Back to Journals » Clinical Ophthalmology » Volume 19
Switching to Faricimab for Polypoidal Choroidal Vasculopathy with Real-World Outcomes in Refractory Cases – The FAR-PEARL Study Report 1
Authors Fong KC, Wong WJJ, Wong HS, Ling KP, Fong SN ![]() , Shunmugam M
, Shunmugam M
Received 12 March 2025
Accepted for publication 4 July 2025
Published 28 July 2025 Volume 2025:19 Pages 2475—2485
DOI https://doi.org/10.2147/OPTH.S527787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Kenneth CS Fong,1 Wilson Jun Jie Wong,1 Hon Seng Wong,1 Kiet Phang Ling,1 Shir-Ning Fong,2 Manoharan Shunmugam1
1OasisEye Specialists, Kuala Lumpur, Kuala Lumpur, Malaysia; 2University of Nottingham Medical School, Nottingham, NG72UH, UK
Correspondence: Kenneth CS Fong, Email [email protected]
Purpose: To present real-world outcomes of switching to faricimab in eyes with polypoidal choroidal vasculopathy (PCV) refractory to previous anti-VEGF treatments.
Methods: This retrospective study included PCV eyes switched to faricimab for recurrent PCV (> 180 days from prior anti-VEGF treatment), suboptimal extension (60– 180 days), or recalcitrant PCV (< 60 days). Patients were followed monthly, with PRN reinjections for persistent subretinal fluid (SRF), intraretinal fluid (IRF), or pigment epithelial detachment (PED) at the fovea, or a 1-line vision drop. The primary outcome was time to injection-free status (no injection for 3 months), analyzed via survival analysis.
Results: We included 49 eyes with PCV (mean age 66.1 ± 9.5 years; 59% women), 29% had recurrent PCV, 37% suboptimal extension, and 34% recalcitrant disease. Patients had a median of 8 prior anti-VEGF injections,the majority being aflibercept and received a median of 3 faricimab injections (Interquartile range (IQR)=2-4, range=1-8)) over 344 days (IQR=198-446). The interval between the first two faricimab injections averaged 64 ± 43 days, longer in recurrent (86 ± 55 days) vs recalcitrant PCV (43 ± 26 days, p=0.008). By day 90, 49% were injection-free, increasing to 73% by day 210. PED resolved in 53% after the first dose, and in those needing repeat injections, the interval peaked after the fourth dose with no SRF, IRF, nor PED.
Conclusion: The differential response to faricimab in PCV depends on disease type, with recurrent cases requiring fewer injections and recalcitrant cases requiring more intensive initial treatment; however, even recalcitrant eyes can achieve extended intervals after initial doses.
Keywords: polypoidal choroidal vasculopathy, faricimab, refractory neovascular AMD, anti-VEGF resistance, visual and anatomical outcomes, real-world study
Introduction
Polypoidal Choroidal Vasculopathy (PCV) is a subtype of neovascular age-related macular degeneration (nAMD), though increasingly considered by some as a distinct clinical entity due to its unique angiographic features, variable treatment response, and different genetic associations.1 PCV is characterised by an abnormal branching vascular network with polyp-like dilations and is more prevalent in Asian populations, accounting for 22–62% of nAMD cases in these cohorts, and is associated with recurrent subretinal hemorrhages and pigment epithelial detachments (PEDs). Compared to typical nAMD, PCV tends to show variable responses to anti-VEGF therapy, often requiring more frequent or sustained treatment.2,3
Faricimab, a bispecific monoclonal antibody, has emerged as a significant advancement in the treatment of nAMD. It uniquely targets both vascular endothelial growth factor A (VEGF-A) and angiopoietin-2 (Ang-2), two critical mediators in the pathophysiology of nAMD and PCV4. By simultaneously inhibiting VEGF-A and Ang-2, faricimab not only suppresses neovascularization but also stabilizes the vascular environment, potentially leading to improved disease control and clinical outcomes in PCV compared to traditional anti-VEGF therapies.5–7
Clinical trials have demonstrated that faricimab is effective in improving best-corrected visual acuity (BCVA) in patients with nAMD. The TENAYA and LUCERNE trials, which were pivotal in establishing its efficacy, showed that faricimab provided non-inferior visual outcomes compared to aflibercept, a well-established treatment for nAMD.8 Positive outcomes in the PCV subgroups of the Phase III TENAYA and LUCERNE trials led to the initiation of the SALWEEN study. SALWEEN is an ongoing Phase IIIb/IV, multicenter, open-label, single-arm study involving 135 treatment-naïve PCV patients across nine Asian countries. At the 16-week interim analysis, faricimab demonstrated robust visual acuity gains, with 80% of patients achieving absence of retinal fluid. More than 50% achieved complete polyp regression, and 86% of polypoidal lesions were inactive; faricimab was well tolerated with a favorable safety profile in PCV.9
These trials have laid the groundwork for understanding the potential benefits of faricimab in PCV and other retinal diseases10
Notably, faricimab allows for extended dosing intervals, with some patients receiving injections every 16 weeks, thereby reducing the treatment burden associated with more frequent anti-VEGF therapies.11 This extended dosing regimen is particularly beneficial in real-world settings, where adherence to treatment schedules can be challenging.12 Importantly, faricimab has shown promise in patients who are resistant to previous anti-VEGF treatments, especially in eyes with PCV, indicating its potential as a second-line therapy in refractory cases.10,13 The ability to switch to faricimab in treatment-resistant patients has been supported by emerging real-world data, which suggest that many patients can achieve meaningful visual improvements after transitioning from other therapies.5,13
However, the response to faricimab in PCV may vary, as indicated by the heterogeneous responses observed in different populations, particularly in Asian patients where PCV is more prevalent.14 This variability underscores the necessity for further research to optimize treatment protocols and identify patient subgroups that may benefit most from faricimab therapy. Only a limited number of studies have reported outcomes for PCV eyes switched to faricimab and treated with multiple injections over a prolonged period. In this study, titled FAR-PEARL (Switching to Faricimab for Polypoidal Choroidal Vasculopathy with Real-World Evidence and Lasting Efficacy), we report outcomes from a series of 49 Asian eyes with PCV that were switched to faricimab.
