Back to Journals » International Medical Case Reports Journal » Volume 19
Superior Mesenteric Artery Syndrome in an Adolescent Presenting with Acute Massive Gastric Obstruction
Authors Chatzichidiroglou A ![]() , Karakasis P, Taousani E, Antonakou A
, Karakasis P, Taousani E, Antonakou A
Received 18 March 2026
Accepted for publication 23 May 2026
Published 27 May 2026 Volume 2026:19 609809
DOI https://doi.org/10.2147/IMCRJ.S609809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Anastasios Chatzichidiroglou,1 Paschalis Karakasis,2 Eleftheria Taousani,1 Angeliki Antonakou1
1Department of Midwifery, International Hellenic University, Thessaloniki, Greece; 2Second Department of Cardiology, Aristotle University of Thessaloniki, Hippokration General Hospital, Thessaloniki, Greece
Correspondence: Paschalis Karakasis, Second Department of Cardiology, Aristotle University of Thessaloniki, General Hospital Hippokration, Greece, Email [email protected]
Abstract: Superior mesenteric artery syndrome (SMAS) is an uncommon cause of proximal intestinal obstruction caused by compression of the third portion of the duodenum between the SMA and the abdominal aorta. We report the case of a 17-year-old boy with a 2-year history of recurrent nausea, vomiting, epigastric pain, early satiety, postprandial fullness, and progressive abdominal distension, followed by recent clinical deterioration. Despite repeated non-diagnostic investigations and empirical dietary and pharmacological treatment, symptoms persisted. Contrast-enhanced computed tomography established the diagnosis by demonstrating a markedly reduced aortomesenteric angle of approximately 10° and an aortomesenteric distance of 5.5 mm, associated with severe gastric and proximal duodenal dilatation. The patient was treated conservatively with nasogastric decompression and nutritional support. Nasogastric tube placement resulted in marked gastric decompression, with substantial improvement in abdominal distension, epigastric discomfort, early satiety, and vomiting, allowing surgical intervention to be deferred during the acute phase. Follow-up showed no further acute obstructive deterioration; however, the absence of meaningful weight gain over the subsequent six months indicated persistence of the chronic nutritional component of SMAS and the need for continued dietary rehabilitation and close monitoring. This case highlights the diagnostic difficulty of SMAS in adolescents with chronic, treatment-refractory upper gastrointestinal symptoms and emphasizes that resolution of acute obstruction should not be equated with definitive correction of the underlying disease process. Early recognition, conservative stabilization, nutritional optimization, and longitudinal reassessment are essential to prevent delayed diagnosis and guide timely escalation to surgery when conservative treatment is insufficient.
Keywords: intestinal obstruction, weight loss, superior mesenteric syndrome, abdominal pain, vomiting
Introduction
Superior mesenteric artery syndrome (SMAS) is a rare cause of proximal intestinal obstruction caused by compression of the third portion of the duodenum between the superior mesenteric artery and the abdominal aorta. This compression is usually related to narrowing of the aortomesenteric angle and reduction of the intervening retroperitoneal and mesenteric fat pad, resulting in impaired duodenal passage and proximal gastrointestinal dilatation (Figure 1).
