Back to Journals » Psychology Research and Behavior Management » Volume 15
Suicidal Ideation and Obsessive-Compulsive Disorder: Links and Knowledge
Authors Benster LL ![]() , Weissman CR, Daskalakis ZJ
, Weissman CR, Daskalakis ZJ
Received 11 September 2022
Accepted for publication 15 December 2022
Published 20 December 2022 Volume 2022:15 Pages 3793—3807
DOI https://doi.org/10.2147/PRBM.S368585
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Lindsay L Benster,1 Cory R Weissman,2 Zafiris J Daskalakis2
1Joint Doctoral Program in Clinical Psychology, SDSU/UC San Diego, San Diego, CA, USA; 2Department of Psychiatry, UC San Diego School of Medicine, San Diego, CA, USA
Correspondence: Lindsay L Benster, Joint Doctoral Program in Clinical Psychology, SDSU/UC San Diego, 6363 Alvarado Ct, San Diego, CA, 92120, USA, Tel +1206 230 0707, Email [email protected]
Abstract: Suicidal ideation (SI) is understudied in obsessive-compulsive disorder (OCD). Nonetheless, evidence suggests increased risk for SI in individuals with OCD compared to the general population. Understanding the relationship between SI and OCD involves investigating risk factors associated with SI. Furthering knowledge of links is essential for enhancing outcomes and decreasing experiences of SI through improving treatment interventions. Additionally, increasing awareness of factors that lead SI to suicide attempts (SA) is vital. To best illustrate the current state of knowledge, this scoping review examines risk factors for SI, including symptom profiles or phenotypes, comorbid diagnoses, sociodemographic and lifestyle factors, childhood trauma, and genetic and familial contributions. Important treatment considerations for targeting SI within the context of OCD are detailed with respect to the current evidence for psychotherapy, pharmacology, brain stimulation, and neurosurgery. Gaps in the literature and future directions are identified, broadly with respect to studies examining the treatment of SI within the context of OCD, particular OCD phenotypes, and factors influencing SI in pediatric OCD. Due to the relative novelty of this area of exploration, many unknowns persist regarding onset of SI in OCD, factors contributing to the maintenance of SI in OCD, and relevant treatment protocols. Findings suggest that individuals with previous SI or SA, history of childhood trauma, significant life stress, and psychiatric comorbidities, particularly depression, should be closely monitored and screened for SI.
Keywords: suicidality, OCD, risk factors, SI treatment
Introduction
Obsessive-Compulsive Disorder (OCD) is a prevalent and chronic psychiatric disorder that significantly impairs global functioning, quality of life, and well-being of the individual and associated support systems. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), OCD is characterized by the presence of obsessions, compulsions, or both.1 Obsessions are conceptualized as uncontrollable intrusive and repetitive thoughts, ideas, or images leading to distress. Compulsions involve urges and behaviors that an individual engages in to alleviate distress or relieve obsessions. Disability from OCD is high, and early onset of OCD is associated with significant deficits in educational attainment and increased risk of labor market marginalization.2 The World Health Organization has historically placed OCD among the top 10 most handicapping conditions, determined by quality of life and loss of income standards.3
Amongst psychiatric disorders, OCD is typically associated with a relatively low risk of suicide. Thus, minimal attention has been allocated to risk factors associated with suicidal behavior in OCD. However, increasing evidence supports a significant correlation between OCD diagnosis and suicide attempts (SA) and ideation. Estimates correlating OCD and suicidal ideation (SI) range from to 27% to 62% of subjects, indicating this relationship has been inadequately addressed.4,5 OCD has been found to significantly increase the odds of having a lifetime SI in comparison to the general population, at 25.95% versus 2%, respectively.6 Further, the presence of either obsessive thoughts or compulsive behavior independent of OCD diagnosis reveals a strong association with lifetime suicide attempts.7 While directionality of this correlation is difficult to pinpoint, evidence for a parsimonious model suggests SI can be best predicted by OCD symptom severity, but not the alternative.8,9 In other words, SI increases as OCD severity increases, but SI does not appear to influence OCD symptom severity. Regrettably, predictors of those with SI who progress to SA are weak at best. It is important to distinguish between SI and SA because the vast majority of individuals who experience SI will not make a suicide attempt, with estimates as low as 7%.10 Studies examining factors contributing to SA often conflate SI and SA, confusing what differences in outcomes are attributed to. A relevant study suggests history of childhood abuse may be one potential distinguishing variable, but evidence is limited.11 Due to the high prevalence of SI and potential etiological differences between SI and SA, this scoping review aims to discuss the current collective knowledge regarding associations between lifetime SI and OCD. To better identify patients at risk, we emphasize evidence for identified risk factors.
Obsessive-Compulsive Disorder
Similar to other psychiatric disorders, OCD is widely heterogeneous in symptom expression and severity. Imaging illuminates certain neurobiological and anatomical abnormalities, particularly of subcortical structures, such as the basal ganglia and the orbitofrontal cortex.12 However, structural differences have not been consistently replicated and postmortem studies of OCD are scarce. Related to structural differences, neurotransmitter hypotheses, such as disruptions in endogenous serotonin concentrations, provide grounding for administration of pharmacological interventions.13 Dysfunctions in glutamate neurocircuitry and modulating agents have also been implicated in OCD.12 Ultimately, knowledge regarding the etiology and perpetuating factors are predominantly correlational and theory-driven, with numerous outstanding gaps.
Beyond neurobiological processes, genetics also appear to play an important role in the onset of OCD, as corroborated through twin, animal, and genome-wide association studies.14 Animal models demonstrate several candidate genes associated with obsessive-compulsive symptoms. The genetics of OCD has remained rather elusive, although certain genes (such as SLCL1A1) are of interest.15 Transmission of this relevant genetic information remains largely obscure. Despite outstanding gaps, the risk of experiencing OCD symptoms has been shown to decrease with degree of genetic relatedness.12
Pediatric OCD
Onset of OCD typically occurs in two general peaks, one in pre-adolescence and a second in early adulthood.16 Notably, the central components of OCD remain the same across the lifespan. However, there are two unique specifiers in the DSM-5 that are particularly important to pediatric diagnoses, which include degree of insight (good or fair insight, poor insight, or absent insight/delusional beliefs), and if the individual presents current or previous tic disorder.1 While the aim of this paper focuses on adult OCD, it is worthwhile to briefly consider nuances of SI in pediatric OCD populations. Only one published study has investigated SI in youth diagnosed with OCD. With minimal direct investigation it is premature to draw conclusions, but the study found correlations between SI and greater depressive and anxiety symptoms, sexuality/religiosity and symmetry-related obsessions and compulsions.17 Associations between SI and overall OCD symptom severity, impulsivity, and comorbidity patterns were not found to be significant. This highlights a need for further exploration in understanding the links between SI and OCD particularly in youth populations.
Methods
This scoping review utilized methodology based on the framework detailed by Arksey and O’Malley (2005), which involved five important steps: 1. Identifying the research question, 2. Identifying relevant studies, 3. Selecting relevant studies, 4. Charting the data, 5. Collating, summarizing, and reporting the results.18
Research Question
This review was directed by the question: “What factors mediate the relationship between SI and OCD?” There is ambiguity in the literature regarding distinctions between SI, suicidal behaviors (SB), and SA. Therefore, while our focus was targeted specifically on SI, we addressed SA in certain contexts in order to not overlook any important findings. It can be assumed that an individual with a history of SA also has experienced SI. OCD was considered with respect to comorbidities when assessing risk factors, but OCD had to be the primary diagnosis for included studies.
Search Strategy
The initial search was conducted in PubMed and PsycNet, between May and June of 2022. A secondary search was conducted in November 2022 to include recent studies published since the original search date. Search terms included: “suicidal ideation” AND “obsessive compulsive disorder”; “suicidality” AND “obsessive compulsive disorder”; “suicide” AND “OCD”. Searches for specific subsections were also conducted. Reference lists of identified studies were also consulted to ensure no relevant studies were missed.
Study Selection
Each of the searches returned a modest amount of articles with significant overlap, speaking to the dearth of research in this particular area. Studies were included if they primarily analyzed suicidality in OCD. Studies were excluded if OCD was not the primary diagnosis and if SI was not assessed.
