Back to Journals » Clinical Optometry » Volume 18
Superficial Keratectomy with Cryopreserved Amniotic Membrane for Ocular Surface Optimization in Patients with Epithelial Basement Membrane Dystrophy
Authors Kimmell SW
Received 11 December 2025
Accepted for publication 27 February 2026
Published 12 March 2026 Volume 2026:18 588116
DOI https://doi.org/10.2147/OPTO.S588116
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Chris Lievens
S Wade Kimmell
Department of Optometry, Eye Surgeons of Indiana, Lafayette, IN, USA
Correspondence: S Wade Kimmell, Optometry, Eye Surgeons of Indiana, 1400 Teal Road Ste 8, Lafayette, IN, 47905, USA, Tel +1-765-477-2020, Fax +1+765-477-8200, Email [email protected]
Purpose: Epithelial Basement Membrane Dystrophy (EBMD)-induced irregular astigmatism can lead to unreliable biometry and suboptimal refractive outcomes in cataract surgery patients. Herein, we assessed the use of superficial keratectomy followed by placement of cryopreserved amniotic membrane (cAM) to improve the ocular surface.
Methods: This was a single-center, retrospective study of consecutive patients with EBMD that underwent superficial keratectomy with adjunctive treatment with cAM between November 2022 and March 2025. Time to complete epithelialization, visual acuity (LogMAR), higher order aberration Root Mean Square (HOA RMS), cylinder power, and IOL biometry were assessed up to two months post-treatment.
Results: A total of 27 eyes of 21 patients with EBMD were included in the study and received cAM for a mean of 3.0 ± 0.4 days. Complete re-epithelialization was noted in an average 7.0 ± 4.7 days, with 96.3% (26/27) of eyes achieved epithelialization within 10 days. At the two month follow up, LogMAR VA slightly improved from 0.34 ± 0.21 to 0.31 ± 0.23 (p=0.42). HOA RMS significantly improved from 0.68 ± 0.53 μm to 0.42 ± 0.23 μm (p=0.006), and cylinder power significantly changed from 1.38 ± 0.75 D to 1.09 ± 0.71 D (p=0.022).
Conclusion: Superficial keratectomy with cAM led to complete re-epithelialization in the majority (96.3%) of cases within 10 days, which was associated with a significant change in HOA RMS, cylinder power and IOL SE. This treatment may be considered in patients prior to cataract surgery to return the cornea to healthy state and change the biometry input for IOL selection.
Keywords: amniotic membrane, anterior basement membrane dystrophy, cataract surgery, cryopreservation, debridement, epithelial basement membrane dystrophy, keratectomy, ocular surface
Introduction
Epithelial basement membrane dystrophy (EBMD) is the most common anterior corneal dystrophy and occurs in up to 15% of the general population and 7.5% of patients presenting for cataract evaluation.1,2 Histologically, EBMD is characterized by an abnormal basement membrane that extends into the epithelium and irregular subepithelial accumulation of fibrillo-granular material that results from a dysfunction in the basal epithelial cells.3 Under slit-lamp examination, this presents as fingerprint lines, map-like configurations, epithelial microcysts or dots, and bleb patterns. When corneal irregularities are present in the visual axis, EBMD can induce irregular astigmatism, higher order aberrations (HOAs), and visual disturbances. This is particularly problematic for patients presenting for cataract surgery, as these corneal distortions can affect biometry measurements and can cause significant post-operative refractive error if untreated.4
Traditional first line treatments for more mild cases of EBMD include topical lubrication, hypertonic saline, and bandage contact lenses. For more severe cases as well as those presenting for cataract surgery, superficial keratectomy or phototherapeutic keratectomy (PTK) is often warranted to remove the irregular epithelium and smooth the corneal surface. While these procedures may help alleviate symptoms,5 they do not directly address the underlying healing process or ensure proper restorative healing, including proper reattachment of the epithelium to the basement membrane. Furthermore, removal of the epithelium in these patients can be accompanied by delayed epithelialization and subepithelial haze, the latter of which occurs in approximately 25% of patients post-debridement.6,7 Thus, adjunctive treatments that promote regenerative healing may help to expedite epithelialization, reduce the risk of post-operative haze, and help to restore a smooth corneal surface.
