Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Superselective Ophthalmic Artery Thrombolytic Therapy for Hyaluronic Acid Embolization: A Case Report
Authors Wu Q, Fu Q, Xu X, Zheng C, Zhang J, Chen M
Received 1 May 2022
Accepted for publication 20 July 2022
Published 1 August 2022 Volume 2022:15 Pages 1459—1463
DOI https://doi.org/10.2147/CCID.S367481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Qian Wu,1,* Qiang Fu,1,* Xiao Xu,2 Can Zheng,1 Jie Zhang,3 Minliang Chen1
1Department of Plastic and Reconstructive Surgery, Senior Department of Burns and Plastic Surgery, The Fourth Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Department of Ophthalmology, The Third Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China; 3Department of Interventional, The Fourth Medical Center of Chinese PLA General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Minliang Chen, Department of Plastic and Reconstructive Surgery, Senior Department of Burns and Plastic Surgery, The Fourth Medical Center of Chinese PLA General Hospital, No. 51 Fucheng Road, Haidian District, Beijing, 10048, People’s Republic of China, Tel +86 13911138381, Email [email protected] Xiao Xu, Department of Ophthalmology, The Third Medical Center of Chinese PLA General Hospital, No. 69 Yongding Road, Haidian District, Beijing, 100039, People’s Republic of China, Tel +86 13381020161, Email [email protected]
Abstract: Blindness caused by embolization of fillers is a rare but catastrophic complication after cosmetic injection. Vision improvement is rarely reported among the various studies on potential clinical treatments. In this case, the patient suffered from ophthalmic artery occlusion with no light perception 48 h after hyaluronic acid injection. After two intra-arterial thrombolytic therapy sessions and traditional sequential therapy, ocular appearance was restored to normal, blood supply to the retina and visual function were improved, and visual acuity was restored to hand motion levels. Our results suggest that intra-arterial thrombolytic therapy with hyaluronidase and papaverine has a positive effect on hyaluronic acid-induced visual loss and is worthy of clinical promotion.
Keywords: complication, filler embolism, intra-arterial thrombolytic therapy, visual function
Introduction
Cosmetic injection is the most common non-surgical cosmetic procedure, with more than 800,000 Americans receiving hyaluronic acid (HA) filler injection each year.1 However, the incidence of vascular complications caused by fillers is estimated to be 0.01%. Retrograde HA emboli to the ophthalmic artery or retinal artery carries a rare yet catastrophic risk of blindness.2 Of the 48 newly published cases of vision loss, vision with no light perception (NLP) has been improved in only two.3 The management varies widely, and none have been shown to be consistently effective.4 We report the first successfully treated case of 48-hour visual loss after HA injection, suggesting that intra-arterial thrombolytic therapy (IATT) with traditional sequential therapy has a positive effect and may be worthy of clinical application.
Case Report
A 46-year-old woman presented to our hospital with a painless, sudden loss of vision in her left eye 48 hours after HA (1 mL, Sutron® (Singclean, Hangzhou, China) injection of the nose and eyebrow at a beauty salon. Physical examination revealed ecchymosis with edema in the injection area, lid ptosis, conjunctival congestion, blunt light reflex, limited eye movement, dilated pupil and no light perception in the left eye (Figure 1A). Color fundus photography revealed filling defects in the branch retinal arteries, and pale optic discs with retinal edema. Flash visual evoked potential (FVEP) showed wave peak delay and amplitude reduction in the left eye (Figures 2A and 3A).