Charting the Data
Charting the data involves key processes of how information is obtained from the primary sources being reviewed.18 For this review, we adopted a narrative review framework, in which outcomes are contextualized for easier comprehension. Specific details of each of the individual studies are not described, but general findings are condensed across studies to contribute to a more wholistic narrative.
Collating, Summarizing and Reporting Results
Due to the nature of a scoping review, the overall aim is not to synthesize evidence and evaluate quality of studies as in a systematic review; rather, the purpose is to highlight interesting avenues and significant gaps that deserve further exploration. By implementing an emphasis on risk factors, we prioritized aspects of the literature that have been largely understudied.
Evidence for SI in OCD
Meta-analyses and systematic reviews have revealed significant associations between SI and OCD.2,19, In a meta-analysis of 61 studies examining either SA or current SI, one out of ten patients with OCD attempted suicide throughout their lifetime, one third was found to have current SI and approximately one half endorsed lifetime SI.2 A second systematic review and meta-analysis including 48 studies also found significant associations between SI, SA, and OCD, with median estimates of SI instances at 27.9% and SA at 10.3%.19 These rates are all significantly higher than the general population. Identifying those at risk of SA is vital for clinicians and patient care at large to save lives and increase patient wellbeing. Understanding mechanisms is necessary to inform who is at greater risk, which begins with identifying risk factors associated with higher SI.
Risk Factors for SI in OCD
Suicide is among the leading causes of premature death in the United States. SI is a vital precursor indicating the potential development of suicidal behaviors.20 Although operational definitions for SI are inconsistent, nondisclosure of SI is a substantial problem thwarting efforts of suicide prevention. For the purposes of this review, SI is characterized as a range of thoughts, ruminations, preoccupations, and wishes related to the possibility of ending one’s life. Due to an increased risk of SI in individuals with OCD compared to the general population, understanding relevant factors can be useful for enlightening the relationship between SI and OCD and identifying individuals at risk of experiencing SI. Further, it provides the opportunity to decrease SI through early intervention. Known risk factors allow for improved screening to flag individuals who may benefit from additional treatment. Several correlational factors are linked to SI in OCD, including various comorbidities, specific symptom profiles, sociodemographic factors, childhood trauma, and genetic and familial contributions. These are organized in accordance with the theorized level of importance or the strongest relationships between SI and OCD first. Table 1 illustrates various sources of evidence for each described risk factor.
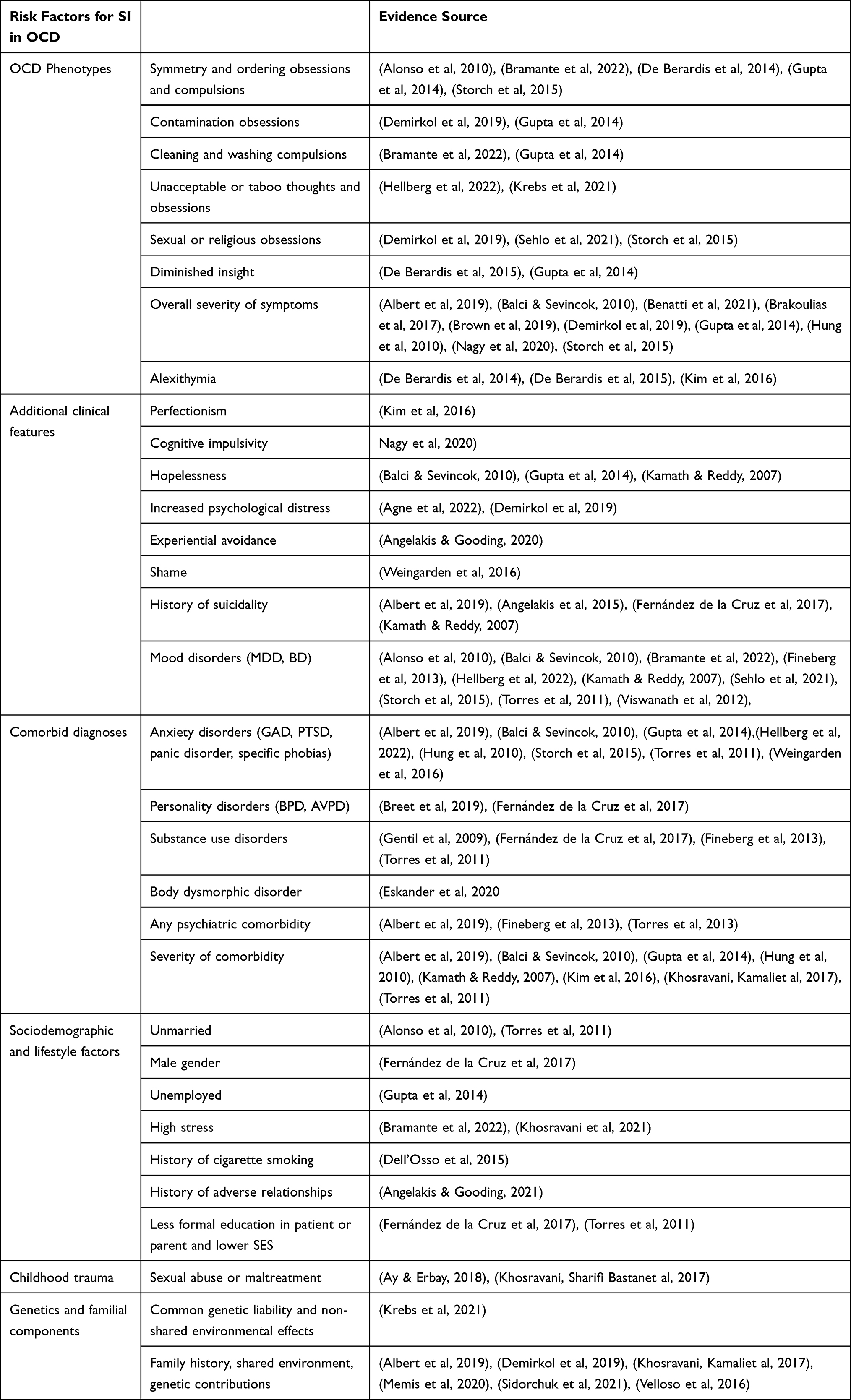 |
Table 1 Risk Factors for SI in OCD |
Comorbid Diagnoses
Comorbid diagnoses are perhaps the strongest link connecting OCD and SI. Lifetime psychiatric comorbidities are present in around 70% of individuals with OCD, with the most common diagnoses consisting of mood and anxiety disorders.19,21,22 The greater the severity of the comorbid disorder, the greater the likelihood of experiencing SI.5,6,23,24 This remains true even after controlling for severity of OCD.25 The high prevalence of mood disorders is particularly important, as it is estimated that up to two-thirds of individuals in the general population who die by suicide suffered from a mood disorder.26 Patients with OCD who endorse high levels of depression and hopelessness are at a significantly higher risk for suicidality than those endorsing lower levels.4,5,9,19,27,28 These two correlates suggest comorbid depression may partially mediate the relationship between suicidal ideation and OCD. Given the considerable proportion of individuals possessing an additional diagnosable disorder, distinguishing SI components unique to OCD that are not attributable to other disorders can be challenging. Individuals diagnosed with comorbid major depressive disorder (MDD) have a significantly higher risk of lifetime SA than those without.7 OCD has been found to significantly influence mood, particularly through increasing feelings of depression and anxious states.3,19 Since mood disorders and related symptomatology are highly associated with suicidality, the extent to which OCD symptoms independently contribute to SI is largely unclear. However, the impact of comorbid depression on suicide in OCD is fairly controversial, with some studies demonstrating an inverse relationship between comorbid depression and SI.29 Notably, comorbidity with bipolar depression appears to have the highest instances of suicidality.6
Personality disorders, borderline personality disorder (BPD) in particular, are independently associated with a high risk for suicidality. Findings suggest comorbid BPD can operate as a predictor for SI.28 Avoidant personality disorder (AVPD) also demonstrated significant correlations with SI, however, low mood and social isolation often accompany AVPD symptomatology and may play a mediating role. Personality disorders are among the most challenging disorders to adequately treat and are frequently diagnosed in individuals presenting with high suicide risk. Those with comorbid anxiety disorders (such as generalized anxiety disorder, panic disorder, and specific phobias), body dysmorphic disorder, and substance use disorders additionally pose higher risk for suicidal ideation.22,30–33 It is evident that experiencing psychiatric disorders in addition to OCD increases the overall risk of SI in patients; however, the exact mechanisms and contributing factors are still widely unknown. More research is warranted to clarify these associations and to determine the effect of interactions of comorbidities on SI.
