Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Supine Positioning in Primary Total Hip Replacement is Associated with a Shorter Hospital Stay Than Lateral Positioning: A Retrospective Propensity-Score Matched Cohort Study
Authors Tsai YF ![]() , Hsu CY
, Hsu CY ![]() , Hsu WT, Lai CW, Lee TY, Huang TW, Wu SC
, Hsu WT, Lai CW, Lee TY, Huang TW, Wu SC ![]()
Received 15 July 2025
Accepted for publication 7 November 2025
Published 13 November 2025 Volume 2025:21 Pages 1579—1591
DOI https://doi.org/10.2147/TCRM.S553963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Yung-Fong Tsai,1,2 Chih-Yi Hsu,3 Wei-Ti Hsu,4 Chiung-Wen Lai,5 Tsung-Yang Lee,5 Tsan-Wen Huang,6,* Shao-Chun Wu2,3,*
1Department of Anesthesiology, Chang Gung Memorial Hospital, Linkou Branch, Taoyuan, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan, Taiwan; 3Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 4Department of Anesthesiology, China Medical University Hospital, Taichung, Taiwan; 5Department of Anesthesiology, Jen-Ai Hospital, Taichung, Taiwan; 6Department of Orthopaedic Surgery, Jen-Ai Hospital, Taichung, Taiwan
*These authors contributed equally to this work: Shao-Chun Wu and Tsan-Wen Huang
Correspondence: Shao-Chun Wu, Department of Anesthesiology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan, Email [email protected] Tsan-Wen Huang, Department of Orthopaedic Surgery, Jen-Ai Hospital, Taichung, Taiwan, Email [email protected]
Background: There is still no definite answer regarding the most advantageous patient positioning during total hip replacement (THR). We compared whether patient position (lateral vs supine) incur a difference on hospital length of stay (LOS) after primary THR.
Methods: This retrospective cohort study included primary THR patients at a single tertiary center (2017– 2022). THR patients prepared in the lateral decubitus position were compared to those in the supine position. Propensity score matching at a 1:4 ratio was applied to minimize selection bias. Matching covariates included age, sex, body weight, comorbidities (hypertension, diabetes), anesthesia time, and intraoperative tranexamic acid use. After matching, 990 patients were analyzed (792 lateral; 198 supine).
Results: In supine group, the median LOS (5 days, IQR: 4– 6) was shorter than the lateral group (5 days, IQR: 5– 6; p< 0.001). More supine patients were discharged before day 5 (45.5% vs 22.7%, p< 0.001). Multivariate analysis revealed supine position as the strongest protective factor against long hospitalization (OR: 0.32, 95% CI: 0.23– 0.46, p< 0.001). Other notable predictors of long LOS included ASA ≥III (OR: 1.74), longer anaesthesia duration (OR: 1.78), and higher IV fluid administration (OR: 1.08). Patient positioning did not notably predict blood transfusion risk (OR: 1.32, p=0.144).
Conclusion: THR patients in supine positioning have a substantial reduction in hospital LOS compared to patients in lateral decubitus positioning, with supine position providing a 68% reduction in risk of long hospitalization. The two groups showed no difference in blood transfusion requirements.
Keywords: blood transfusion, hospital length of stay, lateral position, patient positioning, supine position, total hip replacement
Introduction
Total hip replacement (THR) is one of the most successful surgeries for treating end-stage hip osteoarthritis.1 Since last decade, enhanced perioperative protocols have dramatically reduced hospital length of stay (LOS) in patients receiving THR.2 Median LOS has decreased in contemporary fast-track programs.2 Reducing LOS is desirable for both patients and health systems because prolonged hospitalization can increase costs and risk of nosocomial complications.3,4 Conversely, extended inpatient stays may result in more 30-day readmission and early complications post-operation.5,6 Based on these implications, there is strong interest in identifying factors that influence LOS after THR.
The choice of patient positioning during total hip replacement surgery is typically between lateral decubitus and supine approaches, and they may substantially influence perioperative management and postoperative recovery. Lateral decubitus positioning is conventionally used for posterolateral and direct lateral approaches. Otherwise, supine positioning is commonly employed for the direct anterior approach and some anterolateral approaches. Surgeon preference for surgical approach is the major determinant of patient positioning. As highlighted in a recent systematic review and meta-analysis7 and supported by a randomized clinical trial,8 the choice of position may affect surgical exposure, soft tissue handling, and the use of intraoperative imaging as well as early mobilization. In our institution, more than 85% of lateral-positioned THRs used the posterolateral approach, and nearly all supine-positioned THRs were performed via anterior-based and muscle-sparing techniques. These patterns reflect standard surgical practice and explain the close linkage between surgical approach and intraoperative positioning. And thereby possibly influences pain, blood loss, and functional recovery.
However, it remains unclear which position takes a clear advantage of postoperative recovery acceleration and LOS shortening.7 Prior studies compared supine and lateral positions have mainly focused on surgical metrics rather than recovery milestones, including component alignment and blood loss. Recently, other’s study reported that no notable difference was found in overall clinical outcomes between two positions.7 Notably, that analysis reported that lateral position group slightly lower intraoperative blood loss and postoperative pain (VAS scores) than supine position group, and even the cup anteversion accuracy was marginally better. Previous randomized trials showed some divergent conclusions. Takada et al showed that the acetabular tilt was more accurately measured with the patient in the supine position than in the lateral position during THR using an anterolateral Watson-Jones approach.9 In contrast, the results of a study by Güler et al showed that the supine position was associated with poor intraoperative outcomes, including higher blood loss, especially in obese patients undergoing THR.7 Both positions generally provide acceptable surgical outcomes despite of these subtle differences.10 Thus, whether one position allows faster recovery and discharge remains an open question. Several studies have examined the influence of surgical approach on hospital stay after THR. The studies of Ang et al and Loh et al demonstrated that the direct anterior approach, typically performed in the supine position, was associated with a significantly shorter LOS compared with posterior or lateral approaches.11,12 In contrast, a recent systematic review by Papalia et al and a randomized clinical trial by Xiao et al reported no significant differences in LOS between supine and lateral positioning once approach-related factors were accounted for.7,8 These contrasting findings underscore the difficulty of disentangling the effect of positioning from that of surgical approach. To address this issue, our propensity-matched analysis was specifically designed to minimize patient- and surgery-related confounders in order to better isolate the independent impact of positioning on postoperative LOS.