Methods
This retrospective study was conducted at OasisEye Specialists between December 2022 and December 2023. Approval was obtained from the institutional ethics committee, and the study adhered to the principles outlined in the Declaration of Helsinki. Patient data were anonymized prior to analysis. Consecutive patients diagnosed with nAMD were identified from a computerized database using ICD-10 codes, and eyes with a sub-diagnosis of PCV were further selected. From this group, eyes that were switched to faricimab during the study period were included in the analysis. Informed consent was obtained from all patients prior to receiving injections, and they also provided permission for their data to be used in future research.
Data were collected from all participants at baseline and during all follow-up visits, including information on age, gender, diagnosis, and treatment parameters before switching (name and number of previous injections). The time interval between the last injection and the first faricimab injection, as well as the dates and intervals of faricimab injections during follow-up, were also recorded. Visual acuity was measured using Snellen charts and converted to the logarithm of the minimal angle of resolution (logMAR) for analysis. Optical coherence tomography (OCT) scans were performed at each visit using the SD-OCT (Topcon, Japan). Parameters analyzed included central foveal thickness, and the presence of subretinal fluid (SRF), intraretinal fluid (IRF), pigment epithelial detachment (PED), and subretinal hyperreflective material (SHRM). Following the first faricimab injection, SRF, IRF, PED, and SHRM were assessed at each visit and categorized as absent, resolved, reduced, stable, or increased.
Faricimab was reinjected on a pro-re-nata (PRN) basis from baseline. Patients were advised to follow up every month, and reinjections were administered if there was SRF and/or IRF, fresh haemorrhage at the macula or vision had dropped by 1 line. Follow-up duration was defined as the time interval from the first faricimab injection to the most recent recorded visit or injection during the study period. For the analysis, eyes were categorized based on the interval between the prior anti-VEGF injection and the first faricimab dose: those with an interval exceeding 180 days (quiescent phase) were considered recurrent cases; those with an interval of 60 to 180 days were classified as the “suboptimal extension group”; and those requiring the first faricimab within 60 days of the previous anti-VEGF were classified as having recalcitrant disease. In this retrospective analysis, a loading dose was defined as receiving three consecutive faricimab injections, each separated by no more than 45 days. The average interval between injections was determined by calculating the mean of all intervals between successive injections.
Statistical Analysis
Continuous variables were presented as mean with standard deviation or median with interquartile range (IQR), while categorical variables were summarized as proportions (n, %). Differences in continuous variables between the two groups were analyzed using the Student’s t-test or Wilcoxon rank-sum test for non-parametric distributions. For comparisons across three groups, analysis of variance (ANOVA) or the Kruskal–Wallis test was employed to identify statistically significant differences. Differences in categorical variables were evaluated using the chi-square test or Fisher’s exact test, as applicable. Comparison between values before and at different time points after treatment were compared using the ANOVA with Bonferroni’s adjustment.
Survival analysis was used to assess the time interval between injections (drug durability) and time to injection-free status, defined as no injections over the next 90 days, and was expressed using cumulative proportions with 95% confidence intervals (CI) and Kaplan–Meier curves. Linear regression analysis was used to analyse the factors that could predict intervals between the first and second dose of faricimab, and outputs were expressed as beta coefficients with their 95% CI. Regression diagnostics, including variance inflations, were checked, leverage points were identified, if any, and the best-fit multivariable model was selected using the Akaike Information Criterion.
All data was entered in Microsoft Excel and analysed using STATA 12.1 I/c (Stata Corp, Fort Worth, Texas, USA). All p values < 0.05 were considered statistically significant.
Results
We included 49 eyes of 49 patients with PCV in this study with a mean age of 66.1 ± 9.5 years, and 29 were women (59%). Among the 49 cases, 14 (29%) were categorized as recurrent disease, with a mean interval of 288 days since the previous anti-VEGF injection. Suboptimal extension was observed in 18 cases (37%), with a mean interval of 96 days, while 17 cases (34%) were classified as recalcitrant disease, with a mean interval of 39 days from the prior anti-VEGF injection (Table 1). Patients had received eight previous anti-VEGF agents on average before switching to faricimab, the majority being aflibercept (Table 1), and there were no treatment – naïve eyes in this cohort.
