Back to Journals » International Journal of Women's Health » Volume 17
Systemic Inflammatory Biomarkers as a Predictive Markers for Ovarian Cancer
Authors Kurniadi A ![]() , Ridwan S, Hidayat YM
, Ridwan S, Hidayat YM ![]() , Rauf S, Mantilidewi KI
, Rauf S, Mantilidewi KI ![]() , Winarno GN
, Winarno GN ![]() , Salima S
, Salima S ![]() , Suardi D
, Suardi D
Received 13 September 2024
Accepted for publication 14 February 2025
Published 30 April 2025 Volume 2025:17 Pages 1193—1201
DOI https://doi.org/10.2147/IJWH.S496137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Andi Kurniadi,1 Steven Ridwan,1 Yudi Mulyana Hidayat,1 Syahrul Rauf,2 Kemala Isnainiasih Mantilidewi,1 Gatot NA Winarno,1 Siti Salima,1 Dodi Suardi1
1Department of Obstetrics and Gynecology, Universitas Padjadjaran, Bandung, Indonesia; 2Department of Obstetrics and Gynecology, Universitas Hasanuddin, Makassar, Indonesia
Correspondence: Kemala Isnainiasih Mantilidewi, Department of Obstetrics and Gynecology, Faculty of Medicine, Universitas Padjadjaran, Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +6281220828092, Email [email protected]
Objective: Tumor markers such as CA125 are highly beneficial in predictive ovarian malignancy; however, this advanced test is not always available in remote areas. To address this issue, the author aimed to explore the use of systemic inflammatory biomarkers as complementary modalities for diagnosis of ovarian malignancy.
Methods: This diagnostic study utilized a cross-sectional approach, with outcomes measured by AUC and sensitivity. A total of 132 patients with adnexal tumors were consecutively included and measured a complete blood count. From this, the MLR (Monocyte Lymphocyte Ratio), NLR (Neutrophil Lymphocyte Ratio), PLR (Platelet Lymphocyte Ratio), SII (Systemic Immune Inflammation Index), and SIRI (Systemic Inflammatory Response Index) biomarkers were calculated. After surgery, histopathological examination was performed as the gold standard and the biomarker predictions were then compared to it, followed by statistical analysis.
Results: The AUC values for MLR, NLR, PLR, SII, and SIRI were 0.70, 0.731, 0.696, 0.743, and 0.722, respectively. The p-values were MLR (0.005), NLR (0.001), PLR (0.001), SII (< 0.001), and SIRI (< 0.001), respectively. In multivariate analysis, only SII was significant (p = 0.015). The Exp(B) and 95% CI were 5.472 (1.383– 21.655). The validity test for SII showed satisfactory results: sensitivity 71.64%, specificity 73.84%, PPV 73.84%, NPV 71.64%, accuracy 72.72%, LR+ 2.74%, and LR- 0.38%.
Conclusion: Systemic inflammatory biomarkers, particularly SII may aid in the predictive markers of early ovarian with diagnostic values nearly as good as CA125 (sensitivity 71.64% vs 75.97%). These biomarkers can serve as complementary predictive markes modalities for ovarian malignancy, especially when advanced tumor marker tests like CA125 are not available in remote areas.
Keywords: MLR, NLR, PLR, SII, SIRI, ovarian malignancy
Introduction
Ovarian cancer is the 18th most common cancer in the world and the 8th most common cancer occur in women. Based on 2020 data, there were more than 313,000 new cases of ovarian cancer worldwide. 1 Ovarian cancer prevalence in Indonesia, Jakarta as reported by Winarto et al in 2015 was 45.04%. Feharsal and Andi D. Putra in 2016 also reported the prevalence of 48.74%.2,3 Meanwhile in RSUP Hasan Sadikin, Bandung based on Primary Cancer Registry of Gynaecology Oncology Division there were 480 ovarian cancer cases from 2020 to 2022. Putra reported that during 7 months observation in 2018 there were 58 ovarian cancer cases and 61 benign ovarian tumour cases. Thereby, the prevalence of ovarian cancer in RSUP Hasan Sadikin Bandung is 48.7%.4
Based on Surveillance, Epidemiology, and End Results (SEER) data in the United States, the 5-year survival for all stages combined increased from 33.6% in 1975 to 47.6.2% in 2009–2015. Using statistical models for analysis, rates for new ovarian cancer cases have been falling on average 1% per year over the last 10 years. Death rates have been falling on average 1.6% per year over the same period. The death rate decreased 32% from 10 per 100,000 women per year in 1976 to 6.76 per 100,000 per women per year in 2016. Ovarian cancer rates are highest in women aged 55 to 64 years (median age 63 years), and deaths are highest in women aged 75 to 84 years (median age 71 years). However, in Indonesia, the collected data was estimated to have 396,914 new cancer cases in 2020. Ovarian cancer was the second most common gynecological cancer in Indonesia, after cervical cancer.5
Ovarian cancer early diagnosis is very important in management of this disease, because it is usually diagnosed at advance stage and in consequence the prognosis is poor and the mortality rate is still high. Several tools supported ovarian cancer early diagnosis such as CA125, LDH, AFP, BHCG, RMI (Risk Malignancy Index) and Ultrasound with IOTA (International Ovarian Tumour Analysis) had been used widely in the management of the disease. However, the tools mentioned above are not always available in primary or secondary health care facilities, particularly in archipelagic developing countries with wide diversities like Indonesia.
