Back to Journals » International Medical Case Reports Journal » Volume 19
Suspected Mast Cell Activation Mimicking Heart Failure Exacerbation and Abdominal-Wall Cellulitis in a Resource-Limited Setting: A Case Report
Authors Tahajud OA ![]() , Elmi AH
, Elmi AH ![]() , Hussein AM
, Hussein AM
Received 26 February 2026
Accepted for publication 9 April 2026
Published 13 April 2026 Volume 2026:19 605332
DOI https://doi.org/10.2147/IMCRJ.S605332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Osman Ahmed Tahajud,1 Abdullahi Hassan Elmi,2 Abdiwali Mohamed Hussein1
1Department of Internal Medicine, Dr. Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Nursing and Midwifery, Dr. Sumait Hospitals, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia
Correspondence: Osman Ahmed Tahajud, Email [email protected]
Introduction: Mast cell activation syndrome (MCAS) is a mediator-driven disorder characterized by episodic, multisystem symptoms that can resemble common cardiopulmonary and infectious conditions. Diagnostic confirmation often relies on demonstration of mast cell mediator release (eg, event-related serum tryptase rise) and clinical response to anti-mediator therapy; however, access to specialized testing may be limited in low-resource settings.
Case Presentation: A 75-year-old woman with recently diagnosed heart failure with reduced ejection fraction (HFrEF) presented with seven days of diffuse edema, severe pruritus with abdominal-wall erythema and thickening, wheezing and dyspnea, and nausea with vomiting. Symptoms began one day after ingestion of an unspecified herbal preparation. She was afebrile and hemodynamically stable Laboratory evaluation showed elevated total IgE (634 IU/mL) with normal C-reactive protein and no leukocytosis. Imaging demonstrated cardiomegaly with a small right pleural effusion and diffuse abdominal-wall edema without abscess. Although cellulitis and heart failure exacerbation were initially considered, the combination of multisystem involvement, lack of infectious features, and recent trigger exposure supported a suspected mast-cell–mediated reaction, with MCAS considered in the differential diagnosis. Because detailed long-term symptom history and confirmatory mediator testing were unavailable, definitive diagnosis of MCAS could not be established. Serum tryptase and urinary mediator assays were unavailable. She was treated with cetirizine, famotidine, and montelukast while continuing guideline-directed heart failure therapy and receiving low-dose diuresis; antibiotics were withheld. Symptoms resolved rapidly, and she remained asymptomatic at four-week follow-up.
Conclusion: This case highlights that acute mast-cell–mediated reactions may mimic heart failure exacerbation and cellulitis, particularly when cutaneous, respiratory, and gastrointestinal manifestations occur together after a potential trigger. In low-resource settings, careful exclusion of infection and true cardiogenic worsening, combined with close assessment of therapeutic response, may help guide management. However, in the absence of recurrent episodes and confirmatory mediator testing, a definitive diagnosis of MCAS should be made cautiously.
Keywords: Somalia, mast cell activation syndrome, HFrEF, cellulitis mimic, urticaria, wheeze, low-resource setting, antihistamines, leukotriene receptor antagonist
Introduction
Mast cells are tissue-resident immune cells that play a central role in immediate hypersensitivity and host defense by releasing potent mediators, including histamine, leukotrienes, prostaglandins, and proteases. Dysregulated mast cell activation can lead to a broad spectrum of clinical disorders, ranging from primary clonal diseases (eg, systemic mastocytosis) to secondary activation and idiopathic presentations.1 To standardize terminology and guide clinical decision-making, international experts have proposed consensus definitions and a global classification framework for mast cell disorders, with specific attention to mast cell activation syndromes.1
Mast cell activation syndrome (MCAS) refers to recurrent, episodic symptoms attributable to mast cell mediator release affecting one or more organ systems, most commonly the skin, gastrointestinal tract, cardiovascular system, and respiratory tract.2,3 The clinical phenotype can be highly variable, leading to frequent under-recognition and misattribution to more common conditions, particularly when presentations overlap with cardiopulmonary decompensation, allergic disease, infection, or inflammatory dermatoses.3 Diagnostic evaluation is ideally supported by objective evidence of mediator release (such as a rise in serum tryptase during episodes) together with symptom improvement on anti–mast cell mediator therapy (eg, H1/H2 blockade and leukotriene pathway inhibition)1,2 In practice, however, access to confirmatory testing may be limited, especially in low-resource settings, making careful clinical reasoning and pattern recognition essential.4
Consensus-based diagnostic frameworks generally consider MCAS when recurrent episodic symptoms involve at least two organ systems, objective evidence of mast cell mediator release is demonstrated, and symptoms improve with anti-mediator therapy. Although the true prevalence of MCAS remains uncertain, the condition is likely under-recognized because its manifestations often overlap with more common allergic, infectious, dermatologic, and cardiopulmonary disorders. Reported triggers include medications, foods, supplements, herbal preparations, environmental exposures, and infections. Clinically, mast cell activation disorders may be classified as primary (clonal), secondary, or idiopathic, depending on the underlying mechanism.2,4
Because MCAS may present with edema, dyspnea, wheeze, flushing or urticaria-like skin findings, abdominal symptoms, and systemic discomfort, it can closely resemble heart failure exacerbation, cellulitis, or other infectious processes.3,4 Recognizing MCAS in such contexts has important implications: it can prevent unnecessary antibiotic exposure, facilitate rapid symptom control with targeted therapy, and prompt counseling regarding potential triggers.1,4 We report a case of suspected MCAS triggered by ingestion of an herbal preparation in a patient with established HFrEF, initially mimicking both heart failure decompensation and abdominal-wall cellulitis, highlighting practical diagnostic considerations when advanced mediator assays are unavailable.