Multiple variables may affect LOS such as patient health, perioperative care, and hospital discharge policies. Numerous cohort studies have identified patient-related predictors of prolonged LOS after joint replacement, and they were advanced age, higher comorbidity burden (eg American Society of Anesthesiologists (ASA) class ≥3), medical complications, and discharge disposition.2,4 Patient factors and surgical practice patterns usually result in variabilities in LOS. Surgical technique may be another factor. The direct anterior approach (typically done supine) has shown to lessen hospital stays 0.3–2 days than posterolateral approaches in some studies,11,12 though others found no LOS difference between anterior (often supine) and lateral/posterior approaches.7,8 Because supine positioning commonly accompanies anterior approaches while lateral positioning is used with lateral/posterior approaches, separating the effects of patient positioning from surgical technique on length of stay proves problematic. For example, take intraoperative fluoroscopy under supine positioning may enable improvement on component placement accuracy13 and potentially reduce early complications like dislocation. The lateral positioning, however, may provide easier access for certain surgeons, and possibly induce less muscle trauma in some approaches.
We therefore compared postoperative hospital stay between lateral and supine positioning for primary THR. Propensity score matching was used to balance important confounding variables including patient demographics and comorbidities. Supine positioning is commonly used a minimally invasive anterior or anterolateral approach. Our study hypothesizes that supine positioning promotes early mobilization and pain control, because it results in a shorter LOS compared to lateral positioning. Our study aims to identify independent predictors of long LOS in cohort population to clarify the impact of positioning relative to patient-related factors. The present study shows how the surgical approach decisions and perioperative protocols can impact patient safety and facilitate earlier discharge on best recovery after THR.
Materials and Methods
Study Design and Setting
This study was a retrospective cohort design, and ethical approval was obtained from the Institutional Review Board of Kaohsiung Chang Gung Memorial Hospital (approval number: 202500857B0), and was conducted in accordance with the Declaration of Helsinki. The protocol of present research complied with the STROBE guidelines and followed all pertinent ethical standards.14 Between January 2017 and December 2022, patients who received primary THR at our institution were recruited to the cohort. THR can be performed via different surgical approaches, and patient positioning usually is lateral or supine. All patients were under general anesthesia. After excluding patients with missing data (n = 25), 1551 patients were included in the study. The patients were categorized into two distinct groups: the first was prepared in lateral position (n = 1320) and the second was prepared in supine position (n = 231). A propensity score matching was set for preventing potential selection bias, and logistic regression was analyzed for each patient receiving total hip replacement (THR) in the supine versus lateral position. The relevant variables in model included clinically demographics and comorbidities such as age, sex, body weight, hypertension, diabetes mellitus, anesthesia duration, and intraoperative use of tranexamic acid. These variables were chosen based on clinical reasoning and prior evidence that they might influence both the choice of surgical approach/position and the outcome (LOS).2,4 Ultimately, a 1:4 propensity score-matched analysis was conducted on 990 patients (Figure 1). There were 792 patients allocated to lateral position group, and the other 198 patients were to the supine position group.
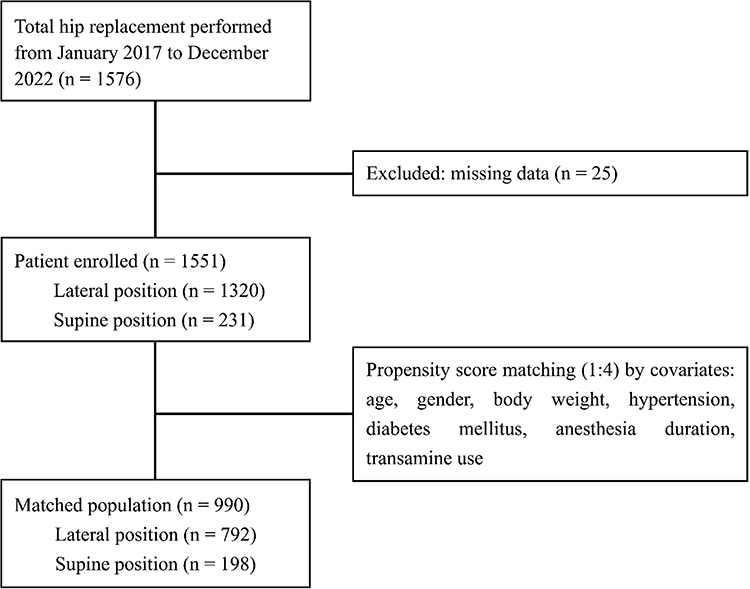 |
Figure 1 Flow diagram of study design and group allocation. Abbreviation: THR, total hip replacement. |
Patient Population
Adult patients (age ≥18) were eligible if they underwent elective primary THR for degenerative joint disease. The exclusion criteria were patients received THRs based on acute fracture, infection, or tumor, as well as revision surgeries. These scenarios often result in prolonged hospitalization in nature for reasons unrelated to patient positioning. Patients were also excluded from cohort if there was a lack of complete records of key variables (eg missing LOS or covariate data). Patients were divided into two groups based on intraoperative positioning. One is the lateral position group where patients are positioned on their side, typically used for posterolateral or direct lateral surgical approach. The other group was the supine position group where patients were positioned on their back, typically used for anterior or anterolateral approach. The assignment of positioning was determined by the operating surgeon’s standard practice and approach. Approximately 85% of the THR procedures were done via a posterolateral approach in lateral decubitus, and the remainder via an anterior-based muscle-sparing approach in supine position. No surgeons routinely performed THR using an anterior approach in the lateral position or posterior approach in the supine position, so patient position closely corresponded to the surgical approach.
Perioperative Care Pathway
All patients were managed in accordance with an institutional enhanced recovery protocol for total hip replacement (THR), and encompassed preoperative patient education, optimization of medical comorbidities, adherence to standardized general anesthesia procedures as well as application of multimodal analgesia (including regional nerve blocks or periarticular local infiltration). The protocol aimed to promote early mobilization on postoperative day 0 or 1 and provide implementation of standardized discharge criteria. Physical therapy was initiated the day after surgery. The preset discharge criteria included stable vital signs, adequate pain control on oral analgesics, ability to ambulate with an assistive device, and no unresolved medical issues.
Primary Outcomes and Predictor Variables
The primary outcome was LOS that was defined as the number of days from the day of surgery to the day of discharge. For reference, at our institution the day of surgery is counted as postoperative day 0; most elective THR patients are discharged on postoperative day 5 or 6 under our practice routine. We also defined long LOS as a stay not less than the mean of the cohort’s LOS distribution (which corresponded to ≥5 days in this study). This threshold represents a long hospitalization referenced by typical recovery. Our study applied logistic regression to evaluate predictors of long LOS (≥5 days, coded as 1; <5 days as 0) and need for blood transfusion (yes = 1; no = 0). Predictor variables are age, gender, body weight, ASA score, patient positioning, anesthesia duration, inhalational agent and dose, intraoperative intravenous (IV) fluid volume, estimated blood loss, urine output, hypertension (HTN), diabetes mellitus (DM), and use of tranexamic acid.
