Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Survey on Polypharmacy and Drug-Drug Interactions Among Elderly People with Cardiovascular Diseases at Yekatit 12 Hospital, Addis Ababa, Ethiopia
Authors Assefa YA, Kedir A, Kahaliw W ![]()
Received 16 September 2019
Accepted for publication 27 December 2019
Published 9 January 2020 Volume 2020:9 Pages 1—9
DOI https://doi.org/10.2147/IPRP.S231286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Yelbeneh Abayneh Assefa,1 Ansha Kedir,1 Wubayehu Kahaliw2
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Pharmacology, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Wubayehu Kahaliw
Department of Pharmacology, College of Medicine and Health Sciences, University of Gondar, P.O, Box 196, Gondar, Ethiopia
Tel +251910532412
Email [email protected]
Background: Elderly people are most commonly associated with cardiac disease. Cardiovascular diseases are interlinked with co-morbidities which require multiple drug therapy in addition to cardiovascular drugs. This results to polypharmacy which carries a high risk of potential drug-drug interactions. Elderly patients are at a particular risk of drug related problems because of increased level of polypharmacy and the physiological changes which accompany aging. This study was aimed to assess polypharmacy and potential drug-drug interactions (DDIs) among elderly people with cardiovascular diseases at Yekatit 12 hospital.
Methodology: A retrospective cross-sectional study using patients chart review was conducted on all elderly people with cardiovascular diseases at Yekatit 12 hospital in the period between March 2018 and March 2019. The types, seriousness and level of potential DDIs were checked using Medscape online drug interaction checker.
Results: The mean number of drugs per prescription was 4.25 ± 1.754 and the prevalence of polypharmacy (concurrent use of 5 and more drugs) was 42.7%. Polypharmacy and potential DDIs were significantly associated with polymorbidity (P = 0.000), being hospitalized (P = 0.047) and congestive heart failure (P = 0.016). A total of 850-potential DDIs were identified, the mean number of potential DDIs was 3.37 per prescription. The potential DDIs were mainly significant (73.29%) in nature and pharmacodynamics (73.06%) in mechanism. The prevalence of total and serious potential DDIs were 84.3% and 17.3%, respectively. Most commonly interacting drug combination was aspirin + enalapril (30.2%).
Conclusion: A higher incidence of polypharmacy and increased risk of potential DDIs in elderly people with cardiovascular disease are major therapeutic issues at Yekatit 12 hospital.
Keywords: polypharmacy, drug-drug interaction, cardiovascular diseases, elderly
Background
In many countries of the world, elderly people are significant in number and 60% of them are found in developing countries.1 Elderly people in Ethiopia account 9.5% from the total population.2 One-cardiovascular disease can occur as co-morbidity with another one. Non-cardiovascular diseases are also highly associated with cardiovascular diseases which impart complications to the heart. These complications cause several dysfunctions resulting in the use of many drugs (polypharmacy).3
Polypharmacy is defined as the concurrent use of five or more drugs.4–8 It is associated with suboptimal prescribing, increase in risk of falls and has a significant effect on increasing health expenditures. Therefore, it is a matter of interest for prescribers since it may be regarded as irrational prescribing and it is a significant problem among older adults.9,10 The practice of polypharmacy leads to drug interactions and this in turn causes adverse drug reactions and deterioration of functional status.11–14
Drug-drug interaction (DDI) is defined as the change in the drugs effect when a second drug is taken concurrently. As a result of drug-drug interaction synergistic or additive, antagonistic or subtractive and idiosyncratic effects may occur.15 Drug-drug interactions can be classified as pharmacokinetic, pharmacodynamics and pharmaceutical interactions. Pharmacokinetic interactions are the result of altered drug delivery to the site of action and can occur at the level of absorption, distribution, metabolism or clearance of the affected agent whereas Pharmacodynamic interactions are the result of altered drug effect at the site of action. Pharmaceutical interaction is the interaction of incompatible drugs which occur outside of the body during mixing.16
Studies indicated that there is an increased level of multiple medications and hence drug-drug interaction among the elderly part of the population.3 The drug-drug interaction rate is higher in cardiovascular diseases compared to other disease. The possible reason behind higher DDI rate in cardiovascular disease may include elder age, polypharmacy and pharmacokinetic or pharmacodynamics nature of drugs used in cardiology.17 People in old age are highly vulnerable to drug adverse effects because of multiple drugs and aging.19,20 Physiological alterations associated with aging make the elderly susceptible to drug-interactions. The physiological alterations which accompany aging are renal insufficiency and liver metabolism abnormality, gut function alterations and poor nutritional status.11
In addition, elderly patients suffering from chronic diseases and taking sedatives/hypnotics without indication and those with hypertension or atrial fibrillation are at high risk of exposure to multiple drugs and potential drug-drug interaction.3 In elderly patients, drug-drug interactions play a significant role in the deterioration of the general health condition, leading to affliction, poor quality of life, prolonged hospital stays, a greater need for ambulatory services and increased health-care costs.13
Although polypharmacy and drug interactions reported to be common, there is sparse data on the prevalence of polypharmacy and drug-drug interactions in Yekatit12 hospital, Addis Ababa, Ethiopia. Hence this study was aimed to evaluate prevalence of polypharmacy and types and severity of possible drug-drug interactions in ambulatory and hospitalized elderly cardiovascular patients.
