Back to Journals » Risk Management and Healthcare Policy » Volume 14
Tapentadol and Oxycodone/Naloxone Prescribing Patterns in Primary Health Care in Catalonia, Spain: A Cross-Sectional Study
Authors Viñas-Bastart M, Oms-Arias M, Pedraza-Gutiérrez À, Lizano-Díez I ![]() , Mariño EL
, Mariño EL ![]() , Modamio P
, Modamio P ![]()
Received 19 March 2021
Accepted for publication 13 September 2021
Published 4 October 2021 Volume 2021:14 Pages 4155—4168
DOI https://doi.org/10.2147/RMHP.S301724
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Montserrat Viñas-Bastart,1 Míriam Oms-Arias,2 Àfrica Pedraza-Gutiérrez,2 Irene Lizano-Díez,1 Eduardo L Mariño,1 Pilar Modamio1
1Clinical Pharmacy and Pharmaceutical Care Unit, Department of Pharmacy and Pharmaceutical Technology, and Physical Chemistry, Faculty of Pharmacy and Food Sciences, University of Barcelona, Barcelona, Spain; 2Costa de Ponent Primary Care Directorate, Catalan Institute of Health, L’Hospitalet de Llobregat, Barcelona, Spain
Correspondence: Pilar Modamio
Clinical Pharmacy and Pharmaceutical Care Unit, Department of Pharmacy and Pharmaceutical Technology, and Physical Chemistry, Faculty of Pharmacy and Food Sciences, University of Barcelona, Av. Joan XXIII, 27-31, Barcelona, 08028, Spain
Tel/ Fax +34 934024544
Email [email protected]
Objective: To characterize the use of tapentadol and the combination oxycodone/naloxone in primary health care. Data on their use and possible misuse will allow the identification of risk factors and to design protocols to reduce and prevent avoidable harm to patients being treated for pain.
Design: A descriptive, cross-sectional and multicenter study was performed.
Setting: Fifty-three primary health care teams, which provides healthcare for 1,300,000 inhabitants.
Patients: A total of 1840 patients had active prescriptions of tapentadol and 985 of oxycodone/naloxone.
Methods: Demographic (age, sex) and clinical (glomerular filtration rate; active liver disease; dosing and duration of treatment), prescribed daily dose (according to age, sex, length of treatment), concomitant analgesic treatment and diagnosis. Patient information was obtained from medical records.
Results: Most of the patients were women (> 74.0% in both cases), and the average age was 69.3 years (women: 70.1± 13.2; men: 66.7± 13.9 years) in the case of tapentadol and 70.6 years (women: 64.0± 13.6; men: 72.6± 14.3 years) in the case of oxycodone/naloxone. Only 12.2% of patients taking tapentadol and 12.1% taking oxycodone/naloxone had a normal renal function. In both cases, 4.1% of patients had active liver disease. The average length of treatment was 246.4 days in oxycodone/naloxone and 199.0 days in tapentadol. It was recorded that 85.1% of patients in the case of tapentadol and 89.0% in the oxycodone/naloxone had at least another drug prescribed for pain. About 42.2% of patients treated with tapentadol and 34.4% of patients treated with oxycodone/naloxone had associated neuralgia as a diagnosis.
Conclusion: The pattern of use and profile of patients with tapentadol and oxycodone/naloxone had more similarities than differences, and suggested that prescribing practice, and monitoring should be assessed regularly to ensure patient safety and effective management of pain.
Keywords: clinical practice pattern, chronic pain, opioids, oxycodone/naloxone, primary health care, culture, tapentadol
Introduction
Although there is no uniformity in terms of its definition, chronic pain is generally understood as the one that persists beyond 3 or 6 months from its appearance or beyond the expected healing period for a given lesion.1 Chronic pain is one of the most frequent causes why general population looks for medical treatment, and is often poorly managed.2,3 Approximately 20% of United States adults have chronic pain4 and it also affects 20% of European citizens.5 Spain shows a prevalence of chronic pain in the adult population (≥18 years) of 16.6%.6
Chronic opioid therapy has limited data supporting its long-term effectiveness more than three months for the management of chronic non-malignant pain7 and the use in the long term remains controversial, also because of the adverse events.8 Besides, it must be taken into account that chronic pain is often accompanied by mood and sleep disorders, and other chronic conditions that can result in complex medication regimens and an increased risk of drug interactions and side effects.7
Regarding opioids’ side effects, the most habitual encompass dry mouth, vomiting, nausea, fatigue, increased sweating, itching, drowsiness and constipation, with a remarkable negative impact on patient quality of life.8,9 Tapentadol demonstrated to have fewer side effects at the central nervous system (CNS), which could reduce dependence10,11 and fewer gastrointestinal side effects than morphine and oxycodone.12 In this regard, the combination of naloxone with oxycodone improves opioid-induced bowel dysfunction, characterized by constipation, incomplete evacuation, bloating, and increased gastric reflux, which helps increase the acceptability of opioid treatment for pain.13,14
In Spain, tapentadol is still covered by patent law and dosage forms are only marketed as trademarks, both the extended-release tablets (dosages of 25, 50, 100, 150, 200 and 250 mg) and the immediate-release tablets (dosages of 50, 75 and 100 mg).15 Oxycodone/naloxone combination is marketed as trademarks and generics of extended-release tablets in different dosages (5/2.5 mg, 10/5 mg, 20/10 mg and 40/20 mg).16 An increase in the consumption of tapentadol and oxycodone/naloxone expressed in defined daily doses per 1000 inhabitants per day (DHD) over the years 2014 to 2017 (1.3% DHD tapentadol and 1.4% DHD oxycodone/naloxone to 2.3% DHD and 1.9% DHD, respectively) was found in our study area of primary health care. Despite the increasing influence of general practitioners on the opioid analgesics’ prescription for the chronic pain treatment, to our knowledge, there were no findings in the literature of descriptive studies and comparative analysis of the use of these drugs in primary care practice.8 Thus, the aim of the present study was to characterize the use of tapentadol and the combination oxycodone/naloxone in primary health care. Data on their use and possible misuse will allow the identification of risk factors and to design protocols to reduce and prevent avoidable harm to patients being treated for pain.
Materials and Methods
Design and Setting of the Study
A descriptive and cross-sectional multicenter study was carried out. It covered fifty-three primary health care teams in the Primary Care Directorate (DAP) Costa de Ponent of the Catalan Institute of Health (ICS), which provides healthcare for 1.3 million inhabitants.17,18
Data Source, Collection, and Variables
The target population were patients with an active prescription of tapentadol or the oxycodone/naloxone combination on August 13, 2018. The Summary of Product Characteristics (SmPC) of all (brand-named and generic) marketed prescription medicines containing these drugs were reviewed to evaluate their authorized therapeutic use. The information of the patients was obtained and extracted anonymously.
