Back to Journals » International Medical Case Reports Journal » Volume 16
Surviving Fetus from a Full Term Abdominal Pregnancy
Authors Legesse TK ![]() , Ayana BA, Issa SA
, Ayana BA, Issa SA ![]()
Received 15 January 2023
Accepted for publication 9 March 2023
Published 15 March 2023 Volume 2023:16 Pages 173—178
DOI https://doi.org/10.2147/IMCRJ.S403180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ronald Prineas
Tesfaye Kebede Legesse,1 Birhanu Abera Ayana,2 Semira Abrar Issa1
1Department of Radiology, Addis Ababa University, College of Health Science, Addis Ababa, Ethiopia; 2Department of Obstetrics and Gynecology, Addis Ababa University, College of Health Science, Addis Ababa, Ethiopia
Correspondence: Tesfaye Kebede Legesse, Tel +251911405854, Email [email protected]
Background: Abdominal pregnancy refers to a rare form of ectopic pregnancy that has been implanted in the peritoneal cavity. Clinical suspicion combined with ultrasound is important for early diagnosis. A surviving fetus from an abdominal pregnancy is extremely rare.
Case Presentation: Herein we report on a case of advanced abdominal pregnancy in a Gravida-III Abortion-II mother who presented with worsening abdominal pain of 1 week duration associated with fetal movement and managed successfully with an outcome of a live neonate and no maternal complication.
Conclusion: A live neonate from term abdominal pregnancy is a rare occurrence. Early diagnosis of abdominal pregnancy is crucial to avoid potentially catastrophic maternal complications even though our patient, fortunately, has a smooth postoperative course. A high level of suspicion combined with ultrasound is helpful in reaching a diagnosis. Skill advancement for radiologists and non-radiology professionals involved in obstetric ultrasound is recommended to avoid misdiagnosis, as in our case. Careful post-operative evaluation is important to look for maternal and fetal complications.
Keywords: abdominal pregnancy, ectopic, term, live neonate, Ethiopia
Introduction
Ectopic pregnancy is derived from the Greek word “ektopos”, meaning out of place, and it refers to the implantation of a fertilized egg anywhere outside the endometrial cavity of the uterus. Ninety-five percent of cases occur in the Fallopian tubes; the remaining five percent occurs in other sites including the cornua of the uterus, the ovaries, the cervix, in a cesarean delivery scar and the peritoneal cavity (abdominal pregnancy).1
Abdominal pregnancy is a very rare condition that represents about 0.6–4% of all ectopic pregnancies.2 Clinical manifestations are usually nonspecific and cases with advanced pregnancy usually have abdominal or suprapubic pain, painfull fetal movements, easily palpable fetal parts and gastrointestinal symptoms.3 The condition is associated with potentially catastrophic complications including maternal death as a result of bleeding from the placental implantation site. A surviving fetus from an abdominal pregnancy is extremely rare and neonates who survive are reported to have a high rate of fetal deformation and perinatal death.4
Case Presentation
A 26-year-old Gravida III Abortion II lady with an unknown date but stated to be amenorrheic for about eight months came with a complaint of worsening lower abdominal pain of 1-week duration. The abdominal pain dated back 5 months which was severe at the beginning and predominantly in the lower abdomen. At that time, she was seen at a private clinic where she was evaluated and ultrasound scanning was done. She was told to be pregnant with an average gestational age of 18 weeks and 4 days, making her gestational age at presentation to be 37 weeks 6 days. The exact site of the pregnancy was missed in the initial ultrasound and considered as a normal intra-uterine pregnancy. Since then, she had similar complaints for which she visited the local health centre repeatedly. The patient was reaffirmed to have a normal pregnancy and no subsequent ultrasound scan was done.
A week before her admission, she started to have abdominal pain associated with each fetal movement which was severe enough to interfere with her day-to-day activity. The patient reported no vaginal bleeding and she had vital signs within the normal range on physical examination.