Methods
Description of Study Setting
Yekatit 12 hospital is a referral hospital owned by Addis Ababa Health Council. The hospital is a teaching hospital associated with Addis Ababa University Black Lion Hospital. It is one of the public hospitals in Ethiopia. The hospital provides services for a population of approximately 4 million. It consists of nine departments and six units and has 265 beds. Yekatit 12 hospital has excellent laboratory facilities that perform most categories of routine diagnostics.
Study Design, Sample Size and Data Collection
A retrospective cross-sectional study was carried out from March 2018 to March 2019 in Yekatit 12 Hospital. All elderly (age 50 years and above) patients’ charts of cardiovascular disease and with adequate documentation were included in the study. All cardiovascular patients’ charts age 49 years and below as well as charts recording non-cardiovascular disease were excluded from the study. Data were collected from 255 patients’ charts using structured data collection format (Patient data abstraction format). The format was prepared with different sections important to fill basic demographic information like age and sex, drugs administered, and co-morbidities or diseases identified. The interactions between the drugs were assessed using Medscape online drug interaction checker.18
Ethical Considerations
Approval of the research ethics was obtained from School of Pharmacy, Addis Ababa University Ethics Review committee. Prior information was sent to the administrative authorities of the Yekatit 12 hospital about the nature and purpose of the study through a letter from school of Pharmacy, Department of pharmacology and clinical pharmacy, Addis Ababa University. The data were accessed only by the researchers and data collector and every precaution was considered for keeping confidentiality of patient data.
Patient written informed consent form to review their medical records was waived due to the following justifications: personal identifiers of prescriptions were not used in the data collection process and the institutional review board of school of pharmacy, Addis Ababa University believed that this study will not adversely affect the rights and welfare of the subjects. In addition, the research involves no more than minimal risk.
Statistical Analysis
Data were entered using Epi Info version 3.5.1 and analyzed using the Statistical Package for Social Sciences (SPSS) version 20.0 for Windows. Results were expressed as means ± standard deviation (SD), frequencies, and percentages. Chi-square test was used to compare the means of different groups among the study population while the Mann–Whitney U-test was used to compare continuous variables in two groups. Values of P < 0.05 were considered as significant.
Results
Socio-Demographic and Related Profiles
In the current study, medical charts of 255 patients with cardiovascular disease were collected and analyzed. The mean age was 63.54 ± 9.248 years. From the medical charts reviewed, majority of patients were above 60 years of age. More than half (57.3%) of prescriptions were orders for males and almost 80% of the patients were ambulatory (Table 1).
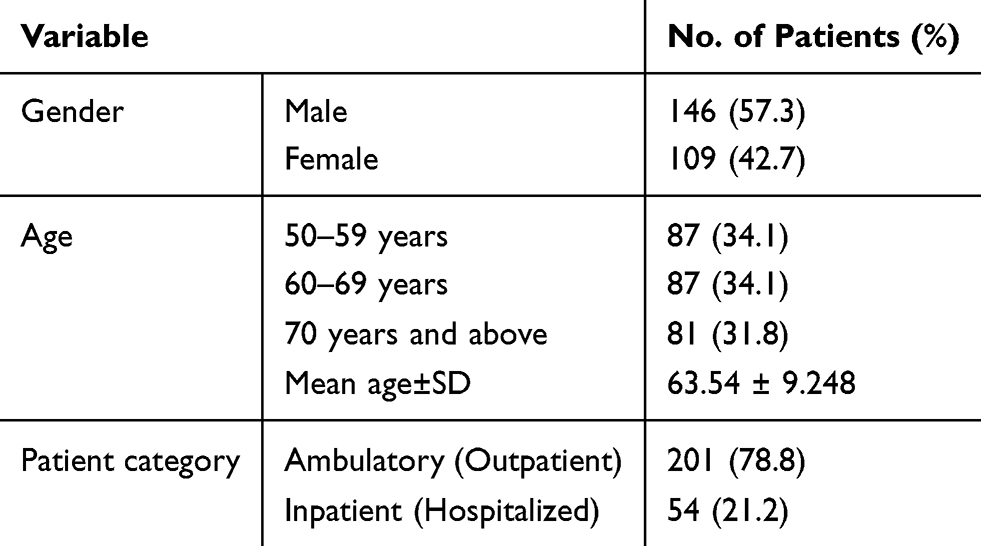 |
Table 1 Socio-Demographic and Related Profiles |
Diagnosis, Commonly Prescribed Drugs and Drug-Drug Interactions
The most common cardiovascular diseases identified were hypertension (46.6%), congestive heart failure (14.5%) and stroke (13.3%). Most frequent co-morbid conditions were endocrine disorders (24.7%), followed by respiratory problems (10.6%) and chronic kidney diseases (9%). The data revealed that at least one co-morbid condition occurred in a majority of patients (68.8%) (Table 2). As indicated in Figure 1, the prevalence of polymorbidity was 71.8% with 1–3 co-morbidity (68.6%) and ≥4 co-morbidities (3.2%). The occurrence of polymorbidity was more frequent in males (76%) than in females (70.4%).