Overcoming the obstacles, we tried to assessed other tools for early diagnosis of ovarian cancer which are inexpensive, always available and easy to perform even in primary or secondary health care facilities with limited resources. The tools were systemic inflammation biomarkers. The systemic inflammation biomarkers consisted of five indicators as follows, MLR (Monocyte Lymphocyte Ratio), NLR (Neutrophil Lymphocyte Ratio), PLR (Platelet Lymphocyte Ratio), SII (Systemic Immune Inflammation Index) and SIRI (Systemic Inflammatory Response Index).6–15
Recent studies have reported that hematological tests such as NLR and PLR play a role in the differential diagnosis of ovarian tumors. It has been reported that NLR and PLR tend to increase in ovarian malignancies, and that these elevated ratios are associated with poor prognosis in cancer patients. However, NLR and PLR are not specific to cancer, and increases in these ratios can also be caused by systemic diseases such as cardiovascular disease, rheumatic diseases, and infections. In 2022, a report highlighted the levels of NLR and PLR in ovarian malignancies, borderline ovarian tumors, and benign ovarian tumors. It was found that NLR and PLR levels were significantly higher in ovarian malignancies compared to borderline and benign ovarian tumors. Lymphocyte counts were also significantly lower in ovarian malignancies compared to borderline and benign ovarian tumors.7,13–15
In 2021, a report suggested that MLR, as a hematological ratio, could replace CA125 in predicting epithelial ovarian cancer. The study found a significant correlation between this biomarker and CA125 levels, concluding that MLR could be used as an alternative to CA125, especially in regions or countries with lower socioeconomic status where CA125 testing is difficult to perform. A high MLR indicates a decrease in lymphocyte count and/or an increase in monocyte count. The prognostic value of MLR in ovarian cancer is presumed to be related to immune cells infiltrating the tumor, such as Tumor Infiltrating Lymphocytes (TIL) and Tumor Associated Macrophages (TAM).12,16
The Systemic Immune Inflammation Index (SII) and the Systemic Inflammatory Response Index (SIRI) are new indicators that reflect inflammation in humans. SIRI is an index based on immune cells in the human circulatory system. Systemically, SIRI reflects the complex interactions and potential synergistic effects between neutrophils, monocytes, and lymphocytes in the tumor microenvironment, reflecting the balance between the body’s inflammatory response and immune response levels, and can be used to assess immune function. In recent years, a large number of clinical studies have evaluated the correlation between SIRI and the prognosis of patients with various tumors, such as those in the digestive, respiratory, endocrine, urinary, and reproductive systems. The results show that high SIRI levels predict poor prognosis.
SII is a comprehensive inflammatory index that combines platelets, neutrophils, and lymphocytes to reflect host immune status and inflammatory response. In recent years, many studies have focused on SII in tumors of the gastrointestinal tract, respiratory system, blood, urinary system, and reproductive system. SII is a potential indicator reflecting the balance between host immunity and inflammation, while SIRI is a good indicator for assessing cancer-related inflammatory responses.10
Huang et al and Feng et al in 2023 reported that SIRI and SII values were significantly positively correlated with CA-125 levels in predicting ovarian malignancies. Furthermore, one of these reports stated that SIRI and SII also positively correlated with CA-153 and HE4 in predicting ovarian malignancies. It appears that SIRI and SII could serve as alternative biomarkers to CA-125 in predicting ovarian malignancies.9,11
From the characteristics of systemic inflammation status as obtained from indicators above, we can predict the nature of neoplasm and thus they can be useful for ovarian cancer early diagnosis.