Amniotic membrane (AM) possesses anti-inflammatory and anti-scarring properties and has been clinically used in ophthalmology for a variety of ocular surface conditions.8 When placed on the ocular surface, AM acts as a biological bandage that protects damaged tissue and promotes corneal wound healing.9–11 In particular, AM can facilitate migration of epithelial cells and re-establish normal extracellular matrices and adhesion complexes between the epithelium and the basement membrane, making it particularly beneficial following debridement.8 This is supported by several studies, which have found that treatment with cryopreserved amniotic membrane (cAM) following superficial keratectomy results in expedited re-epithelialization compared to bandage contact lens.12,13 Furthermore, treatment with cAM resulted in greater changes in IOL power (1.56 D vs 0.95 D) and mean keratometry values (1.1 D vs 0.7 D) compared to bandage contact lens,13 suggesting that cAM may be beneficial in stabilizing the ocular surface prior to cataract surgery. Thus, this study sought to expand upon these findings by evaluating changes in topography, including HOAs, following treatment with superficial keratectomy and cAM in patients with EBMD.
Methods
Study Design
This study was reviewed by Sterling Institutional Review Board (Atlanta, GA) and exempt per 45CFR 46.101(b). All study procedures were conducted in accordance with the tenets of the Declaration of Helsinki, and appropriate measures were undertaken to protect the confidentiality of study subjects. The patients in this study were identified retrospectively through a review of medical records, focusing on patients with EBMD that were treated with SK and self-retained cAM (Prokera Slim, BioTissue Holdings Inc, Miami, FL) between November 2022 and March 2025 at a single center. The diagnosis of EBMD was confirmed in all patients under slit-lamp examination by the presence of subepithelial microcysts, map-like changes, dot formations, or fingerprint patterns observed in the corneal epithelium in conjunction with irregular topography. Only those patients without sufficient follow-up data were excluded from this study. Patients’ medical histories and ophthalmic examination results were reviewed, and anonymized data was collected including demographics, prior therapies, concomitant treatments, time to epithelialization, visual acuity, keratometry, biometry, topography, intraocular lens type implanted following cAM treatment (if applicable), and complications and adverse events.
Treatment
All subjects received two drops of proparacaine followed by a third drop approximately 10 minutes later. Diluted 10% povidone-iodine (Betadine; Alcon, Geneva, Switzerland) was applied to the conjunctiva with a swab. Using a lid speculum and spud, the corneal epithelium was debrided 1–2 mm from the limbus 360 degrees in all cases, and the Bowman’s membrane was polished. A tobramycin-soaked cotton tip applicator was used to further polish the Bowman’s membrane. Self-retained cAM (Prokera Slim; BioTissue Holdings Inc, Miami, FL) was thawed at room temperature for several minutes and rinsed with basic saline solution prior to insertion. cAM was then placed into the superior fornix with the patient looking down and then slid under the lower eyelid. Tape was applied over the lid crease to create a temporary tarsorrhaphy, and patients were instructed to leave in place for one day. All patients were instructed to use a custom drop formulation containing prednisolone acetate 1.0%, Moxifloxacin 0.5%, and Nevanac 0.1% one day prior to surgery, which was continued for 20 days post-operatively (TID for one week and then tapered to BID for two weeks). Preservative free artificial tears were also encouraged. Patients returned to the clinic after three days for cAM removal. If healing was not evident upon removal, a second cAM or bandage contact lens was placed depending on the size of defect.
Assessments and Outcomes
Prior to treatment, all patients underwent a thorough preoperative evaluation, which included measurement of best-corrected distance visual acuity (BCVA) to establish baseline visual function as well as corneal topography to quantify the degree of corneal irregularities including HOAs and astigmatism. BCVA was determined using a Snellen chart and a pinhole occluder, and corneal topography was assessed using the Nidek OPD Scan III. A minimum of three images with optimal centering, focus, and continuous Placido disk lines were captured for each eye, and the root mean square (RMS) HOAs and cylinder power in diopters (D) were recorded. RMS is a commonly used metric to quantify the magnitude of wavefront aberrations and is calculated as the square root of the mean of the squares of the distances of all points of the wavefront from the reference plane; thus, RMS HOAs were assessed at a 6-mm pupil to analyze the specific impact that the HOAs have on the overall optical system.
Following placement of cAM, patients returned to the clinic at post-operative day 3 and 10 to evaluate corneal epithelialization, which was confirmed under slit lamp examination using corneal fluorescein staining. All patients returned two months post-cAM treatment for re-evaluation of visual acuity, degree of corneal astigmatism or cylinder power (D), and measurement of RMS HOAs to assess the changes in corneal surface integrity and visual quality.
Patients that were planning to undergo cataract surgery underwent additional biometry examinations at baseline and approximately two months post-treatment to assess both changes in corneal curvature and recommended IOL power. Biometry was assessed using the IOLMaster® 700 (Carl Zeiss Meditec, Jena, Germany), which included flat keratometry (Kmin), steep keratometry (Kmax), mean keratometry (Kmean), and IOL cylinder power recommendations using the Barrett TK Universal II formula. Patients were scheduled for cataract surgery upon stabilization of the ocular surface two to three weeks after the last follow-up visit. All assessments, including topography and biometry, were assessed before and after treatment by the same examiner and devices to minimize variability.
