Back to Journals » Risk Management and Healthcare Policy » Volume 15
Survival Analysis and Associated Factors for Pulmonary Tuberculosis Death: Evidence from the Information System of Tuberculosis Disease and Mortality Surveillance in China
Authors Liu K ![]() , Ai L
, Ai L ![]() , Pan J, Fei F, Chen S, Zhang Y, Wang W, Wu Q, Chen B
, Pan J, Fei F, Chen S, Zhang Y, Wang W, Wu Q, Chen B ![]() , Pan J, Zhong J
, Pan J, Zhong J
Received 30 March 2022
Accepted for publication 13 May 2022
Published 31 May 2022 Volume 2022:15 Pages 1167—1178
DOI https://doi.org/10.2147/RMHP.S368593
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Kui Liu,1,* Liyun Ai,2,* Jin Pan,3 Fangrong Fei,3 Songhua Chen,1 Yu Zhang,1 Wei Wang,1 Qian Wu,1 Bin Chen,1 Junhang Pan,1 Jieming Zhong3
1Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China; 2Hangzhou Municipal Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China; 3Department of Non-Communicable Disease Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junhang Pan; Jieming Zhong, Email [email protected]; [email protected]
Background: Pulmonary tuberculosis (PTB) is a severe infection, and its factors that influence survival have not been explored in some developed regions. Therefore, this study aimed to identify the factors that influence TB survival in China.
Methods: We acquired data of PTB deaths through matching two manage systems of PTB and mortality surveillance. The Kaplan–Meier method and Cox regression model were used to identify the significant factors under various survival times.
Results: A total of 283 deaths were caused by PTB, in which 53.4% occurred during the first year. In the Cox regression model, regular sputum smear test could reduce the risk of PTB death from the result of one-, three-, and five-year survival; and history of PTB treatment could decline the risk of PTB death in the first year. Additionally, age of “ 75– 90 years” and positive result of sputum smear test significantly increased the risk of PTB death for the findings of three- and five-year survival, while age of “ 60– 75 years” could increase the probability of PTB death for five-year survival.
Conclusion: To reduce PTB deaths, more attention should be paid to the older group especially in the first year. Regular sputum smear test could effectively reduce the mortality of PTB cases. More evidence-based interventions should be implemented to enhance the survival of patients with PTB.
Keywords: tuberculosis, influencing factor, survival analysis
Introduction
With more than 10 million infections each year, tuberculosis (TB) is a major global health problem and listed as one of the top 13 causes of death worldwide.1,2 TB is a chronic infectious respiratory disease caused by Mycobacterium tuberculosis.3 In recent years, a concerted global effort has been undertaken to eradicate TB and reduce TB-related mortality; consequently, the TB incidence and mortality rate have been decreasing by 1.9% and 3.4% annually, respectively.4 However, in 2020, a total of 1.5 million people died worldwide due to TB and of them, approximately 214,000 people had HIV.1 In China, as the second highest burden country, the annual TB mortality decreased by 7.7%, exceeding the worldwide mean.5,6 Although TB mortality declined to a comparatively low level, the persistent deaths due to pulmonary tuberculosis (PTB) remain a cause for concern. Considering the massive occurrence of PTB in China and the possibility of death, the determination of variables associated with PTB mortality can have a vital role in improving TB survival time.
Several previous studies have explored the factors associated with TB mortality, and emphasized three aspects: 1) demographic characteristics and living styles such as age, sex, educational level, employment status, income, dwelling status, alcohol consumption and smoking status; 2) clinical treatment, including comorbidities with HIV, COVID-19, and side effects caused by drugs, personal therapeutic regimen; and 3) other factors such as the health service policy, and social stigma and inequality.7–10
Regrettably, due to the paucity of information or insufficient sample size, limited studies have been conducted to identify the positive or negative factors associated with PTB mortality. Considering the developed economies and higher quality of life in the eastern area of China, this study sampled from Zhejiang Province. We investigated the possible risk factors affecting the survival of people with PTB to aid in improving the survival rate of cases and provide evidence for early intervention.
Materials and Methods
Overview
Zhejiang Province, located in the eastern region of China, includes two sub-provincial cities (Hangzhou and Ningbo) and nine prefecture-level cities (Wenzhou, Jiaxing, Huzhou, Shaoxing, Jinhua, Quzhou, Zhoushan, Taizhou, and Lishui). Although notified TB incidences in Zhejiang showed a successive declining trend (75.38/100,000 in 2009 to 52.25/100,000 in 2018), the epidemic level was not consistent with its economic development.11 Other demographic information and geographic location were described in our previous study.11
Data Sources
This study used the Zhejiang Chronic Disease Surveillance Information and Management System (ZJCDSIMS) and TB Information Management System (TBIMS) for obtaining data.12 We extracted demographics and variables reporting deaths from death certificates derived from the mortality surveillance module (MSM) of ZJCDSIMS.13,14 Additionally, people with suspected PTB would initially be notified by the China Information System for Disease Control and Prevention and then diagnosed PTB records were pushed to TBIMS.15 In TBIMS, specific details such as PTB diagnosis, treatment, and outcomes were recorded.16,17
This study initially collected all death cases directly caused by PTB from the MSM of ZJCDSIMS during 2017–2019. Then, the identity card (ID) number was viewed as a unique code to match the details in TBIMS.12 Considering the paucity or incompletion of ID numbers in the early phase of TBIMS, the combination of keywords—name, sex, address, and age (±3)—were used to match with the MSM. The information was documented included sex, age, occupation, marital status, location, TB classification, treatment history, sputum smear status, normative X-ray examination or not, regular sputum smear test or not, standardized treatment protocol or not, monitored during the whole course, comorbidity of diabetes/cardiovascular diseases or not. The cases were excluded if the records did not contain the above-mentioned information or the patients were transferred to drug resistance treatment; accordingly, 39 cases were excluded. The survival time for each case was defined as the interval between the last TB diagnosis and time of death. If the interval of two TB registrations for the same person was less than three months, we recognized it as single treatment. The survival time was classified as one year, three years, and five years.
