Back to Journals » Psychology Research and Behavior Management » Volume 15
Suicidal Behavior Among Elderly Inpatients: its Relation to Functional Disability and Pain
Authors Wahab S ![]() , Chua TY, Razali R, Mat Saher Z, Zamzam IH, Bujang MA
, Chua TY, Razali R, Mat Saher Z, Zamzam IH, Bujang MA ![]()
Received 28 September 2021
Accepted for publication 8 January 2022
Published 24 March 2022 Volume 2022:15 Pages 737—750
DOI https://doi.org/10.2147/PRBM.S341768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Suzaily Wahab,1 Tien Yong Chua,2 Rosdinom Razali,1 Zanariah Mat Saher,3 Iman Hakimi Zamzam,1 Mohamad Adam Bujang4
1Department of Psychiatry, Universiti Kebangsaan Malaysia Medical Centre, Cheras, Wilayah Persekutuan Kuala Lumpur, 56000, Malaysia; 2Department of Psychiatry and Mental Health, Hospital Bintulu, Bintulu, 97000, Sarawak, Malaysia; 3Department of Psychiatry and Mental Health, Hospital Kuala Lumpur, Kuala Lumpur, Wilayah Persekutuan Kuala Lumpur, 50586, Malaysia; 4Clinical Research Centre, Sarawak General Hospital, Kuching, 93586, Sarawak, Malaysia
Correspondence: Suzaily Wahab, Department of Psychiatry, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaacob Latif, Cheras, 56000, Wilayah Persekutuan Kuala Lumpur, Malaysia, Email [email protected]
Background: Suicidal behavior (SB) among elderly inpatients has exhibited a growing global drift. This study aimed to establish the prevalence of SB among elderly inpatients and identify the relationship between SB and depression and functional disability.
Methods: This cross-sectional study included 136 randomly selected elderly inpatients aged 60 years and older who were hospitalized in a tertiary referral center in Kuala Lumpur, Malaysia. The study utilized the following scales as the assessment tools: The Columbia Suicide Severity Rating Scale (CSSRS), Geriatric Depression Scale (GDS-15), Mini International Neuropsychiatric Interview (M.I.N.I.), the Modified Barthel Index (Shah version) (MBI), and visual analog scale.
Results: The rates of current major depressive disorder (MDD), recurrent MDD, passive suicidal ideation (SI), and active SI were 24.3%, 8.8%, 27.9%, and 5.9%, respectively. Depressed elderly had 6 to 17 times higher risk of developing passive or active SI. “Wish to be dead,” ie, passive SI was associated with admission to oncology or surgical ward and the presence of current MDD. The findings of the study revealed that active SI was associated with being over 80 years old (p = 0.027), being single (p = 0.042), admission to the oncology ward (p = 0.012) or orthopedic ward (p = 0.032), having positive GDS (p = 0.049), and the presence of current MDD (p = 0.019) or recurrent MDD (p = 0.010). According to the study findings, no association has been observed between passive and active SI and level of independence and acute pain.
Conclusion: The risk of depressed elderly inpatients having passive and active SI is high. Hence, screening for depression and SI is crucial for prompt treatment and management.
Keywords: depression, elderly, functional disability, pain, suicidal behavior
Introduction
In the last few decades, the proportion of global aging population has increased considerably. According to “An Aging World 2015” report by He et al, the percentage of those aged 65 years and above has reached 8.5%. This figure is projected to rise to 17% by 2050.1 As a rapidly growing and developing country, Malaysia’s population is not aging as fast as those of developed countries such as Japan, Italy, and Germany. However, in 2021, the percentage of elderly population (over 65 years old) was 7.4%, with an increase of 0.4% compared to 2020.2 It is predicted that the current aging population in Malaysia, ie, 7%, will witness a two-fold rise by 2043.3 The 7% threshold of the total population aged 65 is indicative of an aged-nation status.
In the last few years, suicidal behavior (SB), including suicidal ideation (SI) and attempts among the elderly has witnessed an increasing trend globally. Studies show that suicide is the 10th leading cause of death in the United States, and one completed suicide was reported for every four suicidal attempts in the elderly. A suicide-related death is reported every 40 seconds. SI can be categorized as active and passive ideation. Active SI refers to the situation when the patients purposely want to end their lives through their actions, while passive SI refers to the situation when the patients have desire for death and refuse to take any measures to continue their lives.4 The latter ideation is more common among the older age group, with lifetime prevalence rates between 18.7% to 40.9%.5 However, active and passive SI can have similar manifestations in the elderly, and both conditions can alternate with each other.5 It is a well-known fact that depression is a potential risk factor for SB, commonly found among the elderly. However, the prevalence of major depressive disorder (MDD) varies according to several factors, including the living environment. The prevalence ranged from 0.9% to 9.4% in private households and from 14% to 42% in institutional living.6 In the elderly population, it was observed that the depression rate is higher amongst those with underlying long-standing medical conditions.7,8 As a result, it exacerbates the patient’s medical symptom burden and increases morbidity and mortality.9
Another identified risk factor for SI is unendurable pain.10 Chronic pain, such as back pain, is a common type of pain among the elderly. It has been noted that approximately half of the elderly suffer from chronic back pain at the age of 70.11 A cohort study conducted in Japan showed that completed suicide in men is associated with such pain.12 A possibility for this association is that hopelessness, as an element of demoralization, often seen in the elderly with chronic pain predisposes them to SB.13 This is further highlighted by Clarke and Kissane (2002) that demoralization, even in the absence of depression, is a strong independent factor contributing to suicidal ideation.14
A high level of activity of daily living dependency is also associated with high suicide risk, regardless of depression.15 Previous studies have found considerable relationship between the elderly dependency ratios and the elderly suicide rates in both genders. The presence of younger caretakers who provide moral support and keep the elderly in high esteem would reduce the risk of suicide in the elderly.16,17 However, elderly individuals often perceive themselves as a burden to others, especially family members.18 They might choose to end their lives to alleviate the responsibilities and difficulties of their loved ones.
There is a dearth of concrete research findings concerning SB among the elderly in the local community. Even though the association between SI and depression is well established, this study delves into SI in further details such as the presence of active versus passive SI, presence of suicidal intention, frequency and duration of SI, controllability, deterrents, and reasons for suicide. Although elderly depressed patients with passive or active SI had a similar level of hopelessness, those with active SI had higher depression scores, more self-hatred, and more self-dissatisfaction,19 rendering them a higher risk group. Frequency and duration of SI,20 controllability of suicide,21 and deterrents of suicide,22 were all found to be associated with risks of suicidal act.
This research aimed to investigate the prevalence of SB among elderly inpatients and study the relationship between SB and socio-demographic factors, depression, and functional disability.
Methods
This study was conducted at a tertiary referral hospital that receives referrals from all nearby hospitals and primary healthcare centers in the Klang Valley. The selected hospital caters to 83 wards and 2300 beds, providing most of the medical specialties and facilities.
