Back to Journals » Patient Preference and Adherence » Volume 20
Supportive Care Needs and Patient Preferences Across the Treatment Journey Among Women with Stage III–IV Breast Cancer in Urban and Rural Tasikmalaya, Indonesia: A Qualitative Study
Authors Fauzan NH ![]() , Pahria T, Nursiswati N
, Pahria T, Nursiswati N ![]() , Juniar R
, Juniar R ![]()
Received 17 April 2026
Accepted for publication 10 June 2026
Published 19 June 2026 Volume 2026:20 617816
DOI https://doi.org/10.2147/PPA.S617816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Naufal Hafizh Fauzan, Tuti Pahria, Nursiswati Nursiswati, Rizki Juniar
Faculty of Nursing, Padjadjaran University, Bandung, Indonesia
Correspondence: Naufal Hafizh Fauzan, Faculty of Nursing, Padjadjaran University, Bandung, Indonesia, Tel +62 851-5681-1602, Email [email protected]
Purpose: To explore supportive care needs and patient preferences among women with stage III–IV breast cancer across the entire treatment journey, specifically examining how the urban–rural context shapes these experiences in Tasikmalaya, Indonesia.
Patients and Methods: This qualitative study recruited 10 women with stage III–IV breast cancer receiving routine care (chemotherapy, hormonal therapy, and/or follow-up) at Jasa Kartini Hospital, Tasikmalaya. Participants were purposively sampled. Data were collected through semi-structured in-depth interviews (audio-recorded) and field notes. Reflexive thematic analysis was conducted following Braun and Clarke. Reporting was guided by the COREQ checklist.
Results: Participants experienced treatment delays ranging from 1 to 6 years. Five key findings regarding supportive care needs and preferences were identified: (1) a critical need for credible education to address chemotherapy fears and health-system confusion; (2) a strong preference for psychosocial support through family accompaniment and peer-survivor networks; (3) a reliance on spiritual support (e.g. prayer and dhikr) for hope and acceptance; (4) urgent practical and non-medical financial needs (transport and logistics) that persist despite national insurance coverage; and (5) a dynamic shift in psychological experiences, moving from early distress toward death preparedness and acceptance.
Conclusion: Supportive care needs among women with advanced breast cancer are dynamic and significantly moderated by the urban–rural divide, which creates distinct logistical and non-medical economic hurdles even under universal health coverage. Oncology nursing practice should transition toward phase-sensitive care models that prioritize patient navigation to address “hidden” financial burdens and integrate culturally sensitive spiritual support to enhance patient resilience and treatment continuity throughout the complex illness trajectory.
Keywords: treatment adherence, chemotherapy fear, peer support, spiritual coping, financial toxicity, patient navigation
Introduction
Breast cancer remains a major global health problem and contributes substantially to morbidity and mortality among women.1,2 In Indonesia, the breast cancer burden is high, and a critical challenge is the large proportion of patients presenting with advanced-stage disease. Late presentation affects treatment options, care complexity, and prognosis.3–5
Advanced breast cancer (stage III–IV) often involves extensive locoregional disease and/or metastasis, shifting goals of care beyond cure toward symptom relief and quality-of-life preservation.6,7 At this stage, women experience multidimensional burdens, including chronic pain, fatigue, sleep disturbance, reduced functional capacity, and metastasis-related complications.8–10 Advanced disease is also frequently associated with cachexia (weight and muscle loss, anorexia, chronic inflammation, and hypoalbuminemia), increasing weakness and dependency.9,11
Psychological and social impacts are also prominent. Women with breast cancer are at increased risk of anxiety, reduced self-esteem, and negative self-concept related to bodily changes, prognostic uncertainty, and disrupted roles.12,13 Treatments such as mastectomy, chemotherapy-related changes (eg., hair loss), and hormonal effects may contribute to perceived loss of femininity and body image distress.14,15 In advanced stages, uncertainty and treatment burden often intensify emotional needs for both patients and families.9,16 These challenges underscore the importance of comprehensive, patient-centered care that extends beyond medical treatment to address supportive care needs.
Supportive care encompasses informational, physical, psychological, social, spiritual, and practical needs (eg., transport and accompaniment) and is central to oncology nursing practice.9,16,17 The scope of Patient Preference and Adherence aligns with how patients’ preferences shape engagement with care and adherence to treatment recommendations.18,19 Practical constraints distance, non-medical costs, and limited accompaniment may contribute to delays, missed follow-ups, or discontinuation of care, and treatment delays have been linked to worse outcomes.19,20
In Indonesia, delays in detection and treatment initiation have been associated with limited knowledge, fear, economic constraints, access barriers, the use of traditional/alternative treatments, and variability in family support.21–25 Tasikmalaya provides a regional context where the urban–rural divide serves as a core determinant of care engagement rather than a mere demographic label. In rural areas, the scarcity of advanced medical resources specifically the absence of local radiotherapy necessitates long-distance travel to higher-level referral centers in cities like Bandung, creating profound transportation obstacles. Consequently, caregiver accompaniment becomes a mandatory yet burdensome requirement for rural patients, as families must bear “hidden” non-medical expenses (transportation, meals, and accommodation) and significant income loss despite BPJS (the Social Health Insurance Agency - Indonesia’s government-provided health insurance) coverage.26
Furthermore, in Indonesia, although the national health insurance system covers most medical and clinical care costs, supportive care services are still unevenly distributed across regional oncology facilities. Information support is often limited to basic clinical instructions and may not adequately address cultural misconceptions or fears of chemotherapy that contribute to treatment delays.27–29 Psychological and spiritual support is commonly provided through family and religious networks rather than integrated into routine clinical care, while formal patient navigation services are largely absent, particularly in helping patients manage non-medical financial burdens such as transportation and accommodation costs.29–31 Consequently, despite insurance coverage, these barriers can negatively affect treatment adherence. Moreover, most local studies have examined supportive care needs only at specific points in the cancer trajectory. This study addresses that gap by mapping patients’ needs across the entire treatment journey and providing a dynamic, phase-sensitive framework to guide culturally and geographically tailored oncology nursing interventions that target both clinical and structural barriers.