Definition
All included TB cases met the confirmed PTB case classification and clinical diagnostic criteria for PTB, which was referred to as the National Diagnostic Criteria for Pulmonary Tuberculosis (WS288–2008 and WS 288–2017) and Classification of Tuberculosis (WS196–2017).18,19 In this study, the diagnosis of TB consisted of primary TB, hematogenous disseminated TB, secondary TB, TB pleuritis, and others. A regular sputum smear test was defined as sputum smear tests taken at the first diagnosis and later 2, 5, and 6 months from the start of TB treatment. If the patient records contained these information, it was denoted as finishing the regular sputum smear tests. Additionally, normative X-ray examination indicated that the patient underwent X-ray check twice, before and after TB diagnosis. The Technical Guide for Chinese Tuberculosis Control and Prevention criteria was referenced for standardized treatment protocols for PTB and whole-course surveillance during treatment.
Statistical Analysis
Descriptive analysis and survival analysis were performed using R software (version 3.5.3) and SAS software (version 9.4). The Kaplan–Meier method and Log rank test were used to calculate the survival time and compare the survival time among different variables related to PTB death. In addition, the Cox proportional hazard regression model for survival time at one-year, three-year, and five-year was performed, and hazard ratios (HRs) and their 95% confidence intervals (CIs) were presented. All the covariates were included in the univariate and multivariable analyses. Statistical significance was set at P < 0.05.
Results
Profile of Patients: Death Caused by PTB
In this study, we collected information on 283 deaths caused by PTB from 2017 to 2019 in Zhejiang Province. The study population included 228 males (79.2%) and 55 females (20.8%). The 1-year, 3-year, and 5-year survival percentages were 46.6%, 25.1%, and 14.5%, respectively. The percentage of PTB deaths within the first 2 months after diagnosis was 19.4%. Of all the mortality cases, 86.6% were aged >60 years, 13.4% were 18–60 years, and no cases were <18 years. Moreover, 80.9% were farmers and 67.5% were married. Among the diverse regions in Zhejiang Province, Hangzhou, Jiaxing, and Jinhua ranked the highest with PTB death proportion of 16.3%, 12.0%, and 12.0%, respectively. 