Back to Journals » Journal of Pain Research » Volume 12
Survey on chronic disabling low back pain among care workers at nursing care facilities: a multicenter collaborative cross-sectional study
Authors Yoshimoto T ![]() , Oka H
, Oka H ![]() , Fujii T
, Fujii T ![]() , Kawamata K
, Kawamata K ![]() , Kokaze A
, Kokaze A ![]() , Koyama Y, Matsudaira K
, Koyama Y, Matsudaira K ![]()
Received 25 September 2018
Accepted for publication 18 February 2019
Published 21 March 2019 Volume 2019:12 Pages 1025—1032
DOI https://doi.org/10.2147/JPR.S188125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Takahiko Yoshimoto,1,2 Hiroyuki Oka,2 Tomoko Fujii,2 Kayo Kawamata,2 Akatsuki Kokaze,1 Yoshiko Koyama,3,4 Ko Matsudaira2
1Department of Hygiene, Public Health and Preventive Medicine, Showa University School of Medicine, Tokyo, Japan; 2Department of Medical Research and Management for Musculoskeletal Pain, 22nd Century Medical & Research Center, Faculty of Medicine, The University of Tokyo, Tokyo, Japan; 3Department of Physical Therapy, Faculty of Health Sciences, Kinjo University, Ishikawa, Japan; 4Ishikawa Occupational Health Support Center, Ishikawa, Japan
Purpose: Care workers at nursing care facilities have high rate of low back pain (LBP). Although increasing evidence has revealed the important role of psychosocial factors in chronic LBP, factors associated with chronic LBP interfering with work have not been fully investigated in Japanese workers at nursing care facilities. The present study aimed to determine the prevalence of chronic LBP interfering with work and related factors of chronic LBP including psychosocial factors, among workers at nursing care facilities.
Material and methods: Eligible participants in the present study were Japanese workers at 95 nursing care facilities in Ishikawa Prefecture (n=2,242). Of these, 1,345 participants completed a self-administered questionnaire that included the following items: individual characteristics, severity of LBP, sleep problem, fear-avoidance beliefs (Tampa Scale for Kinesiophobia: TSK), STarT Back Screening Tool (SBST), fatigue, somatizing tendency, and work-related stress such as job satisfaction, job demand, interpersonal stress at work, and social support. The logistic regression analysis was used to assess factors associated with chronic disabling LBP.
Results: Of participants who completed the questionnaires, 159 (11.8%) reported chronic LBP that interfered with their work. The multivariable analysis of related-factors of chronic disabling LBP found statistically significant associations with the following: high score of psychological subscale in SBST (adjusted odds ratio [aOR]: 5.83, 95% confidence interval [CI]: 3.55–9.59), high score of TSK (aOR: 1.08, 95% CI: 1.05–1.13), and high somatizing tendency (aOR: 2.07, 95% CI: 1.31–3.23).
Conclusion: Psychological factors, including fear-avoidance beliefs or somatizing tendency, showed significant association with chronic LBP that interfered with work, among workers at nursing care facilities. Our results suggest that these factors would need to be considered in addition to screening for the risk factors of LBP chronicity by SBST when evaluating workers with chronic disabling LBP.
Keywords: low back pain, care worker, nursing care facility, psychological factor, fear-avoidance, somatizing tendency
Introduction
Low back pain (LBP) is one of the most common musculoskeletal health problems worldwide and is the leading cause of years lived with disability among 291 diseases and injuries globally.1 Care workers at nursing care facilities who provide direct care, face a number of risk factors for LBP such as psychological job demand or interpersonal stress with staffs/users of nursing care facilities,2,3 in addition to physical workloads that are already well-understood. These care workers actually have high prevalence of LBP.4,5 According to occupational disease surveillance in Japan, the number of workers who cannot do social activities for at least 4 consecutive days because of LBP has increased annually in the health care/nursing-care fields.6 LBP has been shown to be an independent predictor for dropout from eldercare work among care workers.7 Therefore, an appropriate strategy for preventing LBP in the workplace is urgently required.
Globally, the association between LBP chronicity with physical (such as manual handling) and psychosocial (such as work-related stress and/or depression) factors has been recognized.8 European Guidelines for prevention of LBP indicated that a mere approach for ergonomic factors does not necessarily lead to the prevention of LBP,9 which was similarly shown in a subsequent systematic review.10 Moreover, Western occupational health guidelines for the management of LBP have emphasized that psychosocial factors, in addition to occupational ergonomic factors, should be considered in the management of chronic LBP with disability.11 Japan epidemiological research of Occupation-related Back pain (JOB) study, a prospective cohort research aimed at examining the risk factors of LBP that interferes with work, reported about the involvement of psychosocial factors in LBP chronicity. Such factors include interpersonal stress at work, job satisfaction, support from supervisors, depression, and somatic symptoms.12,13 Moreover, it has recently been reported that sleep problems, including night shift duration or quality of sleep, are associated with increased likelihood of disabling LBP among workers.14
To assess and stratify patients with LBP according to the risk of LBP chronicity, the STarT (Subgrouping for Targeted Treatment) Back Screening Tool (SBST) has been globally used.15 To classify as high-risk chronic LBP group, five psychological subscale items of the nine overall items in the SBST, are regarded as important.15 The higher the score of the psychological subscale items, the more serious the psychological problem. Previously, Matsudaira et al indicated that stratification of risk groups by Japanese version of the SBST may help predict the 6-month prognosis of LBP.16
Although some studies in the United States and Europe have investigated the relationship between LBP and psychosocial work-related factors among workers at care facilities,2,3,5 little research of a similar nature has been conducted in Asian countries, including Japan. Moreover, most of these previous studies evaluated the psychosocial work environment such as interpersonal stress or support by a boss. However, there is little study about care workers, among whom, in addition to these work environmental factors, investigated psychosocial factors comprehensively including stress response (fatigue and somatizing tendency) or pain-related beliefs. Considering the increasing number of nursing care facilities with the aging society in Japan, determination of the prevalence and related-factors of chronic LBP among workers at these facilities is required for the management of occupational LBP. The present study was designed to investigate the prevalence of chronic LBP that interfered with work among workers at nursing care facilities and to clarify whether various psychosocial factors are associated with chronic disabling LBP.
