Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 14
Tattoo-Associated Viral Infections: A Review
Authors Cohen PR
Received 19 August 2021
Accepted for publication 12 October 2021
Published 23 October 2021 Volume 2021:14 Pages 1529—1540
DOI https://doi.org/10.2147/CCID.S284796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Philip R Cohen1,2
1Department of Dermatology, University of California, Davis Medical Center, Sacramento, CA, USA; 2Department of Dermatology, Touro University California College of Osteopathic Medicine, Vallejo, CA, USA
Correspondence: Philip R Cohen 10991 Twinleaf Court, San Diego, CA, 92131-3643, USA
Email [email protected]
Abstract: Tattoos, a decorative form of body art, are produced by inoculating pigment into the dermis. Tattoo-associated viral infections can be cutaneous and localized to the tattoo ink; however, viral pathogens acquired during inoculation can cause systemic disease. A comprehensive review of the literature only reveals a limited number of published reports regarding patients with tattoo-associated cutaneous viral lesions. Cutaneous viral pathogens causing lesions to occur on a tattoo include herpes simplex virus (HSV), human papillomavirus (HPV), molluscum contagiosum, rubella, and vaccinia. HPV lesions (45 patients) and molluscum contagiosum (14 patients) are the most frequently reported tattoo-associated viral lesions; nearly all the patients were immunocompetent. HPV lesions included verruca vulgaris (29 patients), verruca plana (14 patients) and human immunodeficiency virus (HIV)-associated acquired epidermodysplasia verruciformis (two men). Hypotheses for tattoo-associated HPV lesions and molluscum contagiosum include a black ink-induced cutaneous immunocompromised district since the viral lesions all occurred in black or dark ink and the use of virus-contaminated instruments, pigment, or both during tattoo inoculation. Other sources of HPV include viral spread from a wart that is present but not associated with the tattoo site or virus transmission from the tattooist resulting from contact with a wart on an ungloved hand or HPV-containing saliva used to thin the pigment. Herpes compunctorum (three patients), vaccinia (two patients), and rubella (one patient) were less commonly reported. Blood borne viral pathogens associated with systemic manifestations – such as hepatitis B, hepatitis C and HIV – have also been acquired during tattoo inoculation; however, health care interventions have been adopted to attempt prevention of viral agent transmission during tattoo acquisition.
Keywords: hepatitis, herpes simplex virus, human papillomavirus, molluscum contagiosum, tattoo, virus
Introduction
Tattooing produces a permanent design by inoculating exogenous pigment into the dermis. Dermatologic and systemic complications have been observed in patients who receive tattoos.1–35 In one series of 234 dermatology patients with tattoos, infection–either impetigo or warts–confined to the tattoo was observed in two (0.9%) of the patients.3
Cutaneous viral infections at the site of tattoos have been observed.3,9–11,14–35 In addition, systemic viral infections may develop in individuals who acquire a tattoo.4–8,12,13 Viral infections associated with tattoos are reviewed.
Materials and Methods
The purpose of this paper is to provide a comprehensive traditional narrative review of viral infections that have been described to occur on tattoos. The PubMed archive of biomedical literature at the US National Institutes of Health’s National Library of Medicine was used. Searches were performed of the following combination of terms, tattoo and German measles virus, hepatitis B virus, hepatitis C virus, herpew simplex virus, human immunodeficiency virus, human papillomavirus, molluscum contagiosum virus, rubella virus, smallpox virus, vaccinia virus, and warts.
The abstracts of the papers generated by each search were evaluated. For hepatitis B virus and hepatitis C virus, seminal reviews were selected. For herpes simplex virus, human immunodeficiency virus, molluscum contagiosum virus, rubella (German measles) virus, and vaccinia (smallpox) virus, all the articles generated–and any relevant papers included in the reference section of the articles–were included in this paper. Tattoo-associated human papillomavirus infection had recently been summarized; in addition to that review article, papers describing the initial observations of patients with warts occurring on their tattoos and additional reported patients not presented in the review article are included in this paper.
