Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Systemic Contact Dermatitis Triggered by Benzalkonium Chloride in Laundry Detergent A Case Initially Misdiagnosed as Eczema
Received 28 October 2025
Accepted for publication 15 January 2026
Published 22 January 2026 Volume 2026:19 577154
DOI https://doi.org/10.2147/CCID.S577154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Man Yu,1 Fanlin Meng,2 Shue Tian3
1Department of Dermatology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Emergency Department, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3Department of Dermatology, Deyang Hospital Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Deyang, Sichuan, 618000, People’s Republic of China
Correspondence: Shue Tian, Deyang Hospital Affiliated Hospital of Chengdu University of Traditional Chinese Medicine, Deyang, Sichuan, People’s Republic of China, Tel +86-028-87769233, Email [email protected]
Abstract: This case shows that benzalkonium chloride is an important sensitizer for contact dermatitis.The patient did not respond to conventional eczema treatment. Pathological examination and detailed history-taking revealed that benzalkonium chloride in the detergent was the causative factor. After avoiding exposure to this allergen, the condition improved, emphasizing the need to consider contact dermatitis in patients with refractory eczema.
Keywords: contact dermatitis, benzalkonium chloride, detergent, Eczematous rash
Introduction
Allergic Contact Dermatitis (ACD) is a common clinical inflammatory skin disease that often leads to long-term illness and a decline in patients’ quality of life. Despite advances in dermatology, the diagnosis of ACD remains challenging due to its diverse clinical manifestations, which can easily be confused with other eczematous diseases.1 Among numerous contact allergens, benzalkonium chloride (BAK), a quaternary ammonium compound, is widely used as a disinfectant, preservative, and surfactant in household, medical, and industrial products, and has become an allergen of concern.2 ACD caused by BAK often presents as chronic eczema or atopic dermatitis, leading to misdiagnosis and treatment delays.3,4 Traditional treatments such as corticosteroids and antihistamines can only temporarily relieve symptoms because they do not eliminate allergen exposure at its root.5 This case report highlights misconceptions in the diagnosis of BAK-related dermatitis, emphasizes the importance of detailed patient history taking and product usage inquiry in identifying very common allergens, and further demonstrates the value of such findings in clinical practice.
Case Presentation
Patient Information
A 31-year-old female presented to our dermatology department with a two-month history of worsening skin condition. The eruption consisted of widespread erythema, desquamation, intense pruritus, and localized pain. Initial lesions appeared in the sacrococcygeal region without clear precipitating factors and later extended symmetrically to the trunk and both thighs. During the course of her illness, the patient reported no fever, arthralgia, or mucosal involvement.
Clinical Findings
The patient had sought medical attention at several institutions, where she was diagnosed with “allergic dermatitis” and “eczema.” Previous management included various oral antihistamines (specific agents not recalled) and twice-daily application of topical mometasone furoate 0.1% cream. This regimen initially provided symptomatic relief and partial clearance of lesions; however, the dermatitis recurred within days after discontinuation, with each relapse being more severe and extensive than the previous episode. The patient’s medical history was negative for chronic diseases, atopy, or prior dermatological conditions. She denied known drug allergies, recent medication changes, or exposure to new personal‑care products. Physical examination revealed well‑demarcated erythematous plaques with fine scaling, distributed predominantly over the lower back, buttocks, abdomen, and proximal lower extremities. The lesions followed a pattern corresponding to areas of closest contact with clothing, particularly along waistbands and tight‑fitting garments (Figure 1). No vesicles, bullae, or signs of secondary infection were observed.
 |
Figure 1 (A–D) Clinical photographs of the patient. Well-defined erythematous plaques with fine scaling are observed on the (A) abdomen, (B) Back, (C) Both upper limbs, (D) proximal lower limbs. The lesions are distributed in areas with close contact to clothing. |
Diagnostic Investigations
Routine laboratory tests—complete blood count, comprehensive metabolic panel, and inflammatory markers—were within normal limits. Serum immunoglobulin E levels and autoimmune screening (including ANA and antibodies associated with autoimmune blistering diseases) showed no abnormalities. A 4‑mm punch biopsy taken from a representative lesion in the right lower quadrant demonstrated epidermal atrophy with focal mild spongiosis. The stratum corneum exhibited confluent parakeratosis with retained keratohyalin granules, consistent with granular parakeratosis. The superficial dermis contained a mild perivascular infiltrate composed mainly of lymphocytes with occasional histiocytes (Figure 2). Although not pathognomonic, these histopathological features supported a diagnosis of contact dermatitis.