Materials and Methods
This study aimed to evaluate systemic inflammation biomarkers as tools for the early diagnosis of ovarian cancer. Designed as a diagnostic study, it employed an analytical observational methodology with a cross-sectional approach.
Statistical Analysis
Data obtained were analyzed with IBM SPSS Statistics 25.0 for Windows, using the Receiver Operating Characteristic (ROC) curve to determine the Area Under the Curve (AUC) and the optimal cutoff value for each biomarker. The ROC curve is a graphical representation that evaluates a model’s ability to distinguish between two classes by plotting the true positive rate (sensitivity) against the false positive rate (1-specificity) at various threshold levels. The AUC summarizes this performance as a single scalar value, ranging from 0.5 (no discriminative power) to 1.0 (perfect classification). A higher AUC indicates better performance in distinguishing between the two classes, while the ROC curve itself provides insights into the trade-offs between sensitivity and specificity at different thresholds.
The data were analyzed using both bivariate (Chi-square) and multivariate (logistic regression) analyses. Additionally, a validity test was performed to determine the sensitivity, specificity, and accuracy of the biomarkers. These metrics collectively provide a comprehensive assessment of the diagnostic performance of each biomarker, guiding the interpretation and potential application of the findings.
This study included 132 subjects with ovarian masses who were recruited at Hasan Sadikin General Hospital, Bandung, between February and August 2024. Subjects were excluded if they had a history of other malignancies, prior chemotherapy, bone marrow or blood disorders, acute or chronic inflammation, or steroid hormone use within the last three months.
All participants provided proper informed consent and signed an approval letter for study enrollment. The study adhered to legal and ethical considerations, receiving approval from the Ethical Committee of Health Research at Padjadjaran University and Dr. Hasan Sadikin General Hospital in Bandung.
The participants were patients suspected of having ovarian malignancies and underwent preoperative evaluations. These assessments included a medical history review, physical examination, abdominal and transvaginal ultrasound imaging, and CT scans. Laboratory blood tests were conducted, encompassing a complete blood count and tumor markers such as CA125, LDH, AFP, and HCG. Systemic inflammatory biomarkers were derived from the complete blood count results for each subject. Following these preoperative evaluations, the participants underwent surgery, including surgical staging for early-stage ovarian cancer or debulking procedures for advanced stages. Histopathological examination was performed on the surgical specimens, serving as the gold standard for ovarian cancer diagnosis. The collected data were then statistically analyzed to assess the diagnostic value of systemic inflammatory biomarkers for ovarian cancer.



Study Limitations
This study has several limitations that should be acknowledged. First, it was conducted at a single institution (Hasan Sadikin General Hospital) with a relatively modest sample size of 132 patients, which may limit the generalizability of the findings; a larger, multi-center study would provide more robust and widely applicable results. Second, the cross-sectional design restricts the ability to assess temporal relationships and long-term outcomes, highlighting the need for prospective longitudinal studies to better evaluate the prognostic value of these biomarkers. Third, the inclusion of both epithelial and non-epithelial ovarian cancers introduces population heterogeneity, which may influence the interpretation of inflammatory biomarkers due to differing inflammatory responses among histological types. Additionally, despite the application of exclusion criteria, certain confounding factors—such as subclinical inflammation, metabolic conditions, or medications—may have impacted the inflammatory markers but were not fully controlled for in the analysis. By addressing these limitations, future research will further strengthen the validity and applicability of these findings.
Results
Subjects of this study were 132 women diagnosed with ovarian mass and planned for surgery. Ovarian cancer subjects were 67 of 132 patients (50.75%), thus the prevalence of ovarian cancer was (50.75%). Of the 67 patients diagnosed with ovarian cancer, 51 (76.12%) were epithelial type and 16 (23.88%) were non-epithelial type. The most common epithelial type ovarian cancer was mucinous carcinoma and the most common non-epithelial type ovarian cancer was Adult Granulosa Cell Tumor.
