an inferior juxtafoveal localized area of pigmentary elevation suggestive of MNV, which was confirmed as a neovascular frond by OCT angiography (OCTA). Electrooculography demonstrated an absent light rise with a significantly low Arden ratio of 1.1, confirming the diagnosis of BVMD (Figure 1).
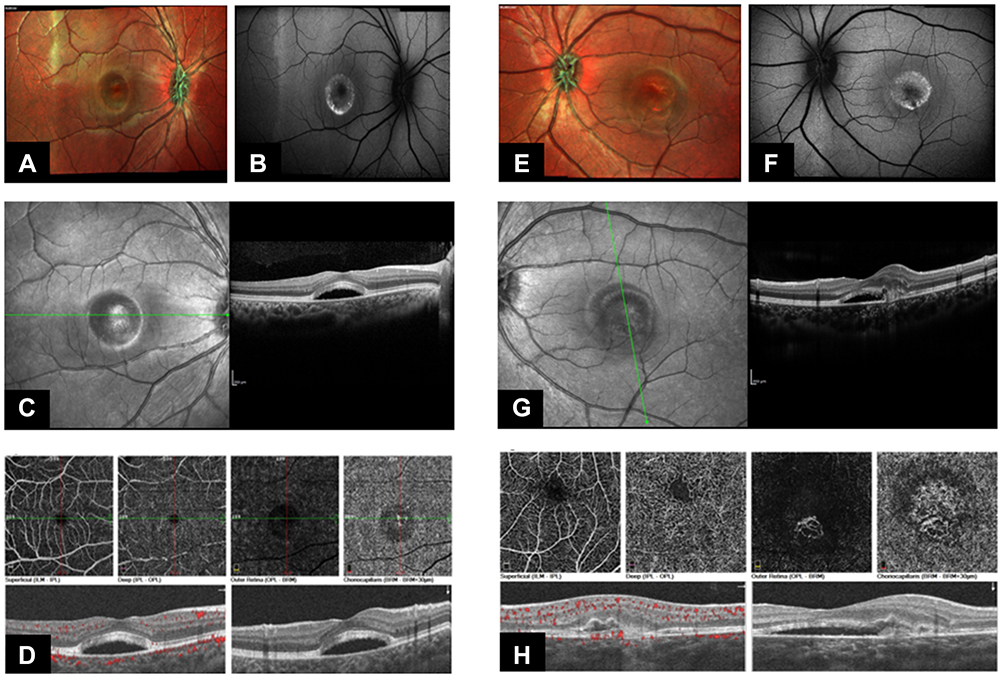 |
Figure 1 Multimodal imaging of Best vitelliform macular dystrophy (BVMD). (A) Multicolor image of the right eye shows an elevated macula with yellow subfoveal deposits, giving off the characteristic “egg yolk” appearance of the vitelliform stage of BVMD. (B) Fundus autofluorescence shows a circular ring of hyperautofluorescence surrounding the fovea. (C) Infrared en face and optical coherence tomography (OCT) B scan shows a subfoveal optically hyporeflective space and thickening of the cone outer segments. (D) OCT angiography (OCTA) confirms the absence of complicating neovascular fronds. (E) Multicolor image of the left eye shows subfoveal vitelliform deposits. (F) Fundus autofluorescence shows a circular ring of hyperautofluorescence surrounding the fovea with a tiny inferior juxtafoveal hypoautofluorescent spot, suggestive of pigmentary disruption. (G) Infrared en face and OCT B scan shows a subfoveal optically hyporeflective space and thickening of the cone outer segments with an inferior juxtafoveal localized area of pigmentary elevation suggestive of macular neovascularization (MNV). (H) OCTA confirms an inferior juxtafoveal neovascular frond in the outer retinal and choriocapillaris slabs. |
Despite an intact BCVA of 20/20, the patient was treated with 2 monthly intravitreal injections of ranibizumab (0.5mg/0.05 mL) based on the experienced metamorphopsia and irregular lines demonstrated on the Amsler grid. A month later, the patient presented with marked subjective regression of the metamorphopsia, which was equally evident on the Amsler grid. Surprisingly, OCT revealed complete resolution of the subfoveal optically hyporeflective space with restoration of the normal foveal contour. On OCTA en face scans of the outer retinal and choriocapillaris slabs, the MNV demonstrated subjectively clear shrinkage in size and arborization. Moreover, the inferior juxtafoveal hypoautofluorescent corresponding to the MNV appeared smaller (Figure 2).