Many of the articles cited in this paper were published in journals with limited, and often non-gratis, access. An effort has been made to summarize the salient features of the patients who were affected by tattoo-associated viral infections. This has been accomplished by providing succinct, yet extensively detailed, tables that present the characteristics of the individuals who were included in this paper.
Discussion
Individuals who have acquired tattoos can also develop cutaneous or systemic viral infections (Table 1).3–35 Herpes simplex virus (HSV), human papillomavirus (HPV), and molluscum contagiosum are common cutaneous viral infections associated with tattoos. Previously, albeit rare, rubella and vaccinia are skin-related viral infections that have also been observed on tattoos.
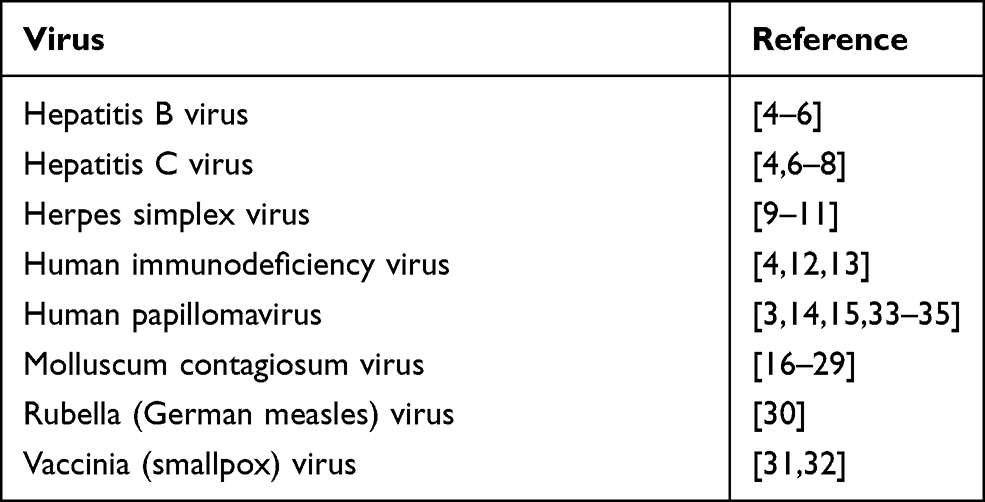 |
Table 1 Viral Infections and Tattoos |
Systemic viral infections associated with the acquisition of tattoos include hepatitis and human immunodeficiency virus (HIV). Both hepatitis B and hepatitis C have been associated with tattooing. Indeed, there is a five to 30% risk of hepatitis B transmission and a three to 7% risk of hepatitis C transmission following a single needlestick injury from an infected individual.4
Hepatitis B Infection
Hepatitis B is a deoxyribonucleic acid (DNA) virus. Blood or sexual contact are the most common modes of transmission of hepatitis B infection. Acquisition of hepatitis B infection results in acute infection that can potentially develop into a chronic infection; thereafter, some individuals develop liver cirrhosis or hepatocellular carcinoma or both. Indeed, in addition to needle stick injury and blood exposure (either through percutaneous or mucous membrane), tattooing (with unsterile needles) can also result in the transmission of hepatitis B in recipients of tattoos.4–6
A comprehensive systematic review and meta-analysis found that individuals involved in high-risk behaviors demonstrate the strongest association between tattooing and risk of acquiring hepatitis B. These individuals include drug users, HIV positive persons, persons who acquire their tattoos with reused needles or in non-professional tattoo parlors, and street youth. However, hepatitis B transmission is also observed in individuals from the community (such as blood donors, pregnant women, and students), patients in the hospital, and prison inmates.4–6
Several interventions have been suggested to prevent hepatitis transmission from tattooing. First is universal hepatitis B immunization. Second is education of individuals likely to get tattoos–prisoners and young adults. And third, not only the development of safe tattoo programs in prisons but also enhanced regulation of tattoo parlors with regard to maintaining the appropriate guidelines for infection control.4–6
Hepatitis C Infection
Hepatitis C is a ribonucleic acid (RNA) virus. Recently acquiring a tattooing has been reported in 6% of patients with acute hepatitis C infection. However, if the tattoo was received at a professional tattoo parlor, definitive evidence of an increased risk of hepatitis C infection was not observed.4,6–8
However, hepatitis C transmission from tattoos is prevalent in persons who use intravenous drugs, prisoners, and veterans. Indeed, there is also an increased risk of hepatitis C virus transmission if a tattoo is applied by friends, acquired in prison using non-sterile equipment, or if the recipient belongs to a high-risk group. The latter include drug users, homeless individuals, patients who attend sexually transmitted disease clinics, and sex workers.4,6–8
Similar to hepatitis B, the use of sterile equipment–particularly in prisons–should be encouraged to prevent hepatitis C virus transmission from tattooing. Also, youths should be educated to avoid receiving tattoos in potentially unsterile environments such as homes and prisons. Finally, educating and monitoring tattoo parlors for proper infection control measures is crucial.4,6–8
Herpes Simplex Virus
Herpes simplex virus-associated tattoo infection has only been, to the best of my knowledge, published in three individuals (Table 2).9–11 The first individual was reported by Marshall et al in 2007; the investigators coined the term “herpes compunctorum” to describe this phenomenon.9 Ten years later, Kluger and Armingaud reported the second patient; a year later, the third patient was described by Gerqari et al.10,11
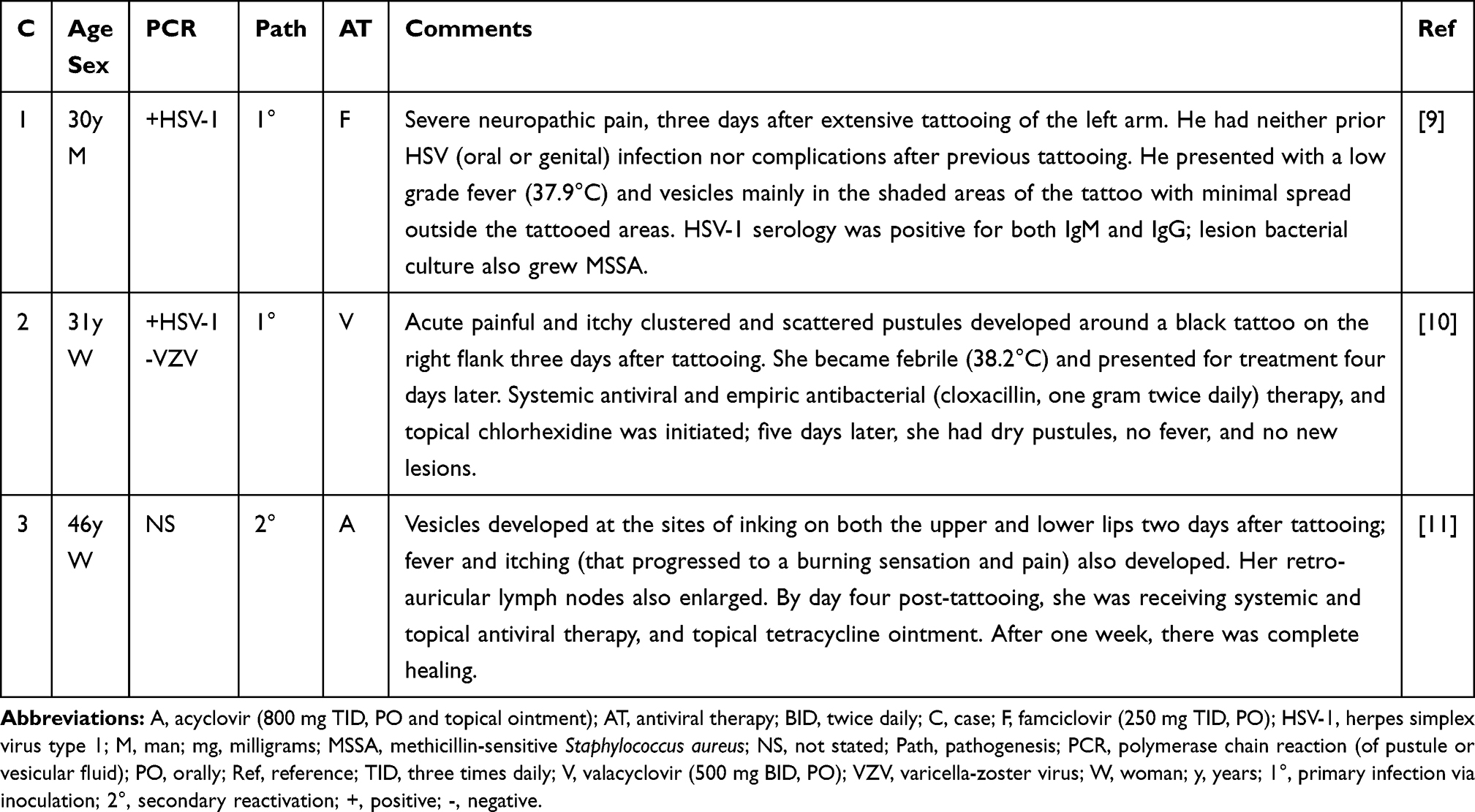 |
Table 2 Tattoo-Associated Herpes Compunctorum |