The optimal cut-off value for all biomarkers were determined using Receiver Operating Characteristic (ROC) analysis and graphics. Optimal cut-off values were MLR (0.259), NLR (2.512), PLR (168.263), SII (890.25) and SIRI (1.241). AUC value for MLR, NLR, PLR, SII and SIRI respectively were 0.70, 0.731, 0.696, 0.743 and 0.722. Statistically, the AUC value for all biomarkers were significant with p < 0.001 (Table 1, Figures 1 and 2).
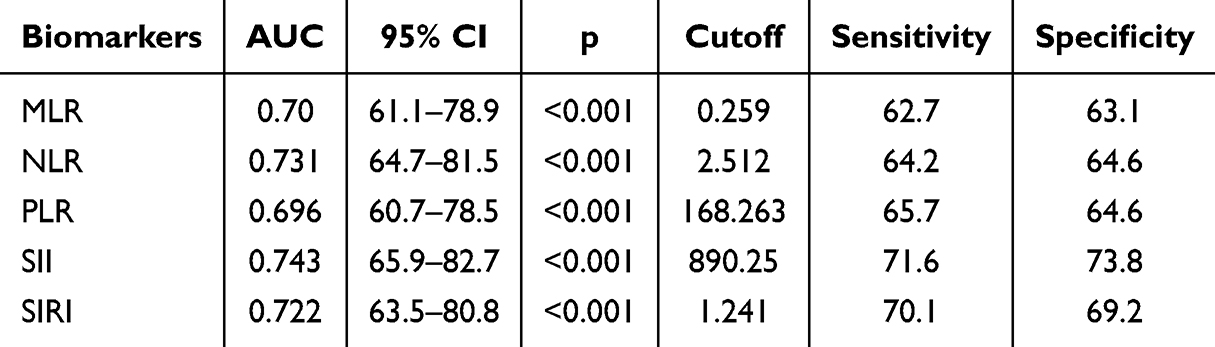 |
Table 1 ROC Analysis and Optimal Cutoff of Biomarkers |
 |
Figure 1 ROC curve of each biomarker. |
 |
Figure 2 Graphics of Optimal cutoff of biomarkers. |
Bivariate analysis (Table 2) revealed that MLR, NLR, PLR, SII dan SIRI were significantly predicted ovarian malignancy. The p value consecutively was MLR (0.005), NLR (0.001), PLR (0.001), SII (<0.001) dan SIRI (<0.001). OR (95% CI) for each biomarker is MLR 2.694 (1.333–5.445), NLR 3.272 (1.604–6.672), PLR 3.493 (1.707–7.149), SII 7.133 (3.313–15.359) and SIRI 5.288 (2.517–11.110).
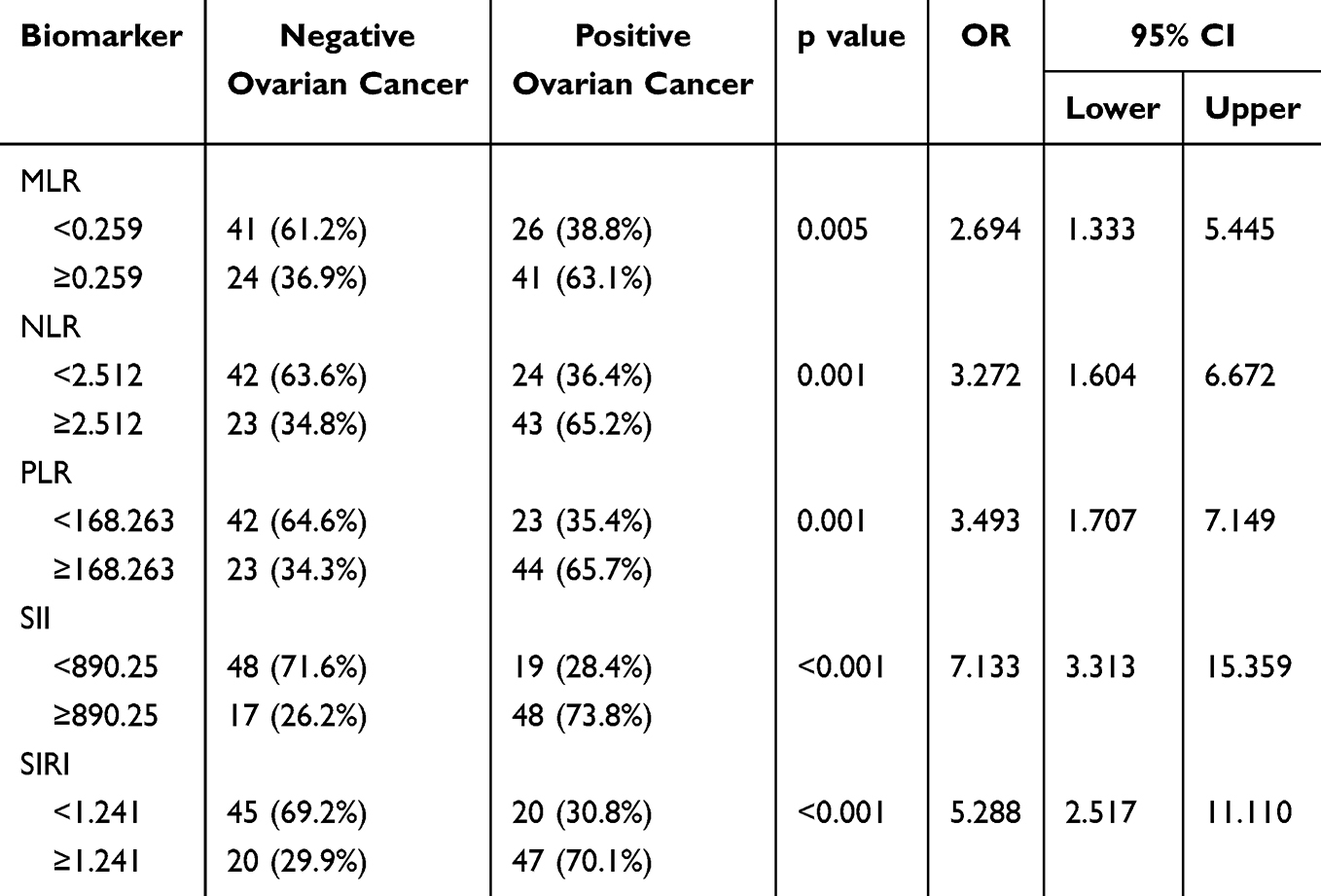 |
Table 2 Bivariate Analysis of Biomarkers |
In multivariate analysis (Table 3), four biomarkers were not significant MLR (p = 0.782), NLR (p = 0.228), PLR (p = 0.319), SIRI (p=0.298), and only one biomarker was significant SII (p = 0.015). The Exp(B) and 95% CI for SII were 5.472 (1.383–21.655). The validity test for SII showed a good enough result as follows, sensitivity 71.64%, specificity 73.84%, PPV 73.84%, NPV 71.64%, accuracy 72.72%, LR+ 2.74% dan LR- 0.38%.
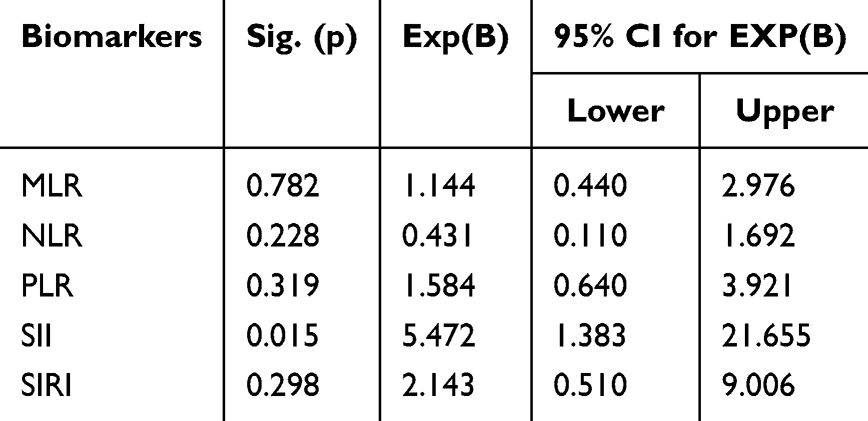 |
Table 3 Multivariate Analysis of Biomarkers |
