Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Successful Treatment of Refractory Chronic Spontaneous Urticaria with Stapokibart After Omalizumab Failure: A Case Report
Authors Chen J, Chen Z, Li X, Chen J ![]() , Zhang L, Peng L, Liang B, Chen Q
, Zhang L, Peng L, Liang B, Chen Q ![]() , Li R, Li H, Zhu H
, Li R, Li H, Zhu H
Received 12 February 2026
Accepted for publication 31 March 2026
Published 25 May 2026 Volume 2026:19 603129
DOI https://doi.org/10.2147/CCID.S603129
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Monica K. Li
Jiaoquan Chen, Ziyan Chen, Xiaofeng Li, Jiajun Chen, Luoyu Zhang, Liqian Peng, Bihua Liang, Quan Chen, Runxiang Li, Huaping Li, Huilan Zhu
Department of Dermatology, Guangzhou Dermatology Hospital, Guangzhou, Guangdong, 510095, People’s Republic of China
Correspondence: Huilan Zhu, Department of Dermatology, Guangzhou Dermatology Hospital, Guangzhou, Guangdong, 510095, People’s Republic of China, Email [email protected]
Abstract: Chronic spontaneous urticaria (CSU) is a mast cell-mediated skin disease characterized by wheals and/or angioedema. Some patients remain symptomatic despite standard-of-care antihistamines or omalizumab. We report a 44-year-old female with refractory CSU with a history of recurrent widespread erythema and wheals with pruritus for over one year. She was failed to achieve adequate disease control with oral antihistamines and 5 doses of omalizumab 300 mg. She was subsequently treated with anti-IL-4Rα antibody stapokibart 300 mg (loading dose 600 mg) for 35 weeks, with an extended-interval dosing regimen (every 2 week for 9 doses, every 3 weeks for 3 doses, and every 6 weeks for 2 doses). Rapid symptom control was observed by week 2 (Urticaria Activity Score [UAS7] of 0 and Urticaria Control Test [UCT] score of 12), with complete disease control achieved by week 22 (UAS7 of 0 and UCT score of 16). No relapse occurred during 3-month follow-up period.
Keywords: chronic spontaneous urticaria, pruritic wheals, erythema, stapokibart
Introduction
Chronic spontaneous urticaria (CSU) is a debilitating skin disease that presents with recurrent pruritic wheals and/or angioedema for ≥6 weeks in the absence of an identifiable trigger.1 It affects approximately 1% of the population worldwide and persists beyond 1 year in over 80% of patients.2,3 Patients with CSU often experience sleep disturbance, impaired daily functioning, and psychological distress, leading to marked deterioration in quality of life and considerable socio-economic burden.4
Achieving complete symptom control is the primary treatment goal for CSU. Second-generation H1-antihistamines are recommended as first-line therapy, allowing dose escalation up to 4-fold in patients with insufficient response.5–7 When symptoms remain inadequately controlled, the addition of omalizumab (anti-immunoglobulin E) is advised.7,8 Although cyclosporine represents an effective third-line option for antihistamine-refractory CSU, its use is constrained by safety concerns.7,9
Type 2 inflammations plays a central role in CSU pathogenesis. Transcriptomic analyses have shown upregulated Th2-related pathways (including interleukin [IL]-4 and IL-13 signaling) in lesional CSU skin,10 supporting the rationale for targeting type 2 cytokines as a therapeutic strategy. Dupilumab is an anti-IL-4 receptor subunit α (IL-4Rα) monoclonal antibody that blocks both IL-4 and IL-13 signaling. Recently, the approval of dupilumab by the US Food and Drug Administration and the European Medicines Agency, and is recommended in the Chinese consensus for the treatment of CSU in adolescents and adults demonstrates that targeting IL-4Rα can effectively improve pruritus, wheals, and urticaria activity.11,12
Stapokibart, a humanized anti-IL-4Rα monoclonal antibody, binds to a distinct epitope on IL-4Rα that is located closer to the ligand-binding site than that of the dupilumab analogue, and exhibits high-affinity, cross-species binding to IL-4Rα from human, cynomolgus monkey, and rat.13 It is approved in China for moderate-to-severe atopic dermatitis inadequately controlled by or refractory to topical therapies, seasonal allergic rhinitis, and severe uncontrolled chronic rhinosinusitis with nasal polyps.14–16 Here, we report on the first case of refractory CSU who showed inadequate responses to multiple prior therapies and subsequently was treated successfully with stapokibart.