The patient was immediately taken for ultrasound evaluation which was done by a senior consultant radiologist and showed an enlarged empty uterus (Figure 1) with placenta separately identified (Figure 2) and a live fetus in the abdominal cavity. The head of the fetus was lying in the splenic hilum, pushing the spleen into the thoracic cavity (Figure 3). The placenta filled the whole abdomen and was attached to the right adnexa. Except for tortuously dilated right uterine vessels (Figure 4) which may suggest that the placenta was getting its supply from it, no other feeding arteries were seen. The placenta was clearly separate from the bowel walls (Figure 5A and B). There was deformity of the foot but details were difficult to make out due to the reduced amniotic fluid. Then the diagnosis of term abdominal pregnancy was made.
 |
Figure 1 Ultrasound picture shows empty uterus with well apposed endometrium which measures 8.4mm. |
 |
Figure 2 The placenta is seen separately adjacent to the uterine fundus. |
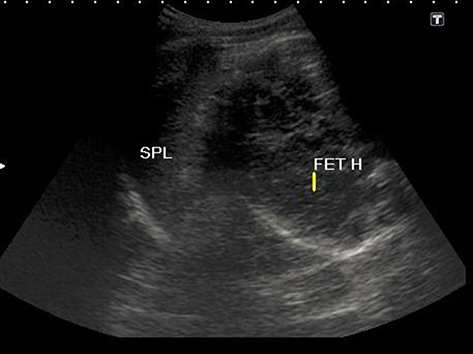 |
Figure 3 Picture shows fetal head adjacent to the splenic hilum. |
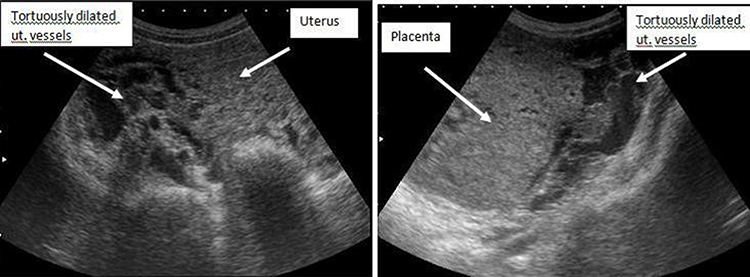 |
Figure 4 Picture shows tortuously dilated uterine vessels suggesting uterine artery is the feeding artery. |
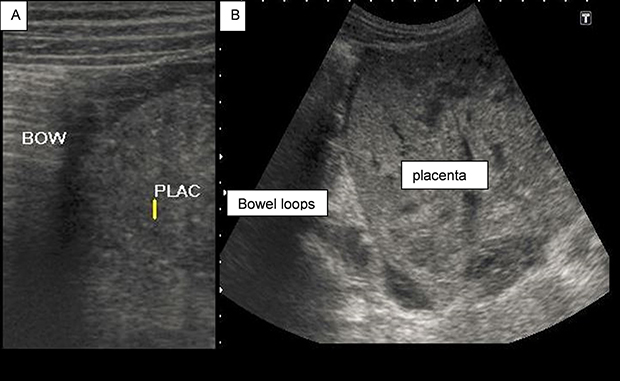 |
Figure 5 Picture showing relation of the placenta with bowel loops on a linear (A) and curvilinear (B) transducer probes. |
The patient was counselled on the diagnosis, the need for surgical intervention, and the possible complications. Her preoperative hemoglobin was determined, which was 12 mg/dL. Four units of blood were prepared prior to the surgery and space was reserved in the neonatal and adult intensive care unit for possible fetal and maternal complications. After providing written consent, the patient was taken to the operating theater.