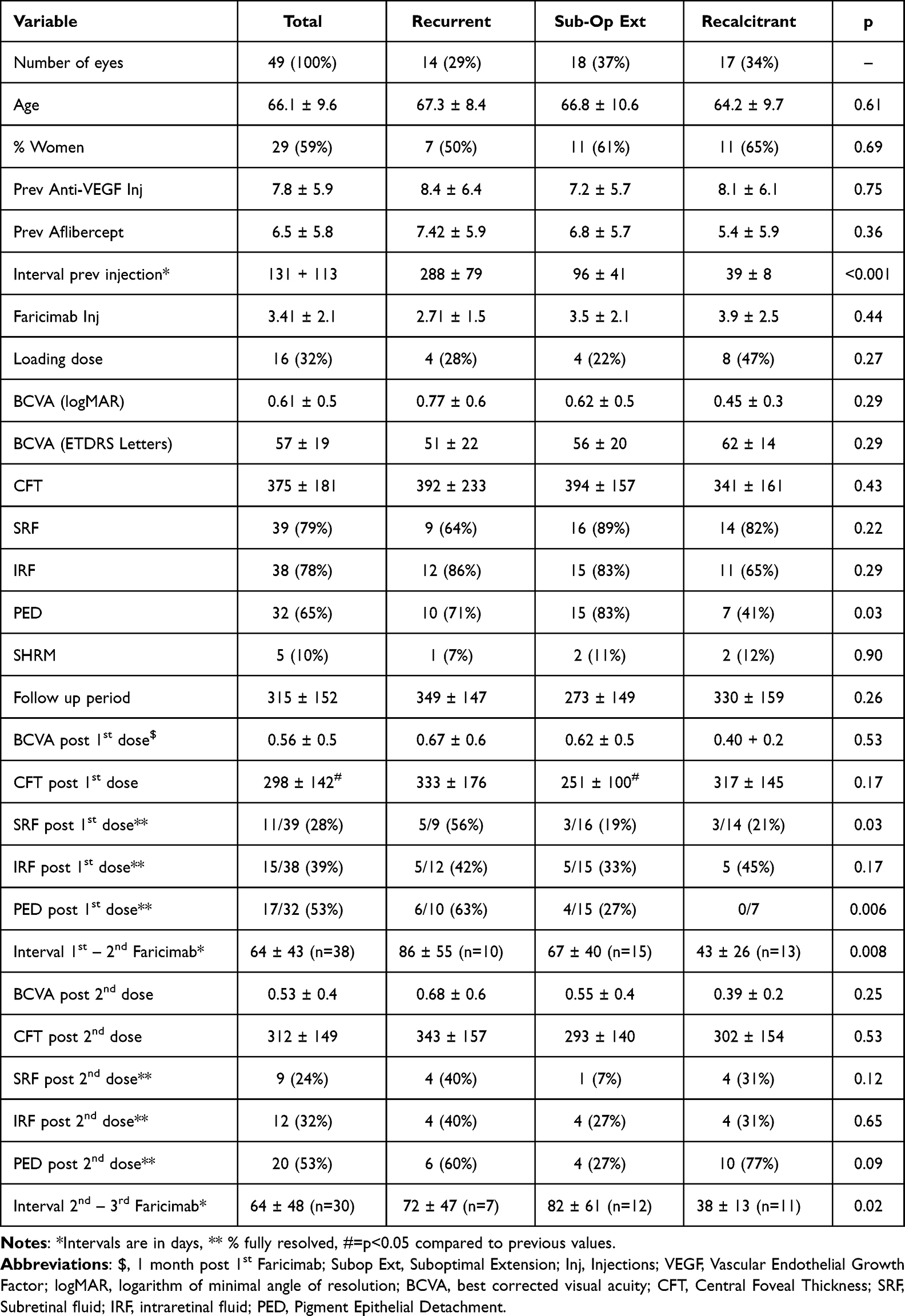 |
Table 1 Baseline Characteristics of All Patients Along with Comparison Across Recurrent, Suboptimal Extension and Recalcitrant Groups |
Overall, patients received a median of 3 faricimab injections (IQR=2-4, range=1-8) over a median follow-up period of 344 days (IQR=198-446, range=40-574 days). A loading dose was used in 16 eyes (32%), half of which were in the recalcitrant group (Table 1). The baseline visual acuity was in the range of 20/60 Snellen’s equivalent with slightly worse vision in the recurrent group compared to the others, though this was not statistically significant (Table 1). Significantly more eyes in the recurrent and suboptimal extension groups had a PED when switching to faricimab compared to the recalcitrant eyes, though the proportions of SRF, IRF and SHRM were similar across groups (Table 1).
The mean BCVA improved marginally at 1 month following the first injection of faricimab; however, this improvement was not statistically significant (p=0.11) overall or within any of the three groups. While the reduction in CFT after the first injection was statistically significant only in the suboptimal extension group (p=0.003), the recurrent PCV group showed the most favourable structural outcomes, with significantly higher rates of complete PED resolution and absence of SRF (Table 1). However, all eyes showed reduced PED size and SRF. This response was also maintained for longer periods in the recurrent group, which showed longer intervals between the first and second injections than the others (Table 1). These trends were similar after the second dose of faricimab across groups (Table 1).
Table 2 compares eyes that received injections ranging from one to eight over the study period. The interval between injections (Figure 1) remained relatively similar for the first four injections and then increased from the fifth dose onwards, though the proportion of eyes requiring subsequent injections kept reducing at every injection time-point such that 18% of eyes did not need a second injection, and an additional 8% did not need a third injection (Table 2). The CFT also reduced with subsequent injections in the eyes where repeat injections were indicated, and the proportion of eyes with persistent SRF, IRF, and PED also reduced with every subsequent injection. The peak effect was seen after the fourth dose (at the time of the fifth dose), where the interval between injections had increased significantly by two weeks (Figure 2), the CFT was normal, and none of the eyes had SRF, IRF and PED (Table 2). Survival analysis showed that the cumulative proportion of eyes that could be injection-free after day 60 was 36% (24–52%) and increased to 49% (35–65%) by day 90 and 73% (58–87%) were without injections by day 210 (Figure 3). The interval between the first and second faricimab injection (Figure 4) as well as the average injection interval was highest in the recurrent PCV group and least in the recalcitrant group.