Case Presentation
In September 2024, a 44-year-old female presented to our department with a history of recurrent widespread erythema and wheals with pruritus for over one year, in the absence of an identifiable trigger, and reported symptom exacerbation during the past week. Physical examination showed scattered erythema on the lower limbs without wheals, and dermographism test was negative. Urticaria Control Test (UCT) score was 8 (range: 0–16), Urticaria Activity Score over 7 days (UAS7) was 16 (range: 0–42), and dermatology Life Quality Index (DLQI) score was 8 (range: 0–30). Auxiliary examination in October 2024 showed positive autologous serum skin test (ASST), total IgE of 34.3 IU/mL (range: 1–190.4 IU/mL), and basophil activation test of 0.42%. There were no abnormalities in blood routine examination, D-dimer, erythrocyte sedimentation rate, immunological parameters, or C-reactive protein. The patient’s mother had a history of urticaria.
Since disease onset in 2023, the patient initially self-administered loratadine tablet, with rash subsiding within 24 hours. However, symptoms recurred frequently without a clear seasonal or temporal pattern. She subsequently received multiple therapies, including oral antihistamines (clemastine fumarate oral solution, cyproheptadine hydrochloride, and loratadine tablet), Xiaofeng Zhiyang granules, and whole-body narrowband ultraviolet B (NB-UVB; 311 nm) phototherapy. Intramuscular injection of compound betamethasone provided only temporary relief during acute flares. Despite treatment with omalizumab (300 mg every 4 weeks for 2 doses) plus oral antihistamines, disease control remained inadequate.
According to the international and domestic guidelines, refractory CSU is defined as inadequate symptom control despite standard or up-dosed H1-antihistamines or their combinations.7,17 Based on these criteria, the patient was diagnosed as refractory CSU.
After presentation at our hospital, the patient showed poor disease control (UCT 6, UAS7 30, and DLQI 21) despite 9 weeks of combined treatments with omalizumab (300 mg every 3 weeks [Q3W]), loratadine (10 mg once daily), and NB-UVB phototherapy Q3W, with new erythema and wheals appearing every 2–3 days. In December 2024, omalizumab was switched to off-label stapokibart (600 mg loading dose, 300 mg thereafter, every 2 weeks), while concomitant therapies maintained (Figure 1). Marked improvements in symptoms and quality of life were evident as early as week 2. By week 19, UCT score increased to 15, and UAS7 and DLQI decreased to 0 and 1, respectively (Figure 1). Considering well-controlled disease and the patient’s economic burden, the dosing interval for stapokibart was extended to every 3 weeks for 3 doses, and later further to every 6 weeks for 2 doses. No relapse occurred during extended-interval dosing or over the 3-month follow-up after discontinuation, with UCT, UAS7, and DLQI scores of 16, 0, and 0, respectively (Figure 1). Follow-up laboratory tests showed a positive ASST, with total IgE of 2.29 IU/mL and a basophil activation test of 2.34%. No adverse events were reported throughout the stapokibart treatment period.
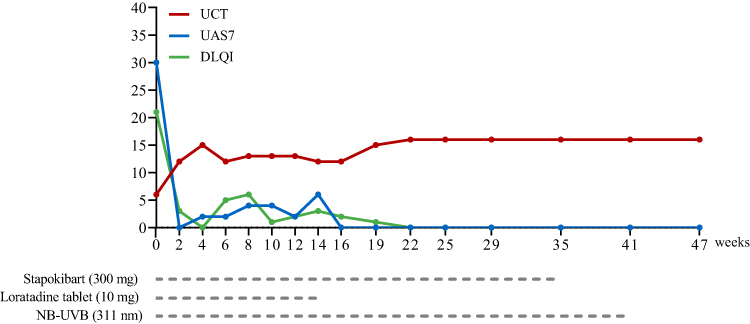 |
Figure 1 Timeline of stapokibart treatment and outcomes. Stapokibart was administered at 300 mg every 2 weeks (9 doses, 600 mg loading dose at week 0, followed by 300 mg at weeks 2, 4, 6, 8, 10, 12, 14, and 16), every 3 weeks (3 doses; at weeks 19, 22, and 25), and every 6 weeks (2 doses; at weeks 29 and 35). Loratadine tablet was used on an as-needed (SOS) basis from weeks 2 to 14. Abbreviations: DLQI, Dermatology Life Quality Index; NB-UVB, narrowband ultraviolet B; UAS7, Seven days urticaria activity score; UCT, Urticaria control test. |
Discussion
CSU is a mast cell-driven inflammatory skin disorder, with basophils also contributing to disease pathogenesis.18 Beyond histamine release, IgE-mediated activation of mast cells and basophils promotes type 2 inflammation through cytokines such as IL-4, IL-5, and IL-13,19 while T cell-mediated cytokine signaling further contributes to immune dysregulation in CSU.7
Recent Phase 3 trials have shown that IL-4Rα blockade with dupilumab improves urticaria disease activity in CSU patients despite H1-antihistamines treatment.11,12 However, among patients who are omalizumab-intolerant/incomplete responders, the clinical benefit appears modest.11,20 Network meta-analyses continue to support omalizumab as the preferred biologic therapy, with dupilumab representing a potential alternative in selected populations.21 These differences may be partly explained by CSU endotypes, broadly classified as type I (IgE autoantibody-mediated), type IIb (autoimmune), type I/type IIb overlap, and non-type I/IIb subtypes. Type I CSU is associated with rapid responses to omalizumab, whereas type IIb disease often shows delayed or inadequate responses and may require alternative therapies.21
This report describes a case of refractory CSU uncontrolled with multiple prior therapies for over one year, including oral antihistamines, Chinese patent medicines, NB-UVB phototherapy, and omalizumab. Persistent ASST positivity together with low total IgE levels suggested a type IIb autoimmune endotype, in which disease activity is largely independent of IgE-mediated pathways.22,23 Consistent with prior observations that ASST-positive patients tend to be late responders,24 this profile may account for the delayed or limited response to omalizumab in this case.