The variables studied about patient data were age, sex, glomerular filtration rate (GFR: >90 mL/min, 60–89 mL/min, 45–59 mL/min, 30–44 mL/min, 15–29 mL/min and data not registered) and active liver disease. As for the prescription data: duration of treatment (>30 days, 31–90 days, 91–180 days, 181–366 days, 1–2 years, and more than 2 years), prescribed daily dose according to age (in case of oxycodone/naloxone doses are only referred to as oxycodone since the dose of naloxone is always half of oxycodone), sex and length of treatment, concomitant analgesic treatment and diagnosis. Patient data was obtained from clinical records (e-CAP computer program), whereas diagnoses were defined according to the International Classification of Diseases (ICD-10). The computer program used (e-CAP) contains patients’ demographic data, clinical history, diseases, drugs, treatment plans, vaccinations, allergies, radiology images, analytical and test results, therapeutic procedures, hospital discharge dates, and visits to hospital emergency.17
Regarding the ICS, it is the main provider of public health services in Catalonia, Spain. It is a leading provider in its three basic areas of activity: healthcare (its main area), research and teaching. The ICS provides health services to 83% of all Catalan citizens (over 5.5 million people).18 It is comprised of 8 hospitals and 287 primary care teams, located throughout the entire Catalan territory. The primary care teams are made up of a varying number of professionals (general practitioners, pediatricians, nurses, auxiliary nurses, dental surgeons, social workers, and administrative staff) and are responsible for providing free primary healthcare to the population that lives within their catchment area. The management structures or DAPs are directly responsible for all the health centers, services, and institutions within their corresponding area. Concretely, DAP Costa de Ponent directly manages primary health care services in the southern Barcelona Metropolitan Area (Catalonia, Spain).18
Ethical Review Board Approval
Given that the extraction of information was carried out anonymously and the relationship was not available to recover which real cases the information corresponds to, it was not necessary to ask for the informed consent of the patients studied or institutional review board approval, in accordance with Spanish regulations prior to January 2, 2021 (Order SAS/3470/2009, of December 16, which publishes the guidelines on post-authorization studies of an observational type for medicines for human use and Chapter VI of Royal Decree 577/2013, of July 26, which regulates pharmacovigilance of medicinal products for human use).
Data Analysis
Discrete variables were expressed in proportions or frequencies, and continuous variables as means and standard deviations, and it was assumed that the data were normally distributed. Frequencies were compared in a bivariate analysis using χ square and means using Student’s t test or analysis of variance. As a post hoc test was used Bonferroni. Pearson’s correlation was used in the relationship of two quantitative variables. A p-value ≤ 0.05 was considered statistically significant. The data were analyzed using SPSS software, version 17.0.
Results
Description of the Population
At the time of the study (13 August 2018), 1840 patients had active prescription of tapentadol and 985 patients of the combination oxycodone/naloxone. In the case of tapentadol, all patients were prescribed extended-release tablets and 0.3% (N = 6) of them had also oxycodone/naloxone at the same time. As for oxycodone/naloxone, 0.6% (N = 6) of patients had also tapentadol at the same time.
The 74.8% (N = 1377) of patients with active prescription of tapentadol extended release and 74.1% (N = 729) of patients in the case of oxycodone/naloxone were women. No statistical differences were found in terms of sex between patients taking tapentadol and those taking oxycodone/naloxone. Regarding patients’ age, the average was 69.3 years (women: 70.1±13.2 years, male: 66.7±13.9 years) in the case of tapentadol and 70.6 years (women: 64.0±13.6 years; male: 72.6±14.3 years) in oxycodone/naloxone. The age of women who took tapentadol was slightly higher but statistically significant than those who took oxycodone. The distribution of patients by age is shown in Figure 1A.
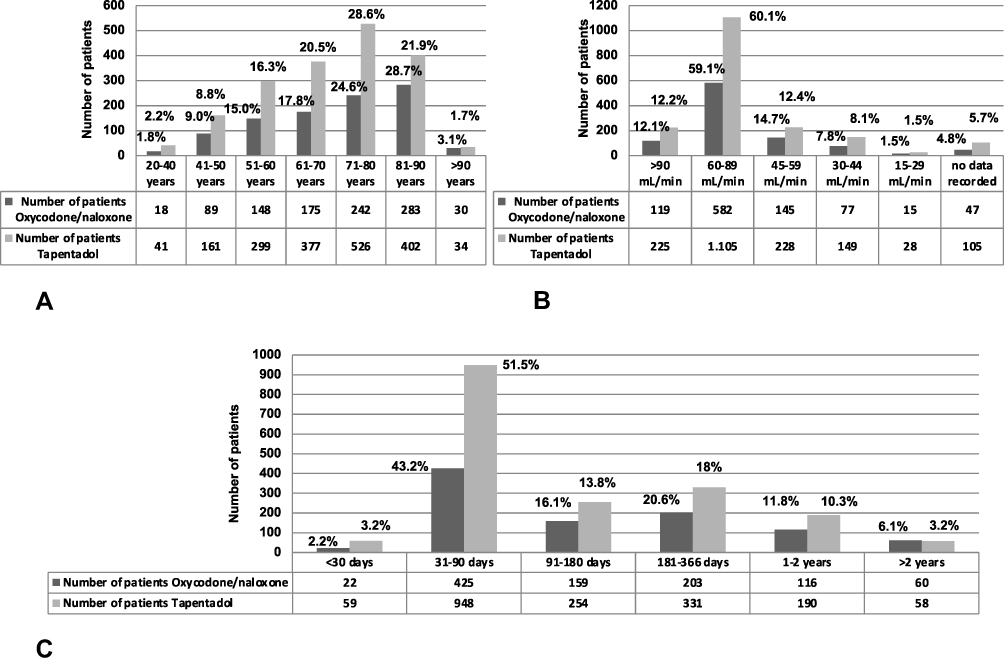 |
Figure 1 Distribution of patients by age (A), by Glomerular Filtration Rate (B), and by duration of treatment (C) with tapentadol vs oxycodone/naloxone. |
Renal and Hepatic Function
As for the renal function, in the case of tapentadol, 12.2% of patients (N = 225) had a normal renal function (GFR> 90 mL/min) and in the case of oxycodone/naloxone, 12.1% (N = 119). Figure 1B shows the distribution of patients depending on the GFR value registered to determine the stage of kidney disease. In addition, it was found that around 5% of patients (5.6%, N = 104 in case of tapentadol and 4.8%, N= 47 in case of oxycodone/naloxone) had no data recorded for their renal function.
Regarding liver function, 4.1% of patients with tapentadol (N=75) had active liver disease. Liver disease includes hepatitis C virus, hepatitis B virus, alcoholic and non-alcoholic fatty liver disease, autoimmune hepatitis, cholestasis/diseases of the biliary tract, hepatotoxicity for medicines or herbal supplements, and hepatotoxicity leading to cirrhosis. In the case of oxycodone/naloxone, 4.1% of patients (N = 40) had active liver disease.
