Back to Journals » Patient Preference and Adherence » Volume 12
Support needs for medication use and the suitability of eHealth technologies to address these needs: a focus group study of older patients with rheumatoid arthritis
Authors Mathijssen EGE, Vriezekolk JE, Eijsbouts AMM, van den Hoogen FHJ ![]() , van den Bemt BJF
, van den Bemt BJF
Received 28 September 2017
Accepted for publication 10 January 2018
Published 7 March 2018 Volume 2018:12 Pages 349—358
DOI https://doi.org/10.2147/PPA.S152759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Elke GE Mathijssen,1 Johanna E Vriezekolk,1 Agnes MM Eijsbouts,1 Frank HJ van den Hoogen,1,2 Bart JF van den Bemt3
1Department of Rheumatology, Sint Maartenskliniek, Nijmegen, the Netherlands; 2Department of Rheumatology, Radboud University Medical Centre, Nijmegen, the Netherlands; 3Department of Pharmacy, Sint Maartenskliniek, Nijmegen, the Netherlands
Objective: The objectives of this study were to explore the needs of patients with rheumatoid arthritis (RA) regarding support for medication use and to gain insight into their perspective on the suitability of eHealth technologies to address these needs.
Methods: Three focus groups were conducted with 28 patients with RA. Audio recordings made during the focus groups were transcribed verbatim. Two researchers independently performed an inductive, thematic analysis on the data (ie, the transcripts and field notes).
Results: The following three themes that described support needs of patients with RA for medication use were identified in the data: 1) informational support; 2) practical support; and 3) emotional support. Informational support reflected the provision of information and facts, including advice, suggestions, and feedback from health care providers. Practical support included the reinforcement of practical skills as well as the provision of medication aids and pharmacy services. Emotional support reflected a trusted patient–health care provider relationship, characterized by good communication. Although potential advantages of eHealth technologies to address the patients’ support needs were recognized, concerns over matters such as personal interaction with health care providers, privacy and data security, and the quality and reliability of online information were prevalent.
Conclusion: Patients with RA have informational, practical, and emotional support needs for medication use. Informational support seems to be most important. From the patients’ perspective, eHealth technologies may have the potential to address these needs. However, these technologies are regarded as a complement to, rather than a replacement of, current practices.
Keywords: qualitative research, rheumatology, information needs, practical needs, emotional needs
Introduction
Rheumatoid arthritis (RA) is a chronic, autoimmune disease that is characterized by inflammation of the joints, causing pain, swelling, and stiffness. If left untreated, RA can cause irreversible damage to the affected joints with resultant deformity and disability.1,2 It can also spread to other parts of the body.1–3 The treatment goal is clinical remission or at least low disease activity.4 Treatment consists primarily of pharmacotherapy or, more specifically, the use of disease-modifying antirheumatic drugs (DMARDs).4,5 Both synthetic and biologic DMARDs (bDMARDs) have proven to be clinically effective in treating RA.6,7
However, patients with RA encounter various problems with their medication. These problems hinder the effectiveness of treatment and have deleterious clinical consequences.8,9 Previous studies have identified various problems. For example, 54% of patients have inadequate knowledge of methotrexate therapy, which may result in incorrect usage,10 and 47% have concerns regarding potential adverse consequences of their medication prescriptions.11 Twenty percent are unable to open the pharmaceutical packages.12 Overall, 30%–80% of DMARD users do not take their medication as prescribed.13 The foregoing implies that current practices do not ensure safe and effective medication use.
Additional support might prevent or fix the problems that patients with RA encounter with their medication. Morgan et al,14 for example, indicated that higher perceived support from health care providers such as addressing treatment beliefs may improve adherence to adalimumab. Knowledge about patients’ support needs is therefore indispensable.15,16 In the light of patient-centered care, which places patients at the center of the health care system, their perspective should be taken into account.17 So far, no studies have explored the support needs of patients with RA for medication use from their own perspective.
Although patients with RA visit health care providers only a few times a year, they deal with their medication on a daily basis. Ongoing support is therefore preferable.18 Additional support could potentially be provided by eHealth, a term defined by the World Health Organization (WHO) as the use of information and communication technologies for health.19 eHealth technologies have the potential of supporting patients independent of place and time.20 However, it remains largely unknown if, or to what extent, patients with RA perceive a need for eHealth technologies and which preconditions should be met in order to implement and use them successfully. Therefore, the objectives of this study were to explore the needs of patients with RA regarding support for medication use and to gain insight into their perspective on the suitability of eHealth technologies to address these needs. To our knowledge, this is the first study approaching these objectives from the point of view of patients themselves.
Methods
Study design
A descriptive, exploratory design was used – thus, this study did not rely on a preexisting theoretical framework. Focus groups were conducted because this method of data collection is likely to yield the most valuable information in exploratory studies.21 Indeed, the group interaction enriched the quantity and quality of the information gathered.22
Two patients with RA (Herman van Duijn [HvD] and Peter van Grinsven [PvG]) were involved in this study as patient research partners. During the first contact meeting, mutual goals and expectations were discussed and these patients agreed that they would fulfill a consulting and advising role in all study phases.