Given the insufficient clinical response, stapokibart was initiated and administered with extended dosing intervals over a 35-week treatment period. Rapid and marked improvements in symptoms and quality of life were evident as early as week 2, with complete resolution of erythema, wheals, and pruritus achieved by week 22. The complete disease control was maintained during the subsequent extended-interval dosing and 3-month follow-up, supporting the feasibility of personalized dosing interval adjustments of stapokibart based on efficacy response in CSU. Although stapokibart suppresses type 2 inflammatory pathways, it does not target the underlying autoantibodies detected by ASST, which may persist during treatment and account for sustained ASST positivity. No treatment-related adverse events were observed during the treatment period.
The limitations of this report include its single-patient nature and short follow-up duration. In addition, a potential delayed effect of prior therapies cannot be excluded, and the absence of mechanistic biomarkers or longitudinal immunologic profiling limits interpretation of the treatment response.
Conclusion
This report demonstrates favorable clinical outcomes following stapokibart treatment in a patients with refractory CSU who had an inadequate response to prior therapies, including omalizumab. Further large, controlled studies are required to confirm the efficacy and safety of stapokibart in this population.
Ethical Statement
This case report was approved by Guangzhou Dermatology Hospital (No. gzsp2503).
Consent Statement
Written informed consent was obtained from the patient for publication of this case report.
Acknowledgments
We sincerely appreciate the patient’s contribution to this case.
Funding
This work was supported by Guangzhou Municipal Science and Technology Program (no. 2023A03J0470 and no. 2024A03J0424).
Disclosure
The authors declare no competing interests in this work.
References
1. Kolkhir P, Bonnekoh H, Metz M, Maurer M. Chronic spontaneous urticaria: a review. JAMA. 2024;332(17):1464–4. doi:10.1001/jama.2024.15568
2. Fricke J, Ávila G, Keller T, et al. Prevalence of chronic urticaria in children and adults across the globe: systematic review with meta-analysis. Allergy. 2020;75(2):423–432. doi:10.1111/all.14037
3. Balp MM, Halliday AC, Severin T, et al. Clinical remission of Chronic Spontaneous Urticaria (CSU): a targeted literature review. Dermatol Ther. 2022;12(1):15–27. doi:10.1007/s13555-021-00641-6
4. Oliver ET, Saini SS. Chronic spontaneous urticaria: etiology and pathogenesis. Immunol Allergy Clin North Am. 2024;44(3):421–438. doi:10.1016/j.iac.2024.03.002
5. Bernstein JA, Winders TA, McCarthy J, et al. Urticaria voices: real-world treatment patterns and outcomes in chronic spontaneous urticaria. Dermatol Ther. 2025;15(8):2201–2215. doi:10.1007/s13555-025-01461-8
6. Kolkhir P, Laires PA, Salameh P, et al. The benefit of complete response to treatment in patients with chronic spontaneous urticaria-CURE results. J Allergy Clin Immunol Pract. 2023;11(2):610–620.e615. doi:10.1016/j.jaip.2022.11.016
7. Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy. 2022;77(3):734–766. doi:10.1111/all.15090
8. Tharp MD, Bernstein JA, Kavati A, et al. Benefits and harms of omalizumab treatment in adolescent and adult patients with chronic idiopathic (Spontaneous) urticaria: a meta-analysis of “real-world” evidence. JAMA Dermatol. 2019;155(1):29–38. doi:10.1001/jamadermatol.2018.3447
9. Kulthanan K, Chaweekulrat P, Komoltri C, et al. Cyclosporine for chronic spontaneous urticaria: a meta-analysis and systematic review. J Allergy Clin Immunol Pract. 2018;6(2):586–599. doi:10.1016/j.jaip.2017.07.017
