Back to Journals » International Journal of Women's Health » Volume 18
Targeted Duct Excision Reduces Recurrence and Shortens Treatment Duration in Periductal Mastitis: A Retrospective Cohort Study
Authors Wang P ![]() , Li L, Liu Y, Shi Y, Zhang X, Wu J
, Li L, Liu Y, Shi Y, Zhang X, Wu J
Received 20 November 2025
Accepted for publication 17 February 2026
Published 20 February 2026 Volume 2026:18 583120
DOI https://doi.org/10.2147/IJWH.S583120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Pin Wang,1,2 Ling Li,3 Ying Liu,4 Yushuya Shi,5 Xiangyu Zhang,5 Jian Wu1,2
1Department of General Surgery, The Third People’s Hospital of Chengdu, Chengdu, 610000, People’s Republic of China; 2Center of Breast and Thyroid Surgery, The Third People’s Hospital of Chengdu, Chengdu, 610000, People’s Republic of China; 3Department of Pathology, The Third People’s Hospital of Chengdu, Chengdu, 610000, People’s Republic of China; 4Department of Ultrasound, The Third People’s Hospital of Chengdu, Chengdu, 610000, People’s Republic of China; 5Department of Hepatobiliary and Breast/Thyroid Surgery, The Second People’s Hospital of Jintang County, Chengdu, 610000, People’s Republic of China
Correspondence: Pin Wang, Email [email protected] Jian Wu, Email [email protected]
Objective: Periductal mastitis (PDM) is characterized by prolonged treatment and high recurrence, yet no large-scale study has identified its recurrence risk factors.
Methods: A total of 150 treatment-naïve patients diagnosed with PDM at the Third People’s Hospital of Chengdu from January 2019 to March 2025 were retrospectively included. Univariate and multivariate Cox regression analyses were used to identify factors associated with recurrence; Kaplan–Meier and log-rank tests assessed recurrence-free survival. Baseline patient characteristics, along with treatment duration, time to recurrence, and cosmetic outcomes, were systematically recorded.
Results: Targeted duct excision was the only independent protective factor against recurrence (adjusted HR = 0.09, 95% CI: 0.04– 0.20; p < 0.001). The recurrence rate was 9.0% (7/78) in the excision group versus 70.8% (51/72) in the non-excision group. Median initial treatment duration was shorter (52 [29– 73] vs 110.5 [81– 145] days; p < 0.001), and among relapsed patients, time from initial treatment end to recurrence was longer (136 [108– 159] vs 75 [54– 96] days; p < 0.001). Among patients who underwent targeted duct excision, cosmetic outcomes were favorable, characterized by inconspicuous periareolar scars, high patient satisfaction (88.5%), and successful correction of inverted nipples in eligible cases.
Conclusion: In patients with PDM, targeted duct excision significantly reduces recurrence risk, shortens treatment duration, and preserves breast appearance, suggesting that this surgical approach should be considered as the primary treatment option for PDM.
Keywords: periductal mastitis, targeted duct excision, recurrence, Cox regression analysis
Introduction
Periductal mastitis (PDM) is a chronic, benign inflammatory breast disease primarily affecting young women of non-lactating age. It typically presents with recurrent erythema, pain, abscess formation, and persistent sinus tracts in the periareolar region, often accompanied by nipple retraction or serous/purulent nipple discharge.1,2 Although PDM is not malignant, its clinical course is highly disruptive: most patients experience multiple acute flares, each requiring needle aspiration, or even incision and drainage. In some cases, repeated ulcerations lead to scar contracture of the breast skin, destruction of glandular architecture, and even significant breast deformity or disfigurement. Compounding the challenge is the exceptionally high recurrence rate—commonly reported at around 50%.3,4 This recurring cycle of “treatment–remission–relapse” causes ongoing physical suffering and psychological distress, including anxiety and social withdrawal. It also substantially prolongs the overall treatment duration and increases the frequency of outpatient visits, imposing a considerable healthcare burden on both individuals and society while further exacerbating physical and emotional trauma.
Although PDM imposes a substantial clinical burden, no retrospective cohort study has specifically investigated risk factors for its recurrence. Existing literature primarily focuses on etiological hypotheses or anecdotal treatment experiences, with a lack of systematic follow-up in large patient cohorts.5–7
To address this gap, we retrospectively enrolled 150 patients with confirmed PDM and systematically evaluated recurrence-associated factors using Cox proportional hazards regression and Kaplan–Meier survival analysis. We further assessed the comprehensive impact of targeted duct excision on treatment duration, time to recurrence, and cosmetic satisfaction, aiming to provide evidence-based guidance for optimizing individualized management strategies in PDM.
