Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 13
Sun Awareness and Sun Protection Practices
Authors Sultana N ![]()
Received 1 June 2020
Accepted for publication 7 August 2020
Published 29 September 2020 Volume 2020:13 Pages 717—730
DOI https://doi.org/10.2147/CCID.S265477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Nahid Sultana
Department of Computer Science, College of Computer Science and Information Technology, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Nahid Sultana Department of Computer Science
College of Computer Science and Information Technology, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Tel +966 13 333 2029
Email [email protected]
Background: The incidence of skin cancer has increased over the past few years, owing to excessive exposure to ultraviolet (UV) radiation. Over the past decade, protection against solar radiation has been highly encouraged in numerous public health education campaigns. The adopted sun protection practices include avoiding exposure to the sun, using protective clothing, and applying sunscreen. The aim of this paper was to analyze the awareness and attitudes towards sun protection practices in some regions of the Arabian Peninsula.
Objective: The main objective of this study is to estimate the level of sun protection practices and determine the factors that have a significant impact on the level of adoption of sun protection practices by residents in the Arabian Peninsula.
Methods: A 35-question self‐reporting online questionnaire to evaluate the sun protection measures adopted by the residents was distributed in the Kingdom of Saudi Arabia and Kingdom of Bahrain. The survey was conducted from January 2018 to May 2019, and a total 830 responses were collected for analysis. The data were analyzed using the statistical software SPSS. The chi-squared test and Spearman’s correlation were performed to determine the association of the sun protection level with factors concerning the socio-demographic characteristics, sun sensitivity, health-conscious lifestyle, adopted sun protection measures, and general awareness about the UV index, skin cancer, and vitamin D. Logistic regression classification was applied in developing the empirical model to predict the sun protection level of the residents.
Results: Based on the analysis, only 34% of the total 830 respondents use sunscreen and most of the sunscreen users are female. The three most popular sun protection practices are: 1) avoiding exposure to the sun during peak hours, 2) using protective clothing, and 3) using sunglasses. The results indicate that 22% of respondents use a low level of sun protection, 53% use a medium level of protection, while 25% of respondents use a high level of sun protection. Many of the respondents understand that exposure to the sun can cause skin cancer and skin aging, while 54% of the respondents still believe that a suntan can be healthy if sunburn is avoided. Thirty percent of the participants of this study are aware of the UV index, and only 20% of all respondents know the correct meaning of the UV index. The overall predictive accuracy of the constructed logistic regression model is 67%. Based on the results of the logistic regression model, the five most significant factors of the sun protection level are: 1) perception that the sun can cause skin aging, or not, 2) age, 3) awareness of the dangerous effects of sun exposure, 4) income with respect to expenses, and 5) taking the UV index into consideration during exposure to the sun.
Conclusion: Most of the respondents are aware about sun protection. However, the sun protection level of the residents is still inadequate. An efficient strategy of increasing the awareness of the effective use of sun protection systems must be established based on the significant factors to prevent skin cancer.
Keywords: sun protection, sunscreen, UV index, skin cancer, vitamin D
Introduction
Frequent and prolonged exposure to ultraviolet (UV) rays over many years is the leading cause of skin cancer.1–7 The increased incidence of skin cancer over the past decade is strongly related to the growing attraction to outdoor activities and recreational sun exposure. Increased exposure to sunlight is also the leading cause of detrimental effects on the skin, eye, and immune system. Four out of five cases of skin cancer can be prevented, and UV damage can be minimized by limiting exposure to the sun.8,9 Protection afforded by shade, protective clothing, hats, and the proper use of sunscreen are important aspects for the essential protection against UV rays to reduce harmful solar radiation effects. On the other hand, a lack of exposure to sunlight is widely identified as the main cause of vitamin D deficiency.10,11 Vitamin D deficiency is linked to several diseases, including various types of cancer, coronary heart disease, type 1 and 2 diabetes, multiple sclerosis, rheumatoid arthritis, hypertension, Alzheimer’s disease, and mental health problems.10,12-15 Hence, effective protection against solar radiation and enhancing awareness about the harmful effects of too much or too little exposure to the sun should be among the leading preventive healthcare strategies.
A number of studies have been conducted in several countries on the awareness of the effects of solar radiation and the practices in place to protect people from its effects.2,16-21 Scerri et al evaluated sun protection practices among the Maltese people and assessed their level of knowledge regarding the harmful effects of solar radiation on the skin.2 Devos et al explored the prevalence and predictors of sunscreen use and skin protection practices among Belgian beachgoers.16 Kunene et al analyzed the practices of the use of sun protection equipment by children living in a rural area, and their acceptability to black African mothers.19 Purdue investigated the predictors of different behavior of Canadian adults in protecting themselves from solar radiation.22 Halpern and Kopp studied the awareness, knowledge, and attitudes among the general public from seven countries (the UK, Italy, Germany, Spain, France, the USA, and Australia) regarding non-melanoma skin cancer and actinic keratosis.23 However, the sun protection practices of people in the countries of the Arabian Peninsula have been rarely studied.
The countries in the Arabian Peninsula are Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates, and Yemen. The climate of the Arabian Peninsula is characterized by its long, hot, dry summer and short winter with occasional rainfall. In the summer, the maximum temperature in some countries can reach 50°C.24 Countries in the Arabian Peninsula have reported the highest UV index scores in the world.25 Hence, protection against UV radiation is essential for people in the countries of the Arabian Peninsula. Thus, analysis of the sun protection practices of the people in this region is an important area of empirical research in dermatology and pharmacology. In this study, the sun protection practices of residents in Saudi Arabia and Bahrain were analyzed. Saudi Arabia occupies the largest area of the peninsula, and the island nation of Bahrain lies off the east coast of the peninsula.