Study Participants
The daily new admissions of elderly patients from June 1, 2017 to August 31, 2017, were identified through the primary hospital admission registry. All participants meeting the inclusion criteria were included in the list for randomization. Patient selection was based on a computer randomly generated number each day. The patients were recruited until the desired sample size was achieved.
Inclusion criteria were inpatients who were (1) 60 years of age and older, (2) able to understand, communicate, read, and write in English or Malay, (3) able to give their informed consent, and (4) from either medical, surgical, orthopedic, oncology, or multi-disciplinary wards of the hospital. Exclusion criteria were patients who were (1) diagnosed to have delirium or major neurocognitive disorders, (2) having severe hearing or vision impairment, and (3) having critically ill conditions (on ventilated support or in high-dependency units).
The approval for this research was obtained from the Institutional Research Ethics Committee and National Medical Research Register, Malaysia. Further approval was obtained from the Director of the hospital and the Head of the Department of the respective units involved in the study. Written consent was requested from all the participants. Patients diagnosed with depression or SB were referred to the psychogeriatric team for further assessment and management.
Data Collection
The patients were interviewed by the researcher on the second day of their hospitalization. Depending on the patient’s condition, short breaks were allowed during the data collection process and minimal guidance was provided by the researcher.
Instruments
Socio-demographic and clinical data of the patients were obtained from the patients and their medical records. The researcher was trained by an experienced consultant psychogeriatrician in using the Geriatric Depression Scale 15 (GDS-15), Mini International Neuropsychiatric Interview (MINI) – major depressive episode, and Modified Barthel Index, or MBI (Shah version). Before administering the questionnaires, the researcher also completed the online training and certification of Columbia Suicide Severity Rating Scale (C-SSRS). Permission to use all tools was obtained from all their respective developers.
C-SSRS
The C-SSRS is considered a definitive suicidal rating scale and is widely used across research and clinical practices internationally, including for patients older than 60 years.23,24 It is an interviewer-rated scale. The validity of C-SSRS was determined with high sensitivity and specificity for SI.25 It utilizes a scale of 1–5 with increasing severity from “a wish to die” to “the active ideation of suicide with plan and intent.” The patients were assessed for the presence of any SI and behavior for the past six months. A translated Malay version of the C-SSRS (https://www.cssrs.columbia.edu) was used for patients fluent in Malay.
GDS-15
The 15-item GDS-15, a self-rated questionnaire, is a screening tool for depressive symptoms in the elderly. Furthermore, the accuracy of the GDS-15 is not affected by the severity of medical burden, age, or other socio-demographic characteristics, even in a medically ill and disabled patient population.26 Furthermore, GDS-15 has acceptable sensitivity and specificity to distinguish between depressed and non-depressed patients.27 The study used a validated 14-item scale Malay version of GDS-15 with a Cronbach alpha value of 0.84.28 If the GDS-15 score is 5 or above, MINI will then be used to diagnose the underlying depressive disorder.
MINI
The MINI is a short diagnostic structured interview, which can provide reliable diagnostic and statistical manual (DSM) diagnoses within a short time frame,29 administered by the researcher (interviewer-rated) on the patient. The MINI was validated according to comparison with Composite International Diagnostic Interview and Structured Clinical Interview for DSM-III-R-Patient version (SCID-P)30,31 and was employed to diagnose the patients with major depressive episodes.
MBI (Shah Version)
Various studies have examined the level of dependence using the Barthel index, a well-established and commonly used nursing tool.32 In this study, the Shah version of MBI was used. The MBI has improved sensitivity and reliability compared to its original version. The internal consistency reliability coefficient for the modified score of the Barthel Index was 0.90 compared to 0.87 for the original score.33 MBI objectively assesses functional independence in activities of daily living.
Visual Analog Scale (VAS) of Pain
One of the most frequently used tools for pain measurement is the VAS of pain. This is a validated scale for estimating variations in intensity of pain experienced by the patients.34 The VAS of pain is shown to the patient to highlight the severity of pain during the assessment.
Statistical Analysis
The sample size was calculated based on a local systematic review of SI among the general population, with a lifetime prevalence of 8.0%.35 Hence, the sample size was 136 (with a precision of 5%), including anticipation of a 20% non-responsive rate.
All the categorical variables were reported as frequency and its percentage. A simple logistic regression was used to determine the association between independent variables and the outcome of “wish to be dead” and active SI, reporting the odds ratio and its 95% confidence interval. A multiple logistic regression analysis (forward logistic regression) was then conducted with the “wish to be dead” ideation outcome. Simple logistic regression was performed to examine the association between the independent variables and active SI among the elderly inpatients . The Mann–Whitney U-test was performed to determine the difference in the pain score between the SI groups.
P values less than 0.05 were considered statistically significant for all analyses. Analyses were performed using Statistical Package for the Social Sciences (SPSS) software version 22.
Results
All 136 inpatients approached for the study were successfully enrolled and completed the questionnaires.
The socio-demographic data and medical conditions are summarized in Tables 1 and 2. Reasons for hospitalization were classified according to Muskoka and Ontario.36 The three most common reasons for hospitalizations were genitourinary (19.1%), respiratory (15.4%), and neoplastic (14.7%) disorders (Table 2). Most of the patients were admitted into the medical wards (51.5%) for less than a week (61%) and they suffered from their illnesses for less than 10 years (46.3%).