There was no found co-prescription of the two drugs in patients with impaired renal or hepatic function.
Treatment Duration
The duration of treatment with extended release tapentadol and oxycodone/naloxone is ranged from less than one month to more than 2 years (Figure 1C). Oxycodone/naloxone treatments had a longer duration than tapentadol treatments (246.4±283.8 days vs.199.0±219.7 days, respectively) and this difference was statistically significant (p < 0.005).
Prescribed Daily Dose
The average daily dose prescribed to patients treated with extended-release tablets of tapentadol and patients treated with oxycodone/naloxone was, respectively, 112.3±87 mg (range: 6.1 mg - 1000 mg) and 23.5±20.6 mg of oxycodone (range: 1.2 mg −160 mg). We found, in the case of tapentadol, 146 patients (7.4%) with doses below 50 mg/day (underdosed) and above 500 mg/day (overdosed). In oxycodone/naloxone, we found 179 patients (18.2%) with doses lower than the recommended 10/5 every 12 h. The daily dose was calculated according to frequency and dosage, finding frequencies of 1 every 99 h. Figure 2A shows the average daily dose established according to age groups. In the case of tapentadol, the highest daily dose was in the age group of 41–50 years (average 123.2±109.3 mg), although there were no significant differences in the daily dose in any of the age ranges established (p = 0.065). In general, younger patients (range: 20–40 years) were taking lower doses of tapentadol, however, three of those patients were taking more than the authorized dose (500 mg according to the SmPC).
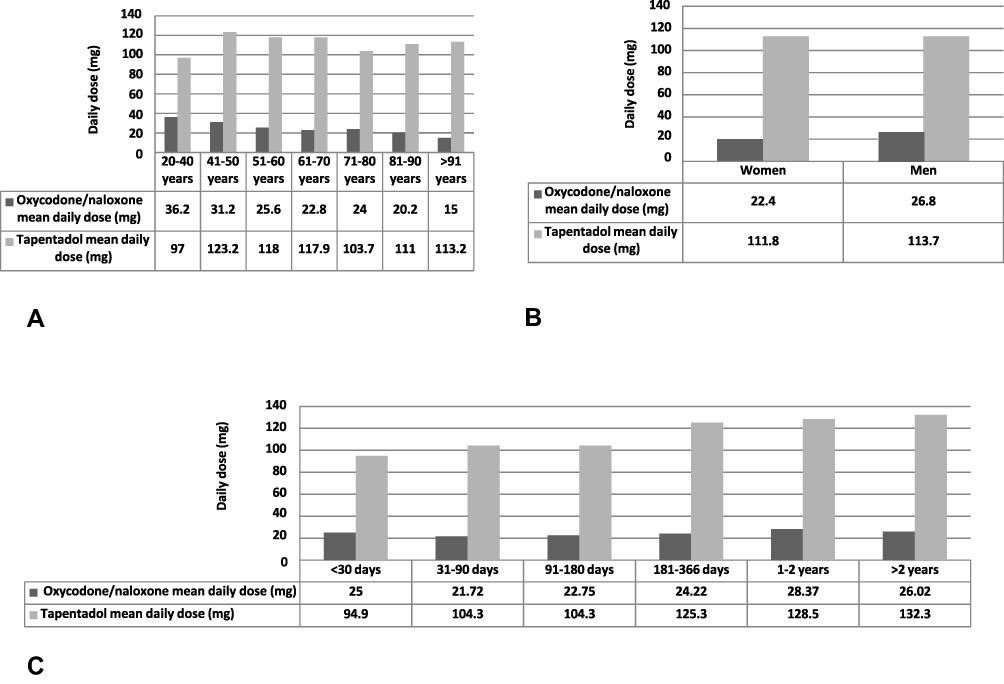 |
Figure 2 Average daily dose according to age groups (A), to sex (B), and to duration of treatment (C). |
With respect to the oxycodone/naloxone, the highest daily dose was in the age group between 20 and 40 years (average of 36.2±35.2 mg of oxycodone). The oldest patients (range: 81 - >91 years) were taking the lowest doses and no patient were taking more than the authorized dose (160 mg of oxycodone/80 mg of naloxone according to the SmPC). There were statistically significant age-related differences in the average daily dose of oxycodone (p < 0.005).
Furthermore, there appeared to be a negative significant correlation between age and average daily dose in patients taking oxycodone/naloxone (r = −0.173; p < 0.005).
On the other hand, the average daily dose used was lower in women than men in both medicines (Figure 2B). In the case of oxycodone, the dose in men (26.8±25.7 mg) was statistically significant higher (p = 0.012) than that of women (22.4±18.3 mg).
When analyzing both the average daily dose data of the drugs and the duration of treatment (Figure 2C), patients treated with the lowest daily dose of tapentadol had the shortest duration of treatment. In addition, there appeared to be a significant positive correlation between the two variables (r = 0.097; p < 0.005). In the case of oxycodone/naloxone, patients with treatment length between one and two years were the ones with the highest average daily dose. In this sense, a significant correlation between the two variables was found (r = 0.073; p = 0.022).
Drug Treatment Combination with Tapentadol and Oxycodone/Naloxone
These drugs were also prescribed along with additional pain drugs, such as, NSAIDs, antiepilectics such as pregabalin, other non-opioid analgesics such as metamizole, anxiolytics and hypnotics, selective inhibitors of serotonin reuptake inhibitors (SSRIs), antiepileptics such us gabapentin, sedatives, tricyclic antidepressants (TCAs) and other opioid analgesics. Besides, patients could be taking simultaneously more than one medication (Figure 3). Therefore, in the case of tapentadol, it was recorded that 85.1% (N = 1566) of patients had at least another drug prescribed for pain. Mainly, 56.0% (N = 1030) of patients had a concomitant acetaminophen, 21.4% (N = 393) pregabalin, 21.1% (N = 388) metamizole, 11.6% (N = 214) diazepam, 7.1% (N = 196) duloxetine and 10.5% (N = 193) gabapentin. As for oxycodone/naloxone, 89.0% of patients (N = 877) had at least another drug prescribed for pain. Predominantly, 60.1% (N = 592) of patients had concomitant acetaminophen, 23.7% (N = 233) pregabalin, 21.8% (N = 215) metamizole, 13.0% (N = 128) diazepam, 11.3% (N = 111) gabapentin and 11.2% (N = 110) duloxetine. Patients with oxycodone/naloxone treatment took more adjuvant drugs (1.9±1.2 drugs) than patients with tapentadol treatment (1.7±1.2 drugs) and this difference was statistically significant (p = 0.005).