Materials and methods
Study populations
The present study was designed as a multicenter collaborative cross-sectional study. The survey was conducted between July 1 and August 31, 2013. All procedures were approved by the research ethics committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (No. 1264) and the medical/ethics review board of the Japan Labour Health and Welfare Organization. Written informed consent was obtained from all participants prior to the initiation of the study. Eligible participants in the present study were Japanese workers at 95 nursing care facilities in Ishikawa Prefecture (n=2,242), and a non-anonymous, self-administered questionnaire was distributed to each employee. All surveyed subjects in the present study were care workers who provide direct care to dependent individuals in their respective nursing facilities. Employees who were engaged in services that were not directly related to the health-related care (including administrators, cooking staff, etc.) were not eligible for the present study. Respondents who provided answers in the questionnaires were 1,704 workers (response rate: 76%). Filled out questionnaires were sent in sealed envelopes through occupational health staff to the researchers. All participants were assured of voluntary participation, while supervisors and occupational health staff were disallowed from opening the sealed envelopes. In total, 1,345 workers completed the self-administered questionnaire with no missing data (completion rate: approximately 60%) and were included in the analysis.
Chronic disabling LBP
Severity of LBP, evaluated by the respondents, was indicated according to four grades: grade 0 (no LBP), grade 1 (LBP not interfering with work), grade 2 (LBP interfering with work), and grade 3 (LBP interfering with work and leading to sick leave). The grades were determined with modification of Von Korff’s grading method.17 LBP was defined as pain in the lower back lasting for more than 1 day and experienced during the preceding 4 weeks, with reference to the standard definition of LBP proposed by Dionne et al.18 Pain associated with menstruation, pregnancy, or experienced during a feverish illness was excluded. A diagram showing the lower back area between the inferior costal margin and gluteal folds19 was provided within the questionnaire. Chronic disabling LBP in the present study was defined as LBP that interfered with work, regardless of work attendance (grade 2 or 3), and persisting for at least 3 months.13
Other variables
The self-administered questionnaire included questions regarding sex, age, sleep problems, fear-avoidance beliefs, and individual and work-related psychosocial factors.
Sleep problems were evaluated using questions about the quantity and quality of sleep in the past month.20 Sleep duration was divided into <5 hrs, 5–6 hrs, and >6 hrs, and sleep duration disability was defined as sleep duration of <6 hrs. Difficulty initiating sleep was defined as taking more than 30 mins to fall asleep. Difficulty maintaining sleep and early morning awakening were defined as nocturnal awakenings or early morning awakenings occurring ≥3 times per week. The quality of sleep was assessed using the sum of scores (range: 0–3) of the three symptoms above, while the deterioration in sleep quality was considered to have occurred if the score was high. For these questions (Japanese version), the validity and reliability have not been assessed; however, they were adapted and modified from those used widely in epidemiological studies on sleep.21,22
We used the SBST to assess the psychological factors related to LBP chronicity.15 The SBST is a simple prognostic questionnaire that enables clinicians to identify modifiable psychological risk factors for back pain disability. Of the nine overall items in the SBST, five psychological subscale items were used, and the sum scores were classified into three groups (0–2, 3, 4–5).16,23 The Japanese version of the SBST has been translated and linguistically validated,24 and its psychometric properties have been assessed.25 Cronbach’s alpha coefficient of the psychological subscale (5 items) used in the present study was 0.66. The area under the curve for the subscale against reference standard questionnaires, as the evaluation of the discriminant validity, ranged from 0.67 to 0.79, mostly indicating acceptable discriminative ability.
The Tampa Scale for Kinesiophobia (TSK) is a 17-item self-reported measure originally developed to discriminate between non-excessive fear and phobia among patients with chronic musculoskeletal pain. TSK is widely used to assess pain-related fear of movement or re-injury in patients with musculoskeletal complaints. We evaluated kinesiophobia using a short-form version of the TSK (TSK-11) which was developed in 2005.26 The TSK-11 employs a 4-point Likert scale, with scoring options ranging from 1 (strongly disagree) to 4 (strongly agree). The TSK-11 has been translated into Japanese and linguistically validated in our previous studies.27,28 Internal consistency was demonstrated with Cronbach’s alpha statistics of 0.919. For concurrent validity, significantly strong correlations were demonstrated between the TSK-11 and Pain Catastrophizing Scale (r=0.602–0.680).