Statistical Analysis
We applied a 1:4 propensity score matching to minimize the bias resulting from baseline differences on outcome measures. The matching was based on a logistic regression model incorporated covariates such as age, sex, body mass, presence of HTN or DM, duration of anesthesia, and use of transamine acid. Following matching, 85.7% of the patients in the supine position group were retained and resulted in the allocation of 792 patients from the lateral position group. Categorical variables are included gender, ASA physical status, Apfel score, inhaled anesthetics, blood loss, comorbidities, and blood transfusion, and their data were presented as raw numbers or percentages and compared using Fisher’s exact or chi-square tests Depending on normality, continuous numeric data were analyzed by Student’s t-test or the Mann–Whitney U-test. Their data were presented as the median (interquartile range (IQR), 25–75%). The normality of the distribution was assessed by using Kolmogorov–Smirnov test. The impact of each variable on long LOS was evaluated via using univariate analysis and multiple logistic regression models, specifically binary logistic regression. We performed age-stratified analysis to evaluate the differential effects of patient positioning across age groups. Patients were categorized into two groups: younger cohort (<65 years) and elderly population (≥65 years). Violin plots were generated to visualize the distribution patterns of hospital LOS between supine and lateral positioning approaches within each age stratum. This visualization method was chosen to demonstrate both the density distribution and variability of LOS data, providing comprehensive insights into recovery patterns across different age groups. The violin plots display the full distribution of data points, median values, and quartile ranges, allowing for detailed comparison of positioning effects within each age category. Statistical analysis was done by SPSS® version 22.0 (IBM® Corp., Armonk, NY, USA). Statistical significance was established if p <0.05.
Results
Patient Characteristics
There were 1576 patients who underwent THR surgery included since January 1, 2017 to December 31, 2022. Twenty-five cases were excluded due to missing data, and 1551 patients remained (1320 in the lateral position, 231 in the supine position). After a propensity score matching, it resulted in an analyzed cohort of 990 patients (792 in the lateral position, 198 in the supine position) (Figure 1). Baseline demographic and clinical profiles of participants are outlined in Table 1. There were no statistically significant differences between the groups in terms of sex, age, body mass, ASA classification, Apfel score, anesthesia time, or the presence of comorbidities such as HTN and DM, as well as the incidence of perioperative blood transfusion (Table 1).
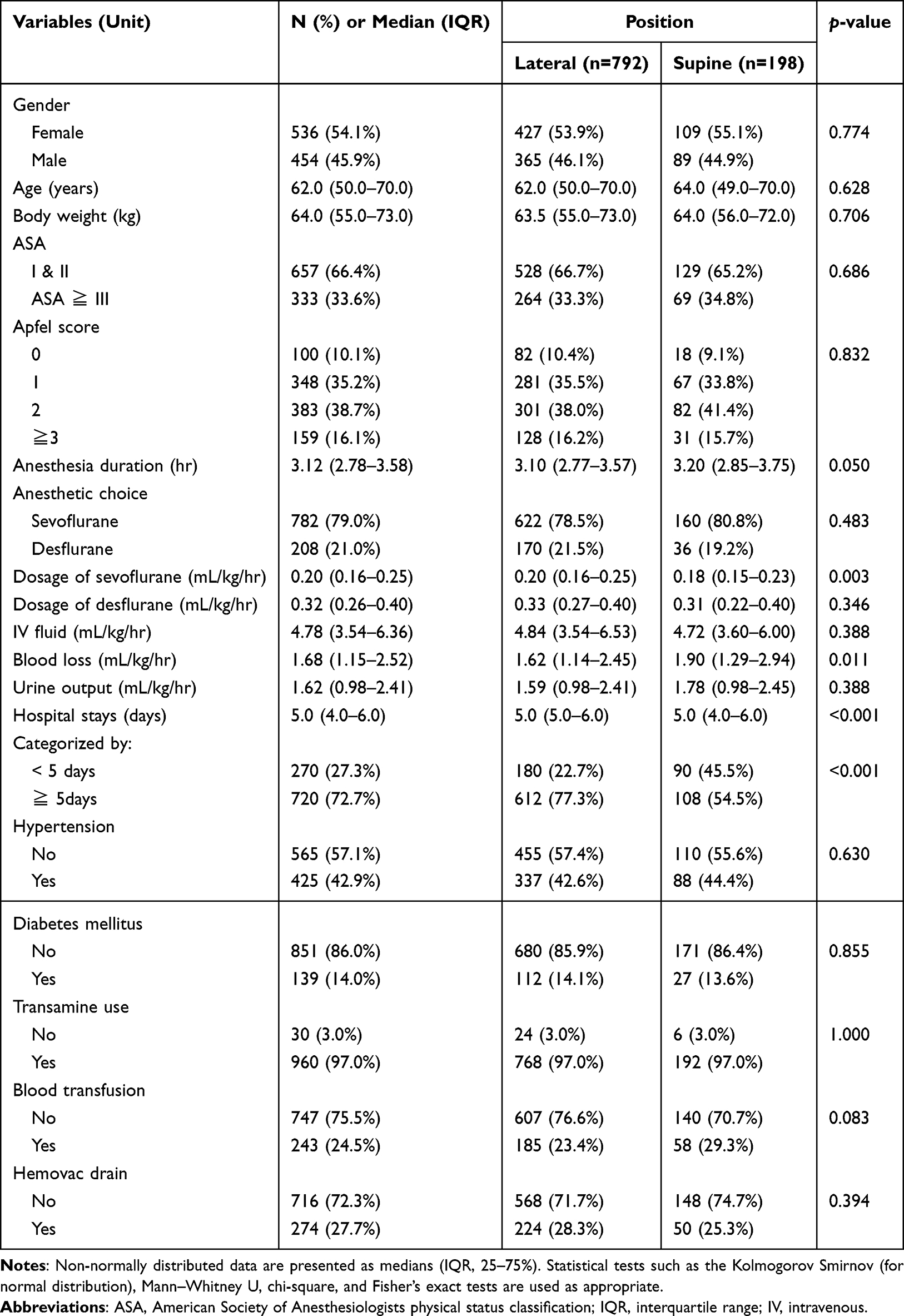 |
Table 1 Baseline Characteristics of Propensity Score-Matched THR Patients by Patient Position (n = 990) |
Regarding intraoperative variables, there were marked differences in the amount of sevoflurane used (p=0.003) and intraoperative blood loss (p=0.011). However, anesthesia duration (lateral: 3.10 hr vs supine: 3.20 hr, p=0.050), desflurane dosage (p=0.346), volume of transfused IV fluid (p=0.388), and urine output (p=0.388) did not differ substantially.
LOS Outcomes
A marked difference between the two groups was observed in the length of hospital stay (p<0.001). Although the median length of hospital stay was 5.0 days in both groups, their IQRs were different as 5.0–6.0 days for the lateral group and 4.0–6.0 days for the supine group (Table 1). When subgroup stratified by LOS, more patients in supine group experienced a hospital stay of fewer than 5 days (45.5%) than lateral group (22.7%) with a statistical significance (p<0.001). Conversely, patients in the lateral group had a higher percentage (77.3%) of hospital stay of 5 days or more compared to the supine group (54.5%). No significant difference was noted in the rates of blood transfusion (p=0.083) or Hemovac drain use (p=0.394).