Aim
One of the objectives of this study was to investigate the most popular sun protection practices in the studied population and estimate their sun protection level. Public awareness among the studied residents about the harmful effects of solar radiation on the skin was also investigated. The factors that have a significant impact on the level of sun protection practices were also determined.
Methods
A quantitative methodology using a simple random survey was employed to achieve the objectives of this study.
Survey Design and Study Area
A variety of questions was developed to evaluate numerous variables to gain a better understanding of the factors that influence the sun protection practices of the residents. The online survey form presented to the respondents contained a cover letter with a brief description of the study theme. To minimize the possible response bias, the cover letter drew attention to the following in the instructions: “there are no correct or incorrect answers; simply the views of the respondents matter”. Moreover, the cover letter clearly mentioned that the confidentiality of the survey would be maintained.
The survey primarily contained six sections: 1) socio-demographic questions; 2) questions to ascertain the sun protective practices adopted by the respondents; 3) questions to ascertain the sun sensitivity and health status of the respondents; 4) questions designed to determine the health-consciousness and the adoption of safety measures in the day-to-day life of the participants; 5) questions to determine the knowledge and awareness about personal sun exposure, UV index, and vitamin D of the participants; and 6) questions to assess the general knowledge of the respondents concerning the harmful effects of the sun on the skin. Questions in Parts 1–6 are shown in Tables 1–6, respectively. All questions were restricted, and the participants could not submit the questionnaire without fully answering every question.
 |
Table 1 General Characteristics of the Respondents |
 |
Table 2 Sun Protection Practices Adopted by the Respondents |
 |
Table 3 Level of Sun Protection According to Sun Sensitivity and Health Status |
 |
Table 4 Level of Sun Protection According to Health-Conscious Lifestyle and Safety Measures Adopted in Day-to-Day Life |
 |
Table 5 Sun Protection Level According to Awareness About Exposure to Solar Radiation, UV Index, and Vitamin D |
 |
Table 6 Sun Protection Level According to General Knowledge Regarding the Harmful Effects of the Sun on the Skin |
The questionnaire was first pretested with ten randomly selected residents of Dammam city in Saudi Arabia to obtain their reaction and ensure that the survey questions were straightforward and easily understood by the respondents.
The survey was conducted in the Kingdom of Saudi Arabia and the Kingdom of Bahrain from January 2018 to May 2019. The online survey form was distributed among participants via social media, such as Twitter, Facebook, WhatsApp, and Instagram. A total of 830 completed questionnaires were available for analysis, which is larger than the smallest sample size (500) required for a statistical evaluation to characterize the parameters for observational studies with a large population size.8
Statistical Analysis
Data analysis was performed using the statistical software SPSS (version 17). Descriptive statistics were used to analyze the variables concerning socio-demographic characteristics, sun sensitivity, health-conscious lifestyle, sun exposure practices, and respondents’ general awareness about the UV index, skin cancer, and vitamin D. The analyses were presented as percentages for categorical variables, and mean and standard deviation for quantitative variables.
Level of Sun Protection Practices
In this study, the level of adoption of means of sun protection by the respondents was defined based on the six most common sun protection practices (using sunscreen, hats, sunglasses, umbrellas, protective clothing, and trying to avoid exposure to the sun during peak hours).2,17,26,27 The following criteria were used to determine the level of protection: 1) low: respondents using no or one means of protection, 2) medium: respondents using two or three means of protection, and 3) high: respondents using four or more means of protection.
Chi-Squared Test and Spearman’s Correlation
The chi-squared test was used to analyze the association of the level of sun protection of the respondents with various relevant variables. The chi-squared statistic is specified as  , where observed and expected denote the observed value of the relevant variable and the expected value of the relevant variable, respectively. Spearman’s correlation analysis was also used to determine the strength and direction of the relationship between the demographic variables. The correlation was determined to be statistically significant when the p-value was <0.05.
, where observed and expected denote the observed value of the relevant variable and the expected value of the relevant variable, respectively. Spearman’s correlation analysis was also used to determine the strength and direction of the relationship between the demographic variables. The correlation was determined to be statistically significant when the p-value was <0.05.
Logistic Regression Model
Logistic regression is a statistical process for data analysis in which one or more explanatory variables are used to determine a categorical response variable. Binary and multinomial logistic regressions are two types of logistic models. In this study, multinomial logistic regression was used to predict the level of sun protection of the residents in Saudi Arabia and Bahrain. Multinomial logistic regression works in the same manner as binomial logistic regression to predict multiple outcomes. In brief, the log of  is used as the dependent variable, with two categorical outcomes (success/failure). This model can predict the probability of a particular outcome by fitting data to a logit function,
is used as the dependent variable, with two categorical outcomes (success/failure). This model can predict the probability of a particular outcome by fitting data to a logit function, 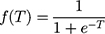 , where
, where  . This function
. This function  increases monotonically from 0 to 1 as
increases monotonically from 0 to 1 as  varies from
varies from  to
to  . The backward stepwise selection method was used to develop the best predictive logistic regression model of the selected variables out of 28 attributes that are considered in this study.
. The backward stepwise selection method was used to develop the best predictive logistic regression model of the selected variables out of 28 attributes that are considered in this study.