96.1% of PTB belonged to the secondary TB, and 78.4% of PTB was the initial PTB. Additionally, 193 cases (68.2%) had the result of positive sputum smear test. The proportion of patients with regular sputum smear tests was 49.1%, and patients with the normative X-ray examination accounted for 18.4%. Of the PTB mortality cases, PTB cavity was reported in 36.0% cases and 6.4%, 11.3%, and 8.8% cases had diabetes mellitus, cardiovascular diseases, and other illnesses, respectively (Table 1).
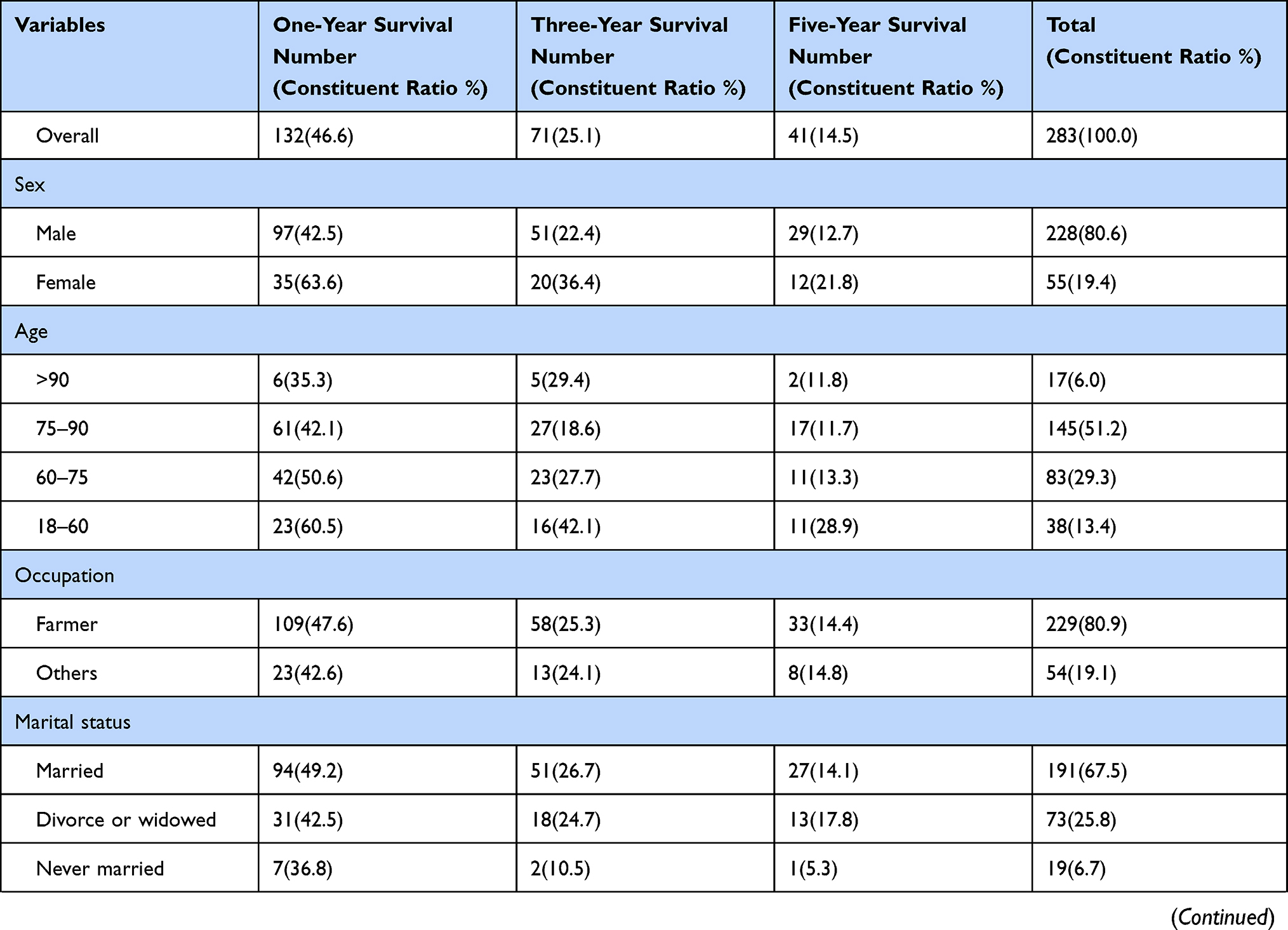 | 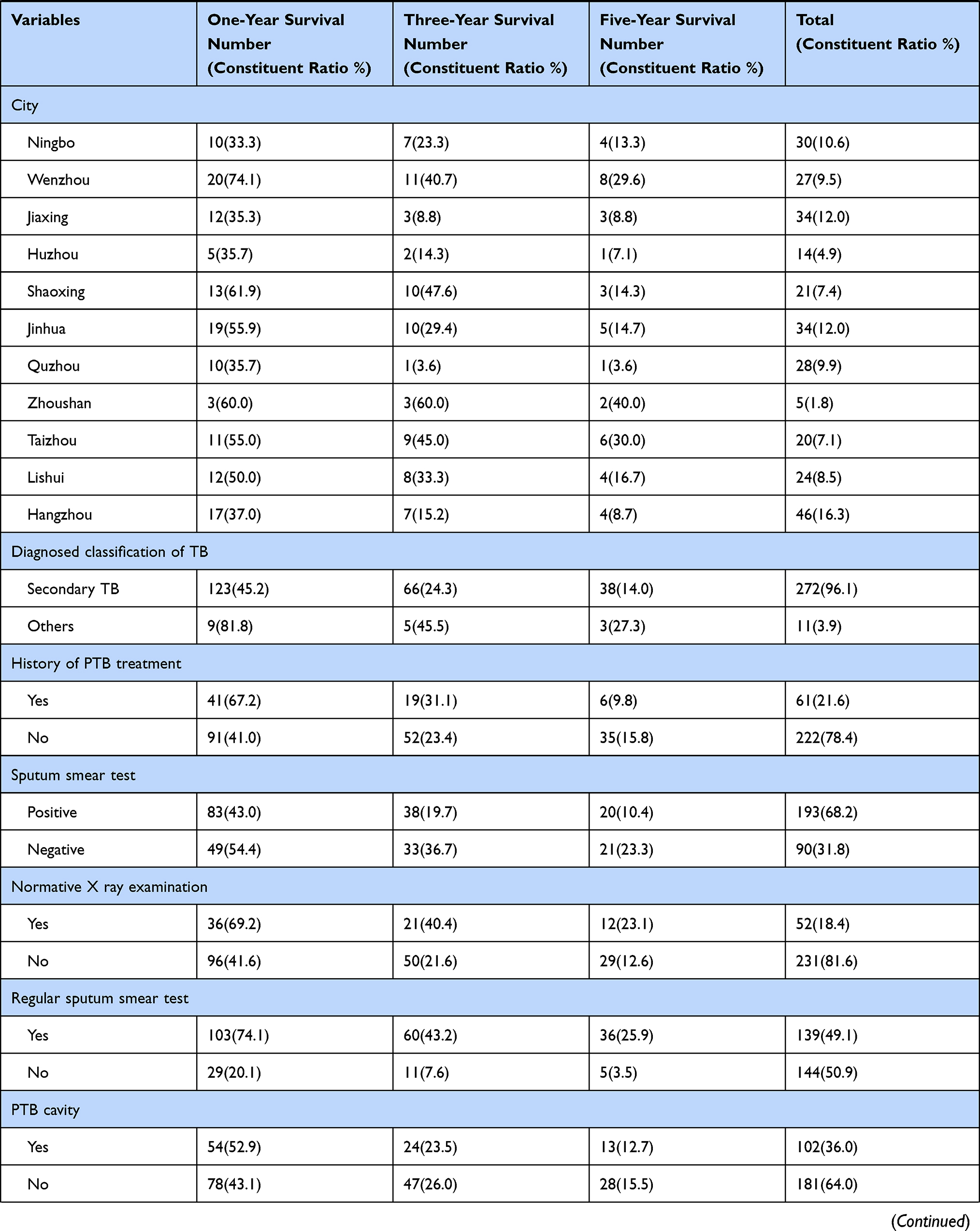 | 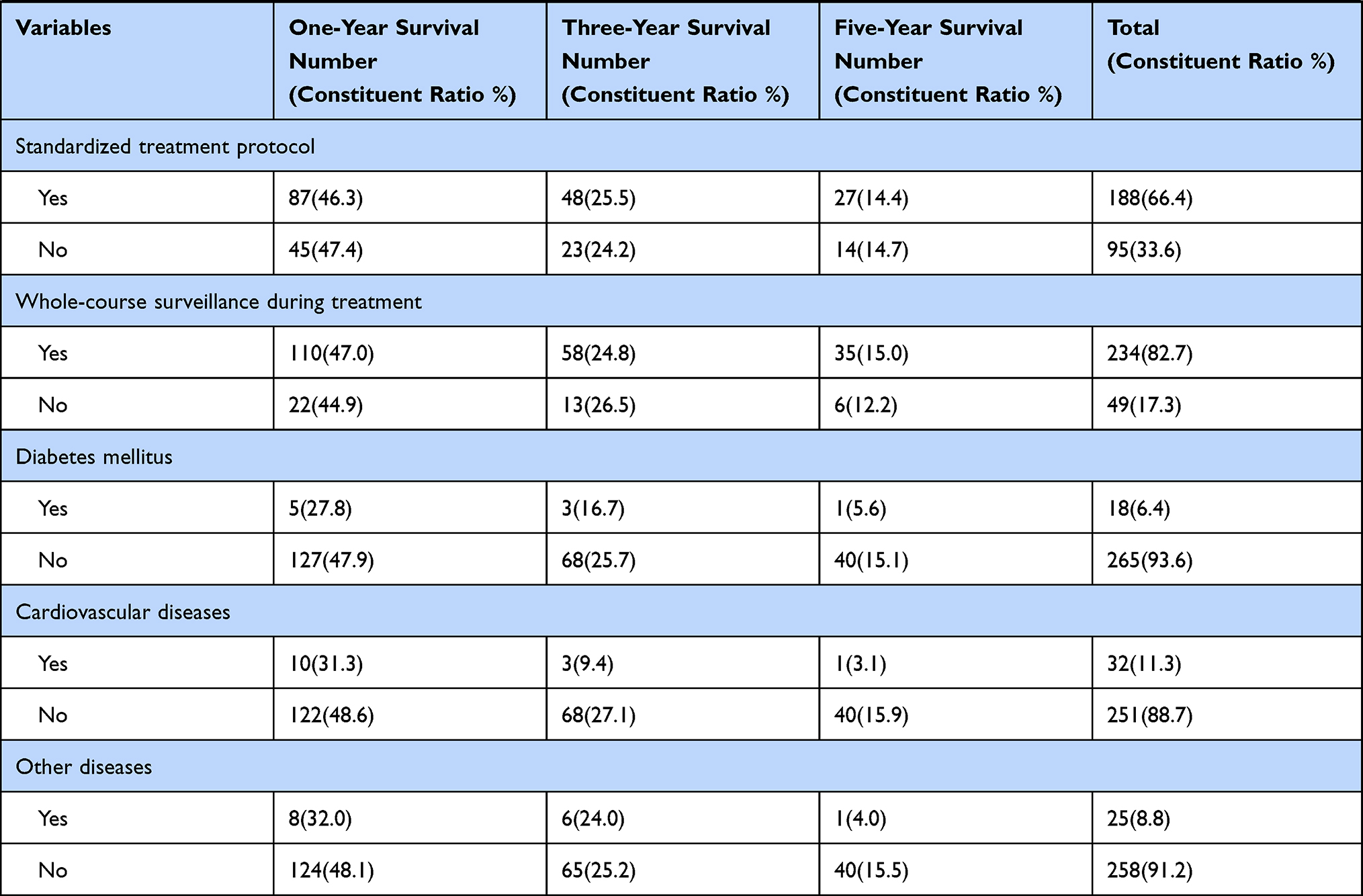 |
Table 1 Basic Characteristics of All Included PTB deaths in Zhejiang Province from 2017 to 2019 |
Survival Analysis of Influencing Factors Among PTB Death
The Kaplan–Meier survival function test and Log rank test were used to compare the cumulative probability among the various associated factors. For the one-year survival period, the variables sex, city, history of TB treatment, normative X-ray examination, regular sputum smear test, diabetes mellitus, and cardiovascular diseases were statistically significant (P<0.05). Additionally, for the three-year survival period, sex, age, city, history of TB treatment, sputum smear test, normative X-ray examination, regular sputum smear test, and cardiovascular diseases were statistically significant (P<0.05). Sex, age, city, sputum smear test, normative X-ray examination, regular sputum smear test, and cardiovascular diseases were shown to have statistical significance (P<0.05) in the five-year survival period.
Cox Regression Model for the Multivariable Analysis Regarding the Factors Associated with PTB Mortality