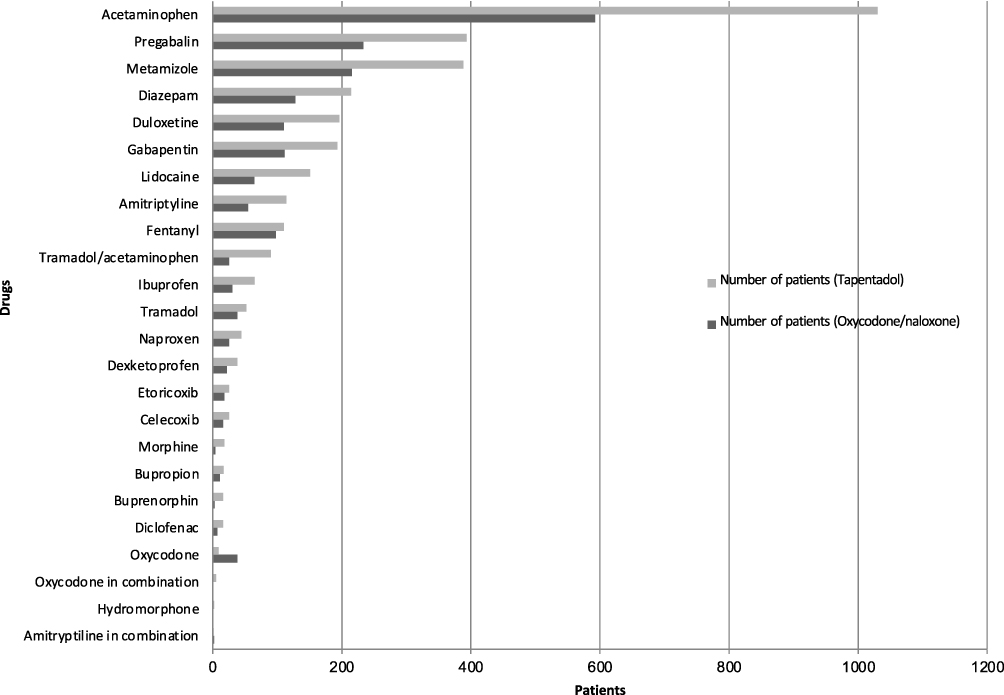 |
Figure 3 Distribution of drug treatment combination and number of patients. |
Diagnoses
The study found that 42.2% of patients treated with tapentadol (N = 776) had neuralgia as a diagnosis, 14.4% of patients (N = 265) osteoarthritis, 7.8% (N = 144) had more than one diagnosis of pain, 5.3% (N = 97) neoplasic processes, 5.3% (N = 94) fracture and osteoporosis, 4.7% (N = 86) fibromyalgia, and 4.3% (N = 76) did not have a diagnosis (Table 1). There were 0.43% of patients (N = 8) with an incorrect indication including depressive disorder (N = 4) and diabetes mellitus (N = 4).
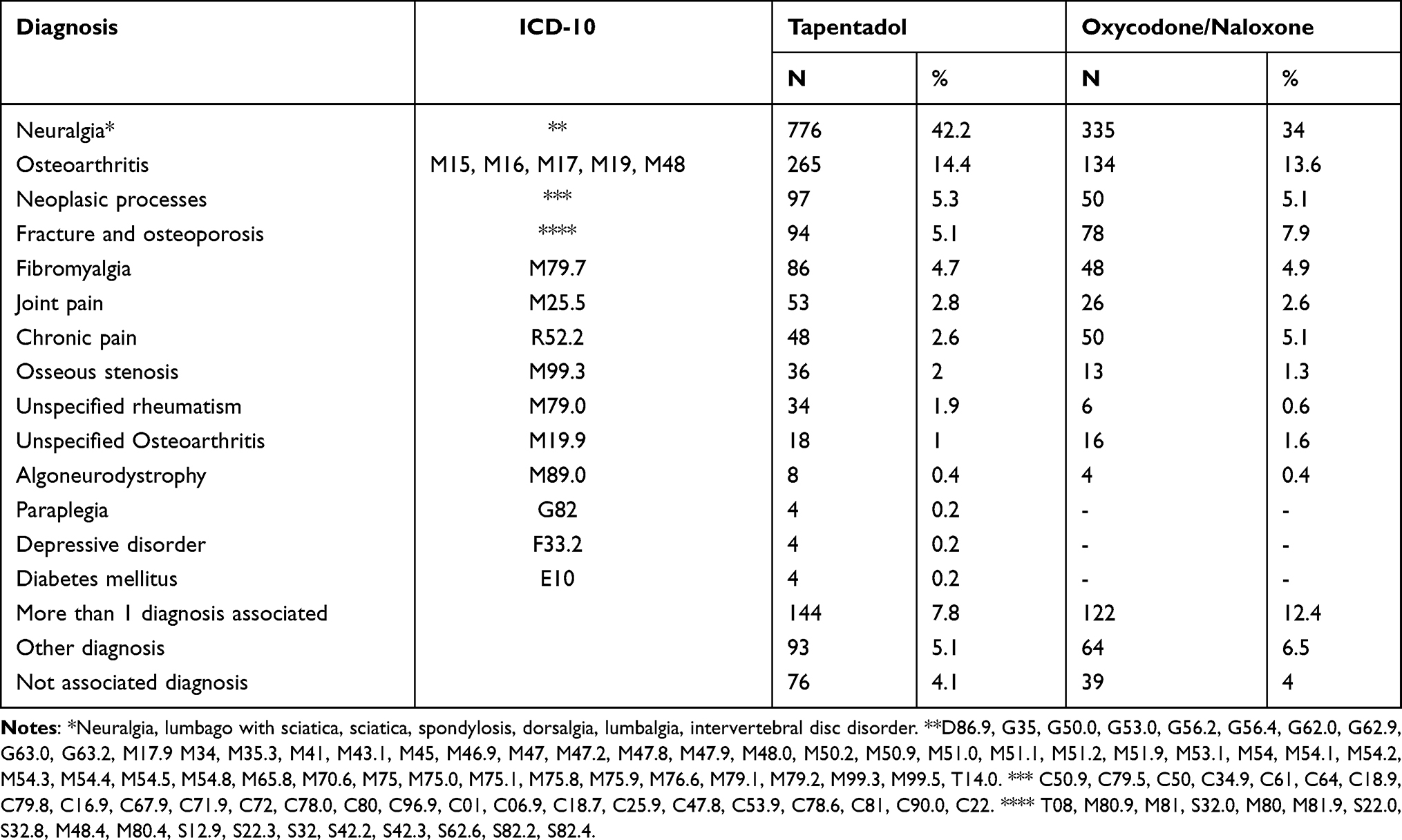 |
Table 1 Distribution of Patients Taking Tapentadol and Oxycodone/Naloxone and Their Diagnoses |
In the case of treatment with oxycodone/naloxone, 34.0% of patients (N = 335) had neuralgia as a diagnosis, lumbago with sciatica, sciatica, and spondylosis, 15.8% (N = 156) intervertebral disc disorders, 13.6% (N = 134) osteoarthritis, 12.4% (N = 122) had more than one diagnosis of pain, 7.9% (N = 78) fracture and osteoporosis, 5.1% (N = 50) neoplasic processes and (N = 50) chronic pain, 4.9% (N = 48) fibromyalgia and 4% (N = 39) did not have a diagnosis (Table 1).
