Back to Journals » Clinical Ophthalmology » Volume 19
Surgical Techniques and Indications for Intraocular Lens Explantation: A Narrative Review
Authors Alkhatib MH, Olson JH, Montezuma SR, Hou JH, Chanbour W ![]()
Received 25 July 2025
Accepted for publication 18 October 2025
Published 4 November 2025 Volume 2025:19 Pages 4053—4065
DOI https://doi.org/10.2147/OPTH.S556153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Comprehensive Guide to Intraocular Lens Explantation – Video S5 [556153]
Views: 129
Mohannad H Alkhatib,1 Joshua H Olson,2 Sandra R Montezuma,2 Joshua H Hou,2 Wassef Chanbour2
1Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 2Department of Ophthalmology and Visual Neurosciences, University of Minnesota, Minneapolis, MN, USA
Correspondence: Wassef Chanbour, Department of Ophthalmology and Visual Neurosciences, University of Minnesota, Minneapolis, MN, USA, Tel +1612-625-4400, Email [email protected]
Abstract: While the outcomes of cataract surgery are remarkably positive, complications do still occur, some of which require intraocular lens (IOL) explantation. These complications often include corneal endothelial loss for anterior chamber IOLs, whereas posterior chamber IOLs are usually explanted because of dislocation, opacification, or patient dissatisfaction with visual quality. Surgical management is challenging, with numerous IOL types/methods of implantation requiring different techniques for explantation. En bloc removal is the simplest of techniques, requiring large incisions with large rates of astigmatism. While folding and cutting methods allow for smaller incisions, the extensive manipulation these techniques require do lead to the potential for endothelial trauma. More novel methods such as cartridge-assisted extraction or IOL scaffolding theoretically minimize anterior chamber manipulation and risk of IOL prolapse into the vitreous but are less widely reviewed with few ophthalmologists having experience with the techniques. If the lens has become displaced into the vitreous, one can also cleave the lens prior to moving it the anterior chamber of the eye, thus even more greatly minimizing corneal endothelial damage. Ultimately, the variety of techniques paired with the rarity of explantation make it difficult to develop expertise in each of these many surgical methodologies. Therefore, it is important to review the indications, complications, general principles, and specific steps for each of the approaches to IOL explantation.
Keywords: intraocular lens, cataract, pseudophakia, intraocular lens dislocation, explantation
Introduction
Cataract surgery is one of the most commonly performed surgeries today, with upwards of 3.7 million in the United States annually.1 Additionally, refractive lensectomy is gaining popularity and contributing to an expanded pseudophakic population.2 While outcomes of cataract surgery are among the best of any surgical procedure, intraocular lens (IOL) explantation remains a serious, albeit rare, necessity. The factors that lead to lens explantation are diverse with some occurring during initial cataract surgery, within the global perioperative period, or even decades later.3 There have been major developments in surgical techniques over the last 20 years. Though there are case reports and literature on many of the methods of explantation in isolation, there is a deft of publications that offer a comparative discussion of multiple techniques of IOL removal. Thus, this review aims to summarize the indications and techniques for IOL explantation, focusing on practical principles for surgeons.
Method of Literature Search
The review was written based on a comprehensive query of English articles published after 1980. The following terms were used to identify relevant literature: “IOL explantation”, “Intraocular lens explantation”, “IOL exchange”, “Intraocular lens exchange”, “IOL explantation techniques”, “Intraocular lens explantation techniques”, “IOL exchange techniques”, “Intraocular lens exchange techniques”, “IOL explantation indications”, “Intraocular lens explantation indications”, “IOL exchange indications”, and “Intraocular lens exchange indications”. Additionally, the references of the articles that showed up in our literature search were also analyzed for inclusion in the review. The literature search was performed exclusively on PubMed Central, and two main types of articles were included in the review. The first were articles that provided general insight into the indications and background for intraocular lens explantation. The other category of included articles were those that described specific techniques for explantation. Preference was given to articles providing robust descriptions and videos of the techniques; however, articles with a limited description of the surgical techniques were included if the published technique was not found elsewhere in the literature.
Indications for Intraocular Lens Explantation
Many complications of cataract surgery may necessitate IOL explantation. The prevalence of these complications and rate of IOL explantation depends on the type of lens and position of initial implantation. The 1990s led to a drastic change in the indications for explantation through the standardization of phacoemulsification and use of foldable posterior chamber IOLs (PCIOLs) over polymethylmethacrylate (PMMA) lenses.4,5 The main reason for explantation in anterior chamber intraocular lenses (ACIOLs) tends to be the result of corneal endothelial cell loss leading to pseudophakic bullous keratopathy (PBK). Specifically, Mamalis et al reported that 39.7% of ACIOL explantations were due to PBK and 19.1% were due to uveitis-glaucoma-hyphema (UGH) while IOL instability caused only 10.3%.6 Despite advancements in IOL design and surgical technique, the complication profile of ACIOL has remained largely unchanged with more recent studies reporting 38.6–63.6% of ACIOL explantations due to PBK and 27.8% due to iritis.7,8
Though indications for IOL explantation are wide, this remains an uncommon complication of cataract surgery. For example, reports from the Moran Eye Center show decreasing rates of IOL explantation: 1.75% (1986–1990), 0.77% (1998–2004), and 0.53% (2007–2011).9–11 This is likely the result of the adoption of PCIOLs, improved surgical training/technique, and enhanced lens designs. More recent data from a Saudi Arabia population reported the average annual incidence of IOL removal/exchange as 2.5 per 10,000.12 However, the follow-up time after cataract surgery was only 8 years in this study, leading to a potential underestimation of the incidence. This conclusion is supported by another study out of Minnesota by Bothun and colleagues that tracked exchange/explantation from 1986 to 2016 and reported a 1.5% 30-year cumulative probability of exchange/explantation.13
Posterior chamber IOLs became the predominant lens in the 1990s, changing the indications for explantation drastically. Studies report 40–80% of PCIOL explantations result from dislocation/decentration, an especially common complication in eyes that have had prior vitrectomy.7,8,11–16 A Hungarian study reported 95.7% of their PCIOL explantations were due to dislocation.8 Incorrect lens power, IOL opacification, and neuroadaptation failure make up the remaining causes of explantation. Improved lens technology has led to a decrease in IOL opacification risk in recent years, but it was particularly common in early hydrophilic acrylic IOLs.17,18 In contrast, there has been a rise in explantation due to patient dissatisfaction caused by visual aberrations and undesired visual acuity, likely owing to the rise in multifocal and extended depth of field (EDOF) IOLs.19,20 These lenses are associated with decreased contrast sensitivity and higher rates of positive and negative dysphotopsia compared to monofocal IOLs; these patients often also have higher expectations at baseline.19,20 Ultimately, the changing complication profile of cataract surgery has led to a shorter duration between IOL implantation and explantation (6–10 years for ACIOLs versus 3–5 years for PCIOLs).3,8 It should be noted that IOLs can also become damaged during the initial implantation procedure (broken haptic, material defect, impaired unfolding, etc).21
As discussed above, most cases of IOL explantation typically occur years after implantation rather than due to acute emergencies. With this in mind, clinicians often need to decide when watchful waiting is appropriate versus surgical intervention. When the reason for explantation is due to corneal endothelial cell loss, which is often the case with ACIOLs, guidelines recommend moving forward with explantation when the endothelial cell density approaches ~1,500 cells/mm² or a total ECD loss ≥25% after 3 years.22,23 This is a reasonable time to proceed with explantation as true decompensation often occurs when the cell density falls to 500 cells/mm²; thus, the cutoff of ~1,500 cells/mm² allows for a permissive buffer of the losses that occur due to surgical trauma.24,25 When explantation is performed due to functionally impaired vision quality/patient dissatisfaction (dysphotopsia, opacification, decentration, or wrong power), it is recommended to first trial nonsurgical methods such as spectacles, YAG capsulotomy, etc. However, one review from Grzybowski et al and one from Patel et al indicate that functionally impairing symptoms/visual acuity, not a specific cutoff, are an indication for explantation as most patients undergoing exchange achieve excellent outcomes with visual acuity usually >20/40.26,27
Explantation rates remain low, with reports of 0.2%–0.3% in 5 and 8 year studies.12,13 However, it is a remarkably important skill for an ophthalmologist to maintain as the pseudophakic population only continues to grow.