The Cox regression model for multivariable analysis was performed in this study. After controlling for other factors, the variables could be estimated more precisely. In multivariable Cox regression analysis for one-year survival, secondary TB (HR: 7.59, 95% CI: 1.83–31.39, P<0.01) had the highest hazard ratio and risk of death was significantly reduced in the cities of Wenzhou (HR: 0.21, 95% CI: 0.08–0.52, P<0.01) and Taizhou (HR: 0.32, 95% CI: 0.15–0.72, P=0.01). Additionally, having a history of PTB treatment (HR: 0.45, 95% CI: 0.27–0.77, P<0.01) and having a regular sputum smear test (HR: 0.13, 95% CI: 0.08–0.20, P<0.01) were associated with reduced risk of death.
For the three-year survival, secondary TB (HR: 3.06, 95% CI: 1.26–7.39, P=0.01), age 75–90 years (HR: 2.03, 95% CI: 1.18–3.48, P=0.01), farmer (HR: 1.50, 95% CI: 1.01-2.22, P=0.05), and positive sputum smear test result (HR: 1.72, 95% CI: 1.09–2.73, P=0.02) significantly increased the risk of PTB death. However, the hazard ratio was reduced for those married (HR: 0.42, 95% CI: 0.22–0.82, P=0.01), those divorced or widowed (HR: 0.45, 95% CI: 0.24–0.82, P=0.01); and those living in the cities of Wenzhou (HR: 0.29, 95% CI: 0.15–0.57, P<0.01), Jinhua (HR: 0.57, 95% CI: 0.33–0.99, P=0.04), and Taizhou (HR: 0.36, 95% CI: 0.18–0.73, P=0.01); and having a regular sputum smear test (HR: 0.18, 95% CI: 0.13–0.26, P<0.01).
For the five-year survival results, the hazard ratio increased for secondary TB (HR: 2.30, 95% CI: 1.35–6.50, P<0.01), positive sputum smear test result (HR: 2.06, 95% CI: 1.35–3.15, P<0.01), age 75–90 years (HR: 1.97, 95% CI: 1.21–3.21, P=0.01), age 60–75 years (HR: 1.74, 95% CI: 1.05–2.88, P=0.03), and farmer (HR: 1.50, 95% CI: 1.03-2.17, P)=0.03; it was reduced for those married (HR: 0.40, 95% CI: 0.21–0.75, P=0.01); those who were divorce or widowed (HR: 0.47, 95% CI: 0.26–0.83, P=0.01); those living in the city of Wenzhou (HR: 0.34, 95% CI: 0.18–0.64, P<0.01) and Taizhou (HR: 0.42, 95% CI: 0.22–0.80, P=0.01); and having a regular sputum smear test (HR: 0.19, 95% CI: 0.14–0.26, P<0.01). The results are shown in Table 2 and Figure 1.