Despite growing research on cancer experiences, qualitative evidence mapping supportive care needs and preferences among Indonesian women with advanced breast cancer remains limited, including how preferences intersect with access barriers in regional settings.23,31 One of the main limitations of the existing cancer literature is the scarcity of qualitative studies; most existing studies provide only a static picture of patients’ needs at specific clinical stages.32–36 This study directly fills this gap by examining the entire treatment journey, providing a foundation for culturally and geographically tailored supportive care interventions that address both medical and structural barriers in Indonesia. By tracking the patient experience from the initial recognition of symptoms and the “cognitive barriers” that lead to treatment delays through to the final stages of active treatment and the end-of-life phase, this study presents a comprehensive framework for stage-specific supportive care that aligns with each patient’s unique disease course.
Therefore, this study aimed to explore supportive care needs and patient preferences among women with stage III–IV breast cancer across the entire treatment journey, specifically examining how the urban–rural context shapes these experiences in Tasikmalaya, Indonesia; considering the urban–rural context shaping access and support. The guiding research question was: How do women with advanced breast cancer (stage III–IV) describe supportive care needs and support preferences across the treatment journey within an urban–rural context?
Materials and Methods
Study Design
This qualitative study explored supportive care needs and patient preferences among women with stage III–IV breast cancer. Data were analyzed using reflexive thematic analysis following Braun and Clarke’s six-phase approach with an inductive orientation.37 Reporting was guided by the COREQ checklist (The results of the COREQ checklist are listed in Section 1. Supplementary Table COREQ).38
Setting
The study was conducted at Jasa Kartini Hospital, Tasikmalaya, Indonesia, through oncology outpatient and chemotherapy services. Interviews were conducted at participants’ residences (as preferred for privacy and comfort). In this regional context, access to radiotherapy often required referral to a higher-level referral center, increasing logistical burden and non-medical costs despite national insurance coverage for medical care.
Participants and Sampling
Participants were 10 adult women with stage III–IV breast cancer receiving routine care (chemotherapy and/or hormonal therapy and/or follow-up). Purposive sampling aimed to capture variation in urban/rural residence, age, and clinical status (metastatic/stable disease, recurrence, or remission). Stage III–IV status was verified using clinical records/medical charts (initial and/or current diagnosis). Urban–rural classification was based on recorded residence (village/subdistrict and district) and used for contextual interpretation rather than quantitative comparison.
We agreed to study 10 participants, a number deemed sufficient for phenomenological research based on Polit & Beck’s theory as cited in Timmins,39 who suggest a range of 3 to 10 participants, as well as Creswell,40 who states that a homogeneous sample of 3–10 people is sufficient to capture the essence of the phenomenon. Furthermore, limiting the study to 10 participants was also justified by the fact that data collected from both urban and rural contexts, representing various clinical conditions and associated challenges, provided a sufficiently rich and comprehensive understanding to map the evolving needs for supportive care among women with advanced-stage breast cancer.
Inclusion criteria were: adult women; stage III or IV breast cancer; first hospital presentation occurred at an advanced stage (III/IV); and ability to communicate in Indonesian and/or Sundanese. Exclusion criteria were: verbal communication impairment; severe symptoms likely to compromise interview participation; and very poor general condition/fatigue.
Recruitment Procedures
After institutional permission was obtained, eligible patients were identified with support from oncology service staff. Potential participants were approached during routine visits. The researcher explained study aims, procedures, potential discomfort, confidentiality, and voluntary participation. Written informed consent was obtained prior to interviews.
Data Collection
Data were collected through in-depth, semi-structured interviews conducted by the first author, Naufal Hafizh Fauzan, a male researcher and Master’s student in Nursing with a specialization in Medical-Surgical Nursing. The researcher has a professional background as an oncology nurse with three years of experience at the study site (through 2024), which provided him with a deep understanding of the clinical and psychological conditions of breast cancer patients. Regarding methodological competence, the researcher received specialized training in qualitative methodology during his graduate studies, with intensive guidance from an advisory team comprising experts in qualitative research on cancer cases.
To demonstrate reflexivity and minimize potential bias or power imbalances (where participants might view the researcher solely as a medical professional), the researcher applied bracketing techniques to set aside personal clinical assumptions in order to understand the phenomena purely from the participants’ perspective. Additionally, the researcher used a reflective journal, conducted peer debriefings, and maintained an audit trail to ensure that data interpretation remained objective and transparent. The researcher also ensured a safe and conducive interview setting to encourage participant openness without feeling pressured by prior clinical relationships. Interviews were conducted in Indonesian and/or Sundanese, lasted approximately 30 minutes, and were audio-recorded with participants’ permission and supplemented by field notes. During the interview process, the researcher formulated key questions related to this topic, namely:
- What was your physical condition and the state of the lump in your breast when you first came to the hospital for treatment?
- What was your experience with having advanced-stage breast cancer before seeking treatment at the hospital?
- How do you feel now about facing your breast cancer diagnosis?
- How were you able to go through the entire breast cancer treatment process?
- What did you do before seeking treatment at the hospital?
- What did you know about your condition before seeking treatment at the hospital?
- Are there any customs or cultural practices in your community or neighborhood that influenced how your condition was managed before and after seeking treatment at the hospital?
Data collection period: January 2026 – March 2026
Interview location: participants’ residences
Repeat interviews: not conducted
End-of-interview clarification: key phrases were briefly summarized and confirmed; appreciation was expressed.
The interview guide was developed under the intensive supervision of academic experts in qualitative cancer research to ensure the questions remained open-ended and non-leading. Key areas of exploration included the initial recognition of physical symptoms (eg., the state of the lump), life experiences prior to hospital-based care, current emotional responses to the diagnosis, the progression through various treatment stages, and the influence of community culture or habits on their treatment choices. To ensure technical effectiveness and logical flow, the researcher conducted interview simulations before the formal data collection process began.
Data Analysis
Audio recordings were transcribed verbatim. Reflexive thematic analysis followed six phases: familiarization, initial coding, generating candidate themes, reviewing themes, defining and naming themes, and reporting with representative quotations.37 The analysis used a manual approach. Reflective thematic analysis was conducted manually by the principal investigator (first author). To ensure the transparency of the analysis and minimize individual bias, the initial codes and resulting categories were reviewed and validated through in-depth discussion sessions with the co-authors. This process involved a systematic transformation in which statements of significance were extracted from verbatim transcripts, organized into descriptive categories (significance statement), and then synthesized into subthemes and five final themes. Further details on the development of the theme are provided in Section 2 Supplementary Table Theme Analysis.