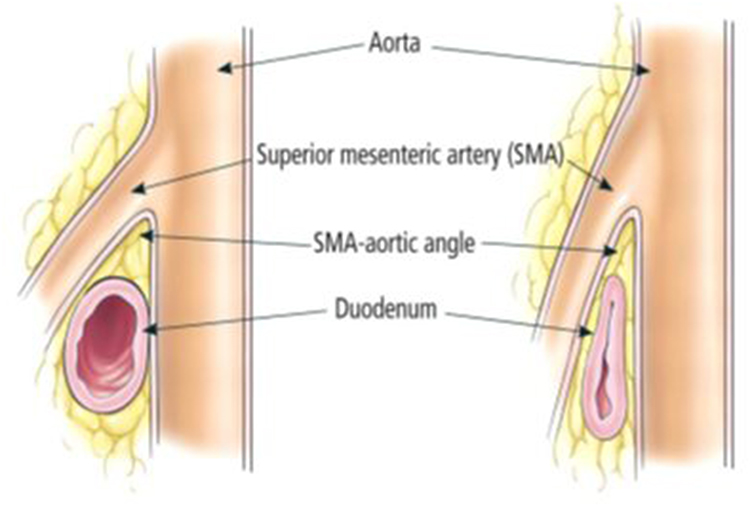 |
Figure 1 Left, the normal angle between the superior mesenteric artery (SMA) and the aorta is 25 to 60 degrees. Right, in SMA syndrome, the aortomesenteric angle is more acute, and the duodenum is compressed between the aorta and the SMA (Reproduced with permission from Pasumarthy et al (2010) Cleveland Clinic Journal of Medicine 77:45–50). |
The syndrome was first described by Von Rokitansky in 1842 and about 400 SMAS cases have been reported so far. The syndrome is characterized mainly by the compression of the third part of the duodenum between the SMA anteriorly and the aorta posteriorly leading to symptoms of upper gastrointestinal obstruction. Among the aetiological factors of SMAS are marked weight loss, external compression of the abdomen, anatomical variations and surgical anatomical alterations.1,2 SMAS mostly occurs in adolescents or young adults and due to its rarity the early clinical recognition is usually difficult. The diagnosis is often late, till the patients are far advanced with their symptoms.1,2 Main symptoms of SMAS are post-prandial epigastric fullness accompanied with pain, eructation, bilious vomiting and, rarely, acute gastric dilation. SMAS may have several complications like dehydration, metabolic alkalosis, gastric necrosis and systemic circulatory failure. The syndrome is extremely rare among children and may easily be neglected by pediatricians.
In this report a SMAS case in an adolescent boy which was treated conservatively is presented,as well as a short review of the literature on this disease.3 The present case is important because it illustrates the diagnostic challenge of SMAS in an adolescent with chronic treatment-refractory symptoms who presented with acute massive gastric obstruction, and highlights the potential for substantial clinical improvement after timely recognition and conservative decompression. This report aims to increase clinical awareness of SMAS as an uncommon but relevant differential diagnosis in adolescents presenting with persistent vomiting, early satiety, abdominal pain, and gastric distension.
Case Presentation
A 17-year-old boy was referred to our internal medicine clinic for evaluation of persistent upper gastrointestinal symptoms that had progressively worsened over a 2-year period. His main complaints were dull epigastric abdominal pain, marked bloating, early satiety with loss of hunger sensation, postprandial fullness, and intermittent non-bloody vomiting. The symptoms were predominantly meal-related and had gradually become more limiting in daily life. He also reported abdominal discomfort during physical activity, which eventually led him to discontinue gymnastics. Bowel habits were irregular, with defecation usually occurring every four days and often requiring laxative use. He denied fever, chills, jaundice, diarrhea, gastrointestinal bleeding, or recent sick contacts. According to the patient, the onset of symptoms followed hospitalization for complicated pneumonia approximately two years earlier.
During the preceding two years, the patient had undergone repeated diagnostic evaluations without a definitive diagnosis. These included laboratory blood testing, abdominal imaging, upper gastrointestinal endoscopy, and colonoscopy, all of which were non-diagnostic. Empirical treatment with proton pump inhibitors and dietary modifications, including gluten-free and lactose-free diets, had been attempted without meaningful clinical improvement. At presentation to our clinic, the patient appeared anxious but was hemodynamically stable, with vital signs within normal limits. Physical examination was notable for a firm, diffusely tender, and markedly distended abdomen. Percussion suggested pronounced gastric distension, while no signs of peritonitis, jaundice, peripheral edema, or systemic infection were present. Routine laboratory evaluation did not reveal clinically significant abnormalities. Given the chronicity of symptoms, the severity of abdominal distension, and the failure of previous empirical treatment, the patient was admitted for further investigation.
Contrast-enhanced computed tomography of the abdomen and pelvis demonstrated severe dilatation of the stomach and proximal duodenum, with an abrupt transition at the level of the third portion of the duodenum. The superior mesenteric artery formed an extremely acute angle with the abdominal aorta, measuring approximately 10° (Figure 2), and the aortomesenteric distance was reduced to 5.5 mm (Figure 3). These findings were consistent with extrinsic compression of the third portion of the duodenum between the superior mesenteric artery and the aorta and established the diagnosis of superior mesenteric artery syndrome.3,4 The imaging findings also explained the patient’s long-standing postprandial symptoms and the recent deterioration characterized by massive gastric distension.