Predictors of Long LOS
Several important predictors were associated with long hospital stay by multivariate logistic regression analysis (n=990) (Table 2). Supine positioning emerged as the strongest protective factor against long hospitalization, with an odds ratio [OR] of 0.32 (95% confidence interval [CI] at 0.23–0.46, p<0.001), representing a 68% reduction in the risk of extended hospital stays. This finding indicates that patients undergoing surgery in the supine position have notably lower odds of long LOS compared to those in lateral positions. Patients with ASA physical status III or higher exhibited substantially increased odds of long hospitalization (OR: 1.74) with 95% confidence interval (CI) at 1.22–2.48, p=0.002. The ASA classification is a well-established preoperative indicator for overall evaluating a patient’s health status and comorbidity burden. Patients with a higher ASA score represented reduced physiological reserve and a diminished ability to tolerate surgical stress that may contribute to long recovery times.
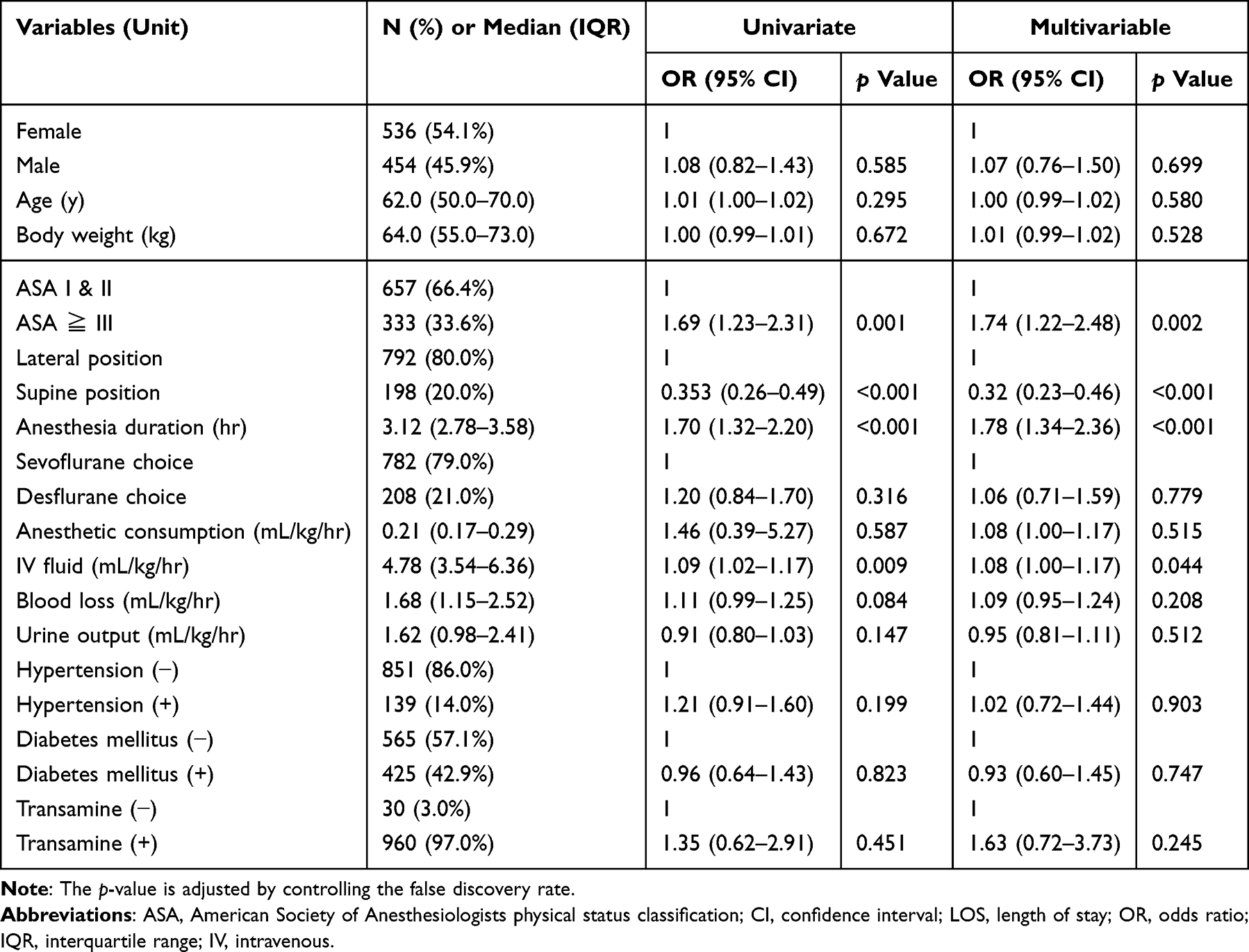 |
Table 2 Univariate and Multivariate Logistic Regression for Predictors of Long Hospital Stay (LOS ≧ 5 Days) (n = 990) |
Furthermore, longer anesthesia duration was a strong risk factor for long LOS (OR: 1.78, 95% CI: 1.34–2.36, p<0.001). Anesthesia duration often correlates with surgical complexity and invasiveness and indicates that more demanding procedures to lead to extended recovery. Higher infusion rate of intraoperative IV fluid also represented greater odds of long LOS (OR: 1.08, 95% CI: 1.00–1.17, p=0.044) (Table 2).
Age-Stratified Analysis of LOS by Positioning
Violin plot analysis of 990 patients revealed distinct distribution patterns of hospital LOS between positioning approaches across age stratifications (Figure 2). In the younger cohort (<65 years), both positioning groups exhibited similar median LOS values centered around 5 days. However, the supine position demonstrated broader distribution variability with increased spread in the lower quartiles, while lateral positioning showed more concentrated distribution around the median, suggesting greater consistency in discharge timing.
