Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Telemedicine for HIV Care: Current Status and Future Prospects
Authors Smith E, Badowski ME ![]()
Received 19 February 2021
Accepted for publication 19 May 2021
Published 10 June 2021 Volume 2021:13 Pages 651—656
DOI https://doi.org/10.2147/HIV.S277893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Erica Smith,1 Melissa E Badowski2
1University of Illinois at Chicago, College of Pharmacy, Chicago, IL, 60612, USA; 2University of Illinois at Chicago, College of Pharmacy, Section of Infectious Diseases Pharmacotherapy, Department of Pharmacy Practice, Chicago, IL, 60612, USA
Correspondence: Melissa E Badowski
University of Illinois at Chicago, College of Pharmacy, Section of Infectious Diseases Pharmacotherapy, Department of Pharmacy Practice, 833 S. Wood Street, MC886, Room 164, Chicago, IL, 60612, USA
Email [email protected]
Abstract: Due to the COVID-19 pandemic, the use of telemedicine has been highlighted, especially in specialties, such as the management of HIV. Recent data were reviewed between January 1, 2019 and March 20, 2021 by searching English language manuscripts for studies documenting clinical outcomes in HIV care and the patient experience. A PubMed, Google Scholar, and bibliography review based on the search terms “HIV,” “telemedicine,” and “telehealth” was conducted. Studies included in this analysis were comprised of adult patients living with HIV, receiving care for HIV via telemedicine with reported clinical outcomes or perceptions of using telemedicine in the management of their HIV care. Of the 179 studies identified, 12 met inclusion for this analysis. Only two studies provided data on clinical outcomes of HIV (virologic outcomes), one pre-pandemic and one during COVID-19. The study evaluating viral suppression during COVID-19 demonstrated lower rates of virologic suppression and lower rates of missed appointments when shelter-in-place orders were issued compared to before the start of the pandemic. The remaining studies focused on patient-related outcomes as they related to the usability and adoption of telehealth models. Many practices documented the benefits and limitations of telemedicine based on the rapid switch from traditional in-person clinics. Benefits included retention in care for patients who lived a far distance from clinic, privacy for patients not wanting to be seen attending an HIV clinic, and more flexibility in scheduling appointments. Some limitations included patients’ access to technology, ability and willingness to use technology, and privacy of patients who are homeless and reside in a shelter where homelessness is 3 times greater in people living with HIV compared to the general population. Healthcare should be tailored to the individual patient by assessing their needs and limitations, particularly with patients who may be at risk for discontinuation of care, particularly in the homeless population. In addition, there are mixed data on factors such as age, sex, and race being limiting factors in willingness to use technology. From the studies reviewed, willingness to engage with technology did not differ by age, sex, or race but did differ by access and willingness to use technology. Greater limitations were access to appropriate devices for telemedicine and digital literacy. Although there have been difficulties with the switch to telemedicine in clinics during the COVID-19 pandemic, many patients have reported being satisfied with care and would be interested in continuing once the shelter-in-place order is lifted. Future studies should focus on the provision of HIV care using telemedicine beyond the pandemic and focus on ways to improve the telemedicine experience for the patient.
Keywords: HIV, telemedicine, telehealth
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, also known as COVID-19, has disrupted much of what we view as normal daily activities, especially in healthcare. Due to the abrupt nature of shelter-in-place orders that took place across much of the world in 2020, change needed to be quickly implemented into healthcare settings.1 The current pandemic showed the promise of telemedicine in all fields of medicine, particularly in people living with HIV (PLWH), due to their immunocompromised state putting them in a more vulnerable position than the general population.2 Despite pre-pandemic models in the management of HIV, 4 in 10 PLWH failed to achieve virologic suppression.3 The role of telehealth in PLWH expanded care into the homes of many patients who were willing to use technology as part of their healthcare, which may have the potential to improve virologic outcomes. Telemedicine previously demonstrated benefits in certain patient populations, including incarcerated individuals requiring specialized care.4 Since change needed to be executed quickly, many specialty clinics providing HIV care switched to telemedicine in order to provide HIV clinical services (ie review of labs, medication adherence, etc.) and retain patients in care while keeping them socially distanced.1 According to a survey of directly funded Ryan White providers, nearly 99% reported offering telehealth services which is up from 22%.3 The goal of this review was to evaluate the current literature and future prospects of providing HIV care via telemedicine during a global pandemic and beyond.