Patient recruitment
A convenience sample was recruited from the Department of Pharmacy at the Sint Maartenskliniek, Nijmegen, the Netherlands. One of the researchers (BJFvdB), a certified clinical pharmacist at the Department of Pharmacy, had access to the register and was legally authorized as pharmacist to view the patients’ hospital records, which were used to identify eligible patients. Eligibility criteria were as follows: 1) clinical diagnosis of RA; 2) current use of at least one DMARD; 3) age ≥18 years; and 4) proficiency in the Dutch language. Eligible patients who received their medication at the Department of Pharmacy between January and April 2016 were sent an invitation by post to participate. Guided by previous experiences with this recruitment technique (ie, impersonal invitations to focus groups on predetermined dates and times), showing response rates of 10%–20%, 250 patients were invited. An incentive for participation was offered in the form of a 25 Euro gift card.
Data collection
The focus groups were conducted in a quiet, comfortable room at the Sint Maartenskliniek. An independent, experienced moderator (Annette Heijnen [AH] or Maaike Abrahamse [MA]) and an assistant moderator (EGEM or Ellen Selten [ES]) facilitated the focus groups. A discussion guide was used to standardize and structure the data collection (Figure 1).
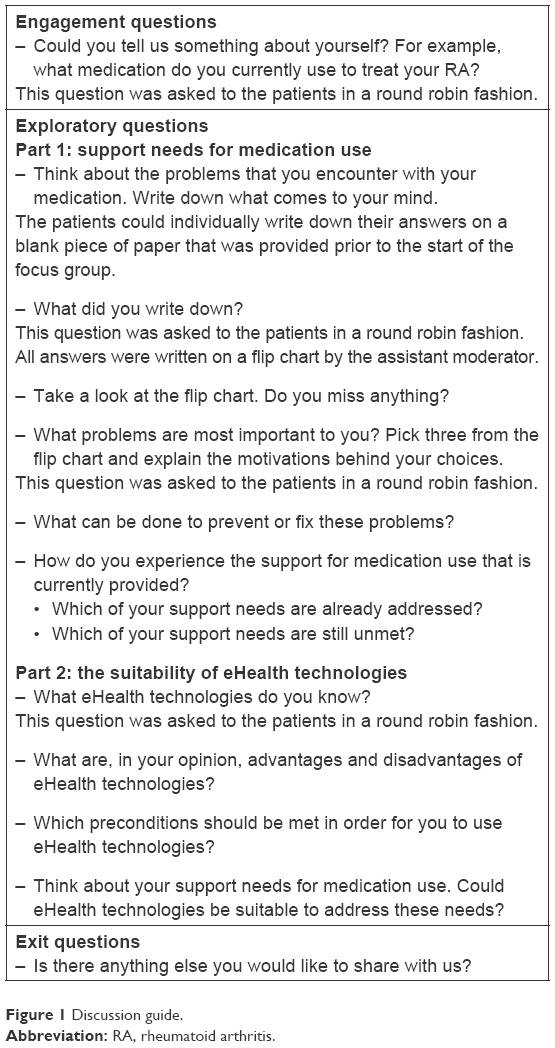 | Figure 1 Discussion guide. |
The discussion guide was developed in collaboration with the patient research partners and informed by a review of relevant literature.23–25 The moderator started with an engagement question and progressed to questions specific to the objectives of this study (ie, exploratory questions). The focus groups ended with an exit question.26 The discussions were audio recorded, and the audio recordings were subsequently transcribed verbatim by a professional transcription service. The assistant moderator did not actively take part in the discussions but monitored nonverbal behavior as well as linguistic and atmospheric elements and recorded these observations in field notes. After each focus group, the field notes were expanded into rich descriptions of these observations. The field notes were complementary to the transcripts since the latter did not reflect the entire atmosphere of the discussions. The field notes were used to aid in interpreting the findings.
Prior to the focus groups, each patient completed a brief questionnaire with demographic and clinical variables, including gender, date of birth, marital status, living status, level of education, employment status, disease duration, and current medication use.
Data analysis
An inductive, thematic analysis was applied to the transcripts and field notes. The six phases of thematic analysis were followed in an iterative manner by constantly moving back and forth between them. This comprised becoming familiarized with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and writing up the results.27 To ensure the trustworthiness of the data analysis, two researchers (EGEM and BJFvdB) independently analyzed the data.28 Discrepancies were resolved through discussion and consensus or referral to a third researcher (JEV). Memos were written to help the researchers keep track of decisions made during analysis of the data.28 The occurrence of data saturation was investigated. The number of focus groups was considered sufficient when the analysis of the last focus group did not result in the identification of new themes. The software program MAXQDA 10 was used to analyze the data. Additionally, a member check was conducted. For each focus group, a summary of the discussions was sent to the patients who participated in that particular group. They were asked to comment on its factual and interpretative accuracy, and adjustments were made accordingly. Some relevant quotes of the patients were selected to support the findings. The quotes were translated from Dutch to English by a certified translation bureau.