Work-related stress was assessed using the Brief Job Stress Questionnaire (BJSQ),29 which was developed by a research working group established by the Japan Labour Health and Welfare Organization. Question items for the BJSQ were composed on the basis of the various standard questionnaires such as the Job Content Questionnaire,30 National Institute for Occupational Safety and Health,31 the Screener for Somatoform Disorders,32 and the Subjective Well-being Inventory.33 The BJSQ consisted of 57 items and provided 19 work-related stress factors. Among various factors, we evaluated the following: job satisfaction (1 item), interpersonal stress at work (3 items), monotonous work (1 item), support by supervisors (3 items), feeling fatigue (3 items), and somatizing tendency (11 items). The questionnaire has been demonstrated to have internal consistency, reliability, and criterion-related validity.34 For each factor above, standardized scores were developed on a 5-point scale ranging from 1 (lowest) to 5 (highest) based on a sample of more than 10,000 Japanese workers. The lowest or highest of the 5-point scale (different by question), was defined as stressful.35
Statistical analyses
Demographic and clinical characteristics were analyzed using Student’s t-test for continuous variables and chi-square test for categorical variables. The univariate and multivariable logistic regression analyses were used to assess the relationship between the psychosocial factors and chronic LBP that interfered with work. In the present study, we identified 159 subjects with chronic disabling LBP as the number of event. Number of confounding variables that could be included in the logistic regression analysis was almost the number of events divided by 10; that is, in this case, confounding factors that could be used in the model were about 15 factors. Based on the above, the following variables were included in the final regression model: sex, age, sleep time, sleep quality, job satisfaction, SBST, interpersonal stress at work, monotonous work, support by a supervisor, feeling fatigue, somatizing tendency, and TSK. Age and TSK score were adjusted for in the model as continuous variables, while the other variables were included as categorical variables. The variance inflation factor (VIF) was used to check for multicollinearity in the model. A P-value <0.05 was considered statistically significant (two-sided). All statistical analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC).
Results