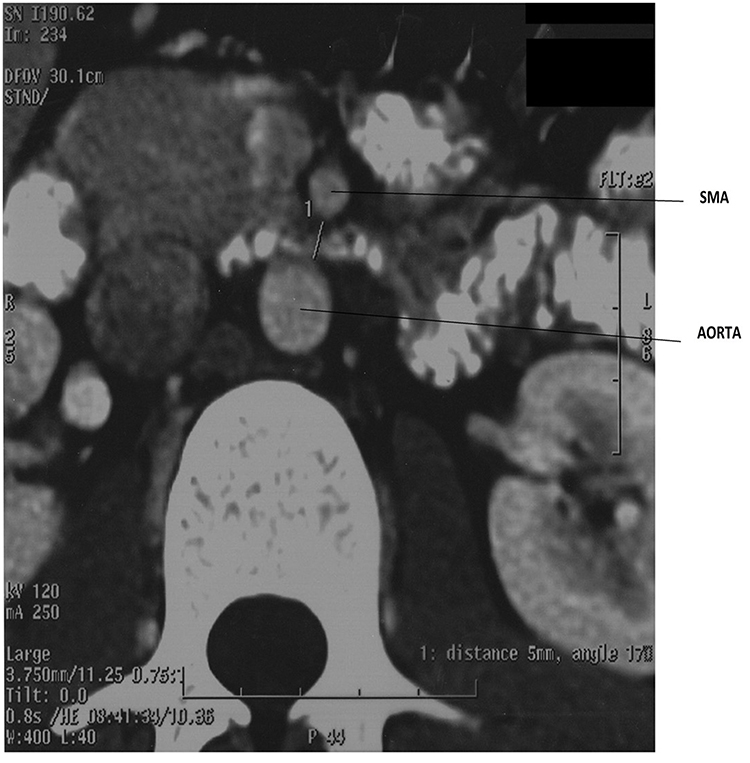 |
Figure 2 CT scan showing the SMA and the aorta separated by a small distance of 5.5 mm and severe gastric distension. SMA; superior mesenteric artery. |
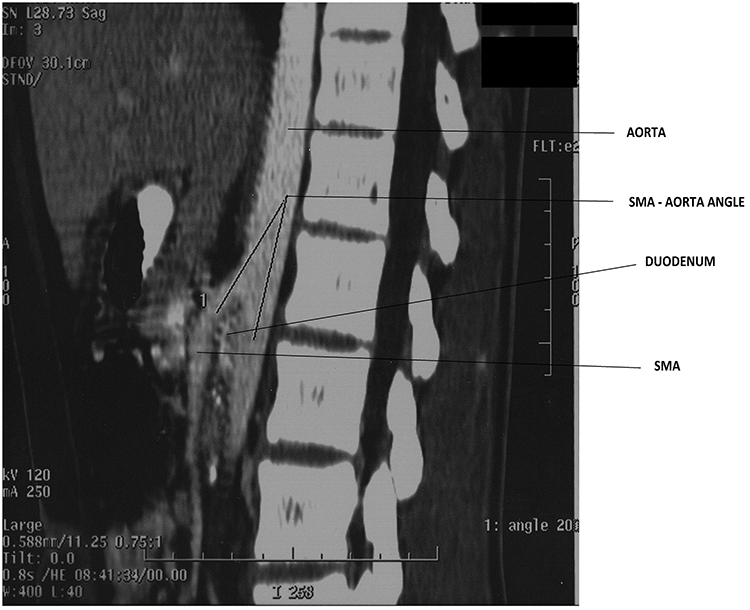 |
Figure 3 Sagittal CT image showing compression of the duodenum between the aorta and the SMA, with an aortomesenteric angle of approximately 10°. SMA, superior mesenteric artery. |
Conservative management was initiated immediately. A nasogastric tube was placed for gastric decompression, resulting in marked evacuation of gastric contents and progressive improvement in abdominal distension, epigastric discomfort, early satiety, and vomiting. The patient remained hemodynamically stable throughout hospitalization and did not develop signs of shock, peritonitis, gastric ischemia, or electrolyte-related clinical deterioration. Nutritional support was introduced with the aim of restoring the retroperitoneal and mesenteric fat pad and reducing duodenal compression. Because of the clear symptomatic response to decompression and the absence of clinical instability, surgical intervention was deferred during the acute phase.