Patients with comorbid tic disorder have demonstrated a higher rate of SA, but not SI.34 This was primarily consistent in individuals with other comorbidities and disadvantageous epidemiological features, indicating the presence of multiple psychopathologies may be more linked to SI than the characteristics of the disorders themselves.
An association pattern between specific comorbid conditions (bipolar disorder, panic disorder and agoraphobia, eating disorders, and substance use disorders) and symmetry/ordering symptoms has been identified.31,35 This highlights the need to investigate risk factors in a multiplicative manner, to better understand possible interaction effects. Further, it reinforces the necessity of approaching the OCD and SI association with a dimensional approach; not all symptom profiles will yield equivalent suicide risk.
OCD Phenotypes
OCD is a highly heterogeneous disorder with a handful of thematic obsessive and compulsive dimensions. Distinct subtypes of OCD have been proposed based on clusters of symptom expression and neuroanatomical differences.36 However, there is not clear consensus regarding potential phenotype divisions. Therefore, this section focuses on unique patterns of OCD symptoms identified in the relevant literature that have been associated with higher SI in OCD. Factor analyses of the 13 symptoms included in the Yale Brown Obsessive-Compulsive Scale (Y-BOCS; the most widely used scale for OCD) across patients with OCD typically produce between 3 and 5 factors, most commonly including symmetry (a strong desire for things to be correctly aligned or symmetrical) and hoarding, contamination and cleaning, and pure obsession.37,38 These factors are considered valid and reliable constructs accounting for approximately 70% of the total symptom variance. Various phenotypes have demonstrated differing associations with SI. Studies examining the relationship between SI and OCD symptoms overall have yielded mixed results. Particular symptoms, such as symmetry and order obsessions and compulsions, repeating and trust seeking compulsions, unacceptable or taboo thoughts and obsessions, contamination obsessions, cleaning and washing compulsions, and sexual or religious obsessions, have been more frequently associated with SI and SA.5,6,17,25,27–31,39,40 Unacceptable thoughts demonstrate the strongest correlation with suicidality, likely due to a higher level of distress accompanying an already distressing experience which is then accentuated by violating expectations dictated by social norms. This remains consistent after controlling for other symptom dimensions, comorbidities, and overall symptom severity.30 In certain reports, symptoms revolving around symmetry and ordering, for instance arranging objects in a particular sequence, have been positively correlated with SI at age 18 but not 24.41 This suggests either factors associated with age (such as social pressures) or brain development may be a mediating factor in this specific association. Cleaning and washing compulsions are unique in that they appear to be more prevalent in individuals with SI who do not endorse depression.5 There is not an obvious explanation for such correlations, indicating it may be attributed to additional variables not captured, such as cultural or symptom dimension factors. Such differences may also result from sample biases. Religious obsessions may affect individuals of certain cultural backgrounds more severely than others. For instance, a study conducted among Egyptian Muslim patients with OCD found religious obsessions to be the highest predictor of SI in this population.40 Therefore, it is important to consider an individual’s cultural and experiential context when approaching assessments and treatment. Severity of overall OCD symptoms and related disability does consistently associate with a higher likelihood of experiencing SI, as well as longer duration of illness prior to treatment and earlier age of onset.6,8,9,22,27,34,42 However, the experience of SI has not been found to influence severity of OCD symptoms overtime.8 Understanding the direction of this relationship is important for intervening in critical situations.
Other clinical features of OCD that appear to contribute to SI include alexithymia, perfectionism, shame, and cognitive impulsivity.9,43–46 Alexithymia has been correlated particularly in individuals with poor insight and severe symptoms.47 Notably, impulsivity may be a distinguishing factor in individuals with SI versus SA.5 This may be partially mediated by responsibility attitudes towards the experience of one’s symptoms.46 Additionally, higher levels of checking symptoms, such as excessive checking of household appliances, have been linked with a decreased risk of SI.41 This necessitates further replication and suggests the potential that certain domains of OCD symptoms may make individuals more vulnerable to SI, while others may be more protective. For instance, greater severity of obsessions has been more strongly implicated in SI than compulsions.19 With further replication, these correlations highlight an OCD-specific set of symptoms that may contribute to SI that is unlikely attributable to comorbid diagnoses or other influential factors.
Schneidman’s model describes how psychological distress can operate as a catalyst on persisting risk factors for suicide.48 The concept of psychological distress or pain, refers to a state of mental suffering or emotional unease resulting from interference of an individual’s basic needs.27 Psychological distress has been identified as a critical risk factor for suicide both within the context and independent of mood disorders.49 Within OCD, distress has been shown to be significantly higher in patients with OCD with previous SA than OCD patients without history of attempts.50 This has also been supported in patients who endorse SI but not SA.43 Additionally, significant correlations between severity of OCD symptoms and psychological pain indicate that the more severe the OCD, the greater the likelihood of experiencing distress and potential for SI. Further, the degree of control over compulsive behaviors has also been directly linked to SI.43 This may also be mediated by increased levels of distress.
Experiential avoidance involves an inability to tolerate particular private experiences and has been implicated in the onset and maintenance of numerous mental health issues, including OCD.51 Such private experiences may include unpleasant thoughts, images, emotions, or bodily sensations. Strong associations have been identified between OCD severity, individual obsessive-compulsive thoughts and behaviors, and suicidality through experiential avoidance.51 Due to the intrusive nature of obsessive-compulsive thoughts, targeting experiential avoidance may be fruitful for decreasing SI. Further, experiential avoidance plays an influential role in the reinforcement and thus maintenance of OCD symptoms. Targeting experiential avoidance may therefore indirectly decrease SI by decreasing overall symptom severity.
Past history of suicidality is an important predictor of current or future suicidal ideation.4,6,19 This includes both previous attempts and ideation. While numerous links between symptom expression and SI in OCD exist, the strongest correlations involve known history of SI and increased severity of symptoms. This further emphasizes the imperativeness of comprehensive assessment and detailed patient histories. In fact, suicidality may be trans-diagnostic in nature and could potentially represent its own phenotype. Rigorous studies have linked compelling biomarkers for suicide to abnormalities in stress pathways and subsequent downstream effects.52 Due to the unique biosignature of suicidality, effective treatment may be reliant upon interventions targeting implicated pathways.
Sociodemographic and Lifestyle Factors
Social support is a widely known protective factor against suicidality. Across studies, analyses have compared various sociodemographic and lifestyle factors with risk for SI in OCD. While largely inconclusive, a few characteristics appear to be associated with greater risk for SI, including being unmarried, male, unemployed, having a high degree of stress, a history of cigarette smoking, and a history of adverse social relationships. Cultural components and other sociodemographic variables have thus far not appeared to mediate significant correlations with SI.22,27,53 Being unmarried has been identified from various studies but requires further replication to affirm its role.31,54 Marital status may be indicative of other factors (such as social disconnectedness, age, etc) and therefore may be an indirect marker. Being female and having higher parental education may operate as protective variables, but findings are contradictory.19,28,33 Unemployment shows early evidence for contributing to SI.5 However, like marital status, unemployment may be a result of functional impairment and requires further probing before drawing conclusions. Individuals with OCD of lower socioeconomic status (SES) appear to be at an increased susceptibility for SI.33 SES is associated with a vast number of other potential confounds, such as access to mental health and medical resources, level of income, employment opportunities, social support, medical comorbidities, among others. Lifestyle components related to higher-stress environments should be thoroughly screened when assessing patients with OCD for SI.