The primary outcome was the time to complete corneal epithelialization in days, which was assessed using corneal fluorescein staining. Secondary outcomes included changes in BCVA, RMS HOAs, keratometry (Kmin, Kmax, and Kmean), cylinder power, and proportion of eyes that were candidates for premium or advanced IOLs. Eyes were deemed candidates of advanced surgery if they demonstrated consistent cylinder power and axis readings across the IOL master and OPD, defined as a difference ≤0.40 D and 40 degrees and RMS HOA ≤ 0.50 µm and angle alpha around 0.35 mm. Complications and adverse events were also assessed.
Statistical Analysis
All statistical analyses were carried out using IBM SPSS version 20.0. Categorical data are reported using percentages and frequencies, and continuous data are reported as means and standard deviations (range). A paired t-test was used to assess continuous repeated measures between time points. If the differences between pairs were not normally distributed, the non-parametric Wilcoxon signed-rank test was used. The independent samples t-test was used to assess continuous variables between groups, and the non-parametric Mann–Whitney U-test was utilized if the assumption of normality was violated. All tests were two-sided, and a p value less than 0.05 was considered statistically significant.
Results
A total of 27 eyes (14 OD, 13 OS) of 21 patients with EBMD met the eligibility criteria and were included in the analysis. The majority of patients were female (70.4%, n=19), and the mean age was 69.8 ± 7.8 years (range: 52–88). Most of the eyes (85.2%) had not been previously treated with other therapies at initial presentation. One patient (2 eyes) was being treated with sodium chloride hypertonicity ophthalmic solution 5% (Muro 128®, Bausch + Lomb) twice daily, one patient had prior treatment with cAM and low level light therapy for meibomian gland dysfunction, and one patient had previously used artificial tears and a sleep mask. The majority of patients (85.3%) also had co-morbidities including dry eye (n=10), cataracts (n=16), hypertension (n=15), Diabetes (n=10), neurotrophic keratopathy (n=2), and stromal haze (n=1).
All eyes were treated with superficial keratectomy followed by placement of cAM for a mean of 3.0 ± 0.4 days (range: 2–4). Three patients received an additional placement of cAM: one patient was treated with a second cAM on post-operative Day 2 for an additional 3 days, Day 3 for an additional 4 days, and a third patient was treated with additional cAM on post-operative Day 15 due to persistent superficial punctate keratopathy. Treatment was uneventful in all cases. Following removal of cAM, a bandage contact lens (BCL) was placed over the cornea of 14 eyes (51.9%) for typically 7 days. One additional patient received ocular surface irrigation with irrigating lid retractor (RinsadaTM; Wildwood, PA) at day of SK.
The mean time to epithelialization was 7.0 ± 4.7 days (range: 3–26), and 26/27 (96.3%) eyes epithelialized within 10 days post-op. One eye with pre-existing neurotrophic keratopathy healed at Day 26. Eyes that received adjunctive BCL post-cAM removal healed significantly slower compared to eyes that received cAM alone (9.2 ± 5.2 days vs 4.5 ± 2.7 days, respectively; p=0.008).
At the two month follow up, LogMAR VA slightly improved from 0.34 ± 0.21 to 0.31 ± 0.23 (p=0.42). VA improved in 13 eyes (48.1%) by a mean of 2.2 ± 1.2 lines (range: 0.8–4.5), stayed the same in 4 eyes (14.8%), and worsened by 1.9 ± 0.8 lines (range: 0.8–3.0) in 10 eyes (37.0%). Change in logMAR VA was significantly correlated with baseline logMAR VA (t=0.37, p=0.010), and eyes that showed no change or worsened VA post-cAM had significantly better VA at baseline (logMAR 0.25 ± 0.24) compared to eyes that improved post-cAM (logMAR 0.43 ± 0.13, p=0.007). Higher order aberrations significantly improved from 0.68 ± 0.53 μm to 0.42 ± 0.23 μm at two months (p=0.006). HOA RMS improved in 61.9% of eyes by a mean of 0.47 ± 0.45 μm. HOA RMS did not change or minimally worsened by a mean of 0.05 ± 0.03 μm in the remainder of eyes (38.1%). Notably, no eyes worsened by more than 0.1 μm. Cylinder power measured with optical path difference (OPD) technology significantly changed from 1.38 ± 0.75 D to 1.09 ± 0.71 D (p=0.022), with a mean change of 0.58 ± 0.46 D (range: 0.01–1.82). Representative cases are shown in Figures 1–3.