At follow-up, no further episode of acute obstructive deterioration was documented. However, despite improvement in the acute symptoms, the patient did not achieve meaningful weight gain during the subsequent six months. This suggested that although conservative decompression was effective in resolving the acute obstructive component, the underlying chronic nutritional and anatomical predisposition to SMAS had not been fully corrected. Continued dietary rehabilitation, close clinical monitoring, and reassessment for possible surgical management in the event of recurrent symptoms or failure of nutritional recovery were therefore considered necessary.
Discussion
The SMA arises from the anterior aspect of the abdominal aorta at approximately the level of the first lumbar vertebra, close to the pancreatic neck, and supplies the distal duodenum, small intestine, proximal two-thirds of the transverse colon, and portions of the pancreas. Under normal anatomical conditions, the SMA forms an aortomesenteric angle of approximately 45° with the abdominal aorta, although values between 38° and 56° are commonly reported. This anatomical configuration creates a narrow but functionally protected three-dimensional aortomesenteric space through which the third portion of the duodenum traverses from right to left, immediately inferior to the left renal vein. The integrity of this space is maintained largely by retroperitoneal, mesenteric, and lymphatic tissue, which preserves both the aortomesenteric angle and the aortomesenteric distance.1
The mean aortomesenteric distance is generally reported to range between 10 and 28 mm and is influenced by the degree of mesenteric adiposity as well as the aortomesenteric angle. Loss of the intervening fat pad, particularly in the setting of rapid or substantial weight loss, can reduce the aortomesenteric angle to less than 25° and the aortomesenteric distance to less than 8 mm.2 This anatomical distortion narrows the space between the SMA and abdominal aorta, predisposing the third portion of the duodenum to extrinsic vascular compression. The resulting proximal obstruction defines SMAS and may manifest with a broad clinical spectrum, ranging from chronic postprandial discomfort and early satiety to recurrent vomiting, severe gastric dilatation, dehydration, electrolyte imbalance, and, rarely, life-threatening complications.5
In the present case, the pathophysiological substrate was particularly relevant because the patient had a chronically low body habitus rather than a clearly documented episode of abrupt weight loss. His weight and height were in the 3rd and 90th–97th percentiles, respectively, with a BMI of 18 kg/m2, consistent with an underweight phenotype. According to his mother, he had been cachectic since early childhood, without a history of sudden weight loss. Therefore, chronic paucity of retroperitoneal and mesenteric adipose tissue was considered a key predisposing factor for the development of SMAS in this patient. This observation is clinically important, as it underscores that SMAS in adolescents may arise not only after acute catabolic events but also in the context of long-standing constitutional thinness, particularly when additional factors increase duodenal compression or impair gastric emptying.
Although SMAS has been more extensively described in adults, the pediatric and adolescent literature remains limited and is composed mainly of case reports and small retrospective series. Pediatric patients often present with nonspecific symptoms, including recurrent vomiting, abdominal pain, early satiety, postprandial fullness, weight loss, or malnutrition, which can delay diagnosis and lead to repeated evaluations for more common gastrointestinal disorders. In a recent 10-year pediatric experience including 14 patients, vomiting and abdominal pain were the most frequent symptoms, malnutrition was present in most cases, and diagnosis was most commonly established by cross-sectional imaging demonstrating narrowing of the aortomesenteric angle and distance.6 Importantly, all patients in that series initially received conservative management; approximately two-thirds achieved complete symptom resolution, whereas the remaining patients required surgery because of persistent or refractory symptoms.6 These findings support a stepwise therapeutic approach but also emphasize the need for close follow-up, as a substantial minority of pediatric patients ultimately require operative treatment.