Methods
This narrative review included publications from PubMed, Google Scholar, and bibliography searches reviewed between January 6, 2019 (one-year pre-pandemic) and March 20, 2021 (one-year post-pandemic) using the following search terms: “HIV,” “telemedicine,” “telehealth.” The search was limited to publications in the English language and clinical trials. Additional inclusion criteria included adult patients living with HIV, receiving care for HIV via telehealth with reported clinical outcomes in HIV care (ie HIV-1 viral load and retention in care) and patient experience (ie attitude toward telemedicine, willingness to use telemedicine). The PRISMA flow diagram was used to identify and exclude manuscripts used in this review (Figure 1). Both the authors independently reviewed manuscripts for inclusion in this review. This manuscript was exempted from ethics review since it did not involve human subjects.
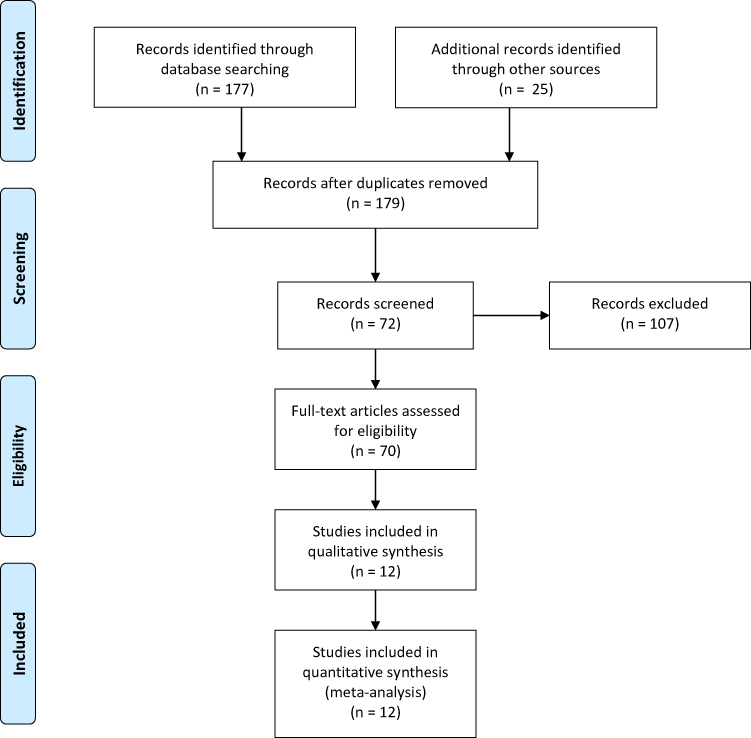 |
Figure 1 Included studies.Note: Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.17 |
Results
Clinical Outcomes and Attitudes Toward Telemedicine
Pre-Pandemic
Of the 179 articles identified, 12 met the inclusion criteria. A study conducted in the Veterans Affairs (VA) health systems in the United States of America (USA) between 2015 and 2016 evaluated the use of telemedicine with secured videoconferencing.5 Nine hundred and twenty-five patients receiving telemedicine were compared to 745 patients receiving traditional face-to-face care in outpatient clinics. With the use of videoconferencing for clinical visits, patients had more visits and slightly higher rates of viral suppression compared to traditional clinics (78.3% vs 74.1%, respectively; relative risk [RR], 1.06; 95% confidence interval [CI], 1.01 to 1.11). A specific benefit that was reported included being able to reach patients who had limited transportation or had substantial travel times. Noted limitations of the study were that the VA system may not reflect the general population and it may not reflect other barriers, such as billing and payment methods. Therefore, the use of telemedicine has been shown to successfully treat patients with a complicated disease state and even provide additional benefits.