Techniques for IOL Explantation
Explantation technique is complex and dependent on a variety of factors. Specifically, the approach is based on the type of lens being explanted, the chamber it is being explanted from, lens adhesions/attachment site, and concurrent anatomical variants/comorbidities. Broadly, the first step of explantation involves freeing the lens from its site of implantation and moving it into the anterior chamber of the eye. Once the lens has been freed to the anterior chamber, it must next be removed from the eye while minimizing the size of the incision used to extract the lens. The main techniques by which the lens can be explanted after being freed to the anterior chamber are by folding, cutting, or en bloc. We will review each of these techniques, indications, complications, and steps in greater detail.
It should be noted that throughout this review, we will name specific tools used by the referenced publications. The specific tools are listed as recommendations, and unless specified, similar tools are reasonable to consider.
Freeing the Lens to the Anterior Chamber
Capsular Bag
The most common type of lens explanted today is a foldable, acrylic lens that is implanted in the capsular bag.11 After making the necessary incisions for access and filling the anterior chamber with viscoelastic, the anterior and posterior leaflets of the capsular bag must be separated using a combination of mechanical and viscoelastic-assisted dissection. If necessary, sharp dissection with a pair of micro scissors can be used to open the capsular bag, but care must be taken here to avoid damaging the bag or causing zonular dehiscence.21 Following this, the haptics should be grasped, freed from the capsular bag, and the lens moved into the anterior chamber.
It should be noted that in cases where extensive fibrosis of the capsular bag precludes the mobilization of the haptics, cuts can be made at the optic-haptic junction.28 Cutting the optic-haptic junction may allow for easier removal of the haptic, however occasionally a haptic may require abandonment within the capsular bag. While lost/broken haptics and lens fragments during IOL implantation have been associated with corneal decompensation, there is not a reported risk associated with leaving haptics in the capsular bag following explantation.29,30 Ultimately, avoiding damage to the capsular bag and zonular support takes priority over explanting a haptic. As an alternative to cutting the optic-haptic junction when the capsule is particularly phimotic/contracted, relaxing incisions in the anterior capsule may need to be made with microscissors, Nd:YAG, or femtolaser to allow mobilization of the optic.31,32
Sulcus
The principles of removing an IOL from the ciliary sulcus are not much different than removing a lens from the capsular bag. Briefly, blunt dissection and viscoelastic material are used to separate the lens from the anterior capsule and posterior iris. The lens can then be migrated into the anterior chamber.
Iris-Fixated
Occasionally sulcus IOLs may need to be fixated to either the iris or sclera due to insufficient capsular support.33 Iris-claw and iris-sutured IOLs create unique challenges. Removal may cause iris trauma, and there is potential for the IOL to become displaced into the vitreous. One technique published avoids cutting sutures by rotating the haptics out of intact sutures.34 Using microforceps, the IOL optic is shifted until the proximal portion of the opposite haptic is visible. The haptic is then grabbed and a second pair of microforceps is used to brace the iris, while the haptic is rotated back until the haptic disengages from the iris suture.34 This step can then be repeated on the opposite haptic, and the IOL can be moved to the anterior chamber and removed. Occasionally, iris-sutured IOLs may be so overly fibrosed that cutting the sutures and haptics are necessary.
Scleral-Fixated
To remove scleral sutured IOL, the scleral flaps from the original scleral fixation operation should be identified. Subsequently, a conjunctival peritomy should be performed to expose the scleral fixation sutures or flanges. To minimize risk of dropping the IOL into the vitreous, miotics may be used to constrict the pupil, allowing for iris capture of the lens optic prior to disinserting the scleral fixation.35 While the method described above should be adequate in most cases, additional steps can be taken when the iris is fragile or insufficient pupil constriction is achieved. For example, sutures can be threaded across the pars plana behind the IOL. This provides posterior support to the IOL when the scleral sutures are cut.36 These techniques have not been published in the context of scleral fixated IOL explantation, and they may require a greater comfort with vitreoretinal surgery than some anterior segment surgeons possess.
Anterior Chamber
While anterior chamber IOLs are less frequently seen today than in the past, an ophthalmologist must still have confidence in explanting them.4,5 Compared to IOLs in the posterior chamber, these lenses are easier to free from their site of implantation. However, as anterior chamber IOLs tend to be rigid, their removal often necessitates a larger incision.37 While clear corneal incisions heal more rapidly, are self-sealing, and have a decreased risk of bleeding compared to scleral shelved incisions, they are known to induce surgically induced astigmatism (SIA), especially with larger incisions.38–40 Scleral incisions have been reported to result in nearly 50% less SIA when compared to clear corneal incisions.39
Occasionally, peripheral anterior synechiae can envelope the haptics of ACIOLs. In these cases, intraocular scissors or YAG laser may be used for synechialysis.41–43The optic can then be removed from the anterior chamber as discussed later in this review. Once the optic is removed, the haptics should be able to be freed from the iris by rotating them out of the adhesions with microforceps.42 However, it should be noted that removing the haptics and optic of ACIOLs separately is quite rare as most are made of PMMA which preclude cutting.