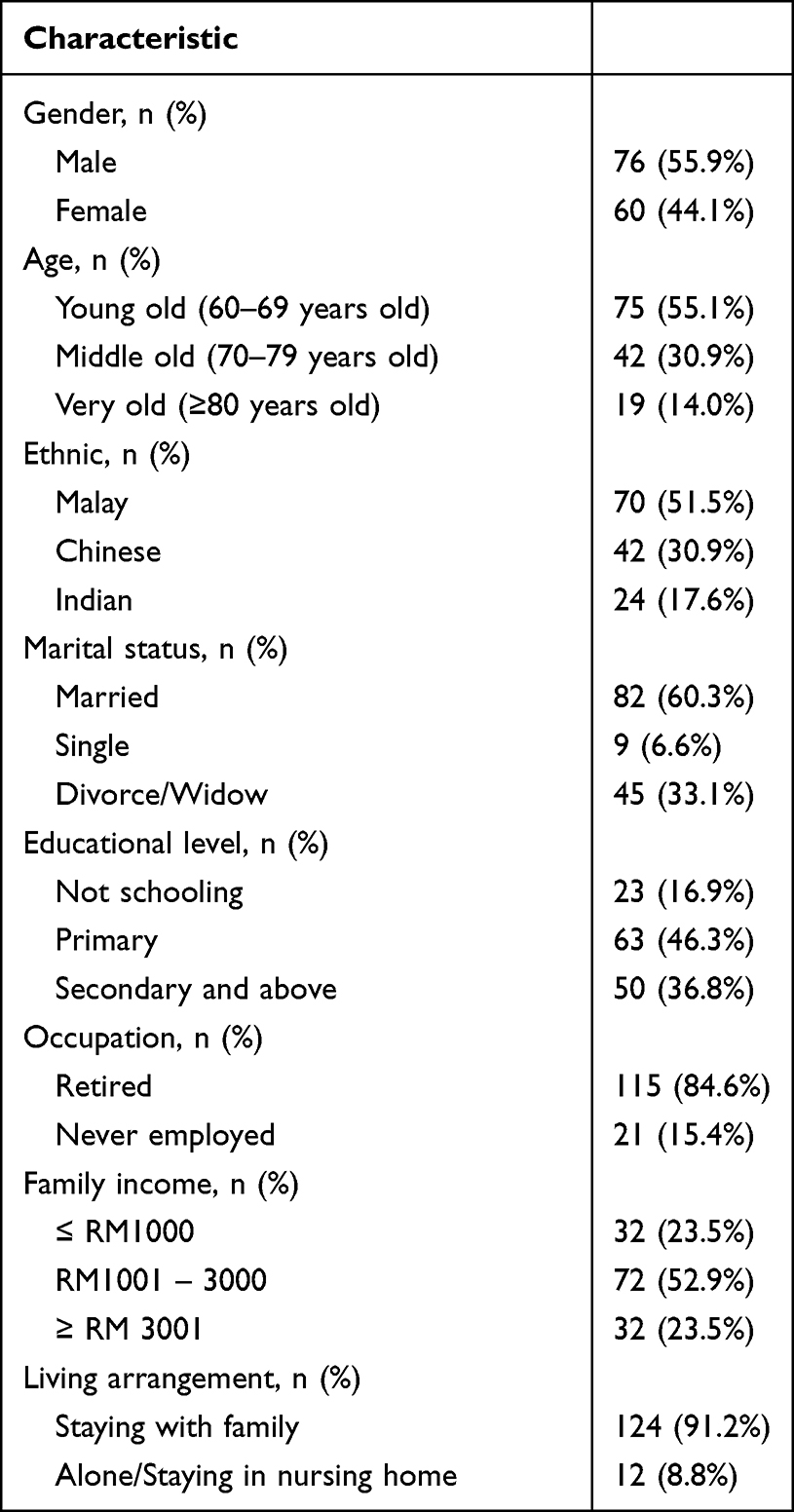 |
Table 1 Socio-Demographic Data of the Study Population (N=136) |
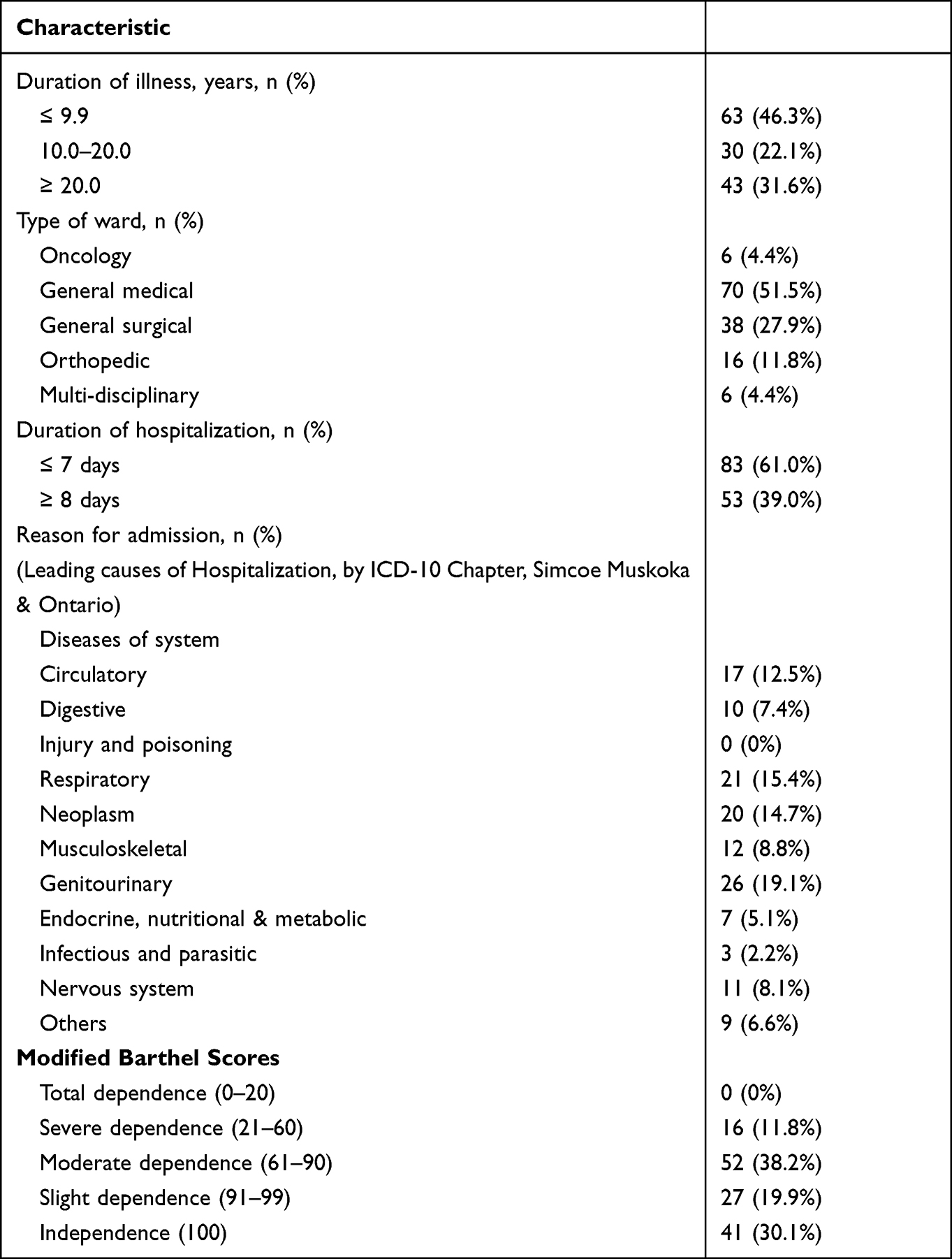 |
Table 2 General Medical Condition of the Study Population (N=136) |
The elderly inpatients’ level of independence was assessed based on MBI scores. Almost one-third of the elderly patients (30.1%) showed high scores, indicating independence of assistance in their daily activities. Most of those who needed physical assistance were moderately dependent on others for their daily activities (38.2%). However, none of them were totally dependent.
In this study, the prevalence of MDD among the elderly inpatients in this hospital was 24.3% for the current major depressive episode and 8.8% for recurrent major depressive episodes.
The frequency of elderly inpatients having “wish to be dead” was 38 (27.9%) during current ward admissions (Table 3). Only eight (5.9%) of 38 elderly inpatients having “wish to be dead” had active SI. Active SI were always with the method (5.9%), without any suicidal intention and a specific plan. The methods reported by these patients were drug overdose, jumping from a height, or hanging themselves. Most of them had SI less than once a week (60.5%), and the duration usually lasted for only a few seconds or minutes (86.9%). Among them, 63.2% found it easy to control the SI, and the deterrents prevented 60.5% from attempting suicide. The majority of them had SI to stop the existing pain (63.2%). No SB (attempt and self-injurious behavior) was reported in this study population in the past six months.