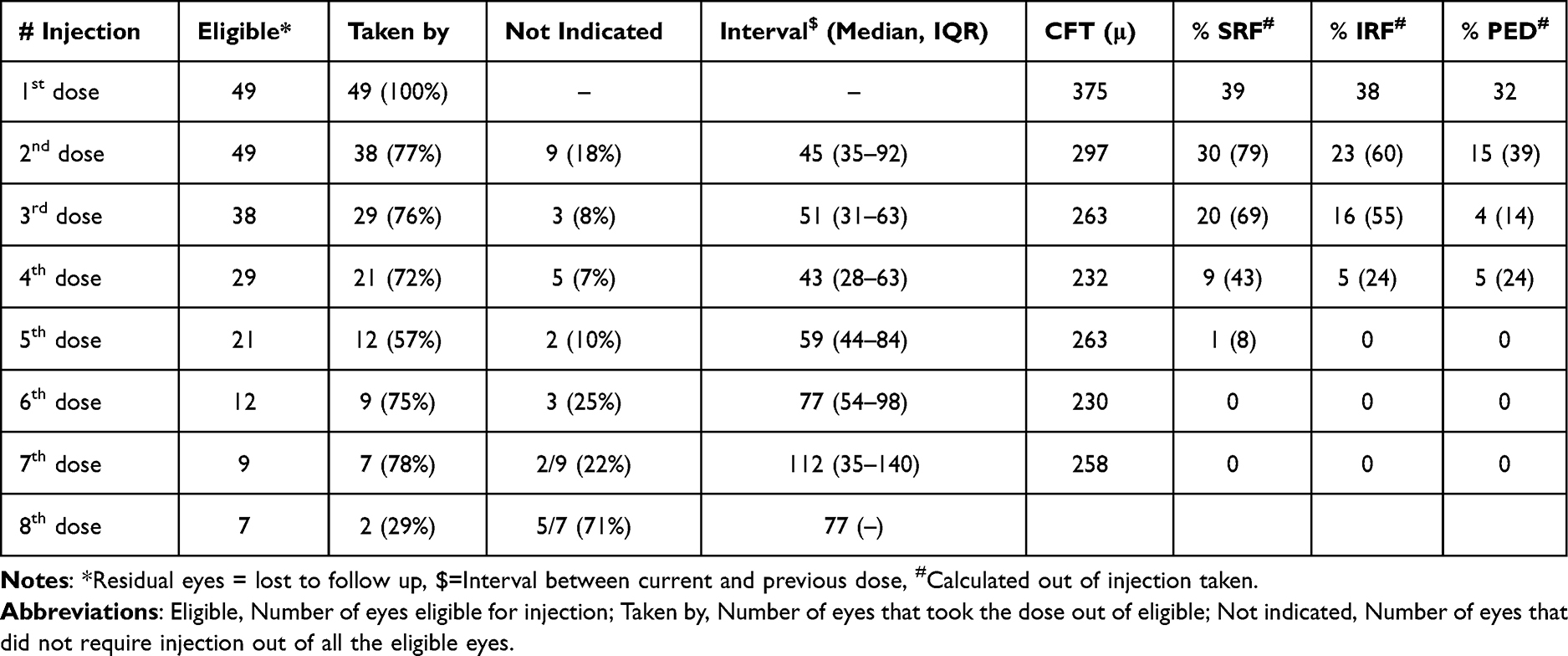 |
Table 2 Comparison of Eyes with Respect to the Number of Injections Taken |
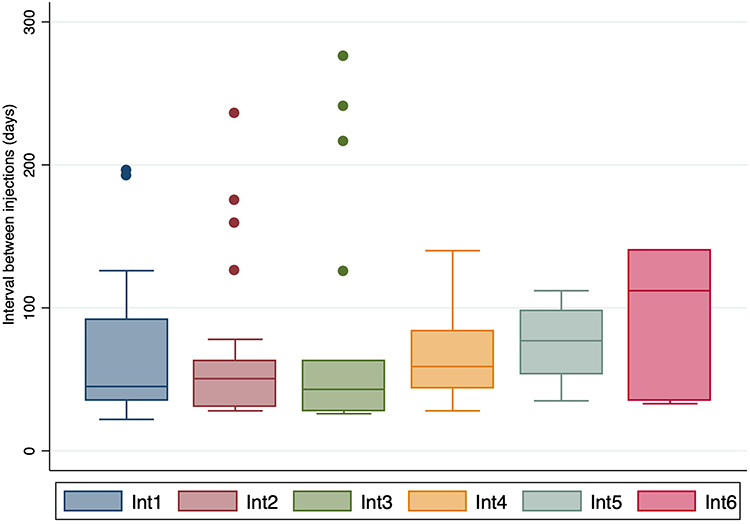 |
Figure 1 Box and whisker plot showing increasing intervals between subsequent faricimab injections. |
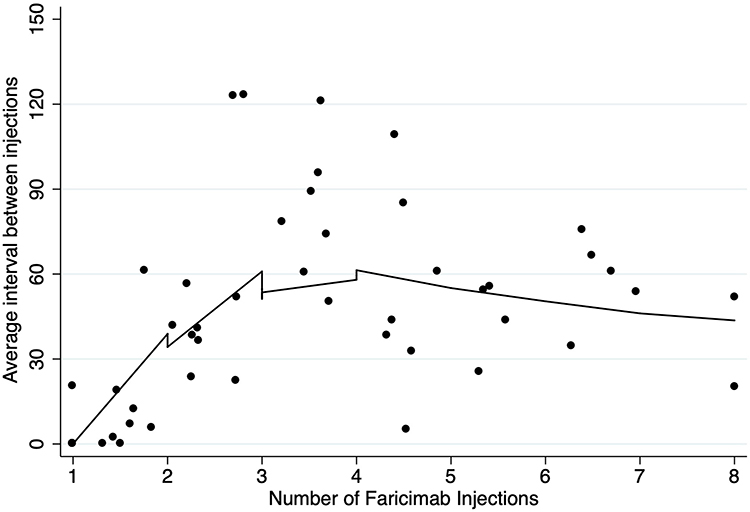 |
Figure 2 Scatter plot with locally weighted curve showing relationship between average injection interval and number of injections. |
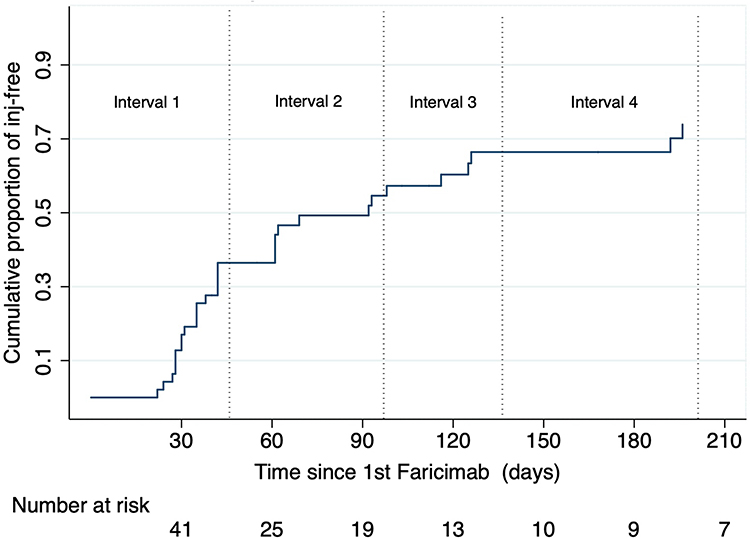 |
Figure 3 Survival analysis showing time to injection-free status after the first injection. |
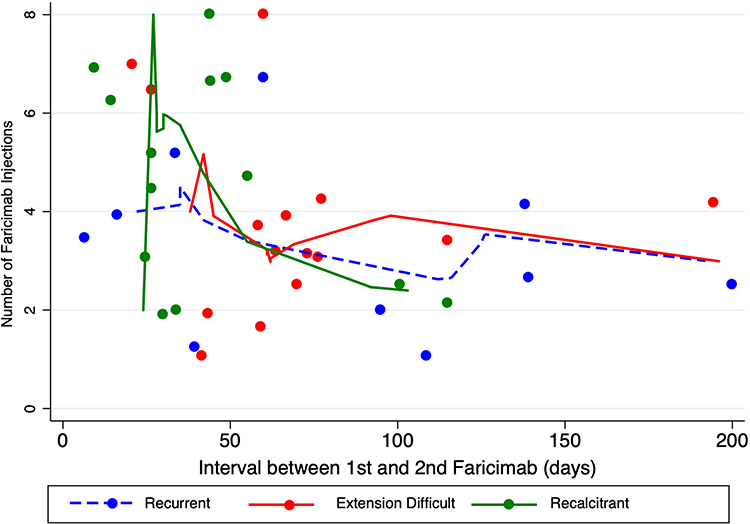 |
Figure 4 Scatter plot with locally weighted curve showing relationship between number of injections and interval between the first and second dose in the three subgroups of PCV. |
Factors predicting the interval between the first and second injections were evaluated using univariate and multivariable linear regression analysis (Table 3). After adjusting for covariates, eyes in the recalcitrant group required the second injection 52 days earlier than those in the recurrent group (p=0.008). Additionally, faricimab lasted 18 fewer days in the suboptimal extension group compared to recurrent PCV eyes, though this difference was not statistically significant (p=0.09). Baseline BCVA also showed a notable effect size, with each one-line decrease in baseline vision associated with a 35-day shorter duration of faricimab’s effect; however, this finding only approached marginal significance (p=0.09). Based on the multivariable model, we found an equation to predict the durability of the first faricimab after switching in eyes with PCV (Table 3, footer), based on the reason to switch, age and baseline BCVA. Additionally, survival analysis (Figure 5) also showed that the interval between the first and second faricimab was significantly shorter in the recalcitrant eyes, with 50% eyes requiring the second injection by day 30, compared to day 60 in suboptimal extension eyes, and day 122 in recurrent PCV eyes (log-rank p = 0.023).