The first patient with a tattoo-associated HSV infection was a 30-year-old man who had his tattoo at a commercial tattoo parlor. The procedure included single-use needles following an initial drawing of the tattoo lines and subsequent shading. His treatment required a seven-day hospitalization. The investigators concluded that this was a primary inoculation of herpes simplex virus infection; although they postulated that the needle had become contaminated with HSV during the tattooing, they could not definitively exclude the possibility that the damaged skin became superinfected with the virus after the procedure.9
The second patient with tattoo-associated HSV infection also had her tattooing done by a professional artist in a parlor. She was a healthy 31-year-old woman. Similar to the initial patient, the researchers concluded that this was a primary HSV infection. However, in contrast to the previous investigators, they favored the possibility of superinfection of the virus occurring on the fresh and healing wounded skin following tattooing in contrast to the viral infection being transmitted by the tattooist during the procedure or contamination of the needle or the ink.10
The third patient with tattoo-associated HSV infection was a 46-year-old woman who worked in the medical sector and had a toxic thyroid adenoma that was treated by lobectomy; she developed post-surgical hypothyroidism and received 75 mg of levothyroxine daily. The cosmetic tattooing had been performed to outline her lips. She also had a prior history of herpes labialis; this was her second herpetic eruption of herpes labialis.11
Human Immunodeficiency Virus (HIV) Infection
Blood or body fluids or both can result in the transmission of HIV. The route of transmission is frequently through sexual intercourse; however, mother to baby transmission is also commonly observed. In addition, the use or abuse of drugs that are injected and acts of body adornment such as piercing and tattooing are skin breaching activities that allow direct inoculation of the virus.4,12,13
Yet, to the best of my knowledge, only three patients with tattoo-associated HIV infection have been reported (Table 3).12,13 Two were HIV-positive men who acquired their virus infection after being tattooed while incarcerated. The third was a woman who developed HIV infection following cosmetic tattooing of her lips, eyebrows and eyelashes.12,13
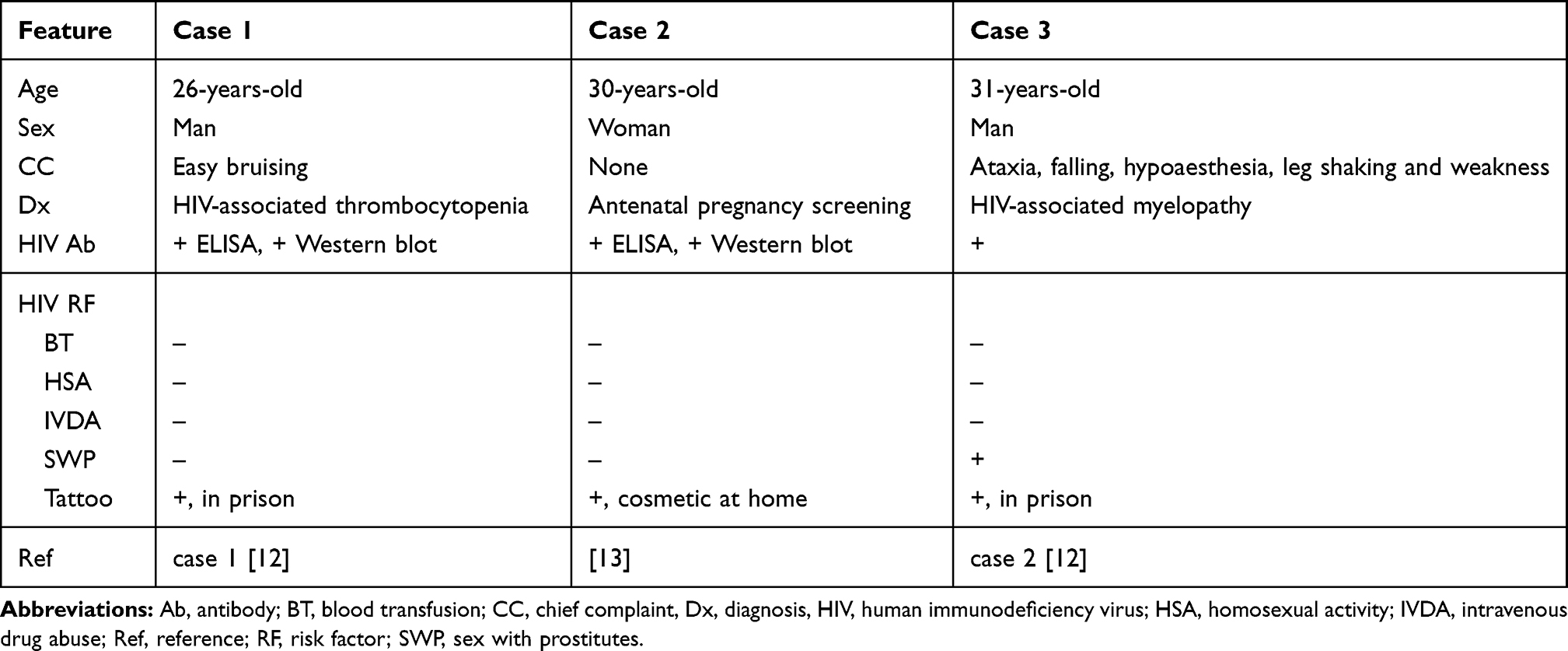 |
Table 3 Tattoo-Associated Human Immunodeficiency Virus Infection |
The first patient was 22-years-old when he received a tattoo while in prison. The tattooing was performed with an unsterilized needle that had previously been used to tattoo other prisoners. His HIV infection was discovered 4 years later when he presented with thrombocytopenia.12
The second patient was a 31-year-old prisoner with a 14-month history of symptoms which were eventually diagnosed as HIV-associated myelopathy. Prior to arriving in prison he had sex with prostitutes and this may have also been an HIV-related risk factor. However, he received multiple tattoos in prison seven months before the onset of his symptoms and was aware that other prisoners had been tattooed with the same dirty needles.12
The third patient was a 30-year-old woman who was experiencing her fifth pregnancy; she terminated her first pregnancy, had two subsequent miscarriages, and finally a healthy boy. Her husband and six-year-old son were HIV-negative. Positive results of the HIV screening performed during her first antenatal visit prompted her physicians to establish the source of her infection. Although she had unprotected intercourse with a new partner two to 3 years prior to the pregnancy (during a temporary separation from her husband), the partner was tested and found to be HIV negative. Additional inquiry revealed a potential mode of HIV transmission–she had permanent makeup cosmetic tattooing in Vietnam at her home by a mobile beauty therapist 3 years earlier. The unregulated home tattoo industry had previously been recognized to have a high incidence of breaches in infection control. She subsequently decided to terminate the pregnancy.13
Human Papillomavirus
Dr. TC Fox, in a single paragraph accompanied by a hand-drawn sketch, reported the first patient with verruca vulgaris on a tattoo in the Transactions of the New York Dermatological Society that were published in 1884 in the June and July issue (volume 2, page 216) of the Journal of Cutaneous and Venereol Diseases. He described a young man who had tattooed his forearm 5 years earlier; about a year after tattoo placement, warts began to develop on the indigo lines of the tattoo. Indeed, 19 of the 20 warts occurred on the tattoo lines.33