During laparotomy, the abdominal pregnancy was apparent with the fetal foot visualized upon entry with intact membrane (Figure 6A), and a live female neonate weighing 2,060 g and an Apgar score of 8 and 9 in the first and fifth minutes, respectively, was extracted. There was an abnormality on the feet; both feet were dorsiflexed with the abduction of the forefoot (Figure 6B). Gestational age by Ballard score was estimated to be 36–38 weeks, corresponding to the GA calculated from the second-trimester estimation. The placenta had attachment to the broad ligament and the right adnexa with a narrow pedicle (Figure 7). There was also fine adhesion with the right ovary. The placenta was evacuated manually, including the right ovary, as it was adherent. The blood supply was from the tubal branch of the uterine artery which was carefully ligated before evacuation of the placenta. The uterus was about 14-week size and intact with no evidence for site of perforation or rupture. There was no defect seen on the fallopian tube, however, the tube was distorted and it was in close proximity with the placenta, suggesting secondary abdominal pregnancy possibly from a tubal abortion. The contralateral ovary and tube looked healthy. The estimated blood loss from the procedure was 400 mL. The mother did not require a blood transfusion in the immediate postoperative period or during her stay in the hospital despite the preparation for massive transfusion. The mother was transferred to the recovery room and later into the puerperium room under close follow-up for possible bleeding and changes in vital signs. The mother had stable vital signs in the course of her hospital stay. Her postoperative hemoglobin was 11 mg/dL and she was discharged with her neonate after 4 days.
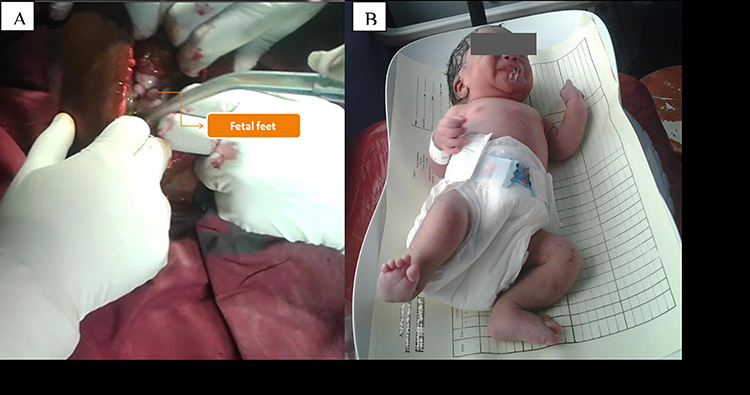 |
Figure 6 Fetal part (foot) seen upon entry to the abdominal cavity (A) and neonate with positional calcaneovalgus deformity (B). |
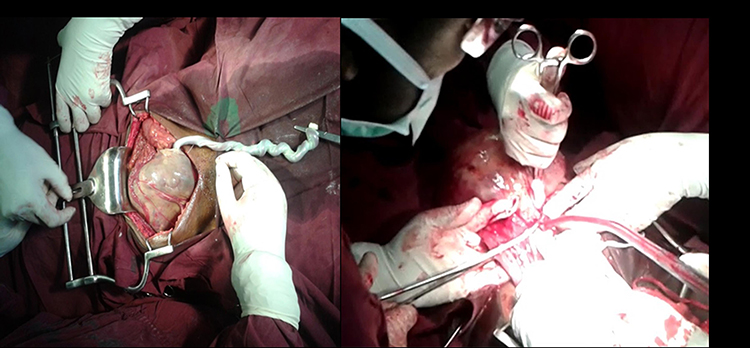 |
Figure 7 Placenta in the peritoneal cavity and the narrow placental pedicle attached to the right adnexa being clamped. |
Discussion
Abdominal pregnancy is a very rare condition that represents about 0.6–4% of all ectopic pregnancies.2 The condition is associated with potentially catastrophic complications, including maternal death as a result of bleeding, sepsis, and renal failure. A surviving fetus from an abdominal pregnancy is extremely unusual and neonates who survive are reported to have a high rate of fetal deformations and perinatal death.4
An abdominal pregnancy can be classified as either primary or secondary. The secondary type is the most common, which is usually the result of tubal abortion or rupture and, less frequently, after uterine rupture with subsequent reimplantation within the abdomen.5,6 The designation of primary peritoneal pregnancy requires certain criteria which include the presence of a pregnancy of less than 12 weeks in which trophoblastic attachments are related solely to a peritoneal surface, normal tubes and ovaries, and the absence of uteroperitoneal fistula.7,8 In our case, even though the patient presented in advanced gestational age, the right tube was buried within the placenta and there was adhesion with the ovary, possibly suggesting a secondary form of abdominal pregnancy. Classification of abdominal pregnancy has limited clinical value as it does not bring a difference to the management.9
Risk factors for abdominal pregnancy are almost similar with any other ectopic pregnancy. These include previous ectopic pregnancy, tubal surgery, and pelvic inflammatory disease.10 Clinical manifestation of abdominal pregnancy varies based on the site of implantation and gestational age. In cases of advanced pregnancies, painful fetal movements, easily palpable fetal part and persistently unusual lie are some of the common presenting symptoms.3,11 A high index of suspicion combined with imaging is critical in making early and accurate diagnosis which prevents potential complications to the mother. These include uncontrollable hemorrhage, which could result in maternal death, intestinal obstruction, abscess, and fistula if there is formation of a lithopedion, which is a dead and calcified abdominal pregnancy. Fetal complications from abdominal pregnancy include fetal malformations and perinatal death. Common fetal malformations reported are talipes equinovarus, hypoplastic limbs, and facial and cranial asymmetries.7