Results
Descriptive Statistics
A descriptive analysis of the profiles of the participants is shown in Table 1. The age of the participants ranges from 16 to 69 years, with a mean age of 25 and a standard deviation of 7.8. About 77% of the respondents are female and 23% are male. Sixty five percent of the respondents are Saudi, 15% are Bahraini and the remaining 20% are of other nationalities. Regarding the educational level, 52% of the respondents hold an undergraduate degree, 17% hold a postgraduate degree, 27% have some college education, and only 4% have a high school or lower educational level. The breakdown indicates that the participants have a fairly high level of education. Seventy five percent of the participants are single and 25% are married. Most of the respondents (73%) live with more than four members of the family in the same household, while 27% of the respondents live with four members or fewer in the same household. Regarding income and expenses, 44% of respondents claimed that their income and expenses are about the same, 33% claimed that their income is not enough to meet their expenses, and 24% reported that their income is more than enough to meet their expenses, indicating that most of the respondents are economically stable.
Sun Protection Practices
The sun protection practices adopted by the respondents are shown in Table 2. The results indicate that only 34% of the respondents use sunscreen, although 64% of the respondents think that sunscreen is not harmful to the skin in any way. The sunscreen users were asked about the sun protection factor (SPF) of their sunscreen to evaluate their knowledge and awareness about sunscreen, and the results are depicted in Figure 1. Forty percent of the sunscreen users use sunscreen with an SPF of more than 30, 24% use sunscreen with an SPF between 15 and 30, and only 5% use sunscreen with an SPF of less than 15, while 31% of sunscreen users do not know the SPF of their sunscreen.
The other common sun protection practices were also evaluated, and the results are shown in Table 2. The most popular sun protection practice adopted is avoiding exposure to solar radiation during the peak hours, with 66% of the respondents employing this practice. The percentages of individuals using sunglasses and protective clothing are both 50%, which indicates that the use of sunglasses and wearing protective clothing are also common sun protection practices. About 18% of the respondents use hats during the daytime and a very few respondents use umbrellas (only 5%).
Level of Sun Protection Practices
The results of the survey on the level of adoption of sun protection practices by the respondents are presented in Figure 2. The data indicate that 22% of the respondents use a low level of sun protection, 53% use a medium level of protection, while 25% of the respondents use a high level of sun protection.
Chi-Squared Test and Spearman’s Correlation
The chi-squared test and Spearman’s correlation were used in the present study to determine the association of the level of sun protection with the factors related to socio-demographic characteristics, sensitivity to solar radiation, adoption of general safety measures in day-to-day life, extent of sun exposure and knowledge of its effects, general awareness about the UV index, skin cancer, and vitamin D.
Effect of Socio-Demographic Characteristics on the Level of Sun Protection
The associations between the socio-demographic characteristics and the level of sun protection of the respondents are shown in Table 7. The majority of both male and female participants use a medium level of sun protection. About half of the respondents with a postgraduate degree use a high level of sun protection, while most of the respondents without a postgraduate degree use a medium level of sun protection. The percentage of use of a medium level of sun protection is higher among participants of all nationalities. The highest percentage (44%) of married people use a high level of sun protection, while a majority (60%) of single respondents use a medium level of protection. Forty one percent of respondents living with fewer than four people in the same household use a high level of sun protection, which is higher than the percentage of those who use low and medium levels of protection. However, a higher percentage of respondents living with four or more people in the same household use a medium level of sun protection. Lastly, most of the respondents with an income more than enough to meet their expenses use a higher level of sun protection, as expected.
 |
Table 7 Association Between the Level of Sun Protection and Socio-Demographic Variables |
The p-value of the chi-squared test of the level of sun protection and six socio-demographic variables is very small (p<0.05), indicating that there is a very strong relationship between the sun protection behavior and these socio-demographic characteristics. Based on the results of the Spearman correlation, several features, namely the age, educational level, and income, are positively associated with the level of sun protection adopted by the respondents, while the number of people living in the same household has a negative association, as expected.
Effect of Sensitivity to Solar Radiation and Health Status on the Level of Sun Protection
The level of protection from the harmful effects of the sun according to the sensitivity to solar radiation and effect of health status is presented in Table 3. In this article, seven attributes were used to determine the sensitivity to solar radiation and the effect of health status. These are the skin type, skin ailments, tendency to burn and tan, whether taking any medications for any disease, a history of skin cancer in the family, and whether any family member has suffered from skin disease caused by solar radiation. The majority of the participants (42%) have type III skin, which tans easily and is not subjected to significant sunburn; about 39% have type II skin, which is subjected to sunburn easily and tans slowly; 11% have type I skin, which is fair skin that is subjected to sunburn easily and never tans; and only 9% have type IV skin, which is dark, tans well and is never subjected to sunburn. Sixty five percent of the participants do not have any skin problems, the skin of 69% of the participants does not have a tendency to burn and tan, 85% of the participants are not on any medications for any disease, 96% do not have any family history of skin cancer, and about 85% of the respondents do not have any family member who has suffered from sun-related skin disease. Therefore, the results indicate that the respondents have a healthy skin and a healthy family history as well.
The chi-squared test indicates that the level of sun protection is strongly associated with four factors: having any skin ailments, with skin having a tendency to sunburn and tan, taking medications for any disease, and any family member suffering from sun-related skin disease. All p-values are less than 0.05. Based on the results of the Spearman correlation, these factors are positively associated with the level of sun protection. A negative association between the skin type and the level of sun protection exists, while the family history of skin cancer is positively correlated. Both factors are non-significant (p-values >0.1).
Effect of Health Consciousness and Safety Measures Adopted in Day-to-Day Life on the Level of Sun Protection
To determine the effect of health consciousness and safety measures adopted by the respondents in their day-to-day life on the level of sun protection, the following three attributes were considered in the present study: being on a health-conscious diet, participating in sports activity/exercise regularly, and using a seatbelt when driving/riding in a motor vehicle. The association of the level of sun protection and the health consciousness and safety measures adopted in day-to-day life was analyzed, and the results are presented in Table 4. Sixty five percent of the participants are not on a health-conscious diet, 61% of the participants do not take part in any sports activity regularly, while a majority (62%) of the participants wear a seatbelt when driving/riding in a motor vehicle. Both the chi-squared test and the Spearman’s correlation coefficient analysis indicate that regular sports activity/exercise and wearing a seatbelt when driving/riding in a motor vehicle have a strong positive association with the level of sun protection (p<0.05), while being on a health-conscious diet is only weakly associated with the level of sun protection.