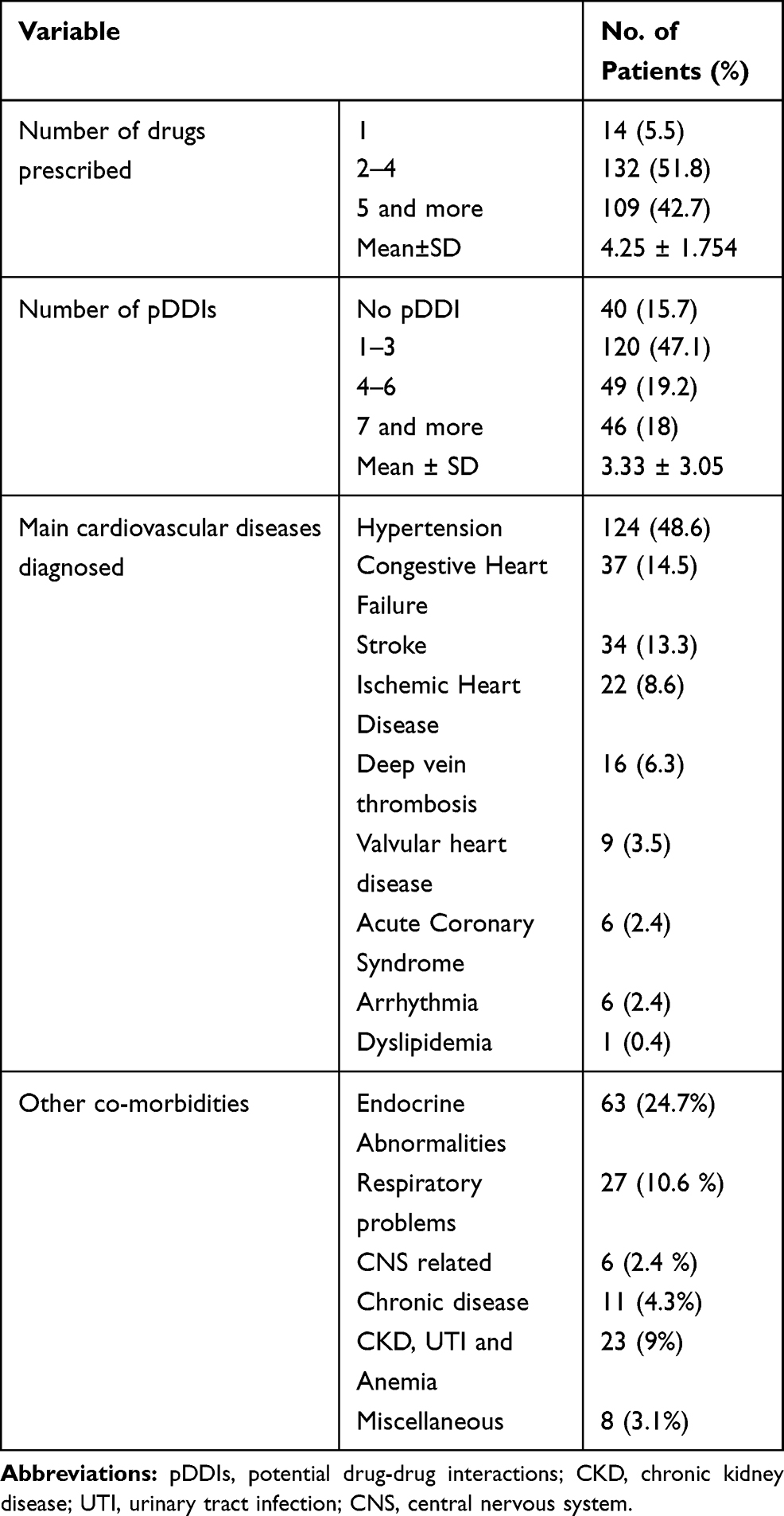 |
Table 2 Diagnosis, Number of Prescribed Drugs and Potential Drug-Drug Interactions |
Most frequently prescribed drugs were aspirin 127 (49.8%), enalapril 122 (47.8%) furosemide 91 (35.7%), nifedipine 90 (35.3%) and spironolactone 82 (32.2%) followed by atenolol 79 (31%) (Figure 2). As shown in Table 2, the average drugs prescribed per prescription was 4.25 ± 1.754 which indicated the practice of polypharmacy in the hospital. Mean number of potential drug-drug interactions was 3.33 ± 3.05 and almost half (47.1%) of the study subjects encountered 1–3 interactions.