Routine ultrasound evaluation is recommended for pregnant woman in the mid-second trimester (18–22 weeks) to detect fetal anomalies and growth abnormalities. First trimester ultrasound (US) is most useful for patients with high risk features such as advanced maternal age and vaginal bleeding.12,13 The US report in these evaluations should include the gestational age, maternal organs (the cervix, uterus, and adnexa), the location of the placenta, and detailed anatomy of the fetus.9 Findings on US that direct to the diagnosis of abdominal pregnancy are the visualization of an empty uterus with a gestational sac or mass in the abdomen, excluding the fallopian tubes and ovaries.10 If the diagnosis of abdominal pregnancy is inconclusive with ultrasound findings, magnetic resonance imaging is an additional imaging option.10,14 In our case, the diagnosis was missed in the initial US and when she came late in the third trimester, she had the typical manifestations; painful and visible fetal movements and abnormal lie. This emphasizes the need for advancing the skill of radiologists and non-radiologist health care workers involved in obstetric ultrasound scans to avoid misdiagnosis of potential pregnancy-related complications.
The maternal mortality rate is very high, particularly with late diagnosis (beyond 20 weeks of gestation). It is estimated to be in the range of 1–18%.15,16 Maternal death can result from spontaneous separation of the placenta causing massive hemorrhage, shock, and multiple organ failure. Manual extraction of the placenta can also result in uncontrollable massive bleeding leading to maternal death. The placenta should be removed only if the procedure will not endanger the blood supply to the organ to which it is attached. Otherwise, leaving the placenta in situ is preferable with follow-up on ultrasound and human chorionic gonadotrophic level.4 In the current case, the placenta was attached to the tube with a narrow pedicle without involvement of the nearby structures and it was easily removed without damage or significant blood loss.
Fetal mortality in abdominal pregnancy remains high, 40% to 90%.7 Birth defects are seen in 21% of surviving babies born after an abdominal pregnancy, assumed to be secondary to compression of the fetus in the absence of the amniotic fluid buffer.5 Improved fetal outcome is reported if there is placental attachment to the uterus.7,17 In our case, the placenta was getting its supply from the tubal branch of the uterine artery and that may have contributed to the advancement of the pregnancy to term. In addition, there was skeletal deformity of the foot bilaterally (positional calcaneovalgus feet) which is expected in the presence of oligohydramnios.
Conclusion
An alive fetus from term abdominal pregnancy is a rare occurrence. Early diagnosis in an abdominal pregnancy is crucial to avoid potentially catastrophic maternal complications, even though our patient, fortunately, had a smooth postoperative course. A high level of suspicion combined with ultrasound is helpful in reaching a diagnosis. Skill advancement for radiologists and non-radiology professionals involved in obstetric ultrasound is recommended to avoid misdiagnosis, as in this case. Careful post-operative evaluation is important to look for maternal and fetal complications.
Ethical Approval and Informed Consent
Informed consent from the baby’s mother was obtained for publication of the patient’s medical case details and image of the baby post-delivery prior to publication. No Institutional approval was required for publication of this case report.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mummert T, Gnugnoli DM. Ectopic pregnancy. In: J StatPearls. Stat Pearls Publishing; 2022.