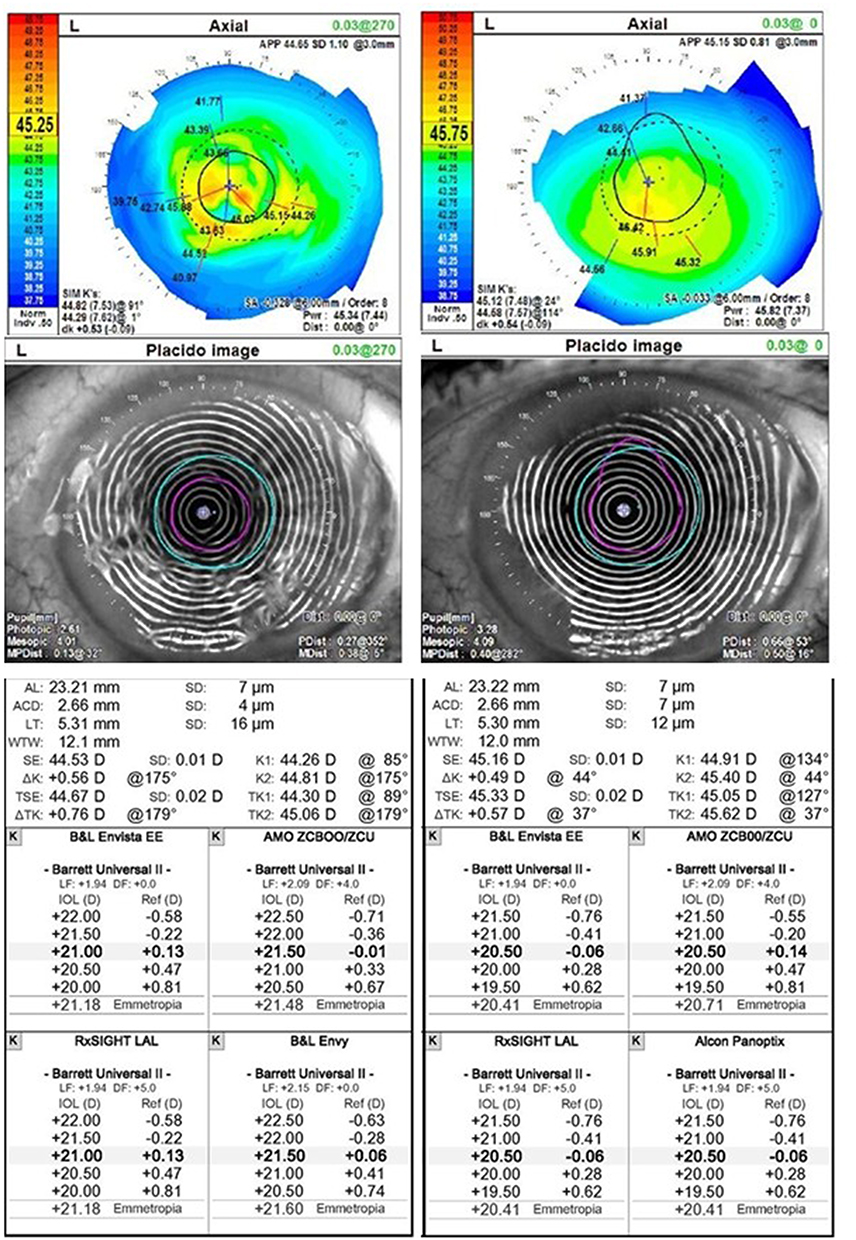 |
Figure 1 Representative Case before and following treatment with cAM. 80-year-old Female presented with EBMD and irregular ocular surface (left column). She was treated with superficial keratectomy and placement of cAM for 3 days. After treatment, complete epithelialization was noted in 10 days. Topography showed smooth ocular surface at 2 months (right column). Visual acuity with correction improved from 20/60 to 20/30. K-values changed from 44.26/44.81 to 44.91/45.40. The refractive error changed from Plano / +1.00 × 27° to –0.25 / +0.75 × 19°. A Toric IOL was implanted with Intelliaxis. |
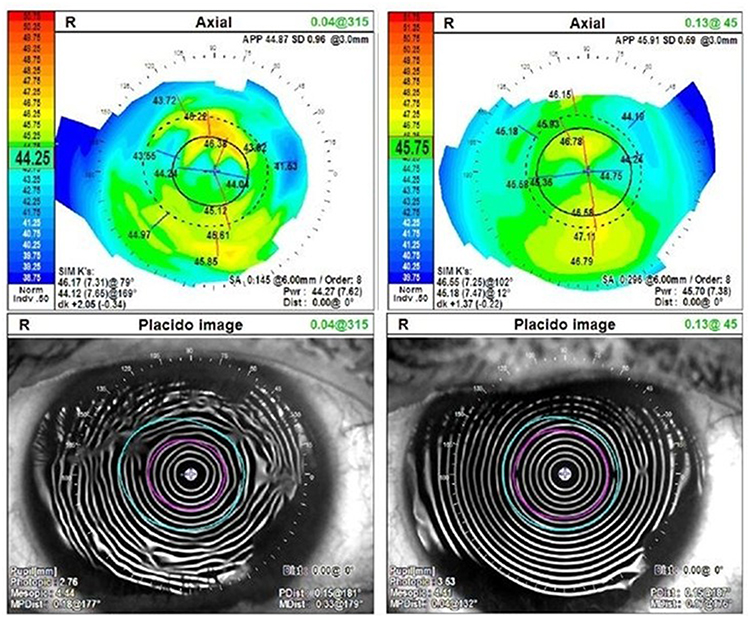 |
Figure 2 Representative Case before and following treatment with cAM. 61-year-old Female presented with EBMD and irregular mires and areas of dropout (left column). Superficial keratectomy was performed and cAM was placed for 3 days, when complete epithelialization was then also noted. RMS changed from 0.82 to 0.52 D. The refractive error changed from −5.75 / +1.75 × 89° to −7.25 / +1.75 × 101°. |
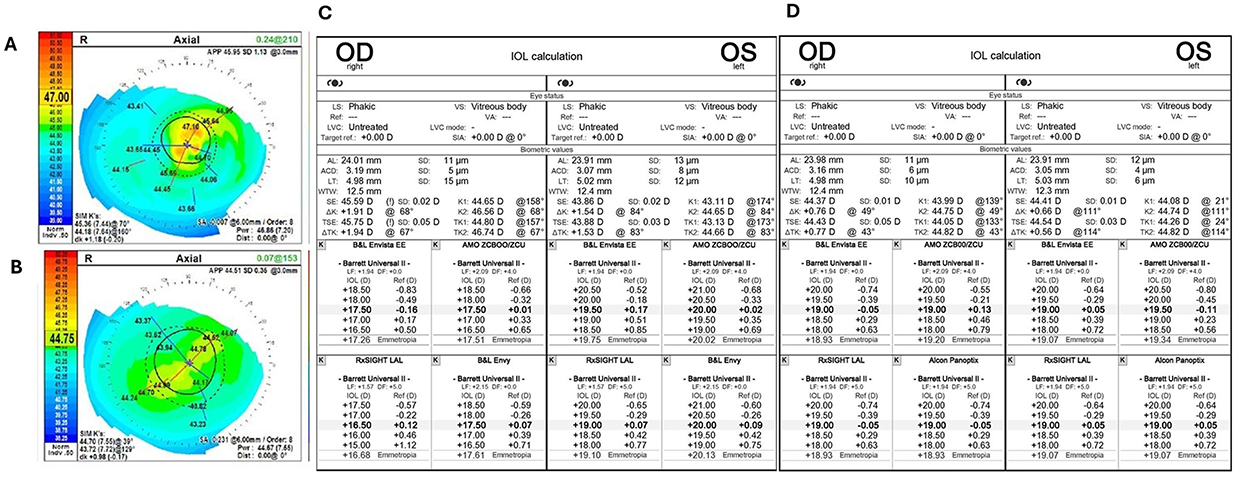 |