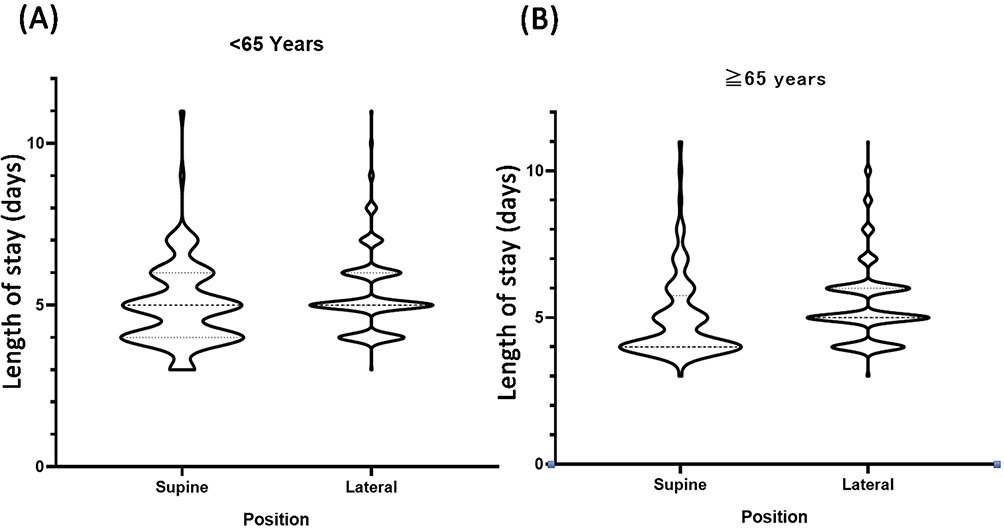 |
Figure 2 The effects of age-related LOS on surgical positions in THR patients. (A) Age <65 years old; (B) Age ≧65 years old. |
The elderly population (≥65 years) revealed more pronounced differences between positioning approaches. The supine group maintained a relatively narrow distribution concentrated around 4 days with minimal variance in the lower quartiles. Conversely, the lateral positioning group demonstrated a bimodal distribution pattern with density peaks at both 5 and 6 days, indicating greater heterogeneity in recovery trajectories. The lateral group also exhibited more extensive upper outliers, with some patients requiring stays exceeding 10 days.
Age-stratified analysis confirmed that the protective effect of supine positioning remained consistent across both age groups, though the magnitude of difference appeared more pronounced in the elderly population. In patients ≥65 years, 52.3% of supine-positioned patients were discharged before day 5 compared to only 19.8% in the lateral group (p<0.001). This difference was less pronounced but still significant in the younger cohort, with 41.2% vs 24.1% early discharge rates, respectively (p=0.032).
Predictors of Blood Transfusion Risk
The multivariate logistic regression analysis showed distinct yet overlapping factors for intraoperative blood transfusion risk (n=990) (Table 3). Notably, patient positioning (supine vs lateral) was not identified as an independent predictor of transfusion risk (OR: 1.32, 95% CI: 0.91–1.93, p=0.144). Patients with lower body weight increased the risk for blood transfusion (OR: 0.98, 95% CI: 0.96–1.00, p=0.008), indicating that smaller patients may have less physiological reserve or a lower blood volume, increasing their susceptibility to transfusion. Consistent with the LOS prediction, patients with higher ASA physical status represented a strong predictor of transfusion (OR: 2.37, 95% CI: 1.66–3.38, p<0.001). This reinforces the concept that patients are more susceptible to substantial blood loss in status of higher systemic disease burden.
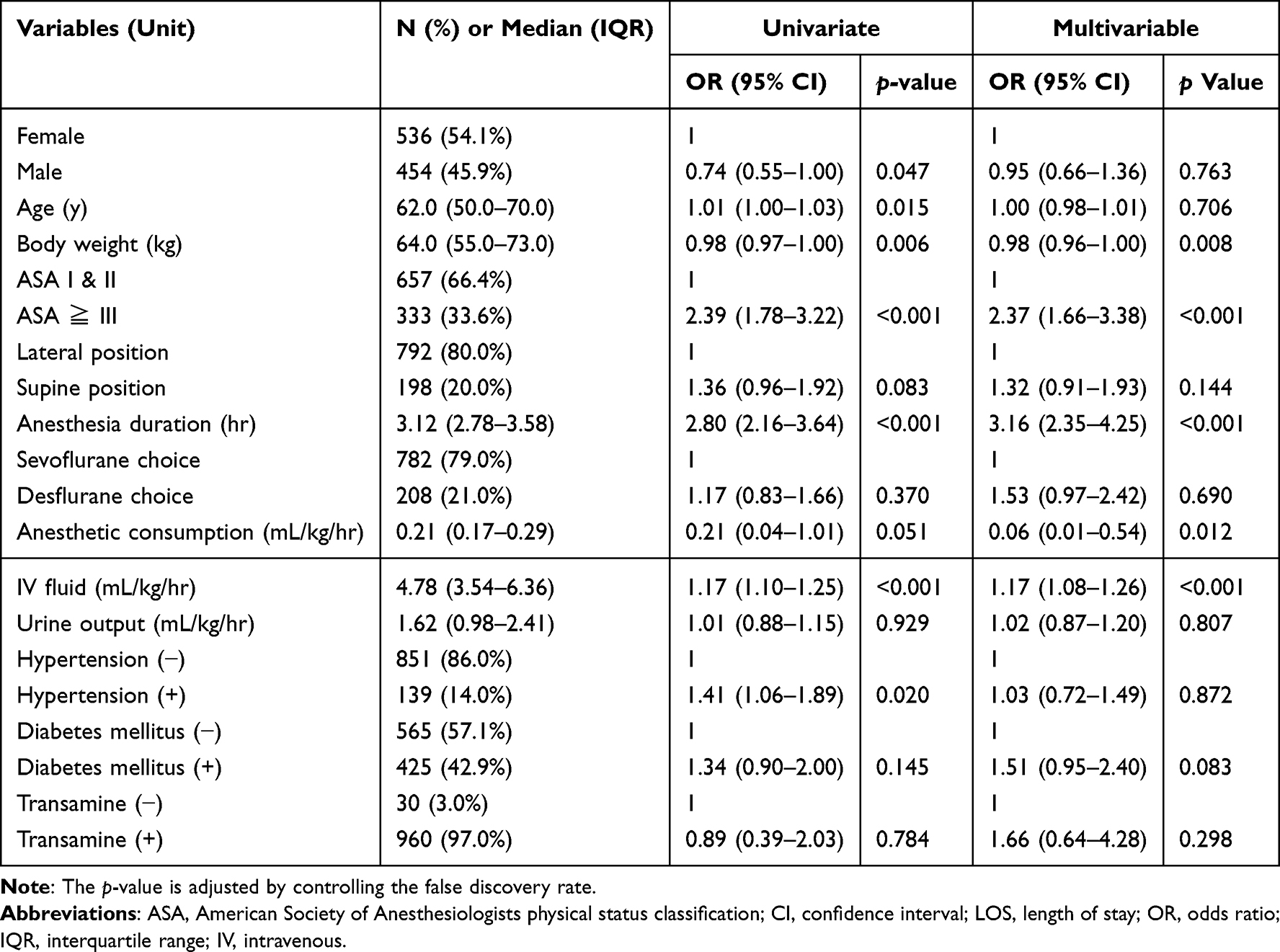 |
Table 3 Univariate and Multivariate Logistic Regression Analysis Assessing Risk for Blood Transfusion (n = 990) |
Anesthesia duration was a very strong predictor for intraoperative blood transfusion (OR: 3.16, 95% CI: 2.35–4.25, p<0.001). Complex or lengthy procedures carry a higher inherent risk of hemorrhage to incur longer anesthesia duration. Higher intraoperative IV fluid volume per kilogram per hour was also a strong predictor for transfusion risk (OR: 1.17, 95% CI: 1.08–1.26, p<0.001). This often reflects significant fluid shifts or ongoing blood loss. It could be served as a real-time indicator of hemodynamic instability. Interestingly, higher anesthetic consumption was unexpected to decrease the risk for transfusion (OR: 0.06, 95% CI: 0.01–0.54, p=0.012). This counter-intuitive finding warrants further investigation, as it may reflect specific anesthetic techniques or patient characteristics that influence both anesthetic requirements and blood loss (Table 3).