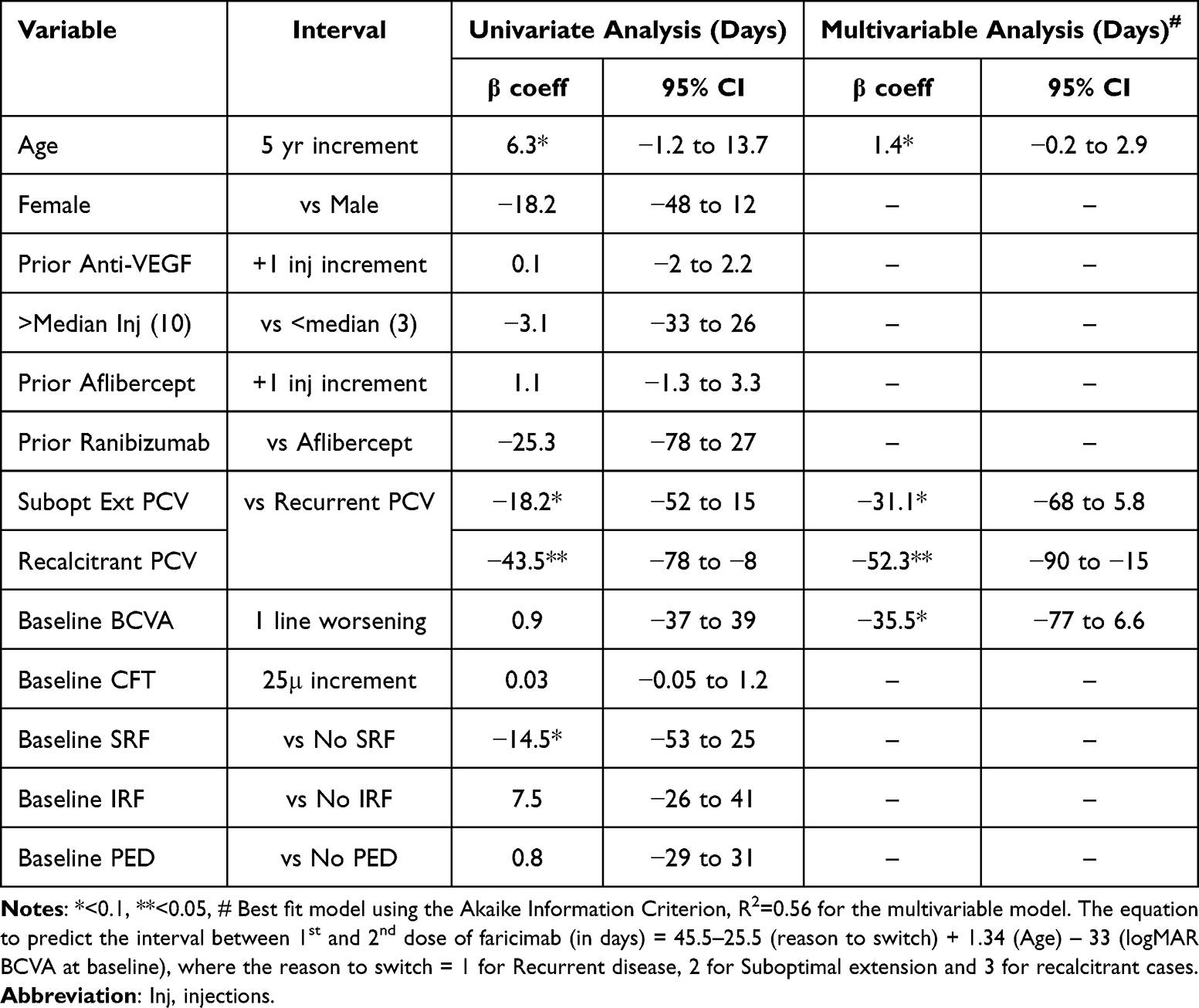 |
Table 3 Univariate and Multivariable Linear Regression Analysis to Find Predictors of the Interval Between the First and second Faricimab Injections |
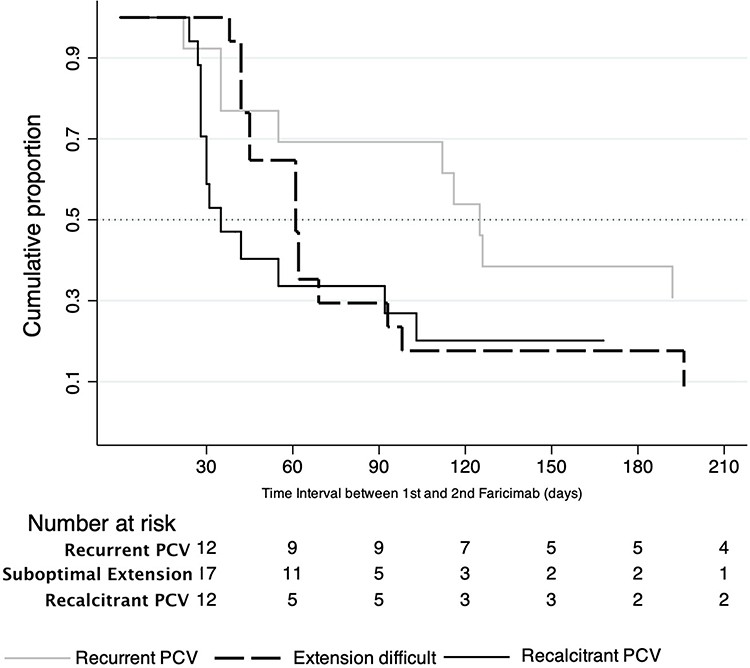 |
Figure 5 Survival analysis showing time to time interval between the first and second injection in the three subgroups of PCV. |
Discussion
In this retrospective study of 49 eyes with PCV switched to faricimab after having taken about seven injections of aflibercept, we found that the majority of eyes showed a favourable response to faricimab with fewer overall injections over a one-year period. The durability of the first injection differed based on the reason to switch, with the recalcitrant disease having the shortest interval between the first and second doses of about 5–6 weeks, similar to their aflibercept regimens, compared to more extended durability in the suboptimal extension and recurrent PCV eyes. However, the need for subsequent injections decreased significantly after each injection, with nearly half of the patients remaining injection-free after day 90. The peak effect was seen after four initial doses, where durability increased by two weeks, and all eyes were dry of fluid by about four and half months of switching. The durability of the first injection was also influenced by baseline visual acuity, even after adjusting for recalcitrant vs recurrent disease, with every one-line worse baseline vision having a 30-day shorter durability, though this was only marginally significant.