10. Prosty C, Gabrielli S, Ben-Shoshan M, et al. In silico identification of immune cell-types and pathways involved in chronic spontaneous urticaria. Front Med. 2022;9(926753). doi:10.3389/fmed.2022.926753
11. Maurer M, Casale TB, Saini SS, et al. Dupilumab in patients with chronic spontaneous urticaria (LIBERTY-CSU CUPID): two randomized, double-blind, placebo-controlled, phase 3 trials. J Allergy Clin Immunol. 2024;154(1):184–194. doi:10.1016/j.jaci.2024.01.028
12. Casale T, Saini S, Bernstein J, et al. Dupilumab significantly improves itch and hives in patients with chronic spontaneous urticaria (CUPID study C). Ann Allergy Asthma Immunol. 2024;133(6, Supplement 2):S2. doi:10.1016/j.anai.2024.10.005
13. Liu W, Zhao Y, He Y, et al. Stapokibart (CM310) targets IL-4Rα for the treatment of type 2 inflammation. iScience. 2024;27(9):110721. doi:10.1016/j.isci.2024.110721
14. Zhao Y, Zhang L, Zhang J. Efficacy and safety of stapokibart (CM310) in adults with moderate-to-severe atopic dermatitis: a multicenter, randomized, double-blind, placebo-controlled phase 3 trial. J Am Acad Dermatol. 2024;91(5):984–986. doi:10.1016/j.jaad.2024.07.1447
15. Zhang Y, Li J, Wang M, et al. Stapokibart for moderate-to-severe seasonal allergic rhinitis: a randomized phase 3 trial. Nat Med. 2025;31(7):2213–2221. doi:10.1038/s41591-025-03651-5
16. Shen S, Yan B, Wang M, et al. Stapokibart for severe uncontrolled chronic rhinosinusitis with nasal polyps: the CROWNS-2 randomized clinical trial. JAMA. 2025;334(11):962–972. doi:10.1001/jama.2025.12515
17. Chinese Society of Dermatology; China Dermatologist Association. Guidelines for the diagnosis and treatment of refractory chronic spontaneous urticaria in China (2025 edition). Chin J Dermatol. 2025;58(06):485–496. doi:10.35541/cjd.20240674
18. Zhou B, Li J, Liu R, Zhu L, Peng C. The role of crosstalk of immune cells in pathogenesis of chronic spontaneous urticaria. Front Immunol. 2022;13(879754). doi:10.3389/fimmu.2022.879754
19. Charles N, Blank U. IgE-mediated activation of mast cells and basophils in health and disease. Immunol Rev. 2025;331(1):e70024. doi:10.1111/imr.70024
20. Hayama K, Ito-Watanabe M, Fujita H. Effectiveness of transitioning from omalizumab to dupilumab in chronic spontaneous urticaria patients with inadequate response to omalizumab. World Allergy Organ J. 2025;18(8):101098. doi:10.1016/j.waojou.2025.101098
21. Xiong G, Rayner DG, Kim L, et al. Comparative efficacy of omalizumab, dupilumab, and remibrutinib in chronic spontaneous urticaria: a network meta-analysis of randomized control trials. J Dermatolog Treat. 2025;36(1):2580374. doi:10.1080/09546634.2025.2580374
22. Su Küçük Ö, Yücel MB. Clinical and molecular aspects of managing chronic spontaneous urticaria: identifying endotypes, phenotypes, and determinants of treatment response and resistance. Front Allergy. 2025;6(1706705). doi:10.3389/falgy.2025.1706705
23. Lang DM, Sheikh J, Joshi S, Bernstein JA. Endotypes, phenotypes, and biomarkers in chronic spontaneous urticaria: evolving toward personalized medicine. Ann Allergy Asthma Immunol. 2025;134(4):408–417.e403. doi:10.1016/j.anai.2024.10.026
24. Palladino A, Villani F, Pinter E, Visentini M, Asero R. The autologous serum skin test predicts the response to anti-IgE treatment in chronic spontaneous urticaria patients: a prospective study. Eur Ann Allergy Clin Immunol. 2025;57(3):115–119. doi:10.23822/EurAnnACI.1764-1489.337
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.