Among 1,704 respondents to the questionnaire, 359 participants were excluded due to missing data on variables in the present study. Thus, 1,345 participants were ultimately included in the analysis. The proportion of gender among the excluded respondents was that 20.2% were men and 79.8% were women. These results were similar to the data of the subjects who were included (25.9% for men and 74.1% for women). Mean age (±SD) in the excluded respondents was 43.7 (±12.5) years. They were a bit older than the included subjects (39.4±11.3 years).
Of included participants, 11.8% reported chronic LBP interfering with work. The proportion of the grade of LBP severity among chronic disabling LBP was 0% (grade 0), 0% (grade 1), 88.7% (grade 2), and 11.3% (grade 3). The proportion among non-chronic disabling LBP was 31.9% (grade 0), 63.7% (grade 1), 3.7% (grade 2), and 0.7% (grade 3). Results of the comparison of characteristics between participants with and without chronic disabling LBP are shown in Table 1. Participants with chronic LBP interfering with work were significantly older compared to those without chronic disabling LBP. The rate of high SBST score was higher in those with chronic disabling LBP. TSK score, which indicated the degree of kinesiophobia, was significantly higher in those with chronic disabling LBP relative to those without chronic disabling LBP.
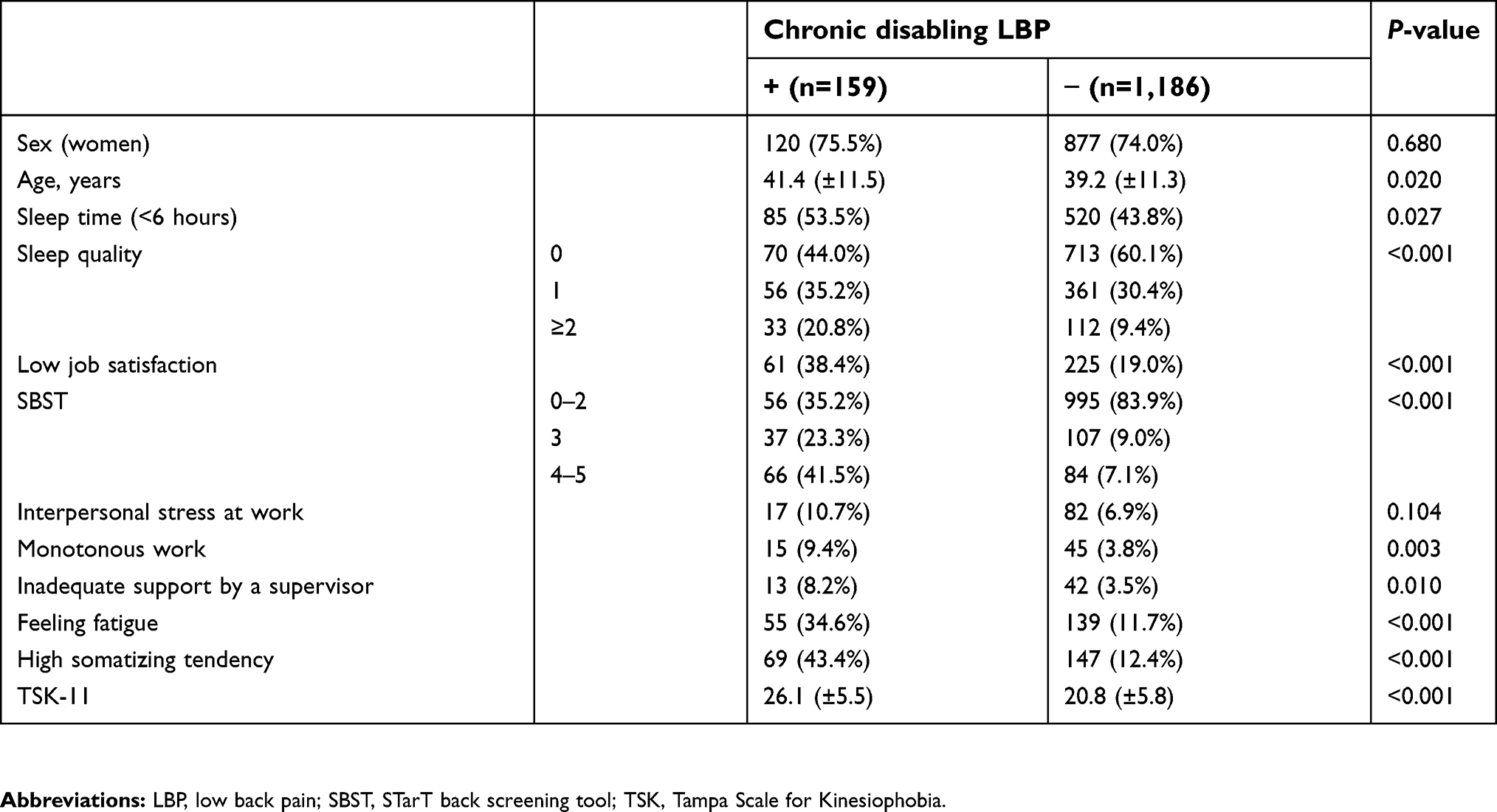 | Table 1 Characteristics of the participants with or without chronic disabling low back pain |
Crude and adjusted odds ratios (aORs) of having chronic LBP interfering with work and the 95% confidence intervals (CIs) are shown in Table 2. From the results of the univariate logistic regression analysis, age, sleep time, sleep quality, job satisfaction, SBST score, monotonous work, support by a supervisor, feeling fatigue, high somatizing tendency, and TSK score were significantly associated with chronic LBP that interfered with work. In the multivariable logistic regression model, the VIF values for age, sleep time, sleep quality (≥2 scores), low job satisfaction, SBST (≥4 scores), interpersonal stress at work, monotonous work, inadequate support by a supervisor, feeling fatigue, high somatizing tendency, and TSK-11 were 1.05, 1.05, 1.06, 1.21, 1.26, 1.16, 1.14, 1.13, 1.26, 1.34, and 1.26, respectively. However, none of the VIF values exceeded 10, which indicates that there was no collinearity in the model.36 In the logistic regression model in the present study, the area under the curve (AUC) of receiver-operating characteristics curve analysis was 0.813, which indicated that the model fitted well (AUC>0.8). At the multivariable analysis, the several explanatory factors, including SBST score ≥4 (aOR: 5.83, 95% CI: 3.55–9.59), high somatizing tendency (aOR: 2.07, 95% CI: 1.31–3.23), and TSK score (aOR: 1.08, 95% CI: 1.05–1.13), were significantly associated with chronic LBP interfering with work.
