Back to Journals » International Medical Case Reports Journal » Volume 18
Superior Sagittal Sinus Thrombosis presented as a migraine headache with normal D Dimer
Authors Ali RM, Metin Ö, Ali HA ![]()
Received 14 August 2025
Accepted for publication 21 November 2025
Published 25 November 2025 Volume 2025:18 Pages 1483—1488
DOI https://doi.org/10.2147/IMCRJ.S558120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Video abstract presented by Ali.
Views: 116
Ridwan Mohamud Ali, Ömer Metin, Hassan Adan Ali
Department of Emergency Medicine, Somali-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia
Correspondence: Ridwan Mohamud Ali, Email [email protected]
Introduction: Superior sagittal sinus thrombosis (SSST) is a rare type of cerebral venous sinus thrombosis (CVST) characterized by blood clot formation in the superior sagittal sinus, leading to increased intracranial pressure. This report highlights a case of SSST presenting atypically as a migraine with normal D-dimer levels, emphasizing the need for thorough evaluation despite normal lab results in at-risk individuals.
Presentation: A 49-year-old female experienced a severe unilateral headache, photophobia, dizziness, and neck tension. She has a history of migraines and hypertension. The patient uses combined oral contraceptives. Examination revealed neck stiffness, and blood pressure of 150/90. CT and D-Dimer were normal. MRV revealed Superior Sagittal Sinus thrombosis and lacunar infarction. Anticoagulation was initiated, leading to good recovery and discharge after 11 days.
Discussion: This case discusses an adult with a history of migraine presenting with a 5-day right-sided throbbing headache, photophobia, dizziness, and neck tension. Despite resembling a migraine exacerbation, red flags indicated a potential secondary cause. Normal D-dimer levels and unremarkable initial CT imaging delayed the diagnosis, but MRV revealed superior sagittal venous thrombosis (SSST) and a Lacunar infarct. Anticoagulation therapy led to significant improvement, and the patient was discharged after 11 days. The case highlights the need for vigilance regarding cerebral venous sinus thrombosis (CVST), in atypical headache presentations.
Conclusion: Clinical surveillance is vital for atypical headaches; inconclusive tests may delay diagnosis of superior sagittal sinus thrombosis (SSST). Advanced imaging and early anticoagulation improve outcomes, highlighting the need for high suspicion of cerebral venous sinus thrombosis.
Keywords: superior sagittal sinus thrombosis, migraine and D-dimer
Introduction
Superior sagittal sinus thrombosis (SSST) is a rare form of cerebral venous sinus thrombosis (CVST). It occurs due to the formation of a blood clot in the superior sagittal sinus, one of the major veins which help in blood drainage.1,2 SSST can result in cerebral edema, an increase in intracranial pressure, and other neurological consequences due to compromised venous drainage and elevated intracranial pressure.3,4 Cerebral venous sinus thrombosis accounts for 0.5% to 1% of all strokes and commonly affects younger individuals especially women in child-bearing period due to hormonal and prothrombotic risk factors.5 Mortality rates for SSST vary based on factors such as age, intracerebral hemorrhage, and associated complications, typically ranging from 4% to 16%, depending on disease severity and time to hospital referral.6–8 SSST can present with a wide range of symptoms, usually symptoms of increased intracranial pressure and localized cerebral damage. The most common symptom is persistent headache occurring in 50% to 80% of the patients. Other manifestations include seizures, hemiparesis, hemianesthesia, blurred vision and disturbed conscious level. In Severe cases, symptoms may worsen and lead to brain herniation and coma.3,9 Many risk factors are implicated in SSST. Acquired conditions such as oral contraceptive pills, dehydration, infections - especially in dangerous areas of the face, malignancies and systemic inflammatory diseases like systemic lupus erythematosus and Behçet’s disease can increase the risk of SSST.10–13 Additionally, Inherited thrombophilia conditions such as protein C and S deficiencies, antithrombin III deficiency, hyperhomocysteinemia and factor V Leiden mutation increase the risk of SSST.14,15
Diagnostic workup for SSST includes laboratory and radiological investigations. D-dimer represent a valuable screening tool for CVST. D-dimer levels correlate with the degree of sinus involvement, which helps in the rapid evaluation and diagnosis.16,17 The focus in diagnosing SSST is neuroimaging, where MR venography MRV) is the gold standard for diagnosis.18,19 A common alternative, especially in ER is CT venography which demonstrates “ empty delta” signs.20,21 This report describes a case of superior sagittal sinus thrombosis with atypical presentation as migraine and normal D-dimer levels, furthering knowledge of CVST’s multiple forms. It also serves as a reminder for clinicians that normal D-dimer does not rule out the need to evaluate for venous thrombosis especially in individuals with risk factors like oral contraceptive use or smoking given their abnormal lab results. In describing this case, we hope to minimize the diagnostic delays by drawing attention to the limitations of D-dimer testing for these patients while encouraging advanced neuroimaging if warranted by clinical suspicion.