Ethical considerations
The Medical Research Ethical Committee of Arnhem-Nijmegen, the Netherlands, waived ethical approval since the medical research involving human subjects act did not apply to this study (file number: 2016-2464). All patients gave written informed consent for participation. Patient data were handled according to the applicable laws and regulations (eg, the Dutch Data Protection Act). Personal identifying information was replaced by study codes. A document that linked the study codes to the patients’ identifying information was digitally stored and protected. Only the researchers directly involved in this study had access to the document.
Results
A total of 28 (11%) eligible patients responded to the invitation. They participated in three focus groups that were conducted in May 2016. The discussions lasted between 100 and 150 minutes. The patient characteristics are shown in Table 1.
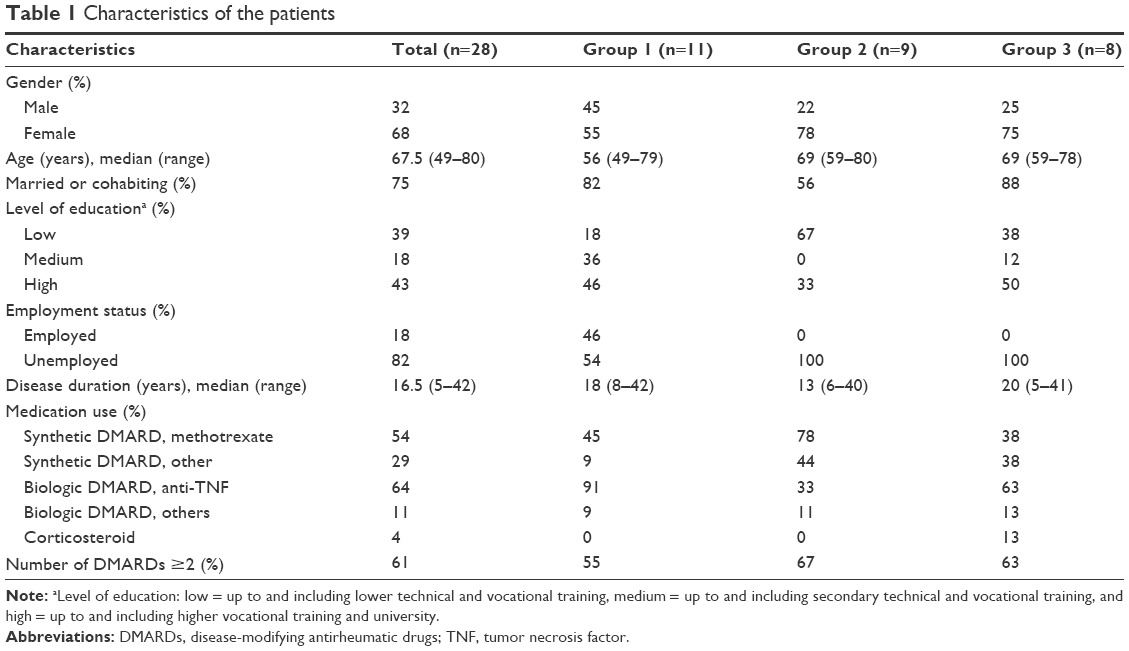 | Table 1 Characteristics of the patients |
The results were described in two separate parts. The following three overarching themes were identified in relation to support needs for medication use (objective 1): 1) informational support; 2) practical support; and 3) emotional support. The following three overarching themes were identified in relation to the suitability of eHealth technologies (objective 2): 1) previous experiences; 2) perceived advantages and disadvantages; and 3) preconditions for use.
Part 1: support needs for medication use
Informational support
Informational support reflected the provision of information and facts, including advice, suggestions, and feedback from health care providers. This overarching theme comprised two interrelated subthemes: unambiguous, high-quality information and more information.
Unambiguous, high-quality information
The patients highly valued being provided with information about their medication. For most patients, this was the first thing they mentioned during the focus groups. They sought information from a variety of sources, both written and oral. Although general, written information was considered valuable, the patients preferred health care providers who provided them oral information directly, tailored to their personal situation.
That they (healthcare providers) really give you the information they know. And that they also give you tips on what you have to watch out for. [Female, 49 years]
Some patients mentioned that, when seeking information, they encountered conflicting information between different information sources.
They say: ‘You always have to ask everything here (in the hospital).’ That’s what I do, but sometimes you also search for information yourself. Then you do sometimes see that there’s a difference in side effects, the way you have to administer it … So, it’s different to the information leaflets or what you read in the brochures. [Female, 49 years]
This resulted in ambiguity and uncertainty. In such cases, the patients preferred contacting their health care providers directly. Health care providers could best deal with these uncertainties by giving advice, suggestions, and feedback.
That’s what’s good about my rheumatologist. He says: ‘Get in touch … what are we going to do …’ […] And having that discussion is great. That you just get confirmation. [Female, 68 years]
However, some patients also mentioned that they received conflicting information from different health care providers. It was stated that health care providers, especially the ones not specialized in rheumatology, needed to be better able to provide unambiguous, high-quality information about the patients’ medication.
More information
Most patients expressed a need to receive more information than currently provided, in particular about side effects, drug–drug interactions, and long-term consequences of medication use. Some patients mentioned that they had difficulties in distinguishing between the side effects and symptoms caused by RA.