Effect of Knowledge and Awareness of Sun Exposure, UV Index, and Vitamin D on Sun Protection Level
Six questions were asked to determine the effects of exposure of the respondents to solar radiation and the awareness of the UV index (Table 5). Sixty percent of the respondents have never suffered sunburn, 31% have suffered sunburn three or fewer times, and only 9% of the respondents have suffered sunburn four or more times in the past. The majority of the respondents (76%) do not sunbathe at least once per week, while 18% of the respondents sunbathe at least once a week depending on the weather, and only 6% of respondents sunbathe at least once per week. The awareness of the respondents of sunburn and the risks of excessive exposure to solar radiation were also analyzed. The results show that 66% of participants are aware of the risks of sunburn from prolonged exposure to sun, and 78% of the participants are aware of the dangers of exposure to solar radiation. However, only 30% of the respondents are aware of the UV index. The number of respondents who consider the UV index in their personal sun exposure and sun protection is also not high (25%). In the survey on awareness about vitamin D, 47% of the respondents have been tested for vitamin D some time during their lifetime, and only 34% of the respondents have taken vitamin D tablets. The results of both the chi-squared test and Spearman’s correlation show that all these eight factors have a positive and strong association with the level of protection from solar radiation.
Respondents’ knowledge about the UV index was assessed by asking for the correct definition of the UV index. The results indicate that 65% of the respondents are not aware of the UV index, and 15% of the respondents who claimed to know the correct definition of the UV index failed to select the correct answer (Figure 3). This means that only 20% of all respondents are aware of the correct meaning of the UV index. The association of the response to the question on the definition of the UV index with gender, educational level, and sun protection level is shown in Table 8. The percentages of men (20%) and women (19%) who are able to choose the right answer are about the same. The results also show that the percentages of respondents selecting the right answer in the high school and some college education groupsare lower than those in the undergraduate and postgraduate groups. Besides, based on the chi-squared test, awareness of the correct meaning of the UV index has a significant association with the level of education and the sun protection level.
 |
Table 8 Association of the Response Regarding the Definition of the UV Index with Gender, Educational Level, and Sun Protection Level |
Level of Sun Protection According to General Knowledge of the Harmful Effects of the Sun on Skin
Four questions were asked to assess the general knowledge of the respondents regarding the harmful effects of the sun on the skin (results are shown in Table 6). Based on the results of the analysis, a majority (more than 80%) know that sun can cause skin cancer and skin aging, and 79% of the respondents know that skin cancer can be fatal. Fifty-four percent of the respondents believe that getting a suntan is healthy if sunburn can be avoided. This view of a healthy suntan has a negative and very weak association with sun protection level (p>0.05), as expected. However, “sun can cause skin cancer”, “sun can cause skin aging”, and “skin cancer can be fatal” have a strong positive association with the sun protection level.
Logistic Regression Model
The data were randomly assigned to training (70%) and testing (30%) datasets. The training dataset was used to construct the model, while the testing dataset was used to observe the errors and prevent overtraining. The value of the response variable  is 0, 1, and 2 when the sun protection level of the respondent is low, medium, and high, respectively. The developed logistic regression model of the selected variable has 19 attributes (namely, age, gender, educational level, nationality, number of people living in the same household, income with respect to expenses, respondent has a tendency to sunburn and tan, whether a family member has a sun-related skin disease, whether sunscreen lotions are harmful to the skin in some way, is on a health-conscious diet, takes part in sports activities regularly, wears a seatbelt when driving/riding in a motor vehicle, the number of times having suffered sunburn, awareness of the dangers of exposure to solar radiation, the respondent takes the UV index into consideration for exposure to the sun, whether been tested for vitamin D during the lifetime, opinion regarding whether skin cancer can be fatal, opinion whether sun can cause skin aging, and opinion whether suntan is healthy if sunburn can be avoided). The confusion matrix was analyzed to evaluate the model, and the results are shown in Table 9. The overall accuracy with the training data set is 67% and is about 66% with the testing data set, indicating a good fit of the model. A predictor importance chart was generated to determine the effect of each predictor in the developed logistic regression model. The top ten significant predictors are: opinion whether sun can cause skin aging, age, awareness of the dangers of exposure to solar radiation, income with respect to expenses, the respondent takes the UV index into consideration when being exposed to the sun, whether been tested for vitamin D during the lifetime, the number of times having experienced sunburn, gender, uses a seat belt, and the number of people living in the same household (Figure 4).
is 0, 1, and 2 when the sun protection level of the respondent is low, medium, and high, respectively. The developed logistic regression model of the selected variable has 19 attributes (namely, age, gender, educational level, nationality, number of people living in the same household, income with respect to expenses, respondent has a tendency to sunburn and tan, whether a family member has a sun-related skin disease, whether sunscreen lotions are harmful to the skin in some way, is on a health-conscious diet, takes part in sports activities regularly, wears a seatbelt when driving/riding in a motor vehicle, the number of times having suffered sunburn, awareness of the dangers of exposure to solar radiation, the respondent takes the UV index into consideration for exposure to the sun, whether been tested for vitamin D during the lifetime, opinion regarding whether skin cancer can be fatal, opinion whether sun can cause skin aging, and opinion whether suntan is healthy if sunburn can be avoided). The confusion matrix was analyzed to evaluate the model, and the results are shown in Table 9. The overall accuracy with the training data set is 67% and is about 66% with the testing data set, indicating a good fit of the model. A predictor importance chart was generated to determine the effect of each predictor in the developed logistic regression model. The top ten significant predictors are: opinion whether sun can cause skin aging, age, awareness of the dangers of exposure to solar radiation, income with respect to expenses, the respondent takes the UV index into consideration when being exposed to the sun, whether been tested for vitamin D during the lifetime, the number of times having experienced sunburn, gender, uses a seat belt, and the number of people living in the same household (Figure 4).