Case Presentation
A 49-year-old female presented with a severe headache for 5 days. The headache was unilateral, mainly to the right side, throbbing in nature and developed on waking from sleep. There is also associated photophobia and dizziness. The patient also reported tension in the occipital region and to the neck. The patient has a history of migraine for 11 years (usually lasts 2–3 hours) and hypertension, for which she uses paracetamol, meloxicam and Candesartan cilexetil, respectively. She is a heavy smoker with 2–3 packs a-day, and use combined oral contraceptive pills. During examination, her temperature was 37.2 C. The patient had neck stiffness, and Blood pressure was 150/90. Native CT examination did not reveal any remarkable findings (Figure 1). The D-Dimer level was within the normal level (483 µg/mL, reference range 0–654 µg/mL) which made the thrombosis unlikely. Initial differential diagnosis was meningitis, stroke and subarachnoid hemorrhage. CRP was 1.89 (reference range 0–5 mg/L). Urea and electrolytes were within normal levels.
 |
Figure 1 Native CT scan of the brain showing no remarkable abnormalities (normal findings). |
Patients were admitted to the internal medicine unit on paracetamol, Zofran and Codeine phosphate. Magnetic Resonance Venography (MRV) with contrast showed Superior Sagittal Sinus thrombosis and lacunar infarct (Figure 2). Anticoagulation started with heparin and warfarin. The patient referred to the neurology unit to complete the treatment course. Eleven days after initiating treatment, the patient demonstrated good recovery and was subsequently discharged home.
 |
Figure 2 Magnetic Resonance Venography (MRV) with contrast demonstrating an interrupted course and filling defects in the superior sagittal sinus. Arrow indicates the site of abnormality, consistent with superior sagittal sinus thrombosis. |
Discussion
This case involves a young adult patient with a known history of migraine, who comes to the clinic with a persistent, right sided throbbing headache for the past 5 days, accompanied by photophobia, dizziness and tension on the occipital part of the head to the neck. Although the clinical picture of this patient resembles a migraine exacerbation, the presence of various red flags such as headache, sleep disturbances, neck stiffness and lack of response towards analgesics raised concern for the possibility of a secondary cause. Notably, the patient’s D-dimer level, which was tested, turned out to be within the normal reference range. This could have falsely reassured clinicians and delayed any further investigation. Initial non-contrast CT imaging was unremarkable; however, Contrast-Enhanced Magnetic Resonance Venography revealed Superior Sagittal Sinus Thrombosis and Lacunar infarct. Immediately anticoagulation therapy was started out with heparin and warfarin which led to significant improvement in the patients’ condition thereby getting discharged in 11 days after initial diagnosis. This case underscores the importance of maintaining a high index of suspicion for any cerebral venous sinus thrombosis in patients with atypical headache patterns even when the D-dimer test and initial imaging proved to be non-diagnostic.