The differential response to faricimab after switching from aflibercept in patients with nAMD and PCV can be influenced by whether the underlying disease is recurrent or recalcitrant. Understanding these distinctions is crucial for optimizing treatment strategies and improving patient outcomes. Recurrent disease typically refers to cases where patients experience a return of symptoms or fluid accumulation after an initial positive response to anti-VEGF treatment, and they usually have a more extended period of quiescence between the previous anti-VEGF and the first faricimab. In contrast, recalcitrant disease describes cases where patients do not respond adequately to treatment despite ongoing therapy. Previous studies have shown that patients with recurrent disease may benefit significantly from switching to faricimab. Schneider et al recently reported that, out of 50 eyes with nAMD who switched from aflibercept to faricimab, approximately one-third of patients achieved complete resolution of IRF and SRF after just one injection, suggesting a favourable response in recurrent cases.15 We found this in about 18% of eyes with PCV who did not need repeat injections after the first dose. This aligns with findings from the TRUCKEE study, which reported similar outcomes in both treatment-naïve and switched patients, showing faricimab’s potential effectiveness in managing recurrent disease.5
In recalcitrant cases where patients show inadequate response to ongoing aflibercept therapy despite frequent injections, the response to faricimab tends to be more variable. This variability may stem from advanced disease stages and the cumulative effects of prior treatments, which can result in irreversible retinal damage and diminish the efficacy of subsequent therapies. While some studies suggest that switching to faricimab can improve visual acuity and central macular thickness, the overall response in these cases is often less predictable compared to recurrent cases, as reflected in our findings. Ibrahim et al reported on 32 Asian eyes with recalcitrant PCV that had received a median of 21 aflibercept injections at six-week intervals before switching to faricimab.14 The patients in their study closely resembled our cohort in terms of ethnicity, baseline vision, and OCT characteristics. They observed significant reductions in CMT, macular volume, and PED height, with stable vision at one-month post-switch. However, the study’s prospective design was limited by the lack of long-term outcome data and results beyond the initial faricimab injection. In a meta-analysis of faricimab for PCV, Arnold-Vangsted et al identified only two studies involving patients switched from other anti-VEGF therapies to faricimab.16 They reported that 57–67% of switch-over eyes experienced fluid reduction, and 21% achieved extended treatment interval, findings consistent with our results. However, the studies included in the meta-analysis were also limited to outcomes following one or two injections, whereas our cohort received a median of three injections over a one-year follow-up, providing a more comprehensive perspective on treatment efficacy. Taken together, these observations suggest that treatment history, disease chronicity, and baseline anatomical features likely play pivotal roles in modulating the response to faricimab. The differing patterns of responsiveness across subgroups may not only reflect variations in disease biology but also the cumulative impact of prior therapy. Our findings underscore the importance of phenotyping PCV patients more precisely before switching treatments and highlight the need for prospective, multicenter studies with predefined subgroup stratifications to better understand the long-term efficacy of faricimab in varied clinical scenarios.
Among patients who continued to receive repeated injections, significant extension of retreatment intervals and complete retinal drying were observed only after the fourth faricimab injection, consistent with findings from clinical trials despite the use of real-world PRN protocols from the outset in our study. Yet, achieving an injection-free interval of three consecutive months is a key goal for patients, and faricimab enabled this for half the cohort after day 90, by which time most had received approximately three injections. Therefore, it may be reasonable to counsel patients on the need for an initial three-dose regimen with aggressive management, particularly in cases involving switched eyes with PCV.
The equation we provide can serve as an interval calculator to guide the timing of the second faricimab injection: Interval, in days, between 1st and 2nd dose of faricimab = 45.5–25.5 (phenotype) + 1.34 (Age) - 33 (logMAR BCVA at baseline), where phenotype is assigned as follows: 1 for recurrent disease, 2 for suboptimal extension, and 3 for recalcitrant cases. This equation, based on goodness of fit statistical modelling and relatively good reliability (R2=0.56) can assist physicians in determining the timing of the second injection and potentially predict reinjection intervals at subsequent time points. The equation incorporates baseline phenotype, age, and baseline visual acuity, with shorter intervals suggested for recalcitrant cases and eyes with poorer baseline vision. However, despite the predictive model being reasonably strong, we caution against overinterpretation given the modest sample size and retrospective design. Future studies with larger, prospective, and multicentric cohorts are necessary to validate the model’s reliability and determine its applicability in routine clinical settings.
This study has several limitations inherent to its retrospective, single-center design. As the analysis was conducted at a tertiary eye care center in Malaysia with an exclusively Asian cohort, the findings may not be fully generalizable to other ethnic or geographic populations. The lack of masked or independent graders for assessing anatomical biomarkers such as SRF, IRF, PED, and SHRM introduces a potential source of observer bias, although efforts were made to standardize data collection based on case file documentation and imaging. Additionally, while the cohort was well-characterized, the relatively modest sample size may limit the power of subgroup analyses. Lastly, the predictive model proposed, though novel, should be interpreted with caution until validated by larger prospective studies. However, its strengths lie in reporting outcomes from repeated faricimab injections over one year in Asian eyes with PCV. To the best of our knowledge, this represents the largest series of PCV eyes switched predominantly from aflibercept to faricimab, with most cases receiving repeated injections over a one-year period.