Sometimes you don’t properly know if it’s because of the medication, or if you are having a flare. […] So, what’s the cause? [Female, 58 years]
Consequently, they were unsure when it would be appropriate to seek medical advice.
Yes, because then I think: Okay, am I going too quickly? Because, maybe, tomorrow will be fine. [Female, 49 years]
The patients said that receiving more information about side effects and drug–drug interactions, no matter how rare, could help them to feel more in control and seek medical advice when appropriate. Concerning long-term consequences of medication use, there was a need for more information about bDMARDs. This was attributed to the fact that bDMARDs have been in clinical use for a relatively short time. Thus, long-term data on safety are still lacking and this can evoke concerns in some patients.
Research is still ongoing of course, to the side effects of biologicals. And of course that takes time, because these things haven’t been around very long … So I think that’s important. Which doesn’t mean that I won’t use them anymore once I know the results. Without those things I just can’t function. I can understand that. But I still think it’s important, as there are a lot of side effects that people don’t know about at all. It makes you think: Hey, can it have that effect on me as well? [Female, 59 years]
Practical support
Practical support included the reinforcement of practical skills as well as the provision of medication aids and pharmacy services. Three subthemes within this overarching theme were as follows: help with practical problems, monitoring of self-administration, and goods and services.
Help with practical problems
Some patients mentioned that they experienced practical problems. First, they struggled to remove the tablets or capsules from the pharmacy blister packs.
Those packages … I just don’t understand it. They’re developed for patients with arthritis. And they’re shut so tightly, we just can’t get them open. Really great. […] It’s just a way of keeping us busy. [Female, 61 years]
To overcome this problem, some patients used scissors. However, they preferred the pharmacy assistant to remove the tablets or capsules from the packs and put them in a container. The self-administration of subcutaneous injections could also cause problems. One patient said that unscrewing the syringe caps and pressing the syringes was difficult for her because she lacked strength in her hands.
I also have a prosthesis here, which makes it a little difficult to inject. Then you have to … The strength to, to unscrew the syringe caps … especially in the beginning they were screwed too tight. They could hardly be unscrewed. So that was a problem. [Female, 69 years]
Furthermore, most patients who self-administered their medication via subcutaneous injections suffered from side effects at the injection site, such as pain, rash, redness, bruises, and swelling. Although the patients usually learned by experience how to alleviate the side effects, they would prefer to be provided with more tips and tricks on how to deal with these side effects.
Well, of course I was given information on how to self-administer the injections. It’s just that loads of things weren’t said at the time. [Female, 79 years]
Monitoring of self-administration
Also, there was a need for regular monitoring of the self-administration process. The patients would feel more confident if they knew that they were still doing it correctly.
Goods and services
The provision of medication aids, such as dispensers, tablet splitters, sharp containers, cooler bags, and reminders, was highly valued by the patients. Nevertheless, some patients said that the storage and transport of their medication was problematic, especially under circumstances such as going on holiday.
As I am going on a holiday … And then it is quite a fuss to take it (the medication) with me on the airplane. That cooler bag takes up space, and if you’re only allowed to take your cabin baggage, that means a lot of inching and pinching. [Male, 70 years]
In general, the patients felt that the pharmacy sufficiently supported them regarding medication use. Services they appreciated were, for example, the offering of help, the alerts when their medication was running out, and the home delivery of medication on a date and time of their choosing.
Emotional support
Emotional support reflected a trusted patient–health care provider relationship, characterized by good communication. This overarching theme comprised the following three interrelated subthemes: openness, active listening, and collaboration.
Openness
A trusted patient–health care provider relationship, characterized by good communication, was important to the patients. They expressed a need to feel at ease to communicate openly. One patient mentioned that she highly valued the openness she had with her rheumatologist.
For 25 years, I had such a nice rheumatologist. I could say everything to him. And he said everything to me. [Female, 67 years]
Active listening
Another important part of good communication was active listening. The patients mentioned that health care providers could pay more attention to, for example, their concerns regarding side effects. They could do this by taking enough time to listen and respond to the patients. According to some patients’ experience, health care providers do not always take enough time to do this.
Then some woman asks you questions about your wellbeing. The rheumatologist doesn’t have time for that anymore. [Female, 79 years]
Above all, the patients wanted health care providers to take them seriously.
I think that’s the very worst … In the pharmacy … They act as if I’m stupid. When I say it (the medication) doesn’t work, they say: ‘That’s not true.’ […] You’re called a liar! [Female, 61 years]
Collaboration
Most patients preferred to use as little medication as possible. They valued tapering of their medication and adjusting doses in consultation with the rheumatologist. Some patients had a need for a flexible medication regimen that allowed them to self-adjust doses.
I also tried it every other week, but then I got the flu. She (the rheumatologist) said: ‘Just start taking it once a week and then extend it again.’ I think that’s really good, that I can just try things out for myself. That’s really important for me. [Female, 55 years]
Having control over their medication use could help the patients to fit this activity into their daily lives in the best possible way. However, close collaboration with the rheumatologist was considered important in this.
I can easily contact my rheumatologist. That works for me. Then we can have a discussion about what to do. [Female, 55 years].
Correspondingly, the patients preferred it when health care providers involved them in decision-making about their treatment. The extent to which they preferred to be involved differed for each individual.