Rigor/Trustworthiness
Trustworthiness was enhanced through peer debriefing, maintaining an audit trail, and using a reflexive journal. Thick description supported transferability, and verbatim quotations enhanced transparency. Despite the researcher’s professional background as an oncology nurse at the study site, no prior clinical or personal contact had occurred with the participants recruited for this study.
Although the full transcripts were not returned to participants for formal revision due to their severe clinical condition and the limited accommodations and transportation available for this study, credibility was maintained through direct verification at the end of each interview. The researcher provided a brief summary of the key phrases and concepts discussed, allowing participants to immediately confirm or clarify their statements to ensure that the findings authentically reflected their life experiences.
A number of authors have argued that member checking is not an effective indicator of research rigor due to a lack of evidence that it improves the quality of research findings. A critical review indicates that this method does not guarantee validity or trustworthiness, and in fact raises various practical and philosophical issues; therefore, researchers are advised to shift toward member reflections (reflective dialogue) rather than merely post-interview truth verification.41,42 This is reinforced by the literature, which highlights various dilemmas in its application, such as the limitations of interpretive legitimacy, power imbalances, and participants’ tendency to merely offer agreement without making a substantive contribution to data validity.43
Ethical Considerations
Ethical approval was obtained from the Health Research Ethics Committee of Universitas Padjadjaran (approval number: 71/UN6.KEP/EC/2026), which mandated that the study be conducted in accordance with the Declaration of Helsinki. All participants have provided written informed consent; the informed consent form includes consent to participate in the study and consent for the findings to be published while maintaining the confidentiality of the participants’ identities. Confidentiality is maintained through anonymization (P1–P10) and secure data storage.
Results
Participant Characteristics
This study included 10 women with stage III–IV breast cancer residing in urban and rural areas of Tasikmalaya. All participants reported delayed initiation of medical treatment (1–6 years). At the time of interview, clinical status varied (metastatic stable disease, recurrence, hormonal therapy, and complete remission). Detailed study characteristics are presented in Table 1, while the complete list of diagnoses is provided in Section 3. Supplementary Table DemoFigureic and Complete Diagnosis of Participants.
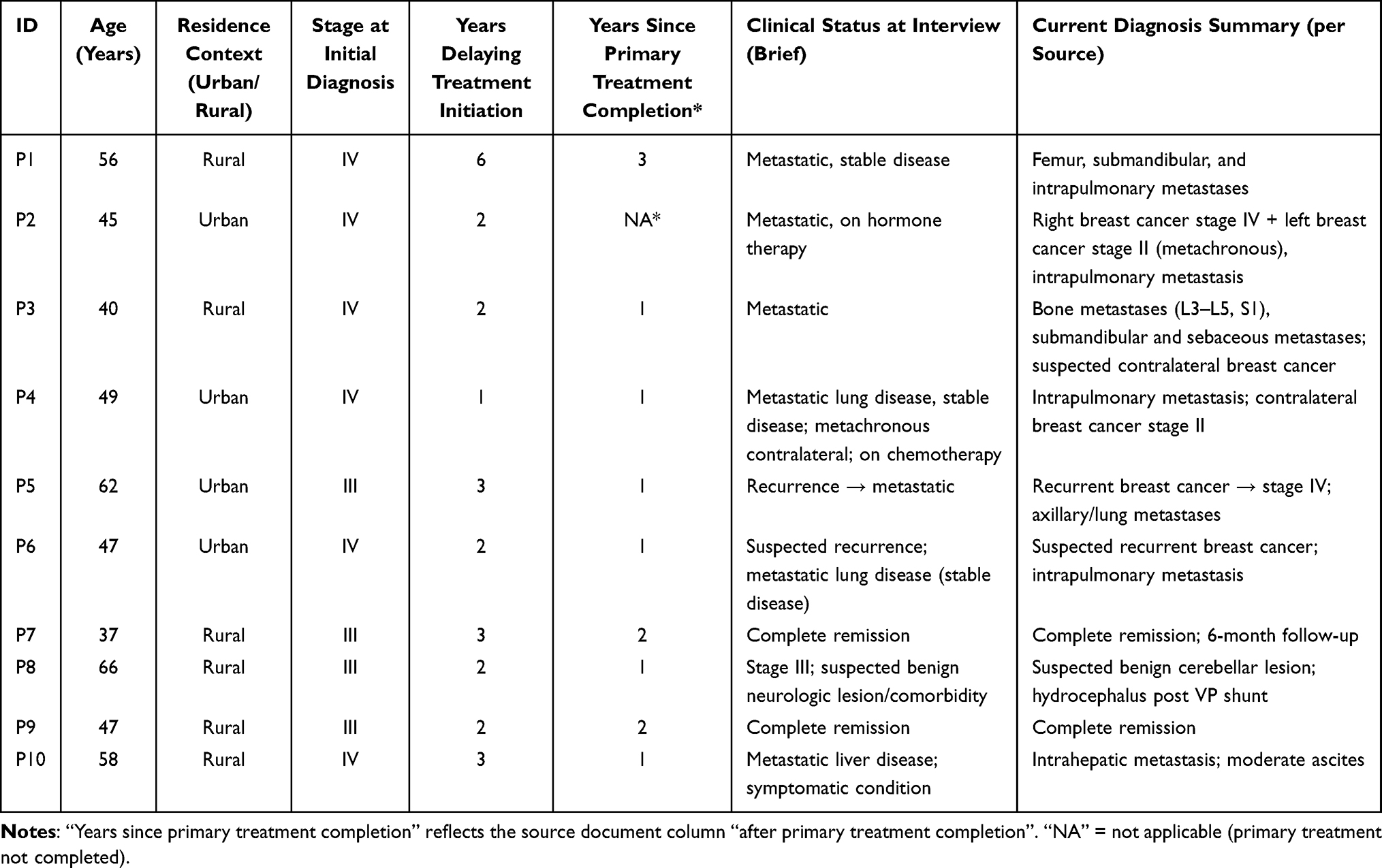 |
Table 1 Demographic and Clinical Characteristics of Participants (N=10) |
Overview of Themes
Reflexive thematic analysis identified five themes describing supportive care needs and patient preferences across the treatment journey (Further details are provided in Table 2 and Section 4. Supplementary Table Illustrative Quotes). Overall, supportive care needs and patient preferences were shaped and evolved across the illness and treatment journey from early symptom recognition and treatment initiation to repeated treatment and follow-up, post-primary treatment, and/or recurrence/metastasis, with some participants describing increasing acceptance, including death acceptance. The systematic development from raw data to final themes is visually illustrated in a coding tree (available in Section 2. Supplementary Table Theme Analysis). This presentation allows readers to track how participants’ specific statements regarding their treatment journeys were categorized and interpreted within a broader thematic structure.