Figure 3 Representative Case before and following treatment with cAM. 67-year-old Male presented with bilateral EBMD and uncertain keratometry/ topographic readings OD (A). Superficial keratectomy was performed and cAM was placed for 3 days. Complete epithelialization was noted in 3 days OD and 6 days OS. Topography was notably improved OD (B). Keratometry values changed from 44.65 / 46.56 (C) to 43.99 / 44.75 OD (D) and 43.11 / 44.65 to 44.08 / 44.74 OS. |
A total of 20 eyes (74.1%) were pre-cataract surgery patients and had repeat biometry measurements 2 months post-cAM. IOL SE (K values) significantly changed from 44.01 ± 1.07 D to 44.37 ± 1.20 D two months post-treatment (p=0.006), with a mean change of 0.65 D ± 0.26 D (range: 0.35–1.32) post-treatment. Kmin values significantly changed from 43.36 ± 1.03 D to 43.84 ± 1.09 D (p=0.007), and Kmax values changed from 44.70 ± 1.24 D to 44.81 ± 1.34 D although not significantly (p=0.60). Average change in Kmin and Kmax values was 0.70 ± 0.47 D (range: 0.03–2.05) and 0.69 ± 0.62 D (range: 0.05–2.64), respectively. Cylinder power using the IOL master improved from 1.33 ± 0.75 D to 1.11 ± 0.68 D although not significantly (p=0.16). Mean change in IOL cylinder power was 0.70 ± 0.44 D, with 63.2% of eyes having a change greater than ±0.5 D.