Explanting the Lens from the Anterior Chamber
En Bloc Removal – Whole Lens Removal
Whole lens removal represents the oldest method of IOL explantation (Video S1).44 This method of lens removal naturally requires the largest incision (typically 6.50 mm), which is not ideal due to the increased intraoperative risk of anterior chamber instability, which could lead to iris prolapse, vitreous loss, and corneal damage.39,40 Moreover, post-operative SIA and increased intraocular pressure have also been correlated with these larger incisions.39,40 However, it is often the only method of removal in the case of non-foldable and rigid IOLs, such as those made of polymethylmethacrylate (PMMA).45 These older IOLs have been largely phased out as they require a large 5.50 mm to 6.00 mm incision for implantation, but they are still used in anterior chamber implantation and are also the primary PCIOLs in resource limited settings, owing to their low production cost.46 Ultimately, thick three-piece acrylic IOLs or PMMA IOLs may require up to a 6.50 mm incision for explantation. In the case of thinner lenses, one technique for explantation involves using a toothed forceps inserted through the main incision to grasp the center of the optic while a lens manipulator is inserted via a side port incision 180° away. A combined force of pulling on the IOL via the main incision while also pushing on the optic through the side port incision should be applied to the lens. The pushing and pulling forces will naturally cause the IOL to fold inside the incision as it exits, thus avoiding the risks that come with cutting or folding the lens in the anterior chamber.47
En Bloc Removal – Refolding
While explantation traditionally relied upon an enlarged main incision to remove the lens whole, the ubiquitous adoption of foldable IOLs and microincision cataract surgery led to new explantation techniques. Specifically, techniques of explanting IOLs via small incisions (down to 2.20 mm) have been developed using refolding methods in the anterior chamber.48–52 It should be noted that this method of explantation is well suited for soft foldable lens such as those made of acrylic, collamer, and silicone; however, this method is incompatible with polymethylmethacrylate (PMMA) lenses or lenses that are too thick to be safely folded (Table 1).
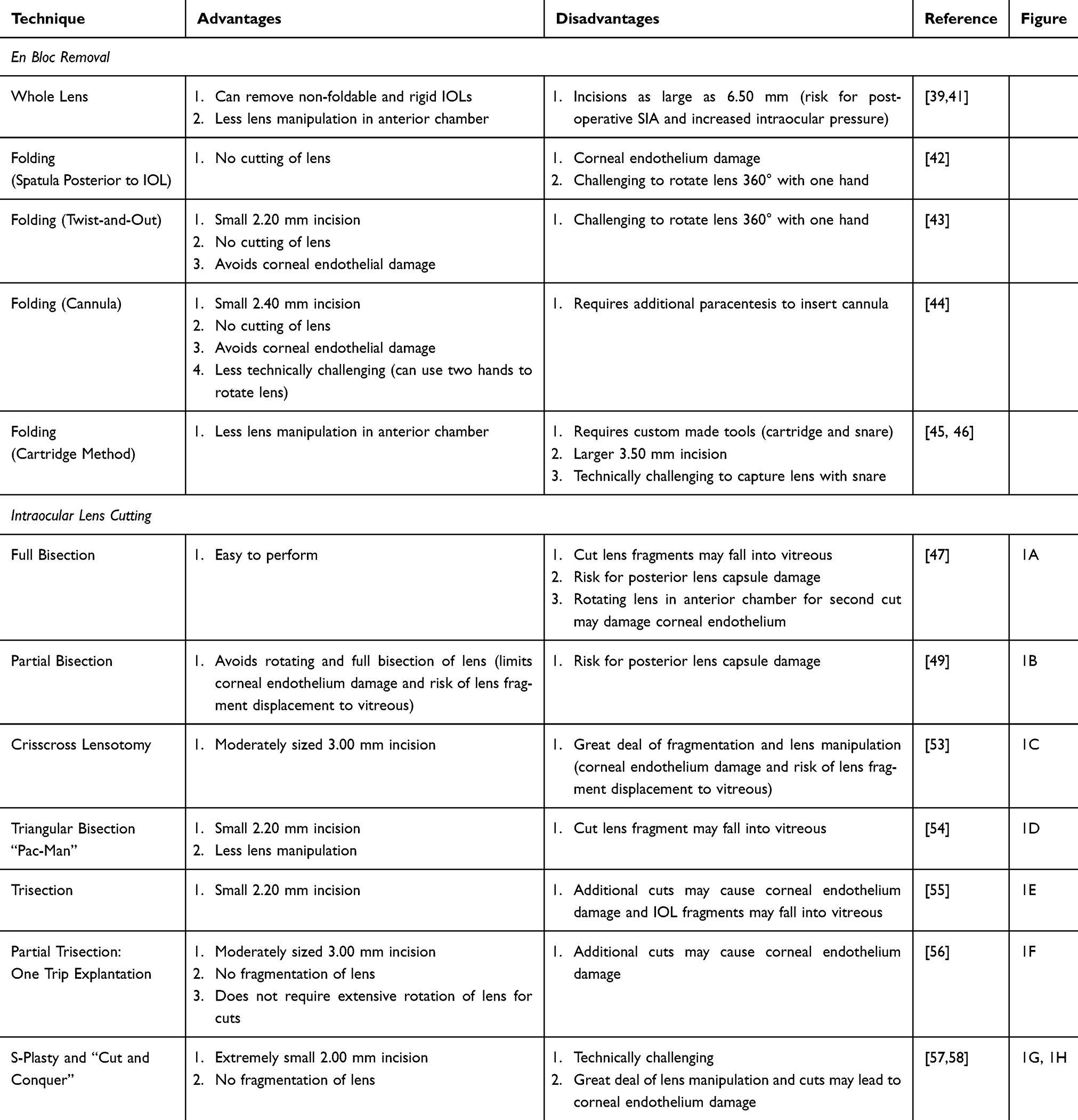 |
Table 1 Concise Summary of the Advantages and Disadvantages of the Various Methods of IOL Explantation |
Folding (Spatula Posterior to IOL)
This method involves folding the lens around a spatula.48 A 3.50 mm limbal tunnel incision and a side port incision 180° away are used for this technique. One of the haptics can be pulled through the limbal incision. Subsequently, a blunt spatula is inserted into the side port incision and positioned under the IOL. Folding forceps can then be inserted into limbal tunnel incision and used to pinch the lens around the spatula. The spatula should be carefully removed from under the lens, and the forceps along with the lens withdrawn. While this technique avoids needing to cut the IOL, it has been shown to lead to a reduction in corneal endothelial cell counts.48 This is likely the result of the posterior positioning of the spatula, which provides zero protection to the corneal endothelium.
Folding (Twist-and-Out)
As a means of avoiding the corneal endothelial damage associated with the previous method, one can use a method termed “twist-and-out”. One haptic is explanted via a clear corneal incision (2.20 mm in the referenced publication) and a straight spatula or cannula is also inserted into a paracentesis 90° from the main incision. With the surgeon’s hand maximally supinated, a straight forceps is introduced through the main incision. It is key to position the forceps across the lens and grasp the optic near the haptic on the side of the paracentesis. Then, the surgeon should attempt to protonate their hand to rotate the lens approximately 360° against the cannula, this way protecting the cornea and essentially rolling the lens. The lens can then be removed via the main incision (Video S2).49 While this method protects the cornea, achieving 360° of rotation with one hand while operating in the anterior chamber is challenging for many surgeons.
Folding (Cannula)
If the previous method is not feasible for a surgeon, there is an alternative method of folding the lens that does not require 360° of one-handed rotation. The initial steps of this method follow the twist-and-out technique, except two side port paracenteses are made 180° from each other and 90° away from the main incision. Instead of using a spatula, a 25-gauge cannula is threaded across the anterior chamber through the two paracenteses. The 25-gauge needle should be adequately secure without being held. This permits two hands to be used to insert serrated forceps into the main clear corneal incision, grasp the lens, rotate it 360° against the cannula, and withdraw it through the main incision. While this method requires an additional paracentesis, it is a more user-friendly technique of intraocular lens refolding, and cases of explantation through 2.40 mm incisions have been published using it.50
Folding (Cartridge Method)
Other groups have turned to explanting IOLs via cartridges. This limits the amount of anterior chamber lens manipulation/folding, thus lowering the potential for complications.