Discussion
The present study aimed to elucidate critical predictors of long LOS and the requirement for intraoperative blood transfusion following primary THR. Supine positioning was identified as the most significant independent predictor of shorter LOS, while it was not a significant predictor of transfusion risk in multivariate analyses in matched cohort of 990 patients. Both LOS and transfusion risk were closely related to several patient-specific and intraoperative factors. These findings offer valuable insights and greatly support the refinement of preoperative risk assessment. They also optimize perioperative management and enhancement of patient outcomes in THR.
Prior studies evaluating LOS after THR have employed a variety of methods. Randomized controlled trials compared different surgical approaches (eg, direct anterior approach vs posterior/lateral) and reported shorter LOS with anterior approaches, though these designs did not isolate positioning.11 Cohort studies with propensity matching (eg, Loh et al)12 similarly found shorter LOS for direct anterior approach versus posterior approaches. Meta-analyses and reviews focusing on positioning per se reported no consistent LOS differences once approach was controlled.7 More recently, Xiao et al8 conducted a randomized trial comparing direct anterior approach in supine versus lateral, and they showed no LOS difference. Based on these observations, we chose propensity score matching to minimize confounding and estimate the independent impact of positioning on LOS. Our findings are consistent with studies reporting shorter LOS with direct anterior approach (typically supine) versus posterior or lateral approaches.11,12 However, they also align with reviews and trials showing no LOS difference once surgical approach is accounted for.7,8 This underscores the challenge of disentangling positioning from approach. Compared with prior designs, our propensity score matching offers high clinical applicability by using large-scale real-world data to balance measurable confounders. While randomized controlled trials provide highest internal validity, propensity score matching is more pragmatic in routine surgical practice and supports the translation of evidence into perioperative management and discharge planning. Although propensity score matching reduces measured confounding, unmeasured factors such as surgeon-specific preferences or rehabilitation protocols may still influence LOS. Nonetheless, our approach complements RCT and meta-analytic evidence by specifically addressing positioning as the exposure of interest in a large-scale real-world cohort.
The ASA physical status classification is one of the powerful predictors for long LOS. If patients with an ASA physical status ≧ III, they faced a substantially increased likelihood of extended hospitalization, with an adjusted OR of 1.74 (95% CI: 1.22–2.48, p=0.002). Our data agree with previous findings and reveal that higher ASA scores indicate poorer systemic health. Higher-scored patients also incur worse postoperative outcomes and delayed recovery across surgeries.15,16 These patients have limited tolerance for surgical stress and complications may result in a longer recovery period.17 Most importantly, choice of supine position in THR was associated with the strongest protective effect against long LOS (OR: 0.32, 95% CI: 0.23–0.46, p<0.001), representing a 68% reduction in the risk of long hospitalization. Although propensity score matching accounted for multiple baseline characteristics, this finding demonstrates the substantial clinical benefit of supine positioning. Supine position is often favored for specific surgical approaches like direct anterior mansion and may be associated with inherently less invasive procedures or a patient cohort with fewer complexities. It is plausible that the supine position may be associated with inherently selection bias in nature not fully captured by the matched variables.18 This selection bias probably existed because surgeons might opt for supine positioning in patients perceived to be at lower risk for complications. Further prospective studies are warranted to clarify whether the supine position directly contributes to shorter hospital stays, or merely acts as a surrogate marker for other unmeasured factors influencing postoperative recovery.7
Moreover, anesthesia duration was a strong predictor of long LOS, and it demonstrated that with each additional hour of anesthesia time correlating with a 1.78-fold increased risk of long LOS (95% CI: 1.34–2.36, p<0.001). Previous surgical studies have well documented this association that a prolonged operative duration exposes patients to extended physiological stress that can hinder recovery and prolong hospitalization. These factors include risk of hypothermia, amplify inflammatory responses, and a higher likelihood of surgical site infections or other complications.1,19 Similarly, an increase in the odds for long LOS was observed in patients with higher IV infusion rate during THR (OR: 1.08, 95% CI: 1.00–1.17, p=0.044). It is important to infuse judicious fluid treatment for maintaining hemodynamic stability, but fluid overload or mismanagement can incur some adverse outcomes. These unwanted side effects include pulmonary congestion, tissue edema, and organ impairment—that may hinder postoperative recovery and prolong hospitalization.20,21 Gender, age, body weight, anesthetic type and use, blood loss, urine output, comorbidities (HTN/DM), and tranexamic acid were not independently associated with long LOS in our analysis. Our data also revealed that supine positioning is associated with a modestly shorter postoperative hospital stay in older THR patients interpretated by a violin plot (Figure 2). A substantially higher proportion of supine patients were discharged before postoperative day 5. This suggested that supine positioning may facilitate earlier recovery and discharge in elderly patients, and potentially enhanced perioperative efficiency and reduced hospital resource utilization. Age-stratified analysis revealed supine positioning benefits are particularly pronounced in elderly patients (≥65 years), demonstrating more predictable recovery patterns around 4 days versus bimodal distribution in lateral positioning.