For the pre-cataract population, higher order aberrations significantly improved from 0.65 ± 0.54 μm to 0.42 ± 0.23 μm at two months (p=0.013). HOA RMS improved in 61.1% of eyes by a mean of 0.40 ± 0.36 μm. HOA RMS did not change or minimally worsened by a mean of 0.05 ± 0.03 μm in the remainder of eyes (38.9%). The presence of total corneal HOAs greater than 0.3 μm before surgery is associated with suboptimal subjective patient perceptions postoperatively. Using this cutoff as a measure of probability for success with a multifocal IOL, 5/20 (25%) patients before and 7/20 (35%) patients after cAM would be considered candidates for a multifocal IOL —a 40% increase in the pool of candidates for advanced technology. Unfortunately, those seven patients with HOA < 0.3 were not multifocal candidates as they also had chord alpha above 0.35 mm. Following cAM treatment, 12 eyes ultimately received a Toric IOL with LENSAR IntelliAxis, 2 eyes received a light adjustable lens, and 5 eyes received a monofocal lens. One patient deferred cataract surgery due to significant visual improvement post-treatment.
Discussion
EBMD and RCE are often associated with abnormal adhesion complexes that anchor the corneal epithelium and the basement membrane, which may lead to epithelial sloughing and associated pain, light sensitivity, and blurred vision. Due to the disruption and damage of tissue architecture, conservative treatments such as topical lubricants, ointments or hyperosmotic solutions typically do not address the underlying issues that prevent normal corneal function. Importantly, the irregular epithelial surface and underlying basement membrane abnormalities can induce significant corneal topographic distortion and unreliable keratometry readings. Such irregularities may lead to errors in intraocular lens (IOL) power calculations, ultimately affecting postoperative refractive outcomes. Rather, mechanical removal via debridement or keratectomy of the abnormal tissue is often warranted. Although these interventions are effective to remove the pathological tissue, they are associated with potential risk of delayed epithelialization, haze or scar formation. Debridement of a loosely adherent corneal epithelium has also been shown to have an 18% recurrence rate.5
CAM mechanistically protects the cornea as mechanical barrier while simultaneously enabling regenerative wound healing with minimal scarring and optimal visual recovery.14 In one study of 10 patients (20 eyes) with bilateral EBMD, treatment with CAM following superficial keratectomy resulted in faster re-epithelialization of corneal wounds than BCL (70% vs 20% at Day 5, respectively).12 Furthermore, the CAM group had a significantly lower incidence of residual haze/scarring at Day 30 compared with the BCL group (20% vs 100%) and a net gain of 2 lines in BCVA compared with a net loss of 2 lines in the BCL group at Day 30. Furthermore, Yeu et al13 also found significantly expedited epithelialization following treatment with CAM compared to BCL in 19 patients.
In our study, mean time to epithelialization was 7.0 ± 4.7 days (range: 3–26), and 26/27 (96.3%) eyes epithelialized within 10 days after application of the cAM. One eye healed at Day 26, however they were known to have pre-existing neurotrophic keratopathy which has been associated with impaired re-epithelialization.15 Previous studies have shown debridement with AM significantly improved time to complete epithelialization16 and prevented recurrence17 compared to debridement with BCL. Previous studies evaluating AM for EBMD/ RCE showed a time to complete healing within 4 to 7 days,16,18–20 which compares similarly to our results.
Treatment of EBMD with superficial keratectomy followed by cAM placement led to a significant improvement in corneal regularity. Higher-order aberrations (HOAs) were significantly reduced (0.71 ± 0.56 μm to 0.43 ± 0.23 μm; p = 0.006), and cylinder power decreased by an average of 0.58 ± 0.46 D, suggesting a more stable and uniform corneal surface. By restoring epithelial integrity and reducing surface irregularity, this approach can help provide accurate biometry used for IOL power calculations. Importantly, normalization of the corneal surface also increased the number of patients eligible for advanced technology or premium IOLs, with a 40% rise in those meeting optical quality criteria based on HOA rms for multifocal lens implantation. These findings suggest that pre-cataract optimization of the ocular surface with superficial keratectomy and cAM may broaden the pool of candidates who can achieve optimal visual outcomes with premium IOL technologies. However, such considerations should be viewed in light of potential recurrence in particular with patients with known risk factors. Further randomized studies are needed to confirm if similar increase in meeting optical quality criteria are noted in patients undergoing superficial keratectomy alone compared to superficial keratectomy and cAM.