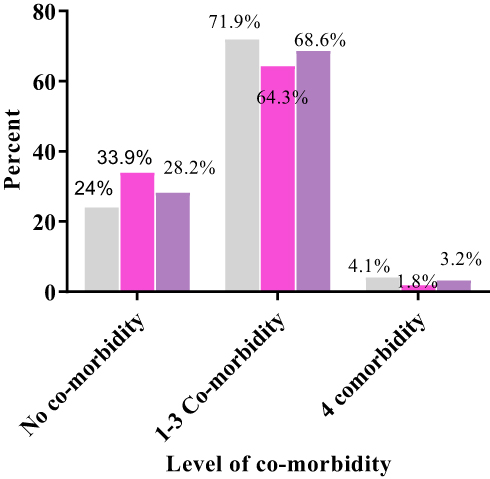 |
Figure 1 Prevalence of Co-morbidity in gender. |



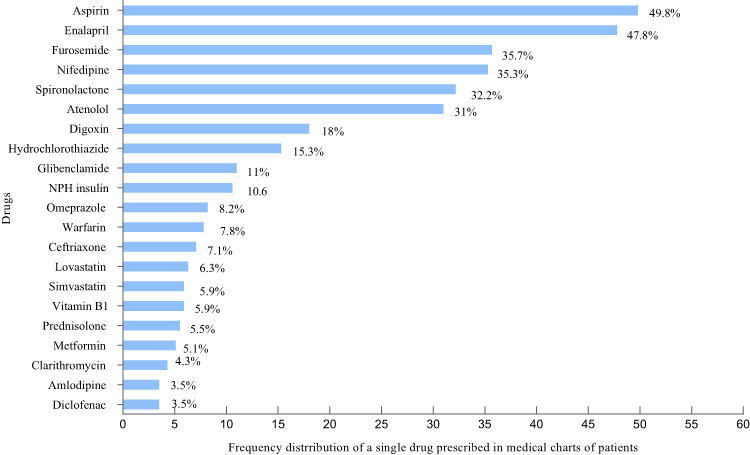 |
Figure 2 Specific drugs prescribed for the management of cardiovascular diseases. |
Prevalence of Polypharmacy
From 255-medical chart records assessed, 5 or more drugs were prescribed in each of the 109 (42.7%) patient charts which indicated the occurrence of polypharmacy in Yekatit 12 hospital. Among 109 patients who took ≥5 drugs concurrently, 65 (44.5%) were males and 44 (40.4%) were females. The prevalence of polypharmacy was high at advanced age; however, the association between polypharmacy and age was statistically insignificant (chi-square; χ2 = 1.291, p = 0.524, phi = 0.071) (Table 3). According to chi-square test for independence, statistically significant association between sex and polypharmacy was not observed (χ2 = 0.287, p = 0.592, phi = −0.042) (Figure 3).
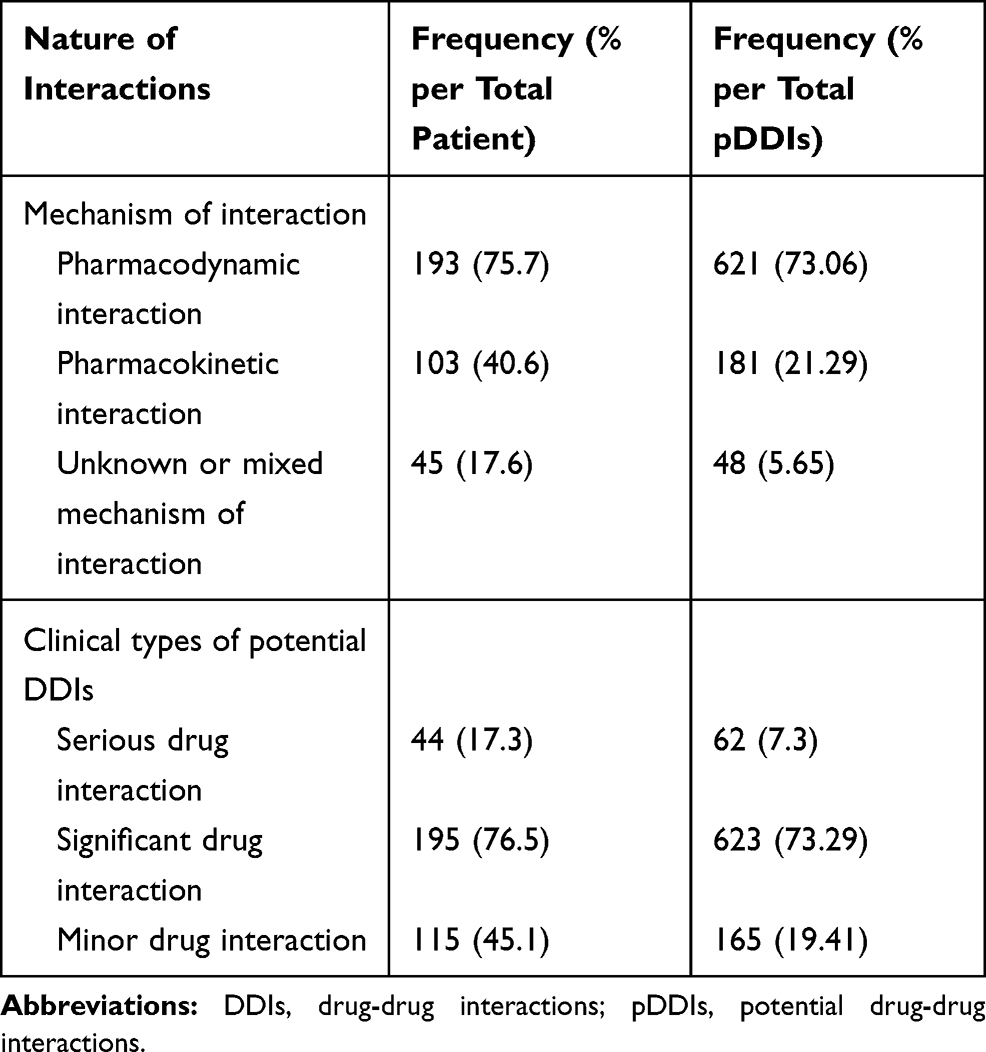 |
Table 3 Nature and Mechanisms of Potential Drug-Drug Interactions |
The assessment of medical records of hospitalized patients revealed that 55.6% of the patients received ≥5 drugs concurrently whereas 39.3% of ambulatory patients received equal number of medications. Polypharmacy was significantly associated with hospitalized patients (chi-square test; χ2 = 3.954, p = 0.047, phi = 0.134) (Figure 3).