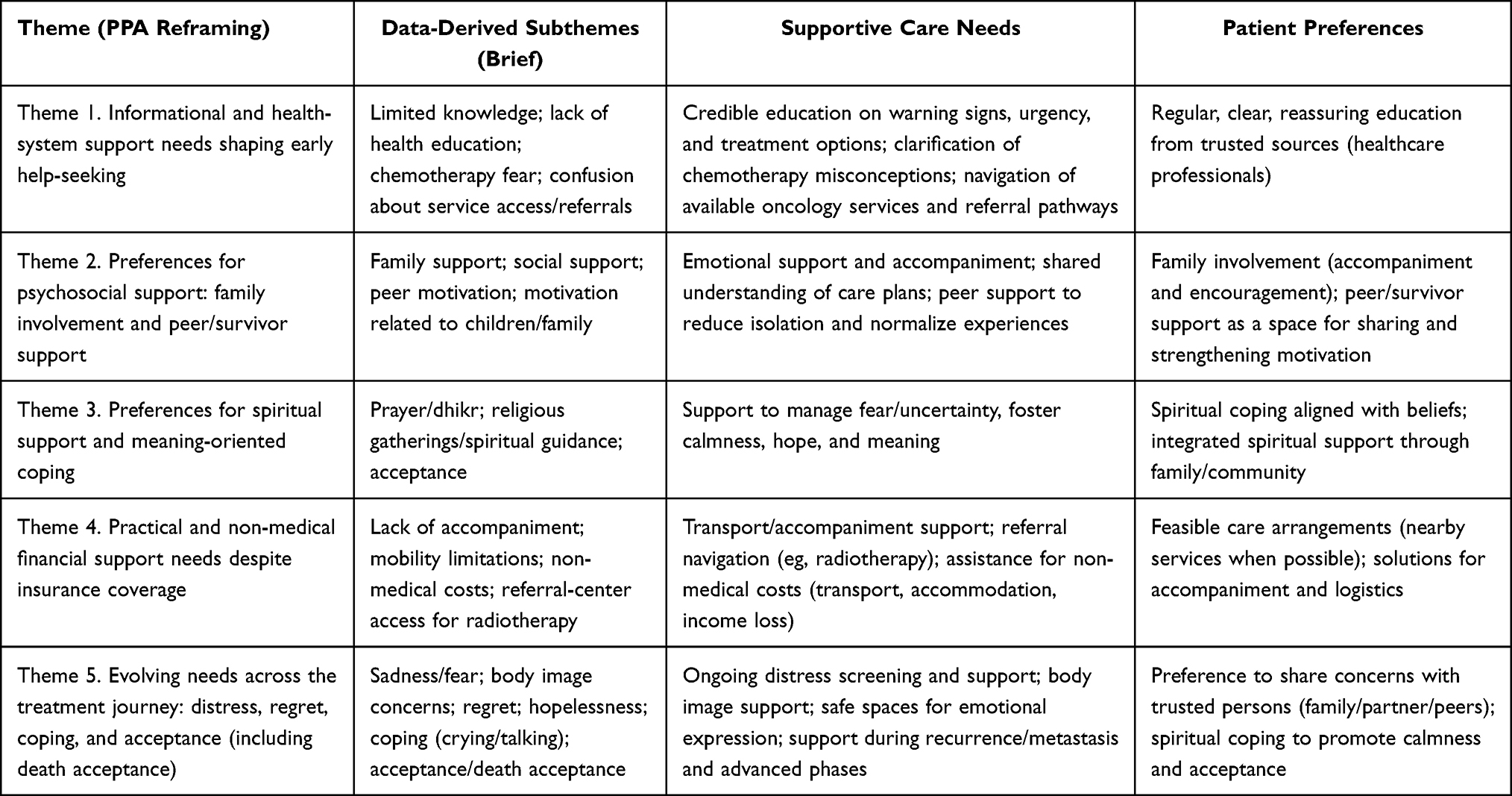 |
Table 2 Supportive Care Needs and Patient Preferences |
Theme 1. Informational and Health-System Support Needs Shaping Early Help-Seeking
In the early phase, participants described information needs as a key determinant of whether they initiated hospital-based care. Delays occurred because some participants did not recognize breast symptoms as dangerous or requiring urgent care: “Before seeking treatment, I didn’t know this was dangerous breast cancer; I thought it wasn’t serious.” (P1; translated). Limited community health education further prolonged uncertainty: “In my area there was no health education… I hope there will be regular sessions so people won’t be as unaware as I was.” (P3; translated). Participants also highlighted chemotherapy-related fears shaped by community narratives, indicating a need for reassuring, evidence-based education: “There were many comments that after chemo people died… so I was afraid to decide to start chemotherapy.” (P3; translated). Confusion about service availability and referral pathways also contributed to delays: “I didn’t know chemotherapy was available at this hospital.” (P3; translated). Overall, participants needed clear education about the disease, treatment options, and referral pathways, and preferred regular, understandable, reassuring information from trusted healthcare professionals.
Theme 2. Preferences for Psychosocial Support: Family Involvement and Peer/Survivor Support
During treatment, meaningful psychosocial support was commonly described as coming from family and peers. Participants emphasized needs for accompaniment, emotional strengthening, and practical/financial assistance. Family support was described as motivating: “My family was always there… accompanying me to appointments… that made me feel motivated.” (P9; translated). Spousal support was also perceived as important for treatment continuity: “My husband supported me to get treatment… from the beginning, he wanted me to seek care quickly.” (P7; translated). Peer/survivor support provided distinct psychological benefits, including reduced isolation, normalization of fear, and strengthened hope: “We were going through it together… we supported each other.” (P2; translated) and “I met many friends… we supported one another.” (P8; translated). These findings indicate ongoing emotional needs and strong preferences for family involvement and peer support as motivators across the treatment journey.