Case Presentation
A 75-year-old woman with a two-month history of heart failure with reduced ejection fraction (HFrEF) presented with seven days of diffuse swelling, intense pruritus (most prominent over the abdominal wall), dry cough, dyspnea, wheeze, and nausea with vomiting. She reported taking an unspecified herbal preparation one day before the onset of symptoms. She had no clearly documented prior history of recurrent flushing, urticaria, unexplained wheezing, episodic gastrointestinal symptoms, or similar multisystem reactions in childhood or adulthood. There was no known history of chronic allergic or inflammatory disease, and no recent viral illness was identified based on the available clinical history. However, detailed long-term allergy history was limited, which should be considered when interpreting the diagnostic possibility of MCAS. Before this episode, her heart failure symptoms were well controlled on guideline-directed therapy (candesartan, dapagliflozin, and spironolactone).
On arrival, she appeared unwell but was afebrile and hemodynamically stable Respiratory examination showed widespread bilateral expiratory wheeze without inspiratory crackles. Abdominal examination revealed diffuse abdominal-wall thickening with erythema, mild tenderness, and marked pruritus, features more consistent with an urticarial process than a localized soft-tissue infection. Mild bilateral pitting edema was noted in the lower extremities.
Laboratory testing demonstrated mild anemia, a normal total white blood cell count with a slight relative monocytosis, and an elevated total IgE level of 634 IU/mL. C-reactive protein was within the normal range (6 mg/L). Thyroid-stimulating hormone was mildly increased (7 mIU/L) with normal free T3 and free T4. Renal and hepatic function tests were unremarkable. Chest radiography showed cardiomegaly with a small right-sided pleural effusion (Figure 1). Abdominal ultrasonography identified diffuse subcutaneous edema and abdominal-wall thickening without a focal collection or abscess (Figure 2); these findings were initially interpreted as possible cellulitis.
 |
Figure 1 Chest X-ray shows cardiomegaly (enlarged cardiac silhouette) along with a right-sided pleural effusion. |
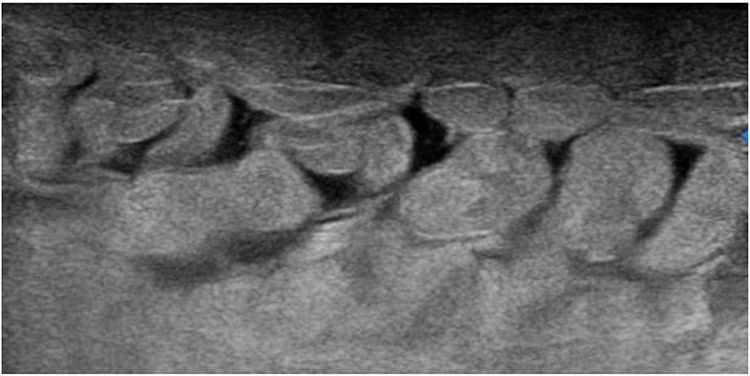 |
Figure 2 Abdominal ultrasound showing swelling and fluid buildup in the soft tissues of the abdominal wall. The fluid appears as dark (hypoechoic) areas between the fat layers, creating a cobblestone-like pattern that can closely resemble cellulitis. |
However, the combination of multisystem involvement (cutaneous, respiratory, and gastrointestinal symptoms), recent exposure to a potential trigger, elevated IgE, normal inflammatory markers, absence of fever, and no imaging evidence of a focal infection supported a clinical diagnosis of mast cell activation syndrome (MCAS). Confirmatory testing (serum tryptase and urinary mast cell mediator assays) was not available in this low-resource setting.