2. Fessehaye A, Gashawbeza B, Daba M, Arusi M, Terefe T. Abdominal ectopic pregnancy complicated with a large bowel injury: a case report. J Med Case Rep. 2021;15(1):127. doi:10.1186/s13256-021-02713-9
3. Tolefac PN, Abanda MH, Minkande JZ, Priso EB. The challenge in the diagnosis and management of an advanced abdominal pregnancy in a resource-low setting: a case report. J Med Case Rep. 2017;11(1):199. doi:10.1186/s13256-017-1369-1
4. Gurjar R. Full-term live secondary abdominal pregnancy: a rare case report. J Obstet Gynaecol India. 2019;69(Suppl 1):36–39. doi:10.1007/s13224-018-1156-y
5. Dahab AA, Aburass R, Shawkat W, et al. Full-term extrauterine abdominal pregnancy: a case report. J Med Case Rep. 2011;5(1):1–4. doi:10.1186/1752-1947-5-531
6. Dahiya K, Sharma D. Advanced abdominal pregnancy: a diagnostic and management dilemma. J Gynecol Surg. 2007;23(2):69–72. doi:10.1089/gyn.2007.B-02259-1
7. Zuñiga LA, Alas-Pineda C, Reyes-Guardado CL, Melgar GI, Gaitán-Zambrano K, Gough S. Advanced abdominal ectopic pregnancy with subsequent fetal and placental extraction: a case report. Biomed Hub. 2022;7(1):42–47. doi:10.1159/000521733
8. Hailu FG, Yihunie GT, Essa AA, Tsega W. Advanced abdominal pregnancy, with live fetus and severe preeclampsia, case report. BMC Pregnancy Childbirth. 2017;17(1):243. doi:10.1186/s12884-017-1437-y
9. Agarwal N, Odejinmi F. Early abdominal ectopic pregnancy: challenges, update and review of current management. J Obstet Gynaecol. 2014;16(3):193–198. doi:10.1111/tog.12109
10. George R, Powers E, Gunby R. Abdominal ectopic pregnancy. Proceedings. 2021;34(4):530–531. doi:10.1080/08998280.2021.1884932
11. Riethmuller D, Courtois L, Maillet R, et al. Prise en charge de la grossesse extra-utérine : les autres ectopies (cervicales et abdominales) [Ectopic pregnancy management: cervical and abdominal pregnancies]. J Gynecol Obstet Biol Reprod. 2003;32(7 Suppl):S101–S108. French.
12. Cargill Y, Morin L, Morin L. Content of a complete routine second trimester obstetrical ultrasound examination and report. J Obstet Gynaecol Can. 2009;31(3):272–275. doi:10.1016/S1701-2163(16)34127-5
13. Lee WA, Nelson G, Grogan SP. Sonography 1st trimester assessment, protocols, and interpretation. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC.; 2022. PMID: 34424643.
14. Mittal SK, Singh N, Verma AK, Agarwal H, Kulkarni CD, Kanaujia R. Fetal MRI in the pre-operative diagnosis and assessment of secondary abdominal pregnancy: a rare sequela of a previous caesarean section. Diagn Interv Radiol. 2012;18(5):496–502. doi:10.4261/1305-3825.DIR.5200-11.1
15. Paluku JL, Kalole BK, Furaha CM, et al. Late abdominal pregnancy in a post-conflict context: case of a mistaken acute abdomen - a case report. BMC Pregnancy Childbirth. 2020;20(1):238. doi:10.1186/s12884-020-02939-3
16. Shurie S, Ogot J, Poli P, Were E. Diagnosis of abdominal pregnancy still a challenge in low resource settings: a case report on advanced abdominal pregnancy at a tertiary facility in Western Kenya. Pan Afr Med J. 2018;31:239. doi:10.11604/pamj.2018.31.239.17766
17. Dubinsky TJ, Guerra F, Gormaz G, et al. Fetal survival in abdominal pregnancy: a review of 11 cases. J Clin Ultrasound. 1996;24(9):513–517. doi:10.1002/(SICI)1097-0096(199611/12)24:9<513::AID-JCU4>3.0.CO;2-Q
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.