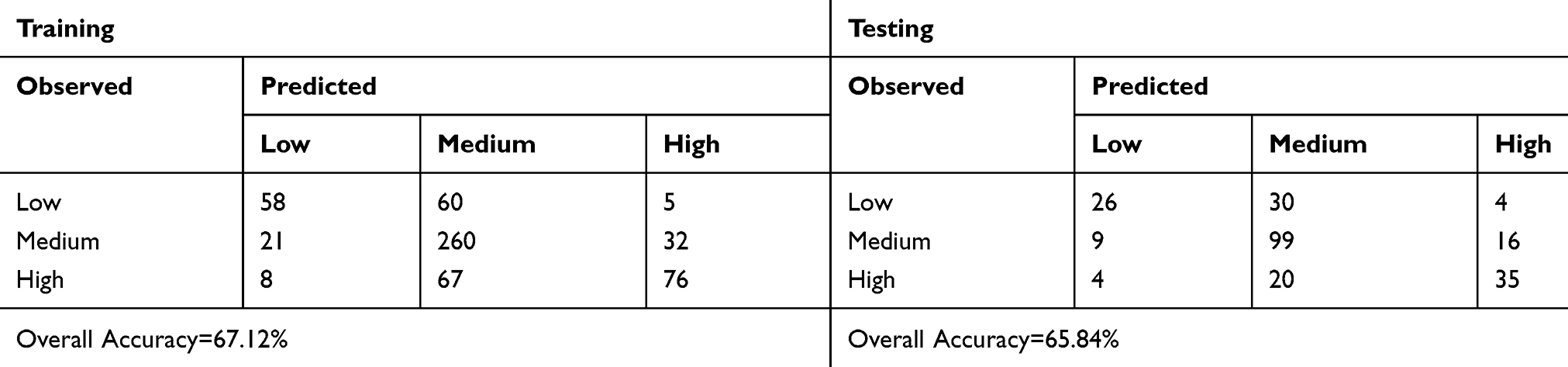 |
Table 9 Confusion Matrix for the Constructed Logistic Regression Model |
Discussion
The most popular sun protection practice is using sunscreen when going out during the daytime, while other common sun protection measures are using a hat, sunglasses, an umbrella, and/or protective clothing, and avoiding exposure to solar radiation during peak hours.2,17,18,26-28 Using sunscreen lotions is not a popular sun protection practice among the respondents. However, using sunscreen is one of the most common sun protection practices in Kuwait,26 which is a country in the north-east corner of the Arabian Peninsula. Sunscreen use is also the most popular preventive measure of people in Belgium, Europe, Australia, Canada, and the USA.16,22,23 Based on the survey results of the present study, a majority of the sunscreen users are females, similarly to the other published results.2,17,26 The awareness of sunscreen users about the SPF of their sunscreen is not satisfactory. The percentage of respondents who avoid exposure to the sun during peak hours is higher than all other sun protection practices considered in this study. The three most popular sun protection practices of the studied sample are avoiding exposure to solar radiation during peak hours, using protective clothing, and using sunglasses. The sun protection practices based on gender were also analyzed in this study, and the results show that the three most popular preventive measures among females are: 1) avoiding exposure to solar radiation during peak hours; 2) using protective clothing, and 3) using sunglasses. However, for males the three most popular preventive measures are: 1) avoiding exposure to solar radiation during peak hours; 2) using sunglasses, and 3) wearing a hat when going out during daytime. Similar results have been reported elsewhere.17
In general, education, the number of people living in the same household, and income with respect to expenses are associated with the use of sunscreen. Eighty-one percent of Canadian adults use a minimum of one sun protection measure, with sunscreen use and wearing protective clothing being most popular among individuals with a higher educational level. Individuals with a higher income level resorted to frequent use of sunscreen.22 In the present study, the overall level of sun protection among individuals is not satisfactory. Twenty five percent of the respondents use a high level of sun protection and the majority of them are female, married, with a higher level of education and economically stable, and the number of family members living in the same household is four or fewer.
Robinson et al found that using sunscreen on children is significantly related with fair skin, sunny weather, earlier record of sunburn, and family history of skin cancer.18 In another study, Ermertcan et al reported that skin type, total nevus count, family history of skin cancer, and sun-related skin disorders are associated with the use of sunscreen.17 Based on the present study, the sun protection level is strongly associated with the presence of skin problems, whether there is a tendency to sunburn and tan, whether taking medication for any disease, and family history of sun-related skin disease. Ermertcan et al also reported that the use of sunscreen by people with skin types I and II is higher than in people with skin types III and IV, as well as among people with a family history of skin cancer and sun-related skin diseases. Similar results regarding the level of sun protection are reported in this present study.