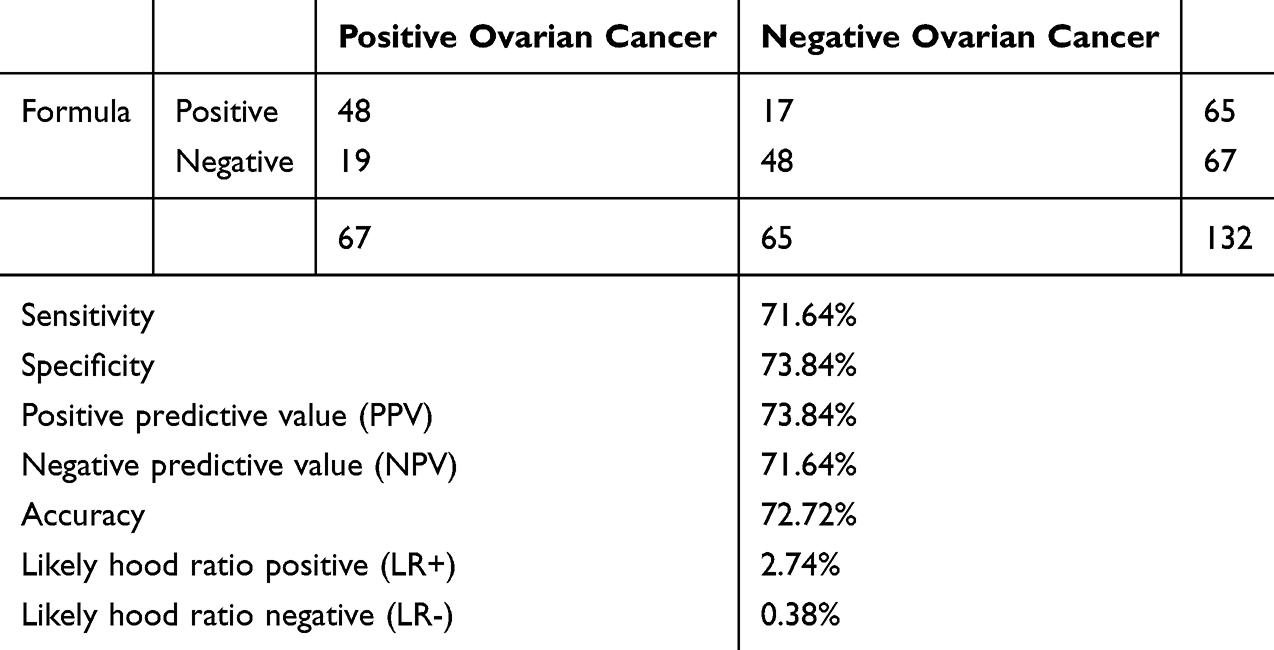 |
Table 4 Validity Test (Diagnostic Test) of SII |
Discussion
During a normal inflammatory response by the innate and adaptive immune system, immune cells carry out their designated task of engulfing and/or destroying foreign invaders.
The systemic immune-inflammation index (SII) and the systemic inflammatory response index (SIRI) are novel indicators reflecting systemic inflammation in humans. They have garnered significant attention in recent years as variables in cancer research. SII serves as an indicator of the balance between inflammation and host immunity, whereas SIRI reflects inflammation-associated responses linked to cancer progression (Wang, Qin et al, 2023).
A European study reported that systemic inflammatory markers can predict malignancy development in humans, suggesting their utility during the pre-diagnostic period for early identification or diagnosis of malignancies (Nøst, Alcala et al, 2021). Additionally, recent studies have highlighted a significant association between elevated SIRI levels and poor prognosis in ovarian cancer (Feng and Wang, 2023). Furthermore, SII has also been reported to predict the disease progression and prognosis of ovarian cancer (Zhang, Lu et al, 2017).
All biomarkers in this study (MLR, NLR, PLR, SII, and SIRI) can be used for predictive biomarkers of ovarian cancer with a significance level of p < 0.001. Two variables demonstrated the best diagnostic value, with an AUC of 0.743 for SII and 0.722 for SIRI. The sensitivity and specificity were 71.6% and 73.8% for SII, and 70.1% and 69.2% for SIRI, respectively. The diagnostic