Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Successful Treatment of Extensive Ritlecitinib-Refractory Alopecia Areata with Upadacitinib
Received 21 January 2026
Accepted for publication 12 June 2026
Published 23 June 2026 Volume 2026:19 597936
DOI https://doi.org/10.2147/CCID.S597936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Wanyu Sun, Huiping Wang, Yuanjun Liu
Department of Dermatovenereology, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
Correspondence: Yuanjun Liu, Department of Dermatovenereology, Tianjin Medical University General Hospital, 154 Anshan Road, Heping District, Tianjin, 300052, People’s Republic of China, Tel +8613752006903, Email [email protected]
Abstract: Alopecia areata is a non-scarring form of hair loss with an undetermined etiology that can profoundly affect patients both cosmetically and psychologically. As immune cells are implicated in the pathogenesis, molecularly targeted drugs can be used for therapy. This report presents a case of a patient who suffered from alopecia areata for two years. Our patient failed to respond to standard therapy using traditional Chinese medicine techniques. This necessitated a shift to a different drug with improved efficacy and outcomes. Initial treatment revealed that the patient had ritlecitinib-resistant alopecia areata, which showed significant signs of recovery following treatment with upadacitinib. By the 24-week follow-up, all symptoms of alopecia had sufficiently normalized. This report also highlights the advantages of upadacitinib and the role of JAK1-mediated pathways in certain patients with alopecia. Thus, It suggests that adoption of personalized treatment strategies might have an effect for patients with alopecia areata.
Keywords: alopecia remediation, molecular targeted therapy, ritlecitinib resistance, JAK-STAT1 signaling pathway
Introduction
Alopecia areata (AA)—a disorder characterized by partial or complete hair loss—is conventionally attributed to autoimmune reactions against hair follicles. Besides cosmetic concerns, AA can induce psychological distress and adversely affect the quality of life. Consequently, it necessitates efficacious treatment. Molecularly targeted drugs—namely, ruxolitinib, tofacitinib, baricitinib, and ritlecitinib—are the latest in the line of therapeutic interventions.1 Ritlecitinib is a JAK3 inhibitor in the Janus kinase and signal transducer and activator of transcription (JAK-STAT) signaling pathway, which has been implicated in the autoimmune reactions involved in alopecia. Similarly, upadacitinib is known to selectively inhibit JAK1. However, there is a lack of sufficient documentation regarding the treatment of patients who do not respond to JAK3 inhibitors. Current research has demonstrated that upadacitinib positively affects alopecia areata.2,3 This report details a severe case of ritlecitinib-resistant AA that was successfully treated with upadacitinib, resulting in restoration of normal hair volume in the patient.
Case Presentation
Our patient, a 38-year-old man, suffered for two years from hair loss induced by alopecia. He initially experienced localized alopecia that progressively exacerbated, leading to complete loss of eyebrows, eyelashes, as well as pubic and axillary hair. Prior treatment with traditional Chinese medicine had proved ineffective. He presented to our hospital in January 2025 and was subsequently diagnosed with AA. Examination revealed multiple patches of hair loss on the entire scalp (Figure 1), a positive hair pull test, a Severity of Alopecia Tool (SALT) score of 79, and a Dermatology Life Quality Index self-assessment score of 18. Furthermore, blood tests evidenced the absence of syphilis antibodies, along with normal thyroid, liver, and kidney functions. Complete autoimmune panel results were also obtained from the patient. He was initially treated with ritlecitinib (50 mg/day). During the follow-up period from January to May 2025, no notable hair regrowth and exacerbation of the SALT score to 83 was noted (Figure 2). Consequently, the patient requested a change in medication and was prescribed upadacitinib (15 mg/day). Seven-week upadacitinib treatment resulted in patches of new black hair growth and a SALT score of 65 (Figure 3). The patient’s hair volume increased gradually, and by the 15-week follow-up, 80% of the normal hair volume was restored, accompanied by partial regrowth of eyebrows and beard and a SALT score of 20 (Figure 4). At the 24-week follow-up, hair growth had completely normalized, with no discernible areas of alopecia (Figure 5). No adverse events or abnormal laboratory test results occurred during treatment and follow-up.