The patient was admitted for four days and treated with cetirizine (H1 antagonist), famotidine (H2 antagonist), and montelukast, while her baseline heart failure regimen was continued, and low-dose furosemide was given. Antibiotics were not initiated due to low suspicion of infection. She improved rapidly during hospitalization: pruritus and abdominal erythema resolved completely, wheezing disappeared, and gastrointestinal symptoms abated. She was discharged in stable condition on day 4 and advised to continue cetirizine and famotidine for one month. At four-week follow-up, she remained symptom-free, reported high satisfaction with her recovery, and her heart failure status was stable without recurrence.
Timeline
Day −1: Ingestion of herbal medication
Day 0: Onset of pruritus, edema, dyspnea, and gastrointestinal symptoms
Day 7: Hospital admission
Days 1–4 (inpatient): Cetirizine + famotidine + montelukast → rapid clinical improvement
Day 4: Discharged home
4 weeks: Asymptomatic at outpatient follow-up
Discussion
This case illustrates how an acute mast-cell–mediated reaction can mimic both heart failure decompensation and cellulitis, particularly in a patient with pre-existing cardiopulmonary disease. Mast cells are key effector cells in allergy and inflammation, and inappropriate mediator release (eg, histamine, leukotrienes, prostaglandins, and proteases) can produce systemic symptoms involving the skin, respiratory tract, gastrointestinal system, and cardiovascular system5 International consensus work has clarified that mast cell activation disorders encompass clonal mast cell disease, secondary mast cell activation, and idiopathic syndromes, and has proposed diagnostic criteria specifically for mast cell activation syndromes.1
In our patient, symptom onset closely followed ingestion of an herbal preparation and was characterized by simultaneous cutaneous (diffuse abdominal-wall erythema with intense pruritus and swelling), respiratory (wheezing and dyspnea), and gastrointestinal (nausea and vomiting) involvement. This multisystem pattern is typical of mast cell mediator release and is repeatedly emphasized in the clinical literature as a major reason MCAS is frequently overlooked or misdiagnosed.2,3 The abdominal-wall findings were initially interpreted as possible cellulitis on ultrasonography; however, the absence of fever, normal inflammatory markers, normal total leukocyte count, lack of focal collection or abscess, and prominent pruritus favored an urticaria-like process rather than bacterial infection.3,4 Recognizing this distinction is clinically important because MCAS-related swelling and erythema can resemble soft-tissue infection, yet inappropriate antibiotic exposure can be avoided when the overall picture is inconsistent with infection.4
This is particularly important in resource-limited settings, where overlapping clinical presentations may increase the risk of diagnostic anchoring toward more familiar conditions such as cellulitis or heart failure exacerbation. Failure to recognize a mast-cell–mediated process may lead to unnecessary antibiotic use, delayed targeted therapy, and avoidable healthcare burden.4
MCAS is ideally diagnosed using a combination of compatible episodic symptoms affecting at least two organ systems, objective evidence of mediator release (most commonly an event-related rise in serum tryptase), and clinical improvement with anti-mediator therapy.1,2 In this low-resource setting, serum tryptase and urinary mediator assays were unavailable, representing a key limitation. In addition, the present episode was isolated rather than clearly recurrent, which reduces confidence in a formal diagnosis of MCAS. Neither baseline nor event-related serum tryptase measurements were available, and urinary mast cell mediator studies could not be performed. As a result, objective confirmation of mast cell mediator release was not possible, and the diagnosis of MCAS could not be established definitively1,2 Nonetheless, practical guidance acknowledges that access to confirmatory testing is variable and that clinicians may need to rely on careful clinical assessment and therapeutic response while excluding other urgent conditions.4 In our case, The rapid clinical improvement after initiation of anti-mediator therapy supported the possibility of a mast-cell–mediated process; however, this response should be interpreted cautiously, as it is not specific to MCAS and may also occur in other allergic or hypersensitivity reactions.1,4,6
The patient’s known HFrEF increased the risk of anchoring on heart failure exacerbation as the primary diagnosis. However, wheezing without inspiratory crackles, marked pruritus, prominent gastrointestinal symptoms, normal inflammatory markers, and a clear temporal association with a new exposure suggested MCAS as a unifying explanation. Mast cell mediators can cause bronchospasm and increased vascular permeability, potentially contributing to dyspnea and edema that resemble cardiogenic congestion.5 The clinical course further supported MCAS; symptoms improved dramatically despite continuation of baseline guideline-directed heart failure therapy and only low-dose diuresis, and there was no recurrence at four weeks.