In clinical samples of patients with OCD, SI has been more pervasive in those with a history of cigarette smoking.55 Individuals with OCD in general smoke less than those with other psychiatric disorders.56 Measures of impulsivity appear to be higher in those who report current or previous smoking.57 Due to the suggested role of impulsivity in SI, impulsivity rather than smoking itself may hold important implications for SI in OCD. Moreover, those expressing more cigarette smoking and impulsivity may represent an OCD phenotype more at risk of developing SI.
Perception of adverse social relationships occurring during childhood appears to influence SI, hypothesized to be mediated by OCD and depressive features.58 These findings highlight the potential for intervening early in social factors that predispose individuals for inferior mental health outcomes later in life. In light of COVID-19, underlying stress attributed to the pandemic may be responsible for increased risk for SI.59 This highlights the potential role of elevated life stress in general in exacerbating underlying psychopathology and ideation.
Childhood Trauma
Experiencing traumatic events during childhood when the individual is psychologically and neurodevelopmentally vulnerable is associated with an increased risk of developing psychopathology and SI later in life.60,61 Especially childhood sexual abuse and the development of early maladaptive schemas.6,62 As previously mentioned, childhood abuse been suggested to be the most notable variable distinguishing SI from SA in OCD.11 While it is associated with both SI and SA, it appears a history of childhood trauma may be an important factor to examine for the prevention of SAs. Experiencing sexual abuse in childhood may contribute to obsessive thoughts related to taboo or unacceptable topics, which itself is a risk factor for SI. Unacceptable thoughts often include religious, violent, or sexual subject matters; such content is often highly relevant and related to forms of maltreatment and childhood abuse. Endorsement of both childhood trauma and unacceptable thoughts has led to increased SI.24 Importantly, this has been supported in samples independent of depression and anxiety, indicating the traumatic event played a highly probable role in SI.60 Presence of comorbid post-traumatic stress disorder (PTSD) has also been associated with greater risk for SI, in which OCD developed following a traumatic event, aptly referred to as post-traumatic OCD.63 It can be difficult to determine whether the SI is tied to obsessive-compulsive symptoms themselves or the experience of an adverse event. Exposure to maltreatment during childhood bears additional complications, as it can negatively impact treatment and treatment-seeking behaviors, potentially exacerbating symptom severity.64 It also has been directly linked to higher OCD symptom severity.65 However, in individuals with OCD and a history of childhood maltreatment, unacceptable obsessional thoughts and responsibility for harm may be critical to this connection.61 Emotion regulation has also been proposed as a potential underlying mechanism of OCD-related suicidality, due to a critical disruption of these abilities following an adverse event.61,66
Genetics and Familial Components
Family history of suicidal attempts additionally places an individual with OCD at higher risk for SI.6,27,39 The risk of death by suicide appears to decrease with genetic distance; in other words, the closer the relative with suicidality, the greater the risk.67 This significant association has been attributed to genetic components, with a nonsignificant contribution of a shared environment. This is also seen in youth with obsessive-compulsive symptoms, in which genetic components accounted for around two-thirds of the association between taboo thoughts and SI at age 18.41
Treatments
The section below discusses the extant knowledge regarding treating SI in OCD. Minimal research has been conducted examining efficacy of interventions specifically targeting SI in OCD. Therefore, discussion largely addresses existing evidence for effective treatments of SI and OCD independently, with suggestions of potential intersections. Notable intersections are highlighted as important areas of future research. Generally, first-line treatments of OCD typically involve cognitive, behavioral, and pharmacological therapies. Due to the complexity, heterogeneity, and idiosyncratic nature of OCD, thorough assessment is vital for identifying individual treatment targets and selecting the most suitable treatment methodology. Assessing for presence and severity of comorbidities is essential for informing whether other psychopathologies may be more urgent to initially target.
Treating SI in OCD
Identifying SI and risk factors for SI is a crucial component of ensuring patient well-being. The best prophylaxis for SI includes the previously mentioned therapeutic interventions targeting OCD symptoms. Understanding the links between risk factors accompanying OCD and SI can point providers to more thoroughly screening. For instance, in those with obsessions and compulsions related to unacceptable thoughts. Ultimately, further research in this area is essential to better understand unique components of SI in OCD in order to optimally target and treat.
There are few pharmacological agents utilized for suicidality, those being lithium in affective disorders and clozapine for schizophrenia.6,68 However, neither of these medications have been directly assessed for the treatment of SI in OCD to date. Reports have indicated potential connection between clozapine and worsening or development of obsessive-compulsive symptoms in individuals with schizophrenia.69,70 While schizophrenia and OCD may differ in etiology and neurobiological mechanisms, these adverse effects are notable and alternative treatments should be considered. Fluoxetine and sertraline, two SSRIs, demonstrated greatest efficacy for pharmacological intervention targeting SI in OCD.71 Psychotherapies have demonstrated efficacy in reducing SI, primarily cognitive-behavioral therapy (CBT), dialectical behavioral therapy (DBT), and problem-solving therapy.72 In individuals who do disclose SI, immediate action and prompt treatment is essential to prevent progression to attempt.6 Moreover, those with comorbid affective disorders should be urgently attended to, particularly mood disorders with higher rates of suicidality, such as bipolar depression.
Psychotherapy
The most popular psychotherapies for OCD are exposure and response prevention (ERP), CBT, acceptance-based approaches. This remains true for those experiencing SI. ERP is a behavioral therapy and the standard first-line psychotherapy treatment for OCD, demonstrating the greatest treatment efficacy.73 This approach originated from a framework highlighting the salience of intrusive thoughts that can lead to maladaptive behavioral responses. Although the experience of intrusive thoughts is nearly universal, obsessions evolve from misattributions of such thoughts, distorting the perception of a benign thought by confusing it with intent or action. This leads the perception of such thoughts to be interpreted as dangerous and salient.73 Further, suicidal thoughts are often intrusive by nature. Distress resulting from obsessional thoughts in turn motivates engaging in compulsions or avoidance behaviors in attempt to reduce an undesirable outcome or the distress itself. Repeated engagement of compulsions or avoidance behaviors is negatively reinforced inhibiting the individual from learning the undesired outcome was unlikely to occur in the first place. If the event did occur, the individual would likely be able to successfully cope with the repercussions. Alternatively, individuals can maintain erroneous beliefs regarding potential threat by engaging in safety behaviors, which are reinforced through their negative correlation with danger.74 ERP disrupts the continuation of this circuit by integrating progressive distress-inducing stimuli in a manner that allows the individual to learn to disassociate the learned compulsion by refraining from engaging in rituals.12 With repeated exposures, refraining becomes less effortful. OCD patients at higher risk for suicide may benefit from increased use of distraction from intrusive thoughts and decreased use of self-punishment.75 These two strategies frequently improve following ERP treatment. ERP can facilitate enhancing useful skills such as thought control while reducing harmful coping strategies. ERP must be more explicitly studied for the treatment of SI in OCD.
DBT has also been suggested as an effective tool for SI in OCD.24 Within the DBT framework, SI reflects a severe form of invalidation. Treatment combines common cognitive-behavioral strategies with additional focus on distress tolerance, mindfulness, acceptance, and emotion regulation. These skills prioritize SI as a primary treatment target and can simultaneously target prominent risk factors in OCD such as unacceptable thoughts. Additionally, functional analytic psychotherapy (FAP)76 can more specifically target emotional components tied to SI, as well as bolster individual’s interpersonal skills and social support. Presence of SI may alter the general therapeutic approach to OCD and recruit additional methods to ensure patient safety.