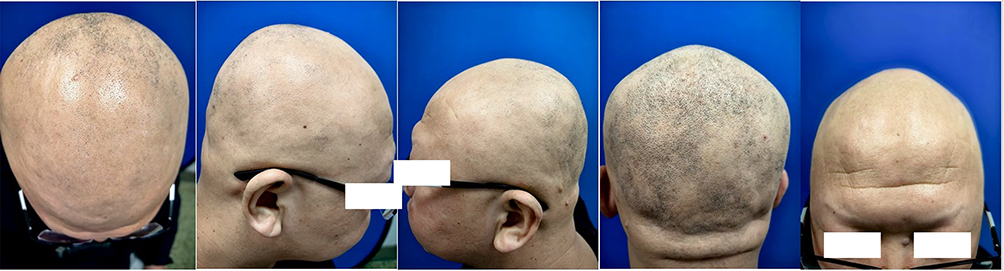 |
Figure 1 Before treatment. Examination revealed multiple patches of hair loss on the entire scalp, Severity of Alopecia Tool (SALT) score was 79. |
 |
Figure 2 After ritlecitinib treatment for 100 days. No notable hair regrowth and exacerbation of the SALT score to 83 was noted. |
 |
Figure 3 After upadacitinib treatment for 7 weeks.Patches of new black hair growth was observed and SALT score was 65. |
 |
Figure 4 After upadacitinib treatment for 15 weeks.80% of the normal hair volume was restored, accompanied by partial regrowth of eyebrows and beard and a SALT score of 20. |
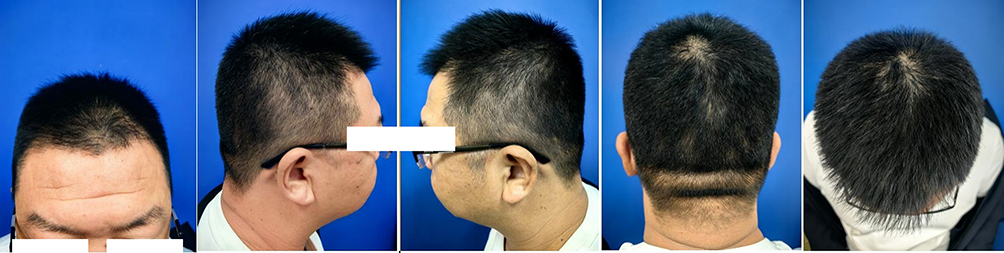 |
Figure 5 After upadacitinib treatment for 24 weeks.Hair growth had completely normalized, with no discernible areas of alopecia. |
Discussion
The pathogenesis of AA remains poorly understood and can be potentially attributed to a combination of genetic, immunological, as well as environmental factors. Moreover, several cytokines are implicated in the pathogenesis of AA, including JAK-STAT signaling.4 Interferon-gamma (IFN-γ) activates the JAK-STAT1 signaling pathway, which subsequently upregulates interleukin-15 (IL-15) expression in hair follicle epithelial cells. Thereafter, IL-15 can bind to receptors on CD8+ T cell surfaces and upregulate IFN-γ expression via downstream JAK1, JAK3, and STAT5 signaling pathways, thereby forming a positive feedback loop in the pathogenesis of alopecia areata.5 Upadacitinib is a selective JAK1 inhibitor approved by the US Food and Drug Administration, the European Medicines Agency, and other global regulatory agencies for treating various chronic inflammatory diseases. In dermatology, upadacitinib is prescribed for conditions such as moderate-to-severe atopic dermatitis, psoriatic arthritis, and ankylosing spondylitis.6 The efficacy of upadacitinib against refractory AA is already well-known.7,8 Furthermore, it has also demonstrated potential in treating baricitinib-resistant AA.8 Although upadacitinib treatment for AA is yet to receive approval, the present case study documents its efficacy in treating severe ritlecitinib-resistant AA. This can be attributed to ritlecitinib being a JAK3 inhibitor, whereas upadacitinib functions primarily as a selective JAK1 inhibitor. The pathogenesis of AA may involve JAK1-mediated signaling pathways more predominantly, thus potentially rendering upadacitinib more effective in inhibiting this pathway. Although both ritlecitinib and upadacitinib act by inhibiting JAK signaling pathways, their impact on different immune cell types and cytokines may differ, consequently influencing their efficacy in specific patients. Furthermore, significant variations in genetic background, immune status, and disease phenotype among patients may lead to different responses to various JAK inhibitors. The limitation of this case is the lack of a washout period, this does not preclude the potential for a synergistic impact or a delayed pharmacodynamic response following the treatment switch. Therefore, further research on the effects of upadacitinib on AA can elucidate its potential as an efficacious therapeutic modality for refractory AA.