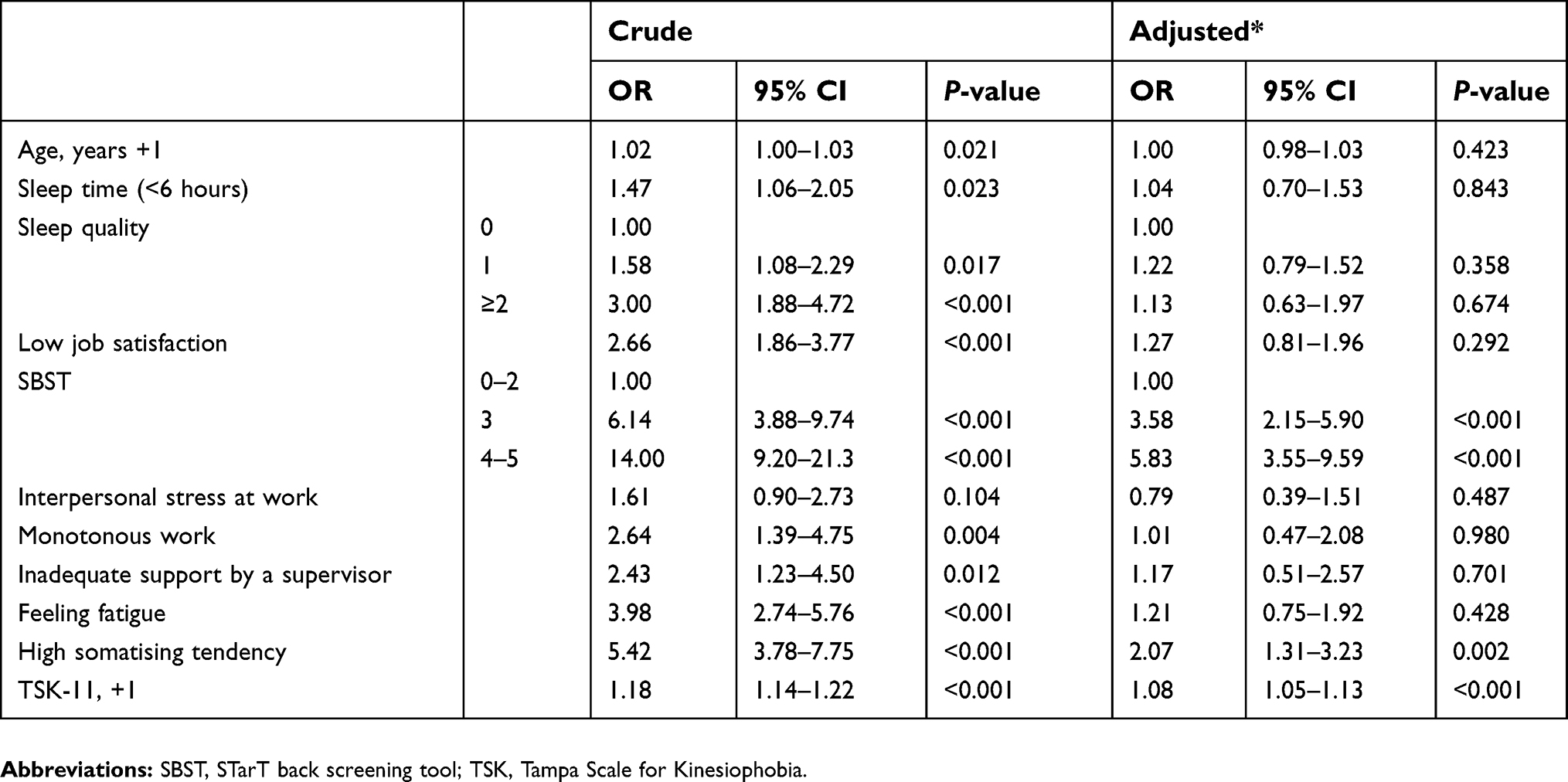 | Table 2 Association between chronic disabling low back pain and related factors from logistic regression model |
Discussion
This multicenter collaborative cross-sectional study determined the prevalence of chronic LBP that interfered with work among workers at nursing care facilities, and the association between psychosocial factors and chronic disabling LBP. Of these participants, more than 10% suffered from LBP that interfered with work and persisted for at least 3 months. Multivariable analysis showed that the factors associated with chronic disabling LBP were high SBST and TSK scores, and high somatizing tendency. To the best of our knowledge, this is the first study to investigate associated psychosocial factors of chronic disabling LBP in Japanese workers at nursing care facilities.
In the present study, severity of LBP was classified from the standpoint of disability at work,13 with reference to the Chronic Pain Grade indicated in the original paper.17 We limited the subjects to care workers, and focused on the work-related musculoskeletal disorder in the present study. Recently, in the workplace, it has been considered problematic that LBP is not only a common reason for absenteeism, but it also leads to decreased work productivity (known as presenteeism).37 This implies that it is more important whether there is LBP interfering with work than merely the presence or absence of LBP. For these reasons, we used the LBP severity grade that considered disability at work, with modification of the Von Korff’s grading method.17
We found high SBST score to be an independent variable of chronic LBP that interfered with work. SBST was developed as a screening tool and a prognostic indicator of back pain for clinical decision-making in primary care settings in the UK.15 SBST stratifies subjects into three risk groups based on the modifiable prognostic factors of LBP. The stratified management care, based on the SBST risk classification, is clinically and economically beneficial for individuals with LBP.38,39 In the present study, 41.5% of the subjects with persistent LBP were high-risk group, defined as psychological scores of ≥4 points, compared to 7.1% in subjects without persistent LBP. These data imply that psychological factors were implicated with persistent LBP in the workers at nursing care facilities. In subjects with LBP, SBST has been reported as a useful tool to predict 6-month pain and disability outcomes, including LBP chronicity.16 At nursing care facilities, screening subjects with poor prognosis of LBP using SBST may be useful in preventing chronic disabling LBP.