The number of medications prescribed per prescription (≥5 drugs per prescription) was higher with polymorbidity (≥4 co-morbidities). According to Mann–Whitney U-test the number of cases of polypharmacy was significantly higher in the presence of polymorbidity (p < 0.001). Forty-five (36.3%) medical charts of hypertensive patients were identified with polypharmacy. However, hypertension was not significantly associated with polypharmacy (χ2 = 3.612, p=0.057, phi= −0.127). On the other hand, 23 (62.2%) congestive heart failure patients’ medical charts were identified with polypharmacy and a chi-square test for independence showed a significant association between congestive heart failure and polypharmacy (χ2 = 5.772, p = 0.016, phi = 0.162) (Figure 3).
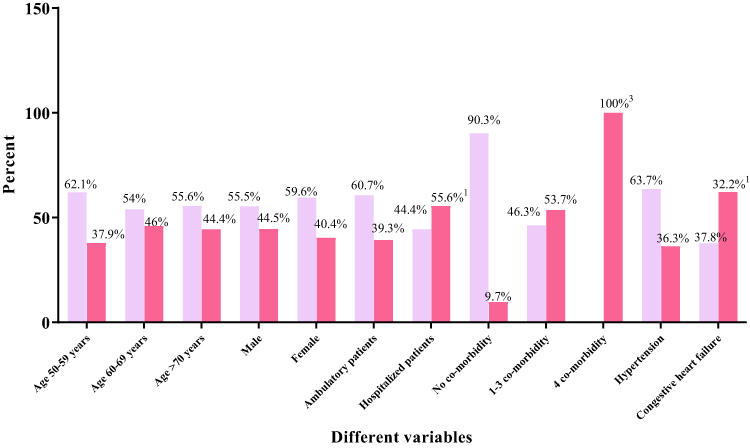 |
Figure 3 Polypharmacy status among different variables. |


Nature and Mechanism of Drug-Drug Interactions
The nature and mechanisms of DDIs are summarized in Tables 3 and 4. Among 850-potential DDIs, pharmacodynamic interactions were the most common constituting 73.06%, followed by pharmacokinetic (21.29%) and mixed (5.65%) interactions. Significant DDIs were most common constituting 73.29%, followed by minor (19.41%) and serious (7.3%) interactions.
 |
Table 4 Different Variables and Potential Drug-Drug Interactions |
Demographic variables and nature of potential DDIs are illustrated in Table 4. In 125 (85.6%) male and 90 (82.6%) female patients’ prescriptions potential DDIs were present. The number of potential DDIs in 60–69 years old age group, ambulatory and hospitalized patients’ medical charts were 77 (88.5%), 171 (85.1%) and 44 (81.5%), respectively. However, the association between DDIs and demographic variables (gender, age and ambulatory or hospitalized patients) was not statistically significant using chi-square test. On the other hand, potential DDIs in patients with congestive heart failure and four-co-morbid conditions and polypharmacy were 100% and 98.2%, respectively. The association between DDIs and congestive heart failure, four-co-morbid conditions and polypharmacy were statistically extremely significant (P = 0.001) using Mann–Whitney U-test (Table 4).
Common Drug Groups
The most frequent potential drug-drug interactions with their respective importance and possible risks are presented in Table 5. The most common drug groups identified were angiotensin-converting enzyme (ACE) inhibitors (enalapril), NSAIDs (low dose aspirin), diuretics (furosemide, hydrochlorothiazide and Spironolactone), ß-blockers (Atenolol), digoxin and calcium channel blocker (Nifedipine), lipid lowering agents (Simvastatin and Lovastatin), proton pump inhibitors (Omeprazole) and prednisolone.