Dr. HFB Walker, 24 years later, described the second patient with tattoo-associated warts. In a short communication published in October 10, 1908, issue (volume 2, page 1104) of the British Medical Journal, the infective warts of a young Englishman were reported. The publication included a figure that showed not only the position but also the relative size of the warts on the tattoo lines. He had neither current nor prior history of other warts. Six months earlier he had received a tattoo created with Indian ink by an Italian in Port Elizabeth, South Africa; a month later, the warts began to appear. There was one larger bleeding wart and the 37 smaller warts.34
Subsequently, more than 50 years after Dr. Walker published his patient, Captain Dale B. Watkins (who was working at the US Naval Hospital in Key West, Florida) reported another man whose tattoo had warts in a paper titled “Viral disease in tattoos: verruca vulgaris” that was included in the August 1961 issue of Archives in Dermatology (volume 84, pages 306–309). He described a 21-year-old man with a rose tattoo on his left arm that was received 2 years prior; soon after the application of the tattoo, biopsy-confirmed warts appeared. The man, who had no other verruca, presented with seven warts in the black pigment of the tattoo. Both the patient and his father were emotionally traumatized by the alteration of the tattoo at the biopsy site. The remaining warts were not treated since a course of management that was agreeable could not be established.35
Including these three men, tattoo-associated HPV infections have included not only verruca vulgaris (29 patients) (Figure 1) but also verruca plana (14 patients), and acquired epidermodysplasia verruciformis (two HIV-positive men) (Table 4);3,14,15 epidemiologic and clinical features were not completely described in all the individuals. HPV lesions on tattoos occurred three times more frequently in men (75%, 21 patients) as compared to women (25%, 7 patients). Depending on the HPV lesion, the median onset age in both men and women was in their 30s or 20s.15
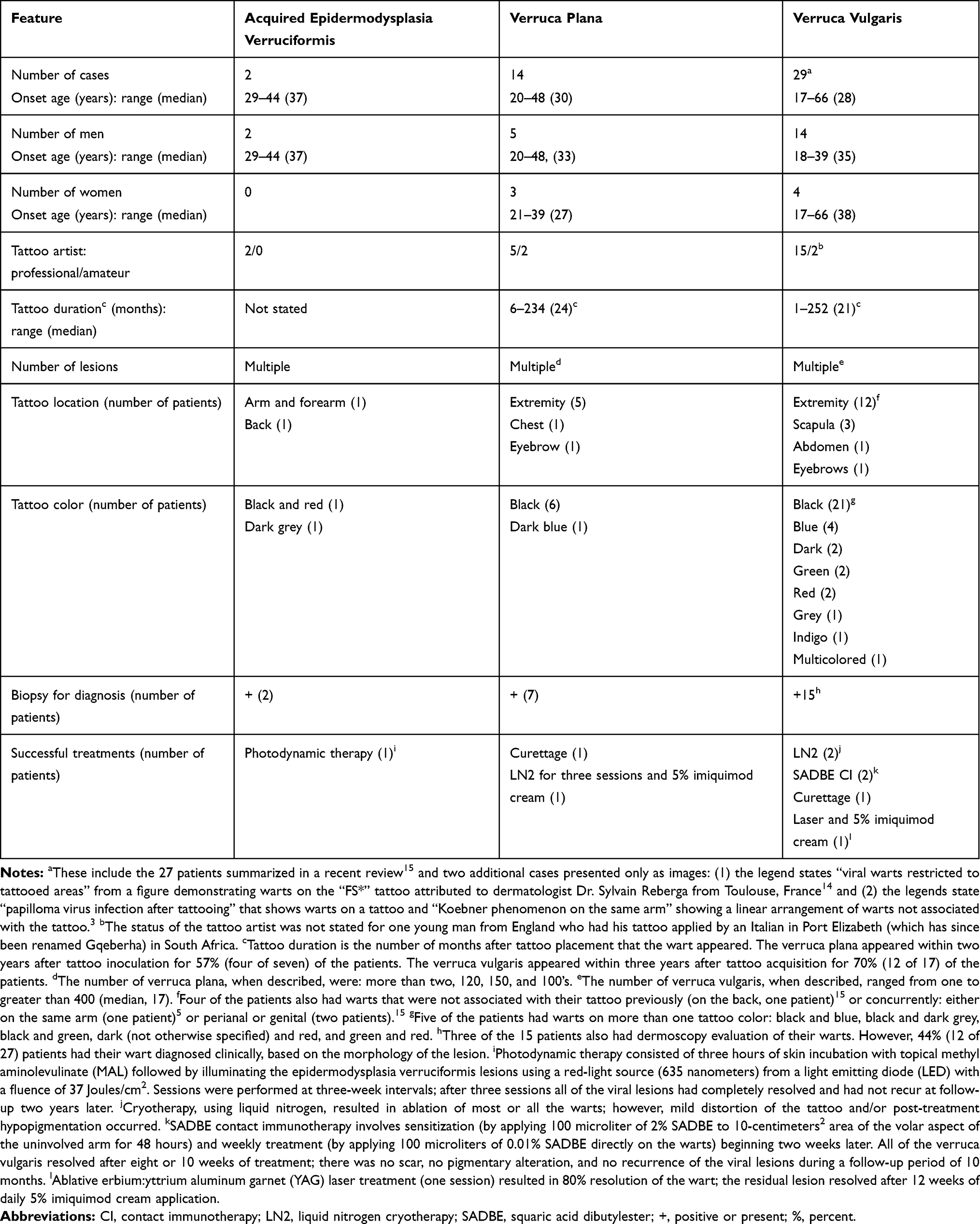 |
Table 4 Tattoo-Associated Human Papillomavirus Infections |
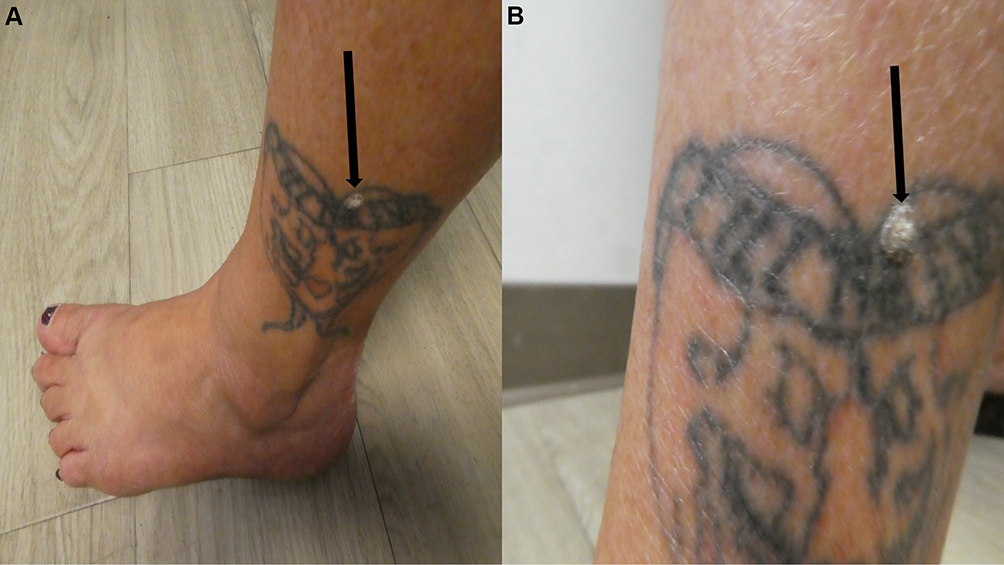 |
Figure 1 Tattoo-associated human papillomavirus infection. Distant (A) and closer (B) views of the left ankle of a 44-year-old woman show a verruca vulgaris (black arrow) that has developed on the black inked tattoo. She received her tattoo when she was 18 years old; the asymptomatic wart that developed within her tattoo appeared five years ago–26 years after tattoo inoculation–and subsequently increased in size. The patient’s tattoo-associated verruca vulgaris has been reported.15 |
Nearly all the patients were immunocompetent. Both men with HIV-associated acquired epidermodysplasia verruciformis were immunosuppressed because of their HIV infection. In addition, one of the men with verruca vulgaris was HIV positive. Several of the other patients with tattoo-associated HPV lesions were not only tested for HIV infection, but also for other viral infections (hepatitis B and hepatitis C) and syphilis; none of these individuals demonstrated any of these additional infections.15
All but four of the tattoos were performed by professional tattooists; in addition, one Englishman’s tattoo was inoculated by an Italian when he was in South Africa. The technique of the amateur tattoo artist may have been a factor in the acquisition of the patient’s tattoo-associated HPV infection. For example, one artist used a staple to inoculate a mixture of ball point pen ink and melted plastic; however, prior to creating the tattoo, he used his saliva to thin the material used for pigment.15
Four patients had additional evaluation (such as in situ hybridization, polymerase chain reaction and/or deoxyribonucleic acid sequencing) to identify the HPV type associated with their infection. One woman with tattoo-associated verruca vulgaris had HPV type 27 detected. Two men with tattoo-associated verruca plana had either HPV type 6B or HPV type 47. However, a positive reaction for HPV could not be demonstrated for one man with tattoo-associated verruca vulgaris.15
The tattoo duration prior to the onset of the HPV lesion ranged from 6 months to more than 19.5 years (median, 2 years) in patients with verruca plana and from 1 month to 21 years (median, 21 months) in patients with verruca vulgaris. However, the tattoo-associated HPV lesions appeared within either 2 years (57% of the seven patients with verruca plana) or 3 years (70% of the 17 patients with verruca vulgaris) after inoculation of the tattoo. Yet, in some individuals, prolonged duration between tattoo acquisition and the development of the associated HPV lesion was observed: 43% after 10 or more years for patients with verruca plana and either 24% between 5 and 8 years and 6% after 21 years for patients with verruca vulgaris.15