Our result indicated that kinesiophobia was significantly associated with chronic disabling LBP among workers at nursing care facilities. People may avoid movements or activities based on excessive fear that pain may bring about additional functional restriction.40 Avoidance of physical activities by fear of movement (kinesiophobia) can result in muscle weakness and dysfunction, which may partly affect or lead to delay in recovery. This repeated cycle of fear of movement and avoidance behaviors may be closely linked with the chronicity of the condition, resulting in disability. Fear avoidance beliefs (FABs) have been reported as an important risk factor of LBP chronicity.41 FABs have also been reported as the most useful factor for predicting recovery in patients with acute LBP.42
Recently, Wakaizumi et al reported the significant association between high FABs (assessed using TSK) and chronic pain in Japanese white-collar workers.43 This study supports our results, showing the association between FABs and chronic LBP. Considering our result and previous studies, early intervention to reduce FABs, such as cognitive behavioral therapy or activity pacing strategy may avoid the chronicity (delayed recovery) of LBP. However, overactivity and endurance behavior44 are also important factors which could lead to the development and maintenance of chronic pain from the standpoint of the avoidance-endurance model.45 Recently, it has been indicated that differences in activity patterns including avoidance and overactivity could affect the outcome in patients with pain.46,47 Because we did not assess overactivity and endurance behavior in the present study, further study including the assessment of activity pattern is needed to provide the individually targeted intervention in those suffering from LBP.
In the present study, the results indicated that high somatizing tendency was related to chronic LBP that interfered with work. Somatizing tendency is a predisposition to be more aware of and to worry about common somatic symptoms.48 The somatizing tendency has been shown to be associated with musculoskeletal pain,49 and absence from work.50 Previous studies have indicated that somatizing tendency has a role in the progression to LBP chronicity8 and the treatment outcome in patients with LBP.51 Matsudaira et al reported that somatizing tendency (assessed using the BJSQ) predicted the development of persistent LBP in individuals with mild LBP.13 Individuals with LBP who are affected by psychosocial factors might complain about various somatic symptoms; therefore, clinical practitioners may need to conduct a careful medical interview about such complaints.
There are some limitations in the present study. First, causality regarding the influences between LBP and psychosocial factors cannot be inferred because of the cross-sectional study design. However, Matsudaira et al reported, in a two-year prospective cohort study, that psychological factors such as somatizing tendency were associated with occupational LBP chronicity.13 Further researches at nursing care facilities including prospective cohort study will be needed. Second, the participants in the present study were workers at 95 nursing care facilities in Ishikawa Prefecture, and inclusion of study participants was not based on random sampling, but volunteer-based; so, our results are not necessarily representative of the Japanese population. Also, the use of non-anonymized questionnaire at the workplace might have made data collection difficult (completion rate 60%). Thus, selection bias might have influenced our results to some degree. The possibility of information bias such as recall bias cannot be denied also. Finally, our results showed that chronic LBP was affected by individuals’ psychological factors; however, as the etiology of LBP is multifactorial, confounding factors that were not considered in our study, including overactivity and endurance behavior, working hours, family environment, or socioeconomic status, might affect our findings.
Conclusion
This multicenter collaborative study indicated that psychological factors such as kinesiophobia or somatizing tendency, and high score of SBST were associated with chronic disabling LBP among care workers at nursing care facilities. Although further prospective study is needed to clarify the causality, it may be necessary to take such psychological factors into account to prevent chronic disabling LBP at nursing care facilities.
Ethics approval and informed consent
This study was approved by the research ethics committee of the Graduate School of Medicine and Faculty of Medicine at the University of Tokyo (No. 1264) and the medical/ethics review board of the Japan Labour Health and Welfare Organization. Written informed consent was obtained from all participants prior to the initiation of the study.
Acknowledgments
This study was supported by a grant from Industrial Disease Clinical Research Grants (No. 14020301). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
KM reports grants from the Ministry of Health, Labor and Welfare during the conduct of the study; grants and personal fees from AYUMI Pharmaceutical Corporation, Nippon Zoki Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd, Shionogi & Co., Ltd., Eli Lilly Japan, Astellas Pharma Inc., Toto Ltd., Eisai Co., Ltd., Teijin Pharma Limited, Japan Inc., and Hisamitsu Pharmaceutical Co., Inc.; personal fees from Pfizer Inc., Janssen Pharmaceutical K.K., Kaken Pharmaceutical Co., Ltd., Mochida Pharmaceutical Co., Ltd., and Daiichi Sankyo Company, Limited; grants from Sompo Holdings, Inc., MTG, NuVasive Japan , and Murata Manufacturing Co., Ltd.; grants from Okamura Corporation; and non-financial support from Trunk Solution Co., Ltd. outside the submitted work. The other authors report no conflicts of interest in this work.
References
1. Buchbinder R, Blyth FM, March LM, Brooks P, Woolf AD, Hoy DG. Placing the global burden of low back pain in context. Best Pract Res Clin Rheumatol. 2013;27(5):575–589. doi:10.1016/j.berh.2013.10.007
2. Dhaini SR, Zuniga F, Ausserhofer D, et al. Care workers health in Swiss nursing homes and its association with psychosocial work environment: a cross-sectional study. Int J Nurs Stud. 2016;53:105–115. doi:10.1016/j.ijnurstu.2015.08.011
3. Gold JE, Punnett L, Gore RJ. ProCare research team. Predictors of low back pain in nursing home workers after implementation of a safe resident handling programme. Occup Environ Med. 2017;74(6):389–395. doi:10.1136/oemed-2016-103930
4. Alexopoulos EC, Burdorf A, Kalokerinou A. A comparative analysis on musculoskeletal disorders between Greek and Dutch nursing personnel. Int Arch Occup Environ Health. 2006;79(1):82–88. doi:10.1007/s00420-005-0033-z
5. Andersen LL, Clausen T, Mortensen OS, Burr H, Holtermann A. A prospective cohort study on musculoskeletal risk factors for long-term sickness absence among healthcare workers in eldercare. Int Arch Occup Environ Health. 2012;85(6):615–622. doi:10.1007/s00420-011-0709-5
6.