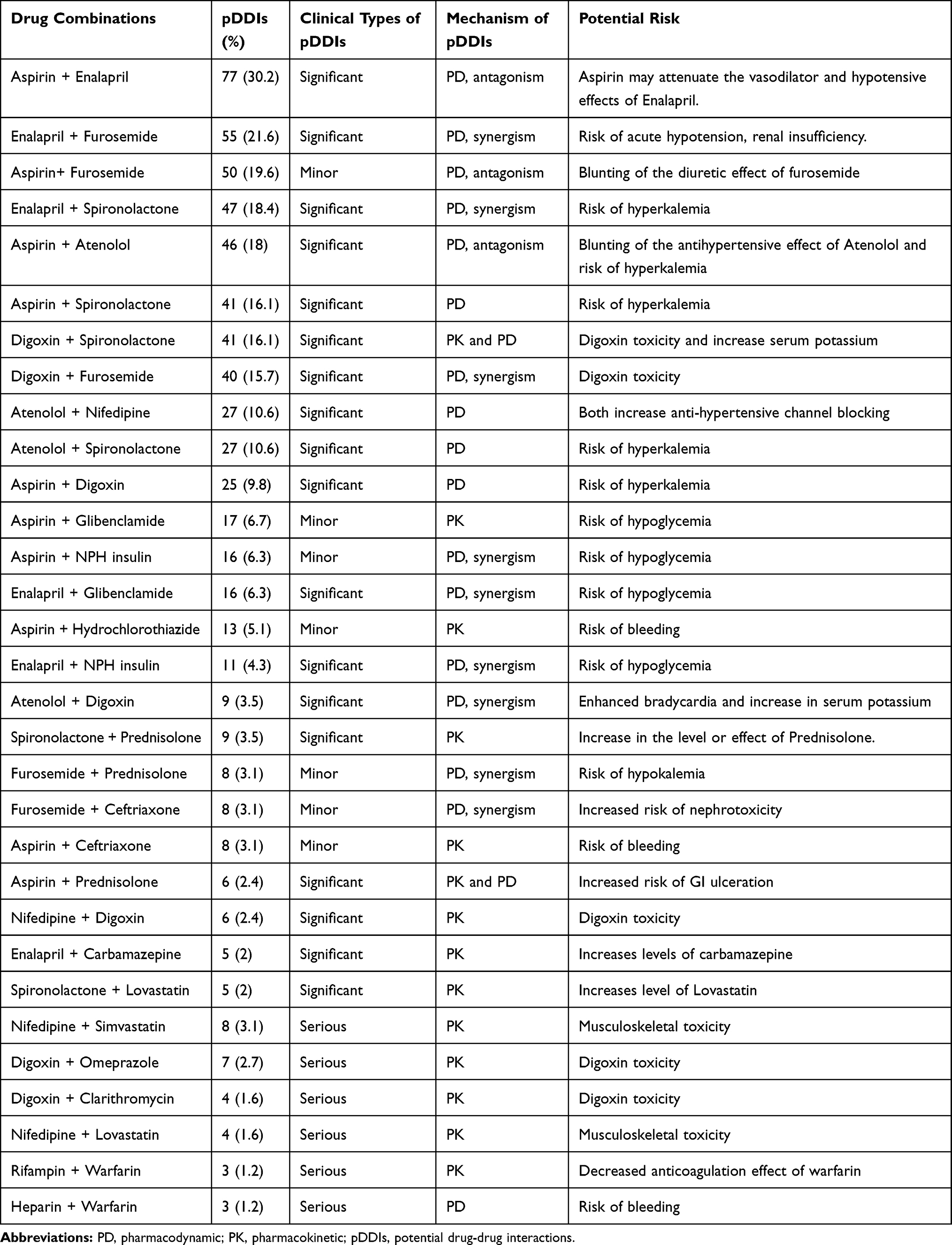 |
Table 5 Potential Drug-Drug Interactions Identified from Medical Records in Yekatit 12 Hospital |
The most commonly identified combination of drugs with potential dug-drug interactions were Aspirin + Enalapril (30.2%), Enalapril + furosemide (21.6%), Aspirin + Furosemide (19.6%), Enalapril + Spironolactone (18.4%), Aspirin + Atenolol (18%), Aspirin + Spironolactone (16.1%), Digoxin + Spironolactone (16.1%) and Digoxin + Furosemide (15.7%).
Discussion
In this study, medical charts of elderly (aged 50 year and above) people with cardiovascular diseases were examined and analyzed for the prevalence of polypharmacy and potential drug-drug interactions. In addition, the nature and mechanisms of drug-drug interactions, most commonly involved combination of drugs and the most frequently occurred potential drug-drug interactions were assessed. The majority of patients with cardiovascular diseases were males (57.3%), which is in line with the fact that men are more prone to heart disease compared to women of a similar age.3 The most common diagnosis identified was hypertension (48.6%) followed by congestive heart failure and stroke. Similarly, hypertension (57.8%) was the most frequent diagnosis found on the study done in Italy on general elderly patients.21 The prevalence (71.8%) of co-morbidity in our study is in line with the prevalence of co-morbidity (35–80%) in other studies on elderly populations.5 The most commonly identified co-morbidities were cardiovascular disease, endocrine abnormalities (diabetes mellitus II) and respiratory problems (pneumonia and chronic obstructive pulmonary disease), which is in line with the previous study in Bosnia and Herzegovina.22 In this study, the mean number of co-morbidity in hospitalized patients was 4.8. The finding of this study is lower than hospitalized patients in Japan which depicted 7.7 mean number of co-morbidity.8
The mean number of drugs per prescription was 4.25 with standard deviation of 1.754 which is comparable to the data reported from previous studies in southern Brazil (4.4 drugs per prescription) and Nigeria (3.8 drugs per prescription).23 The mean number of prescribed drugs in this study is lower than the study in South Africa (7.7) and Bangladesh (7.34).1,24 The maximum number of drugs recorded per patient were 10 which is comparable to the finding of similar studies done in Nigeria and southern Brazil which show a maximum of 8 and 11 drugs prescribed per patient, respectively.1,23
In the current study, prevalence of polypharmacy (42.7%) is comparable with the polypharmacy prevalence reported from previous studies in Indian teaching hospitals (45%), Japan (49%) and southern Brazil (43.1%).7,8,23 The data revealed that prevalence of polypharmacy was not significantly associated with age (P = 0.524) and gender (P = 0.592). However, it was significantly associated with inpatients (P = 0.047) which indicated that hospitalized patients are at a higher risk of polypharmacy compared to ambulatory patients.