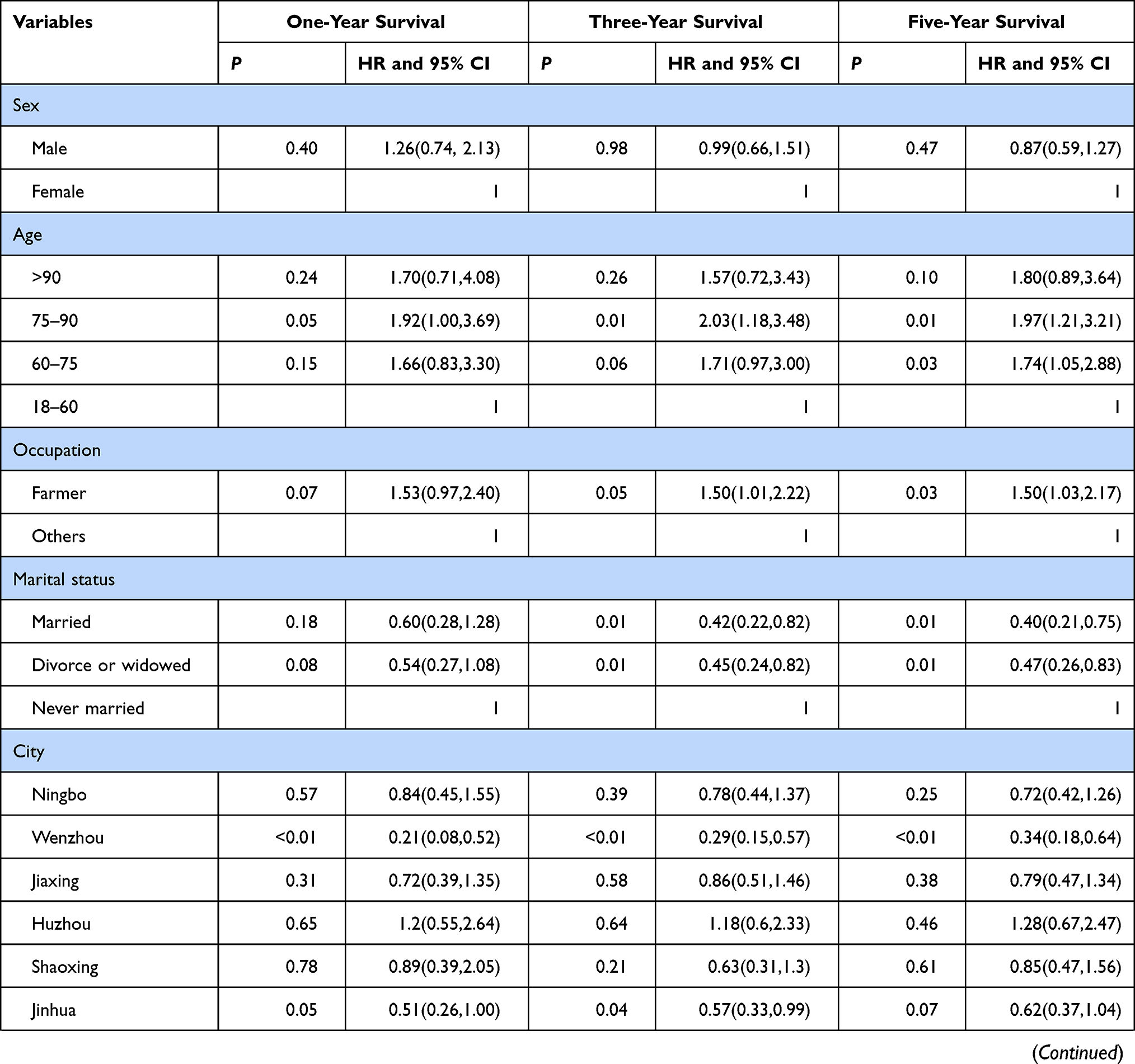 | 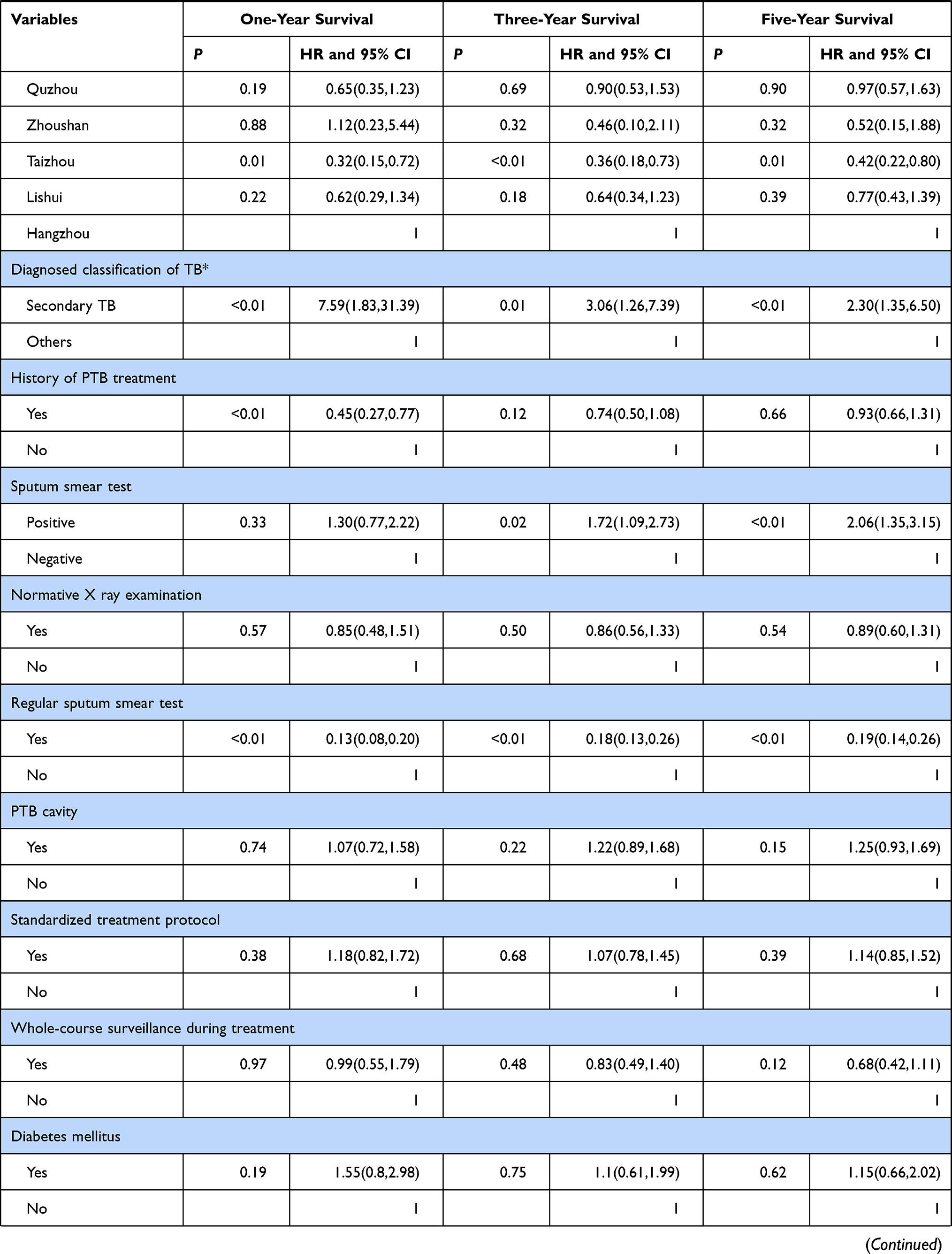 | 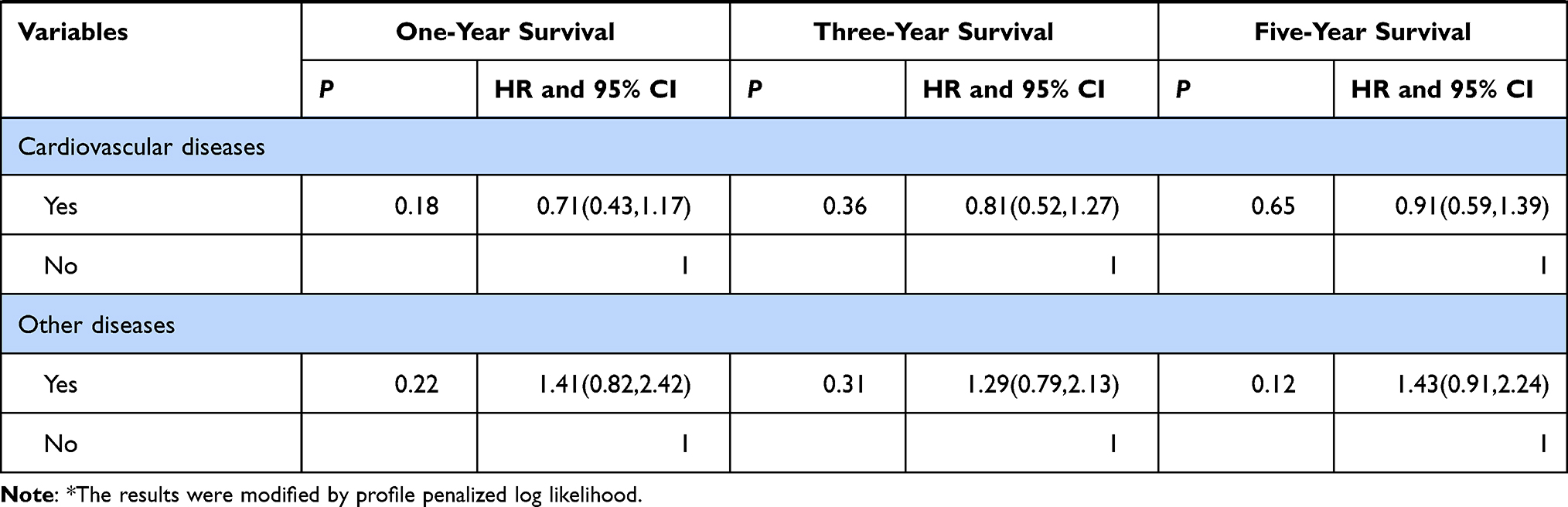 |
Table 2 The Cox Proportional Hazard Regression Model Regarding the Influencing Factors Related to PTB Death at Three Different Periods |
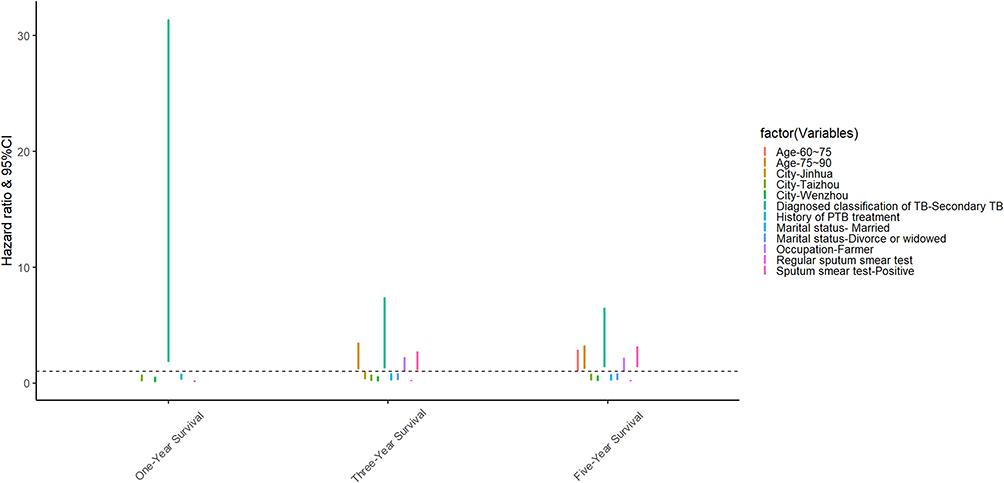 |
Figure 1 Summary of variables associated with risk of PTB death from the Cox regression analysis. |
Discussion
In this study, we investigated the factors associated with PTB death in Zhejiang Province, located in the eastern area of China. In contrast to the previous studies that recruited volunteers in the hospital population or program groups to observe the survival time and its associated factors, our study considered all direct deaths caused by PTB in Zhejiang Province through the accurate matching of two available surveillance systems.20–22 The strength of our study, which has comprehensive sample and precise outcome, could clarify associations and provide more robust results.
In our study, only 14.5% of included PTB death cases had a survival time of more than five years. Considering that 86.6% of participants were older than 60 years in our study, it is suggested that weakened individual immunity and some existing comorbidities in these older groups may aggravate the PTB infection, onset, and even death.23,24
In addition, findings from one study showed a higher risk of death during the first year of antituberculosis treatment.25 Furthermore, a study identified a significant reduction in cumulative survival rate in the initial 2 months of antituberculosis treatment, while another study showed that nearly 75% of deaths occurred at the end of treatment period.26,27 Our results showed that among all PTB deaths, nearly 19.4% of deaths occurred in the first 2 months and 53.4% of PTB deaths occurred in the first year (In China nearly all PTB cases begin treatment once diagnosed). Thus, PTB cases in the older group need further attention to reduce PTB deaths in the first year. Meanwhile, this discrepancy of early death might be potentially attributed to nutritional support and aging composition, which highlights the importance of regular follow-up and nutritional supplement.28
No statistically significant differences were found for sex during the different periods of the survival analysis. This result was similar to that of Kabtamu Tolosie’s study in Ethiopia but differed from the findings of other studies.29–31 Some factors, such as diverse socioeconomic levels and ethnicity, might have contributed to such differences.