The present study found that the level of sun protection has a positive association with the factors related to health consciousness and the use of safety measures in day-to-day life. Geller et al reported similar results, showing that the use of sun protection is higher among students of all ages who do not have other health risks.29 The adoption of sun protection measures was related to positive attitudes about individual appearance and self-image. Based on a study among students and personnel of Celal Bayar University, sun protection is not significantly associated with obesity, use of cigarettes and alcohol, and the use of sunscreen and sunglasses, while it is correlated with driving a car and participating in sports activities.17 However, the respondents adopted sun protection measures to avoid distraction by the sun while driving a car and during sports activities, and not because they wanted to be healthy. The authors also found that the use of sunscreen and being on a diet among young males and females are due to cosmetic reasons, and not for protection from solar radiation.
This study also examined the changes in the level of sun protection adopted by the respondents based on their history of sunburn. The percentage of respondents who adopt a higher level of sun protection is higher among those who have suffered sunburn four times or more compared to those who have suffered sunburn fewer times or never. Similar results have been found in numerous studies. Tamir et al evaluated the variation in the adoption of sun protection measures in Israel from 1994 to 1998. The number of people using sun protection measures increased from 34% in 1994 to 41% in 1996 and to 46% in 1998.30 A study has also found that the adoption of sun protection measures changes among people who suffered sunburn during the previous summer.17
The results of the present study indicate that the respondents do not have an adequate understanding of the UV index. Thirty percent of the participants are aware of the UV index. Similar results were found in Germany, where only 27% of the people were aware of the UV index.5 Wester and Paulsson reported similar results for the Swedish population.31 Only 25% of the respondents in the present study take the UV index into consideration when adopting sun protection measures. Studies have found similar results for the Swedish and German populations.5,31,32 Studies conducted in several regions in Australia indicate that the percentage of respondents who adjust their use of sun protection measures based on the UV index is only 24–40%, despite their higher awareness about the UV index.32–34 Studies in Canada have found that Canadian adults who have a higher level of awareness of the UV index are more prone to being sunburned.22 In the present study, only 20% of the participants were able to provide the correct meaning of the UV index. Numerous studies in Canada, the USA, Australia, New Zealand, England, and Germany indicate that the understanding of the UV index is not adequate and additional public awareness programs are needed.22,29,32-35 Furthermore, some researchers are of the view that the numerical UV index followed by a technical explanation is hard to comprehend.22,31,32,34-36 Hence, an easily understood presentation of the UV index with direct links to personal exposure to solar radiation and outdoor behavior should be developed. This study also assessed the awareness and attitudes toward vitamin D. The results suggest that the awareness level about vitamin D among people in this region needs to be improved.
Previous research37 indicates that individuals in the Middle East with a fair skin are at higher risk of skin cancer from accumulative sunburn. However, a majority are still unaware of the dangers posed by living in this hot, sunny climate, and many in this region are surprised to know that skin cancer can be fatal. Estimates indicate that more than 10,000 people in the USA die each year from skin cancer. Based on World Health Organization (WHO) estimates, more than 60,000 people die each year from “getting too much sun” and most of these deaths are from skin cancer. In the present study, a large number of respondents is aware that the sun can cause skin cancer and skin aging, similarly to other studies.2,17,23,38,39 However, 54% of the respondents still think that a suntan can be healthy if sunburn can be avoided. Similar results have been found in other studies on the adoption of sun protection measures by the population in several countries.2,17 This attitude must be changed, considering that 85% of skin cancer cases can be prevented by controlling exposure to solar radiation.
In the present study, the logistic regression model was constructed to predict the level of sun protection practices adopted by people living in Saudi Arabia and Bahrain. The model fitting information was analyzed to compare the constructed logistic regression model with the “intercept only” (null) model. The p-value of the likelihood-ratio test is very small (0.000), indicating that there is a significant difference between the “intercept only” and populated model. The pseudo R-squared measures were analyzed to estimate the coefficient of determination, i.e., how much of the variance in the dependent variable can be explained by the model. The results indicate that the proposed logistic regression model can explain between 45.9% (Cox and Snell R squared) and 52.9% (Nagelkerke R squared) of the variance in the sun protection level. The confusion matrix indicates that the prediction accuracy of the developed logistic regression model is about 67%. Based on the predictor importance chart of the constructed logistic regression model, the top ten most significant predictors of the level of adopted sun protection are: opinion whether the sun can cause skin aging, age, awareness of the dangers of exposure to solar radiation, income with respect to expenses, the respondent takes the UV index into consideration when being exposed to the sun, whether been tested for vitamin D during the lifetime, the number of times having suffered sunburn, gender, wearing a seatbelt while driving or riding in a motor vehicle, and the number of people living in the same household.
Conclusion
This study shows that the people in Saudi Arabia and Bahrain have adequate knowledge and are aware of the harmful effects of exposure to solar radiation. However, their sun protection practices do not seem to reflect their good level of knowledge regarding the dangerous effects of the sun on the skin. The rectification of the incorrect behavior regarding protection from the effects of the sun is a difficult but vital obligation of the government. Hence, the people of these regions in the Arabian Peninsula must be more knowledgeable to increase their awareness level about the UV index and its harmful effects on the skin. An efficient policy of education on the effective use of sun protection methods must be developed to increase the level of sun protection. Public awareness campaigns can also be initiated to convince people that it is worthwhile to protect themselves from the sun. These initiatives can create a more sun-conscious population, which may stop the growing incidence of skin cancers in these regions of the Arabian Peninsula. However, future research is expected to enlarge the scope of the survey, in terms of both the size of the samples and the nature of the questions, offering more insight into the knowledge about the UV index and sun protection measures adopted by residents in the Arabian Peninsula. The results of such studies will help decision makers to formulate effective strategies to increase the awareness of the harmful effects of solar radiation among the population.