The number of viral lesions varied from 1 to 100s; many of the reports used descriptive terms such as multiple or numerous or countless. The warts were most frequently located on an extremity (18 patients); other sites included the back (four patients), eyebrow (two patients), and one patient on either the chest or the abdomen. Previous (one woman with a wart on her back) or concurrent warts (condyloma in either the genital or perianal area of two men and linearly distributed warts on the ipsilateral arm of one patient), not associated with the tattoo, were noted in four individuals.15
The tattoo-associated HPV lesion was in a dark-inked area of the tattoo in both patients with HIV-associated epidermodysplasia verruciformis and seven patients with verruca plana; one of the HIV-positive men also had wart in the red inked area of his tattoo. The wart was also in the dark-colored portion of the tattoo in all 29 patients with verruca vulgaris; in 24 of these patients, the wart was only found in one tattoo color whereas the viral lesion appeared in more than one tattoo color in five patients. It has been suggested that the black ink has caused the development of a cutaneous immunocompromised district that more readily enables the development of HPV lesions in that skin area.3,14,15
The diagnosis of tattoo-associated HPV lesions was based on the clinical impression in 33% (12 of 36) patients. Biopsy-confirmation of a suspected wart was performed in the remaining 67% of individuals. Three of the patients with verruca vulgaris also had dermoscopic evaluation of their lesions, prior to microscopic evaluation of a lesion biopsy.15
Successful treatment of warts on tattoos was only observed in seven patients; however, some of the individuals declined additional therapy after the diagnosis had been established. Curettage was effective in a man with verruca plana and a woman with verruca vulgaris. Cryotherapy with liquid nitrogen was useful either as a single modality (in two men with verruca vulgaris) or as a precursor to topical 5% imiquimod cream (one woman with verruca plana); however, both men experienced post-treatment hypopigmentation and one man noted mild distortion of his tattoo. In addition, monotherapy with liquid nitrogen resulted in no improvement for two men–one with HIV-associated epidermodysplasia verruciformis and one with verruca plana.15
Two men with verruca vulgaris were successfully treated, after eight or 10 weeks, with squaric acid dibutylester contact immunotherapy. One man with HIV-associated epidermodysplasia verruciformis had a complete resolution of his viral lesions after three sessions. And, one man with verruca vulgaris had a combination therapy consisting of ablative erbium:yttrium aluminum garnet (YAG) laser treatment (with 80% wart resolution after one session) followed by topical immunotherapy (with daily 5% imiquimod cream for 12 weeks).15
Several hypotheses have been proposed to account for the development of tattoo-associated HPV lesions. In addition to black (or dark) ink, tattoo inoculation-related trauma can also potentially contribute to the development of a cutaneous immunocompromised district and subsequent HPV infection at that skin site. However, viral contamination of either the instruments or pigment or both used by the tattooist during tattoo inoculation is the most likely etiology for pathogen introduction at the site of the tattoo. Also, the tattoo artist may be the source of HPV infection–either a wart-containing ungloved hand or virus-containing saliva being used to thin the pigment to the appropriate consistency. Other possibilities include inoculation-related traumatic spread of an unrecognized preexisting wart at the site of tattoo inoculation or subsequent spread of HPV from currently existing or previous warts at different locations than where the tattoo is created.15
Molluscum Contagiosum
Molluscum contagiosum, a poxvirus-associated infection, clinically presents as umbilicated papules. It is frequently observed in children and may be located on the antecubital and popliteal fossa, the axilla, and the trunk. However, in adult patients, it may be a sexually transmitted disease–particularly when the lesion is in the genital region.19,23
Tattoo-related molluscum contagiosum has been observed (Table 5).16–29 Characteristics of these individuals have been provided for 11 of the patients: one woman and 10 men. The individuals were most frequently from Spain (five patients) and Italy (three patients); one patient was from either Brazil, England, or France.