Methods
Study Design and Population
This single-center retrospective cohort study included patients diagnosed with PDM who were treated at the Department of Breast and Thyroid Surgery, The Third People’s Hospital of Chengdu, between January 2019 and March 2025. The diagnosis of PDM was based on the following composite criteria: all patients were non-lactating women presenting with periareolar erythema, pain, inflammatory mass, abscess, or sinus tract formation. Breast ultrasound revealed subareolar duct dilatation (diameter ≥2 mm), duct wall thickening, and a hypoechoic halo around the duct. All patients underwent core needle biopsy.8 Histopathological confirmation of PDM required dense periductal infiltration by lymphocytes and plasma cells, in the absence of granulomatous inflammation, epithelioid histiocytes, multinucleated giant cells, lobular involvement, or malignant cells—thereby excluding breast carcinoma and granulomatous lobular mastitis.9
Inclusion criteria: (1) Treatment-naïve patients at initial presentation (ie, first visit to our center for PDM-related symptoms, with no prior surgical intervention, ductal aspiration, or systemic medical therapy for this condition received elsewhere); (2) age ≥18 years; (3) confirmed diagnosis of PDM based on integrated clinical, imaging, and histopathological findings; (4) complete baseline clinical data; and (5) completion of at least 3 months of follow-up, or documented recurrence within the first 3 months of follow-up.
Exclusion criteria: (1) Concurrent or prior breast malignancy; (2) Immunodeficiency, active tuberculosis, granulomatous mastitis, or other systemic inflammatory/autoimmune diseases; (3) Missing key clinical or outcome data; (4) Change in initial treatment strategy during follow-up (eg, transition from non-surgical to surgical management, or vice versa).
A total of 150 patients were ultimately included. All participants provided informed consent, and the study protocol was approved by the Ethics Committee of The Third People’s Hospital of Chengdu (Approval No. 2024-S-403), and the study complies with the Declaration of Helsinki.
Clinical Management and Definition of Interventions
In this study, the clinical management of periductal mastitis (PDM) was based on three distinct phases of disease progression: the inflammatory mass phase, the abscess phase, and the chronic sinus tract phase. Treatment decisions at each stage were made through shared decision-making, taking into account both clinical features and patient preferences.
During the inflammatory mass phase, patients presented with a well-defined breast mass without fluctuance, erythema, or purulent discharge. At this stage, we offered targeted duct excision combined with mass excision as a definitive treatment option. Patients who declined surgery were managed conservatively with close observation. However, in our cohort, nearly all patients in the conservative group eventually developed suppuration and progressed to the abscess phase.
Upon entering the abscess phase, characterized by local erythema, fluctuance, and/or pus formation, acute infection was first addressed according to our institutional protocol. Patients underwent either ultrasound-guided aspiration or periareolar incision and drainage, and pus samples were sent for bacterial culture. Antibiotics were adjusted based on antimicrobial susceptibility results when cultures were positive.10 Once acute inflammation resolved and purulent discharge ceased, patients were re-evaluated: those who consented proceeded to targeted duct excision, while those who declined continued local wound care until complete healing.
In the chronic sinus tract phase, patients presented with persistent or recurrent draining sinuses after initial abscess resolution. Initial management focused on daily wound dressing and infection control. After inflammation subsided and the sinus tract stabilized (typically over several weeks), we offered combined targeted duct and sinus tract excision as curative surgery. For patients who refused surgery, conservative management with ongoing wound care was maintained until spontaneous closure occurred.
Targeted duct excision was performed as follows: preoperative localization of abnormal ducts was achieved using color Doppler ultrasound and breast MRI. In cases with nipple discharge, methylene blue was injected through the discharging orifice to delineate the affected lactiferous duct. A 2–3 cm curvilinear incision was made along the periareolar margin (or around the sinus opening), and the involved duct—including any blue-stained segments—was excised. For distal lesions, intraoperative ultrasound-guided vacuum-assisted excision (eg, Mammotome system) was employed. Concurrent correction of preexisting nipple inversion was performed when indicated.
The non-excision group included only patients who did not undergo any duct excision procedure at any point during follow-up. Their management was strictly limited to non-surgical interventions, such as antibiotic therapy, abscess drainage (aspiration or incision), and local wound care for sinus tracts.
Data Collection and Variable Definitions
Demographic, clinical, and disease-related data were extracted retrospectively from the electronic medical records system. Demographic variables included age and body mass index (BMI), categorized according to WHO Asia-Pacific criteria (<18.5: underweight; 18.5–22.9: normal; 23.0–24.9: overweight; ≥25.0: obese).
Clinical characteristics included smoking status (defined as ≥1 cigarette per day for >6 months), breastfeeding history, oral contraceptive use, history of breast trauma, hyperprolactinemia (serum prolactin >25 μg/L), and nipple inversion (defined as nipple level below the areolar plane at rest). Disease-related features included the disease phase at diagnosis (inflammatory mass, abscess, or chronic sinus tract) and the maximum lesion diameter on ultrasound (<1 cm, 1–2 cm, 2–3 cm, 3–4 cm, or >4 cm). For patients who underwent targeted duct excision, incision length, operative duration, and intraoperative blood loss were recorded.