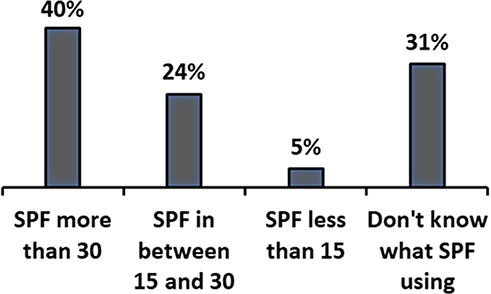 |
Figure 1 Sun protection factor (SPF) of sunscreen lotions used by the respondents. |
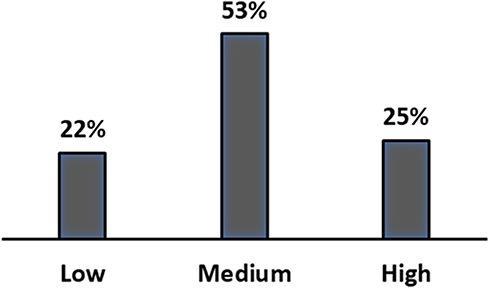 |
Figure 2 Level of sun protection. |
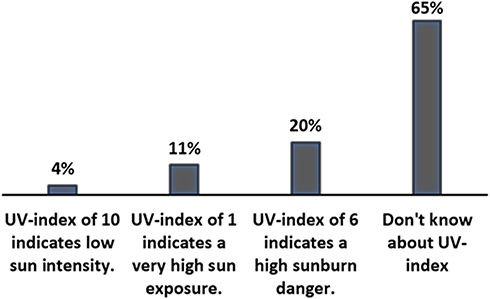 |
Figure 3 Responses of the participants about the definition of the UV index. |
 |
Figure 4 Predictor importance chart of the logistic regression model. |
Abbreviations
UV, ultraviolet; SPF, sun protection factor.
Data Sharing Statement
The questionnaire used in your study was developed for this research project. The datasets are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This project is approved by the institutional review board of Imam Abdulrahman Bin Faisal University (IRB number: IRB-2020-09-141). This is questionnaire-based research and data were collected from the public anonymously. The online questionnaire was designed to include a brief description of the research topics, aim, guidelines for survey submission, possible risks, and confidential statement. Consent from individual respondents was obtained prior to their completion of the survey.
Acknowledgment
Imam Abdulrahman Bin Faisal University is acknowledged for some of the facilities utilized in this research.
Funding
No funding was received for this study.
Disclosure
The author states that there are no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper and reports no conflicts of interest for this work.
References
1. Seerri L, Keefe M. The adverse effects of the sun on the skin - a review. Malta Med J. 1995;26(vii):26–31.
2. Scerri L, Aquilina S, Gauci AA, Dalmas M. Sun awareness and sun protection practices in Malta. J Eur Acad Dermatol Venereol. 2002;16(1):47–52. doi:10.1046/j.1468-3083.2002.00376.x
3. Yilmaz M, Yavuz B, Subasi M, et al. Skin cancer knowledge and sun protection behavior among nursing students. Jpn J Nurs Sci. 2014;12(1):69–78. doi:10.1111/jjns.12049
4. Heckman CJ, Darlow S, Cohen-Filipic J, et al. Psychosocial correlates of sunburn among young adult women. Int J Environ Res Public Health. 2012;9(6):2241–2251. doi:10.3390/ijerph9062241
5. Börner FU, Schütz H, Wiedemann P. The influence of the UV-index on attitudes toward sun exposure in the German population. J Cancer Educ. 2010;25(4):643–649. doi:10.1007/s13187-010-0108-8
6. Grandahl K, Ibler KS, Laier GH, Mortensen OS. Skin cancer risk perception and sun protection behavior at work, at leisure, and on sun holidays: a survey for Danish outdoor and indoor workers 11 medical and health sciences 1117 public health and health services. Environ Health Prev Med. 2018;23(1). doi:10.1186/s12199-018-0736-x
7. O’leary S, Fotouhi A, Turk D, et al. OCT image atlas of healthy skin on sun-exposed areas. Ski Res Technol. 2018;24:570–586. doi:10.1111/srt.12468
8. World Health Organization. How common is skin cancer. World Health Organization. Available from: http://www.who.int/uv/faq/skincancer/en/index1.html.