Part 2: the suitability of eHealth technologies
Previous experiences
Only a few patients were familiar with the term eHealth. After explaining the WHO’s definition of the term, it turned out that almost all patients had used some form of an eHealth technology at least once. In particular, the patients had frequently searched the Internet to obtain information about their medication.
I use Google. Every now and then I look it up. If I get anything new, like: What is it? And what are the side effects? [Female, 59 years]
They also made use of eHealth technologies by ordering medication online, consulting health care providers by email, and connecting with other patients via online communities. These forms were, however, used infrequently and only by a few patients.
Perceived advantages and disadvantages
Most patients believed that they could benefit from eHealth in some way. They thought that it could complement current practices. However, the awareness of its advantages was low. The patients mentioned that eHealth technologies could have the advantages of being less time-consuming, as compared to hospital visits, and easily accessible.
It would be easy for once. That you can just send a quick email with your question and have an answer the next morning. […] Well, yes, then you don’t need to go for check-ups anymore. [Male, 77 years]
The patients had several concerns regarding eHealth technologies. Some patients were concerned that eHealth technologies would contribute to impersonal care by replacing face-to-face interactions with health care providers. Traditional, real-life visits were still preferred by most patients, and they emphasized that these should never be replaced by eHealth technologies.
That’s the danger. You do need to keep your eye on it and make sure that there’s still personal contact. [Female, 49 years]
One patient also mentioned that it would be difficult for him to express himself by typing instead of speaking when using an eHealth technology such as email consultation. Other patients added that in particular patients belonging to the “older generation” could experience difficulties with this form of communication as they are just not used to it.
No, there’s nothing better than having someone on the other side of the desk who you can just ask questions. Because otherwise we’re just one tiny step away from you being the robot and I being the patient. […] No, as far as I’m concerned, it shouldn’t have to go that far. [Female, 64 years]
Also, the patients expressed concerns about matters such as privacy and data security. This was partially based on noted media reports about data leakage.
We’re actually already being spied on by everyone, because if you’ve got a phone like this (smartphone), then it’s not a secret for anyone. You don’t have any privacy then. [Female, 61 years]
The quality and reliability of information they obtained from the Internet was also a point of concern for the patients. This was especially the case when the source of this online information was unclear, and commercial interests may possibly be involved.
Preconditions for use
The patients mentioned several preconditions for the use of eHealth technologies. These preconditions were mostly related to the previously described concerns. Some patients said that they were not interested in using eHealth technologies at all. A reason for their lack of interest was that they considered themselves unable to use modern, electronic technologies such as computers, smartphones, and the Internet. They also believed that they were already provided with sufficient support regarding medication use, making it of little interest to use eHealth technologies. However, they were concerned that, due to the rapid development of modern, electronic technologies, they would be forced to use them. It was stated that eHealth technologies should never be mandatory and that patients should always have the choice whether to use them or not.
It’s making it mandatory. People just don’t want that. [Female, 59 years]
The ease of use was mentioned as an important precondition. According to one patient, using an eHealth technology should require as few actions as possible.
Well, if I talk and that thing just works, yes. No. But if I just speak and I say: ‘Start up, do this, do that …’ [Female, 61 years]
Assuring privacy and data security were also mentioned here. Furthermore, when it comes to online information, the patients found it important that they could obtain information about their medication from trusted sources.
I can imagine if this (information about medication on the Internet) all falls under the responsibility of the hospital … And I know, if I’m logged in and search for something, that all the information I get is reliable … [Female, 56 years]
Discussion
This is the first study to document the needs of patients with RA regarding support for medication use from their own perspective. The provision of unambiguous, high-quality information was the most important need expressed by the patients. They preferred receiving oral information, tailored to their personal situation, directly from health care providers. Besides informational support needs, a variety of practical (eg, the provision of medication aids and pharmacy services) and emotional (eg, a trusted patient–health care provider relationship) support needs were identified. The identification of the themes – informational, practical, and emotional support – corresponds to the three types of support distinguished by Schaefer et al.29 The distinction of these support types is widely used in research on social support. The findings of this study suggest that, next to friends and family members, health care providers could also provide these types of support. This is supported by the studies of Garwick et al,30 Warwick et al,31 and Masters et al.32 These researchers also identified health care providers as a source of informational as well as practical and social support. Although potential advantages of eHealth technologies to address the patients’ support needs were recognized, concerns over matters such as personal interaction with health care providers, privacy and data security, and the quality and reliability of online information were prevalent.
We found that, above all, the patients had a need for unambiguous, high-quality information about their medication. They sought information from a variety of sources and mentioned that they encountered conflicting information between different sources, including health care providers. Conflicting information is a point of concern because it is associated with nonadherence and medication-related anxiety.33–35 As the amount of information available to patients increases, especially as a result of more and more health-related websites, this problem has increased. Moreover, research has shown that online information targeted at patients with RA varies widely in terms of its quality.36,37 Therefore, it may be desirable for health care providers to direct patients with RA to carefully screened websites with high-quality information as a part of routine patient education and counseling. Furthermore, to ensure better alignment, health care providers may want to consider who provides what information.