Treatment duration was defined as the interval from the first PDM-related clinic visit to complete resolution of all clinical symptoms (eg, erythema, pain, discharge, sinus tract) confirmed by both clinical assessment and breast ultrasound, and was categorized as <1, 1–2, 2–3, 3–4, or >4 months. Follow-up began after completion of initial treatment and was conducted via outpatient visits, breast imaging (ultrasound or MRI), and telephone interviews. The primary endpoint was disease recurrence, defined as reappearance of a clinically significant inflammatory mass, abscess, or sinus tract in the same breast quadrant or anatomical location after confirmed resolution of initial disease. Follow-up was censored on June 30, 2025. Recurrence-free survival time (in days) was calculated from treatment completion to first recurrence; patients without recurrence were censored at their last documented follow-up. Given the benign nature of PDM, death was not considered an endpoint.
Breast cosmetic outcome was assessed at 3 months postoperatively for surgical patients and classified as satisfactory or unsatisfactory. Satisfactory appearance required an inconspicuous periareolar scar (2–3 cm) well blended into the areolar border, with no contour deformity, nipple displacement, or parenchymal indentation. Unsatisfactory outcomes included visible or hypertrophic scarring, or structural distortion (eg, indentation, malposition). In non-surgical patients, cosmetic outcome was deemed unsatisfactory if chronic inflammation resulted in tissue destruction (eg, persistent sinus, parenchymal loss, or deformity). Assessments were based on clinical notes, independently reviewed by two investigators blinded to recurrence status; discrepancies were resolved by a third reviewer.
Statistical Analysis
Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA) and R software version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Categorical variables are presented as frequencies (percentages) and were compared between the two groups using the chi-square (χ2) test or Fisher’s exact test, as appropriate. Continuous variables are expressed as mean ± standard error of the mean (SEM) if normally distributed, or as median (interquartile range, IQR) if non-normally distributed. Group comparisons for continuous variables were conducted using the independent-samples t test for normally distributed data and the Mann–Whitney U test for non-normally distributed data.
Univariate Cox proportional hazards regression models were used to calculate hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for potential predictors of recurrence. Variables with a p-value < 0.05 in univariate analysis were entered into a multivariate Cox regression model, and independent prognostic factors were selected using backward stepwise elimination (likelihood ratio method). Model performance was evaluated based on the Wald test for individual coefficients, the concordance index (C-index), and information criteria (Akaike Information Criterion [AIC] and Bayesian Information Criterion [BIC]).
Recurrence-free survival curves were estimated using the Kaplan–Meier method and compared between groups with the log-rank test.
All statistical tests were two-sided, and a p < 0.05 was considered statistically significant.
Result
Baseline Characteristics of the Study Cohort
A total of 150 patients diagnosed with PDM were included in this analysis. The median follow-up duration for the entire cohort was 184.5 days (IQR: 97.0–384.5 days) with a follow-up range of 33 to 974 days. Most patients were aged between 31 and 40 years (44.0%), followed by those aged 18–30 years (32.7%); only 2.0% were older than 50 years. Most patients had a normal body mass index (BMI 18.5–23.9 kg/m2, 55.3%), while 25.3% were overweight (BMI 24.0–27.9 kg/m2) and 11.3% were obese (BMI ≥28 kg/m2). Smoking was reported in 16.0% of the cohort. Nipple retraction was present in 28.7% of cases, and 58.0% reported a history of lactation. Hyperprolactinemia was rare (5.3%), and 28.7% of patients reported contraceptive use. A history of breast trauma was noted in 19.3% of individuals.
At initial presentation, 64.7% of patients were in the abscess stage, 20.0% in the mass stage, and 15.3% in the sinus stage. Lesion diameter ranged from <1 cm to >4 cm, with the largest proportion (33.3%) measuring 2–3 cm.
Treatment duration varied: 23.3% of patients required more than 4 months of therapy, while 12.0% completed treatment within 1 month. Baseline characteristics of the entire cohort are summarized in Table 1.