value of SIRI in this study slightly differs from other reports, where SIRI had an AUC of 0.793, sensitivity of 82.4%, and specificity of 62.7%. This difference may be due to the different cutoff points used in this study compared to others (1.24 vs 0.69).11 The diagnostic value of SII also differs between this study and other reports, where SII at a cutoff point of 945.2 had an AUC of 0.793, sensitivity of 47.1%, and specificity of 92.8%.6
The diagnostic potential of the Systemic Immune-Inflammation Index (SII) and Systemic Inflammation Response Index (SIRI) in this study offers an opportunity for comparison with CA125, a widely used ovarian cancer biomarker. A 2018 study reported an AUC of 81.1% and a sensitivity of 71.4% for CA125 in detecting ovarian cancer. Similarly, a 2014 Indonesian study noted a sensitivity of 67.2% for CA125, highlighting some regional variation. While CA125 is a well-established marker, its specificity is limited due to elevated levels in various benign conditions. Comparing SII and SIRI with CA125 could provide valuable insights, as these inflammation-based indices may offer complementary diagnostic value, especially in cases where CA125 alone may fall short.3
Table 2 provides information on the relationship between each variable (biomarker) and histopathology, which is considered the gold standard for diagnosing ovarian malignancy. It is evident that all biomarkers used are significantly associated with histopathological diagnosis, with all p values being less than 0.05. The two variables with the highest Odds Ratios (OR) are SII and SIRI (7.133 and 5.288, respectively).