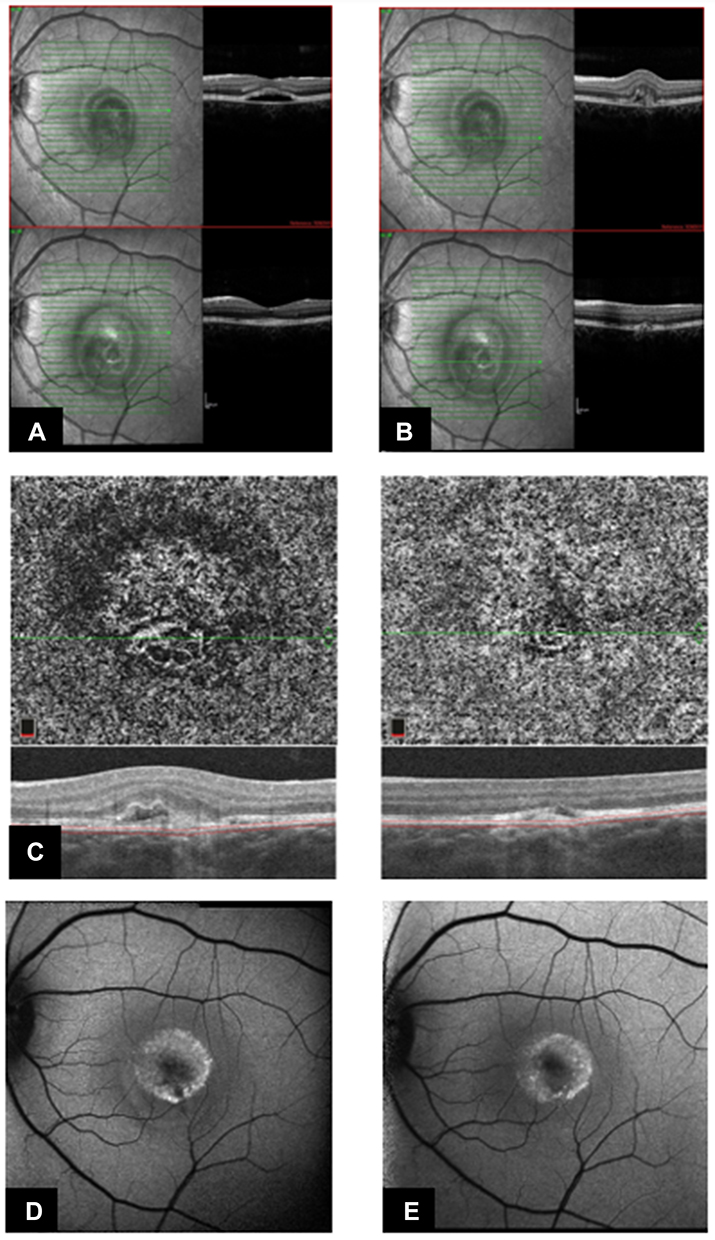 |
Figure 2 One month follow-up after two intravitreal ranibizumab injections. (A) Comparative OCT B scans before (top) and after (bottom) injection reveal a surprising disappearance of the subfoveal optically hyporeflective space. (B) Comparative OCT B scans reveal regression of the MNV after the injections. (C) Comparative OCTA choriocapillaris en face and B scans before (left) and after (right) injection reveal marked shrinkage of the neovascular frond. (D and E) Comparative FAF images before (D) and after (E) injection show disappearance of the inferior juxtafoveal hypoautofluorescent spot, consistent with regression of the MNV. |
Based on the above, the patient was not offered any more injections, and was advised to follow up after four weeks while maintaining weekly monitoring at home using serial Amsler grid testing. A month later (2 months after the injection), the patient reported near disappearance of the symptoms and OCTA continued to demonstrate shrinking of the MNV. Of note, there was a small, but evident increase in the size of the subfoveal optically hyporeflective space, indicating rebound accumulation of the lipofuscin in the subfoveal space.
Over the course of 2 years, the patient reported no new symptoms both on the Amsler grids or in his day-to-day activities. Serial en face OCTA images demonstrated near disappearance of the neovascular frond, and the inferior juxtafoveal hypoautofluorescent spot was undetectable. Strikingly, the most peculiar finding encountered on OCT was the gradual increase in the subfoveal space with a steady buildup of lipofuscin deposits. No further signs of activity were detected, and the right eye was not complicated by MNVs (Figure 3).