On the other hand, 5.1% (N = 93) and 6.5% (N = 64) of patients had other diagnoses, respectively (Tables 1–3).
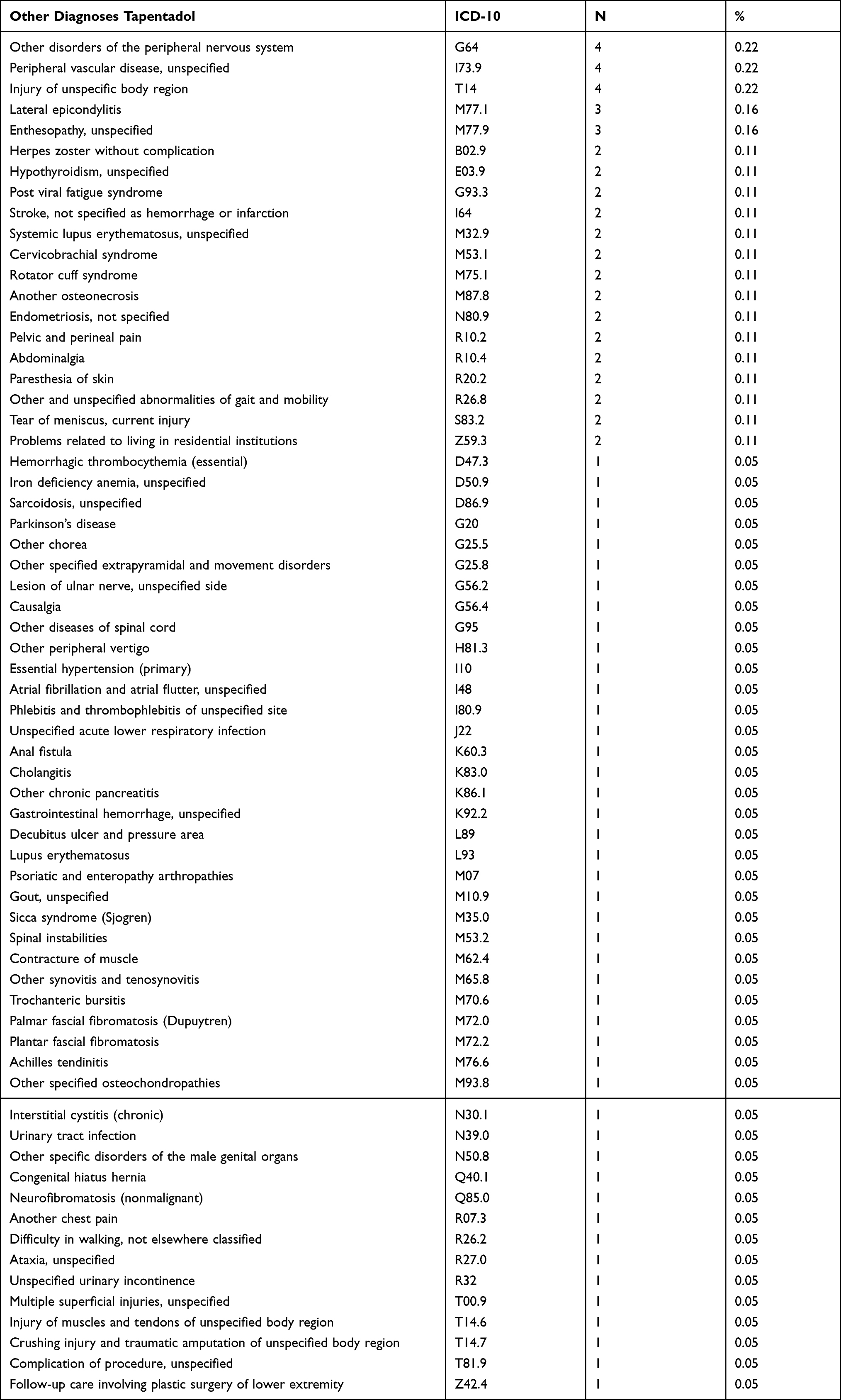 |
Table 2 Other Diagnoses Associated with Tapentadol Prescription |
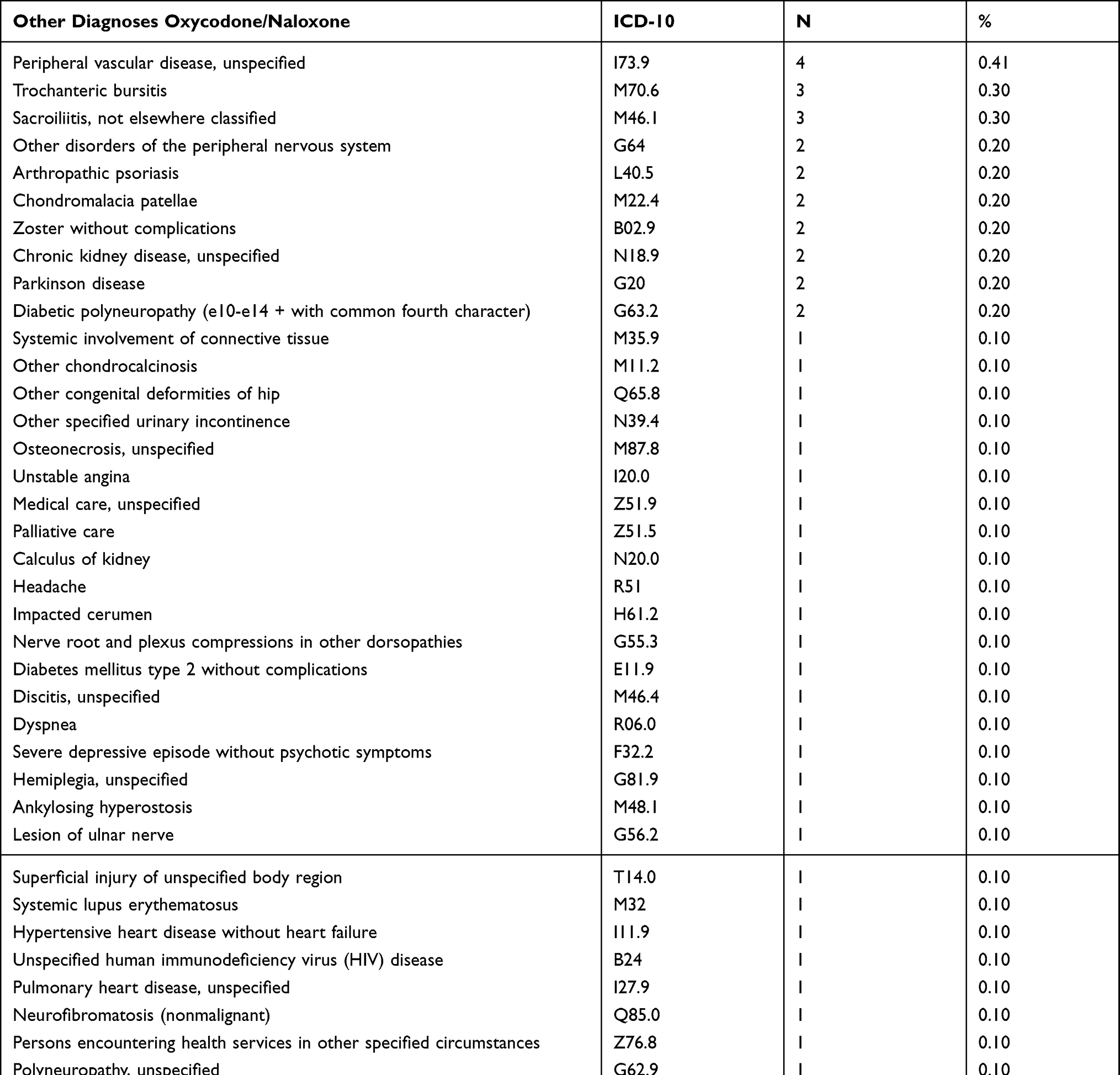 |
Table 3 Other Diagnoses Associated with Oxycodone/Naloxone Prescription |
Diagnoses vs Daily Dose
In the case of tapentadol, the highest daily dose was in the incorrect indications of depressive disorder and diabetes mellitus (175.0±155.4 mg and 137.5±75 mg, respectively) followed by unspecified rheumatism (135.3 ±170.6 mg) and the lowest was for unspecified osteoarthritis (62.5 ±28.8). There were no statistically significant differences in the daily dose in tapentadol according to diagnosis (p = 0.094).
In oxycodone/naloxone the highest daily dose was for unspecified rheumatism (33.3 ±26.6 mg) and the lowest for unspecified osteoarthritis (17.5±12.8 mg). Nevertheless, there were statistically significant differences in the daily dose of oxycodone with respect to the diagnoses (p = 0.049). The significant differences (p = 0.032) were found between the daily dose of osteoarthritis (21.0±16.4 mg) and neoplasic processes (33.2±29.3 mg), after applying Bonferroni test.
Diagnoses vs Treatment Duration
In the case of tapentadol, the highest treatment duration was in the incorrect indication of depressive disorder (365.5±301.7 days) followed by osseous stenosis (242.8±223.1 days) and unspecified rheumatism (242.2±316.5 days) and the shortest was for non-associated diagnoses (94.8±66.8 days). There were statistically significant differences in the duration of tapentadol treatment concerning the diagnoses (p < 0.005). Concretely, the significant differences were found concerning neoplasic processes (122.3±102.2 days) and neuralgia (208.3±225.7 days), and neoplasic processes and other diagnosis (239.2±279.7 days), neuralgia (208.3±225.7 days) and not associated diagnosis (94.8±66.8 days), osteoarthritis (198.4±199.5 days) and not associated diagnosis (94.8±66.8 days), fibromyalgia (229±278.1 days) and not associated diagnosis (94.8±66.8 days), more than one diagnosis associated (216.5±236.2 days) and not associated diagnosis (94.8±66.8 days), other diagnosis (239.2±279.7 days) and not associated diagnosis (94.8±66.8 days), after applying Bonferroni test (p=0.035, p=0.031, p=0.002, p=0.036, p=0.013, p=0.012, p=0.031, respectively).
The highest duration of treatment with oxycodone/naloxone was in patients with more than one diagnosis (315.5±371.8 days) and the shortest for algoneurodystrophy (90.0±0 days). There were statistically significant differences in the duration of oxycodone/naloxone treatment about the diagnoses (p < 0.005). In this case, the significant differences were found about neoplasic processes (135.9±76 days) and more than one diagnosis associated (315.5±371.8 days), not associated diagnosis (92.1±61.1 days) and more than one diagnosis associated (315.5±371.8 days), fibromyalgia (311.4±379.5 days) and more than one diagnosis associated (315.5±371.8 days), after applying Bonferroni test (p=0.013, p=0.001, p=0.027, respectively).
Discussion
This is a drug utilization study focus on a population with active prescription of tapentadol or the combination oxycodone-naloxone in a specific region of a country, and its results do not necessarily be directly applicable to others. However, it provides information about prescription patterns such as dose prescribed and the extent of use by higher-risk populations and their results could be representative of other countries.