CVST is a very rare or uncommon presentation of thrombosis with an annual reported incidence rate in adults ranging from 3–7/1,000,000 among populations.9,11,22 In regions with high infection rates, such as Pakistan CVST is even more prevalent, accounting for up to 18% of cases, although data across various ethnic groups is still lacking.23 There are two theories that explain the pathophysiology of CVST and each of these theories are seen to be either together or separate during the development of CVST. One theory suggests that thrombosis of the cerebral veins and venous sinus, elevates the intracranial pressure by disrupting the blood-brain-barrier and also impairing the cerebral perfusion. Increased venous pressure may lead to vasogenic edema, while the reduced cerebral perfusion and Na⁺/K⁺ ATPase pump failure may cause cytotoxic edema.24,25 While the second theory focuses on the direct thrombosis of the major venous sinuses, especially the SSS, which elevates the sinus pressure and disrupts the cerebrospinal fluid (CSF) absorption via the arachnoid villi. This impaired absorption leads to intracranial hypertension.25 The Superior Sagittal Sinus is a crucial venous structure that is prone to thrombotic emergencies. The common presentations include headache, papilledema, sixth nerve palsy, hemiparesis or seizures. It should be always considered in young women with cryptogenic stroke, particularly those women who are taking any form of oral contraceptives who may have some hypercoagulable states. Bacterial meningitis or sinus infections can cause thrombosis in certain rare occasions.26,27 Due to its contiguity with the falx cerebri, the superior sagittal sinus is always involved with meningioma development. Any kind of tumor invasion of the sinus complicates the surgical resection, often resulting in an incomplete removal and leading to a higher recurrence rate. Elevated Intracranial Pressure (ICP) can cause a reversing of venous flow through diploic and emissary veins thus increasing the risk of hemorrhage during craniotomy. Surgeons must carefully localize the sinus which is relative to the sagittal suture to avoid any injury that may be caused while placing the burr holes.27,28
The clinical presentation of cerebral venous thrombosis (CVT) is often non-specific and varies based on its lesion location, the extent, the age of the patient, and any known comorbidities. About 40% of cases seem to be present with acute stroke-like symptoms within 48 hours, like an acute headache often without any neurological deficits. Frequently reported manifestations include headache (70–90%), seizures (30–40%), papilledema (30–60%), aphasia (15–20%), coma (5–15%) and rarely, movement disorders.29 A non-contrast CT scan is generally the first line investigation that may appear normal or only show indirect signs such as sulcal effacement or any atypical infarcts. CT venography improves the detection by revealing the “empty delta sign”, which is a classic finding. MRI and MR Venography are more sensitive and provide a clearer visualization of thrombus with the sinus and show any parenchymal changes although they have limitations such as signal loss and misinterpretation of sinus variants. While no single blood test can confirm CVT, lab values investigations can help to identify the contributing factors such as infection, inflammation or prothrombotic states.29 To further illuminate the clinical presentation, diagnostic modalities, and outcomes associated with SSST, a comparative analysis mentioning the key findings was conducted. Table 1 summarizes 4 representative studies. Across the studies, headache emerged as the most common presenting symptom just like the patient in our case. The role of D-dimer as a diagnostic tool was variable with most cases showing elevations in the tool, while also showcasing the test’s insensitivity. Imaging modalities such as MRI, MRV and CT venography were utilized to confirm the diagnosis.