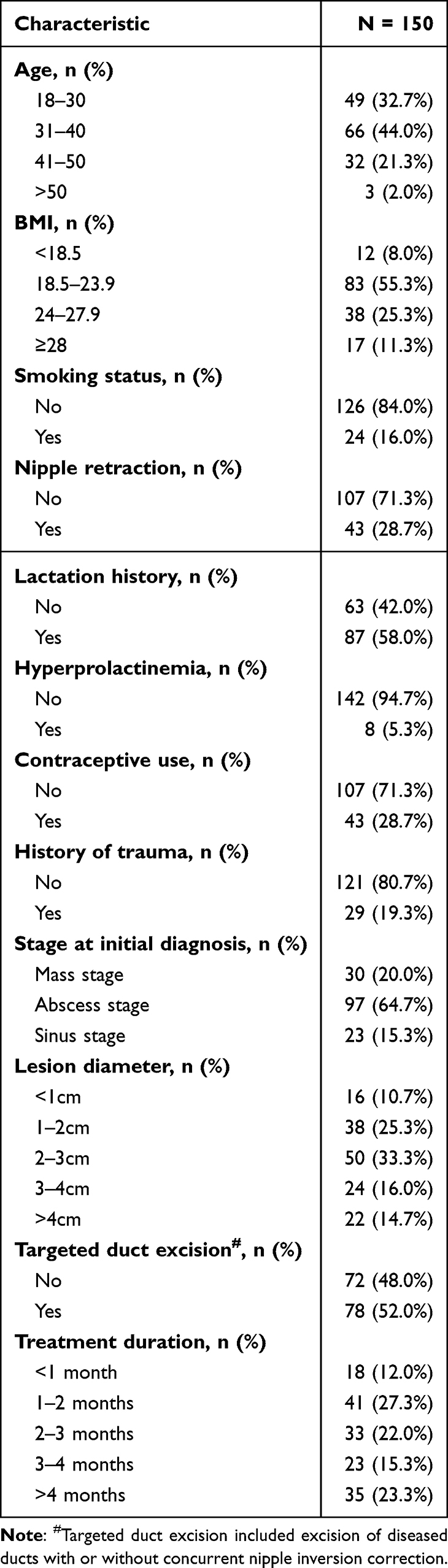 |
Table 1 Patient Demographics and Baseline Characteristics |
Univariate and Multivariate Analyses of Recurrence Risk
Univariate Cox regression showed that age >50 years (HR = 3.57, 95% CI: 1.03–12.35, p = 0.044), sinus-stage disease (HR = 2.44, 95% CI: 1.03–5.75, p = 0.042), and nipple retraction (HR = 0.20, 95% CI: 0.08–0.49, p < 0.001) were significantly associated with recurrence. Targeted duct excision was strongly protective (HR = 0.08, 95% CI: 0.03–0.17, p < 0.001).
In multivariate analysis, only targeted duct excision remained an independent predictor of reduced recurrence risk (adjusted HR = 0.09, 95% CI: 0.04–0.20, p < 0.001). All other factors—including age, disease stage, and nipple retraction—were no longer significant (p > 0.05). The model demonstrated good discrimination (c-index = 0.798) and fit (AIC = 487, BIC = 502). Detailed results are presented in Table 2.
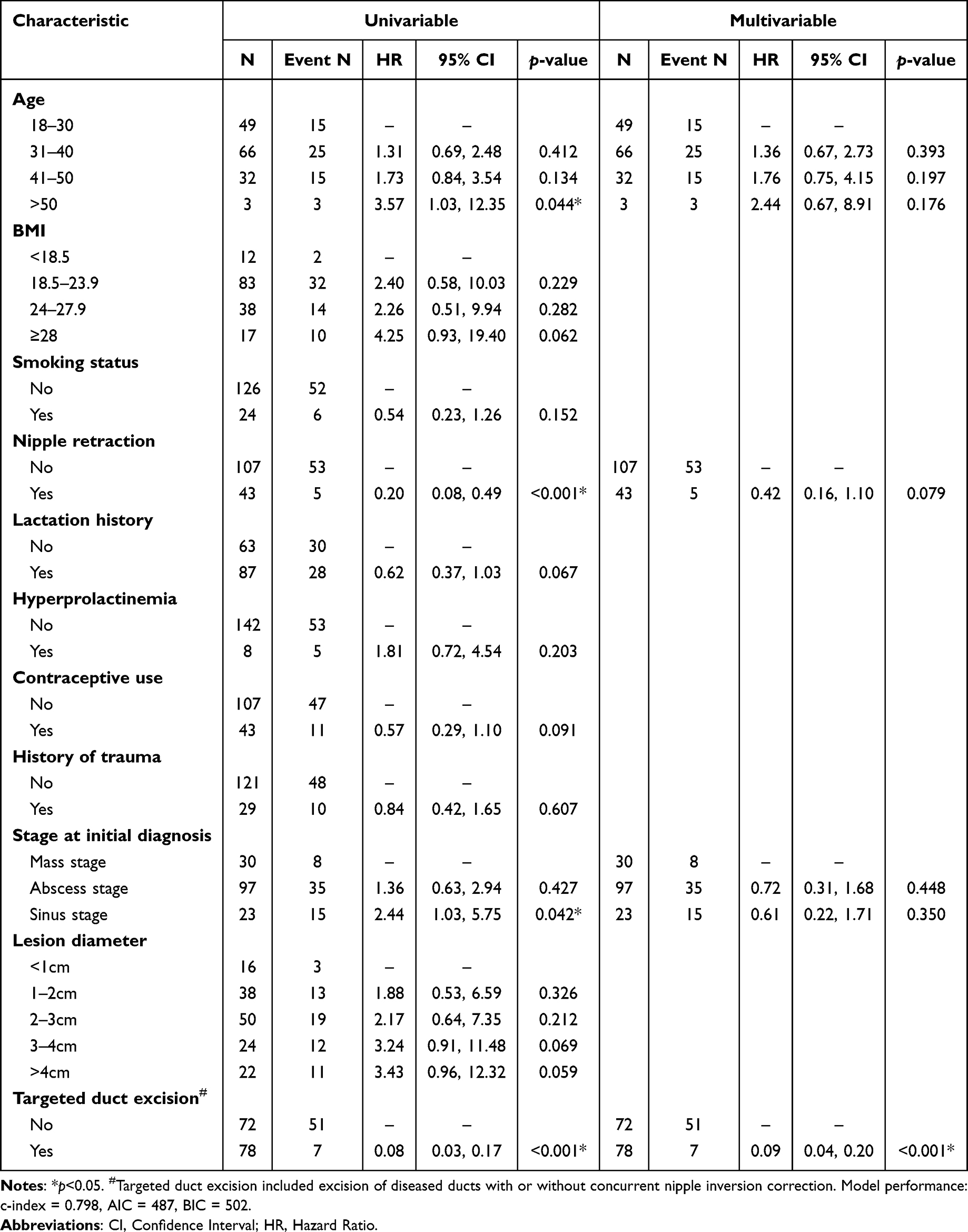 |
Table 2 Univariate and Multivariate Analysis of Influencing Factors (Cox Regression) |
Impact of Targeted Duct Excision on Clinical Outcomes
Patients were stratified into a targeted duct excision group (n = 78) and a non-excision group (n = 72). As summarized in Table 3, the two groups differed significantly in the prevalence of nipple retraction (p < 0.001) and history of breast trauma (p = 0.036), while all other baseline characteristics were comparable. In the duct excision group, mean incision length was 2.87 ± 0.64 cm, operative time 59 ± 12 minutes, and intraoperative blood loss 20 ± 8 ml. Satisfactory cosmesis was achieved in 69/78 (88.5%) excision group versus 45/72 (62.5%) in the non- excision group (p < 0.001).