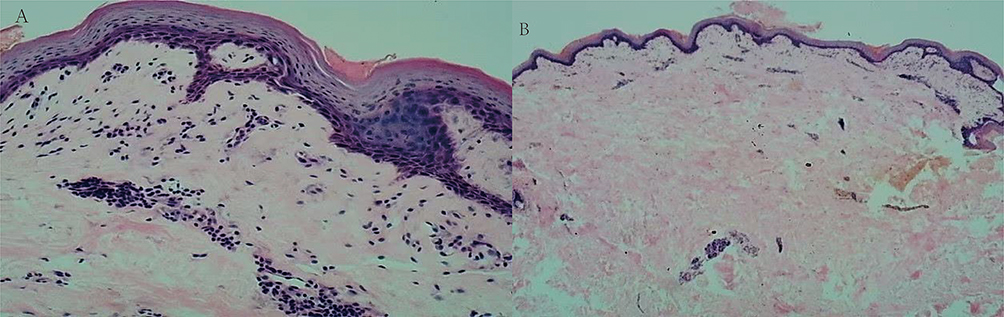 |
Figure 2 (A and B) Histopathological examination of a skin biopsy from the right lower abdomen. (A) The image shows epidermal atrophy with mild spongiosis and confluent parakeratosis (H&E stain, ×100). (B) Higher magnification reveals retained keratohyalin granules within the stratum corneum (granular parakeratosis) and a mild perivascular lymphocytic infiltrate in the superficial dermis (H&E stain, ×400). |
Diagnosis and Management
The distinctive distribution prompted a thorough reinvestigation of environmental exposures. Upon systematic questioning about household products, the patient recalled starting to use a new laundry disinfectant approximately eight weeks before symptom onset. Examination of the product label confirmed benzalkonium chloride as the active antimicrobial ingredient. A diagnosis of allergic contact dermatitis due to benzalkonium chloride exposure was established based on the temporal relationship, distribution pattern, and exclusion of other diagnoses.
Management consisted of an intramuscular injection of compound betamethasone (containing betamethasone dipropionate and betamethasone sodium phosphate) and twice‑daily application of topical fusidic acid 2% cream to prevent secondary infection, supplemented by once‑daily use of mometasone furoate 0.1% cream on active lesions. The patient was comprehensively educated on complete avoidance of the identified disinfectant and instructed to thoroughly clean all clothing and linens.
Outcome and Follow-Up
At the two‑week follow‑up, significant improvement was noted, with marked reduction in erythema, scaling, and subjective symptoms. The patient remained asymptomatic at the one‑month reassessment, confirming the association with benzalkonium chloride exposure.
Discussion
This case illustrates a typical yet often overlooked presentation of ACD triggered by BAK from a laundry disinfectant.6 The diagnostic journey, involving initial misdiagnosis, a temporary response to anti-inflammatory treatments followed by rapid recurrence, is a common challenge in managing ACD.3 The definitive diagnosis hinged on correlating the distinctive clinical distribution (aligning with textile contact) with histopathological findings and, most importantly, a meticulous exposure history that pinpointed BAK as the culprit.2,7
Benzalkonium chloride (BAK) is a component widely used in disinfectants, topical medications, and various household products, and there is extensive literature confirming it as a well-defined contact allergen.2 This case further demonstrates that laundry disinfectants, as an important source of sensitization, are often overlooked.8 Additionally, as a broad-spectrum disinfectant, BAK may disrupt the skin microbiome, a factor that should also be considered as a potential contributor to exacerbating or inducing dermatitis.8 Clinicians should also be aware of other quaternary ammonium compounds, such as cetyltrimethylammonium bromide, and surfactants, as these substances may also cause similar clinical symptoms.2
The important clinical significance of this case lies in the complete resolution of the skin lesions after avoiding the allergen, which definitively confirms the pathogenic role of BAK. Although patch testing was not performed to formally validate the diagnosis, multiple factors strongly support the conclusion of benzalkonium chloride-induced ACD.3 These factors include the strong temporal association between symptom onset and disinfectant use, the typical distribution of lesions in areas where clothing contacts the skin, and the exclusion of other potential etiologies through differential diagnostic evaluation.