Previous literature has identified age as a potential risk factor for TB survival, suggesting mortality increases by 5.9% with increasing yearly age.3 The findings of our study further implied the “60–75” age group was a negative influencing factor for long-term survival (five-year survival) and the “75–90” age group was a negative influencing factor for medium/long-term survival (three/five-year survival). For these older age group, affected factors including lower immunity levels, more comorbidities, and delayed diagnosis, might explain the effect on survival time.32 However, for the aged groups “>90”, no significant difference was observed in short/medium/long-term survival, which could be attributed to the sample size in our study. Thus, reaching people earlier to test for PTB and to receive treatment immediately requires increased awareness and targeting the age groups most at risk.
Economic and educational levels can affect access to health services and subsequently affect TB survival time.33 Interestingly, for the farmer group, no significant association was identified concerning short-term survival, but it was a potential negative factor for medium-and long-term survival. We speculated that this particular group had limited nutritional level and insufficient health knowledge related to PTB that affect survival time, which should be investigated and verified in future studies.
The result regarding marital status implied that an experience of marriage might benefit the medium/long-term survival of PTB cases, perhaps through social support. Additionally, our study identified an association between TB mortality and various regions. Some regions such as Taizhou, and Wenzhou had significantly lower risk of PTB mortality, suggesting excellent health services.
Moreover, PTB cases with a history of PTB treatment had a positive impact on short-term survival. It might be that previous treatment provided a reference for these people, which could cause fewer delays for seeking healthcare and increased awareness of the importance of adherence in the latest treatment. Moreover, the literature has demonstrated that the success rate of retreated patients was lower than that of those initially treated, indicating that retreated PTB cases may have a longer treatment time.3 Thus, for reasons like longer treatment periods, such beneficial effects may be weakened in the former, and no statistically significant benefits were found for the medium/long-term survival of PTB.
A sputum smear test with positive result was associated with a higher risk for medium/long-term survival, but not short-term survival. This may be attributed to the cumulative tissue damage caused by Mycobacterium tuberculosis, which seriously affects the life span of patients.
In this study, a regular sputum smear test was found to be a protective factor against death at different survival times, but no significant difference was identified among normative X-ray examinations. The regular sputum smear test could reflect PTB progression more accurately and directly, which is helpful in developing specific therapeutic regimens, while the normative X-ray examinations entail morphological observations that might exist with some lag occasionally. Thus, for the regular sputum smear test, the clinical doctor could make more precise decisions for subsequent treatment to enhance successful treatment and decrease PTB deaths.
Diabetes mellitus, cardiovascular disease, and other diseases did not increase the risk of PTB mortality at the different time points. This finding was similar to a previous study that associated diabetes mellitus, chronic obstructive pulmonary disease, and cancer with all-cause mortality but not with mortality due to PTB.25 Although our study only considered survival time, controlling these comorbidities was still vital to shortening the progress of PTB and enhancing the therapeutic effect.
Our study has some limitations. First, we chose PTB death at limited time periods, and overwhelming majority of the PTB patients include those in older age group, which influenced the extrapolation of our findings. Second, some possible factors were not verified in our study, such as delayed time for diagnosis, drug resistance status, education level of patients, smoking status, and comorbidity of HIV.21,34,35 Meanwhile, some explorations in clinical data such as radiologic severity and drug adverse effects were not considered. We, however, investigated three different survival periods providing the dynamic characteristics of associated factors, which contributed to a better understanding of PTB survival features.
Conclusion
To reduce PTB mortality, more attention should be paid to the older population, especially during the first year. Regular sputum smear test could effectively reduce the mortality in PTB cases. Based on the findings of factors associated with PTB survival, more evidence-based interventions should be formulated and implemented to enhance the survival of patients with PTB, reduce PTB mortality, and achieve the “End TB” target.
Abbreviations
PTB, pulmonary tuberculosis; TBIMS, TB Information Management System; MSS, Mortality Surveillance System; CDC, Centers for Disease Control; HIV, human immunodeficiency virus.
Data Sharing Statement
All data and materials were included in this paper. The corresponding author could provide all data upon reasonable request.
Ethical Approval and Consent to Participate
The included cases with TB deaths were fully anonymized after the data matching phase. Our study was approved by the Ethics Committee of the Zhejiang Provincial Center for Disease Control and Prevention. Considering only public health surveillance data used in this research, informed consent was exempted by ethics institutional review board above. Moreover, all details used in this research followed the Law of the Prevention and Treatment of Infectious Diseases in the People’s Republic of China.
Consent for Publication
Not applicable.
Acknowledgments
Thanks for the assistance from Chronic Disease Prevention and Control in Zhejiang province and vital suggestions from Leonardo Martinez at Stanford University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Zhejiang Provincial Science and Public Welfare (LGF19H260004), Philosophy and Social Science Project of Zhejiang Province (19NDJC243YB), and Zhejiang Provincial Medical and Health Project (2021KY618 and 2019RC135).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Global tuberculosis report 2021. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
2. Furin J, Cox H, Pai M. Tuberculosis. Lancet. 2019;393(10181):1642–1656. doi:10.1016/s0140-6736(19)30308-3
3. Xie Y, Han J, Yu W, Wu J, Li X, Chen H. Survival analysis of risk factors for mortality in a cohort of patients with tuberculosis. Can Respir J. 2020;2020:1654653. doi:10.1155/2020/1654653
4. Floyd K, Glaziou P, Zumla A, Raviglione M. The global tuberculosis epidemic and progress in care, prevention, and research: an overview in year 3 of the end TB era. Lancet Respir Med. 2018;6(4):299–314. doi:10.1016/s2213-2600(18)30057-2