In multivariate analysis using logistic regression (Table 3), it is apparent that when used together, only SII remains significant (p = 0.015) with an Exp(B) value of 5.472. It can be concluded that among all systemic inflammatory biomarkers, SII is the most recommended for early diagnosis of ovarian malignancy.
Previous studies have highlighted the diagnostic value of CA125 as a predictive marker for epithelial ovarian malignancy. Notably, Han Zheng et al (2019) reported that CA125 exhibited a sensitivity of 75.97%, specificity of 79.59%, positive predictive value (PPV) of 71.01%, negative predictive value (NPV) of 83.42%, accuracy of 78.15%, positive likelihood ratio (LR+) of 3.72, and negative likelihood ratio (LR-) of 0.3. These findings underscore the reliability of CA125 as a biomarker in detecting ovarian malignancies.
In comparison, our study assessed the diagnostic performance of the Systemic Immune-Inflammation Index (SII) for ovarian cancer detection, yielding promising results. The sensitivity of SII was 71.64%, specificity was 73.84%, PPV was 73.84%, NPV was 71.64%, accuracy was 72.72%, LR+ was 2.74, and LR- was 0.38. These metrics indicate that the diagnostic value of SII is comparable to CA125, particularly in terms of sensitivity and specificity (Table 4).
The similarity in performance suggests that SII, as an inflammation-based biomarker, has potential as a supplementary tool to CA125, or even as an alternative in settings where CA125 is not accessible or its specificity is insufficient due to elevated levels in benign conditions. Integrating SII into diagnostic protocols could enhance the accuracy of ovarian cancer detection, particularly when used in combination with existing markers like CA125. This alignment reinforces the value of further exploring inflammation-based indices as reliable diagnostic tools in gynecological oncology.17
Conclusion
Systemic inflammatory biomarkers, with a particular emphasis on the systemic immune-inflammation index (SII), have shown promise as potential diagnostic tools for ovarian malignancies. The diagnostic performance of SII was observed to be nearly comparable to that of the widely used tumor marker CA125, with sensitivity rates of 71.64% and 75.97%, respectively. Beyond their diagnostic accuracy, systemic inflammatory biomarkers present several noteworthy advantages. These include their relatively easier accessibility, reduced costs, and the ability to obtain results in a shorter timeframe compared to advanced tumor marker tests like CA125.
Such advantages make these biomarkers valuable as complementary diagnostic tools, particularly in resource-limited settings or remote areas where sophisticated tumor marker tests may not be readily available. In these situations, systemic inflammatory biomarkers could provide a practical and effective alternative for the early detection of ovarian malignancies, potentially improving diagnostic capabilities in underserved regions.
However, while these findings are encouraging, the author acknowledges certain limitations in the current study and suggests ways to enhance its rigor and applicability. The study would benefit significantly from a larger sample size to provide more robust statistical power and generalizability of the results. Furthermore, the author proposes that designing the study as a multicenter investigation, involving multiple healthcare institutions, would enhance the reliability and external validity of the findings. A multicenter approach could capture a more diverse patient population and varying clinical settings, thereby strengthening the evidence supporting the use of systemic inflammatory biomarkers as diagnostic tools for ovarian malignancy.
Ethics Approval and Informed Consent
This research has been reviewed and approved by the Research Ethics Committee of Dr. Hasan Sadikin General Hospital Bandung (Ethical Approval Number: DP.04.03/D.XIV.6.5/90/2024). All patients have agreed and signed the consent form. This research has complied with the guidelines outlined in the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. WCRF-International. Ovarian cancer statistics. World Cancer Research Fund International. 2024. Available from: https://www.wcrf.org/cancer-trends/ovarian-cancer-statistics/.