Coming to DDIs, both ambulatory and hospitalized patients are at higher risk of potential drug-drug interactions. Majority of potential DDIs were significant (73.29%) in nature and pharmacodynamic (73.06%) in mechanism. According to the present study, prevalence of potential DDIs were not associated with age (P = 0.343) and gender (P = 0.626) which is in agreement with other studies at different settings.23 This study showed that a significant association was observed between congestive heart failure and potential DDIs (P = 0.01). This indicated that patients diagnosed and treated for congestive heart failure are at higher risk of suffering from the adverse effects of DDIs. The prevalence of potential DDIs were also significantly associated with polypharmacy (P = 0.000) and four co-morbidities (P = 0.000) which showed multiple medications and polymorbidity (≥4 co-morbidities) are significant predictors of potential DDIs.23
With respect to specific drugs prescribed, aspirin, enalapril, furosemide, nifedipine and spironolactone were the most frequent which is in line with previous study in Italy.23 The most commonly identified potential DDIs were mainly due to aspirin, enalapril, furosemide, spironolactone, atenolol, digoxin and nifedipine in combination with each another or with other drugs.
The majorities of identified interactions were of significant in nature, pharmacodynamic in mechanism and mainly related to drugs acting on cardiovascular system which is in agreement with findings elsewhere.23 In fact, there are DDI reports in the literature, but there is little agreement among them with respect to the type, nature and clinical importance of interactions. From potential interaction with minor intensity, aspirin and furosemide combination was the most frequently identified one in which the diuretic effect of furosemide could be blunted by the pharmacodynamic antagonism caused by aspirin. An interaction between aspirin with antidiabetic agents (Glibenclamide and NPH insulin) was also common and lead to possible risk of hypoglycemia. In addition, minor interaction was identified between aspirin and hydrochlorothiazide which is pharmacokinetic in mechanism and might lead to bleeding.
The data revealed that significant DDIs were pharmacodynamic in mechanism. Among medication combinations, Aspirin + enalapril, enalapril + furosemide, aspirin + atenolol, aspirin + spironolactone and digoxin + furosemide were the most commonly encountered combination with significant interactions. Such types of interaction require close monitoring of the clinical outcome or possible risks. Aspirin might attenuate vasodilator and hypotensive effects of enalapril while an interaction between enalapril and furosemide might have a combined risk of acute hypotension and renal insufficiency.
Even though diuretics are widely used to optimize therapeutic effects and diminish adverse events, loop and thiazide diuretics largely contribute to moderate intensity interactions. The interaction between loop and thiazide diuretics is pharmacodynamic interaction and leads to loss of drug efficacy.
Nifedipine + simvastatin, digoxin + omeprazole and digoxin + clarithromycin combinations were the most common serious intensity pharmacokinetic interactions. A combination of nifedipine and simvastatin affects the metabolism and increases the level of simvastatin which lead to musculoskeletal toxicity while those interactions between digoxin and omeprazole or clarithromycin increase level of digoxin and lead to digoxin toxicity. Another serious pharmacodynamic interaction identified was between heparin and warfarin which ultimately lead to increased anticoagulation (higher incidence of bleeding). Co-administration of drugs which are potentially interacting might increase the number of adverse events which can be confused with the severity of co-morbidities. The consequences of such interactions include a longer duration of treatment period with administration of more drugs to patients, resulting in a higher probability of drug-drug interactions.
Conclusion
The prevalence of polypharmacy was found associated with increased number of co-morbidity and inpatient prescriptions. The prevalence of total and serious potential drug-drug interactions were 84.3% and 17.3%, respectively. The majority of interactions were pharmacodynamic in mechanism (73.06%) and significant in nature (73.29%). The prevalence of potential drug-drug interactions were significantly associated with polypharmacy and polymorbidity (≥4 co-morbidities). Based on the finding in the current study, drugs acting on cardiovascular system including low dose aspirin, diuretics, angiotensin-converting enzyme inhibitors, calcium channel blockers, beta-blockers and digoxin were most commonly and frequently implicated in potential drug-drug interactions. A higher incidence of polypharmacy and increased risk of potential drug-drug interactions in elderly people with cardiovascular disease are major therapeutic issues at Yekatit 12 hospital.
Disclosure
The authors have no conflict of interest to disclose.
References
1. Fadare OJ, Agboola MS, Opeke AO, Alabia AR. Prescription pattern and prevalence of potentially inappropriate medications among elderly patients in a Nigerian rural tertiary hospital. Ther Clin Risk Manag. 2013;9:115–120. doi:10.2147/TCRM.S40120
2. Central statistical agency of Ethiopia: the 2007 national statistics. Available from: http://ethiopianreview.com/pdf/001/Cen2007_firstdraft(1).pdf.