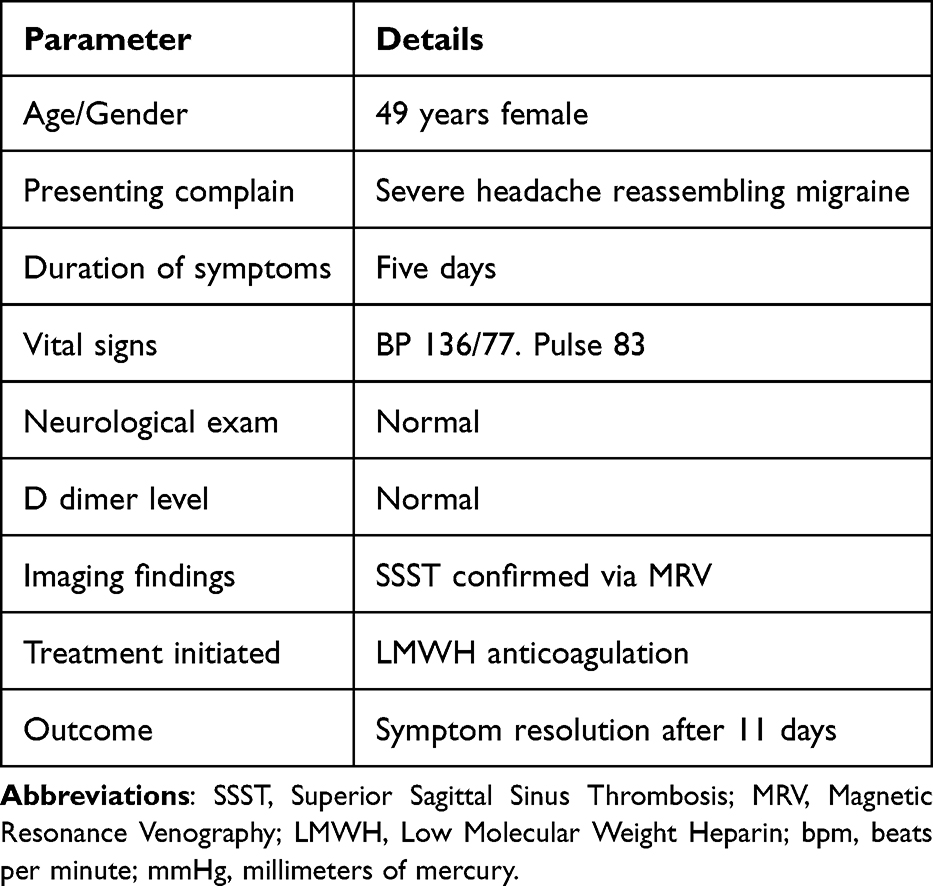 |
Table 1 Patient Clinical Summary |
Conclusion
This case highlights the critical need for clinical surveillance in evaluating atypical headaches, especially when the initial tests such as D-dimer and non-contrast CT were inconclusive. SSST can mimic benign conditions like migraine, leading to delay in diagnostic workup. As supported by literature, timely use of advanced imaging techniques like MRV and CT venography is essential for an accurate diagnosis. The variability in D-dimer sensitivity further emphasizes that it should not be relied upon for any possible exclusion. Early recognition and initiation of anticoagulation therapy significantly can improve outcomes, showcasing the importance of maintaining a high index of suspicion for cerebral venous sinus thrombosis in any appropriate clinical contexts.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
Institutional approval was not required for publication of this case report. The study was conducted at Somali-Turkey Recep Tayyip Erdoğan Training and Research Hospital, Mogadishu, Somalia. Methods The case has been reported in line with the surgical case report (SCARE) 2025 criteria.30
Patient Consent
Written Informed consent had obtained by the patient and her brother to have the case details, published. A copy of the written consent is available for review by the editor in chief of this journal on request.
Consent for Publication
Written informed consent was obtained from the patient and her brother for publication of the case details and any accompanying images. A copy of the consent is available for review by the Editor-in-Chief upon request.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Botz B, Gaillard F. Superior sagittal sinus thrombosis. Radiopaedia Org. 2005. doi:10.53347/rID-6517
2. Nakase H, Takeshima T, Sakaki T, Heimann A, Kempski O. Superior sagittal sinus thrombosis: a clinical and experimental study. Skull Base Surg. 1998;8(04):169–174. doi:10.1055/s-2008-1058178
3. Ferro JM, Canhão P, Stam J, Bosser M-G, Barinaga Rementeria F. ISCVT investigators. prognosis of cerebral vein and dural sinus thrombosis: results of the international study on cerebral vein and dural sinus thrombosis (ISCVT). Stroke. 2004;35(3):664–670. doi:10.1161/01.STR.0000117571.76197.26
4. Sanz Gallego I, Fuentes B, Martínez-Sánchez P, Díez Tejedor E. Do cerebral venous thrombosis risk factors influence the development of an associated venous infarction? Neurology. 2011;26:13–19. doi:10.1016/j.nrl.2010.10.001
5. Danwang C, Mazou TN, Tochie JN, Tankeu R, Bigna JJ. Global epidemiology and patterns of cerebral venous thrombosis: a systematic review and meta-analysis protocol. BMJ Open. 2018;
6. Patil VC, Chararria K, Desai N, Agrawal S. Clinical profile and outcome of cerebral venous sinus thrombosis at tertiary care center. J Neurosis Rural Pracht. 2014;5(3):218–224. doi:10.4103/0976-3147.133559
7. Borhani Haghighi A, Edgell RC, Cruz-Flores S, et al. Mortality of cerebral venous-sinus thrombosis in a large national sample. Stroke. 2012;43(1):262–264. doi:10.1161/STROKEAHA.111.635664
8. Canhão P, Ferro JM, Lindgren AG, et al. Causes and predictors of death in cerebral venous thrombosis. Stroke. 2005;36(8):1720–1725. doi:10.1161/01.STR.0000173152.84438.1c
9. Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791–1798.