2. Feharsal Y, Putra AD. International ovarian tumor analysis (IOTA) scoring system to predict ovarian malignancy preoperatively. Indones J Obstet Gynecol. 2016;4(1).
3. Winarto H, Laihad BJ, Nuranna L. Modification of cutoff values for HE4, CA125, the risk of malignancy index, and the risk of malignancy algorithm for ovarian cancer detection in Jakarta, Indonesia. Asian Pac J Cancer Prev. 2014;15(5):1949–1953. doi:10.7314/APJCP.2014.15.5.1949
4. Putra YAE. Peran Serum Angiotensin-2, Palmitat, Trombositosis, Rasio Netrofil Limfosit, Rasio Trombosit Dan RMI2 Sebagai Prediktor Tumor Ganas Ovarium. Universitas Padjadjaran; 2018.
5. Berek JS, Friedlander ML, Hacker NF. Epithelial ovarian, fallopian TUBE, AND PERITONEAL CANCER. In: Berek JS, Hacker NF, editors. Berek & Hacker’s Gynecologic Oncology. Wolters Kluwer; 2021.
6. Song L, Qi J, Zhao J, Bai S, Wu Q, Xu R. Diagnostic value of CA125, HE4, and systemic immune-inflammation index in the preoperative investigation of ovarian masses. Medicine. 2023;102(37):e35240. doi:10.1097/MD.0000000000035240
7. Yun TH, Jeong YY, Lee SJ, Choi YS, Ryu JM. Neutrophil–lymphocyte and platelet–lymphocyte ratios in preoperative differential diagnosis of benign, borderline, and malignant ovarian tumors. J Clin Med. 2022;11(1355):1355. doi:10.3390/jcm11051355
8. Nie D, Gong H, Mao X, Li Z. Systemic immune-inflammation index predicts prognosis in patients with epithelial ovarian cancer: a retrospective study. Elsevier Inc. 2018.
9. Feng J, Wang Q. Correlation of systemic immune-inflammatory response index with clinical data in patients with malignant ovarian tumor. Am J Transl Res. 2023;15(5):3309–3317.
10. Wang L, Qin X, Zhang Y, Xue S, Song X. The prognostic predictive value of systemic immune index and systemic inflammatory response index in nasopharyngeal carcinoma: a systematic review and meta-analysis. Front Oncol. 2023;13;1006233.
11. Huang H, Wu K, Chen L, Lin X. Study on the application of systemic inflammation response index and platelet–lymphocyte ratio in ovarian malignant tumors. Inter J Gen Med. 2021;14:10015–10022. doi:10.2147/IJGM.S346610
12. Hu Q, Shen G, Li Y, et al. Lymphocyte-to-monocyte ratio after primary surgery is an independent prognostic factor for patients with epithelial ovarian cancer: a propensity score matching analysis. Front Oncol. 2023;13:1139929.
13. Yildirim M, Cendek BD, Avsar AF. Differentiation between benign and malignant ovarian masses in the preoperative period using neutrophil-to lymphocyte and platelet-to-lymphocyte ratios. Molecular Clin Oncol. 2015;3(2):317–321. doi:10.3892/mco.2014.481
14. Bairi KE, Jarroudi OA, Afqir S. Inexpensive systemic inflammatory biomarkers in ovarian cancer: an umbrella systematic review of 17 prognostic meta-analyses. Front Oncol. 2021;11:694821. doi:10.3389/fonc.2021.694821
15. Psomiadou V, Prodromidou A, Galati E, et al. The role of inflammation biomarkers in differential diagnosis of pelvic tumours of ovarian origin: a single-centre observational study. Contemp Oncol. 2021;25(1):7–11. doi:10.5114/wo.2021.105072
16. Gao X-P, Liu Y-H, Liu Z-Y, et al. Pretreatment lymphocyte-to-monocyte ratio as a predictor of survival among patients with ovarian cancer: a meta-analysis. Cancer Manage Res. 2019;11:1907–1920. doi:10.2147/CMAR.S184970
17. Zheng H, Tie Y, Wang X, Yang Y, Wei X, Zhao X. Assessment of the diagnostic value of using serum CA125 and GI-RADS system in the evaluation of adnexal masses. Medicine. 2019;98(7):e14577. doi:10.1097/MD.0000000000014577
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.