7. Faber A, Giver H, Stroyer J, Hannerz H. Are low back pain and low physical capacity risk indicators for dropout among recently qualified eldercare workers? A follow-up study. Scand J Public Health. 2010;38(8):810–816. doi:10.1177/1403494810379891
8. Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine (Phila Pa 1976). 2002;27(5):E109–E120.
9. Burton AK, Balagué F, Cardon G, et al. How to prevent low back pain. Best Pract Res Clin Rheumatol. 2005;19(4):541–555. doi:10.1016/j.berh.2005.03.001
10. Driessen MT, Proper KI, van Tulder MW, Anema JR, Bongers PM, van der Beek AJ. The effectiveness of physical and organisational ergonomic interventions on low back pain and neck pain: a systematic review. Occup Environ Med. 2010;67(4):277–285. doi:10.1136/oem.2009.047548
11. Waddell G, Burton AK. Occupational health guidelines for the management of low back pain at work: evidence review. Occup Med (Lond). 2001;51(2):124–135.
12. Matsudaira K, Kawaguchi M, Isomura T, et al. Assessment of psychosocial risk factors for the development of non-specific chronic disabling low back pain in Japanese workers-findings from the Japan Epidemiological Research of occupation-related back pain (JOB) study. Ind Health. 2015;53(4):368–377. doi:10.2486/indhealth.2014-0260
13. Matsudaira K, Konishi H, Miyoshi K, Isomura T, Inuzuka K. Potential risk factors of persistent low back pain developing from mild low back pain in urban Japanese workers. PLoS One. 2014;9(4):e93924. doi:10.1371/journal.pone.0093924
14. Takahashi M, Matsudaira K, Shimazu A. Disabling low back pain associated with night shift duration: sleep problems as a potentiator. Am J Ind Med. 2015;58(12):1300–1310. doi:10.1002/ajim.22493
15. Hill JC, Dunn KM, Lewis M, et al. A primary care back pain screening tool: identifying patient subgroups for initial treatment. Arthritis Rheum. 2008;59(5):632–641. doi:10.1002/art.23563
16. Matsudaira K, Oka H, Kikuchi N, Haga Y, Sawada T, Tanaka S. The Japanese version of the STarT back tool predicts 6-month clinical outcomes of low back pain. J Orthop Sci. 2017;22:224–229. doi:10.1016/j.jos.2016.11.023
17. Von Korff M, Ormel J, Keefe FJ, Dworkin SF. Grading the severity of chronic pain. Pain. 1992;50(2):133–149.
18. Dionne CE, Dunn KM, Croft PR, et al. A consensus approach toward the standardization of back pain definitions for use in prevalence studies. Spine (Phila Pa 1976). 2008;33(1):95–103. doi:10.1097/BRS.0b013e31815e7f94
19. Krismer M, van Tulder M. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007;21(1):77–91. doi:10.1016/j.berh.2006.08.004
20. Nakata A, Ikeda T, Takahashi M, et al. Sleep-related risk of occupational injuries in Japanese small and medium-scale enterprises. Ind Health. 2005;43(1):89–97.
21. Bliwise DL, King AC, Harris RB, Haskell WL. Prevalence of self-reported poor sleep in a healthy population aged 50-65. Soc Sci Med. 1992;34(1):49–55.
22. Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6(2):97–111.
23. Oka H, Matsudaira K, Fujii T, et al. Estimated risk for chronic pain determined using the generic STarT back 5-item screening tool. J Pain Res. 2017;10:461–467. doi:10.2147/JPR.S129585
24. Matsudaira K, Kikuchi N, Kawaguchi M, et al. Development of a Japanese version of the STarT (Subgrouping for Targeted Treatment) back screening tool: translation and linguistic validation. J Musculoskelet Pain Res. 2013;5(1):11–19. Japanese.
25. Matsudaira K, Oka H, Kikuchi N, Haga Y, Sawada T, Tanaka S. Psychometric properties of the Japanese version of the STarT back tool in patients with low back pain. PLoS One. 2016;11(3):e0152019. doi:10.1371/journal.pone.0152019
26. Woby SR, Roach NK, Urmston M, Watson PJ. Psychometric properties of the TSK-11: a shortened version of the Tampa scale for kinesiophobia. Pain. 2005;117(1–2):137–144. doi:10.1016/j.pain.2005.05.029
27. Kikuchi N, Matsudaira K, Sawada T, Oka H. Psychometric properties of the Japanese version of the Tampa Scale for Kinesiophobia (TSK-J) in patients with whiplash neck injury pain and/or low back pain. J Orthop Sci. 2015;20(6):985–992. doi:10.1007/s00776-015-0751-3
28. Matsudaira K, Inuzuka K, Kikuchi N, et al. Development of a Japanese version of the Tampa Scale for Kinesiophobia (TSK-J): translation and linguistic validation. Rinsho Seikei Geka (Clin Orthop Surg). 2013;48(1):13–19. Japanese.