10. Coutinho JM, Ferro JM, Canhão P, et al. Cerebral venous and sinus thrombosis in women. Stroke. 2009;40(7):2356–2361. doi:10.1161/STROKEAHA.108.543884
11. Bousser M-G, Ferro JM. Cerebral venous thrombosis: an update. Lancet Neurol. 2007;6(2):162–170. doi:10.1016/S1474-4422(07)70029-7
12. Vedavati MC, Shu L, Henninger N, et al. Cerebral venous sinus thrombosis associated with cancer: analysis of the ACTION-CVT study. J Thrombolysis. 2024;57(6):1008–1017. doi:10.1007/s11239-024-02997-w
13. Shi J, Huang X, Li G, et al. Cerebral venous sinus thrombosis in Behçet’s disease: a retrospective case-control study. Clin Rheumatol. 2018;37(1):51–57. doi:10.1007/s10067-017-3718-2
14. Roach ES, Golomb MR, Adams R, et al. Management of stroke in infants and children: a scientific statement from a special writing group of the American heart association stroke council and the council on cardiovascular disease in the young. Stroke. 2008;39(9):2644–2691. doi:10.1161/STROKEAHA.108.189696
15. Wysokinska EM, Wysokinski WE, Brown RD, et al. Thrombophilia differences in cerebral venous sinus and lower extremity deep venous thrombosis. Neurology. 2008;70(8):627–633. doi:10.1212/01.wnl.0000297195.97325.a8
16. Kosinski CM, Mull M, Schwarz M, et al. Do normal D dimer levels reliably exclude cerebral sinus thrombosis? Stroke. 2004;35(12):2820–2825. doi:10.1161/01.STR.0000147045.71923
17. Dentali F, Squizzato A, Marchesi C, Bonzini M, Ferro JM, Ageno W. D-dimer testing in the diagnosis of cerebral vein thrombosis: a systematic review and a meta-analysis of the literature. J Thromb Haemost. 2012;10(4):582–589. doi:10.1111/j.1538-7836.2012.04637.x
18. Choi JE, Weon YC, Park GM, et al. Comparison of MRI sequences for the detection of cerebral venous sinus thrombosis during follow-up. J Korean Soc Radiol. 2018;78(5):330. doi:10.3348/jksr.2018.78.5.330
19. Saposnik G, Barinagarrementeria F, Brown RD, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American heart association/American stroke association. Stroke. 2011;42(4):1158–1192. doi:10.1161/STR.0b013e31820a8364
20. Khandelwal N, Agarwal A, Kochhar R, et al. Comparison of CT venography with MR venography in cerebral sinovenous thrombosis. AJR Am J Roentgenol. 2006;187(6):1637–1643. doi:10.2214/AJR.05.1249
21. Shinohara Y, Yoshitoshi M, Yoshii F. Appearance and disappearance of empty delta sign in superior sagittal sinus thrombosis. Stroke. 1986;17(6):1282–1284. doi:10.1161/01.STR.17.6.1282
22. Zhang H, Zhang X, Zheng D. Superior sagittal sinus thrombosis as a rare complication of spontaneous intracranial hypotension syndrome: a case report and review of the literature. Int J Neurosci. 2019;129(4):4015. doi:10.1080/00207454.2018.1538144
23. Khealani BA, Wasay M, Saadah M, et al. Cerebral venous thrombosis: a descriptive multicenter study of patients in pakistan and middle east. Stroke. 2008;39(10):2707–2711. doi:10.1161/STROKEAHA.107.512814
24. Gotoh M, Ohmoto T, Kuyama H. Experimental study of venous circulatory disturbance by dural sinus occlusion. Acta Neurochirurgica. 1993;124(2–4):12026. doi:10.1007/BF01401133
25. Aristotelis F, Kapsalaki E, Patramani G, Fountas KN. Cerebral venous sinus thrombosis: review of the demographics, pathophysiology, current diagnosis, and treatment. Neurosurgical Focus. 2009;27(5):E3. doi:10.3171/2009.8.FOCUS09167
26. Patchana T, Zampella B, Berry JA, Lawandy S, Sweiss RB. Superior sagittal sinus: a review of the history, surgical considerations, and pathology. Cureus. 2019. doi:10.7759/cureus.4597
27. Letchuman V, Donohoe C. Neuroanatomy, superior sagittal sinus. StatPearls. Treasure Island (FL):StatPearls Publishing;2025. http://www.ncbi.nlm.nih.gov/books/NBK546615/.
28. Bi N, Rui-Xue X, Liu R-Y, et al. Microsurgical treatment for parasagittal meningioma in the central gyrus region. Oncol Lett. 2013;6(3):781–784. doi:10.3892/ol.2013.1429
29. Ranjan R, Ken-Dror G, Sharma P. Pathophysiology, diagnosis and management of cerebral venous thrombosis: a comprehensive review. Medicine. 2023;102(48):e36366. doi:10.1097/MD.0000000000036366
30. Kerwan A, Al-Jabir A, Mathew G, et al. Revised surgical case report (SCARE) guideline: an update for the age of artificial intelligence. Premier J Sci. 2025;(10):100079.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.