Theme 3. Preferences for Spiritual Support and Meaning-Oriented Coping
Spiritual support emerged as a consistent preference and was perceived to help manage fear, uncertainty, and psychological fatigue. Participants described coping through faith practices and community-based religious activities: “Getting closer to God became a strong motivation… I had hoped and surrendered the outcome.” (P2; translated). Spiritual support was viewed as more effective when facilitated within family/community ecosystems: “Our extended family holds regular religious gatherings… it helped my mental state and made me calmer.” (P9; translated). Participants also described a need for spiritual guidance to prevent self-blame and support acceptance: “There needs to be spiritual guidance; without it, I would blame myself.” (P4; translated). Overall, participants preferred spiritual coping aligned with their beliefs and integrated within family/community support.
Theme 4. Practical and Non-Medical Financial Support Needs Despite Insurance Coverage
Participants reported practical support needs that directly influenced treatment continuity and follow-up adherence. Lack of accompaniment led to delayed visits and worsened symptoms: “I was late for follow-up because no one could take me.” (P1; translated). These needs became more pronounced when referral-center services (eg., radiotherapy) were required, with accompaniment described as a key barrier: “I should have gone to a referral center, but no family member could accompany me.” (P1; translated). Non-medical financial needs also emerged, including transport and other operational costs: “My financial situation wasn’t stable… I saved money first, then started treatment and registered for insurance.” (P7; translated). Collectively, participants needed logistical and non-medical financial support and preferred feasible solutions through referral navigation and accompaniment support.
Theme 5. Evolving Needs Across the Treatment Journey: Distress, Regret, Coping, and Acceptance (Including Death Acceptance)
This theme illustrates the dynamic nature of supportive care needs. In early or intensive treatment phases, participants described profound distress and associated diagnosis with death: “At first it felt like my world collapsed… like death was right in front of me.” (P4; translated). Some later expressed regret about delayed treatment or postponing chemotherapy: “Sometimes I regret why I didn’t agree to chemo earlier.” (P3; translated). Participants described coping strategies such as talking/venting to relieve emotional burden: “Talking about it makes me feel relieved.” (P3; translated). For some, spiritual meaning-making contributed to acceptance, including readiness to face death: “I feel calmer now and ready to face death… I pray for a good ending.” (P5; translated). Overall, participants required ongoing psychological support, safe spaces for emotional expression, body image support, and spiritual support, and preferred support from trusted persons (family/partner/peers) and approaches that facilitated calmness and acceptance.
To summarize relationships across themes and phases of care, we developed a patient journey aligned supportive care needs map (See Figure 1 and Supplementary Figure 1).
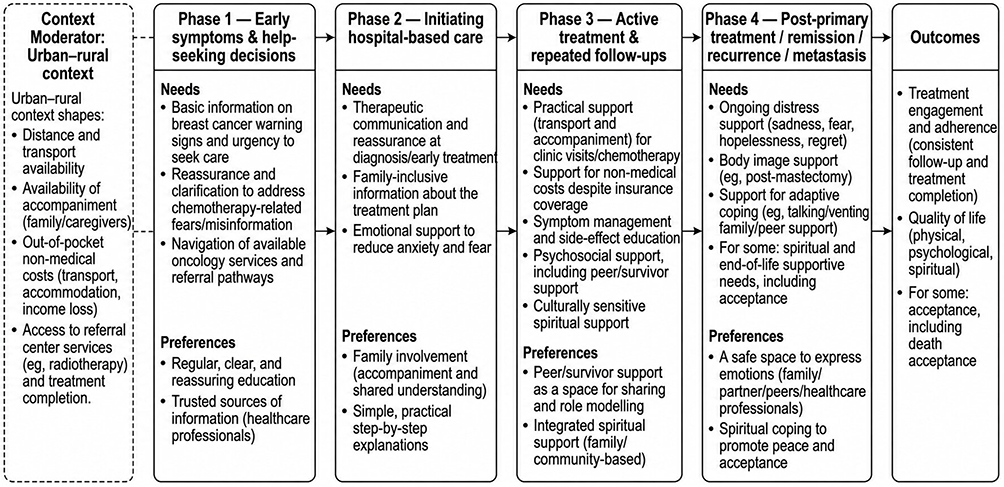 |
Figure 1 Patient journey–aligned map of supportive care needs and patient preferences among women with stage III–IV breast cancer in Tasikmalaya, Indonesia. The figure illustrates how informational, psychosocial (family and peer/survivor support), spiritual, and practical/financial needs evolve across phases of care. Urban–rural context is presented as a moderator shaping access, accompaniment, non-medical costs, and access to referral center services (e.g., radiotherapy), which may influence treatment engagement and adherence. |
Discussion
This qualitative study mapped supportive care needs and patient preferences among women with stage III–IV breast cancer across the treatment journey in an urban–rural regional context. Overall, needs and preferences were dynamic, shifting from early information and reassurance needs to ongoing psychosocial, spiritual, and practical support needs that influenced treatment engagement and continuity.
Principal Findings
A central finding of this study is that supportive care needs are not static but form a dynamic trajectory that shifts significantly across the entire treatment journey. While initial needs are dominated by health-system navigation and fears of medical procedures, these evolve into complex psychosocial and spiritual requirements as patients move through active treatment toward phases of recurrence or death acceptance.Five key insights emerged. First, informational needs and health-system navigation were most prominent early and shaped help-seeking decisions. Participants described limited knowledge of warning signs, minimal community health education, and uncertainty about service availability. Importantly, chemotherapy-related fear was often reinforced by community narratives, indicating that supportive education should include reassurance and empathic risk communication rather than solely factual information.
Second, psychosocial support preferences centered on family involvement and peer/survivor support. Family support was valued not only emotionally but also for accompaniment and practical problem-solving. Peer/survivor support provided normalization, hope, and role modeling, suggesting that supportive care models grounded in family and peer networks may be both preferred and feasible.
Third, participants consistently preferred spiritual support and meaning-oriented coping. Prayer/dhikr and community-based religious activities were perceived as sources of calmness and hope and helped participants move toward acceptance, including death acceptance in some cases.