3. Al-Amin M, Zinchenko A, Rana S, Nasir Uddin MM, Pervin S. Study on polypharmacy in patients with cardiovascular diseases. JAPS. 2012;2(12):53–60.
4. Mamun K, Lein CTC, Goh-Tan C, Ang WST. Polypharmacy and inappropriate medication use in Singapore nursing homes. Ann Acad Med. 2004;33(1):49–52.
5. Nobili A, Licata G, Salerno F, et al. Association between clusters of diseases and polypharmacy in hospitalized elderly patients: results from the REPOSI study. EJIM. 2011;22:597–602.
6. Hovstadius B, Hovstadius K, Astrand B, Petersson G. Increasing polypharmacy - an individual based study of the Swedish population 2005–2008. BMC Clin Pharmacol. 2010;10:16. doi:10.1186/1472-6904-10-16
7. Harugeri A, Joseph J, Parthasarathi G, Ramesh M, Guido S. Prescribing patterns and predictors of high-level polypharmacy in the elderly population: a prospective surveillance study from two teaching hospitals in India. Am J Geriatr Pharmacother. 2010;8(3):271–281. doi:10.1016/j.amjopharm.2010.06.004
8. Mizokami F, Koide Y, Noro T, Furuta K. Polypharmacy with common diseases in hospitalized elderly patients. Am J Geriatr Pharmacother. 2012;10(2):123–128. doi:10.1016/j.amjopharm.2012.02.003
9. Hilmer SN. The dilemma of polypharmacy. Aust Prescr. 2008;31(1):2–3. doi:10.18773/austprescr.2008.001
10. Papapetrou I, Jelastopulu E, Symeonidou E, Kleridou M, Floridou D, Charalambous G. Investigation of polypharmacy and rational prescribing in elderly patients in a health centre of Nicosia, Cyprus. China-USA Bus Rev. 2012;11(12):1587–1594.
11. Venturini CD, Engroff P, Ely LS, et al. Gender differences, polypharmacy and potential pharmacological interactions in the elderly. Clinics. 2011;66(11):1867–1872. doi:10.1590/s1807-59322011001100004
12. Rossi MI, Young A, Robert Maher R, et al. Polypharmacy and health beliefs in older outpatients. Am J Geriatr Pharmacother. 2007;5(4):317–323. doi:10.1016/j.amjopharm.2007.12.001
13. Steinman MA. Polypharmacy and the balance of medication benefits and risks. Editorial comment. Am J Geriatr Pharmacother. 2007;5(4):314–316. doi:10.1016/j.amjopharm.2007.12.009
14. Nguyen JK, Fours MM, Kotabe ES, Eunice LE. Polypharmacy as a risk factor for adverse drug reactions in geriatric nursing home residents. Am J Geriatr Pharmacother. 2006;4(1):36–41. doi:10.1016/j.amjopharm.2006.03.002
15. Nidhi S. Concept of drug interaction. IRJP. 2012;3(7):120–122.
16. Gebretsadik Z, Gebrehans M, Getnet D, Gebrie D, Alema T, Belay Y. Assessment of drug-drug interaction in Ayder comprehensive specialized Hospital, Mekelle, Northern Ethiopia: a retrospective study. Hindawi BioMed Res Int. 2017;2017.
17. Murtaza G, Khan MYG, Azhar S, Khan SA, Khan TM. Assessment of potential drug-drug interactions and its associated factors in the hospitalized cardiac patients. Saudi Pharm J. 2016;24:220–225. doi:10.1016/j.jsps.2015.03.009
18. Available from: https://reference.medscape.com/drug-interactionchecker. Accessed August 12, 2019
19. Clarke R, Ross S, Walker T, Woods D Polypharmacy; BPAC Polypharmacy Report. 2006. Available from: http://bpac.org.nz.pdf/.
20. Doubova VS, Reyes-Morales H, Torres-Arreola L, Suarez-Ortega M. Potential drug-drug and drug-disease interactions in prescriptions for ambulatory patients over 50 years of age in family medicine clinics in Mexico City. BMC Health Serv Res. 2007;7:147–155. doi:10.1186/1472-6963-7-147
21. Nobili A, Licata G, Salerno F, et al. Polypharmacy, length of hospital stay, and in-hospital mortality among elderly patients in hospital internal medicine wards. the REPOSI study. EJCP. 2011;67(5):507–519.
22. Trumic E, Pranjic N, Begic L, Bečić F. Prevalence of polypharmacy and drug interaction among hospitalized patients: opportunities and responsibilities in pharmaceutical care. Mat Soc Med. 2012;24(2):68–72. doi:10.5455/msm.2012.24.68-72
23. Teixeira JV, Crozatti MTL, Dos Santos CA, Romano-Lieber NS. Potential drug-drug interactions in prescriptions to patients over 45 years of age in primary care, Southern Brazil. PLoS One. 2012;7(10):1–6. doi:10.1371/journal.pone.0047062
24. Kapp PA, Klop AC, Jenkins LS. Drug interactions in primary health care in the George subdistrict, South Africa: a cross-sectional study. S Afr Fam Pract. 2013;55(1):78–84.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.