It is a critical concern to transfuse blood component intraoperation due to its association with increased morbidity, mortality, and healthcare costs.22,23 Several major independent predictors for this outcome were analyzed in our study. Importantly, patient positioning (supine vs lateral) was not identified as an independent predictor of transfusion risk (OR: 1.32, 95% CI: 0.91–1.93, p=0.144), despite its substantial protective effect on LOS. Patients with lower body weight exerted a notably increased risk of requiring transfusion (OR: 0.98, 95% CI: 0.96–1.00, p=0.008). This finding presumed that individuals with smaller body mass may have a proportionally smaller circulating blood volume and thus more likely to meet transfusion triggers. They were rendered more vulnerable to the effects of surgical blood loss.24 Consistent with its role in predicting long LOS, an ASA physical status of III or higher was a substantial predictor for intraoperative blood transfusion, and it showed an increase of the risk by 2.37-fold (95% CI: 1.66–3.38, p<0.001). This evidence supports the finding that patients with substantial systemic disease burdens often have reduced physiological reserves, which limits their ability to compensate for blood loss and thereby increased their susceptibility to transfusion requirements.25,26 Anesthesia duration also emerged as a very strong predictor for intraoperative blood transfusion and showed increased the odds of transfusion per hour by a noTable 3.16-fold (95% CI: 2.35–4.25, p<0.001). This strong correlation demonstrates the inherent risk of hemorrhage associated with more complex or lengthy surgical procedures and emphasizes the importance of surgical efficiency and meticulous hemostasis.27,28 In addition, a higher rate of intraoperative IV fluid transfusion was strongly associated with an increased transfusion risk (OR: 1.17, 95% CI: 1.08–1.26, p<0.001). This relationship can be multifaceted. The increased fluid administration might be a direct response to ongoing blood loss and hemodynamic instability. It also could contribute to a dilutional coagulopathy to lower hemoglobin concentration and thereby triggers transfusion.29
Notably, a counterintuitive finding that higher anesthetic consumption demonstrated an inverse association with transfusion risk, and achieved statistical significance (OR: 0.06, 95% CI: 0.01–0.54, p=0.012). This unexpected inverse association warrants further investigation for validation. More anesthetic consumption potentially achieved deeper levels of anesthesia or the use of specific agents and thus may promote hemodynamic stability. It also suppresses sympathetic activation, optimize coagulation parameters, and collectively contributing to reduced blood loss.30 However, multivariate analysis of tranexamine use showed no significance on intraoperative blood transfusion risk. It raises contradiction to the well-established efficacy of tranexamic acid in reducing blood loss and transfusion requirements in THR.31–33 The extensive use of tranexamic acid in our cohort (97.0%) may have attenuated its detectability as an independent predictor in the multivariate model. As its broad application likely minimized inter-patient variability in bleeding risk and reduced statistical power to isolate its effect.34,35 Future research is recommended to explore the role of tranexamic acid for reducing transfusion rates in THR.36,37
However, there are some limitations in our study. First, the retrospective nature of this study may limit causal interpretation of the identified associations. Although propensity score matching was employed for analyzing observed confounders, the potential bias to confounding variables may be not entirely excluded. Second, as a single-center study, our data may not be easily generalizable to other institutions with different patient populations. And even surgical practices or anesthetic protocols may be limited. Third, the details of different surgical techniques within each positioning group, such as direct anterior, posterior, or lateral approach, were not available. These differences could substantially influence blood loss and recovery trajectories. The independent effect of patient positioning remains uncertain because surgical approach and position were tightly linked (supine: direct anterior; lateral: posterolateral). Thus, the observed LOS benefit may be confounded by approach-specific factors (eg, tissue handling, imaging, mobilization). Future multicenter, prospective studies separating approach and position effects are needed to confirm positioning’s true impact on hospital stay. Additionally, while our age-stratified analysis provides valuable insights, future studies should consider more granular age categorizations and longer-term functional outcomes to fully understand the positioning effects across the patient lifespan. Future prospective studies by multi-centers would be beneficial to reduce these limitations and to validate our findings on THR outcomes.
Conclusion
Supine positioning emerged as the most significant protective factor against long hospitalization following primary THR, with a 68% reduction in the risk of extended hospital stays (OR: 0.32, p<0.001). Additional predictors of long LOS included ASA physical status ≥III, longer anesthesia duration, and higher IV fluid administration. For blood transfusion risk, significant predictors were ASA physical status ≥III, anesthesia duration, IV fluid volume, and lower body weight. While supine positioning substantially improved LOS outcomes, patient positioning was not shown as an independent predictor for transfusion risk. Our data highlights the importance of comprehensive preoperative risk assessment to optimize patient recovery, and to enhance resource utilization in THR procedures.
Abbreviations
ASA, American Society of Anesthesiologists; BMI, body mass index; CI, confidence interval; DM, diabetes mellitus; HTN, hypertension; IQR, interquartile range; IV, intravenous; LOS, length of stay; OR, odds ratio; PACU, post-anesthesia care unit; SD, standard deviation; SPSS, statistical package for the social sciences; THR, total hip replacement.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Ethics Committee of the Chang Gung Medical Foundation (approval number: 202500857B0). The need for informed consent was waived owing to the nature of its retrospective design and anonymized dataset.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Papalia R, Zampogna B, Torre G, et al. Preoperative and perioperative predictors of length of hospital stay after primary total hip arthroplasty-our experience on 743 cases. J Clin Med. 2021;10(21):5053. doi:10.3390/jcm10215053
2. Sheridan GA, Howard LC, Neufeld ME, Garbuz DS, Masri BA. Factors associated with length of stay for hip and knee arthroplasty: a 20-year single-province population-based analysis of longitudinal temporal trends. Arthroplast Today. 2023;24:101274. doi:10.1016/j.artd.2023.101274
3. Martinkovich SC, Trott GL, Garay M, Sewecke JJ, Sauber TJ, Sotereanos NG. Patient characteristics and surgical start time affect length of stay following anterior total hip arthroplasty. J Arthroplasty. 2020;35(8):2114–2118. doi:10.1016/j.arth.2020.03.049
4. Roger C, Debuyzer E, Dehl M, et al. Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary Hip or knee arthroplasty: retrospective Cohort Study. Orthop Traumatol Surg Res. 2019;105(5):949–955. doi:10.1016/j.otsr.2019.04.012
5. Benito J, Stafford J, Judd H, Ng M, Corces A, Roche MW. Length of stay increases 90-day readmission rates in patients undergoing primary total joint arthroplasty. J Am Acad Orthop Surg Glob Res Rev. 2022;6(3):e21. doi:10.5435/JAAOSGlobal-D-21-00271
6. DeMik DE, Carender CN, An Q, Callaghan JJ, Brown TS, Bedard NA. Longer length of stay is associated with more early complications after total knee arthroplasty. Iowa Orthop J. 2022;42(2):53–59.