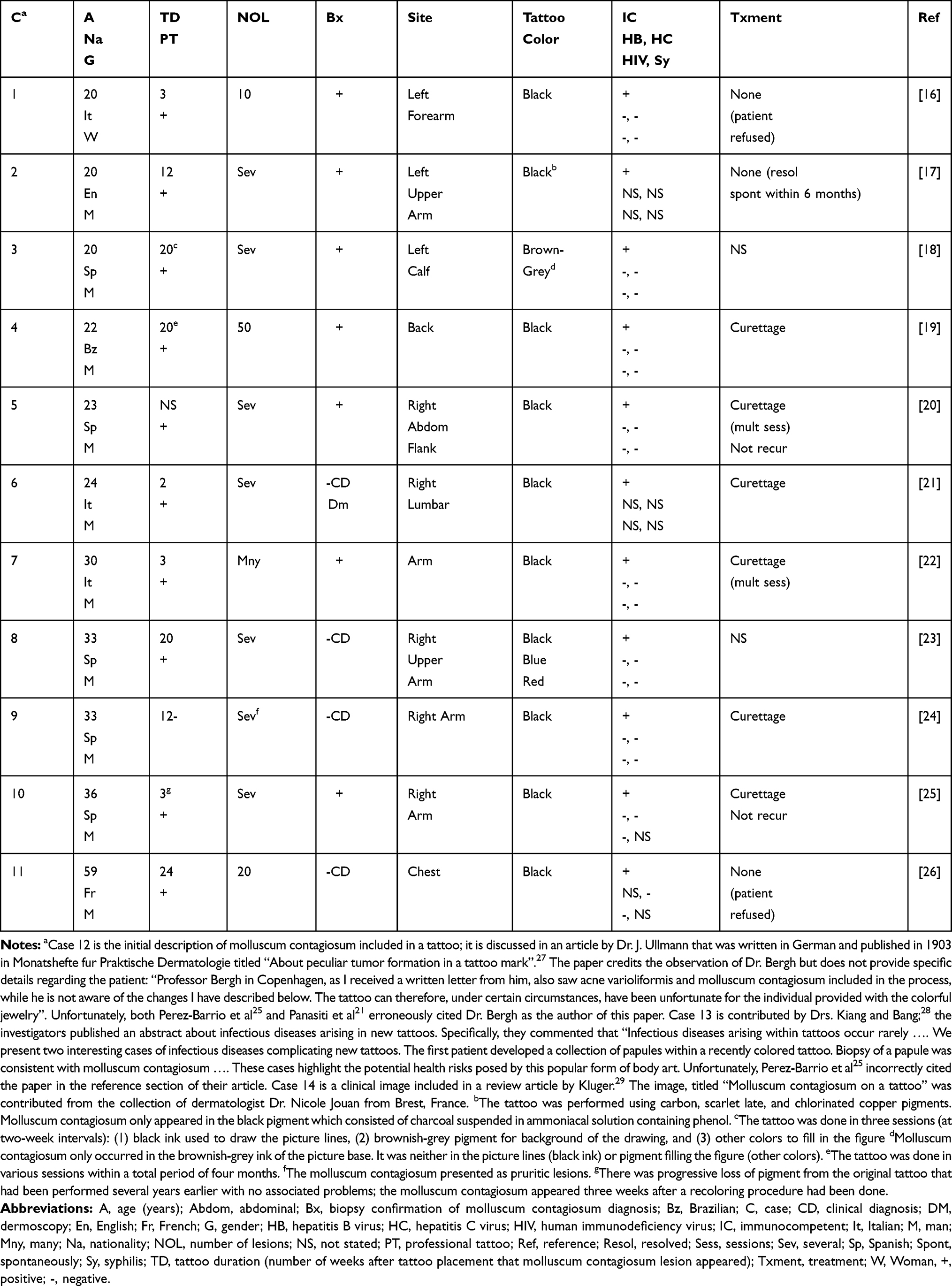 |
Table 5 Tattoo-Associated Molluscum Contagiosum Virus Infection |
The woman was 20 years old. The men ranged in age from 20 years to 59 years (median, 27 years). Ninety percent of the men were 36 years old or younger.
Ten of the tattoos were professionally done. However, for one individual, the patient’s friend–without protective measures–performed his tattoo. Subsequently, 3 months later, the 33-year-old Spanish man presented with several pruritic molluscum contagiosum located on the inked lines of the tattoo on his right arm.24
The molluscum contagiosum appeared two to 24 weeks (median, 12 weeks) after the tattoo was performed. When specified, the number of lesions ranged from 10 to 50 lesions (median, 20 lesions). However, the lesion number was most frequently described as several (seven patients); for one patient, the lesion number was described as many.
The diagnosis of molluscum contagiosum was confirmed by microscopic examination of a tissue specimen of the lesion for seven patients. The diagnosis was established based on clinical morphology of the lesions for four patients. Dermoscopy was performed for one patient–a 24-year-old man who, 2 weeks after receiving a tattoo of a lion on his right lumbar region–developed several asymptomatic popular lesions; examination of each individual lesion revealed a small whitish discoid area in the center of a round white shiny lesion.21
The most common locations of the molluscum contagiosum-containing tattoo were the upper extremity (six patients: arm, three patients; upper arm, two patients; and forearm, one patient) and the torso (three patients: back, two patients; and abdomen, one patient). Less often, each site in only one patient, the tattoo with its associated molluscum contagiosum was on the calf or chest. In all the individuals, viral lesions were not found at any other site.
The tattoo pigment color in which the molluscum contagiosum developed was black for 10 of the patients. A 33-year-old Spanish man with a multi-colored tattoo developed molluscum contagiosum not only in the areas of black ink but also in locations inked in either blue or red.23 A 20-year-old Spanish man with a multi-colored tattoo only had molluscum contagiosum over the brown-grey tattoo background; lesions did not occur on either black-inked picture lines or the other colors that were used to fill in the tattoo.18
All the patients were immunocompetent. Eight of the patients were also evaluation for other sexually transmitted diseases that could also be transmitted by tattooing. Hepatitis B (eight patients), hepatitis C (nine patients), HIV (nine patients), and syphilis (seven patients) were absent in all these individuals.