5. Global tuberculosis report 2019. Geneva: World Health Organization; 2019.
6. Houben RMGJ, Menzies NA, Sumner T, et al. Feasibility of achieving the 2025 WHO global tuberculosis targets in South Africa, China, and India: a combined analysis of 11 mathematical models. Lancet Glob Health. 2016;4(11):e806–e15. doi:10.1016/S2214-109X(16)30199-1
7. Dos Santos DT, Arroyo LH, Alves YM, et al. Survival time among patients who were diagnosed with tuberculosis, the precocious deaths and associated factors in southern Brazil. Trop Med Health. 2021;49(1):31. doi:10.1186/s41182-021-00320-4
8. Parry C, Ferreira-Borges C, Poznyak V, Lönnroth K, Rehm J. The international study on alcohol and infectious diseases: three priorities for research. Addiction. 2013;108(1):1–2. doi:10.1111/j.1360-0443.2012.04000.x
9. Berra TZ, Queiroz AAR, Yamamura M, et al. Spatial risk of tuberculosis mortality and social vulnerability in Northeast Brazil. Rev Soc Bras Med Trop. 2017;50(5):693–697. doi:10.1590/0037-8682-0160-2017
10. Nabity SA, Han E, Lowenthal P, et al. Sociodemographic characteristics, comorbidities, and mortality among persons diagnosed with tuberculosis and covid-19 in close succession in California, 2020. JAMA network open. 2021;4(12):e2136853. doi:10.1001/jamanetworkopen.2021.36853
11. Liu K, Li T, Vongpradith A, et al. Identification and prediction of tuberculosis in Eastern China: analyses from 10-year population-based notification data in Zhejiang Province, China. Sci Rep. 2020;10(1):7425. doi:10.1038/s41598-020-64387-5
12. Li T, Zhang H, Shewade HD, Soe KT, Wang L, Du X. Patient and health system delays before registration among migrant patients with tuberculosis who were transferred out in China. BMC Health Serv Res. 2018;18(1):786. doi:10.1186/s12913-018-3583-y
13. Fei FR, Hu RY, Gong WW, Pan J, Wang M. Analysis of mortality and survival rate of liver cancer in Zhejiang Province in China: a General Population-Based Study. Can J Gastroenterol Hepatol. 2019;2019:1074286. doi:10.1155/2019/1074286
14. Fei FR, Zhong JM, Yu M, et al. Impact of injury-related mortality on life expectancy in Zhejiang, China based on death and population surveillance data. BMC Public Health. 2017;18(1):24. doi:10.1186/s12889-017-4566-3
15. Huang F, Cheng S, Du X, et al. Electronic recording and reporting system for tuberculosis in China: experience and opportunities. JAMIA. 2014;21(5):938–941. doi:10.1136/amiajnl-2013-002001
16. Li T, Du X, Shewade HD, Soe KT, Zhang H. What happens to migrant tuberculosis patients who are transferred out using a web-based system in China? PLoS One. 2018;13(11):e0206580. doi:10.1371/journal.pone.0206580
17. Li T, Shewade HD, Soe KT, et al. Under-reporting of diagnosed tuberculosis to the national surveillance system in China: an inventory study in nine counties in 2015. BMJ open. 2019;9(1):e021529. doi:10.1136/bmjopen-2018-021529
18. National Health and Family Planning Commission, Classification of Tuberculosis. 2018.
19. Ministry of Health P.R. China: Diagnostic Criteria for Pulmonary Tuberculosis. People’s Medical Publishing House; 2008.
20. Carter BB, Zhang Y, Zou H, et al. Survival analysis of patients with tuberculosis and risk factors for multidrug-resistant tuberculosis in Monrovia, Liberia. PLoS One. 2021;16(4):e0249474. doi:10.1371/journal.pone.0249474
21. Olaleye AO, Beke AK. Survival of smear-positive multidrug resistant tuberculosis patients in Witbank, South Africa: a retrospective cohort study. Infect Dis. 2016;48(6):422–427. doi:10.3109/23744235.2016.1153806
22. Balaky STJ, Mawlood AH, Shabila NP. Survival analysis of patients with tuberculosis in Erbil, Iraqi Kurdistan region. BMC Infect Dis. 2019;19(1):865. doi:10.1186/s12879-019-4544-8
23. Hochberg NS, Horsburgh CR
24. Negin J, Abimbola S, Marais BJ. Tuberculosis among older adults–time to take notice. Int J Infect Dis. 2015;32:135–137. doi:10.1016/j.ijid.2014.11.018
25. Liu Y, Zheng Y, Chen J, et al. Tuberculosis-associated mortality and its risk factors in a district of Shanghai, China: a retrospective cohort study. Int J Tuberc Lung Dis. 2018;22(6):655–660. doi:10.5588/ijtld.17.0726
26. Birlie A, Tesfaw G, Dejene T, Woldemichael K. Time to death and associated factors among tuberculosis patients in Dangila Woreda, Northwest Ethiopia. PLoS One. 2015;10(12):e0144244. doi:10.1371/journal.pone.0144244
27. Getahun B, Ameni G, Biadgilign S, Medhin G. Mortality and associated risk factors in a cohort of tuberculosis patients treated under DOTS programme in Addis Ababa, Ethiopia. BMC Infect Dis. 2011;11(1):1–8. doi:10.1186/1471-2334-11-127
28. Harries AD, Hargreaves NJ, Gausi F, Kwanjana JH, Salaniponi FM. High early death rate in tuberculosis patients in Malawi. Int J Tuberc Lung Dis. 2001;5(11):1000–1005.
29. Tolosie K, Sharma MK. Application of cox proportional hazards model in case of tuberculosis patients in selected Addis Ababa health centres, Ethiopia. Tuberc Res Treat. 2014;2014:536976. doi:10.1155/2014/536976
30. Zenebe T, Tefera E. Tuberculosis treatment outcome and associated factors among smear-positive pulmonary tuberculosis patients in Afar, Eastern Ethiopia: a retrospective study. Braz J Infect Dis. 2016;20(6):635–636. doi:10.1016/j.bjid.2016.07.012
31. Wu YC, Lo HY, Yang SL, Chu DC, Chou P. Comparing the factors correlated with tuberculosis-specific and non-tuberculosis-specific deaths in different age groups among tuberculosis-related deaths in Taiwan. PLoS One. 2015;10(3):e0118929. doi:10.1371/journal.pone.0118929
32. Machado D, Couto I, Viveiros M. Advances in the molecular diagnosis of tuberculosis: from probes to genomes. Infect Genet Evol. 2019;72:93–112. doi:10.1016/j.meegid.2018.11.021
33. Hossain S, Quaiyum MA, Zaman K, et al. Socio economic position in TB prevalence and access to services: results from a population prevalence survey and a facility-based survey in Bangladesh. PLoS One. 2012;7(9):e44980. doi:10.1371/journal.pone.0044980
34. Azeez A, Mutambayi R, Odeyemi A, Ndege J. Survival model analysis of tuberculosis treatment among patients with human immunodeficiency virus coinfection. Int J Mycobacteriology. 2019;8(3):244–251. doi:10.4103/ijmy.ijmy_101_19
35. Wang J, Zhou M, Chen Z, et al. Survival of patients with multidrug-resistant tuberculosis in Central China: a retrospective cohort study. Epidemiol Infect. 2020;148:e50. doi:10.1017/s0950268820000485
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.