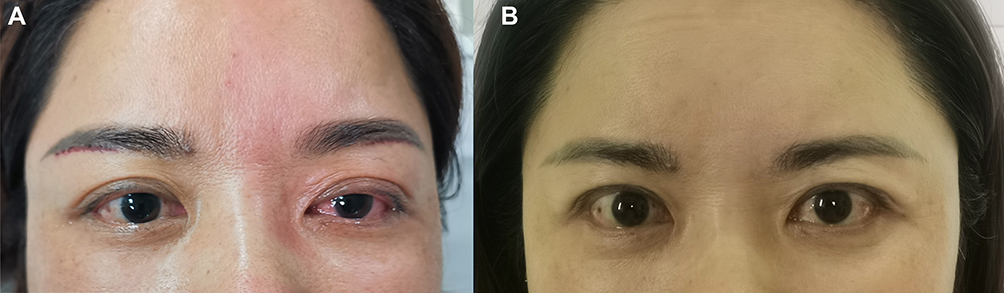 |
Figure 1 (A) Appearance on admission. (B) Appearance at month 3. |
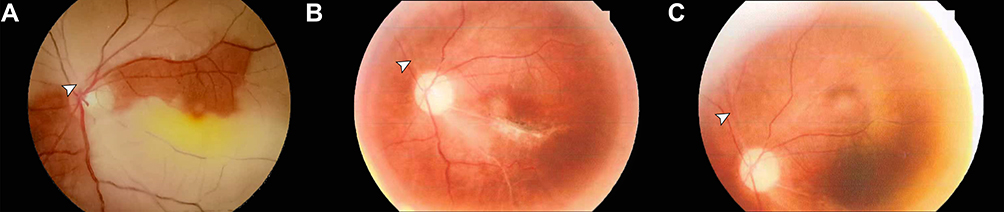 |
Figure 2 (A) Fundus photograph on admission: branch retinal arteries were segmented or absent (arrowheads). (B) Fundus photograph (posterior pole) at month 3: superior nasal arteriole of retina was recanalized (arrowheads). (C) Fundus photograph (above the optic disc) at month 3: superior nasal arteriole of retina was recanalized (arrowheads). |
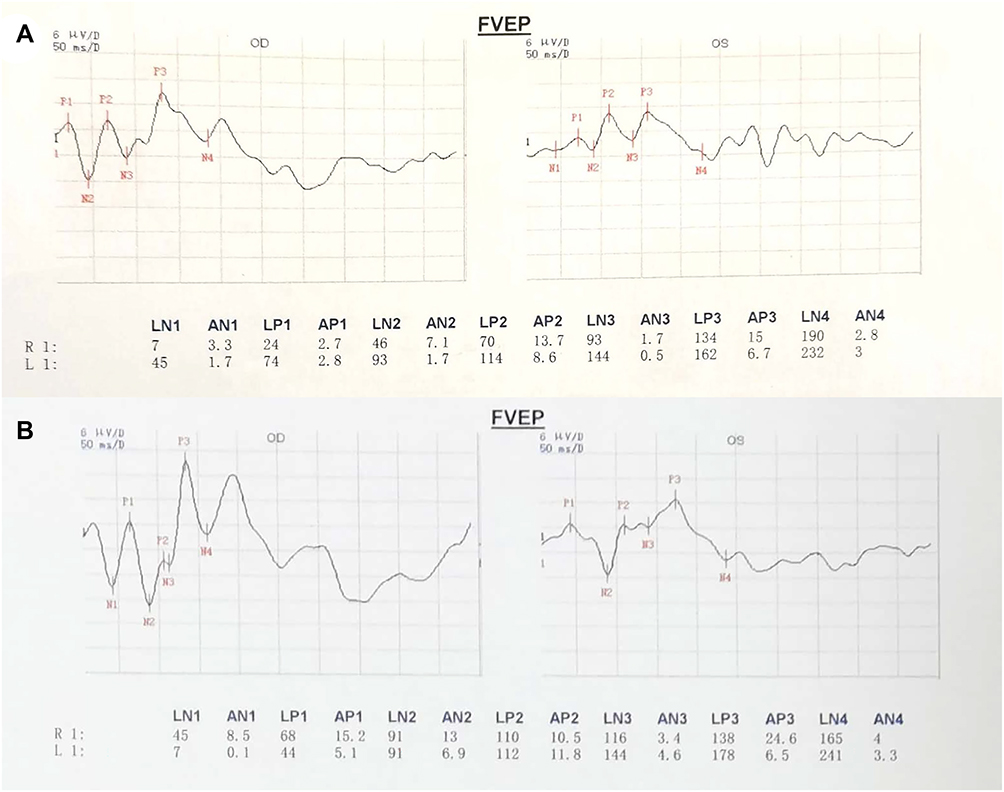 |
Figure 3 (A) Flash visual evoked potential on admission. (B) Flash visual evoked potential at month 3. |
After an emergency IATT with 1500U hyaluronidase and 30mg papaverine superselected to the opening of the left ophthalmic artery, digital subtraction angiography revealed that the blood flow of the embolized ophthalmic artery was significantly accelerated (Figure 4A and B).5 Assisted by traditional sequential therapy (high-dose pulsed methylprednisolone, alprostadil, neurotrophic agents, mannitol and other general symptomatic treatments), the patient reported a slight recovery of eyelid movement and reacquired light perception on the first postoperative day. Fundus photography revealed segmental changes in the branch retinal arteries. The next day, we performed the IATT again (Figure 4C). Her left visual acuity improved to hand motion. After three months, the ocular appearance and eye movement were completely healed, retinal edema disappeared, and FVEP showed wave peak delay and normal amplitude, while visual acuity did not change (Figures 1B, 2B, 2C and 3B).