COVID-19 Data
The COVID-19 pandemic has transformed the way that society functions with shelter-in-place mandates and social-distancing orders to minimize infection exposure. Telemedicine has provided a mechanism for patients to access medical care without leaving home. One study explained how a safety-net clinic for PLWH in San Francisco, CA, USA, transitioned to phone or video visits during the pandemic.6 The study analyzed viral suppression through HIV-1 viral load testing and retention in care through a number of missed appointments prior to the shelter-in-place order (December 1, 2019–February 29, 2020) and during the shelter-in-place order (April 1, 2020–April 30, 2020). Telemedicine accounted for 54% of all visits after a shelter-in-place order was enacted. There were fewer missed appointments for telephone vs in-person visits [adjusted odds ratio (aOR) 0.56; 95% CI [0.36–0.86] and younger patients (<35 years) were less likely to miss appointments (aOR 1.11; 95% CI [0.82–1.51]), whereas prior to the pandemic they were more likely (aOR 1.57; 95% CI [0.28–1.93]). The odds of having a detectable HIV-1 viral load were 31% higher during shelter-in-place (aOR 1.31; 95% CI 1.08–1.53) than in the previous year. For the homeless population, it was noted that 32% of homeless patients used telephone visits (P < 0.001). Though patients had higher odds of a detectable HIV-1 viral load (aOR 3.36; 95% CI [2.74–4.12]) compared to the previous year (aOR 2.27; 95% CI [1.91–2.71]), there were less missed appointments (aOR 0.64; 95% CI [0.48–0.85]) compared to the previous year (aOR 1.15; 95% CI [0.95–1.32]), which is similar to the overall population. The authors attributed this increase in detectable HIV-1 viral loads to a lack of access to social support services that the clinic provides. The economic impact, housing instability, and COVID-19 outbreaks in shelters can all have an adverse effect on patients. Since homelessness is 3 times higher in PLWH than in the general population, this is important to consider when developing interventions in this population.7 Although telemedicine can be swiftly implemented, and patients were willing to transition to telephone visits, there were other components that were not conducive to homeless patient populations, such as access to technology and social services.
Patient-Related Outcomes (Satisfaction, Utilization, Etc.)
Pre-Pandemic
Though there are many studies that outline the benefits of telemedicine, there are underlying social determinants that can factor into patients’ willingness to use telehealth. A survey-based study conducted between June 2016 and April 2017 evaluated 1268 low-income people living with HIV (PLWH) in Florida, USA, using Ryan White case management.8 Participants took a survey that evaluated demographics, personal technology use and access to technology. Factors associated with patients’ willingness to use any form of telemedicine for the management of their HIV care included age, race, geographic location, and access to technology. Some patients (13.6%) were unable to access the internet from their home and some (25.6%) were only able to access the internet through a mobile device. Furthermore, depending on the device being used, between 67% and 80% of patients reported they would use technology in order to access HIV-related information. The study also found that patients who were Black and/or Hispanic were less likely to utilize telemedicine. Finally, patients who were older than 65 were less interested in using technology to access information about HIV. This study demonstrated that health inequities remain with any form of telehealth and that willingness to engage in telehealth is affected by social determinants.
Another study highlighted additional factors responsible for affecting a patient’s use of telemedicine. This was highlighted in a study conducted between February and June 2018 where 371 PLWH were surveyed at the Thomas Street Health Center in Houston, Texas, USA.9 Fifty-seven percent of patients reported they would use telehealth, if available. Many patients reported several benefits of using telehealth, including telehealth being a better fit for their life schedule (69%), not needing to travel to clinic (63%), and having more privacy at home (62%). Findings from this study correlated with the mean HIV stigma score being higher in patients who were more interested in telehealth. This study showed no association between age, sex, race, household income, drug use, alcohol use, depression, or self-reported health status with the likelihood of using telehealth.
COVID-19 Data
One clinic in Rhode Island, USA, explained their expansion in telemedicine during COVID-19.10 This clinic utilized Zoom for Healthcare™ as a platform for visits in addition to the telephone visits. With Zoom™, the patients were texted a link prior to visit to check-in on the platform with staff and then participated in a virtual appointment with the provider in a private room. Appointments were conducted the same as any in-person visit, except for a physical examination. There were a few challenges with conducting these visits. One patient who was homeless and currently residing in a shelter had difficulty finding space to conduct the visit as they did not want to expose their HIV status to other residents of the shelter. An elderly patient did not have digital literacy to be able to use Zoom™ and the patient had to be called multiple times. However, the clinic addressed this by providing clear instructions on how to use technology prior to the medical visit. The clinic also sent out a survey to telemedicine participants. Of the 22 patients participating in the survey, 75% reported interest in continuing telemedicine after the pandemic. Though most of the feedback was positive, there were some concerns about privacy and data-breaches. Additionally, not every patient has a place available to conduct confidential medical appointments.