Specifically, one method involves using a snare-like device threaded through an Alcon A cartridge to remove IOLs.51 The snare is made by blunting the tip of a 20-gauge needle with a pumice stone and creating two side holes in the tip of the cannula. Subsequently, the two ends of either a 3–0 prolene suture or guitar string should be threaded through the two holes in the 20-gauge needle, creating a loop that is approximately 3/4th the length of the Alcon A cartridge. The loop can then be secured by clamping the cannula with pliers at various points. Next, the Alcon A cartridge is modified by making two 2.50 mm incisions in the nozzle tip along the horizontal axis, 180° apart. Now, the created snare can be threaded through the modified cartridge and used to explant the IOL. It should be noted that it is critical to warm the modified cartridge immediately prior to the procedure as a means of increasing its flexibility/ease of taking up the IOL.51
Interestingly, the publication demonstrating this technique also made use of an intraocular lens scaffold prior to inserting the cartridge-snare device (discussed later in the review). Once the new IOL is placed (if lens exchange is indicated), the cartridge-snare must be filled with warmed viscoelastic for lubrication and to prevent iris incarceration. It can then be inserted into the anterior chamber bevel down through a (3.50 mm corneal or limbal incisions in referenced publication). Here, a secondary instrument, such as forceps or a spatula, should be inserted via a side port incision and used to hook the haptic onto the snare. Finally, the combined forces of pushing the cartridge while pulling on the snare will pull/fold the lens fully into the device. The device can then be removed from the eye. While unorthodox, this method is advantageous as the guitar string and 3–0 prolene suture are both less likely to damage the corneal endothelium or posterior capsule than rigid metal tools. Additionally, no folding or cutting needs to be performed in the anterior chamber; however, the use of custom devices, a large main incision, and only being able to explant one-piece IOLs has hampered widespread adoption of this technique.51
Fortunately, there is a method that can explant a wide variety of one- and three-piece soft IOLs using a similar system. This method uses a D1 cartridge and Fukuoka IOL extraction forceps instead of the custom snare.52 Specifically, the metal forceps are threaded through the D1 cartridge, and the cartridge-forceps system is inserted into the anterior chamber. Subsequently, the metal forceps can be minimally advanced through the cartridge, used to grasp the optic, and withdrawn back into the D1 cartridge.52 While this method still uses metal forceps to fold the lens, most manipulation occurs within the cartridge, protecting the anterior chamber. Moreover, ophthalmologists likely are more comfortable grasping the lens with forceps than with the snare employed by the previously discussed technique. Ultimately, a few cartridge-based systems for lens explantation have been reported in the literature in recent years but refolding and cutting (discussed later in the review) remain the dominant methods of lens removal used by ophthalmologists today.
Intraocular Lens Cutting
Explantation via certain refolding techniques is widely adopted and provides a nice balance between minimizing incision size and extensive anterior chamber IOL manipulation. However, it is also standard practice to cut the lens in the anterior chamber to facilitate its removal through a potentially smaller incision53–55 (Table 1).
Full Bisection
The first method of intraocular lens cutting that was described in the literature is the full bisection method. An inferior main incision (3.50 mm scleral incision used in referenced publication) should be made. The lens should be positioned so the haptics are oriented temporally and nasally. The lens can then be cut along its radius with IOL cutters, partially bisecting it. The lens should then be rotated 180° with a Sinskey hook and cut again along its radius, fully bisecting the lens (Figure 1A). The surgeon can then remove the lens in two pieces by pulling on the optic with McPherson forceps.53 Ultimately, this method allows for a moderately sized incision, but rotating the lens is technically challenging and could lead to corneal endothelium and posterior lens capsule damage, despite appropriate viscoelastic usage.56,57 Moreover, by fully bisecting the lens, there is a risk for the resulting fragments to fall into the vitreous, especially in cases where the posterior capsule is compromised.58 A modified variant of this technique that bisects the lens in the context of an IOL scaffold (discussed later in the review) is included for reference (Video S3).
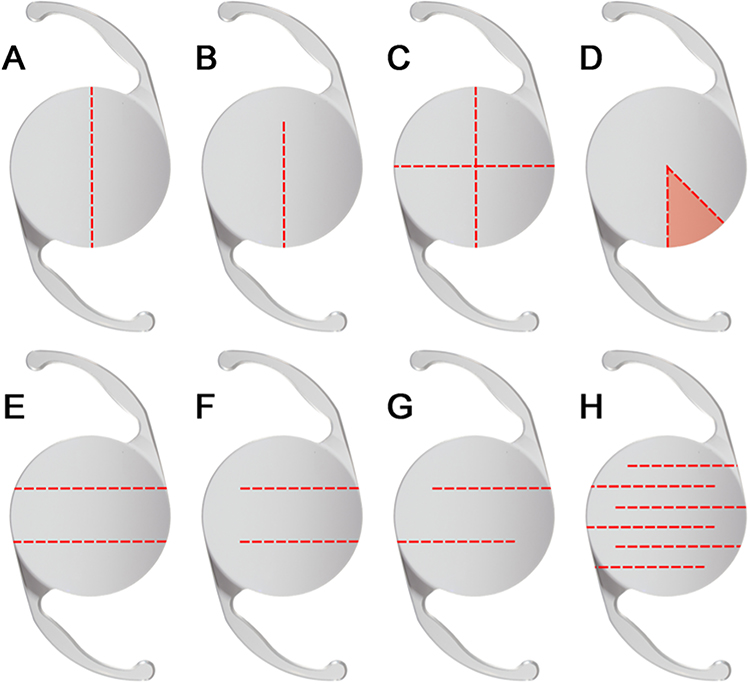 |
Figure 1 Schematic representation of IOL cuts for explantation via full bisection (A), partial bisection (B), crisscross lensotomy (C), triangular bisection “Pac-Man” (D), trisection (E), partial trisection (F), S-Plasty (G), and “Cut and Conquer” (H). |
Partial Bisection
Given the technical difficulty and risk of complications that can arise with rotating and fully bisecting the lens, there is a simpler method of explantation that involves partial bisection. A 3.20 mm incision was used by the authors. McPherson forceps should then be used to pull and anchor the haptic outside of the main corneal incision, and a radial cut is to be made halfway through the optic. The surgeon should then be able to embed half of the lens into the main incision along the radial optic cut. Finally, McPherson forceps can be used to rotate the remainder of the IOL out of the eye (Figure 1B).55 As demonstrated, this technique does not require complex manipulation or complete fragmentation of the IOL (Video S4). However, smaller main incisions can be used via alternative techniques that involve additional cuts in the lens.