Description of the Population
Tapentadol was used approximately 2 times more than oxycodone/naloxone at the cutoff date. This could be explained by the fact that tapentadol extended release is related with substantially lesser incidences of gastrointestinal side effects than oxycodone/naloxone combination.12,19–21
In addition, all patients used prolonged-release tablets also in tapentadol (the only one that has immediate-release tablets), which are indicated to control severe chronic pain and not acute pain.15,16,22 This also indicates that the six patients who were taking the two medications simultaneously were a duplication that would have to be intervened by de-prescribing one of the two opioids, since they did not intend to treat breakthrough pain in which immediate-release analgesics are used as a “rescue” medication.15,16
Although the use of tapentadol or oxycodone/naloxone between sex was diverse, there was a higher percentage of women than men with active prescriptions of these drugs. This difference could be explained because the pain threshold in women and men is different.23–25
Renal and Hepatic Function
In the study, 1.5% of patients treated with tapentadol (N = 28) and 1.5% of patients treated with oxycodone/naloxone (N = 15) had severe (GFR: 15–29 mL/min) chronic kidney disease (CKD). According to the SmPC, tapentadol has not been studied in controlled efficacy trials in patients with severe CKD; therefore, its use is not recommended in this population.15 Also, patients with CKD have shown higher plasma concentrations of oxycodone and naloxone. Thus, caution should be taken when using oxycodone/naloxone medications in patients with mild CKD (GFR: 60–89 mL/min) and in the case of patients with severe CKD, strict medical surveillance is needed.16
As for liver function, around 4% of patients from each group (28 patients treated with tapentadol and 15 with oxycodone/naloxone) suffered from impaired liver function. The impairment of opioid metabolism increases in line with increased liver dysfunction, hence major changes in opioid metabolism have been detected mainly in patients suffering from severe liver diseases, ie, cirrhotic patients. Therefore, among opioids that could require a prolonged dose interval, or a dose reduction are tapentadol and oxycodone.26 According to the SmPC, tapentadol should be used with caution in patients with moderate hepatic impairment. In the case of severe hepatic impairment, no clinical studies have been found with tapentadol; therefore, its use is not recommended in this population.15 As for oxycodone/naloxone, clinical trials have shown that plasma concentrations of both oxycodone and naloxone are higher in patients with impaired liver function. This means that medicines containing oxycodone and naloxone as active ingredients are contraindicated in patients with moderate or severe liver failure.16
Finally, although in general no dose adjustment was necessary in elderly patients in any of the treatments, considering the age profile of the population of the present study and that elderly patients are more likely to have kidney and liver dysfunction, caution must be exercised when choosing the dose, as recommended.