Pharmacological Intervention
Antidepressants are the first-line pharmacological intervention for SI and currently utilized for OCD treatment independent of SI. However, controversy has arisen from conflicting evidence that certain antidepressants, such as selective serotonin reuptake inhibitors (SSRIs), may increase SI. While inconsistent, instances of SI increasing in OCD has largely been determined as a rare occurrence.77 Medication for OCD are primarily serotonergic. SSRIs and clomipramine, a tricyclic antidepressant (TCA) that acts upon serotonin, occupy the primary pharmacological intervention of choice for OCD and have demonstrated superiority to placebo in a large number of randomized clinical trials (RCTs).12,78–80 Higher doses of SSRIs, as classified per American Psychiatric Association (APA) dose recommendations, exhibit higher treatment efficacy than lower doses.81 Ultimately, SSRIs are independently effective in both OCD and SI, and taken together with evidence for serotonin deficits provide a valuable tool for this particular intersection, albeit understanding of precise mechanisms is lacking.52,82
Medications capable of modulating the glutamatergic and dopaminergic systems have been receiving increasing attention, particularly considering circuit-based theories regarding OCD.12,81 From a combination of case studies and synaptic and molecular exploration of related circuitry, drugs capable of modifying these neurochemicals have been included in the therapeutic armamentarium for OCD. Interestingly, combination of psychotherapy and medications has not yielded significant synergistic effects in OCD.78 Fortunately, antidepressants are the first-line pharmacological intervention for SI, and therefore, such medications can potentially treat both OCD and SI simultaneously. Notably, controversy has arisen from certain studies reporting increased instances of suicidality following use of SSRI in vulnerable patients with depression, primarily in young adults.83,84 However, a large meta-analysis of RCTs exploring the treatment of OCD with SSRIs suggested that the benefits of SSRIs significantly outweigh potential adverse effects.85 As for the capability to treat SI itself, more evidence is needed.
Psychedelic therapy is emerging as a promising intervention for a range of psychopathologies. Early results suggest psychedelics may effectively reduce experiential avoidance, depression severity, and SI.86 Further research should explore mechanisms of this intervention technique, as well as expand upon broader implications for SI treatment.
Neurostimulation
Treating SI with neurostimulation within the context of OCD has not been explored according to a review of the literature. However, evidence suggests neuromodulation techniques can be effective for attenuating SI in mood disorders, suggesting they may be effective for SI in other psychiatric disorders as well.87 Further, stimulation techniques have shown efficacy for treating OCD. Neurostimulation is a rapidly evolving field of intervention and exploration, capable of altering neural activity from the deliverance of energy to targeted brain regions of interest. Electroconvulsive therapy (ECT), magnetic seizure therapy (MST), and repetitive transcranial magnetic stimulation (rTMS) have all demonstrated efficacy in decreasing SI in individuals with depression, with MST presenting superiority in terms of remission from suicidality as well as treatment side effects.88 A form of rTMS that targets deep structures (dTMS) has been FDA approved for the treatment of OCD following a series of effective trials.89 Treatment response rates have been as high as 72.6% acute response and 58% after one month of intervention. rTMS is particularly useful in cases where the individuals failed to adequately respond to pharmacological intervention.90 Targeted brain regions are predominantly midline structures: medial prefrontal cortex and anterior cingulate cortex. Other cortical regions such as the dorsolateral prefrontal cortex and orbitofrontal cortex have yielded mixed results.91 Supplementally, rTMS has shown efficacy for reducing SI in approximately 40% of individuals with treatment-resistant depression.92 Significant reductions in SI have also been seen at the end of ECT treatment, in up to 80% of patients with depression.93 These treatments may impact SI independent of underlying diagnosis, which should be probed in future trials.
MST is a newer psychiatric intervention, and early pilot studies suggest this may not be useful for individuals with OCD until more appropriate stimulation targets are identified.94 Deep brain stimulation (DBS) targeting the ventral capsule/ventral striatum is additionally FDA-approved for treatment-resistant OCD.95 DBS requires surgical implantation and thus is only utilized in severe cases. In such cases, symptoms have been shown improve between 45% and 60% with response rates between 62% and 83%.96 Despite evident utility, the number of OCD patients treated with neurostimulation is relatively low. Due to the severity of symptoms and potential resistance to first-line treatments, neurostimulation may prove a valuable avenue for individuals suffering from OCD and SI. Answering the persisting questions regarding mechanisms of action for various stimulation modalities will yield a greater understanding of the symptomatology itself and burgeon support for implementing them into therapeutic practice.
Other Treatments
Neurosurgery is occasionally used in highly treatment-resistant OCD. This typically involves one of the two stereotactic ablation procedures: dorsal anterior cingulotomy and anterior capsulotomy.12 Considering the invasiveness and regulatory confinements, such procedures are uncommon and only recommended as a component of a comprehensive treatment plan including psychotherapeutic or pharmacological counterpart.97 Evidence does not point to one ablative procedure over the other in terms of symptom reduction. Little is known about the direct impact of neurosurgery on SI in OCD.
Summary
SI is highly correlated with OCD diagnosis, with varying degrees of increased risk based on the presence or absence of additional factors. SI can be particularly challenging to identify and accurately represent due to the potential repercussions associated with disclosure. This is supported by frequent reports of higher SA then SI, such as Nagy et al’s study indicating rates of 27% and 33% for SI and SA, respectively.9 Improving sensitivity of assessments and therapeutic settings to detect underreported SI is an important step for eventually treating SI. Further, due to the high frequency of comorbidities often accompanying OCD, it can be challenging to disentangle causal factors and the specific role of OCD in the experience of SI. Understanding mechanisms of OCD itself may further enlighten risk factors of SI. There are numerous important gaps in the current consensus of causal factors of OCD. Little consistent evidence has been accumulated for the contribution of genetics to the development of OCD. Additionally, there are numerous routes to the progression of symptoms; for instance, some children acutely develop OCD following a streptococcal infection with potential basal ganglia neurodegeneration.98 Due to the high heterogeneity of cognitive and behavioral phenotypes, it is plausible that what the DSM-5 currently conceptualizes as OCD, may represent multiple underlying neural disruptions. The two hallmark symptoms of OCD, obsessional thoughts and compulsive behavior, are not exclusive to OCD itself and can be found in several other psychiatric disorders. Therefore, understanding the relationship between particular symptom clusters and SI may be more fruitful for unveiling mechanisms of action. Neural correlates and underlying psychological mechanisms are not clearly established. Alterations in some structures and cognitive processes such as the orbitofrontal cortex and cognitive control have been implicated, but more evidence is needed. Research investigating mechanisms of OCD will not only help identify individuals at risk for SI but could also inform effective treatment procedures.
From the existing literature, the most prominent risk factors were indicated as those with a history of SI or SA, psychiatric comorbidities (particularly depression), symptoms that involve unacceptable or taboo thoughts, childhood trauma, significant life stress, and individuals with a high degree of reported distress. Individuals endorsing any of these risk factors should be closely monitored and screened for SI. Patients with a history of childhood trauma should receive thorough assessment for SI given the higher likelihood of SAs. Ultimately, thorough assessment of symptoms and screening for SI and risk factors is essential for the ability to detect suicidality and intervene when appropriate. Limited research has been dedicated to the treatment of SI within OCD. More research is required to clarify links between associations and unveil directionality. Enlightening connections between risk factors and SI in OCD will benefit both the SI and OCD. It is important to dedicate efforts towards better understanding treatment implications of SI within the context of OCD as well. Although effective treatments for both SI and OCD exist, the intersection of these two experiences is vastly understudied. Nuances of SI in OCD are not adequately captured by the current body of evidence. While SI may respond in a similar manner across psychiatric diagnoses, exploring unique features of SI within OCD is important for the development of effective treatment targets and interventions.