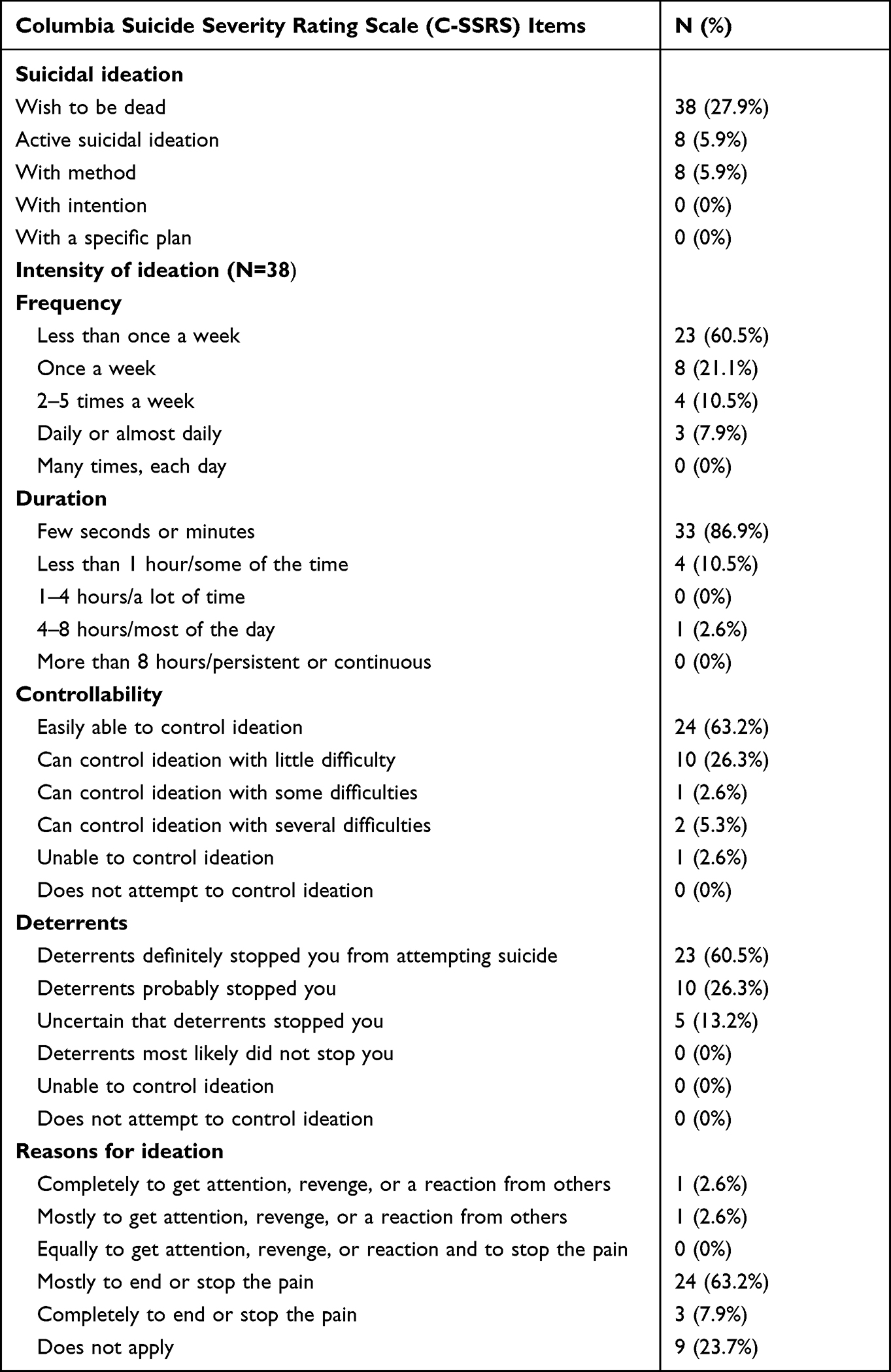 |
Table 3 Suicidal Ideation (C-SSRS) Among the Study Population |
Surprisingly, through crude and adjusted analyses of the socio-demographic data, none of the independent variables, including gender, age, marital status, race, educational level, occupation, family income, and living arrangement, were associated with the wish to be dead. However, those very old and single elderly patients were at risk of having active SI (p = 0.027 and p = 0.042, respectively).
Regarding the general medical conditions, the independent variables that were significantly associated with the desire for death were oncology ward, surgical ward, and current MDD. Compared to the medical ward, patients in the oncology and surgical wards were at risk of having this desire with the aOR = 37.79 and 4.42, respectively. Patients with current MDD had 17 times higher risk (aOR = 16.52) for having desire for death compared to non-current patients with MDD (Table 4). The “wish to be dead” and active SI were significantly related to depression while unrelated to the level of dependency (Tables 4 and 5). Independent variables associated with active SI were admission to oncology ward (p = 0.012), orthopedic ward (p = 0.032), positive GDS (p = 0.049), current MDD (p = 0.019), and recurrent MDD (p = 0.010) in the simple logistic regression (Table 5).