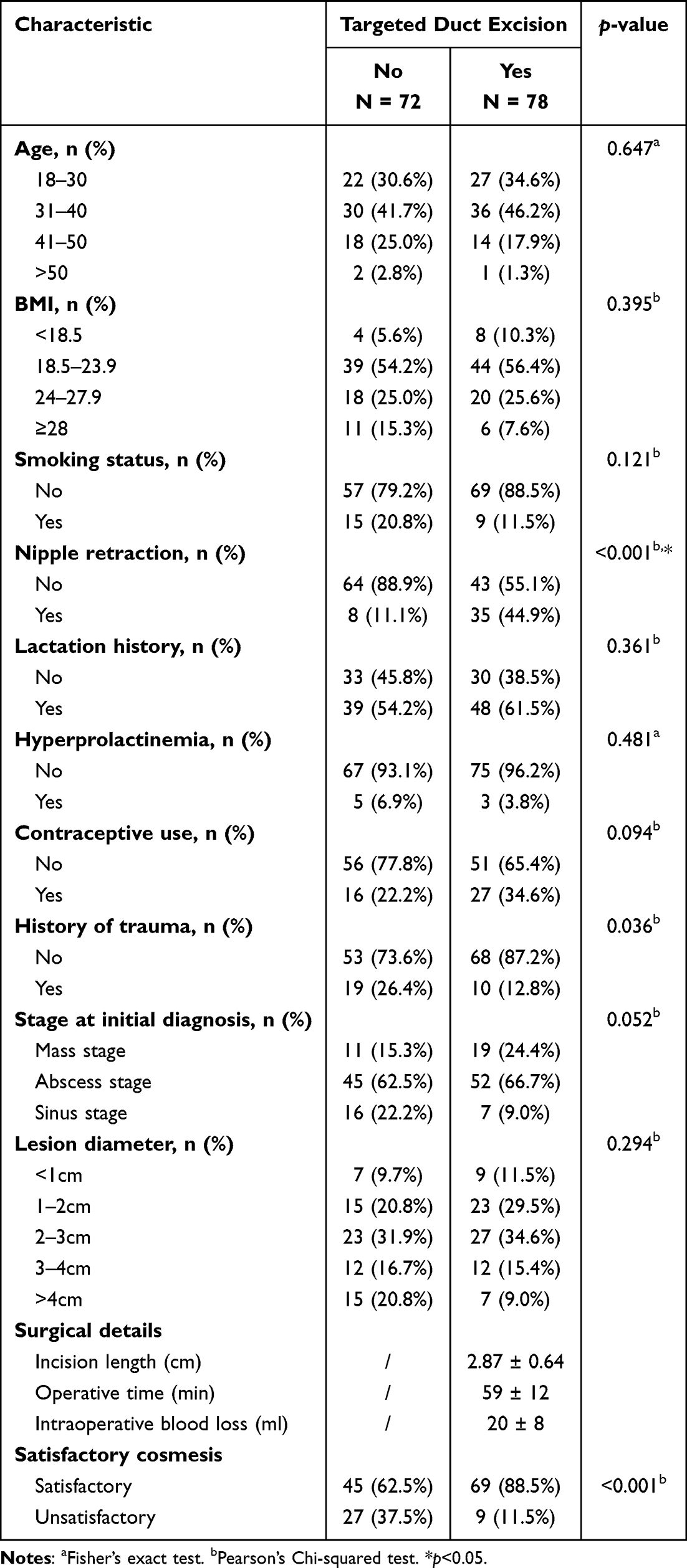 |
Table 3 Comparison of Treatment Characteristics and Clinical Outcomes Between the Targeted Duct Excision Group and the Non-Excision Group |
Patients who underwent targeted duct excision had a significantly lower risk of recurrence compared to those managed without excision. Kaplan–Meier analysis revealed a markedly prolonged recurrence-free survival in the excision group (log-rank p < 0.001) (Figure 1A). Consistently, the overall recurrence rate was dramatically lower in the excision group (9.0%, 7/78) than in the non-excision group (70.8%, 51/72) (Figure 1B). Moreover, the median duration of initial treatment was significantly shorter in the excision group than in the non-excision group (52 [29–73] days vs 110.5 [81–145] days; p < 0.001) (Figure 1C). Among the 58 patients who experienced recurrence, the time from completion of initial treatment to recurrence was significantly longer in the excision group (136 [108–159] vs 75 [54–96], p < 0.001) (Figure 1D). This benefit persisted across all initial disease stages: at the mass, abscess, and sinus stages, the number of patients remaining recurrence-free was consistently higher in the targeted duct excision group (Figure 1E).
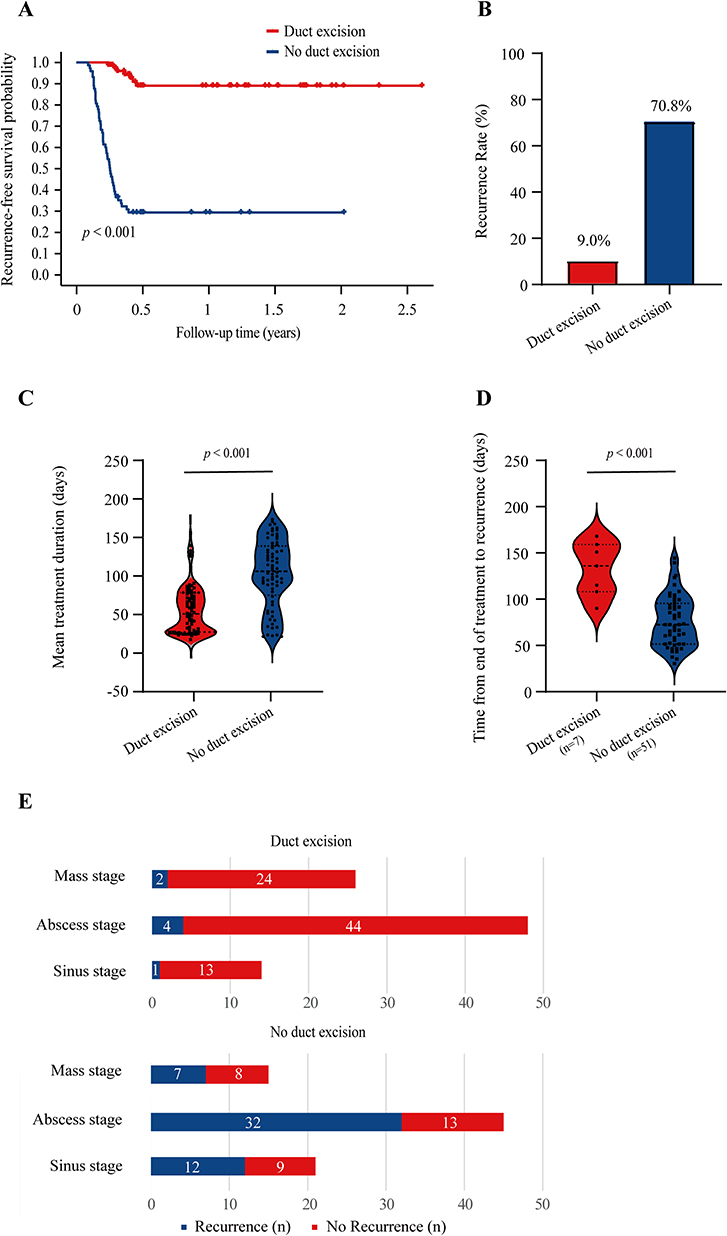 |
Figure 1 Comparison of clinical outcomes in patients with PDM with versus without targeted duct excision. (A) Kaplan–Meier recurrence-free survival curves stratified by duct excision status (log-rank test). (B) Recurrence rates (%) in the duct excision and no duct excision