This study showed that the need for informational support is constant and variable. The patients did not only have a need for information at the start of their medication but during the entire duration of usage, as concerns emerged. Thus, needs varied over time. Regular monitoring of a patient’s informational support requirements is therefore warranted.38 Most patients expressed a need for more information about their medication than is currently provided. Detailed information about side effects, drug–drug interactions, and long-term consequences of medication use was preferred. However, another important finding of this study was that each patient needed a different amount of information. Previous studies of patients with RA have documented an association between the need for more information and being a woman, being younger, and having a longer disease duration.39–43 Regarding medication use, only one study has shown that, in men, using more DMARDs and suffering from side effects are associated with a need for more information.42 This supports the notion that the provision of information should be tailored to an individual’s personal situation.38
The patients preferred increased support regarding the self-administration of subcutaneous injections and regular monitoring of this process. Patients are provided with information leaflets and step-by-step guides to correctly self-administer subcutaneous injections. In our hospital, they are also trained by the rheumatology nurse or the pharmacy assistant in self-administering their medication via subcutaneous injections until competency is achieved. However, we found that in time, patients may become uncertain about their competency. Creating an opportunity for patients to refresh their knowledge and practical skills once in a while may be desirable in order for them to self-administer subcutaneous injections with confidence.
The patients valued a trusted patient–health care provider relationship. Above all, they wanted to be taken seriously. Research has shown that, for the development of trust, the patients’ feeling of being taken seriously is a prerequisite.44–46 Moreover, good communication between patients and health care providers may bring numerous benefits, including better adherence rates.47–49 A meta-analysis has shown that good communication is highly correlated with better adherence rates. There is a 19% higher risk of nonadherence among patients whose health care providers communicate poorly.47 Therefore, a trusted patient–health care provider relationship, characterized by good communication, is pivotal in pursing adherence. This makes it worthwhile for health care providers to keep investing in the development of good communication skills.
Potential advantages of eHealth technologies to address the patients’ support needs for medication use were recognized. Although most patients believed that they could benefit from eHealth in some way, they still had concerns. This finding is in line with previous studies that described chronic disease patients’ concerns regarding a changing patient–health care provider relationship, involving less personal interaction.50,51 It suggests that the use of eHealth technologies has to complement current practices rather than replacing them. One possible solution is provided by a blended care model, in which a combination of face-to-face interactions between patients and health care providers are coupled with information provided by the way of eHealth technologies. There already has been some experience with this new form of health care in other chronic diseases.52–54 Although it is seen as a promising strategy, the actual use of blended care in practice is disappointing. Moreover, evidence regarding its feasibility and acceptability in the treatment of RA is lacking. Given this information, we suggest that future research should explore the possibilities of blended care in the treatment of RA.
Other concerns over matters such as privacy and data security and the quality and reliability of online information are also described in the literature.50,51,55,56 In order to improve the adoption of eHealth technologies by patients with RA, addressing their concerns should be a priority. This may be accomplished by providing them with detailed information regarding their points of concern. Also, it has to make sure that all preconditions for use are met.
The biggest strength of this study is that it shed light on the point of view of patients themselves. Their perspective still remains too much in the background in contemporary research. No other studies have explored the needs of patients with RA regarding support for medication use from their own perspective. Therefore, this study contributes to filling to the aforementioned gap of knowledge. Another strength is the involvement of two patient research partners. Their additional insights gave, among others, credibility to the findings. The methods used during the data analysis, such as investigating the occurrence of data saturation, analyzing the data independently by two researchers (ie, researcher triangulation), and conducting a member check, are also considered strengths as they enhanced this study’s quality. However, some limitations also need to be addressed. Two hundred and fifty patients were invited to participate in the focus groups, but 222 (89%) patients did not respond to the invitation. The reasons for not responding are unknown. As focus groups are usually made up of a very small number of patients who voluntarily participate, it cannot be assumed that the patients who participated in the focus groups are representative of a random sample of the total patient population. Moreover, mostly older patients with a longer disease duration participated. The fact that the findings are limited to patients with these characteristics cannot be ignored. It should be noted that the interest in eHealth technologies varies with age.57 The lack of the perspective of younger patients may therefore have implications for the findings.
Conclusion
We found that patients with RA have informational, practical, and emotional support needs for medication use. Informational support seems to be most important. From the patients’ perspective, eHealth technologies may have the potential to address these needs. However, these technologies are regarded as a complement to, rather than a replacement of, current practices.