Conclusion
In summary, the differential response to faricimab after switching from aflibercept in patients with nAMD and PCV is influenced by the nature of the underlying disease—recurrent versus recalcitrant, with suboptimal extension being in between these extremes. Patients with recurrent disease tend to experience more favorable outcomes with fewer injections and more intervals between injections, while those with recalcitrant disease may require more intensive management in the beginning and may not respond as effectively due to treatment history and potential pre-existent retinal damage. However, even in recalcitrant eyes, it is possible to extend intervals following the initial loading doses.
Importantly, while significant anatomical improvements were observed, functional gains in BCVA were modest, with most patients maintaining stable vision or gaining up to one line of improvement. This highlights the potential of faricimab to stabilize disease even in previously refractory cases. Given the single-center nature of this study and its exclusively Asian cohort, where PCV prevalence is higher, these findings may not fully generalize to other populations. Nevertheless, the classification of PCV eyes into these three phenotypes and use of the proposed regression model may help guide expectations and management strategies. Further large-scale, multiethnic prospective studies are essential to validate these findings and refine individualized treatment protocols for PCV.
Acknowledgment
The authors gratefully acknowledge Roche (Malaysia) Sdn Bhd for providing financial support for medical writing and publication. We also sincerely thank Dr. Dr Sabyasachi Sengupta (India) for his guidance and valuable contributions to the preparation of this manuscript.
Portions of the data and findings reported in this manuscript were previously presented, in part, at the Malaysian Ophthalmology Scientific Congress (MOSC), held in Kuala Lumpur from 25 to 27 April 2025.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sen P, Manayath G, Shroff D, Salloju V, Dhar P. Polypoidal choroidal vasculopathy: an update on diagnosis and treatment. Clin Ophthalmol. 2023;17:53–70. doi:10.2147/OPTH.S385827
2. Wang L, Liu S, He T, Liu C, Duan J. Efficacy of intravitreal anti-VEGF agents in neovascular age-related macular degeneration patients with or without polypoidal choroidal vasculopathy: a meta-analysis. Br J Hosp Med. 2025;86(2):1–22. doi:10.12968/hmed.2024.1013
3. Allehyani MH, Alsaeedi AK, Alqthmi RO, et al. Comparative efficacy of brolucizumab and aflibercept in polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Cureus. 2025;17(1):e77073. doi:10.7759/cureus.77073
4. Downey L, Sivaprasad S, Chhabra R, et al. Dual pathway inhibition with faricimab for previously treated neovascular age-related macular degeneration and diabetic macular oedema: guidance from a UK panel of retina specialists. Eye. 2024;38(16):3077–3086. doi:10.1038/s41433-024-03223-w
5. Khanani AM. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the TRUCKEE study – 6 month results. Eye. 2023;37(17):3574–3581. doi:10.1038/s41433-023-02553-5
6. Panos G. Faricimab: transforming the future of macular diseases treatment - A comprehensive review of clinical studies. Drug Des Devel Ther. 2023;17:2861–2873. doi:10.2147/DDDT.S427416
7. Leung EH, Oh DJ, Alderson SE, et al. Initial real-world experience with faricimab in treatment-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:1287–1293. doi:10.2147/OPTH.S409822
8. Khanani AM, Kotecha A, Chang A, et al. TENAYA and LUCERNE: two-year results from the phase 3 neovascular age-related macular degeneration trials of faricimab with treat-and-extend dosing in year 2. Ophthalmology. 2024;131(8):914–926. doi:10.1016/j.ophtha.2024.02.014
9. Cheung G, Chen SJ, Iida T, et al.
10. Fujimoto S, Kokame GT. Response to faricimab for anti-vascular endothelial growth factor resistant eyes with neovascular age-related macular degeneration. Research Square; 2023. Available from: https://www.researchsquare.com/article/rs-2715544/v1.
11. Larsen H, Grauslund J, Vergmann AS. Efficacy, durability and safety of faricimab in neovascular age-related macular degeneration and diabetic macular oedema: lessons learned from registration trials. Ophthalmol Ther. 2023;12(5):2253–2264. doi:10.1007/s40123-023-00753-6
12. Kelkar A, Webers C, Shetty R, et al. Factors affecting compliance to intravitreal anti-vascular endothelial growth factor therapy in Indian patients with retinal vein occlusion, age-related macular degeneration, and diabetic macular edema. Indian J Ophthalmol. 2020;68(10):2143. doi:10.4103/ijo.IJO_1866_19
13. Ng B, Kolli H, Ajith Kumar N, et al. Real-world data on faricimab switching in treatment-refractory neovascular age-related macular degeneration. Life. 2024;14(2). doi:10.3390/life14020193
14. Ibrahim FNI, Teo KYC, Tan TE, Chan HH. Initial experiences of switching to faricimab for neovascular age-related macular degeneration and polypoidal choroidal vasculopathy in an Asian population. Front Ophthalmol. 2024;11(3):1346322. doi:10.3389/fopht.2023.1346322
15. Schneider M, Bjerager J, Hodzic-Hadzibegovic D, Klefter ON, Subhi Y, Hajari J. Short-term outcomes of treatment switch to faricimab in patients with aflibercept-resistant neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2024;262(7):2153–2162. doi:10.1007/s00417-024-06421-0
16. Arnold-Vangsted A, Schou MG, Balaratnasingam C, et al. Efficacy of intravitreal faricimab therapy for polypoidal choroidal vasculopathy: a systematic review and meta-analysis. Acta Ophthalmol. 2025;103(3):247–256. doi:10.1111/aos.16797
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.