Trigger identification is not always possible in MCAS, but medications, foods, and supplements are frequently implicated, and avoidance counseling is a central element of care.2,4,7 The close temporal relationship with the herbal preparation makes it a plausible precipitant in this patient, highlighting the importance of explicitly asking about over-the-counter and traditional remedies.4 Although total IgE elevation is not diagnostic for MCAS, it may coexist with allergic-type phenotypes and does not exclude mast cell activation disorders.2,3 Gastrointestinal symptoms are also well described across mast cell diseases, reinforcing that nausea and vomiting can be part of the mediator-release spectrum rather than a separate primary gastrointestinal pathology.8
Overall, this case reinforces that mast-cell–mediated reactions should be considered in patients presenting with acute multisystem symptoms, especially when cutaneous, respiratory, and gastrointestinal features occur after a possible trigger and when common diagnoses such as infection or heart failure exacerbation do not fully explain the presentation, even when comorbidities such as heart failure make alternative explanations tempting.2–4 Early recognition can prevent unnecessary antibiotics, support prompt symptom relief with targeted anti-mediator therapy, and facilitate trigger counseling and follow-up planning.1,4,6 This report is presented in accordance with CARE guideline principles to enhance transparency and clinical interpretability.7
Conclusion
This case highlights that acute mast-cell–mediated reactions may present with edema, dyspnea, wheeze, and erythematous soft-tissue swelling, closely mimicking heart failure exacerbation and cellulitis. In patients with acute multisystem symptoms, especially when cutaneous, respiratory, and gastrointestinal features occur together after a likely trigger, mast-cell–mediated disease should be considered in the differential diagnosis to reduce misdiagnosis and unnecessary treatment. This is particularly important in resource-limited settings, where limited access to confirmatory testing may require greater reliance on careful clinical assessment, exclusion of infection or true cardiogenic worsening, and close observation of response to therapy. However, in the absence of recurrent episodes and confirmatory mediator testing, definitive diagnosis of MCAS should be made cautiously.
Abbreviations
MCAS, Mast Cell Activation Syndrome; HFrEF, Heart Failure with Reduced Ejection Fraction; IgE, Immunoglobulin E; CRP, C-reactive protein; TSH, Thyroid-stimulating hormone; FT3, Free triiodothyronine; FT4, Free thyroxine; H1, Histamine H1 receptor; H2, Histamine H2 receptor; GI, Gastrointestinal; GDMT, Guideline-Directed Medical Therapy.
Ethics and Consent
Written informed consent was obtained from the patient for publication of this case report and the accompanying images. According to the policy of Dr. Sumait Hospital formal ethics committee approval was not required for publication of a single-patient case report.
Acknowledgments
This study was supported by SIMAD University, Mogadishu, Somalia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Valent P, Akin C, Arock M, et al. Definitions, criteria and global classification of mast cell disorders with special reference to mast cell activation syndromes: a consensus proposal. Int Arch Allergy Immunol. 2012;157(3):215–6. doi:10.1159/000328760
2. Akin C. Mast cell activation syndromes. J Allergy Clin Immunol. 2017;140(2):349–355. doi:10.1016/j.jaci.2017.06.007
3. Afrin LB, Butterfield JH, Raithel M, Molderings GJ. Often seen, rarely recognized: mast cell activation disease--a guide to diagnosis and therapeutic options. Ann Med. 2016;48(3):190–201. doi:10.3109/07853890.2016.1161231
4. Lee E, Picard M. Diagnosis and management of mast cell activation syndrome (MCAS) in Canada: a practical approach. Allergy Asthma Clin Immunol. 2025;21(1):49. doi:10.1186/s13223-025-00998-9
5. Theoharides TC, Kalogeromitros D. The critical role of mast cells in allergy and inflammation. Ann NY Acad Sci. 2006;1088(1):78–99. doi:10.1196/annals.1366.025
6. Castells M, Butterfield J. Mast cell activation syndrome and mastocytosis: initial treatment options and long-term management. J Allergy Clin Immunol Pract. 2019;7(4):1097–1106. doi:10.1016/j.jaip.2019.02.002
7. Gagnier JJ, Kienle G, Altman DG, Moher D, Sox H, Riley D; CARE Group. The CARE guidelines: consensus-based clinical case report guideline development. J Clin Epidemiol. 2014;67(1):46–51. doi:10.1016/j.jclinepi.2013.08.003
8. Elvevi A, Elli EM, Lucà M, et al. Clinical challenge for gastroenterologists-Gastrointestinal manifestations of systemic mastocytosis: a comprehensive review. World J Gastroenterol. 2022;28(29):3767–3779. doi:10.3748/wjg.v28.i29.3767
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.