Management of the molluscum contagiosum was described in nine of the patients. Curettage of the viral lesions–either once (four patients) or on multiple occasions (two patients) was performed for six patients; there was no recurrence observed at follow-up of two of these individuals.20,25 Three patients did not receive any treatment; two of the individuals refused therapy16,26 and the lesions resolved spontaneously within 6 months in a 20-year-old English man who had several molluscum contagiosum on his left upper arm tattoo.17
Two potential mechanisms of pathogenesis were postulated for the development of tattoo-associated molluscum contagiosum. The first hypothesis for the transmission of poxvirus involves exposure to a contaminated fomite–particularly the instruments (needles) used for tattooing.16,18,19,22,23 The second theory is that either the tattoo ink or the water used to dilute the ink contained poxvirus.16–19,23 Some of the investigators have also suggested that the black pigment in the ink created a cutaneous immunocompromised district by promoting a reduction of cellular immunity or humoral immunity or both and enabling the development of molluscum contagiosum within the black-inked areas of the tattoo.16,24
Rubella (German Measles) Virus
Rubella, also known as German measles, is a viral infection that presents with a maculopapular rash on the face and subsequently spreads to the trunk and extremities; accompanying symptoms include fever, lymphadenopathy, headaches, arthralgias, and conjunctivitis. Currently, the mumps, measles and rubella (MMR) vaccine has interrupted the transmission of rubella. However, prior to vaccination, rubella lesions were observed not only in tattoos but also on the remainder of the skin; indeed, in 1979, Dr. Goldstein published an image provided by R. G. Davis, MD of rubella in a tattooed lady.30
Vaccinia (Smallpox) Virus
A bifurcated needle containing vaccine is used to repeatedly traumatize the skin to deliver vaccinia smallpox vaccine. Once inoculated, the live virus replicates in the dermis and–within 2 to 5 days–a small papule appears that progresses into a vesicle and then a pustule (which designates that the vaccine has successfully taken) during a total period of 8 to 10 days. Eventually, a scab develops at the pustule site, which subsequently detaches, leaving a residual scar.31
Tattoo-associated vaccinia (smallpox) autoinoculation has been reported in two men (Table 6).31,32 The first report, published in 1930 by Dr. Wilde, included vivid descriptions not only of the soldier’s recently acquired tattoo but also of the reaction to the smallpox vaccination that was inoculated near the tattoo’s upper edge.32 The more recently published paper in 2019 describes a soldier who, 4 days after vaccination, received a “touch up” directly over his inoculation site of a previous tattoo and experienced smallpox autoinoculation.31
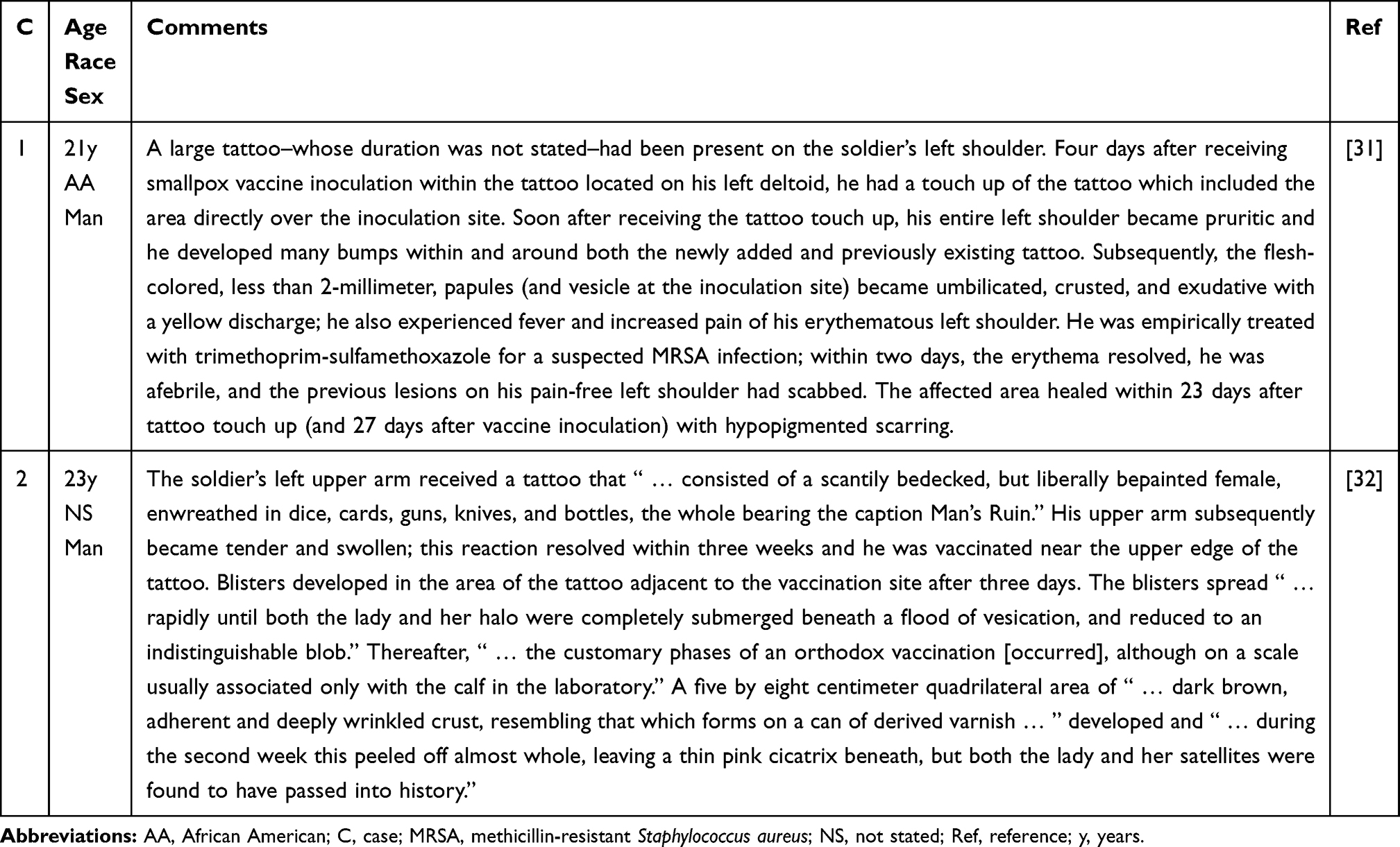 |
Table 6 Tattoo-Associated Vaccinia (Smallpox) Autoinoculation |
In addition, from 2003 to 2018, the Vaccine Adverse Events Reporting System (VAERS) database was search using the following terms: smallpox, tattoo and vaccinia. Thirteen cases associated with tattoo and smallpox inoculation complications were discovered. The tattoo was placed either directly over or adjacent to the vaccinia inoculation site within 96 hours following vaccine administration in six cases; however, reactions occurred up to 3 years post-inoculation. When described, the reactions included bumps and pustules; one person was febrile.31
The investigators postulate that both the tattoo and the vaccine create a cutaneous immunocompromised district of local immune dysregulation that is prone to the development of skin adverse events or cutaneous conditions in the affected area. Hence, the Assistant Secretary of Defense for Health Affairs (ASDHA) advised that tattooed skin not be selected as a vaccination site; subsequently, the United States Army Public Health Command (USAPHC) clarified this recommendation with regard to vaccinia administration: new tattoos should not be acquired until the vaccination site is healed and receiving tattoos within 30 days or less of vaccinia vaccination was contraindicated. Thereafter, the Military Vaccine Agency extended the period from vaccination to tattoo acquisition to 60 days.31
Conclusion
Tattoo-associated viral infections have been caused by pathogens that predominantly present with either cutaneous lesions (HSV infection, HPV, molluscum contagiosum, rubella, and vaccinia) or systemic manifestations (hepatitis B, hepatitis C, and HIV). HPV lesions in 45 patients (predominantly verruca vulgaris and verruca plana and less often acquired epidermodysplasia verruciformis) and molluscum contagiosum in 14 patients are the most observed viral lesions occurring on tattoos. Nearly all the patients were immunocompetent; however, both men who developed acquired epidermodysplasia verruciformis were HIV-positive. Herpes compunctorum (tattoo-associated HSV infection) has only been described in three patients; similarly, viral infections of tattoos caused by rubella (one patient) and vaccinia (two patients) were rare. The observation of individuals with newly acquired tattoo-associated rubella is unlikely based upon current medical practice of routine childhood vaccination for rubella. Likewise, new patients with tattoo-associated vaccinia are not anticipated since the use of smallpox vaccination has been significantly diminished. The potential to acquire blood-borne viral pathogens such as hepatitis B, hepatitis C and HIV during tattooing still exists; however, health care interventions to prevent transmission of these viral agents during the acquisition of a tattoo may be helpful in reducing the development of the virus-associated diseases in these individuals.