Fourth, practical and non-medical financial needs strongly shaped continuity of care despite national insurance coverage for medical costs. Transport, accompaniment, operational expenses, and access to referral-center services (eg, radiotherapy) were recurrent barriers closely linked to adherence behaviors such as delayed follow-ups.
Fifth, psychological needs evolved across phases of care: early distress could progress to regret about delayed care, and in some cases to acceptance, including death acceptance. This highlights the need for repeated, phase-sensitive psychosocial support rather than one-time counseling.
Comparison with Literature
Drivers of delayed treatment in this study limited knowledge, fear of medical treatment, and social narratives align with evidence from Indonesia and other low- and middle-income settings, where delays are associated with low awareness, access constraints, economic burden, and the use of traditional/alternative treatments.21–25 The prominence of chemotherapy-related fear supports the importance of culturally responsive education that addresses misconceptions and anticipatory anxiety.
Family involvement is widely recognized as a key factor in treatment engagement and decision making, particularly in collectivist contexts. Our findings extend this by showing that family involvement was also essential for practical adherence-related tasks such as accompaniment. Peer/survivor support has been associated with reduced isolation and improved coping; in this study it appeared to function as a “real-world credibility anchor” that helped patients reinterpret chemotherapy as manageable.
Spiritual coping and meaning-making have been reported as central resources in advanced and metastatic cancer. Our findings align with qualitative evidence that spirituality and psychosocial resources support coping with uncertainty and fear of death.44–46 Community-based religious practices in this setting appeared acceptable and calming, suggesting that spiritual care integration may be feasible through collaboration with existing community resources.
Practical barriers and non-medical expenses reflect global discussions of financial toxicity and access barriers even when medical costs are covered. These barriers can disrupt follow-up schedules and treatment pathways; treatment delay has been associated with poorer outcomes.20,47,48 Although this qualitative study does not quantify outcomes, participants’ narratives indicate pathways by which non-medical costs and accompaniment constraints may undermine continuity of care.
Furthermore, a novel contribution of this research is its exploration of the illness experience as a continuous process rather than a snapshot in time. Most existing studies in the literature are cross-sectional, providing only a limited view of patient needs at a specific clinical stage.34,35 In contrast, our study captures the evolving nature of these needs from the initial “cognitive and structural barriers” that cause treatment delays to the eventual “spiritual peace and death preparedness”. By tracking these changes from diagnosis through the various stages of treatment and follow-up, this study offers a more comprehensive framework for oncology nurses to provide phase-sensitive support that aligns with the patient’s specific position in their treatment journey.
Implications for Oncology Nursing Practice
These findings suggest several practice directions aligned with patient preferences and the goal of improving engagement and adherence:
- Reassuring, patient-centered education to address chemotherapy fears and misinformation. Use clear explanations of treatment goals in advanced stages, what to expect during chemotherapy, and practical self-management strategies; apply teach-back for both patients and families.
- Family-inclusive supportive care. With patient permission, involve family members in education and planning, including schedules, side-effect management, and red-flag symptoms.
- Peer support and survivor navigator approaches. Structured peer groups (in-person or messaging-based) may match patient preferences; nurse facilitation can maintain information accuracy and psychological safety.
- Culturally sensitive spiritual care integration. Conduct brief spiritual assessment and offer referral options (faith leaders/community resources). Spiritual support should complement—not replace—medical treatment.
- Routine distress screening and referral pathways. Because distress and regret emerge across phases, screening should be repeated, with clear referral pathways for severe anxiety/depression/hopelessness and persistent body image distress.
- Patient navigation for transport, accompaniment, and non-medical costs. Collaboration with social workers is essential to map resources (transport support, community assistance) and reduce practical adherence barriers.
Urban–Rural Context Considerations
Furthermore, the urban–rural context in this study serves as a critical moderator of care accessibility rather than a mere demographic label. In the regional setting of Tasikmalaya, rural patients face profound transportation obstacles and a total reliance on family accompaniment due to the absence of essential services like radiotherapy in local facilities. This geographic divide intensifies what is globally recognized as “financial toxicity,” yet in our Indonesian context, the burden is distinctly non-medical. Despite medical costs being covered by BPJS, the cumulative “hidden costs” including long-distance travel to referral centers in cities like Bandung, accommodation, and the loss of household income for caregivers create a significant structural barrier that directly triggers treatment delays. These findings highlight a gap in the current supportive care model in Indonesia, which often overlooks the logistical and economic realities of regional patients.
The practice of spiritual support through prayer, dhikr, and community religious activities serves as a significant coping mechanism for survivors; however, its manifestation is influenced by the participants’ residential context. In urban settings, spiritual coping tends to be practiced personally and individually as a form of self-regulated emotional regulation. This is demonstrated by Participant 2 (P2), who comes from an urban area, where they routinely perform dhikr and pray at night to gain inner strength and peace in facing their illness.
Conversely, in rural contexts, spiritual support is more deeply integrated into the family ecosystem and broader social networks through collective activities. Participant 9 (P9), from a rural area, revealed that regular family gatherings serve as the primary pillar of mental support for them. These gatherings involve collective prayers for sick family members, which directly provide P9 with a sense of calm and mental preparedness as they navigate their treatment journey. This contrast highlights how the urban context emphasizes internal spiritual coping, while the rural context leverages strong religious social capital to build survivors’ resilience.
Strengths and Limitations
Strengths include in-depth exploration across multiple phases of the treatment journey, supported by verbatim quotes and a practical conceptual map. Limitations include single-center sampling, small sample size, and heterogeneity of clinical status (remission vs metastatic/recurrence), which may affect the salience of specific needs. The researcher’s oncology nursing background may have influenced data collection and interpretation; reflexivity and audit trails were used to mitigate this risk. Urban–rural classification was used for contextual interpretation rather than systematic comparison.
Furthermore, this study is limited by the absence of formal member checking for the final themes and findings, which may affect the confirmability of the results. However, this was mitigated by maintaining a rigorous audit trail, using a reflexive journal, and conducting frequent peer debriefing among the research team to ensure the depth and accuracy of the qualitative interpretation.
Recommendations for Future Research
Future studies should include multi-site sampling, caregiver-focused research, and the development and feasibility testing of nurse-led supportive care interventions (anti-misinformation education, navigation models, and repeated distress screening workflows). Research should also evaluate peer support/survivor navigator programs and apply more objective urban–rural classification to clarify how geographic context shapes access barriers and non-medical financial burden.