groups. (C) Distribution of initial treatment duration (days) in the duct excision group (n = 7) and non-excision group (n = 51). Violin plots show kernel density estimates with embedded boxplots indicating median and interquartile range, and individual data points overlaid (Mann–Whitney U test). (D) Distribution of time from end of initial treatment to recurrence in relapsed patients, comparing the duct excision group and the no duct excision group, shown as violin plots with embedded boxplots and individual data points (Mann–Whitney U test). (E) Number of patients with and without recurrence, stratified by initial clinical stage at diagnosis (mass phase, abscess phase, sinus phase), in each group. |
Discussion
This retrospective cohort study of 150 patients with periductal mastitis (PDM) found that targeted duct excision was strongly associated with improved clinical outcomes. The recurrence rate was markedly lower in the excision group (9.0%) compared to the non-excision group (70.8%). Patients undergoing targeted duct excision also experienced significantly prolonged recurrence-free survival and a shorter median treatment duration (52 days [IQR: 29–73] vs 110.5 days [IQR: 81–145]). Notably, after adjusting for potential confounders—including disease phase at diagnosis and age—multivariable Cox regression analysis identified targeted duct excision as an independent protective factor against recurrence (adjusted hazard ratio [aHR] = 0.09; 95% CI: 0.04–0.20; p < 0.001). These findings provide robust evidence supporting targeted duct excision as a preferred definitive treatment strategy for PDM.