The differential diagnosis of vomiting in children is broad and commonly includes acute viral gastroenteritis, food poisoning, gastritis, functional gastrointestinal disorders, pancreatitis, and mechanical obstruction at different levels of the gastrointestinal tract.7 Most benign causes respond promptly to antiemetic therapy, rehydration, and supportive care. However, persistent or recurrent vomiting that is resistant to standard medical therapy, particularly when accompanied by upper abdominal pain, early satiety, postprandial fullness, dehydration, or marked gastric distension, should prompt consideration of uncommon obstructive entities such as SMAS. In this context, early recognition is essential because delayed diagnosis may perpetuate a vicious cycle of vomiting, reduced oral intake, worsening malnutrition, further loss of mesenteric fat, and progressive narrowing of the aortomesenteric space.
The severity of this case lies in the presence of massive gastric dilatation secondary to duodenal obstruction. Acute gastric dilatation increases intragastric pressure and may compromise gastric wall perfusion through elevated mural tension and vascular insufficiency. If unrecognized, this process can progress to mucosal ischemia, necrosis, perforation, severe dehydration, metabolic alkalosis, and shock. In the present patient, the stomach was markedly dilated and extended into the pelvis, yet he remained hemodynamically stable and did not develop clinical evidence of vascular collapse, ischemia, or perforation. Nevertheless, the degree of gastric dilatation was clinically meaningful, as downward displacement and distension of the stomach may further increase traction and pressure at the level of the duodenum, thereby aggravating the obstructive mechanism and worsening SMAS-related symptoms.
Management of SMAS is typically individualized and should proceed in a stepwise manner. Initial treatment is conservative in hemodynamically stable patients without evidence of perforation, ischemia, or complete persistent obstruction. Conservative management aims to relieve acute obstruction while restoring the retroperitoneal and mesenteric fat pad that normally protects the duodenum from vascular compression. Recommended measures include nasogastric decompression, correction of fluid and electrolyte disturbances, nutritional rehabilitation, frequent small meals, positional therapy, and enteral feeding when oral intake is insufficient.8 In selected cases, nasojejunal feeding or parenteral nutrition may be necessary to achieve adequate caloric intake and weight restoration. The rationale of conservative treatment is not merely symptomatic relief but reversal of the underlying anatomical predisposition through nutritional recovery and expansion of the aortomesenteric space.
Surgical intervention should be considered when conservative therapy fails, when symptoms recur despite adequate nutritional rehabilitation, or when patients are unable to maintain sufficient oral or enteral intake.5,9 Surgical options include Strong’s procedure, gastrojejunostomy, and duodenojejunostomy. Strong’s procedure involves mobilization of the duodenum by division of the ligament of Treitz, allowing the duodenum to fall away from the aortomesenteric angle; however, its efficacy may be limited when fixed vascular compression persists. Gastrojejunostomy can decompress the stomach but does not directly address duodenal obstruction and may leave patients vulnerable to persistent duodenal stasis. By contrast, duodenojejunostomy directly bypasses the compressed third portion of the duodenum and is increasingly favored, particularly when performed laparoscopically in appropriately selected patients.9 Recent pediatric experience with laparoscopic duodenojejunostomy suggests that this approach can be safe and clinically effective in refractory SMAS, although recovery may be complicated by coexisting gastrointestinal, psychiatric, or connective tissue disorders.10
In the present patient, both clinical and radiological findings improved substantially after nasogastric decompression, allowing surgical intervention to be avoided during the acute phase. This favorable initial response supports the appropriateness of conservative management in stable pediatric patients, even in the presence of severe gastric dilatation, provided that close monitoring is ensured. However, the absence of meaningful weight gain during follow-up indicates that acute decompression alone did not fully correct the chronic nutritional and anatomical substrate of SMAS. This point is central to the long-term management of the patient: symptomatic improvement should not be equated with definitive resolution unless nutritional rehabilitation, weight gain, and sustained clinical stability are achieved. Continued dietary support, reassessment of growth parameters, and surveillance for recurrent vomiting, postprandial fullness, or gastric distension are therefore essential. Surgical reassessment should be pursued promptly if symptoms recur or if adequate nutritional recovery cannot be achieved.