7. Papalia GF, Zampogna B, Albo E, et al. The role of patient surgical positioning on Hip arthroplasty component placement and clinical outcomes: a systematic re-view and meta-analysis. Orthop Rev. 2023;15:74116. doi:10.52965/001c.74116
8. Xiao Y, Li Z, Feng E, et al. Direct anterior approach for total Hip arthroplasty with patients in the lateral decubitus versus supine positions: a prospective, double-blinded, randomized clinical trial. J Orthop Surg. 2022;30(1):23094990221074758. doi:10.1177/23094990221074758
9. Takada R, Jinno T, Miyatake K, et al. Supine versus lateral position for accurate positioning of acetabular cup in total Hip arthroplasty using the modified Watson-Jones approach: a randomized single-blind controlled trial. Orthop Traumatol Surg Res. 2019;105(5):915–922. doi:10.1016/j.otsr.2019.05.004
10. Pearsall C, Denham M, Frederick JS, et al. A comparison of postoperative outcomes between supine and lateral patient positioning in total hip arthroplasty using the anterior-based muscle sparing surgical approach. Arthroplast Today. 2024;29:101515. doi:10.1016/j.artd.2024.101515
11. Ang JJM, Onggo JR, Stokes CM, Ambikaipalan A. Comparing direct anterior approach versus posterior approach or lateral approach in total Hip arthroplasty: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol. 2023;33(7):2773–2792. doi:10.1007/s00590-023-03528-8
12. Loh B, Padki A, Yew A, Pang HN. Functional outcome of direct anterior versus posterior approach in total Hip arthroplasty: a propensity-matched Asian study. Singapore Med J. 2024;2024:10–4103. doi:10.4103/singaporemedj.SMJ-2021-125
13. Naito Y, Hasegawa M, Tone S, Wakabayashi H, Sudo A. Registration in the supine position improve the accuracy of cup placement in total Hip arthroplasty using a portable navigation system. Sci Rep. 2023;13(1):20222. doi:10.1038/s41598-023-47674-9
14. Vandenbroucke JP, von Elm E, Altman DG, et al. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4(10):e297. doi:10.1371/journal.pmed.0040297
15. Ahmad M, Shaikh A, Ahmad AS, Awan N. Enhanced recovery program - impact of ASA grade on length of hospital stay in patients undergoing hip and knee arthroplasties. Surgeon. 2023;21(1):16–20. doi:10.1016/j.surge.2022.01.003
16. Meyer AC, Eklund H, Hedstrom M, Modig K. The ASA score predicts infections, cardiovascular complications, and hospital readmissions after hip fracture - A nationwide cohort study. Osteoporos Int. 2021;32(11):2185–2192. doi:10.1007/s00198-021-05956-w
17. Kilinc G, Karakus O, Gurer B. The role of ASA score and Charlson comorbidity index in predicting in-hospital mortality in geriatric hip fracture patients. Eur Rev Med Pharmacol Sci. 2023;27(15):7065–7072. doi:10.26355/eurrev_202308_33279
18. Yan JF, Zhao L, Li Q. Clinical comparison between direct anterior approach and posterior lateral approach in total hip arthroplasty and risk factors for lateral femoral cutaneous nerve injury. Front Surg. 2025;12:1482731. doi:10.3389/fsurg.2025.1482731
19. Qadan M, Gardner SA, Vitale DS, Lominadze D, Joshua IG, Polk HC. Hypothermia and surgery: immunologic mechanisms for current practice. Ann Surg. 2009;250(1):134–140. doi:10.1097/SLA.0b013e3181ad85f7
20. Han IW, Kim H, Heo J, et al. Excess intraoperative fluid volume administration is associated with pancreatic fistula after pancreaticoduodenectomy: a retrospective multicenter study. Medicine. 2017;96(22):e6893. doi:10.1097/MD.0000000000006893
21. Kim JA, Ahn HJ, Oh AR, Choi J. Restrictive intraoperative fluid management was associated with higher incidence of composite complications compared to less restrictive strategies in open thoracotomy: a retrospective cohort study. Sci Rep. 2020;10(1):8449. doi:10.1038/s41598-020-65532-w
22. Klasan A, Dworschak P, Heyse TJ, et al. Transfusions increase complications and infections after hip and knee arthroplasty: an analysis of 2760 cases. Technol Health Care. 2018;26(5):825–832. doi:10.3233/THC-181324
23. Lee JH, Han SB. Patient blood management in hip replacement arthroplasty. Hip Pelvis. 2015;27(4):201–208. doi:10.5371/hp.2015.27.4.201
24. Zhao J, Li J, Zheng W, Liu D, Sun X, Xu W. Low body mass index and blood loss in primary total Hip arthroplasty: results from 236 consecutive ankylosing spondylitis patients. Biomed Res Int. 2014;2014:742393. doi:10.1155/2014/742393
25. Al-Husinat L, Azzam S, Sharie SA, et al. Impact of the American Society of Anesthesiologists (ASA) classification on Hip fracture surgery outcomes: insights from a retrospective analysis. BMC Anesthesiol. 2024;24(1):271. doi:10.1186/s12871-024-02660-0
26. Hong DL, Zhu Q, Chen WC, et al. Factors contributing to perioperative blood transfusion during total Hip arthroplasty in patients continuing preoperative aspirin treatment: a nomogram prediction model. BMC Musculoskelet Disord. 2025;26(1):138. doi:10.1186/s12891-025-08399-0
27. Buddhiraju A, Shimizu MR, Subih MA, Chen TL, Seo HH, Kwon YM. Validation of machine learning model performance in predicting blood transfusion after primary and revision total hip arthroplasty. J Arthroplasty. 2023;38(10):1959–1966. doi:10.1016/j.arth.2023.06.002
28. Meissner N, Strahl A, Rolvien T, Halder AM, Schrednitzki D. Blood transfusion in elective total Hip arthroplasty: can patient-specific parameters predict transfusion? Bone Jt Open. 2024;5(7):560–564. doi:10.1302/2633-1462.57.BJO-2023-0157.R1
29. Cecconi M, Fasano N, Langiano N, et al. Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia. Crit Care. 2011;15(3):R132. doi:10.1186/cc10246
30. Kawano H, Manabe S, Matsumoto T, et al. Comparison of intraoperative blood loss during spinal surgery using either remifentanil or fentanyl as an adjuvant to general anesthesia. BMC Anesthesiol. 2013;13(1):46. doi:10.1186/1471-2253-13-46
31. Borsinger TM, Chandi SK, Puri S, Debbi EM, Gausden EB, Chalmers BP. The efficacy and safety of tranexamic acid in total hip and knee arthroplasty: a literature review. HSS J. 2024;20(1):10–17. doi:10.1177/15563316231208716
32. Fillingham YA, Ramkumar DB, Jevsevar DS, et al. The efficacy of tranexamic acid in total hip arthroplasty: a network meta-analysis. J Arthroplasty. 2018;33(10):3083–3089e4. doi:10.1016/j.arth.2018.06.023
33. Ker K, Prieto-Merino D, Roberts I. Systematic review, meta-analysis and meta-regression of the effect of tranexamic acid on surgical blood loss. Br J Surg. 2013;100(10):1271–1279. doi:10.1002/bjs.9193
34. Haider MA, Ward SA, Rajahraman V, et al. Blood transfusion in the age of tranexamic acid: who needs a type and screen before total hip arthroplasty? J Arthroplasty. 2025;40(1):119–126. doi:10.1016/j.arth.2024.06.053
35. Thapaliya A, Mittal MM, Ratcliff TL, Mounasamy V, Wukich DK, Sambandam SN. Usage of tranexamic acid for total hip arthroplasty: a matched cohort analysis of 144,344 patients. J Clin Med. 2024;13(16):4920. doi:10.3390/jcm13164920
36. Zha GC, Zhu XR, Wang L, Li HW. Tranexamic acid reduces blood loss in primary total hip arthroplasty performed using the direct anterior approach: a one-center retrospective observational study. J Orthop Traumatol. 2022;23(1):12. doi:10.1186/s10195-022-00638-7
37. Zhang S, Huang Q, Xu B, Ma J, Cao G, Pei F. Effectiveness and safety of an optimized blood management program in total hip and knee arthroplasty: a large, single-center, retrospective study. Medicine. 2018;97(1):e9429. doi:10.1097/MD.0000000000009429
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.