Paired box homeotic gene 6 (Pax6) is a highly conserved transcription factor that is essential for eye development and plays a pivotal role in supporting the self‐renewal of limbal epithelial stem cells21 and maintaining the normal corneal epithelial phenotype.22,23 Pax6 haploinsufficiency causes limbal stem cell deficiency, and down-regulation of Pax6 is associated with abnormal differentiation of corneal epithelial cells in severe ocular surface diseases such as Stevens-Johnson syndrome (SJS), chemical burn, and recurrent pterygium.22 More recently, Stachon et al demonstrated that PAX6 expression is also decreased in the corneal epithelium in patients with EBMD,23 suggesting that downregulation of PAX6 may play a key role in the pathophysiology of EBMD. HC‐HA/PTX3, a unique matrix purified from amniotic membrane (AM), is capable of reverting senescent LNC to nuclear Pax6+ neural crest progenitors as demonstrated by a significant upregulation of Pax6 transcript levels and nuclear Pax6 immunofluorescence staining.24 This suggests that cryopreserved AM, which contains HC-HA/PTX3, may be able support these stem cells to aid in the regeneration of a normal corneal epithelium.
Despite these findings, it is important to note limitations in the present study. First, the lack of a comparative control group limits our ability to definitively state that the provided treatment is superior to superficial keratectomy alone. Some subjects also received concurrent placement of another cAM (n=3) or BCL (n=14). Furthermore, the study design was retrospective which introduces potential selection bias and relies on the consistency of historical medical records. However, as noted, our results related to re-epithelialization rate are consistent with prior controlled studies that have been evaluated in the EBMD population.12,13 Overall, our data adds a real-world perspective on the integration of cAM into standard surgical workflows for EBMD management. Future multi-center, randomized, controlled trials are warranted to further validate these findings.
Conclusions
This retrospective study of 27 eyes of 21 patients with EBMD suggests that superficial keratectomy followed by cAM placement is a generally safe and effective treatment modality, leading to rapid epithelial healing and significant improvements in corneal optics. A total of 96.3% of eyes achieved epithelialization within 10 days, with a mean time of 7.0 ± 4.7 days. This was associated with a significant improvement in HOA RMS from 0.68 ± 0.53 μm to 0.42 ± 0.23 μm and cylinder power significantly changed from 1.38 ± 0.75 D to 1.09 ± 0.71 D. For the pre-cataract surgery patients, the treatment resulted in a significant change in IOL SE (44.01 ± 1.07 D to 44.37 ± 1.20 D) and K-minimum values (43.36 ± 1.03 D to 43.84 ± 1.09 D), suggesting the potential role in stabilizing and regularizing the corneal surface prior to IOL calculation. While the retrospective nature of this study and the absence of a parallel control group are noted, these elements reflect the real-world clinical setting in which these interventions were evaluated.
Funding
An educational grant for this investigator-initiated study was awarded by BioTissue Holdings to cover the pass-through direct costs associated with the article processing charge and institutional review board.
Disclosure
The author reports speaker fees from BioTissue, outside the submitted work.
References
1. Miller DD, Hasan SA, Simmons NL, Stewart MW. Recurrent corneal erosion: a comprehensive review. Clin Ophthalmol. 2019;13:325–9. doi:10.2147/OPTH.S157430
2. Gupta PK, Drinkwater OJ, VanDusen KW, Brissette AR, Starr CE. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44:1090–1096. doi:10.1016/j.jcrs.2018.06.026
3. Waring GO, Rodrigues MM, Laibson PR. Corneal dystrophies. I. dystrophies of the epithelium, Bowman’s layer and stroma. Survey Ophthalmol. 1978;23:71–122. doi:10.1016/0039-6257(78)90090-5
4. Ho VW, Stanojcic N, O’Brart NA, O’Brart DP. Refractive surprise after routine cataract surgery with multifocal IOLs attributable to corneal epithelial basement membrane dystrophy. J Cataract Refract Surg. 2019;45:685–689. doi:10.1016/j.jcrs.2018.12.029
5. McGrath LA, Lee GA. Corneal epithelial debridement for diagnosis and therapy of ocular surface disease. Clin Exp Optom. 2015;98:155–159. doi:10.1111/cxo.12213
6. Sayegh RR, Kouyoumjian PB, Vedula GG, Nottage JM, Nirankari VS. Cocaine-assisted epithelial debridement for the treatment of anterior basement membrane dystrophy. Cornea. 2013;32:889–892. doi:10.1097/ICO.0b013e318288ad4d
7. Itty S, Hamilton SS, Baratz KH, Diehl NN, Maguire LJ. Outcomes of epithelial debridement for anterior basement membrane dystrophy. Am J Ophthalmol. 2007;144:217–221. doi:10.1016/j.ajo.2007.04.024
8. Tighe S, Mead OG, Lee A, Tseng SCG. Basic science review of birth tissue uses in ophthalmology. Taiwan J Ophthalmol. 2020;10:3–12. doi:10.4103/tjo.tjo_4_20
9. Tseng SC. HC-HA/PTX3 purified from amniotic membrane as novel regenerative matrix: insight into relationship between inflammation and regeneration. Invest Ophthalmol Visual Sci. 2016;57:ORSFh1–8. doi:10.1167/iovs.15-17637
10. FDA. Request for designation: amniotic membrane for ocular surface reconstruction. Available from: https://www.fda.gov/downloads/CombinationProducts/JurisdictionalInformation/RFDJurisdictionalDecisions/RedactedDecisionLetters/UCM113701.pdf20012001.