Crisscross Lensotomy
If one would like to achieve an even smaller incision than possible via the partial bisection method, they can make use of a technique termed “crisscross lensotomy”, a technique first demonstrated with a silicone plate IOL. The group that published this method used a single, inferior 3.00 mm clear corneal incision to move the lens to the anterior chamber and then oriented it in long axis relative to the 3.00 mm incision. Here, the surgeon can then use Osher cutting scissors to make a longitudinal, long axis cut 1/3 the way across the IOL. The IOL must then be rotated 90° and an additional cut made, freeing a small rectangle segment. This segment is then removed from the eye using forceps. The above procedure should be repeated freeing an additional rectangle segment. The resulting crisscross-shaped lens can then be easily removed (Figure 1C).59 Ultimately, this method allows for a smaller incision than the partial bisection technique, but it requires a great deal of fragmentation and lens manipulation.
Triangular Bisection “Pac-Man”
While the crisscross lensotomy technique was a great technique at the time it was developed, a more recently developed triangular bisection method of IOL explantation is superior. This involves making two radial incisions to remove a triangle segment from the lens, permitting the lens to be explanted via clear corneal incisions as small as 2.20 mm. Once in the anterior chamber, IOL cutters are used to make two radial cuts approximately 40° degrees apart on the optic. This will free a small triangular fragment of the lens that is able to be removed with McPherson forceps. The remaining IOL segment can subsequently be pulled out of the small corneal incision with a circular motion (Video S5).60 Ultimately, this technique takes minimal IOL manipulation, and the removed triangular segment enables greater flexibility and a smaller incision than would be afforded by a single radial cut. The main downside of this technique is the risk of the triangle fragment falling into the vitreous (Figure 1D).58
Trisection
In cases where the surgeon is particularly interested in minimizing the incision size, the IOL can also be trisected. Specifically, through a 2.20 mm temporal incision and a superior paracentesis 90° away, the IOL should be moved to the anterior chamber and positioned so the haptics are oriented superiorly and inferiorly. With IOL cutters, two full length cuts must then be made on the same side of the optic at its superior-middle junction and middle-inferior junction. The three pieces of the lens are then subsequently withdrawn from the 2.20 mm temporal corneal incision with McPherson forceps. This technique is especially useful in the context of modern day microincision cataract surgery as it requires a very small cut and does not require difficult rotation of the optic.61 However, as with all techniques, more cuts and IOL fragments increase the risk of corneal damage, posterior capsular tears, and dropping fragments into the vitreous (Figure 1E).56–58
Partial Trisection: One Trip Explantation
If one wishes to avoid the risks that come with fragmentation and is comfortable with a slightly larger incision, they can use partial trisection to remove the lens. To begin the operation, a 3.00 mm scleral tunnel incision at 11 o’clock and a side paracentesis incision at 2 o’clock should be used to free the IOL to the anterior chamber. Once in the anterior chamber, a pair of vitreoretinal forceps should be inserted into the side paracentesis to stabilize the IOL with its haptics oriented temporally and nasally. Scissors should then be used to make two partial vertical cuts (leave 1.00 mm uncut) on the same side of the IOL. This will create a middle flap in the IOL, which can then be grasped and dragged out through the 3.00 mm scleral tunnel. In doing so, the two outer segments of the cut IOL will fold in and overlap each other as they pass through the incision (Figure 1F). A variety of IOLs including 1-piece acrylic hydrophilic, 3-piece hydrophobic, and 4-haptic hydrophilic acrylic lenses have all been explanted using this technique.62 In addition to being demonstrated with a variety of lenses, this method is ideal as it does not require extensive rotation or fragmentation of the lens.
S-Plasty and “Cut and Conquer”
While the triangular bisection and trisection techniques enable the surgeon to remove the lens via small 2.20 mm incisions, these techniques both require fragmentation of the IOL. There is a way to explant the IOL through small 2.20 mm and even 2.00 mm incisions as a single unit.
Using the methods described throughout this paper, the surgeon should create a 2.20 mm temporal clear corneal incision. Next scissors should be introduced into the main corneal incision and a Nagahara chopper should also be inserted into the side paracentesis for countertraction. Two 4.50 mm deep slits that are 2.00 mm apart must then be created on opposite sides of the optic, producing an S pattern. It is key that the incisions are made near each optic-haptic junction to allow for optimal uncurling of the lens during removal; these two slits will effectively segment the IOL into three 2.00 mm wide pieces that are connected by uncut “hinges” (Figure 1G). This will permit the resulting lens to be pulled out haptic first while remaining in one piece.63 Fechin has further developed this method through a technique termed “cut and conquer”, where up to 8 oppositely oriented partial cuts are made, enabling the resulting zig-zag/snake shaped lens to be pulled out of a 2.00 mm incision (Figure 1H).64 While the resultant IOLs in these two techniques are remarkably small and can be removed from tiny tunnels without stressing the incision, creating the “S-shape” or “snake” is challenging and requires a great deal of IOL manipulation in the anterior chamber. If the surgeon is not proficient in their technique, it opens up a great deal of risk for complications. Nonetheless, when performed well, the small incision size minimizes SIA.39,40
Bimanual Cleavage in the Vitreous Chamber
The previous techniques enable the removal of lens fragments from profoundly small incisions. However, most of these techniques rely on cutting and manipulation of the IOL after it has been moved to the anterior chamber which has the potential to cause endothelial corneal damage.56,57 To address this concern, a recent technique effective in ten patients with IOL subluxation/dislocation utilized the vitreous cavity as the surgical workspace.65 The technique began by performing a standard pars plana vitrectomy to clear vitreous and create adequate working space. The authors then used a 23-G serrated forceps and a vitrectomy probe to separate and remove the capsular bag from the IOL. Following this and without moving the intact IOL into the anterior chamber, scissors are used to make a horizontal cut to the midpoint of the lens plate. Subsequently, two forceps are used to grasp the lens at both haptics, and the two forceps are pulled apart, exerting perpendicular force on the cut, cleaving the IOL. The IOL fragments can then be moved into the anterior chamber and extracted through a 2.2 mm corneal incision. While this technique requires the expertise of an ophthalmologist trained to operate in the vitreous, it allows one to handle lenses that have become displaced into the vitreous and minimizes endothelial corneal damage.
Intraocular Lens Scaffold
In cases with a damaged posterior capsule, vitreous prolapse can occur and IOL fragments can potentially be lost into the vitreous.56–58 Implanting the new IOL prior to removing the original IOL from the anterior chamber (Video S3) may lessen the chance of capsular damage and posterior lens dislocation.66–68
Discussion
IOL explantation is a necessary skill for every cataract surgeon, especially given the increasing use of multifocal and extended depth of field (EDOF) IOLs and rising expectations that patients have. Each IOL model and method of IOL implantation requires different explantation techniques. Reports of these techniques in the literature are scattered and may be difficult to thoroughly review as a result. This review encompasses both common and uncommon techniques in depth.