This case is important because it illustrates an uncommon but clinically significant cause of severe gastric outlet-type obstruction in adolescence. While common gastrointestinal disorders such as acute gastroenteritis or viral illness frequently present with vomiting and abdominal pain, rare anatomical conditions such as SMAS should remain in the differential diagnosis when symptoms are recurrent, severe, postprandial, or refractory to standard therapy.11 The case also highlights the dual nature of SMAS management: conservative treatment may be effective and should be attempted first in stable patients, but failure of nutritional recovery or recurrence of obstructive symptoms should lower the threshold for surgical evaluation. Early recognition, appropriate imaging, prompt decompression, and structured follow-up are therefore essential to prevent recurrent morbidity and potentially serious complications.
Conclusion
SMAS should be considered in adolescents presenting with persistent or recurrent postprandial vomiting, abdominal pain, early satiety, and marked gastric distension, particularly when symptoms are refractory to standard medical therapy and occur in the setting of an underweight or cachectic body habitus. This case highlights that SMAS may develop not only after rapid weight loss but also in patients with long-standing low mesenteric fat reserves. Early recognition is essential because delayed diagnosis can lead to severe gastric dilatation and potentially serious complications. In hemodynamically stable patients, initial conservative management with gastric decompression, correction of fluid and electrolyte disturbances, and structured nutritional rehabilitation remains appropriate. However, clinical improvement after decompression should not be regarded as definitive resolution unless accompanied by sustained nutritional recovery and absence of recurrent obstructive symptoms. Close follow-up is therefore mandatory, and surgical evaluation should be pursued when conservative treatment fails, symptoms recur, or adequate weight gain cannot be achieved.
Data Sharing Statement
No data were generated in this study.
Patient Consent
Written informed consent for publication of this case report and the accompanying images was obtained from the patient’s parent/legal guardian. Institutional review board approval was not required for this single-patient case report in accordance with local institutional policy.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors for its design or conduction.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Strong EK. Mechanics of arteriomesenteric duodenal obstruction and direct surgical attack upon etiology. Ann Surg. 1958;148:725–7. doi:10.1097/00000658-195811000-00001
2. Singal R, Sahu PK, Goyal SL, et al. Superior mesenteric artery syndrome: a case report. North Am J Med Sci. 2010;2:392e394.
3. Mandarry M, Zhao L, Zhang C, Wei Z. A comprehensive review of superior mesenteric artery syndrome. EurSurg. 2010;42:229–236.
4. Unal B, Aktaş A, Kemal G, et al. Superior mesenteric artery syndrome: CT and ultrasonography findings. Diagn Interv Radiol. 2005;11:90–95.
5. Merrett ND, Wilson RB, Cosman P, Biankin AV. Superior mesenteric artery syndrome: diagnosis and treatment strategies. J Gastrointest Surg. 2009;13:287–292. doi:10.1007/s11605-008-0695-4
6. Zhang T, Luo W, Jiang M. Analysis of superior mesenteric artery syndrome in children: a 10-year experience. Asian J Surg. 2025. doi:10.1016/j.asjsur.2025.10.068
7. Reynolds EW, Kinnard TB, Kriss VM, Perman JA. Superior mesenteric artery syndrome: an uncommon cause of feeding intolerance in infancy. J Pediatr Gastroenterol Nutr. 2008;46:92–95. doi:10.1097/01.mpg.0000304461.15047.c9
8. Ahmed AR, Taylor I. Taylor I: Superior mesenteric artery syndrome. Postgrad Med J. 1997;73(866):776–778. doi:10.1136/pgmj.73.866.776
9. Gustafsson L, Falk A, Lukes PJ, Gamklou R. Diagnosis and treatment of superior mesenteric artery syndrome. Br J Surg. 1984;71:499–501. doi:10.1002/bjs.1800710706
10. Mauney CA, Florissi I, Etchill EW, Garcia AV. Laparoscopic duodenojejunostomy for the treatment of pediatric superior mesenteric artery syndrome: a case series. J Pediatr Surg Open. 2023;4:100065. doi:10.1016/j.yjpso.2023.100065
11. Pickering LK, Snyder JD. Gastroenteritis. In: Berhman RE, Kliegman RM, Jenson HB, editors. Nelson’s Textbook of Pediatrics.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.