29. Muto S, Muto T, Seo A, Yoshida T, Taoda K, Watanabe M. Prevalence of and risk factors for low back pain among staffs in schools for physically and mentally handicapped children. Ind Health. 2006;44(1):123–127.
30. Kawakami N, Kobayashi F, Araki S, Haratani T, Furui H. Assessment of job stress dimensions based on the job demands- control model of employees of telecommunication and electric power companies in Japan: reliability and validity of the Japanese version of the job content questionnaire. Int J Behav Med. 1995;2(4):358–375. doi:10.1207/s15327558ijbm0204_5
31. Haratani T, Kawakami N, Araki S. Reliability and validity of the Japanese version of NIOSH generic job questionnaire. Sangyo Igaku (Jpn J Ind Health). 1993;35(suppl):S214. Japanese. doi:10.1539/joh1959.35.214
32. Isaac M, Tacchini G, Janca A. Screener for Somatoform Disorders (SSD). Geneva: World Health Organization; 1994.
33. Ono Y, Yoshimura K, Yamauchi K, Momose T, Mizushima H, Asai M. Psychological well-being and ill-being: WHO Subjective Well-being Inventory (SUBI). Jpn J Stress Sci. 1996;10:273–278.
34. Shimomitsu T, Odagiri Y. The brief job stress questionnaire. Occup Mental Health. 2004;12(1):25–36.
35. Shimomitsu T Manual for the evaluation of stress using Brief Job Stress Questionnaire. 2005; Available from:
36. Hair JF, Anderson RE, Tatham RL, Black WC. Multivariate Data Analysis.
37. Wada K, Arakida M, Watanabe R, Negishi M, Sato J, Tsutsumi A. The economic impact of loss of performance due to absenteeism and presenteeism caused by depressive symptoms and comorbid health conditions among Japanese workers. Ind Health. 2013;51(5):482–489.
38. Foster NE, Mullis R, Hill JC, et al. Effect of stratified care for low back pain in family practice (IMPaCT Back): a prospective population-based sequential comparison. Ann Fam Med. 2014;12(2):102–111. doi:10.1370/afm.1625
39. Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378(9802):1560–1571. doi:10.1016/S0140-6736(11)60937-9
40. Leeuw M, Goossens ME, Linton SJ, Crombez G, Boersma K, Vlaeyen JW. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94. doi:10.1007/s10865-006-9085-0
41. Wertli MM, Rasmussen-Barr E, Weiser S, Bachmann LM, Brunner F. The role of fear avoidance beliefs as a prognostic factor for outcome in patients with nonspecific low back pain: a systematic review. Spine J. 2014;14(5):816–836. doi:10.1016/j.spinee.2013.09.036
42. Chou R, Shekelle P. Will this patient develop persistent disabling low back pain? JAMA. 2010;303(13):1295–1302. doi:10.1001/jama.2010.344
43. Wakaizumi K, Yamada K, Oka H, et al. Fear-avoidance beliefs are independently associated with the prevalence of chronic pain in Japanese workers. J Anesth. 2017;31(2):255–262. doi:10.1007/s00540-016-2303-1
44. Andrews NE, Strong J, Meredith PJ. Activity pacing, avoidance, endurance, and associations with patient functioning in chronic pain: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2012;93(11):2109–2121. doi:10.1016/j.apmr.2012.05.029
45. Hasenbring MI, Verbunt JA. Fear-avoidance and endurance-related responses to pain: new models of behavior and their consequences for clinical practice. Clin J Pain. 2010;26(9):747–753. doi:10.1097/AJP.0b013e3181e104f2
46. Hasenbring MI, Hallner D, Klasen B, Streitlein-Bohme I, Willburger R, Rusche H. Pain-related avoidance versus endurance in primary care patients with subacute back pain: psychological characteristics and outcome at a 6-month follow-up. Pain. 2012;153(1):211–217. doi:10.1016/j.pain.2011.10.019
47. Cane D, Nielson WR, Mazmanian D. Patterns of pain-related activity: replicability, treatment-related changes, and relationship to functioning. Pain. 2018;159(12):2522–2529. doi:10.1097/j.pain.0000000000001357
48. Vargas-Prada S, Coggon D. Psychological and psychosocial determinants of musculoskeletal pain and associated disability. Best Pract Res Clin Rheumatol. 2015;29(3):374–390. doi:10.1016/j.berh.2015.03.003
49. Coggon D, Ntani G, Palmer KT, et al. Patterns of multisite pain and associations with risk factors. Pain. 2013;154(9):1769–1777. doi:10.1016/j.pain.2013.05.039
50. Coggon D, Ntani G, Vargas-Prada S, et al. International variation in absence from work attributed to musculoskeletal illness: findings from the CUPID study. Occup Environ Med. 2013;70(8):575–584. doi:10.1136/oemed-2012-101316
51. Nickel R, Egle UT, Rompe J, Eysel P, Hoffmann SO. Somatisation predicts the outcome of treatment in patients with low back pain. J Bone Joint Surg Br. 2002;84(2):189–195.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.