Acknowledgments
We thank the moderators, Annette Heijnen (AH) and Maaike Abrahamse (MA), and an assistant moderator, Ellen Selten (ES), for their great work facilitating the focus groups. Also, we thank Herman van Duijn (HvD) and Peter van Grinsven (PvG) for fulfilling a consulting and advising role as patient research partners. This study received no specific grant from any funding agency in the public, commercial, or nonprofit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376(9746):1094–1108. | ||
Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis. Eur J Radiol. 1998;27(Suppl 1):S18–S24. | ||
Young A, Koduri G. Extra-articular manifestations and complications of rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2007;21(5):907–927. | ||
Smolen JS, Landewe R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2013 update. Ann Rheum Dis. 2014;73(3):492–509. | ||
Singh JA, Saag KG, Bridges SL Jr, et al. 2015 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2016;68(1):1–26. | ||
Ramiro S, Gaujoux-Viala C, Nam JL, et al. Safety of synthetic and biological DMARDs: a systematic literature review informing the 2013 update of the EULAR recommendations for management of rheumatoid arthritis. Ann Rheum Dis. 2014;73(3):529–535. | ||
Singh JA, Cameron DR. Summary of AHRQ’s comparative effectiveness review of drug therapy for rheumatoid arthritis (RA) in adults – an update. J Manag Care Pharm. 2012;18(4 Suppl C):S1–S18. | ||
Waimann CA, Marengo MF, De Achaval S, et al. Electronic monitoring of oral therapies in ethnically diverse and economically disadvantaged patients with rheumatoid arthritis: consequences of low adherence. Arthritis Rheum. 2013;65(6):1421–1429. | ||
Pasma A, Schenk CV, Timman R, et al. Non-adherence to disease-modifying antirheumatic drugs is associated with higher disease activity in early arthritis patients in the first year of the disease. Arthritis Res Ther. 2015;17:281. | ||
Barton JL, Schmajuk G, Trupin L, et al. Poor knowledge of methotrexate associated with older age and limited English-language proficiency in a diverse rheumatoid arthritis cohort. Arthritis Res Ther. 2013;15(5):R157. | ||
Neame R, Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology (Oxford). 2005;44(6):762–767. | ||
Sormunen E, Nevala N, Sipilä S. Critical factors in opening pharmaceutical packages: a usability study among healthcare workers, women with rheumatoid arthritis and elderly women. Packag Technol Sci. 2014;27(7):559–576. | ||
Van den Bemt BJ, Zwikker HE, Van den Ende CH. Medication adherence in patients with rheumatoid arthritis: a critical appraisal of the existing literature. Expert Rev Clin Immunol. 2012;8(4):337–351. | ||
Morgan C, McBeth J, Cordingley L, et al. The influence of behavioural and psychological factors on medication adherence over time in rheumatoid arthritis patients: a study in the biologics era. Rheumatology (Oxford). 2017;54(10):1780–1791. | ||
Ndosi M, Adebajo A. Patient education in rheumatoid arthritis: is the needs-based approach the way forward? Clin Rheumatol. 2015;34(11):1827–1829. | ||
Wright J, Williams R, Wilkinson JR. Development and importance of health needs assessment. BMJ. 1998;316(7140):1310–1313. | ||
Epstein RM, Street RL Jr. The values and value of patient-centered care. Ann Fam Med. 2011;9(2):100–103. | ||
Bukhari M, Bamji AN, Deighton C. Is it ever appropriate to discharge patients with rheumatoid arthritis? Rheumatology (Oxford). 2007;46(11):1631–1633. | ||
World Health Organization. eHealth. 2017. Available from: http://www.who.int/ehealth/en/. Accessed April 6, 2017. | ||
Keselman A, Logan R, Smith CA, Leroy G, Zeng-Treitler Q. Developing informatics tools and strategies for consumer-centered health communication. J Am Med Inform Assoc. 2008;15(4):473–483. | ||
Coenen M, Stamm TA, Stucki G, Cieza A. Individual interviews and focus groups in patients with rheumatoid arthritis: a comparison of two qualitative methods. Qual Life Res. 2012;21(2):359–370. | ||
Kitzinger J. Qualitative research. Introducing focus groups. BMJ. 1995;311(7000):299–302. | ||
Law AV, Ray MD, Knapp KK, Balesh JK. Unmet needs in the medication use process: perceptions of physicians, pharmacists, and patients. J Am Pharm Assoc. 2003;43(3):394–402. | ||
Gordon K, Smith F, Dhillon S. Effective chronic disease management: patients’ perspectives on medication-related problems. Patient Educ Couns. 2007;65(3):407–415. | ||
Ryan R, Santesso N, Lowe D, et al. Interventions to improve safe and effectivemedicines use by consumers: an overview of systematic reviews. Cochrane Database Syst Rev. 2014;4:1–72. | ||
Krueger RA. Developing Questions for Focus Groups. Thousand Oaks: SAGE; 1998. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
Boeije H. Analysis in Qualitative Research. Thousand Oaks: SAGE; 2007. | ||
Schaefer C, Coyne JC, Lazarus RS. The health-related functions of social support. J Behav Med. 1981;4(4):381–406. | ||
Garwick AW, Patterson JM, Bennett FC, Blum RW. Parents’ perceptions of helpful vs unhelpful types of support in managing the care of preadolescents with chronic conditions. Arch Pediatr Adolesc Med. 1998;152(7):665–671. | ||