Disclosure
Dr. Philip R Cohen reports he is a consultant for ParaPRO. However, this relationship has no financial conflict of interest regarding the current paper.
References
1. Islam PS, Chang C, Selmi C, et al. Medical complications of tattoos: a comprehensive review. Clin Rev Allergy Immunol. 2016;50(2):273–286. doi:10.1007/s12016-016-8532-0
2. Cohen PR, Erickson CP, Uebelhoer NS, Calame A. Tattoo-associated basal cell carcinoma: coincident or coincidence. Biomed Hub. 2020;5(2):2055–2062. doi:10.1159/000508208
3. Kazandjieva J, Tsankov N. Tattoos: dermatological complications. Clin Dermatol. 2007;25(4):375–382. doi:10.1016/j.clindermatol.2007.05.012
4. Messahel A, Musgrove B. Infective complications of tattooing and skin piercing. J Infect Public Health. 2009;2(1):7–13. doi:10.1016/j.jiph.2009.01.006
5. Jafari S, Buxton JA, Afshar K, Copes R, Bahariou S. Tattooing and risk of hepatitis B: a systematic review and meta-analysis. Can J Public Health. 2012;103(3):207–212. doi:10.1007/BF03403814
6. Nishioka SDA, Gyorkos TW, Joseph L, Collet JP, Maclean JD. Tattooing and risk for transfusion-transmitted diseases: the role of the type, number and design of the tattoos, and the conditions in which they were performed. Epidemiol Infect. 2002;128(1):63–71. doi:10.1017/S0950268801006094
7. Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012;54(8):1167–1178. doi:10.1093/cid/cir991
8. Jafari S, Copes R, Baharlou S, Etminan M, Buxton J. Tattooing and the risk of transmission of hepatitis C: a systematic review and meta-analysis. Int J Infect Dis. 2010;14(11):e928–e940. doi:10.1016/j.ijid.2010.03.019
9. Marshall CS, Murphy F, McCarthy SE, Cheng AC. Herpes compunctorum: cutaneous herpes simplex virus infection complicating tattooing. Med J Aust. 2007;187(10):598. doi:10.5694/j.1326-5377.2007.tb01435.x
10. Kluger N, Armingaud P. Herpes simplex infection on a recent tattoo. A new case of “herpes compunctorum”. Int J Dermatol. 2017;56(1):e9–e10. doi:10.1111/ijd.13388
11. Gerqari AB, Ferizi M, Kotori M, et al. Activation of herpes simplex infection after tattoo. Acta Dermatovenerol Croat. 2018;26(1):75–76.
12. Doll D. Tattooing in prison and HIV infection. Lancet. 1988;1(8575–8576):66–67. doi:10.1016/S0140-6736(88)91054-9
13. Garland SM, Ung L, Vujovic OV, Said JM. Cosmetic tattooing: a potential transmission route for HIV? Aust N Z J Obstet Gynaecol. 2006;46(5):458–459. doi:10.1111/j.1479-828X.2006.00635.x
14. Kluger N. Cutaneous and systemic complications associated with tattooing. Presse Med. 2016;45(6Pt1):567–576. doi:10.1016/j.lpm.2016.02.016
15. Cohen PR. Verruca vulgaris occurring on a tattoo: case report and review of tattoo-associated human papillomavirus infections. Cureus. 2021;13(8):e17575.
16. Salmaso F, Gnecchi L, Gianotti R, Verladi S. Molluscum contagiosum on a tattoo. Acta Derm Venereol. 2001;81(2):146–147. doi:10.1080/00015550152384362
17. Foulds IS. Molluscum contagiosum: an unusual complication of tattooing. Br Med J (Clin Res Ed). 1982;285(6342):607. doi:10.1136/bmj.285.6342.607
18. Perez Gala S, Alonso Perez A, Rios Buceta L, Aragues Montanes M, Garcia Diez A. Molluscum contagiosum on a multicoloured tattoo. J Eur Acad Dermatol Venereol. 2006;20(2):221–222. doi:10.1111/j.1468-3083.2005.01363.x
19. Molina L, Romiti R. Molluscum contagiosum on tattoo. An Bras Dermatol. 2011;86(2):352–354. doi:10.1590/S0365-05962011000200022
20. Ruiz-Villaverde R, Sanchez-Cano D. Pearled papules over tattoo: molluscum contagiosum. Pan Aft Med J. 2013;16:49.
21. Panasiti V, Devirgiliis V, Roberti V, Curzio M, Calvieri S. Molluscum contagiosum on a tattoo: usefulness of dermoscopy. Int J Dermatol. 2008;47(12):1318–1319. doi:10.1111/j.1365-4632.2008.03747.x
22. De Giorgi V, Grazzini M, Lotti T. A three-dimensional tattoo: molluscum contagiosum. CMAJ. 2010;182(9):E382. doi:10.1503/cmaj.091480
23. Grillo E, Urech M, Vano-Galvan S, Jaen P. Lesions on tattooed skin–a case study. Aust Fam Physician. 2012;41(5):308–309.
24. Blasco-Morente G, Naranjo-Diaz MJ, Perez-Lopez I, Martinez-Lopez A, Garrido-Colmenero C. Molluscum contagiosum over tattooed skin. Sultan Qaboos Univ Med J. 2016;16(2):e257–e258. doi:10.18295/squmj.2016.16.02.022
25. Perez-Barrio S, Gonzalez-Hermosa MR, Raton JA, Diaz-Perez JL. Molluscum contagiosum over a tattoo. Actas Dermosifiliogr. 2009;100(2):152–154.
26. Kluger N, Comte C, Guillot B. Molluscum contagiosum on a tattoo. Ann Dermatol Venereol. 2007;134(5 Pt 1):506–507. doi:10.1016/S0151-9638(07)89231-3
27. Ullmann J. About peculiar tumor formation in a tattoo mark. Monatshefte Fur Praktische Dermatologie. 1903;37(2):49–52.
28. Kiang S-H, Bang RH. Infectious diseases arising in new tattoos: molluscum contagiosum and methicillin-resistant Staphylococcus aureus [P2011–Abstract at Poster Session]. J Am Acad Dermatol. 2006;54(3, Suppl. AB):AB155.
29. Kluger N. Cutaneous infections related to permanent tattooing. Med Mal Infect. 2011;41(3):115–122. doi:10.1016/j.medmal.2010.09.013
30. Goldstein N
31. Carius BM, Dodge PM, Randles JD. Smallpox autoinoculation via tattoo in a soldier. Mil Med. 2019;184(1–2):e275–e279. doi:10.1093/milmed/usy180
32. Wilde AG. Vaccina infected tattoo. Case report. New Orleans Med Surg J. 1929–1930;82:385–386.
33. Fox TC. Warts occurring on tattooed lines. J Cutan Vener Dis. 1884;2:216.
34. Walker HFB. Infective warts. Br Med J. 1908;2:1104.
35. Watkins DB. Viral disease in tattoos: verruca vulgaris. Arch Dermatol. 1961;84:306–309. doi:10.1001/archderm.1961.01580140132017
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.