Furthermore, as environmental exposure factors become increasingly complex, a systematic Trace back of various recent exposure histories should be conducted during clinical history collection.
In the context of increasingly complex environmental exposures, a broad differential is essential. For instance, skin adverse reactions to vaccines—which can manifest as eczematous or urticarial lesions—have been reported.9,10 However, such reactions typically occur shortly after vaccination and lack the specific clothing-contact distribution pattern observed in our patient. The distinct chronicity and distribution of the lesions, coupled with their rapid resolution upon cessation of the laundry disinfectant, effectively rule out a vaccine-related etiology and further solidify the causal link to BAK.
This case report suggests that benzalkonium chloride (BAK) is an allergen that requires vigilance in household products, and systematic environmental exposure assessment is of significant clinical importance for patients with refractory dermatitis.
Conclusion
This case confirms benzalkonium chloride as a key sensitizer in contact dermatitis. It underscores that detailed history-taking, including specific inquiries about household and laundry products, is crucial for diagnosing ACD masquerading as refractory eczema. Increased clinician awareness of such allergens can significantly reduce diagnostic delays and improve patient outcomes.
Informed Consent for Publication
The patient had signed informed consent and provided informed consent for the publication of the case details and any accompanying images.
Ethics Approval
The publication of case report does not require ethical approval. We confirm that no institutional approval was required for publishing the case details.
Consent for Publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. This article adheres to the applicable CAse REport (CARE) guidelines.
Acknowledgments
Man Yu is first authors for this study. The authors would like to thank all the people involved in this work.
Author Contributions
All authors made significant contributions to the reported work, including conception, study design, execution, data acquisition, analysis, and interpretation. They also participated in drafting, revising, or critically reviewing the article. All authors gave final approval of the version to be published, agreed on the journal for submission, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sheikh HM, Jha RK. Triggered skin sensitivity: understanding contact dermatitis. Cureus. 2024;16(5):e59486. doi:10.7759/cureus.59486
2. Dear K, Palmer A, Nixon R. Contact allergy and allergic contact dermatitis from benzalkonium chloride in a tertiary dermatology center in Melbourne, Australia. Contact Dermatitis. 2021;85:146–5. doi:10.1111/cod.13826
3. Zhang L, Wang YJ, Ma YH, et al. Case report: systemic contact dermatitis caused by benzalkonium chloride in a family (a child and parents). Front Pediatr. 2025;13:1531992. doi:10.3389/fped.2025.1531992
4. Darrigade AS, Léauté-Labrèze C, Boralevi F, et al. Allergic contact reaction to antiseptics in very young children. J Eur Acad Dermatol Venereol. 2018;32(12):2284–2287. doi:10.1111/jdv.15140
5. Li Y, Li L. Contact dermatitis: classifications and management. Clin Rev Allergy Immunol. 2021;61(3):245–281. doi:10.1007/s12016-021-08875-0
6. Isaac J, Scheinman PL. Benzalkonium chloride: an irritant and sensitizer. Dermatitis. 2017;28(6):346–352. doi:10.1097/DER.0000000000000316
7. Lazarov A. Textile dermatitis in patients with contact sensitization in Israel: a 4-year prospective study. J Eur Acad Dermatol Venereol. 2004;18(5):531–537. doi:10.1111/j.1468-3083.2004.00967.x
8. Dear K, Gan D, Stavrakoglou A, et al. Hyperkeratotic flexural erythema (more commonly known as granular parakeratosis) with use of laundry sanitizers containing benzalkonium chloride. Clin Exp Dermatol. 2022;47(12):2196–2200. doi:10.1111/ced.15358
9. Aquino MR, Bingemann TA, Nanda A, Maples KM. Delayed allergic skin reactions to vaccines. Allergy Asthma Proc. 2022;43(1):20–29. doi:10.2500/aap.2022.43.210105
10. Grieco T, Maddalena P, Sernicola A, et al. Cutaneous adverse reactions after COVID-19 vaccines in a cohort of 2740 Italian subjects: an observational study. Dermatol Ther. 2021;34(6):e15153. doi:10.1111/dth.15153
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.