Disclosure
Dr Cory R Weissman reports consulting fees from Goodcap Pharmaceuticals, outside the submitted work. Dr Zafiris J Daskalakis reports grants from Magventure and Brainsway; and is part of the Scientific Advisory Board for Brainsway, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. American Psychiatric Association, American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
2. Pellegrini L, Maietti E, Rucci P, et al. Suicide attempts and suicidal ideation in patients with obsessive-compulsive disorder: a systematic review and meta-analysis. J Affect Disord. 2020;276:1001–1021. doi:10.1016/j.jad.2020.07.115
3. Veale D, Roberts A. Obsessive-compulsive disorder. BMJ. 2014;348(apr076):g2183–g2183. doi:10.1136/bmj.g2183
4. Kamath P, Reddy YCJ, Kandavel T. Suicidal behavior in obsessive-compulsive disorder. J Clin Psychiatry. 2007;68(11):20274. doi:10.4088/JCP.v68n1114
5. Gupta G, Avasthi A, Grover S, Singh SM. Factors associated with suicidal ideations and suicidal attempts in patients with obsessive compulsive disorder. Asian J Psychiatry. 2014;12:140–146. doi:10.1016/j.ajp.2014.09.004
6. Albert U, De Ronchi D, Maina G, Pompili M. suicide risk in obsessive-compulsive disorder and exploration of risk factors: a systematic review. Curr Neuropharmacol. 2019;17(8):681–696. doi:10.2174/1570159X16666180620155941
7. Lee MK, Hong JP, Fava M, et al. Obsessive thought, compulsive behavior, and their associations with suicide ideation and attempts and major depressive disorder: a nationwide community sample of Korean adults. J Nerv Ment Dis. 2021;209(11):820–828. doi:10.1097/NMD.0000000000001382
8. Brown LA, Wakschal E, Russman-Block S, et al. Directionality of change in obsessive compulsive disorder (OCD) and suicidal ideation over six years in a naturalistic clinical sample. J Affect Disord. 2019;245:841–847. doi:10.1016/j.jad.2018.11.006
9. Nagy NE, El-Serafi DM, Elrassas HH, Abdeen MS, Mohamed DA. Impulsivity, hostility and suicidality in patients diagnosed with obsessive compulsive disorder. Int J Psychiatry Clin Pract. 2020;24(3):284–292. doi:10.1080/13651501.2020.1773503
10. Klonsky ED, Dixon‐Luinenburg T, May AM. The critical distinction between suicidal ideation and suicide attempts. World Psychiatry. 2021;20(3):439–441. doi:10.1002/wps.20909
11. Memis CO, Dogan B, Sevincok D, Tunagur T, Memis SD, Sevincok L. Which factors may differentiate lifetime suicide attempters from ideators in obsessive-compulsive disorder patients? Indian J Psychiatry. 2020;62(4):392–399. doi:10.4103/psychiatry.IndianJPsychiatry_540_19
12. Goodman WK, Storch EA, Sheth SA. Harmonizing the neurobiology and treatment of obsessive-compulsive disorder. Am J Psychiatry. 2021;178(1):17–29. doi:10.1176/appi.ajp.2020.20111601
13. Szechtman H, Harvey BH, Woody EZ, Hoffman KL. The psychopharmacology of obsessive-compulsive disorder: a preclinical roadmap. Pharmacol Rev. 2020;72(1):80–151. doi:10.1124/pr.119.017772
14. Robbins TW, Vaghi MM, Banca P. Obsessive-compulsive disorder: puzzles and prospects. Neuron. 2019;102(1):27–47. doi:10.1016/j.neuron.2019.01.046
15. Arnold PD, Sicard T, Burroughs E, Richter MA, Kennedy JL. Glutamate transporter gene SLC1A1 associated with obsessive-compulsive disorder. Arch Gen Psychiatry. 2006;63(7):769–776. doi:10.1001/archpsyc.63.7.769
16. Geller DA, Homayoun S, Johnson G. Developmental considerations in obsessive compulsive disorder: comparing pediatric and adult-onset cases. Front Psychiatry. 2021;12:678538. doi:10.3389/fpsyt.2021.678538
17. Storch EA, Bussing R, Jacob ML, et al. Frequency and correlates of suicidal ideation in pediatric obsessive-compulsive disorder. Child Psychiatry Hum Dev. 2015;46(1):75–83. doi:10.1007/s10578-014-0453-7
18. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
19. Angelakis I, Gooding P, Tarrier N, Panagioti M. Suicidality in obsessive compulsive disorder (OCD): a systematic review and meta-analysis. Clin Psychol Rev. 2015;39:1–15. doi:10.1016/j.cpr.2015.03.002
20. Weissman CR, Hadas I, Yu D, et al. Predictors of change in suicidal ideation across treatment phases of major depressive disorder: analysis of the STAR*D data. Neuropsychopharmacology. 2021;46(7):1293–1299. doi:10.1038/s41386-020-00953-9
21. Sharma E, Sharma LP, Balachander S, et al. Comorbidities in obsessive-compulsive disorder across the lifespan: a systematic review and meta-analysis. Front Psychiatry. 2021;12:703701. doi:10.3389/fpsyt.2021.703701
22. Brakoulias V, Starcevic V, Belloch A, et al. Comorbidity, age of onset and suicidality in obsessive-compulsive disorder (OCD): an international collaboration. Compr Psychiatry. 2017;76:79–86. doi:10.1016/j.comppsych.2017.04.002
23. Kim H, Seo J, Namkoong K, et al. Alexithymia and perfectionism traits are associated with suicidal risk in patients with obsessive–compulsive disorder. J Affect Disord. 2016;192:50–55. doi:10.1016/j.jad.2015.12.018
24. Khosravani V, Kamali Z, Jamaati Ardakani R, Samimi Ardestani M. The relation of childhood trauma to suicide ideation in patients suffering from obsessive-compulsive disorder with lifetime suicide attempts. Psychiatry Res. 2017;255:139–145. doi:10.1016/j.psychres.2017.05.032
25. Hellberg SN, Buchholz JL, Ojalehto HJ, Butcher MW, Riemann BC, Abramowitz JS. Prevalence and correlates of suicidality in obsessive-compulsive disorder. J Obsessive-Compuls Relat Disord. 2022;32:100711. doi:10.1016/j.jocrd.2022.100711
26. Isometsä E. Suicidal behaviour in mood disorders—who, when, and why? Can J Psychiatry Rev Can Psychiatr. 2014;59(3):120–130. doi:10.1177/070674371405900303
27. Demirkol ME, Namlı Z, Eriş Davul Ö, Karaytuğ MO, Tamam L, Yılmaz H. Psychache and suicidal history in patients with obsessive-compulsive disorder. Neuropsychiatr Dis Treat. 2019;15:3531–3539. doi:10.2147/NDT.S237369
28. Breet E, Kidd M, McGregor NW, Stein DJ, Lochner C. Suicide ideation and attempts in obsessive-compulsive disorder. Ann Clin Psychiatry off J Am Acad Clin Psychiatr. 2019;31(3):192–199.
29. Apter A, Horesh N, Gothelf D, et al. Depression and suicidal behavior in adolescent inpatients with obsessive compulsive disorder. J Affect Disord. 2003;75(2):181–189. doi:10.1016/S0165-0327(02)00038-1
30. Cervin M, Do Rosário MC, Fontenelle LF, et al. Taboo obsessions and their association with suicidality in obsessive-compulsive disorder. J Psychiatr Res. 2022;154:117–122. doi:10.1016/j.jpsychires.2022.07.044
31. Alonso P, Segalàs C, Real E, et al. Suicide in patients treated for obsessive–compulsive disorder: a prospective follow-up study. J Affect Disord. 2010;124(3):300–308. doi:10.1016/j.jad.2009.12.001
32. Eskander N, Limbana T, Khan F. Psychiatric comorbidities and the risk of suicide in obsessive-compulsive and body dysmorphic disorder. Cureus. 2020;12(8):e9805. doi:10.7759/cureus.9805
33. Fernández de la Cruz L, Rydell M, Runeson B, et al. Suicide in obsessive-compulsive disorder: a population-based study of 36 788 Swedish patients. Mol Psychiatry. 2017;22(11):1626–1632. doi:10.1038/mp.2016.115
34. Benatti B, Ferrari S, Grancini B, et al. Suicidal ideation and suicidal attempts in patients with obsessive-compulsive tic-related disorder vs obsessive-compulsive disorder: results of a multicenter Italian study. CNS Spectr. 2021;26(4):354–361. doi:10.1017/S1092852920001157
35. De La Vega D, Giner L, Courtet P. Suicidality in subjects with anxiety or obsessive-compulsive and related disorders: recent advances. Curr Psychiatry Rep. 2018;20(4):26. doi:10.1007/s11920-018-0885-z
36. Han S, Xu Y, Guo HR, et al. Two distinct subtypes of obsessive compulsive disorder revealed by heterogeneity through discriminative analysis. Hum Brain Mapp. 2022;43(10):3037–3046. doi:10.1002/hbm.25833
37. Miguel EC, Leckman JF, Rauch S, et al. Obsessive-compulsive disorder phenotypes: implications for genetic studies. Mol Psychiatry. 2005;10(3):258–275. doi:10.1038/sj.mp.4001617
38. Cameron DH, Streiner DL, Summerfeldt LJ, Rowa K, McKinnon MC, McCabe RE. A comparison of cluster and factor analytic techniques for identifying symptom-based dimensions of obsessive-compulsive disorder. Psychiatry Res. 2019;278:86–96. doi:10.1016/j.psychres.2019.05.040
39. Velloso P, Piccinato C, Ferrão Y, et al. The suicidality continuum in a large sample of obsessive–compulsive disorder (OCD) patients. Eur Psychiatry. 2016;38:1–7. doi:10.1016/j.eurpsy.2016.05.003
40. Sehlo MG, Youssef UM, El-Gohari HM. Prevalence and risk factors of suicidal ideations among patients with obsessive-compulsive disorder in Egypt. Middle East Curr Psychiatry. 2021;28(1):9. doi:10.1186/s43045-021-00087-8
41. Krebs G, Mataix-Cols D, Rijsdijk F, et al. Concurrent and prospective associations of obsessive-compulsive symptoms with suicidality in young adults: a genetically-informative study. J Affect Disord. 2021;281:422–430. doi:10.1016/j.jad.2020.10.065
42. Storch EA, Kay B, Wu MS, Nadeau JM, Riemann B. Suicidal and death ideation among adults with obsessive-compulsive disorder presenting for intensive intervention. Ann Clin Psychiatry off J Am Acad Clin Psychiatr. 2017;29(1):46–53.