Traditionally, PDM has been managed conservatively with antibiotics, abscess drainage, or immunosuppressive agents; however, recurrence rates remain high—approximately 50%—leading to repeated clinical visits, diminished quality of life, and increased healthcare burden.3,4 Our study demonstrates that surgical intervention reduces the risk of recurrence by 91%, a finding highly consistent with the underlying pathophysiology of PDM: the disease originates from obstruction or dilation of the subareolar collecting ducts, creating a persistent nidus of chronic inflammation and infection.11 Targeted excision of the affected duct system directly eliminates this source of ongoing irritation at its origin. Although extensive duct excision combined with oncoplastic techniques—such as dermoglandular flap transposition—has been used by some investigators for complex sinus tracts and has shown certain efficacy,12–14 these procedures are associated with significant surgical trauma, substantial tissue loss, and considerable adverse impact on breast cosmesis.15
In contrast to extensive resection techniques, the targeted duct excision strategy adopted in this study offers a favorable balance between disease control and breast preservation. By integrating preoperative ultrasound and MRI for precise mapping of abnormal ductal anatomy, and utilizing a small periareolar incision (mean 2.87 cm) to remove the affected duct and its major branches, this approach effectively eliminates the inflammatory nidus while simultaneously correcting nipple retraction secondary to periductal fibrosis.
Importantly, the limited tissue excision and concealed scar placement translate into superior cosmetic outcomes: 88.5% of patients reported satisfactory breast appearance, significantly higher than the 62.5% in the non-excision group (p < 0.001). Given that PDM primarily affects young women of reproductive age—many of whom are highly concerned about body image—this minimally invasive, cosmesis-conscious technique may substantially reduce the psychological distress often associated with more aggressive surgical approaches. Moreover, by aligning effective source control with aesthetic expectations, it likely enhances patient willingness to undergo definitive treatment and improves long-term adherence.
Notably, for patients who desire future pregnancy and breastfeeding, even limited duct excision may disrupt a portion of the lactiferous ductal system and potentially impair lactation capacity. Therefore, clinical decision-making should be grounded in thorough informed discussion, with careful consideration of the patient’s individual preferences, reproductive plans, and personal values.
Furthermore, this study helps clarify a clinical controversy. For example, nipple retraction was associated with a higher recurrence risk in univariate analysis, but lost statistical significance in the multivariable model, suggesting that its link to poor prognosis may not be causal. Notably, nipple retraction was significantly more prevalent in the excision group (p < 0.001), reflecting real-world clinical practice—surgeons are more likely to perform surgery in patients with nipple retraction because the procedure allows simultaneous correction of the deformity. In univariate analysis, nipple retraction appeared to have a “protective effect” (HR = 0.20); however, this association disappeared in the multivariable model, indicating that it is not an independent protective factor but rather a classic example of confounding bias. In other words, it is the surgical intervention itself—not the phenotype of nipple retraction—that reduces recurrence risk. This also explains the observation by Xu et al that “nipple inversion correction reduces PDM recurrence”: the underlying mechanism is effective excision of the diseased ducts.16
Finally, in patients with established abscesses or chronic sinus tracts, residual necrotic tissue and granulation tissue often lead to prolonged wound healing and extended dressing changes. Performing targeted duct excision at this stage not only allows concomitant removal of inflammatory and necrotic debris but also promotes wound healing and significantly shortens the overall treatment duration—shifting management from symptomatic control toward definitive source control by addressing the underlying pathological ductal lesion.
This study has several limitations. First, as a single-center retrospective analysis, it may be subject to selection bias due to the exclusion of patients who discontinued treatment or transferred to other institutions during follow-up. Second, although we adjusted for several disease-related confounders in the multivariable Cox regression model, residual confounding from unmeasured factors—such as socioeconomic status, treatment adherence, or psychosocial variables—cannot be ruled out.