Another clinic in Missouri, USA, also used a Zoom™ platform featuring many benefits from patients transitioning to telemedicine.11 This clinic was the only clinic providing specialty HIV care in much of the state where many patients spent hours driving to attend their clinic appointment. Ninety percent of patients using telemedicine reported liking it and ranked it as better or just as good as traditional in-clinic visits. With the implementation of telemedicine, barriers to care such as difficulties with transportation, work schedules, stigma of being seen at an HIV clinic were overcome. Noted limitations included patients being concerned about the lack of a physical exam, not being able to properly communicate, and giving private information over the internet. Therefore, the clinic will likely continue telemedicine after the pandemic as they have seen a higher retention in patients.
Preexposure Prophylaxis (PrEP)
Aside from HIV care, there are also models for telemedicine expansion into PrEP care as a method for ending the HIV epidemic. One model evaluated retention in care for PrEP services in Iowa, USA, prior to the SARS-CoV-2 pandemic and found that of the 83 patients who engaged in telemedicine services, 60% were retained in care on day 180.12 Of these patients who were not retained, 18 had a documented plan for transition of care, while 15 were lost to follow up. With the telemedicine service, 96% obtained necessary labs per protocol with 100% adherence to required HIV testing, which is higher compared to traditional in-person clinic that obtained 77% of HIV tests indicated. Therefore, telemedicine for PrEP was effective.
One article evaluated the willingness of patients in Brazil to use telemedicine for PrEP.13 The study assessed 680 PrEP users where 23% consented to use telemedicine for PrEP care with HIV self-testing kits and 89% felt satisfied with their care when asked in a survey. This study also reported 79% of PrEP users expressed willingness to use HIV self-testing kits as part of their care. Interestingly, another study conducted in Brazil surveyed 11000 men who have sex with men and found only 44% expressed willingness to use HIV home testing for PrEP use and 87% expressed desire for follow-up consultation after test use.14 Therefore, use of telemedicine can be used for PrEP care, but should be tailored to how comfortable the patient is with self-testing and willingness to use telemedicine.
Discussion
The Infectious Diseases Society of America (IDSA) and HIV Medicine Association (HIVMA) recently released a guideline entitled “Advancing Digital Health Equity” that addresses many of the problems that came with the swift transition to telemedicine that many ambulatory clinics faced during the COVID-19 pandemic.1 One of the topics touched upon was the “digital divide,” where patients who were an ethnic minority and who lived in a more rural area were less likely to use desktop computers and rely on smartphones for internet access. It also addressed the lack of privacy some patients have. Noted suggestions included that programs offer technology to use during visits and provide headphones to allay privacy concerns, develop educational materials and offer instructions prior to the visit, conduct a test visit before the appointment, and train staff to use and assist in technology use.
A systematic review of mobile HIV interventions demonstrated the potential for telemedicine for PLWH to further expand beyond video-conferencing and telephone appointments.15 There were various protocols in place that included further education for patients, behavioral modification, linkage to care, and social support utilizing mobile apps, traditional websites, and messaging boards. Additionally, educating patients on various aspects of technology in people who may have low digital literacy to use can help overcome barriers. In a study assessing how older PLWH could utilize a health app, results showed patients over the age of 50 years had low usability of the app, yet, setting simple reminders to use the app increased usage.16
Although the impact of telemedicine on HIV was previously documented prior to the development of a global pandemic, these studies laid fundamental groundwork and implementation examples for implementation and adoption.4,5 Various models exist and can range from a mix of telephone, video, in-person visits or a hybrid approach to fit the patient and their healthcare needs. As clinicians, we cannot just assume a one size fits all approach but rather discuss preferences with each patient. It is important to ensure if telehealth is used as part of a patient’s care, they are comfortable with engaging in and using the technology. Clinical staff should assess if the patient has the necessary resources (ie device, private space, stable connection) and knowledge to participate in a telehealth visit.
There remains a paucity of data on the effects of telemedicine on clinical outcomes of HIV during COVID-19. What does show promise is patient interest in using telemedicine as part of their healthcare. The COVID-19 pandemic accelerated the expansion of telemedicine exponentially.