Corneal incisions are more commonly used today due to better healing and less bleeding, but they can cause SIA.38–40Although the risk of SIA is minimized by the smaller incisions used in modern-day cataract surgery, scleral tunnel incisions are still best when SIA is a major concern.40 With that said, reopening the main incision from the primary operation is usually the best choice, most commonly in the early post-operative period following cataract surgery. Once incisions are made, viscoelastic should be used to fill the anterior chamber. Cohesive viscoelastic is primarily used, but dispersive viscoelastic and a combined “sandwich” technique can also be employed based on the preferences of the surgeon.67
Once viscoelastic has been used to fill the anterior chamber, the lens must be freed to the anterior chamber. The specific methods of doing so depend on where the IOL is implanted. However, a combination of blunt dissection and viscoelastic are ultimately used to free the haptics and IOL.21 In patients with extensive fibrosis, scissors and YAG lasers can be used to make cuts at the optic-haptic junction to facilitate removal.41–43 The haptics can be left in the capsular bag if there is concern of damaging the capsular bag and zonules during removal.32,33 In cases of iris-sutured IOL explantation, iris trauma can be minimized by removing the IOL without cutting the sutures.34 However, removing scleral-sutured IOLs may not require sutures to be cut.35
After the IOL is secure in the anterior chamber, the surgeon must decide between refolding it, cutting it, using a cartridge system, or removing the lens whole. In cases where lens exchange is indicated, IOL scaffolding may prevent posterior capsular damage or posterior dislocation of the IOL being explanted.66,67,69 Folding the lens against an anteriorly positioned spatula using the “twist-and-out” technique or with the assistance of a cannula allows one to remove the lens via a small incision while protecting the cornea.49,55 Alternatively, the “S-plasty” and “cut-and-conquer” techniques enable one to remove the lens from a remarkably small incision, although these methods do require extensive cutting and rotating of the lens.63,64 If this extensive manipulation is a concern for the surgeon, “trisection” or “partial bisection” of the IOL require less manipulation and cutting while still enabling removal through a small incision.55,61 In cases where the IOL has become dislocated into the vitreous, a pars plana vitrectomy can be performed. Following this, the lens can be cleaved within the vitreous cavity, with subsequent removal of the fragments through a small corneal incision, thereby minimizing endothelial corneal damage seen with cutting in the anterior chamber.
Ultimately, the choice of IOL explantation technique depends not only on lens type and the patient anatomy but also on the surgeon’s level of experience. As discussed throughout the review, ophthalmologists less experienced in IOL removal may be more comfortable with approaches such as partial bisection, trisection, or twist-and-out refolding. On the other hand, techniques such as S-plasty, cut-and-conquer, or IOL scaffolding are newer techniques that do demand greater dexterity, likely necessitating greater comfort/training in the anterior segment. Similarly, the bimanual cleavage in the vitreous chamber technique should only be attempted by a retina specialist who is comfortable operating in the vitreous chamber.
While we have curated a comprehensive review of all the techniques of surgical explantation present in the literature, only one study has directly compared the outcomes of different methods of explantation. In a retrospective comparative series of 175 eyes undergoing explantation or exchange of one-piece foldable acrylic IOLs between 2010 and 2022, surgically induced astigmatism was minimal in the refolding and bisection groups (≈0.08 ± 0.13 D and 0.09 ± 0.17 D, respectively) but substantially higher (~0.83 ± 0.29 D) in cases managed with en bloc removal via an enlarged incision. Visual acuity outcomes were otherwise equivalent across groups. Complication rates were low overall; however, bisection was associated with the highest rates of corneal edema (15.1%) and anterior chamber reaction (6.0%), both resolving with steroid treatment without consequence (70).
Other than the abovementioned study, most articles are case reports and case series that simply describe innovative techniques. This is a gap that future investigation could fill, but it will be challenging given the rarity of explantation. Even reports simply describing the techniques are rare, with only one or two case reports comprising the entire literature on many of the techniques. While it is difficult to assess outcomes of explantation, it might be beneficial to investigate which of the techniques are best performed/most efficient for ophthalmology residents to learn. This way, residents can be trained on the techniques most easily mastered in the few cases of explantation that they will encounter throughout their training.
While comparative data remain limited, it appears that visual acuity is largely equivalent across explantation techniques. With that said, en bloc removal without folding is associated with significantly higher rates of surgically induced astigmatism and should generally be avoided unless necessary (eg, rigid anterior chamber IOLs). Cutting the IOL with scissors in the anterior chamber does also appear to carry a higher risk of transient corneal edema and irritation than methods of refolding, particularly the twist-and-out method, but these complications tend to typically resolve without lasting consequence. Since cutting and refolding approaches appear comparable in outcomes, surgeon familiarity and comfort with a given technique should guide the choice of method. In cases of IOL posterior dislocation, cutting the IOL while it is still in the vitreous cavity prior to displacing it into the anterior chamber is recommended as a means to minimize unnecessary cornea endothelial damage. In summary, an abundance of techniques for IOL explantation have been described, allowing surgeons to select a few versatile techniques to master for different clinical scenarios (Table 1).
Consent Statement
Consent was obtained from all patients for the publication of clips from their surgeries in this review. All surgical videos are devoid of identifiable patient information and anonymized.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Minnesota Lions Vision Foundation (1701- 11820- 20090- UMF0011830).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Moshirfar M, Milner D, Patel BC. Cataract surgery. StatPearls. StatPearls Publishing; 2024. Available from: http://www.ncbi.nlm.nih.gov/books/NBK559253/.
2. Ong LF, Oh A, Yi JK, et al. Refractive lens exchange – who is getting it, what are they getting, how are they doing? Curr Opin Ophthalmol. 2023;34(4):280–289. doi:10.1097/ICU.0000000000000956
3. Marques FF, Marques DMV, Osher RH, Freitas LL. Longitudinal study of intraocular lens exchange. J Cataract Refract Surg. 2007;33(2):254–257. doi:10.1016/j.jcrs.2006.10.036
4. Leaming DV. Practice styles and preferences of ASCRS members--1998 survey. J Cataract Refract Surg. 1999;25(6):851–859.
5. Leaming DV. Practice styles and preferences of ASCRS members—1994 survey. J Cataract Refract Surg. 1995;21(4):378–385. doi:10.1016/S0886-3350(13)80524-X
6. Mamalis N, Crandall AS, Pulsipher MW, Follett S, Monson MC. Intraocular lens explantation and exchange: a review of lens styles, clinical indications, clinical results, and visual outcome. J Cataract Refract Surg. 1991;17(6):811–818. doi:10.1016/S0886-3350(13)80416-6
7. Oltulu R, İ E, Şatırtav G, Donbaloglu M, Kerimoğlu H, Özkağnici A. Intraocular lens explantation or exchange: indications, postoperative interventions, and outcomes. Arquivos Brasileiros de Oftalmologia. 2015;78(3). doi:10.5935/0004-2749.20150040
8. Magyar M, Szentmáry N, Ujváry L, et al. Indications and outcomes of intraocular lens explantation in a tertiary eyecare center in Hungary between 2006 and 2020. J Ophthalmol. 2024;2024:1–9. doi:10.1155/2024/6653621