Warwick R, Joseph S, Cordle C, Ashworth P. Social support for women with chronic pelvic pain: what is helpful from whom? Psychol Health. 2004;19(1):117–134. | ||
Masters KS, Stillman AM, Spielmans GI. Specificity of social support for back pain patients: do patients care who provides what? J Behav Med. 2007;30(1):11–19. | ||
Carpenter DM, DeVellis RF, Fisher EB, DeVellis BM, Hogan SL, Jordan JM. The effect of conflicting medication information and physician support on medication adherence for chronically ill patients. Patient Educ Couns. 2010;81(2):169–176. | ||
Carpenter DM, Elstad EA, Blalock SJ, DeVellis RF. Conflicting medication information: prevalence, sources, and relationship to medication adherence. J Health Commun. 2014;19(1):67–81. | ||
Hameen-Anttila K, Nordeng H, Kokki E, et al. Multiple information sources and consequences of conflicting information about medicine use during pregnancy: a multinational Internet-based survey. J Med Internet Res. 2014;16(2):e60. | ||
Ansani NT, Vogt M, Henderson BA, et al. Quality of arthritis information on the Internet. Am J Health Syst Pharm. 2005;62(11):1184–1189. | ||
Culver M, Chadwick A. Internet information on rheumatoid arthritis: an evaluation. Musculoskeletal Care. 2005;3(1):33–43. | ||
Zangi HA, Ndosi M, Adams J, et al. EULAR recommendations for patient education for people with inflammatory arthritis. Ann Rheum Dis. 2015;74(6):954–962. | ||
Meesters J, de Boer I, van den Berg M, Fiocco M, Vliet VT. Unmet information needs about the delivery of rheumatology health care services: a survey among patients with rheumatoid arthritis. Patient Educ Couns. 2011;85(2):299–303. | ||
Fraenkel L, Bogardus S, Concato J, Felson D. Preference for disclosure of information among patients with rheumatoid arthritis. Arthritis Rheum. 2001;45(2):136–139. | ||
Gordon MM, Capell HA, Madhok R. The use of the Internet as a resource for health information among patients attending a rheumatology clinic. Rheumatology (Oxford). 2002;41(12):1402–1405. | ||
Neame R, Hammond A, Deighton C. Need for information and for involvement in decision making among patients with rheumatoid arthritis: a questionnaire survey. Arthritis Rheum. 2005;53(2):249–255. | ||
Meesters JJ, Vliet Vlieland TP, Hill J, Ndosi ME. Measuring educational needs among patients with rheumatoid arthritis using the Dutch version of the Educational Needs Assessment Tool (DENAT). Clin Rheumatol. 2009;28(9):1073–1077. | ||
Calnan MW, Sanford E. Public trust in health care: the system or the doctor? Qual Saf Health Care. 2004;13(2):92–97. | ||
Hallowell N. Encounters with medical professionals: a crisis of trust or matter of respect? Med Health Care Philos. 2008;11(4):427–437. | ||
Croker JE, Swancutt DR, Roberts MJ, Abel GA, Roland M, Campbell JL. Factors affecting patients’ trust and confidence in GPs: evidence from the English national GP patient survey. BMJ Open. 2013;3(5):e002762. | ||
Zolnierek KB, Dimatteo MR. Physician communication and patient adherence to treatment: a meta-analysis. Med Care. 2009;47(8):826–834. | ||
Salt E, Frazier SK. Adherence to disease-modifying antirheumatic drugs in patients with rheumatoid arthritis: a narrative review of the literature. Orthop Nurs. 2010;29(4):260–275. | ||
Polinski JM, Kesselheim AS, Frolkis JP, Wescott P, Allen-Coleman C, Fischer MA. A matter of trust: patient barriers to primary medication adherence. Health Educ Res. 2014;29(5):755–763. | ||
Steele GC, Miller D, Kuluski K, Cott C. Tying eHealth tools to patient needs: exploring the use of eHealth for community-dwelling patients with complex chronic disease and disability. JMIR Res Protoc. 2014;3(4):e67. | ||
Currie M, Philip LJ, Roberts A. Attitudes towards the use and acceptance of eHealth technologies: a case study of older adults living with chronic pain and implications for rural healthcare. BMC Health Serv Res. 2015;15:162. | ||
Tabak M, Brusse-Keizer M, Van der Valk P, Hermens H, Vollenbroek-Hutten M. A telehealth program for self-management of COPD exacerbations and promotion of an active lifestyle: a pilot randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2014;9:935–944. | ||
Bossen D, Kloek C, Snippe HW, Dekker J, De Bakker D, Veenhof C. A blended intervention for patients with knee and hip osteoarthritis in the physical therapy practice: development and a pilot Study. JMIR Res Protoc. 2016;5(1):e32. | ||
Wentzel J, Van der Vaart R, Bohlmeijer ET, Van Gemert-Pijnen JE. Mixing online and face-to-face therapy: how to benefit from blended care in mental health care. JMIR Ment Health. 2016;3(1):e9. | ||
Simon SR, Evans JS, Benjamin A, Delano D, Bates DW. Patients’ attitudes toward electronic health information exchange: qualitative study. J Med Internet Res. 2009;11(3):e30. | ||
Silver MP. Patient perspectives on online health information and communication with doctors: a qualitative study of patients 50 years old and over. J Med Internet Res. 2015;17(1):e19. | ||
Spooner KK, Salemi JL, Salihu HM, Zoorob RJ. eHealth patient-provider communication in the United States: interest, inequalities, and predictors. J Am Med Inform Assoc. 2017;24(e1):e18–e27. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.