Conclusion
This report demonstrated the efficacy of upadacitinib in treating severe ritlecitinib-resistant AA. It indicated the clinical implications of using an alternative JAK inhibitor in cases where other common JAK drugs exhibit failure. Nevertheless, further research is required to determine the efficacy and safety of upadacitinib in diverse patient populations, along with establishing its optimal applicability in AA remediation.
Data Sharing Statement
The original contributions presented in the study are included in the article material. Further inquiries can be directed to the corresponding author.
Ethics Statement
This study did not require any institutional approval.
Consent Statement
The authors state that they have obtained both verbal and written informed consent from the patient and their guardian for the treatment strategy within this case report. Additionally, the patient and the guardian provided their express consent to publish the case details and images.
Acknowledgments
This study was funded by Tianjin Key Medical Discipline Construction Project (Grant No:TJYXZDXK-3-010C).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas: took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. King BA, Craiglow BG. Janus kinase inhibitors for alopecia areata. J Am Acad Dermatol. 2023;89(2S):S29–4. doi:10.1016/j.jaad.2023.05.049
2. Gori N, Cappilli S, Di Stefani A, Tassone F, Chiricozzi A, Peris K. Assessment of alopecia areata universalis successfully treated with upadacitinib. Int J Dermatol. 2023;62(2):e61–e63. doi:10.1111/ijd.16342
3. Youssef S, Bordone LA. Effective treatment of alopecia universalis with oral upadacitinib. JAAD Case Rep. 2022;19(31):80–82. doi:10.1016/j.jdcr.2022.08.014
4. Park H, Yu DA, Kwon O. Janus kinase inhibitors: an innovative treatment for alopecia areata. J Dermatol. 2019;46(8):724–730. doi:10.1111/1346-8138.14986
5. Divito SJ, Kupper TS. Inhibiting Janus kinases to treat alopecia areata. Nat Med. 2014;20(9):989–990. doi:10.1038/nm.3685
6. Mohamed MEF, Bhatnagar S, Parmentier JM, Nakasato P, Wung P. Upadacitinib: mechanism of action, clinical, and translational science. Clin Transl Sci. 2024;17(1):e13688. doi:10.1111/cts.13688
7. Wang Q, Shen L, Sha Y, et al. Upadacitinib for refractory alopecia areata unresponsive to prior systemic therapies: a retrospective study. J Am Acad Dermatol. 2025;93(3):761–763. doi:10.1016/j.jaad.2025.04.070
8. Chambres F, Tétart F, Janela-Lapert R, et al. Efficacy of upadacitinib in patients with severe alopecia areata, including baricitinib-refractory cases: a case series of 22 patients. J Am Acad Dermatol. 2025;94(1):269–271. doi:10.1016/j.jaad.2025.08.109
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.