9. Lyle WA, Jin JC. An analysis of intraocular lens exchange. Ophthalmic Surg. 1992;23(7):453–458.
10. Jin GJC, Crandall AS, Jones JJ. Changing indications for and improving outcomes of intraocular lens exchange. Am J Ophthalmol. 2005;140(4):688.e1–688.e9. doi:10.1016/j.ajo.2005.05.015
11. Jones JJ, Jones YJ, Jin GJC. Indications and outcomes of intraocular lens exchange during a recent 5-year period. Am J Ophthalmol. 2014;157(1):154–162.e1. doi:10.1016/j.ajo.2013.08.019
12. Abdalla Elsayed MEA, Ahmad K, Al-Abdullah AA, et al. Incidence of intraocular lens exchange after cataract surgery. Sci Rep. 2019;9(1):12877. doi:10.1038/s41598-019-49030-2
13. Bothun ED, Cavalcante LCB, Hodge DO, Patel SV. Population-based incidence of intraocular lens exchange in olmsted county, minnesota. Am J Ophthalmol. 2018;187:80–86. doi:10.1016/j.ajo.2017.12.016
14. Mamalis N, Brubaker J, Davis D, Espandar L, Werner L. Complications of foldable intraocular lenses requiring explantation or secondary intervention—2007 survey update. J Cataract Refract Surg. 2008;34(9):1584–1591. doi:10.1016/j.jcrs.2008.05.046
15. Alió F, Barraquer R, Cantó-Cerdán M, Alió JL. Causes of intraocular pseudophakic lens explantation in Spain. Euro J Ophthalmol. 2023;34(2):432–439. doi:10.1177/11206721231187921
16. Riedl JC, Rings S, Schuster AK, Vossmerbaeumer U. Intraocular lens dislocation: manifestation, ocular and systemic risk factors. Intl Ophthalmol. 2022;43(4):1317–1324. doi:10.1007/s10792-022-02529-6
17. Izak AM, Werner L, Pandey SK, Apple DJ. Calcification of modern foldable hydrogel intraocular lens designs. Eye. 2003;17(3):393–406. doi:10.1038/sj.eye.6700341
18. Werner L, Apple DJ, Kaskaloglu M, Pandey SK. Dense opacification of the optical component of a hydrophilic acrylic intraocular lens: a clinicopathological analysis of 9 explanted lenses. J Cataract Refract Surg. 2001;27(9):1485–1492. doi:10.1016/S0886-3350(01)00841-0
19. Woodward MA, Randleman BJ, Stulting DR. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. doi:10.1016/j.jcrs.2009.01.031
20. Hu J, Sella R, Afshari NA. Dysphotopsia. Curr Opin Ophthalmol. 2018;29(1):61–68. doi:10.1097/icu.0000000000000447
21. Morkos FF, Fawzy NF, El Bahrawy M, Elkitkat RS. Watany Research and Development Center, Watany eye hospital, Cairo 11799, Egypt, Morkos FF,Bahrawy ME, Watany Research and Development Center, Watany Eye Hospital, Cairo 11799, Egypt, Elkitkat RS, Watany Research and Development Center, Watany Eye Hospital, Cairo 11799, Egypt; Department of Ophthalmology, Faculty of Medicine, Ain Shams University, Cairo 11799, Egypt. Introduction of longstanding complicated sulcus intraocular lens into the intact capsular bag. Int J Ophthalmol. 2021;14(11):1779–1783. doi:10.18240/ijo.2021.11.19
22. Tang Y, Xu J, Chen J, Lu Y. Long-term destiny of corneal endothelial cells in anterior chamber intraocular lens-implanted eyes. J Ophthalmol. 2020;2020:5967509. doi:10.1155/2020/5967509
23. MacRae S, Holladay JT, Hilmantel G, et al. Special report: American Academy of Ophthalmology Task Force recommendations for specular microscopy for phakic intraocular lenses. Ophthalmology. 2017;124(1):141–142. doi:10.1016/j.ophtha.2016.09.034
24. Vaiciuliene R, Rylskyte N, Baguzyte G, Jasinskas V. Risk factors for fluctuations in corneal endothelial cell density. Exp Ther Med. 2022;23(2):129. doi:10.3892/etm.2021.11052
25. Yoon HY, Byun YS, Kim HS, Chung SH. Cornea endothelial cell loss before and after explantation of artisan and artiflex iris-fixated phakic intraocular lenses. Am J Ophthalmol. 2025;270:52–60. doi:10.1016/j.ajo.2024.10.010
26. Grzybowski A, Markeviciute A, Zemaitiene R. A narrative review of intraocular lens opacifications: update 2020. Ann. Transl Med. 2020;8(22):1547. doi:10.21037/atm-20-4207
27. Patel V, Pakravan P, Lai J, et al. Intraocular lens exchange: indications, comparative outcomes by technique, and complications. Clin Ophthalmol. 2023;17:941–951. doi:10.2147/OPTH.S399857
28. Geggel HS. Simplified technique for acrylic intraocular lens explantation. Ophthalmic Surg Lasers Imaging. 2000;31(6):506–507. doi:10.3928/1542-8877-20001101-15
29. Elyashiv S, Barequet I. A surprising cause for corneal edema after cataract surgery: a missed posterior chamber intraocular lens haptic remnant. Seminars Ophthalmol. 2015;30(5–6):450–453. doi:10.3109/08820538.2013.874477
30. Hoffman RS, Fine HI, Packer M. Retained IOL fragment and corneal decompensation after pseudophakic IOL exchange. J Cataract Refract Surg. 2004;30(6):1362–1365. doi:10.1016/j.jcrs.2003.08.015
31. Fram NR, Masket S, Alsetri H, Pham D. Femtosecond laser–assisted intraocular lens exchange. J Cataract Refract Surg. 2021;47(12):e84–e87. doi:10.1097/j.jcrs.0000000000000752
32. Chawla JS, Moin Shaikh M. Neodymium:YAG laser parabolic anterior capsulotomy in extreme capsule contraction syndrome. J Cataract Refract Surg. 1999;25(10):1415–1417. doi:10.1016/s0886-3350(99)00154-6
33. Mehta R, Aref A. Intraocular lens implantation in the ciliary sulcus: challenges and risks. Clin Ophthalmol. 2019;13:2317–2323. doi:10.2147/OPTH.S205148
34. Elhusseiny AM, Sanders RN, Sallam AB. Explantation of iris-sutured intraocular lens. Can J Ophthalmol. 2023;58(2):e73–e74. doi:10.1016/j.jcjo.2022.07.005
35. Mikhail M, Sallam A. Scleral suture-fixated intraocular lens explantation. Eye. 2014;28(6):767–768. doi:10.1038/eye.2014.65
36. Masket S, Fram NR. Safety-basket suture for management of malpositioned posterior chamber intraocular lens. J Cataract Refract Surg. 2013;39(11):1633–1635. doi:10.1016/j.jcrs.2013.08.038
37. Werner L. Intraocular lenses. Ophthalmology. 2021;128(11):e74–e93. doi:10.1016/j.ophtha.2020.06.055
38. Cooper BA, Holekamp NM, Bohigian G, Thompson PA. Case-control study of endophthalmitis after cataract surgery comparing scleral tunnel and clear corneal wounds. Am J Ophthalmol. 2003;136(2):300–305. doi:10.1016/S0002-9394(03)00202-2