9. Diffey BL, Norridge Z. Reported sun exposure, attitudes to sun protection and perceptions of skin cancer risk: a survey of visitors to cancer research UK’s SunSmart campaign website. Br J Dermatol. 2009;160(6):1292–1298. doi:10.1111/j.1365-2133.2009.09149.x
10. Holick M. Vitamin D deficiency. N Eng J Med. 2007;357(3):266–281. doi:10.1056/NEJMra070553
11. Glerup H, Mikkelsen K, Poulsen K, Al E. Commonly recommended daily intake of vitamin D is not sufficient if sunlight exposure is limited. J Intern Med. 2000;247:260–268. doi:10.1046/j.1365-2796.2000.00595.x
12. Grant W. An estimate of premature cancer mortality in the U.S due to inadequate doses of solar ultraviolet- B radiation. Cancer. 2005;94:1867–1875. doi:10.1002/cncr.10427
13. Lappe J, Travers-Gustafson D, Davies K, Recker R, Heaney R. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007;85:1586–1591. doi:10.1093/ajcn/85.6.1586
14. Vieth R, Kimball S. Vitamin D in congestive heart failure. Am J Clin Nutr. 2006;83(4):731–732. doi:10.1093/ajcn/83.4.731
15. Hyppönen E, Läärä E, Reunanen A, Jarvelin M, Virtanen S. Intake of vitamin D and risk of type 1 diabetes: a birth-cohort study. Lancet. 2001;358(9292):1500–1503. doi:10.1016/S0140-6736(01)06580-1
16. Devos SA, Baeyens K, Van Hecke L. Sunscreen use and skin protection behavior on the Belgian beach. Int J Dermatol. 2003;42(5):352–356. doi:10.1046/j.1365-4362.2003.01665.x
17. Ermertcan AT, Ozturkcan S, Dinc G, Yurtman D, Pala T, Sahin MT. Sunscreen use and sun protection practices in students and personnel of Celal Bayar University. Photodermatol Photoimmunol Photomed. 2005;21(4):191–197. doi:10.1111/j.1600-0781.2005.00158.x
18. Robinson JK, Rigel DS, Amonette RA. Summertime sun protection used by adults for their children. J Am Acad Dermatol. 2000;42(5 Pt 1):746–753.doi:10.1067/mjd.2000.103984
19. Kunene Z, Albers PN, Lucas RM, Banwell C, Mathee A, Wright CY. ‘My child did not like using sun protection’: practices and perceptions of child sun protection among rural black African mothers. BMC Public Health. 2017;17(1):677. doi:10.1186/s12889-017-4688-7
20. Duffy SA, Ronis DL, Waltje AH, Choi SH. Protocol of a randomized controlled trial of sun protection interventions for operating engineers. BMC Public Health. 2013;13(1):273. doi:10.1186/1471-2458-13-273
21. Manne SL, Coups EJ, Jacobsen PB, Ming M, Heckman CJ, Lessin S. Sun protection and sunbathing practices among at-risk family members of patients with melanoma. BMC Public Health. 2011;11(1). doi:10.1186/1471-2458-11-122
22. Purdue MP. Predictors of sun protection in Canadian adults. Can J Public Health. 2002;93(6):470–474. doi:10.1007/BF03405042
23. Halpern AC, Kopp LJ. Awareness, knowledge and attitudes to non-melanoma skin cancer and actinic keratosis among the general public. Int J Dermatol. 2005;44(2):107–111. doi:10.1111/j.1365-4632.2005.02090.x
24. Patlakas P, Stathopoulos S, Flocas F, Kalogeri K, Kallos K. Regional climatic features of the Arabian Peninsula. Atmosphere. 2019;10(4):220. doi:10.3390/ATMOS10040220
25. Roshan DR, Koc M, Abdallah A, Martin-Pomares L, Isaifan R, Fountoukis C. UV index forecasting under the influence of desert dust: evaluation against surface and satellite-retrieved data. Atmosphere. 2020;11(1):96. doi:10.3390/ATMOS11010096
26. Al-Mutairi N, Nair V, Issa B. Photoprotection and vitamin D status: a study on awareness, knowledge and attitude towards sun protection in general population from Kuwait, and its relation with vitamin D levels. Indian J Dermatol Venereol Leprol. 2012;78(3):342–349. doi:10.4103/0378-6323.95451
27. Mortier L, Lepesant P, Saiag P, et al. Comparison of sun protection modalities in parents and children. J Eur Acad Dermatol Venereol. 2015;29:16–19. doi:10.1111/jdv.12897
28. Mahler HIM, Kulik JA, Harrell J, Correa A, Gibbons FX, Gerrard M. Effects of UV photographs, photoaging information, and use of sunless tanning lotion on sun protection behaviors. Arch Dermatol. 2005;141(3):373–380. doi:10.1001/archderm.141.3.373
29. Geller AC, Hufford D, Miller DR, et al. Evaluation of the ultraviolet index: media reactions and public response. J Am Acad Dermatol. 1997;37(6):935–941. doi:10.1016/s0190-9622(97)70068-9
30. Tamir D, Tamir J, Dayan I, Josef H, Orenstein A, Shafir R. Positive changes in sun-related behavior in Israel (1994–1998). Prev Med. 2002;35(4):369–375. doi:10.1006/pmed.2002.1078
31. Wester U, Paulsson L-E. The influence of a UV index on the attitudes of a swedish population towards sun exposure. Radiat Prot Dosimetry. 2000;91(1):323–324. doi:10.1093/oxfordjournals.rpd.a033229
32. Bränström R, Ullén H, Brandberg Y. A randomised population-based intervention to examine the effects of the ultraviolet index on tanning behaviour. Eur J Cancer. 2003;39(7):968–974. doi:10.1016/s0959-8049(03)00117-5
33. Blunden A, Lower T, Slevin T. Knowledge, awareness, and use of the UV index amongst the west Australian public. J Health Commun. 2004;9(3):207–221. doi:10.1080/10810730490447057
34. Alberink AM, Valery PC, Russell A, Green A. Do forecasts of UV indexes influence people’s outdoor behaviour? Aust N Z J Public Health. 2000;24(5):488–491. doi:10.1111/j.1467-842x.2000.tb00498.x
35. Bulliard JL, Reeder A. Getting the message across: sun protection information in media weather reports in New Zealand. N Z Med J. 2001;114(1126):67–70.
36. Dixon HG, Hill DJ, Karoly DJ, Jolley DJ, Aden SM. Solar UV forecasts: a randomized trial assessing their impact on adults’ sun-protection behavior. Health Educ Behav. 2007;34(3):486–502. doi:10.1177/1090198106294644
37. Middle East Health Magazine. Available from: http://www.middleeasthealthmag.com/index_m.htm.
38. Nikolaou V, Stratigos AJ, Antoniou C, et al. Sun exposure behavior and protection practices in a Mediterranean population: a questionnaire-based study. Photodermatol Photoimmunol Photomed. 2009;25(3):132–137. doi:10.1111/j.1600-0781.2009.00424.x
39. Saridi M, Toska A, Kafkia T, et al. Evaluation of students’ knowledge and attitudes on sun radiation protection. Available from: www.internationaljournalofcaringsciences.org.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.