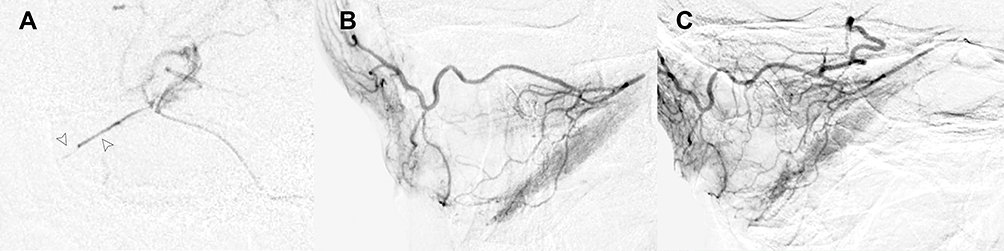 |
Figure 4 (A) Digital subtraction angiography image shows the segmental changes of the left ophthalmic artery (arrowheads). (B) Recanalization of the ophthalmic artery and its partial branches. (C) Digital subtraction angiography image after the second IATT. |
Discussion
Injectable fillers are popular for mid-face rejuvenation, replacing lost volume and providing contour support.6 Meanwhile the incidence of filler embolism has increased significantly in recent years. Retinal artery occlusion is an ophthalmic emergency that can result from HA filler cosmetic injections and is characterized by sudden painless and catastrophic vision loss. However, few treated cases of vision loss caused by HA injection have been reported to improve vision. A large number of aesthetic practitioners without strict professional training, lack the necessary knowledge of ophthalmic side effects and complications, and miss the optimal treatment timing.5,7–10
During glabellar injection, the needle may puncture small arteries and then fillers invade the ophthalmic artery and its branch with high injection pressure.11 The central retinal artery is the first branch that nourishes the inner retinal layers. Its diameter is approximately 160 μm and is easily blocked by HA with a size of 400 μm. Its occlusion can lead to macular ischemia and sudden vision loss.12 Most of the distal branches of the ophthalmic artery are susceptible to occlusion, which can cause corneal edema, ophthalmoplegia, horizontal strabismus, and ptosis.13
The retina is vulnerable to ischemia, which causes photoreceptor cells to suffer irreversible damage after 90 min.14 The therapeutic window may be slightly prolonged in this case because of an incomplete occlusion and the auto-fibrinolytic mechanism. FVEP at admission indicated that the bioelectrical signals of the visual pathway were weakened and light-sensitive neurons were less excited. Therefore, early reperfusion of the occluded artery is critical for retinal nerve cells. Hyaluronidase is a proteolytic enzyme that breaks down HA, but cannot pass through the dural sheath of the optic nerve.15 This suggests the usefulness of IATT, which provides rapid, precise and minimally invasive perfusion improvements. In the first IATT, there was significant recanalization of the ophthalmic artery but little improvement in the branch retinal arteries. We believe that hyaluronidase cannot provide sufficient benefits given its limited contact with emboli due to the extensibility of HA and its short plasma half-life; moreover, some small HA emboli dissolve incompletely and move to the distal artery causing secondary embolization.16 Then IATT was performed again to improve the thrombolytic effect and to examine ophthalmic artery recanalization. After the second IATT, the ophthalmic artery and the superior nasal arteriole of retina were recanalized. Experienced interventional doctors must operate carefully in such circumstances to reduce risks such as arterial dissection. This is because IATT is still an invasive treatment, especially for the ophthalmic artery, which has a diameter similar to that of a micro-guidewire.
Physicians should be acutely aware of the risks and severity of filler injections. Suitable and timely management not only improves visual acuity, but can also prevents other complications, including strabismus, ischemic optic neuropathy, and ocular atrophy.
Conclusion
IATT with hyaluronidase and papaverine is a promising procedure to treat HA embolization. Physicians should exercise extreme caution before and during injection procedures, and salvage systems and protocols should be established such that if ophthalmic artery occlusion is suspected, all possible treatments, including IATT, can be performed immediately.