39. Olsen T, Dam-Johansen M, Bek T, Jø H. Corneal versus scleral tunnel incision in cataract surgery: a randomized study. J Cataract Refract Surg. 1997;23(3):337–341. doi:10.1016/S0886-3350(97)80176-9
40. Febbraro JL, Wang L, Borasio E, et al. Astigmatic equivalence of 2.2-mm and 1.8-mm superior clear corneal cataract incision. Graefes Arch Clin Exp Ophthalmol. 2015;253(2):261–265. doi:10.1007/s00417-014-2854-5
41. Johnson SH, Kratz RP, Olson PF. Clinical experience with the Nd:YAG laser. Ame Intra Ocular Implant Soc J. 1984;10(4):452–460. doi:10.1016/S0146-2776(84)80046-4
42. Marques FF, DMV M, Smith CM, Osher RH. Intraocular lens exchange assisted by preoperative neodymium:YAG laser haptic fracture. J Cataract Refract Surg. 2004;30(1):247–249. doi:10.1016/S0886-3350(03)00469-3
43. Gorn RA, Steinert RF. Neodymium:YAG laser cutting of intraocular lens haptics. Ame Intra Ocular Implant Soc J. 1985;11(6):568–571. doi:10.1016/S0146-2776(85)80134-8
44. Menapace R, Yalon M. Exchange of IOGEL hydrogel one-piece foldable intraocular lens for bag-fixated J-loop poly(methyl methacrylate) intraocular lens. J Cataract Refract Surg. 1993;19(3):425–430. doi:10.1016/S0886-3350(13)80320-3
45. Yildirim TM, Khoramnia R, Son HS, et al. Reasons for explantation of phakic intraocular lenses and associated perioperative complications: cross-sectional explant registry analysis. BMC Ophthalmol. 2021;21(1):80. doi:10.1186/s12886-021-01847-0
46. Kapoor S, Gupta S. Basic science of intraocular lens materials. In: Wang X, Ferreri M editors. Intraocular Lens. IntechOpen;2020. doi:10.5772/intechopen.92573
47. Henderson BA, Yang EB. Intraocular lens explantation technique for one-piece acrylic lenses. J Refract Surg. 2012;28(7):499–502. doi:10.3928/1081597X-20120531-01
48. Neuhann TH. Intraocular folding of an acrylic lens for explantation through a small incision cataract wound. J Cataract Refract Surg. 1996;22(Supplement 2):1383–1386. doi:10.1016/S0886-3350(96)80104-0
49. Pandit RT, Devgan U, Chapman JM. Twist and out intraocular lens removal. J Cataract Refract Surg. 2020;46(8):1072–1074. doi:10.1097/j.jcrs.0000000000000161
50. Duncan NB, Micheletti JM. Modified adaptation of the twist-and-out technique for intraocular lens exchange. J Cataract Refract Surg. 2022;48(12):1469–1471. doi:10.1097/j.jcrs.0000000000001047
51. Bhaumik A, Mitra S. A simple technique of intraocular lenses explantation for single-piece foldable lenses. Indian J Ophthalmol. 2017;65(12):1428. doi:10.4103/ijo.IJO_664_17
52. Fukuoka S, Kinoshita T, Morita S, Sakurai T. Intraocular lens extraction using the cartridge pull-through technique. J Cataract Refract Surg. 2021;47(12):e70–e74. doi:10.1097/j.jcrs.0000000000000695
53. Koo EY, Lindsey PS, Soukiasian SH. Bisecting a foldable acrylic intraocular lens for explantation. J Cataract Refract Surg. 1996;22(Supplement 2):1381–1382. doi:10.1016/S0886-3350(96)80103-9
54. Batlan SJ, Dodick JM. Explantation of a foldable silicone intraocular lens. Am J Ophthalmol. 1996;122(2):270–272. doi:10.1016/S0002-9394(14)72024-0
55. Mehta JS, Wilkins MR, Gartry DS. Explantation of an acrylic Acrysof ® intraocular lens without wound enlargement. Acta Ophthalmologica Scandinavica. 2005;83(2):262–263. doi:10.1111/j.1600-0420.2005.00373.x
56. Dagres E, Khan MA, Kyle GM, Clark D. Perioperative complications of intraocular lens exchange in patients with opacified Aqua-sense lenses. J Cataract Refract Surg. 2004;30(12):2569–2573. doi:10.1016/j.jcrs.2004.04.055
57. Kim TY, Moon IH, Park SE, Ji YW, Lee HK. Long-term follow-up of corneal endothelial cell changes after iris-fixated phakic intraocular lens explantation. Cornea. 2023;42(2):150–155. doi:10.1097/ICO.0000000000003001
58. AKF Y, ASY N. Complications and clinical outcomes of intraocular lens exchange in patients with calcified hydrogel lenses. J Cataract Refract Surg. 2002;28(7):1217–1222. doi:10.1016/S0886-3350(02)01357-3
59. Osher RH. Crisscross lensotomy: new explantation technique. J Cataract Refract Surg. 2006;32(3):386–388. doi:10.1016/j.jcrs.2005.12.133
60. Karamaounas N, Kourkoutas D, Prekates C. Surgical technique for small-incision intraocular lens exchange. J Cataract Refract Surg. 2009;35(7):1146–1149. doi:10.1016/j.jcrs.2009.02.036
61. Por YM, Chee SP. Trisection technique: a 2-snip approach to intraocular lens explantation. J Cataract Refract Surg. 2007;33(7):1151–1154. doi:10.1016/j.jcrs.2007.02.043
62. Ye H, Zhang S, Cao L, et al. Modified trisection technique: one-trip explantation for foldable intraocular lens. Retina. 2023;43(12):2075–2079. doi:10.1097/IAE.0000000000003430
63. Coassin M, Mori T, McLeod SD. Single-piece S-plasty for small-incision IOL removal. J Cataract Refract Surg. 2021;47(10):1367–1368. doi:10.1097/j.jcrs.0000000000000471
64. Fechin O. IOL explantation through small incision: cut and conquer. 2023. Available from: https://www.aao.org/education/clinical-video/iol-explantation-through-small-incision-cut-conque.
65. Carlà MM, Mateo C. An alternative technique for intraocular lens removal. Bimanual Cleavage Vitreous Chamber Retina. 2025;45(3):574–578. doi:10.1097/IAE.0000000000004168
66. Kumar DA, Agarwal A, Prakash G, Jacob S, Agarwal A, Sivagnanam S. IOL scaffold technique for posterior capsule rupture. J Refract Surg. 2012;28(5):314–315. doi:10.3928/1081597X-20120413-01
67. Parikakis EA, Chalkiadakis SE, Mitropoulos PG. Piggybacking technique for vitreous protection during opacified intraocular lens exchange in eyes with an open posterior capsule. J Cataract Refract Surg. 2012;38(7):1130–1133. doi:10.1016/j.jcrs.2012.05.019
68. Borkenstein AF, Borkenstein EM, Malyugin B. Ophthalmic Viscosurgical Devices (OVDs) in challenging cases: a review. Ophthalmol Ther. 2021;10(4):831–843. doi:10.1007/s40123-021-00403-
69. Narang P, Steinert R, Little B, Agarwal A. Intraocular lens scaffold to facilitate intraocular lens exchange. J Cataract Refract Surg. 2014;40(9):1403–1407. doi:10.1016/j.jcrs.2014.07.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.