Conclusion
Women with stage III–IV breast cancer in Tasikmalaya experience complex, dynamic supportive care needs that evolve across the entire treatment journey, shifting from early informational gaps and chemotherapy-related fears toward a profound requirement for spiritual peace and death preparedness in advanced phases. The urban–rural divide significantly moderates these experiences; while urban patients often utilize individual spiritual coping, rural patients face intensified accessibility barriers and rely heavily on collective social capital and family-integrated spiritual support to navigate care. Furthermore, despite BPJS coverage, “financial toxicity” remains a critical barrier driven by non-medical costs such as long-distance transport, accommodation, and loss of household income. To bridge these gaps, oncology nursing practice must transition toward phase-sensitive care models that incorporate repeated distress screening and culturally sensitive spiritual interventions. Specifically, implementing nurse-led patient navigation in formal collaboration with social workers is essential to map logistical resources and coordinate accompaniment support, thereby mitigating non-medical economic burdens and ensuring treatment continuity for patients across diverse regional contexts.
Acknowledgments
The authors thank all participants for sharing their experiences, and Jasa Kartini Hospital, Tasikmalaya, for supporting study implementation. We also thank academic supervisors and colleagues who contributed to the research process and manuscript development. This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Breast cancer. World Health Organization. 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer.
2. International Agency for Research on Cancer. Cancer today. World Health Organization. 2022. Available from: https://gco.iarc.who.int/today.
3. Ministry of Health of the Republic of Indonesia. National cancer plan 2024–2034. Ministry of Health of the Republic of Indonesia. 2024. Available from: https://www.iccp-portal.org/sites/default/files/plans/Rencana_Kanker_Nasional_2024-2034.pdf.
4. Azhar Y, Agustina H, Abdurahman M, Achmad D. Breast cancer in west java: where do we stand and go? Indones J Cancer. 2020;14(3):91. doi:10.33371/ijoc.v14i3.737
5. Gautama W. Breast cancer in Indonesia in 2022: 30 years of marching in place. Indones J Cancer. 2022;16(1):1. doi:10.33371/ijoc.v16i1.920
6. Koo MM, Von Wagner C, Abel GA, McPhail S, Rubin GP, Lyratzopoulos G. Typical and atypical presenting symptoms of breast cancer and their associations with diagnostic intervals: evidence from a national audit of cancer diagnosis. Cancer Epidemiol. 2017;48:140–12. doi:10.1016/j.canep.2017.04.010
7. National Breast Cancer Foundation. Breast Cancer Stages. National Breast Cancer Foundation. 2026. Available from: http://www.nationalbreastcancer.org/breast-cancer-stages.
8. Humairah Nasution SA, Chalil MJA. Pengaruh stadium kanker payudara terhadap derajat nyeri dan kualitas hidup pasien kanker payudara di rsu. haji medan. J Kedokt Dan Kesehat Publ Ilm Fak Kedokt Univ Sriwij. 2023;10(3):317–324. doi:10.32539/jkk.v10i3.22072
9. Ebbestad FE, Ammitzbøll G, Horsbøll TA, et al. The long-term burden of a symptom cluster and association with longitudinal physical and emotional functioning in breast cancer survivors. Acta Oncol. 2023;62(7):706–713. doi:10.1080/0284186X.2023.2185909
10. Hammer MJ, Cooper B, Paul SM, et al. Identification of distinct symptom profiles in cancer patients using a pre-specified symptom cluster. J Pain Symptom Manage. 2022;64(1):17–27. doi:10.1016/j.jpainsymman.2022.03.007
11. Wawolumaja A, Pontoh V, Merung M. Terapi pada pasien kanker payudara stadium lanjut menurunkan kadar C- Reaktif protein dan meningkatkan kadar albumin. J Biomedik. 2019;11(2):116. doi:10.35790/jbm.11.2.2019.23324
12. Yektatalab S, Ghanbari E. The relationship between anxiety and self-esteem in women suffering from breast cancer. J Midlife Health. 2020;11(3):126–132. doi:10.4103/jmh.JMH_140_18
13. Ng CG, Mohamed S, Kaur K, Sulaiman AH, Zainal NZ, Taib NA. Perceived distress and its association with depression and anxiety in breast cancer patients. PLoS One. 2017;12(3). doi:10.1371/journal.pone.0172975
14. Thakur M, Sharma R, Mishra AK, Gupta B. Body image disturbances among breast cancer survivors: a narrative review of prevalence and correlates. Cancer Res Stat Treat. 2022;5(1):90–96. doi:10.4103/crst.crst_170_21
15. Pintado S. Self-concept and emotional well-being in patients with breast cancer. Rev Iberoam Psicol y Salud. 2017;8(2):76–84. doi:10.23923/j.rips.2017.08.007
16. Challinor JM, Alqudimat MR, Teixeira TOA, Oldenmenger WH. Oncology nursing workforce: challenges, solutions, and future strategies. Lancet Oncol. 2020;21(12):e564–e574. doi:10.1016/S1470-2045(20)30605-7
17. Drury A, Dowling M, Diez de Los Rios de la Serna C, et al. Advanced breast cancer education for cancer nurses: a systematic review. Nurse Educ Today. 2022;117(105477). doi:10.1016/j.nedt.2022.105477
18. Weiner SJ, Schwartz A, Sharma G, et al. Patient-centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158(8):573–579. doi:10.7326/0003-4819-158-8-201304160-00001
19. Brandstetter LS, Jírů-Hillmann S, Störk S, Heuschmann PU, Wöckel A, Reese JP. Differences in preferences for drug therapy between patients with metastatic versus early-stage breast cancer: a systematic literature review. Patient. 2024;17(4):349–362. doi:10.1007/s40271-024-00679-6
20. Pathak R, Leslie M, Dondapati P, et al. Increased breast cancer mortality due to treatment delay and needle biopsy type: a retrospective analysis of SEER-medicare. Breast Cancer. 2023;30(4):627–636. doi:10.1007/s12282-023-01456-3