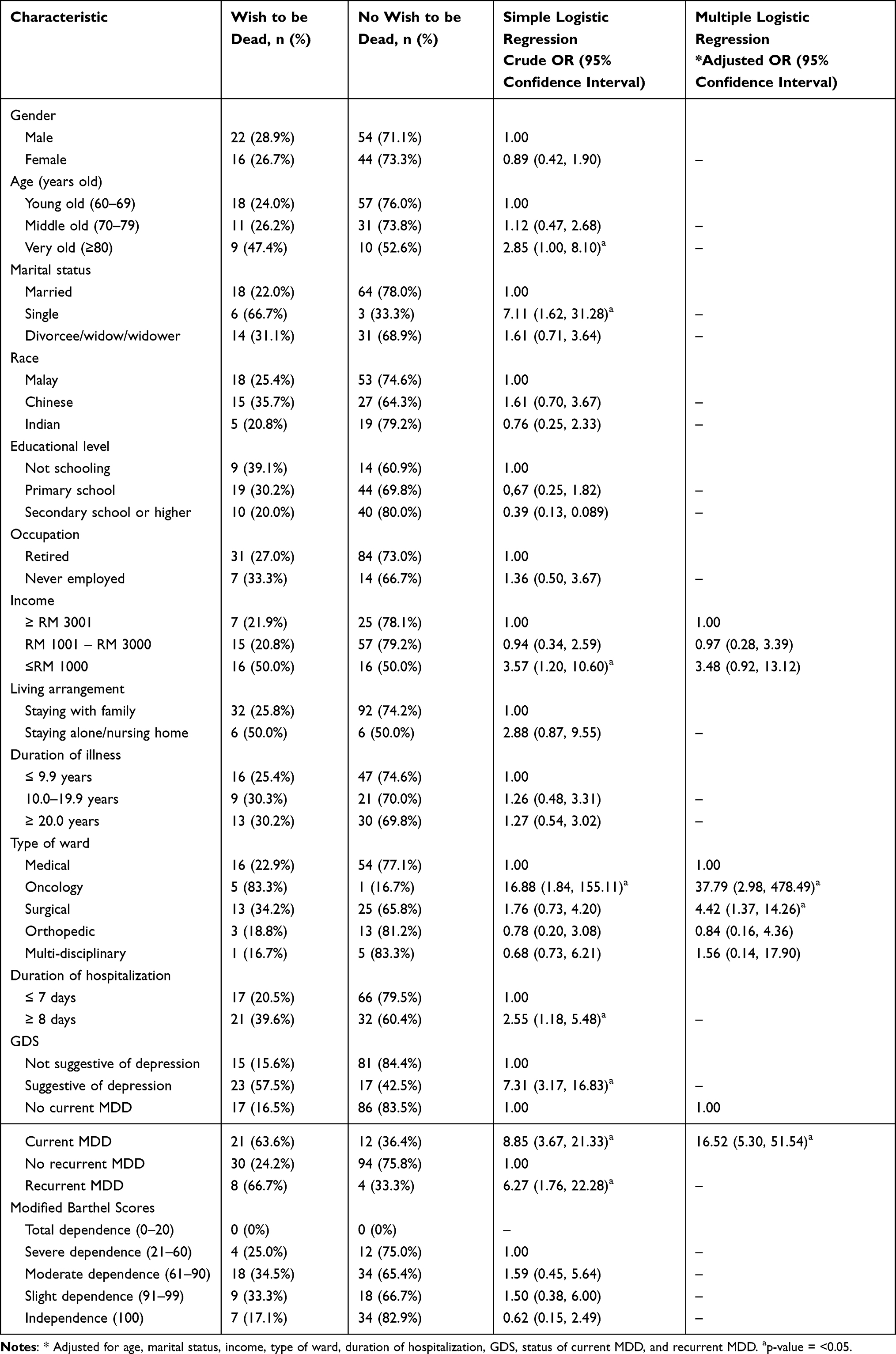 |
Table 4 Associations Between “Wish to Be Dead” Ideation, Socio-Demographic Data, General Medical Conditions, Depression, and Functional Disability |
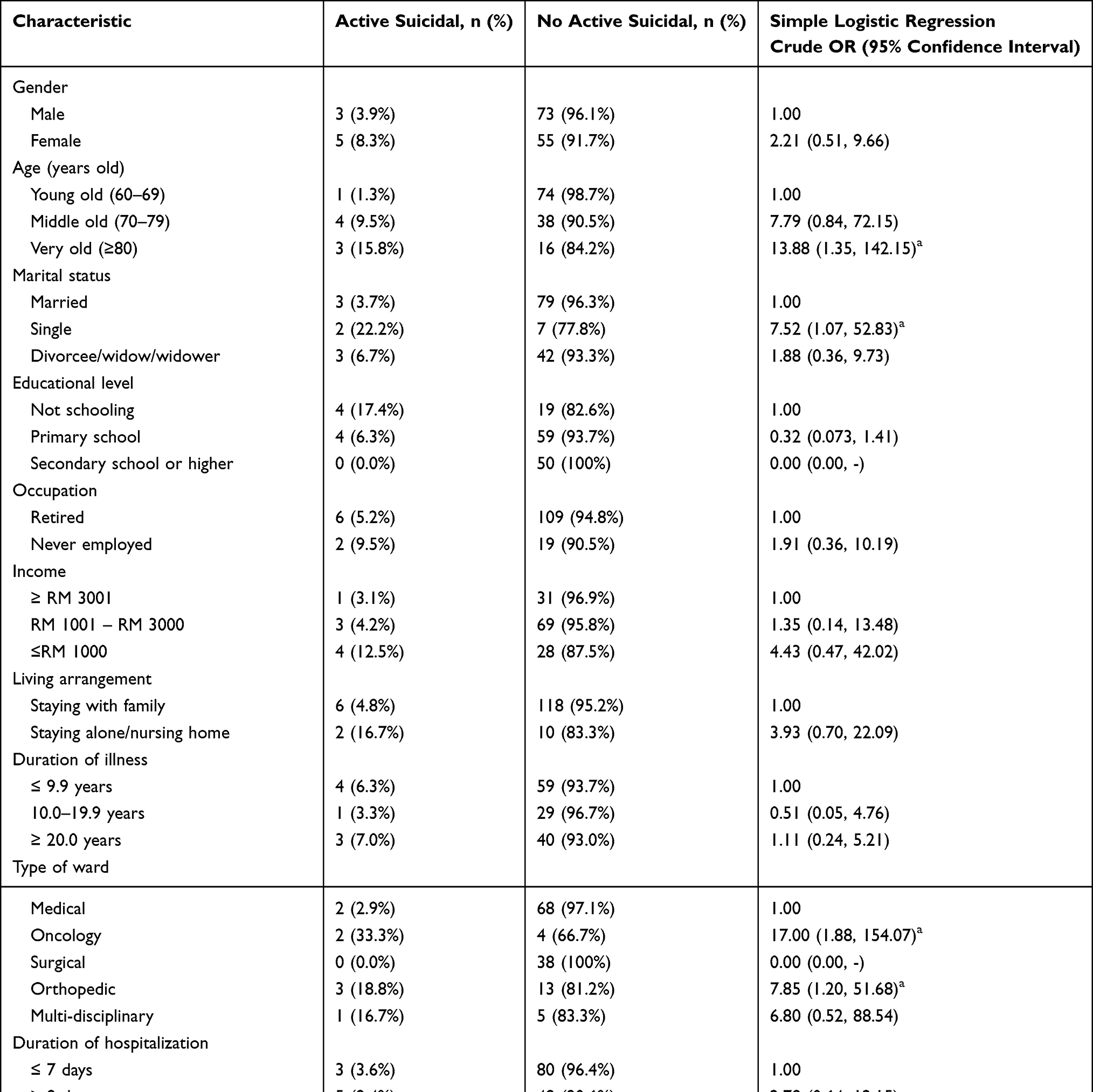 |
Table 5 The Associations Between Socio-Demographic Data, General Medical Conditions, Depression, Functional Disability, and Active Suicidal Ideation |
Finally, no significant relationship of pain scores was observed with the “wish to be dead” and active SI (p = 0.514 and p = 0.091, respectively).
Discussion
The prevalence of SI in the elderly differs among studies. The findings of this study revealed that passive SI were notably higher (27.9%) in elderly inpatients than active SI (5.9%). However, both were higher than the prevalence of SI of the general elderly Malaysian population at 3%.37 Multiple factors could contribute to the presence of active SI. This study showed that being single/unmarried is one of the most important factors at increasing risk of having active SI. Single elderlies had a higher risk of having active SI. Interestingly, elderlies who lost their partners were not at risk of having SI. A possible explanation for this situation may be that the elderlies continued to receive financial, social, and emotional support from their children after the death of their partners.