11. Röck T, Bartz-Schmidt KU, Landenberger J, Bramkamp M, Röck D. Amniotic membrane transplantation in reconstructive and regenerative ophthalmology. Ann Transplant. 2018;23:160–165. doi:10.12659/AOT.906856
12. Desai NR. A comparison of cryopreserved amniotic membrane and bandage contact lens in their ability to provide high-quality healing after superficial keratectomy. Rev Ophthalmol. 2014.
13. Yeu E, Hashem O, Sheha H. Treatment of epithelial basement membrane dystrophy to optimize the ocular surface prior to cataract surgery. Clin Ophthalmol. 2022;16:785. doi:10.2147/OPTH.S356421
14. Sheha H, Tighe S, Fortes B. Self-retained amniotic membrane for epithelial basement membrane dystrophy.
15. Cheung AY, Holland EJ, Lee WB. Neurotrophic keratopathy: an updated understanding. Ocular Surf. 2023;30:129–138. doi:10.1016/j.jtos.2023.09.001
16. Yeu E, Hashem O, Sheha H. Treatment of epithelial basement membrane dystrophy to optimize the ocular surface prior to cataract surgery. Clin Ophthalmol. 2022;16:785–795.
17. Hauswirth SG. The effect of debridement and amnion tissue on vision in patients with anterior basement membrane dystrophy: a short case series. Invest Ophthalmol Visual Sci. 2015;56:5641.
18. Huang YSH, Tseng SCG. Self-retained amniotic membrane for recurrent corneal erosion. Clin Exp Ophthalmol. 2013;4:1–4.
19. Cheng AMS, Tseng SCG. Self-Retained amniotic membrane combined with antiviral therapy for herpetic epithelial keratitis. Cornea. 2017;36:1383–1386. doi:10.1097/ICO.0000000000001316
20. Sheha H, Tighe S, Cheng AMS, Tseng SCG. A stepping stone in treating dendritic keratitis. Am J Ophthalmol Case Rep. 2017;7:55–58. doi:10.1016/j.ajoc.2017.06.002
21. Chen SY, Cheng AMS, Zhang Y, et al. Pax 6 controls neural crest potential of limbal niche cells to support self-renewal of limbal epithelial stem cells. Sci Rep. 2019;9:9763. doi:10.1038/s41598-019-45100-7
22. Li W, Chen YT, Hayashida Y, et al. Down-regulation of Pax6 is associated with abnormal differentiation of corneal epithelial cells in severe ocular surface diseases. J Pathol. 2008;214:114–122. doi:10.1002/path.2256
23. Stachon T, Fries FN, Li Z, et al. Decreased PAX6 and DSG1 protein expression in corneal epithelium of patients with epithelial basal membrane dystrophy, salzmann nodular degeneration, and pterygium. J Clin Med. 2025;14:1456. doi:10.3390/jcm14051456
24. Chen SY, Zhu Y, Zhang Y, Hsu D, Tseng SCG. HC-HA/PTX3 from amniotic membrane reverts senescent limbal niche cells to Pax6+ neural crest progenitors to support limbal epithelial progenitors. Stem Cells. 2021;39:280–295. doi:10.1002/stem.3323
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Dry Eye Disease Among Individuals Scheduled for Cataract Surgery in a Norwegian Cataract Clinic
Graae Jensen P, Gundersen M, Nilsen C, Gundersen KG, Potvin R, Gazerani P, Chen X, Utheim TP, Utheim ØA
Clinical Ophthalmology 2023, 17:1233-1243
Published Date: 27 April 2023
Therapeutic Outcomes of Shelf-Stable, Cryopreserved Amniotic Membrane in Recalcitrant Keratopathy
Stevanovic M, Ciarmiello G, Eden R, Schultze R
Clinical Ophthalmology 2025, 19:4545-4550
Published Date: 9 December 2025