Treatment Duration
Almost half of the patients, both in tapentadol (51.5%) and oxycodone/naloxone (43.2%), had durations of treatment between one and three months. However, almost the other half (45.3 and 48.6% in tapentadol and oxycodone/naloxone, respectively) had treatment durations ranging from more than 90 days to more than 2 years, despite the very limited evidence on the efficacy and safety of long-term opioid treatment.27,28
Often, the liability for chronic pain management and decision in starting an opioid therapy lies on the general practitioners and other non-specialist opioid prescribers, as emergency doctors.26 Insufficient training and information about opioid management protocols, time pressure to assess patients properly are some of the reasons that could explain the off-label prescription of opioids.26 A pain specialist or access to specialized and integrative care to re-evaluate the treatment might be needed in patients who had no improvement for the first three months.7,9
Prescribed Daily Dose
In this study variable differences were found between the two drugs. Thus, in the case of tapentadol, no statistically significant differences were found in the prescribed daily dose as a function of age. However, an increase in daily doses is observed in older patients (age groups 81–90 and >90 years). Quite the opposite happened in the oxycodone/naloxone combination, where there was a trend of decreasing daily dose values with increasing age that was statistically significative.
The general warning on the safety of patients based on the daily dose used, considering the majority age group found in the present study and the renal and liver functions of these patients, could be especially relevant in the case of tapentadol. Furthermore, only in the case of tapentadol, 3 patients were found who, although young, exceeded the authorized dose according to the SmPC.16 On the other hand, underdosed patients were found in both tapentadol and oxycodone/naloxone (7.2% and 18.2%, respectively).
Therefore, some patients included in this study had improper dosages, so prescribed daily doses for these patients should be reviewed in the prescription program to prevent both overdosing and underdosing. According to European Pain Federation, the correct dose of an opioid is the lowest possible dose that achieves the desired outcome.9,26 The decision to modify opioid dosage must be made considering pain reassessment since increased risk of serious harms appears to be dose-dependent,27,28 patient adherence on treatment, and frequency of monitoring, among others.
Besides, additional evidence confirms an association between opioids and increased risk of serious harms that appears to be dose-dependent,27,28 they should only be introduced when strictly necessary and with due respect to a continuous risk-benefit analysis.
If we analyze the daily dose according to sex in both treatments, men took more doses than women. Although these differences were significant only in the case of oxycodone/naloxone, this is consistent with published data suggesting that elderly patients and females may suffer from bias in pain assessments or dosing23 this could be, as it was commented before because women had less intensity of pain than men.23–25 Results of a genome wide association study suggested that differences experienced by men and women in chronic pain are likely to have a genetic basis.29
By studying the daily dose depending on the duration of treatment, in both cases an increasing length of treatment increased the daily dose used, being significant, both positive correlations. The literature shows a strong relationship between initial exposure to opioids and the likelihood of long-term use and, therefore, an increase in tolerance.30 Thus, the progression of long-term opioid use, should be prevented, in cases where it is not necessary, or it is clinically inadequate.9,26,31
Drug Treatment Combination with Tapentadol and Oxycodone/Naloxone
Tapentadol and oxycodone/naloxone followed a similar pattern related to concomitant medications. It is remarkable that more than 85% of patients were taking simultaneously so many pain medications, being some of the most used analgesics, antiepileptics, antidepressants, anxiolytics, selective serotonin reuptake inhibitor and sedatives. As it was mentioned before, polymedication is considered an important risk factor, because involves a major therapeutic complexity and a lower adherence to treatment, which negatively influences the achievement of expected clinical improvement. In addition, the increase in potential drug interactions and side effects, especially in the elderly due to the decrease in hepatic, renal and cardiac functions, should be noted.16
Diagnoses
The diagnoses for which tapentadol and oxycodone/naloxone are prescribed followed a similar pattern. Around 42% of tapentadol and around 34% of oxycodone/naloxone prescriptions were for neuralgia, spondylosis, lumbago with sciatica or intervertebral disc disorders. The second common diagnoses in both drugs were related to osteoarthritis, which is the most usual form of joint disease and the main cause of pain and physical disability in the elderly.26 The third were related to fractures and osteoporosis.
Only around 5% of diagnoses were neoplasms for the two drugs studied. Around 4% of patients had not associated diagnosis, in those cases, the dose was lower than in the others, and length of treatment was 94 days.
At this point, it is important to highlight, that opioids should only be introduced when strictly necessary. Many patients may tolerate and respond to this treatment, and it should not be denied to them when deemed medically necessary by a responsible physician.9,26,31
Throughout the discussion, several interventions that would be necessary to improve the use of these drugs have already been indicated. Thanks to this study, inappropriate posology of tapentadol and oxycodone/naloxone has been detected and in September 2019 the recommended posology of both drugs has been added to the electronic primary care clinical station (ECAP). The ECAP prescription module proposes now the approved dosage regimen for each drug and the physician should review and modify the prescription if necessary. Furthermore, other interventions would be, for example, better practices in promotion of medicines and subsequent training to prescribers and other health professionals to raise awareness about opioids risk.26 Wong et32 al pointed out the implementation of interventions for emergency department utilizing patients with chronic noncancer pain could decrease the frequency of visits, care‐associated costs, amount of opioid administration and prescription.
Conclusions
We found that the use of tapentadol and the combination oxycodone/naloxone in primary health care was characterized by female patients between 71 and 90 years of age and with mild or moderate decrease in renal function. Typical use was of one of these opioids at lower doses than men for an average of 31 to 90 days. Daily doses were higher in longer treatments, mainly of between one and two years of duration.
To conclude, the pattern of use and profile of patients with tapentadol and oxycodone/naloxone had more similarities than differences. The study suggested that prescribing practices and patient monitoring should be assessed regularly to ensure patient safety and effective management of pain.
Patient and Public Involvement
Patients and the public were not involved in the design or execution of this study.
Data Sharing Statement
Data used in this study are available from the corresponding author upon reasonable request.
Ethics Approval
Ethical approval was not required as it was made a secondary analysis of suitably anonymized data sets. It was not an experimental study and patients were not recruited.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All the authors report no conflicts of interest for this work and have disclosed that they have no significant relationships with or financial interests in any commercial companies related to this study or article.