Conclusion
In summary, targeted duct excision was identified as the sole independent protective factor against recurrence in our multivariable analysis. It significantly reduces recurrence risk and shortens treatment duration while preserving favorable breast cosmesis. These findings support considering targeted duct excision as a primary therapeutic strategy for patients with periductal mastitis.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Pin Wang, upon reasonable request. Due to privacy and ethical restrictions related to patient confidentiality, the raw data are not publicly archived. However, de-identified datasets used for the statistical analyses presented in this manuscript may be shared with qualified researchers for purposes of reproducing or verifying the results, subject to institutional review board approval and a signed data use agreement.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Medical Research Project of the Health Commission of Chengdu City (No. 2025051), the Sichuan Province Medical Youth Innovation Research Project Plan (No. Q23009), and the Technology Innovation and Development Project of Chengdu Science and Technology Project (No. 2024-YF05-02017-SN).
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Jiao Y, Chang K, Jiang Y, Zhang J. Identification of periductal mastitis and granulomatous lobular mastitis: a literature review. Ann Transl Med. 2023;11(3):158. doi:10.21037/atm-22-6473
2. Dalci K, Gumus S, Saritas AG, et al. Modified techniques versus Hadfield’s procedure in patients with periductal mastitis. BMC Surg. 2022;22(1):40. doi:10.1186/s12893-022-01496-0
3. Li S, Grant CS, Degnim A, Donohue J. Surgical management of recurrent subareolar breast abscesses: mayo Clinic experience. Am J Surg. 2006;192(4):528–11. doi:10.1016/j.amjsurg.2006.06.010
4. Xing M, Zhang S, Zha X, Zhang J. Current understanding and management of plasma cell mastitis: can we benefit from what we know? Breast Care. 2022;17(3):321–329. doi:10.1159/000517572
5. Ramalingam K, Vuthaluru S, Srivastava A, Dinda AK, Dhar A. Ultra structural changes occurring in duct ectasia and periductal mastitis and their significance in etiopathogenesis. PLoS One. 2017;12(3):e0173216. doi:10.1371/journal.pone.0173216
6. Zhou F, Liu L, Wang F, et al. Periductal mastitis, a disease with distinct clinicopathological features from granulomatous lobular mastitis. J Inflamm Res. 2024;17:3815–3823. doi:10.2147/JIR.S464585
7. Liu L, Zhou F, Wang P, et al. Periductal mastitis: an inflammatory disease related to bacterial infection and consequent immune responses? Mediators Inflamm. 2017;2017:5309081. doi:10.1155/2017/5309081
8. Zhou F, Shang XC, Tian XS, Yu ZG; Chinese Society of Breast S. Clinical practice guidelines for diagnosis and treatment of patients with non-puerperal mastitis: chinese Society of Breast Surgery (CSBrS) practice guideline 2021. Chin Med J. 2021;134(15):1765–1767. doi:10.1097/CM9.0000000000001532
9. Ortiz-Mendoza CM, Sanchez NAA, Dircio AC. Fine-needle aspiration cytology to identify a rare mimicker of breast cancer: plasma cell mastitis. Rev Bras Ginecol Obstet. 2018;40(8):491–493. doi:10.1055/s-0038-1666809
10. Ramalingam K, Srivastava A, Vuthaluru S, Dhar A, Chaudhry R. Duct ectasia and periductal mastitis in Indian women. Indian J Surg. 2015;77(Suppl 3):957–962. doi:10.1007/s12262-014-1079-5
11. Sargent RE, Sener SF. Benign breast disease: periareolar mastitis, granulomatous lobular mastitis, and lymphocytic or diabetic mastopathy. Surg Clin North Am. 2022;102(6):1007–1016. doi:10.1016/j.suc.2022.06.004
12. Zhang Y, Zhou Y, Mao F, Guan J, Sun Q. Clinical characteristics, classification and surgical treatment of periductal mastitis. J Thorac Dis. 2018;10(4):2420–2427. doi:10.21037/jtd.2018.04.22
13. Taffurelli M, Pellegrini A, Santini D, Zanotti S, Di Simone D, Serra M. Recurrent periductal mastitis: surgical treatment. Surgery. 2016;160(6):1689–1692. doi:10.1016/j.surg.2016.06.048
14. Beechey-Newman N, Kothari A, Kulkarni D, Hamed H, Fentiman IS. Treatment of mammary duct fistula by fistulectomy and saucerization. World J Surg. 2006;30:63–68. doi:10.1007/s00268-005-0116-8
15. Xu H, Liu R, Lv Y, et al. Treatments for periductal mastitis: systematic review and meta-analysis. Breast Care. 2022;17(1):55–62. doi:10.1159/000514419
16. Xu Y, Da B, Zhao F, et al. Corrective surgery for nipple depression in patients with plasmacytic mastitis - A single-center experience. Front Med. 2023;10:1156628. doi:10.3389/fmed.2023.1156628
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.