43. Kim ST, Seo JH, Park CI, et al. core clinical symptoms and suicidal ideation in patients with obsessive-compulsive disorder: a network analysis. Psychiatry Clin Neurosci. 2022. doi:10.1111/pcn.13503
44. Weingarden H, Renshaw KD, Wilhelm S, Tangney JP, DiMauro J. Anxiety and shame as risk factors for depression, suicidality, and functional impairment in body dysmorphic disorder and obsessive compulsive disorder. J Nerv Ment Dis. 2016;204(11):832–839. doi:10.1097/NMD.0000000000000498
45. Khosravani V, Samimi Ardestani M, Sharifi Bastan F, Kamali Z. The relationship between alexithymia and symptom dimensions in patients with obsessive-compulsive disorder. J Obsessive-Compuls Relat Disord. 2017;14:127–133. doi:10.1016/j.jocrd.2017.04.001
46. De Berardis D, Serroni N, Campanella D, et al. Alexithymia, responsibility attitudes and suicide ideation among outpatients with obsessive-compulsive disorder: an exploratory study. Compr Psychiatry. 2015;58:82–87. doi:10.1016/j.comppsych.2014.12.016
47. De Berardis D, Fornaro M, Orsolini L, et al. Alexithymia and suicide risk in psychiatric disorders: a mini-review. Front Psychiatry. 2017;8:148. doi:10.3389/fpsyt.2017.00148
48. Shneidman ES. Commentary: suicide as psychache. J Nerv Ment Dis. 1993;181(3):145–147. doi:10.1097/00005053-199303000-00001
49. Verrocchio MC, Carrozzino D, Marchetti D, Andreasson K, Fulcheri M, Bech P. Mental pain and suicide: a systematic review of the literature. Front Psychiatry. 2016;7:108. doi:10.3389/fpsyt.2016.00108
50. Agne NA, Tisott CG, Ballester P, Passos IC, Ferrão YA. Predictors of suicide attempt in patients with obsessive-compulsive disorder: an exploratory study with machine learning analysis. Psychol Med. 2022;52(4):715–725. doi:10.1017/S0033291720002329
51. Angelakis I, Gooding P. Obsessive–compulsive disorder and suicidal experiences: the role of experiential avoidance. Suicide Life Threat Behav. 2020;50(2):359–371. doi:10.1111/sltb.12593
52. Oquendo MA, Sullivan GM, Sudol K, et al. Toward a Biosignature for Suicide. Am J Psychiatry. 2014;171(12):1259–1277. doi:10.1176/appi.ajp.2014.14020194
53. Bramante S, Maina G, Borgogno R, Pellegrini L, Rigardetto S, Albert U. Assessing suicide risk in patients with obsessive-compulsive disorder: a dimensional approach. Rev Bras Psiquiatr Sao Paulo Braz. 2022. doi:10.47626/1516-4446-2022-2632
54. Torres AR, Ramos-Cerqueira ATA, Ferrão YA, Fontenelle LF, Rosári O, Miguel EC. Suicidality in obsessive-compulsive disorder: prevalence and relation to symptom dimensions and comorbid conditions. J Clin Psychiatry. 2011;72(1):20314. doi:10.4088/JCP.09m05651blu
55. Dell’Osso B, Nicolini H, Lanzagorta N, et al. Cigarette smoking in patients with obsessive compulsive disorder: a report from the international college of obsessive compulsive spectrum disorders (ICOCS). CNS Spectr. 2015;20(5):469–473. doi:10.1017/S1092852915000565
56. Bejerot S, Knorring L, Ekselius L. Personality traits and smoking in patients with obsessive-compulsive disorder. Eur Psychiatry. 2000;15(7):395–401. doi:10.1016/S0924-9338(00)00509-5
57. Sharma P, Gale TM, Fineberg NA. Clinical correlates of tobacco smoking in OCD: a UK, case-controlled, exploratory analysis. J Behav Addict. 2012;1(4):180–185. doi:10.1556/jba.1.2012.008
58. Angelakis I, Gooding P. Adverse social relationships in childhood: are there links with depression, obsessive-compulsive disorder and suicidality in adulthood? Child Psychiatry Hum Dev. 2021;52(5):945–956. doi:10.1007/s10578-020-01077-3
59. Khosravani V, Samimi Ardestani SM, Sharifi Bastan F, McKay D, Asmundson GJG. The associations of obsessive–compulsive symptom dimensions and general severity with suicidal ideation in patients with obsessive–compulsive disorder: the role of specific stress responses to COVID‐19. Clin Psychol Psychother. 2021;28(6):1391–1402. doi:10.1002/cpp.2602
60. Ay R, Erbay LG. Relationship between childhood trauma and suicide probability in obsessive-compulsive disorder. Psychiatry Res. 2018;261:132–136. doi:10.1016/j.psychres.2017.12.054
61. Rajabi Khamesi S, Najafi M, Khosravani V. The effect of childhood maltreatment on suicidal ideation through cognitive emotion regulation strategies and specific obsessive–compulsive symptoms in obsessive–compulsive disorder. Clin Psychol Psychother. 2021;28(6):1435–1444. doi:10.1002/cpp.2582
62. Khosravani V, Sharifi Bastan F, Samimi Ardestani M, Jamaati Ardakani R. Early maladaptive schemas and suicidal risk in an Iranian sample of patients with obsessive-compulsive disorder. Psychiatry Res. 2017;255:441–448. doi:10.1016/j.psychres.2017.06.080
63. Fontenelle LF, Cocchi L, Harrison BJ, et al. Towards a post-traumatic subtype of obsessive–compulsive disorder. J Anxiety Disord. 2012;26(2):377–383. doi:10.1016/j.janxdis.2011.12.001
64. Gershuny BS, Baer L, Parker H, Gentes EL, Infield AL, Jenike MA. Trauma and posttraumatic stress disorder in treatment-resistant obsessive-compulsive disorder. Depress Anxiety. 2008;25(1):69–71. doi:10.1002/da.20284
65. Boger S, Ehring T, Berberich G, Werner GG. Impact of childhood maltreatment on obsessive-compulsive disorder symptom severity and treatment outcome. Eur J Psychotraumatology. 2020;11(1):1753942. doi:10.1080/20008198.2020.1753942
66. Paul S, Simon D, Endrass T, Kathmann N. Altered emotion regulation in obsessive–compulsive disorder as evidenced by the late positive potential. Psychol Med. 2016;46(1):137–147. doi:10.1017/S0033291715001610
67. Sidorchuk A, Kuja-Halkola R, Runeson B, et al. Genetic and environmental sources of familial coaggregation of obsessive-compulsive disorder and suicidal behavior: a population-based birth cohort and family study. Mol Psychiatry. 2021;26(3):974–985. doi:10.1038/s41380-019-0417-1
68. Zalsman G, Hawton K, Wasserman D, et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry. 2016;3(7):646–659. doi:10.1016/S2215-0366(16)30030-X
69. Szmulewicz AG, Smith JM, Valerio MP. Suicidality in clozapine-treated patients with schizophrenia: role of obsessive-compulsive symptoms. Psychiatry Res. 2015;230(1):50–55. doi:10.1016/j.psychres.2015.07.089
70. Kim DD, Barr AM, Lu C, et al. Clozapine-associated obsessive-compulsive symptoms and their management: a systematic review and analysis of 107 reported cases. Psychother Psychosom. 2020;89(3):151–160. doi:10.1159/000505876