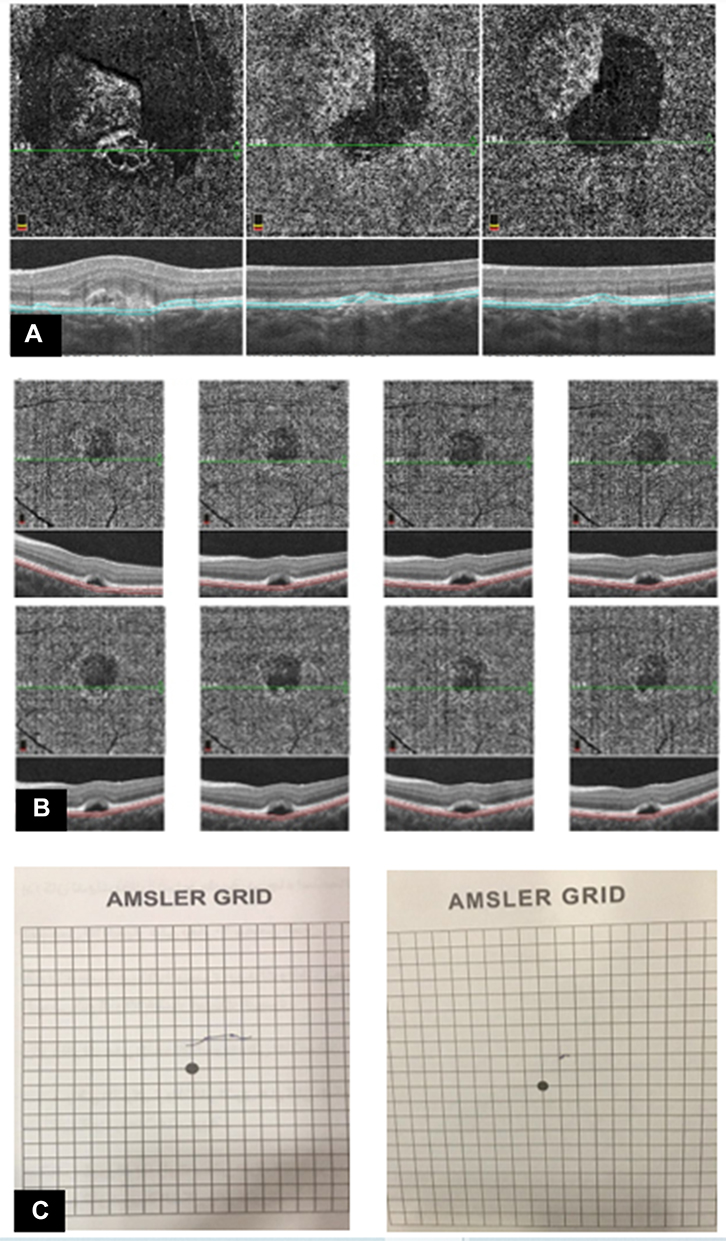 |
Figure 3 Two-year follow-up after two intravitreal ranibizumab injections. (A) Serial comparative 3×3 OCTA choriocapillaris slabs showing baseline (left), 6 months (middle) and 2 years (right) after injection reveal consistent shrinkage of the neovascular frond. (B) Serial comparative 6×6 OCTA choriocapillaris slabs taken from 8 follow-up visits over a 2-year follow-up period confirm the regression of the MNV, and the surprising gradual reaccumulation of the subfoveal deposits which began 2 months after the injections and persisted throughout the follow-up. (C) Comparative Amsler grids at baseline (left) and after 2 years (right) demonstrates the profound and long-lasting improvement of the patient’s metamorphopsia. |
Discussion and Conclusions
As with other chorioretinal pathologies, the development of MNVs in BVMD is thought to reflect a mechanical, ischemic and/or oxidative stress at the level of the Bruch’s membrane brought on by diseased RPE & photoreceptors, leading to the development of various pro-angiogenic factors, including VEGF.4 Consistent with the above, we demonstrated near-complete resolution of the metamorphopsia symptoms experienced by the patient and identified significant shrinkage in the size of the complicating neovascular frond on OCTA after 2 intravitreal anti-VEGF injections. Adding to other reports,2,3,5 our findings provide a follow-up period of over 2 years after injection, suggesting a favorable long-term outcome for intravitreal anti-VEGF injections and the possibility of effectively controlling MNVs complicating BVMD.