The literature has evidenced that SI is higher among elderly people with medical comorbidities, severe depression, and poor social support. It was reported that 10.6% of elderly patients in homecare have passive SI, while 1.2% have active SI.38 Even though nearly 70% of the elderly individuals had contact with the healthcare services a month before committing suicide,39 and approximately half of the elderly who committed suicide visited a doctor a week before,40 they rarely expressed their death-related ideation to the medical staff. Instead, they tended to present with masked depressive symptoms,41 such as having somatic symptoms.42 This is not surprising as studies have also shown that the elderly people rarely expressed their feelings openly and wish to die to others.43 Therefore, it is critical to identify those ill elderly patients who sought medical attention in a healthcare center to detect those at risk of suicide.
The findings of the study also revealed that the presence of medical illness in elderly patients, especially those with malignancies, was highly related to both passive (83.3%) and active SI (33.3%). The discomfort of lengthy hospitalization and side effects from chemotherapy could also contribute to the considerable passive ideation of dying.44 Besides oncology inpatients, those in the orthopedic wards also had relatively high active SI (18.8%), most likely due to pain and mobility-related issues such as bone fractures.45 However, this study did not find any correlation between the duration of medical illness and the duration of hospitalization with SI. A reasonable explanation for this could be that the patients examined in this study were not critically ill, and the length of hospitalization was not excessively long.
A local study looking at the autopsied cases of committed suicide retrospectively showed that the most common elderly suicide victims had an average age of 73 years.46 This study had similar findings that seven of eight (87.5%) active SI occurred in the elderly people over 70. Those in the very-old age group (80 years or older) were at risk of suicide, evidenced by a significant association between age groups and active SI.
As per the National Suicide Registry Malaysia (NSRM) records for 2009, the majority of patients who committed suicide were Chinese (78.26%). The data were similar to the findings of this study, which also revealed active SI occurring in elderly inpatients were mainly Chinese (87.5%). The Chinese had the highest prevalence of active SI (16.7%), whereas the Malays had none. This can be explained by religious factors, as suicide is strongly prohibited in Islamic doctrine. A previous study confirmed that religiously affiliated depressed patients were associated with less SB.47 In terms of passive ideation, however, no ethnic difference related to death was observed in this study.
In this study, three suicide methods reported by elderly patients harboring active SI were drug overdose, jumping from a height, and hanging. This finding is consistent with one epidemiologic study conducted in Iran showing drug overdose was the popular method among elderly.48 One retrospective study conducted among cases of suicide reported among the elderly found that hanging was the most common method, followed by jumping from a height.49 Nevertheless, choice of methods depends on availability of the method, acceptability of socio-cultural, and physical and cognitive availability of the person.50 It is worth noting that the frequency of SI among the elderly inpatients in this study might be under-reported due to cultural and religious issues. Some elderly could be feeling ashamed of expressing or harboring their SI, as this is often portrayed as a sign of personal weakness or failure, particularly in men.
The findings of this study also revealed that about two-thirds of depressed elderly inpatients had passive SI, while 5.9% had active SI (Table 1). The prevalence of major depressive episode (24.3%) was comparable to a previous forensic study in Malaysia, which showed that 21.7% of elderly who committed suicide had underlying psychiatric illness.46 Two studies conducted in the United States41 and Korea51 reported that depression in the elderly was the most substantial factor for SI and attempts. Therefore, it is vital to stress that the presence of a major depressive episode in the elderly warrants urgent attention to curb the suicidal risk.
In this study, however, no significant association was observed between the level of dependence and SI. The findings of this study contrasted with the findings of previous research revealing a significant association between those who attempted suicide and high levels of interpersonal dependence.52 There are multiple factors that may have affected such findings. One of such factors may be the presence of support by caregivers, which could have acted as a protective factor against SI. The elderly inpatients of this study mostly stayed with their families (91.2%), which could have played the supporting role as commonly seen among Malaysian households.53 On top of that, a clear majority of the participants (88.2%) were less dependent, indicated by their MBI score of >60, making them less likely to experience distress contributing to SI.
In terms of pain factor, the findings of this study also did not reveal a significant correlation between the pain scores and SI compared to the findings of previous studies. This insignificant result may be attributed to the sampling of this study, which had excluded severely ill and critical elderly inpatients and the cross-sectional nature of obtaining the pain score data. Alternately, pain management using analgesics such as opioids, commonly prescribed to oncology, surgical, and orthopedic patients, could have altered the study outcome and was not investigated.
Strengths and Limitations
It is worth noting that this study has some limitations. The exclusion of severely ill elderly inpatients might have affected the true frequency of SI among the elderly inpatients. However, their exclusion was due to them not being in the best physical and mental state to participate in this study. The screening instrument for depression (GDS-15) only screened elderly inpatients in acute or recurrent episodes of a depressive disorder. In view of this, the prevalence of MDD (current and lifetime) could have been higher than 24.3%. Other than that, several factors can affect SI but were not assessed in this study, such as religion, family history of suicide, and pre-existing psychiatric illness other than depression. Religion is commonly reported to be a protective factor against suicide,54,55 whereas a strong family history of suicide and psychiatric illness can increase the risk of suicide.56,57 Other important factors that were not included in this study are medication history and substance use. These factors are known contributing factors for both active and passive suicide ideation.58–60 However, one of the strengths of this study is that all instruments were translated and validated to fit the needs of the local population with an adequate number of participants enrolled.
Conclusion
Overall, this study shows that elderly inpatients who were single, very old, admitted to oncology or orthopedic wards, had positive GDS, current MDD, or recurrent MDD were at risk of developing active SI. Meanwhile, the “wish to be dead” thought was associated with admission to oncology ward, surgical ward, and having current MDD. Therefore, it is imperative to explore the mental health issues of terminally ill and physically disabled patients as it is an opportunity that should not be missed while the patients are in these wards. Furthermore, as suggested by Costanza et al,61 exploring these issues in the Emergency Department (ED) is yet another opportunity that should not be overlooked. By combining efforts in both the wards and the ED, SB in the elderly can be recognized more frequently, and treatment can be given swiftly.
The authors suggest that healthcare personnel managing the elderly patients in these wards should be given training about suicide prevention and intervention. These trainings should include recognizing the symptoms and signs of mood disorders leading to suicide and providing lessons on developing suicide safety plans. Furthermore, as suicide or SB is often considered taboo, especially among the local community, the training offered should also address stigma among healthcare personnel toward SB. Thus, to ensure an effective and holistic management of elderly patients, healthcare personnel should be taught not to be judgmental and to provide care without prejudice.
Abbreviations
C-SSRS, Columbia Suicide Severity Rating Scale; GDS-15, Geriatric Depression Scale; M.I.N.I, Mini International Neuropsychiatric Interview; MBI, Modified Barthel Index; VAS, Visual Analogue Scale; ADL, Activity of daily living; NSRM, National Suicide Registry Malaysia; MDD: Major Depressive Disorder.
Data Sharing Statement
The datasets generated for this study are not available to request due to confidentiality issues.