71. Boaden K, Tomlinson A, Cortese S, Cipriani A. Antidepressants in children and adolescents: meta-review of efficacy, tolerability and suicidality in acute treatment. Front Psychiatry. 2020;11:717. doi:10.3389/fpsyt.2020.00717
72. Brown GK, Jager-Hyman S. Evidence-based psychotherapies for suicide prevention: future directions. Am J Prev Med. 2014;47(3,Supplement 2):S186–S194. doi:10.1016/j.amepre.2014.06.008
73. Öst LG, Havnen A, Hansen B, Kvale G. Cognitive behavioral treatments of obsessive-compulsive disorder. A systematic review and meta-analysis of studies published 1993–2014. Clin Psychol Rev. 2015;40:156–169. doi:10.1016/j.cpr.2015.06.003
74. Angelakis I, Austin JL. The effects of the non-contingent presentation of safety signals on the elimination of safety behaviors: an experimental comparison between individuals with low and high obsessive-compulsive profiles. J Behav Ther Exp Psychiatry. 2018;59:100–106. doi:10.1016/j.jbtep.2017.12.005
75. Allen KJD, Krompinger JW, Mathes BM, Crosby JM, Elias JA. Thought control strategies in patients with severe obsessive–compulsive disorder: treatment effects and suicide risk. J Obsessive-Compuls Relat Disord. 2016;8:31–37. doi:10.1016/j.jocrd.2015.11.004
76. Wetterneck CT, Williams MT, Tellawi G, Bruce SL. Treatment of Suicide Obsessions in Obsessive-Compulsive Disorder with Comorbid Major Depressive Disorder. In: Storch EA, Lewin AB editors. Clinical Handbook of Obsessive-Compulsive and Related Disorders: A Case-Based Approach to Treating Pediatric and Adult Populations. Springer International Publishing; 2016:431–445. doi:10.1007/978-3-319-17139-5_29
77. Stübner S, Grohmann R, Greil W, et al. Suicidal ideation and suicidal behavior as rare adverse events of antidepressant medication: current report from the AMSP multicenter drug safety surveillance project. Int J Neuropsychopharmacol. 2018;21(9):814–821. doi:10.1093/ijnp/pyy048
78. Pittenger C, Bloch MH. Pharmacological treatment of obsessive-compulsive disorder. Psychiatr Clin North Am. 2014;37(3):375–391. doi:10.1016/j.psc.2014.05.006
79. Richter PMA, Ramos RT. Obsessive-compulsive disorder. Contin Minneap Minn. 2018;24:828–844. doi:10.1212/CON.0000000000000603
80. Katz RJ, DeVeaugh-Geiss J, Landau P. Clomipramine in obsessive-compulsive disorder. Biol Psychiatry. 1990;28(5):401–414. doi:10.1016/0006-3223(90
81. Bloch MH, McGuire J, Landeros-Weisenberger A, Leckman JF, Pittenger C. Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder. Mol Psychiatry. 2010;15(8):850–855. doi:10.1038/mp.2009.50
82. Goddard AW, Shekhar A, Whiteman AF, McDougle CJ. Serotonergic mechanisms in the treatment of obsessive–compulsive disorder. Drug Discov Today. 2008;13(7):325–332. doi:10.1016/j.drudis.2007.12.009
83. Nischal A, Tripathi A, Nischal A, Trivedi JK. Suicide and antidepressants: what current evidence indicates. Mens Sana Monogr. 2012;10(1):33–44. doi:10.4103/0973-1229.87287
84. Read J, Williams J. Adverse Effects of Antidepressants Reported by a Large International Cohort: emotional Blunting, Suicidality, and Withdrawal Effects. Curr Drug Saf. 2018;13(3):176–186. doi:10.2174/1574886313666180605095130
85. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297(15):1683–1696. doi:10.1001/jama.297.15.1683
86. Zeifman RJ, Wagner AC, Watts R, Kettner H, Mertens LJ, Carhart-Harris RL. Post-psychedelic reductions in experiential avoidance are associated with decreases in depression severity and suicidal ideation. Front Psychiatry. 2020;11:782. doi:10.3389/fpsyt.2020.00782
87. Baeken C, Wu GR, van Heeringen K. Placebo aiTBS attenuates suicidal ideation and frontopolar cortical perfusion in major depression. Transl Psychiatry. 2019;9(1):38. doi:10.1038/s41398-019-0377-x
88. Weissman CR, Blumberger DM, Dimitrova J, et al. Magnetic seizure therapy for suicidality in treatment-resistant depression. JAMA Netw Open. 2020;3(8):e207434. doi:10.1001/jamanetworkopen.2020.7434
89. Roth Y, Tendler A, Arikan MK, et al. Real-world efficacy of deep TMS for obsessive-compulsive disorder: post-marketing data collected from twenty-two clinical sites. J Psychiatr Res. 2021;137:667–672. doi:10.1016/j.jpsychires.2020.11.009
90. Bergfeld IO, Dijkstra E, Graat I, et al. Invasive and non-invasive neurostimulation for OCD. In: Fineberg NA, Robbins TW, editors. The Neurobiology and Treatment of OCD: Accelerating Progress. Current Topics in Behavioral Neurosciences. Springer International Publishing; 2021:399–436. doi:10.1007/7854_2020_206
91. Carmi L, Tendler A, Bystritsky A, et al. Efficacy and safety of deep transcranial magnetic stimulation for obsessive-compulsive disorder: a prospective multicenter randomized double-blind placebo-controlled trial. Am J Psychiatry. 2019;176(11):931–938. doi:10.1176/appi.ajp.2019.18101180
92. Weissman CR, Blumberger DM, Brown PE, et al. Bilateral repetitive transcranial magnetic stimulation decreases suicidal ideation in depression. J Clin Psychiatry. 2018;79(3):5831. doi:10.4088/JCP.17m11692
93. Kellner CH, Fink M, Knapp R, et al. Relief of expressed suicidal intent by ECT: a consortium for research in ECT study. Am J Psychiatry. 2005;162(5):977–982. doi:10.1176/appi.ajp.162.5.977
94. Tang VM, Blumberger DM, Weissman CR, et al. A pilot study of magnetic seizure therapy for treatment-resistant obsessive-compulsive disorder. Depress Anxiety. 2021;38(2):161–171. doi:10.1002/da.23097
95. Nuttin B, Cosyns P, Demeulemeester H, Gybels J, Meyerson B. Electrical stimulation in anterior limbs of internal capsules in patients with obsessive-compulsive disorder. Lancet Lond Engl. 1999;354(9189):1526. doi:10.1016/S0140-6736(99
96. Acevedo N, Bosanac P, Pikoos T, Rossell S, Castle D. Therapeutic neurostimulation in obsessive-compulsive and related disorders: a systematic review. Brain Sci. 2021;11(7):948. doi:10.3390/brainsci11070948
97. Balachander S, Arumugham SS, Srinivas D. Ablative neurosurgery and deep brain stimulation for obsessive-compulsive disorder. Indian J Psychiatry. 2019;61(Suppl 1):S77–S84. doi:10.4103/psychiatry.IndianJPsychiatry_523_18
98. Williams KA, Swedo SE. Post-infectious autoimmune disorders: sydenham’s chorea, PANDAS and beyond. Brain Res. 2015;1617:144–154. doi:10.1016/j.brainres.2014.09.071
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.