21. Cut Sidrah N, Rizka A, Humaira Z. Utara Tahun 2020-2021 delay factors in breast cancer treatment at the cut meutia general hospital. J Ilm Mns Dan Kesehat. 2023;6:88–99. doi:10.31850/makes.v6i1.1942
22. Anwar SL, Tampubolon G, Van Hemelrijck M, Hutajulu SH, Watkins J, Wulaningsih W. Determinants of cancer screening awareness and participation among Indonesian women. BMC Cancer. 2018;18(1). doi:10.1186/s12885-018-4125-z
23. Shabrina A, Iskandarsyah A. Pengambilan keputusan mengenai pengobatan pada pasien kanker payudara yang menjalani pengobatan tradisional. J Psikol. 2019;46(1):72. doi:10.22146/jpsi.31902
24. Hasibuan AR, Pasaribu AF, Alfiyah S, Utami JN, Harahap NRY, Nurhayati. Peran pendidikan kesehatan dalam meningkatkan kesadaran masyarakat terhadap pola hidup sehat di era digital. Didakt J Kependidikan. 2024;13:305–318. doi:10.58230/27454312.1515
25. Hutajulu SH, Prabandari YS, Bintoro BS, et al. Delays in the presentation and diagnosis of women with breast cancer in Yogyakarta, Indonesia: a retrospective observational study. PLoS One. 2022;17(1 January). doi:10.1371/journal.pone.0262468
26. Suryanegara FDA, Iskandar D, Ekaputra E, et al. Costs analysis of radiotherapy for breast cancer in Indonesia: a comparison between reimbursement tariffs and actual costs. BMC Health Serv Res. 2025;25(1). doi:10.1186/s12913-025-12849-9
27. Prabandari YS, Hartanti W, Syafriani, et al. “Alas … my sickness becomes my family’s burden”: a nested qualitative study on the experience of advanced breast cancer patients across the disease trajectory in Indonesia. Breast. 2022;63:168–176. doi:10.1016/j.breast.2022.04.001
28. Martina D, Kustanti CY, Dewantari R, et al. Advance care planning for patients with cancer and family caregivers in Indonesia: a qualitative study. BMC Palliat Care. 2022;21(1). doi:10.1186/s12904-022-01086-0
29. Tjokroprawiro BA, Novitasari K, Saraswati W, Yuliati I, Ulhaq RA, Sulistya HA. The challenging journey of cervical cancer diagnosis and treatment at the second largest hospital in Indonesia. Gynecol Oncol Rep. 2024;51. doi:10.1016/j.gore.2024.101325
30. Sunarsih IM, Prabandari YS, Aryandono T, Sastrowijoto S. Exploring possible causes for delays seeking medical treatment among indonesian women with breast cancer. Asian J Pharm Clin Res. 2018;11(6):284–288. doi:10.22159/ajpcr.2018.v11i6.25211
31. Suarilah I, Nihayati HE, Wahyudi AS, Asmoro CP, Felipe-Dimog EB. Treatment decision-making experience among Indonesian women with obstetrics and gynecology-related cancer. Med Palliat. 2023;22(2):68–76. doi:10.1016/j.medpal.2022.08.004
32. Prawesti Priambodo A, Trisyani Y, Anna A, et al. The information needs of breast cancer patients at all stages of their journey: a protocol of scoping review. Padjadjaran Acute Care Nurs J. 2025;4(2):578182. doi:10.2147/ppa.s578182
33. Shariff NM, Azman N, Hami R, Mujar NMM, Bin Abdullah MFIL. Multicentre prospective cohort study of unmet supportive care needs among patients with breast cancer throughout their cancer treatment trajectory in Penang: a PenBCNeeds Study protocol. BMJ Open. 2021;11(3). doi:10.1136/bmjopen-2020-044746
34. Bu X, Jin C, Fan R, et al. Unmet needs of 1210 Chinese breast cancer survivors and associated factors: a multicentre cross-sectional study. BMC Cancer. 2022;22(1). doi:10.1186/s12885-022-09224-w
35. Cai T, Huang Q, Yuan C. Emotional, informational and instrumental support needs in patients with breast cancer who have undergone surgery: a cross-sectional study. BMJ Open. 2021;11(8). doi:10.1136/bmjopen-2020-048515
36. Sousa H, Almeida S, Bessa J, Pereira MG. The developmental trajectory of cancer-related cognitive impairment in breast cancer patients: a systematic review of longitudinal neuroimaging studies. Neuropsychol Rev. 2020;30(3):287–309. doi:10.1007/s11065-020-09441-9
37. Braun V, Clarke V. Teaching thematic analysis: overcoming challenges and developing strategies for effective learning. Psychologist. 2013;26:120–123.
38. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Heal Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
39. Timmins F. Nursing Research Generating and Assessing Evidence for Nursing Practice. Vol. 13.
40. Creswell JW. A concise introduction to mixed methods research. 2016.
41. Thomas DR. Feedback from research participants: are member checks useful in qualitative research? Qual Res Psychol. 2017;14(1):23–41. doi:10.1080/14780887.2016.1219435
42. Smith B, McGannon KR. Developing rigor in qualitative research: problems and opportunities within sport and exercise psychology. Int Rev Sport Exerc Psychol. 2018;11(1):101–121. doi:10.1080/1750984X.2017.1317357
43. Candela AG. Exploring the function of member checking. Qual Rep. 2019;24(3):619–628. doi:10.46743/2160-3715/2019.3726
44. Noriega Esquives BS, Walsh EA, Penedo FJ, et al. Coping strategies and psychosocial resources among women living with metastatic breast cancer: a qualitative study. J Psychosoc Oncol. 2024;42(3):381–397. doi:10.1080/07347332.2023.2254754
45. Lin HR, Bauer-Wu SM. Psycho-spiritual well-being in patients with advanced cancer: an integrative review of the literature. J Adv Nurs. 2003;44(1):69–80. doi:10.1046/j.1365-2648.2003.02768.x
46. Tao Y, Yu H, Liu S, et al. Hope and depression: the mediating role of social support and spiritual coping in advanced cancer patients. BMC Psychiatry. 2022;22(1). doi:10.1186/s12888-022-03985-1
47. Carrera PM, Kantarjian HM, Blinder VS. The financial burden and distress of patients with cancer: understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J Clin. 2018;68(2):153–165. doi:10.3322/caac.21443
48. Abrams HR, Durbin S, Huang CX, et al. Financial toxicity in cancer care: origins, impact, and solutions. Transl Behav Med. 2021;11(11):2043–2054. doi:10.1093/tbm/ibab091
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.