Ethics Statement
The approval for this research has been obtained from the Ethics Committee of Universiti Kebangsaan Malaysia Medical Centre (UKMMC) (FF-2016-428) and National Medical Research Registration (NMRR) Malaysia (NMRR-16-1485-31223 IIR). It also received approval from the Director of the hospital and Head of Department of respective units involved in the study. The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Acknowledgments
We wish to express our gratitude to Universiti Kebangsaan Malaysia Medical Centre (UKMMC) for supporting the study. We also would like to record our heartfelt thank you to all participants and their family members for their willingness to take part in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research is funded by Universiti Kebangsaan Malaysia Medical Centre (UKMMC).
Disclosure
The authors report no conflicts of interest for this work and declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. He W, Goodkind D, Kowal P. An aging world: 2015. U.S. Government Publishing Office; 2016. Available from: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf.
2. DOSM. Department of Statistics Malaysia current population estimates 2020. Department of Statistics Malaysia; 2021. Available from: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=155&bul_id=OVByWjg5YkQ3MWFZRTN5bDJiaEVhZz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09.
3. Tengku Abdul Hamid TA. Population ageing in malaysia; 2015.
4. Marson SM, Powell RM. Suicide among elders: a Durkheimian proposal. Int J Ageing Later Life. 2011;6(1):59–79. doi:10.3384/ijal.1652-8670.116159
5. Van Orden KA, Conwell Y. Issues in research on aging and suicide. Aging Ment Health. 2016;20(2):240–251. doi:10.1080/13607863.2015.1065791
6. Djernes JK. Prevalence and predictors of depression in populations of elderly: a review. Acta Psychiatr Scand. 2006;113(5):372–387. doi:10.1111/J.1600-0447.2006.00770.X
7. Manaf MRA, Mustafa M, Rahman MRA, Yusof KH, Aziz NAA. Factors influencing the prevalence of mental health problems among malay elderly residing in a rural community: a cross-sectional study. PLoS One. 2016;11(6):e0156937. doi:10.1371/JOURNAL.PONE.0156937
8. Seed HF, Hazli Z, Perumal M, Azlin A. Depression among chronic pain patients at Hospital Tengku Ampuan Rahimah, Klang. Med J Malaysia. 2015;70(5):303–306.
9. Katon WJ. Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues Clin Neurosci. 2011;13(1):7. doi:10.31887/DCNS.2011.13.1/WKATON
10. Ilgen MA, Zivin K, McCammon RJ, Valenstein M. Pain and suicidal thoughts, plans and attempts in the United States. Gen Hosp Psychiatry. 2008;30(6):521–527. doi:10.1016/J.GENHOSPPSYCH.2008.09.003
11. Jacobs JM, Hammerman-Rozenberg R, Cohen A, Stessman J. Chronic back pain among the elderly: prevalence, associations, and predictors. Spine. 2006;31(7):E203–E207. doi:10.1097/01.brs.0000206367.57918.3c
12. Kikuchi N, Ohmori-Matsuda K, Shimazu T, et al. Pain and risk of completed suicide in Japanese men: a population-based cohort study in Japan (Ohsaki Cohort Study). J Pain Symptom Manage. 2009;37(3):316–324. doi:10.1016/j.jpainsymman.2008.03.012
13. Chytas V, Costanza A, Piguet V, Cedraschi C, Bondolfi G. Démoralisation et sens dans la vie dans l’idéation suicidaire: un rôle chez les patients douloureux chroniques? Rev Med Suisse. 2019;15(656):1282–1285.
14. Clarke DM, Kissane DW. Demoralization: its phenomenology and importance. Aust NZ J Psychiatry. 2002;36(6):733–742. doi:10.1046/j.1440-1614.2002.01086.x
15. Nuns N, Loas G. Interpersonal dependency in suicide attempters. Psychopathology. 2005;38(3):140–143. doi:10.1159/000085846
16. Shah A, Padayatchi M, Das K. The relationship between elderly suicide rates and elderly dependency ratios: a cross-national study using data from the WHO data bank. Int Psychogeriatr. 2008;20(3):596–604. doi:10.1017/S104161020700628X
17. Ibrahim N, Din NC, Ahmad M, et al. Relationships between social support and depression, and quality of life of the elderly in a rural community in Malaysia. Asia Pac Psychiatry. 2013;5(SUPPL. 1):59–66. doi:10.1111/APPY.12068
18. Puteh SE, Bakar IM, Borhanuddin B, Latiff K, Amin RM, Sutan R. A prevalence study of the Activities of Daily Living (ADL) dependency among the elderly in four districts in Selangor, Malaysia. J Epid Prev Med. 2018. doi:10.19104/jepm.2015.110
19. Szanto K, Reynolds CF, Frank E, et al. Suicide in elderly depressed patients: Is active vs. passive suicidal ideation a clinically valid distinction? Am J Geriatr Psychiatry. 1996;4(3):197–207. doi:10.1097/00019442-199622430-00003
20. Miranda R, Ortin A, Scott M, Shaffer D. Characteristics of suicidal ideation that predict the transition to future suicide attempts in adolescents. J Child Psychol Psychiatry. 2014;55(11):1288–1296. doi:10.1111/JCPP.12245
21. Nock MK, Millner AJ, Joiner TE, et al. Risk factors for the transition from suicide ideation to suicide attempt: results from the army study to assess risk and resilience in Servicemembers (Army STARRS). J Abnorm Psychol. 2018;127(2):139–149. doi:10.1037/ABN0000317
22. Conway PM, Erlangsen A, Teasdale TW, Jakobsen IS, Larsen KJ. Predictive validity of the columbia-suicide severity rating scale for short-term suicidal behavior: a danish study of adolescents at a high risk of suicide. Arch Suicide Res. 2017;21(3):455–469. doi:10.1080/13811118.2016.1222318
23. Shear MK, Wang Y, Skritskaya N, Duan N, Mauro C, Ghesquiere A. Treatment of complicated grief in elderly persons: a randomized clinical trial. JAMA Psychiatry. 2014;71(11):1287–1295. doi:10.1001/jamapsychiatry.2014.1242
24. Grover S, Avasthi A, Sahoo S, et al. Relationship of loneliness and social connectedness with depression in elderly: a multicentric study under the aegis of Indian Association for Geriatric Mental Health. J Geriatr Ment Health. 2018;5(2):99. doi:10.4103/jgmh.jgmh_26_18
25. Posner K, Brown GK, Stanley B, et al. The Columbia–Suicide severity rating scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266–1277. doi:10.1176/APPI.AJP.2011.10111704
26. Marc LG, Raue PJ, Bruce ML. Screening performance of the 15-item geriatric depression scale in a diverse elderly home care population. Am J Geriatr Psychiatry. 2008;16(11):914–921. doi:10.1097/JGP.0B013E318186BD67
27. Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine ED. Screening for Depression in elderly primary care patients: a comparison of the center for epidemiologic studies—Depression scale and the geriatric depression scale. Arch Intern Med. 1997;157(4):449–454. doi:10.1001/ARCHINTE.1997.00440250107012
28. Teh EE, Ismail HC. Validation of Malay version of geriatric depression scale among elderly inpatients. Univ Sains Malaysia. 2005;17:65–74.
29. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(SUPPL. 20):22–33.
30. Lecrubier Y, Sheehan DV, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. Eur Psychiatry. 1997;12(5):224–231. doi:10.1016/S0924-9338(97)83296-8
31. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The validity of the Mini International Neuropsychiatric Interview (MINI) according to the SCID-P and its reliability. Eur Psychiatry. 1997;12(5):232–241. doi:10.1016/S0924-9338(97)83297-X
32. Mahoney FI, Barthel DM. Functional evaluation: the Barthel index. Md State Med J. 1965;14(2):61–65.
33. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. doi:10.1016/0895-4356(89)90065-6
34. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. 1983;16(1):87–101. doi:10.1016/0304-3959(83)90088-X
35. Armitage CJ, Panagioti M, Abdul Rahim W, Rowe R, O’Connor RC. Completed suicides and self-harm in Malaysia: a systematic review. Gen Hosp Psychiatry. 2015;37(2):153–165. doi:10.1016/j.genhosppsych.2014.12.002
36. Leading causes of hospitalization; 2018. Available from: https://www.simcoemuskokahealthstats.org/topics/leading-causes/leading-causes-of-hospitalizations.
37. Syed Elias SM, Makhtar A, Ahmad Tarmidi NH. Factors associated with suicidal ideation among older people in medical outpatient clinic. Enferm Clin. 2021;31:S356–S360. doi:10.1016/j.enfcli.2020.09.026
38. Raue PJ, Meyers BS, Rowe JL, Heo M, Bruce ML. Suicidal ideation among elderly homecare patients. Int J Geriatr Psychiatry. 2007;22(1):32–37. doi:10.1002/gps.1649
39. Pitkälä K, Isometsä ET, Henriksson MM, Lönnqvist JK. Elderly suicide in Finland. Int Psychogeriatr. 2000;12(2):209–220. doi:10.1017/s1041610200006335
40. Juurlink DN, Herrmann N, Szalai JP, Kopp A, Redelmeier DA. Medical illness and the risk of suicide in the elderly. Arch Intern Med. 2004;164(11):1179–1184. doi:10.1001/ARCHINTE.164.11.1179
41. Szanto K, Prigerson HG, Reynolds CF. Suicide in the elderly. Clin Neurosci Res. 2001;1(5):366–376. doi:10.1016/S1566-2772(01)00039-1
42. Morin RT, Nelson C, Bickford D, Insel PS, Mackin RS. Somatic and anxiety symptoms of depression are associated with disability in late life depression. Aging Ment Health. 2019;24(8):1225–1228. doi:10.1080/13607863.2019.1597013
43. Bonnewyn A, Shah A, Bruffaerts R, Demyttenaere K. Factors determining the balance between the wish to die and the wish to live in older adults. Int J Geriatr Psychiatry. 2017;32(6):685–691. doi:10.1002/GPS.4511
44. Latha KS, Bhat SM. Suicidal behaviour among terminally ill cancer patients in India. Indian J Psychiatry. 2005;47(2):79. doi:10.4103/0019-5545.55950
45. Hinkley BS, Jaremko ME. Effects of pain duration on psychosocial adjustment in orthopedic patients: the importance of early diagnosis and treatment of pain. J Pain Symptom Manage. 1994;9(3):175–185. doi:10.1016/0885-3924(94)90128-7
46. Rahimi R, Ali N, Md Noor S, Mahmood MS, Zainun KA. Suicide in the elderly in Malaysia. Malays J Pathol. 2015;37(3):259–263.
47. Dervic K, Oquendo MA, Grunebaum MF, Ellis S, Burke AK, Mann JJ. Religious affiliation and suicide attempt. Am J Psychiatry. 2004;161(12):2303–2308. doi:10.1176/appi.ajp.161.12.2303
48. Mokhtari AM, Sahraian S, Hassanipour S, Baseri A, Mirahmadizadeh A. The epidemiology of suicide in the elderly population in Southern Iran, 2011–2016. Asian J Psychiatr. 2019;44:90–94. doi:10.1016/j.ajp.2019.07.027
49. Crestani C, Masotti V, Corradi N, Schirripa ML, Cecchi R. Suicide in the elderly: a 37-years retrospective study. Acta Biomed. 2019;90(1):68–76. doi:10.23750/abm.v90i1.6312
50. Kõlves K, McDonough M, Crompton D, de Leo D. Choice of a suicide method: trends and characteristics. Psychiatry Res. 2018;260:67–74. doi:10.1016/j.psychres.2017.11.035
51. Ro J, Park J, Lee J, Jung H. Factors that affect suicidal attempt risk among Korean elderly adults: a path analysis. J Prev Med Public Health. 2015;48(1):28–37. doi:10.3961/jpmph.14.030
52. Bornstein RF, O’Neill RM. Dependency and suicidality in psychiatric inpatients. J Clin Psychol. 2000;56(4):463–473. doi:10.1002/(SICI)1097-4679(200004)56:4<463::AID-JCLP2>3.0.CO;2-5
53. Wan-Ibrahim WA, Zainab I. The availability of family support of rural elderly in Malaysia. World Appl Sci J. 2014;30(7):899–902. doi:10.5829/idosi.wasj.2014.30.07.14080
54. Gearing RE, Lizardi D. Religion and suicide. J Relig Health. 2009;48(3):332–341. doi:10.1007/s10943-008-9181-2
55. Cook CCH. Suicide and religion. Br J Psychiatry. 2014;204(4):254–255. doi:10.1192/bjp.bp.113.136069
56. Brent DA, Mann JJ. Family genetic studies, suicide, and suicidal behavior. Am J Med Genet. 2005;133 C(1):13–24. doi:10.1002/ajmg.c.30042
57. Qin P. The impact of psychiatric illness on suicide: differences by diagnosis of disorders and by sex and age of subjects. J Psychiatr Res. 2011;45(11):1445–1452. doi:10.1016/j.jpsychires.2011.06.002
58. Zisook S, Lesser IM, Lebowitz B, et al. Effect of antidepressant medication treatment on suicidal ideation and behavior in a randomized trial: an exploratory report from the combining medications to enhance depression outcomes study. J Clin Psychiatry. 2011;72(10):1322–1332. doi:10.4088/JCP.10m06724
59. Favreau H, Bacon SL, Joseph M, Labrecque M, Lavoie KL. Association between asthma medications and suicidal ideation in adult asthmatics. Respir Med. 2012;106(7):933–941. doi:10.1016/j.rmed.2011.10.023
60. Poorolajal J, Haghtalab T, Farhadi M, Darvishi N. Substance use disorder and risk of suicidal ideation, suicide attempt and suicide death: a meta-analysis. J Public Health. 2016;38(3):e282–e291. doi:10.1093/pubmed/fdv148
61. Costanza A, Amerio A, Radomska M, et al. Suicidality assessment of the elderly with physical illness in the emergency department. Front Psychiatry. 2020;11:1–6. doi:10.3389/fpsyt.2020.558974
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.