Conclusion
The use of telemedicine for HIV treatment has been successful in achieving viral suppression and benefitted patients living far distances from clinics. The COVID-19 pandemic has shown that telemedicine can be beneficial if used for certain patients interested in engaging with and using telemedicine, but there is a paucity of data. Although there may be limitations to the use of telemedicine, implementing and continuing the use of telemedicine beyond a global pandemic has demonstrated success in providing access to HIV care. Future studies should focus on the provision of HIV care using telemedicine beyond the pandemic and focus on ways to improve the telemedicine experience for the patient.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wood BR, Young JD, Abdel-Massih RC, et al. Advancing digital health equity: a policy paper of the infectious diseases society of America and the HIV medicine association. Clin Infect Dis. 2020;70(7):ciaa1525. doi:10.1093/cid/ciz410
2. Centers for Disease Control and Prevention. Using telehealth to expand access to essential health services during the COVID-19 pandemic; June 10, 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/telehealth.html.
3. Kaiser Family Foundation. Delivering HIV care and prevention in the COVID era: a national survey of Ryan White providers. Available from: https://www.kff.org/report-section/delivering-hiv-care-prevention-in-the-covid-era-a-national-survey-of-ryan-white-providers-issue-brief/.
4. Young JD, Patel M, Badowski M, et al. Improved virologic suppression with HIV subspecialty care in a large prison system using telemedicine: an Observational Study with historical controls. Clin Infect Dis. 2014;59(1):123–126. doi:10.1093/cid/ciu222
5. Ohl ME, Richardson K, Rodriguez-Barradas MC, et al. Impact of availability of telehealth programs on documented HIV viral suppression: a cluster-randomized program evaluation in the veterans health administration. Open Forum Infect Dis. 2019;6(6):ofz206. doi:10.1093/ofid/ofz206
6. Spinelli MA, Hickey MD, Glidden DV, et al. Viral suppression rates in a safety-net HIV clinic in San Francisco destabilized during COVID-19. AIDS. 2020;34(15):2328–2331. doi:10.1097/QAD.0000000000002677
7. Doorways. Homelessness and HIV. Available from: https://www.doorwayshousing.org/about-housing-hiv/homelessness-and-hiv/.
8. Marhefka SL, Lockhart E, Turner D, et al. Social determinants of potential eHealth engagement among people living with HIV receiving Ryan White case management: health equity implications from project TECH. AIDS Behav. 2020;24(5):1463–1475. doi:10.1007/s10461-019-02723-1
9. Dandachi D, Dang BN, Lucari B, Teti M, Giordano TP. Exploring the attitude of patients with HIV about using telehealth for HIV care. AIDS Patient Care STDS. 2020;34(4):166–172. doi:10.1089/apc.2019.0261
10. Rogers BG, Coats CS, Adams E, et al. Development of telemedicine infrastructure at an LGBTQ+ clinic to support HIV prevention and care in response to COVID-19, providence, RI. AIDS Behav. 2020;24(10):2743–2747. doi:10.1007/s10461-020-02895-1
11. Dandachi D, Freytag J, Giordano TP, Dang BN. It is time to include telehealth in our measure of patient retention in HIV care. AIDS Behav. 2020;24(9):2463–2465. doi:10.1007/s10461-020-02880-8
12. Hoth AB, Shafer C, Dillon DB, Mayer R, Walton G, Ohl ME. Iowa TelePrEP: a public-health-partnered telehealth model for human immunodeficiency virus preexposure prophylaxis delivery in a rural state. Sex Transm Dis. 2019;46(8):507–512. doi:10.1097/OLQ.0000000000001017
13. Hoagland B, Torres TS, Bezerra DRB, et al. High acceptability of PrEP teleconsultation and HIV self-testing among PrEP users during the COVID-19 pandemic in Brazil. Braz J Infect Dis. 2020;101037.
14. Hoagland B, Torres TS, Bezerra DRB, et al. Telemedicine as a tool for PrEP delivery during the COVID-19 pandemic in a large HIV prevention service in Rio de Janeiro-Brazil. Braz J Infect Dis. 2020;24(4):360–364. doi:10.1016/j.bjid.2020.05.004
15. Maloney KM, Bratcher A, Wilkerson R, Sullivan PS. Electronic and other new media technology interventions for HIV care and prevention: a systematic review. J Int AIDS Soc. 2020;23(1):e25439. doi:10.1002/jia2.25439
16. Puig J, Echeverría P, Lluch T, et al. Health application for older HIV-infected patients: usability and patient’s satisfaction. Telemed J E Health. 2020;27(4):432–440. doi:10.1089/tmj.2020.0098.
17. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339 :b2535. doi:10.1136/bmj.b2535.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.