Ethics Approval and Patient Consent
This case report has been reported following the CARE guidelines and adhered to the tenets of the Declaration of Helsinki. The patient gave written informed consent for the case publication including the images. Institutional approval was not required to publish the case details. Ethics approval was obtained from the Ethics Committee of the Fourth Medical Center of Chinese PLA General Hospital in Beijing, China, with the decision number 2021KY018-KS001.
Disclosure
Drs Wu and Fu are co-first authors. The authors report no conflicts of interest in this work.
References
1. Aesthetic Society. Aesthetic plastic surgery national databank statistics 2020. Aesthet Surg J. 2021;41(Suppl 2):1–16. doi:10.1093/asj/sjab178
2. Schelke L, Decates T, Kadouch J, Velthuis P. Incidence of vascular obstruction after filler injections. Aesthet Surg J. 2020;40(8):457–460. doi:10.1093/asj/sjaa086
3. Beleznay K, Carruthers JDA, Humphrey S, Carruthers A, Jones D. Update on avoiding and treating blindness from fillers: a recent review of the world literature. Aesthet Surg J. 2019;39(6):662–674. doi:10.1093/asj/sjz053
4. Nagendran ST, Ali MJ, Dogru M, Malhotra R. Complications and adverse effects of periocular aesthetic treatments. Surv Ophthalmol. 2021;67(3):741–757. doi:10.1016/j.survophthal.2021.04.009
5. Xu X, Zhou G, Fu Q, et al. Efficacy of intra-arterial thrombolytic therapy for vision loss resulting from hyaluronic acid filler embolization. J Cosmet Dermatol. 2021;20(10):3205–3212. doi:10.1111/jocd.14111
6. Trevidic P, Kaufman-Janette J, Weinkle S, et al. Injection guidelines for treating midface volume deficiency with hyaluronic acid fillers: the ATP approach (Anatomy, Techniques, Products). Aesthet Surg J. 2022. doi:10.1093/asj/sjac007
7. Zhang L, Luo Z, Li J, et al. Endovascular hyaluronidase application through superselective angiography to rescue blindness caused by hyaluronic acid injection. Aesthet Surg J. 2021;41(3):344–355. doi:10.1093/asj/sjaa036
8. Nguyen HH, Tran HT, Duong QH, Nguyen MD, Dao HX, Le DT. Significant vision recovery from filler-induced complete blindness with combined intra-arterial injection of hyaluronidase and thrombolytic agents. Aesthetic Plast Surg. 2021;46:1–5.
9. Zhang L-X, Lai L-Y, Zhou G-W, et al. Evaluation of intraarterial thrombolysis in treatment of cosmetic facial filler-related ophthalmic artery occlusion. Plast Reconstr Surg. 2020;145(1):42e–50e. doi:10.1097/PRS.0000000000006313
10. Kapoor KM, Kapoor P, Heydenrych I, Bertossi D. Vision loss associated with hyaluronic acid fillers: a systematic review of literature. Aesthetic Plast Surg. 2020;44(3):929–944. doi:10.1007/s00266-019-01562-8
11. Liu L, Yin M, Liu S, Hu M, Zhang B. Facial filler causes stroke after development of cerebral fat embolism. Lancet. 2020;395(10222):449. doi:10.1016/S0140-6736(20)30001-5
12. Lee JS, Kim JY, Jung C, Woo SJ. Iatrogenic ophthalmic artery occlusion and retinal artery occlusion. Prog Retin Eye Res. 2020;78:100848. doi:10.1016/j.preteyeres.2020.100848
13. Lee YJ, Woo SJ. Long-term outcomes of ophthalmic and retinal artery occlusion after cosmetic facial filler injection. Aesthet Surg J. 2022;42(2):196–204. doi:10.1093/asj/sjab099
14. Lazzeri D, Agostini T, Figus M, Nardi M, Pantaloni M, Lazzeri S. Blindness following cosmetic injections of the face. Plast Reconstr Surg. 2012;129(4):995–1012. doi:10.1097/PRS.0b013e3182442363
15. Paap MK, Milman T, Ugradar S, Silkiss RZ. Assessing retrobulbar hyaluronidase as a treatment for filler-induced blindness in a cadaver model. Plast Reconstr Surg. 2019;144(2):315–320. doi:10.1097/PRS.0000000000005806
16. Chen J, Ruan J, Wang W, et al. Superselective arterial hyaluronidase thrombolysis is not an effective treatment for hyaluronic acid-induced retinal artery occlusion: study in a rabbit model. Plast Reconstr Surg. 2021;147(1):69–75. doi:10.1097/PRS.0000000000007449
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.