Strikingly, our patient’s OCT scans revealed complete resolution of the subfoveal optically hyporeflective spaces after the injections, suggesting a temporary resolution of the vitelliform deposits. To our knowledge, this finding is unique to our patient and cannot be explained by the reduction of intraocular VEGF load by the injections. BVMD is caused by mutations in the BEST1 gene located on chromosome 11q13 gene, which is responsible for the transcription of the bestrophin-1 protein. It localizes to the basolateral plasma membrane of the retinal pigment epithelium (RPE) and is believed to regulate intracellular calcium levels.6 The alteration in this protein results in the accumulation of large amounts of lipofuscin at the level of the RPE & the subretinal space, which is responsible for the morphological features and potential complications attributed to the disease. This is not a VEGF-driven process, and the apparent resolution of the subfoveal lipofuscin deposits is highly unusual and difficult to understand. A possible theory is that in the presence of a complicating MNV, the subfoveal space contains an amalgam of lipofuscin from the diseased RPE and exudative fluid from the neovascular frond. The reduction in the VEGF loads may lead to a regression in the activity of the neovascular frond and resolution of the exudative component of the subfoveal collection. It is possible that the reduction of the pro-angiogenic and pro-inflammatory markers brought on by the MNV may have caused a temporary relief to the diseased RPE with subsequent resolution of the lipofuscin deposits. It is clear that this relief is short-lived, as evident by the accumulation of the lipofuscin deposits within 2 months from the injection. Another theory to understand this finding is based on the fact that vitelliform deposits are widely thought to represent damaged outer photoreceptor segments. The presence of active MNV may contribute to the photoreceptor disruption adding to the damaged photoreceptor load and vitelliform accumulation. The regression of MNV activity by anti-VEGF may possibly cause a temporary halt in this process, leading to decreased vitelliform material. Eventually, the photoreceptor damage is resumed after the effect of the injection wears off.
In conclusion, we present a case of a 12-year-old boy with BVMD with a unilateral complicating MNV. The patient was treated with two intravitreal injections of ranibizumab with marked symptomatic improvement and significant shrinkage of the neovascular frond on OCTA. Surprisingly, OCT also demonstrated a temporary resolution of the subfoveal lipofuscin deposits, which began to reaccumulate 2 months later. The patient remained asymptomatic over a period of 2 years after the injection, and serial multimodal imaging confirmed persistent regression of the MNV, suggesting a favorable long-term outcome for intravitreal anti-VEGF injections in eyes with BVMD presenting with early complicating MNV.
Abbreviations
BCVA, best corrected visual acuity; BVMD, Best vitelliform macular dystrophy; MNV, macular neovascularization; OCT, optical coherence tomography; OCTA, optical coherence iomography angiography; RPE, retinal pigment epithelium; VEGF, vascular endothelial growth factor.
Data Sharing Statement
The images used in this report are available from the corresponding author on reasonable request.
Ethics Approval
The report followed the tenets of the Declaration of Helsinki and was performed in accordance with Health Insurance Portability and Accountability Act regulations.
Consent for Publication
Institutional approval was sought and was not required prior to publication. Verbal informed consent was obtained from the patient’s guardian to publish the patient details and images, which was approved by the institutional ethical committee. Written consent was not obtained because the patient’s guardian was illiterate. The consent was witnessed, documented, and held on file. No identifying features exist in the manuscript.
Funding
There is no funding to report.
Disclosure
The author declares no conflicts of interest in relation to this work.
References
1. Hartzell HC, Qu Z, Yu K, Xiao Q, Chien L-T. Molecular physiology of bestrophins: multifunctional membrane proteins linked to best disease and other retinopathies. Physiol Rev. 2008;88(2):639–672.
2. Leu J, Schrage NF, Degenring RF. Choroidal neovascularisation secondary to Best’s disease in a 13-year-old boy treated by intravitreal bevacizumab. Graefes Arch Clin Exp Ophthalmol. 2007;245(11):1723–1725.
3. Chhablani J, Jalali S. Intravitreal bevacizumab for choroidal neovascularization secondary to Best vitelliform macular dystrophy in a 6-year-old child. Eur J Ophthalmol. 2012;22(4):677–679.
4. Shahzad R, Siddiqui MAR. Choroidal neovascularization secondary to Best vitelliform macular dystrophy detected by optical coherence tomography angiography. J Am Assoc Pediatr Ophthalmol Strabismus. 2017;21(1):68–70.
5. Qaseem Y, German O, Cicinelli MV, Mirza RG. The role of optical coherence tomography angiography (Octa) in detecting choroidal neovascularization in different stages of best macular dystrophy: a case series. Medicina. 2021;57(3):213.
6. Marmorstein AD, Marmorstein LY, Rayborn M, Wang X, Hollyfield JG, Petrukhin K. Bestrophin, the product of the Best vitelliform macular dystrophy gene (VMD2), localizes to the basolateral plasma membrane of the retinal pigment epithelium. Proc Natl Acad Sci. 2000;97(23):12758–12763.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Ranibizumab Combined with Dexamethasone Intravitreal Implant Sequential Therapy for Macular Edema Secondary to Non-Ischemic Retinal Vein Occlusion
Gao L, Cai X, Dang Y
Drug Design, Development and Therapy 2026, 20:604539
Published Date: 30 March 2026