Montserrat Viñas-Bastart: No conflict; Míriam Oms-Arias: No conflict; Àfrica Pedraza-Gutiérrez: No conflict; Irene Lizano-Díez: No conflict; Eduardo L. Mariño: No conflict, Pilar Modamio: No conflict.
References
1. Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
2. Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770.
3. International Association for the Study of Pain (IASP). European Federation of IASP Chapters. Right to pain relief. 4A. Unrelieved pain is a major global healthcare problem; 2004. Available from: https://www.iasp-pain.org/GlobalYear/RighttoPainRelief.
4. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high impact chronic pain among adults – United States, 2016. MMWR. 2018;67(36):1001–1006.
5. Breivik H, Collett B, Ventafridda V, et al. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333.
6. Dueñas M, Salazar A, Ojeda B, et al. A nationwide study of chronic pain prevalence in the general Spanish population: identifying clinical subgroups through cluster analysis. Pain Med. 2015;16(4):811–822.
7. Provenzano DA, Viscusi ER. Rethinking the role of opioids in the outpatient management of chronic nonmalignant pain. Curr Med Res Opin. 2014;30(10):2051–2062.
8. Els C, Jackson TD, Kunyk D, et al. Adverse events associated with medium- and long-term use of opioids for chronic non-cancer pain: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;10:CD012509.
9. Manchikanti L, Kaye AM, Knezevic NN, et al. Responsible, safe, and effective prescription of opioids for chronic non-cancer pain: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician. 2017;20(2S):
10. Meske DS, Lawal OD, Elder H, et al. Efficacy of opioids versus placebo in chronic pain: a systematic review and meta-analysis of enriched enrolment randomized withdrawal trials. J Pain Res. 2018;11:923–934.
11. Faria J, Barbosa J, Moreira R, et al. Comparative pharmacology and toxicology of tramadol and tapentadol. Eur J Pain. 2018;22(5):827–844.
12. Morgan CL, Jenkins-Jones S, Currie C, et al. Outcomes associated with treatment of chronic pain with tapentadol compared with morphine and oxycodone: a UK primary care observational study. Adv Ther. 2019;36(6):1412–1425.
13. Vondrackova D, Leyendecker P, Meissner W, et al. Analgesic efficacy and safety of oxycodone in combination with naloxone as prolonged release tablets in patients with moderate to severe chronic pain. J Pain. 2008;9:1144–1154.
14. Huang L, Zhou JG, Zhang Y, et al. Opioid-induced constipation relief from fixed-ratio combination prolonged-release oxycodone/naloxone compared with oxycodone and morphine for chronic non-malignant pain: a systematic review and meta-analysis of randomized controlled trials. J Pain Symptom Manage. 2017;54(5):737–748.e3.
15. The Spanish Agency of Medicines and Medical Devices (AEMPS). Summary of Product Characteristics tapentadol (Palexia retard®, Grünenthal pharma, S.A). Available from: https://cima.aemps.es/cima/dochtml/ft/75917/FT_75917.html.
16. The Spanish Agency of Medicines and Medical Devices (AEMPS). Summary of Product Characteristics oxycodone/naloxone (Targin®, Mundipharma pharmaceuticals, S.L.). Available from: https://cima.aemps.es/cima/dochtml/ft/71124/FT_71124.html.
17. Viñas-Bastart M, Oms-Arias M, Pedraza-Gutiérrez À, et al. Clinical use of pregabalin in general practice in Catalonia, Spain: a population-based cross-sectional study. Pain Med. 2018;19:1639–1649.
18. Government of Catalonia. Department of Health. Organization Chart: unit of coordination and strategy of the medicine; 2019. Available from: http://www14.gencat.cat/sacgencat/AppJava/organigrama.jsp?codi=10137&jq=200001.
19. Afilalo M, Etropolski MS, Kuperwasser B, et al. Efficacy and safety of tapentadol extended release compared with oxycodone controlled release for the management of moderate to severe chronic pain related to osteoarthritis of the knee: a randomized, double-blind, placebo and active-controlled Phase III study. Clin Drug Investig. 2010;30:489–505.
20. Baron R, Jansen J-P, Binder A, et al. Tolerability, safety, and quality of life with tapentadol prolonged release (PR) compared with oxycodone/naloxone PR in patients with severe chronic low back pain with a neuropathic component: a randomized, controlled, open- label, phase 3b/4 trial. Pain Pract. 2016;16(5):600–619.
21. D’Amato T, Martorelli F, Fenocchio G, et al. Tapentadol vs oxycodone/naloxone in the management of pain after total hip arthroplasty in the fast track setting: an observational study. J Exp Orthop. 2019;6(1):36.
22. Anekar AA, Cascella M. WHO Analgesic Ladder.In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
23. Zhang L, Losin EAR, Ashar YK, Koban L, Wager TD. Gender biases in estimation of others’ pain. J Pain. 2021. doi:10.1016/j.jpain.2021.03.001
24. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anesth. 2013;111(1):52–58.
25. Packiasabapathy S, Sadhasivam S. Gender, genetics, and analgesia: understanding the differences in response to pain relief. J Pain Res. 2018;11:2729–2739.
26. O’Brien T, Christrup LL, Drewes AM, et al. European Pain Federation position paper on appropriate opioid use in chronic pain management. Eur J Pain. 2017;21(1):3–19.
27. Canadian Agency for Drugs and Technologies in Health. Long-acting opioids for chronic non-cancer pain: a review of the clinical efficacy and safety; 2015. Available from: https://cadth.ca/sites/default/files/pdf/htis/aug-2015/RC0698%20Opioids%20Final.pdf.
28. Agency for Healthcare Research and Quality (AHRQ). Opioid Treatments for Chronic Pain. Comparative Effectiveness Review No. 229. AHRQ Publication No. 20-EHC011; 2020. Available from: https://effectivehealthcare.ahrq.gov/sites/default/files/pdf/opioids-chronic-pain.pdf.
29. Johnston KJA, Ward J, Ray PR, et al. Sex-stratified genome-wide association study of multisite chronic pain in UK Biobank. PLoS Genet. 2021;17(4):e1009428.
30. Hadlandsmyth K, Mosher H, Lund BC. Associations between initial opioid exposure and the likelihood for long-term use. J Am Pharm Assoc. 2019;59(1):17–22.
31. Bialas P, Maier C, Klose P, et al. Efficacy and harms of long-term opioid therapy in chronic non-cancer pain: systematic review and meta-analysis of open-label extension trials with a study duration ≥26 weeks. Eur J Pain. 2020;24:265–278.
32. Wong CK, O’Rielly CM, Teitge BD, et al. The characteristics and effectiveness of interventions for frequent emergency department utilizing patients with chronic noncancer pain: a systematic review. Acad Emerg Med. 2020;27(8):742–752.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.