Back to Journals » International Medical Case Reports Journal » Volume 19
Successful Pregnancy After Therapeutic Apheresis in a Complex Case of PCOS, Hashimoto Thyroiditis, Recurrent Implantation Failure, and Potential Occupational Environmental Exposure
Authors Och P, Bornstein SR, Steenblock C ![]()
Received 2 April 2026
Accepted for publication 28 May 2026
Published 12 June 2026 Volume 2026:19 614140
DOI https://doi.org/10.2147/IMCRJ.S614140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Philipp Och,1 Stefan R Bornstein,1– 3 Charlotte Steenblock1
1Department of Internal Medicine III, University Hospital Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany; 2School of Cardiovascular and Metabolic Medicine and Sciences, Faculty of Life Sciences & Medicine, King’s College London, London, UK; 3Department of Endocrinology, Diabetology and Clinical Nutrition, University Hospital Zurich (USZ) and University of Zurich (UZH), Zurich, Switzerland
Correspondence: Charlotte Steenblock, Department of Internal Medicine III, University Hospital Carl Gustav Carus, Technische Universität Dresden, Fetscherstrasse 74, Dresden, 01307, Germany, Tel +4935145816130, Email [email protected]
Abstract: Both polycystic ovary syndrome and Hashimoto thyroiditis are commonly associated with female infertility. Each condition may impair reproductive function through distinct but sometimes overlapping mechanisms, and their co-occurrence has been associated with an even higher risk of infertility. In this single-case report, we describe a 33-year-old female with established polycystic ovary syndrome (anti-Müllerian hormone [AMH] 20 ng/mL) and autoimmune thyroiditis (anti-thyroid peroxidase [anti-TPO] antibodies 917 IU/mL) with infertility persisting since 2020. After multiple unsuccessful cycles of ovarian stimulation, advanced fertility treatment with in vitro fertilization and repeated embryo transfers was initiated in 2023, initially without success. Extracorporeal therapeutic apheresis was applied as an adjunctive intervention with the aim of modulating markers of oxidative stress (baseline nitrotyrosine level 883 ng/mL). It was also intended to reduce potential environmental contaminants, including elemental mercury and anesthetic gases, which the patient, a dentist, may have been exposed to in her occupational setting. These exposures have been associated with adverse reproductive outcomes. Pregnancy was successfully documented in December 2024, followed by the birth of a healthy girl in September 2025. This case demonstrates a temporal association between targeted interventions and successful pregnancy, highlighting the importance of considering both immunological and environmental factors in the management of complex infertility. The findings underscore the need for individualized strategies to address multifactorial infertility challenges.
Keywords: infertility, PCOS, Hashimoto thyroiditis, therapeutic apheresis
Introduction
Infertility is defined by the WHO as the failure to conceive despite regular, unprotected sexual intercourse for at least twelve months. Current estimates suggest that approximately 16.6% of individuals of reproductive age worldwide are affected by infertility.1 Polycystic ovary syndrome (PCOS) and Hashimoto thyroiditis are among the most common endocrine and autoimmune disorders in women of reproductive age. PCOS is a leading cause of anovulatory infertility worldwide, affecting approximately 10–13% of women in this population and accounting for an estimated 70–80% of anovulatory infertility cases, primarily through hormonal imbalance, chronic anovulation, and metabolic disturbances.2–4 Hashimoto thyroiditis, mediated by thyroid autoimmunity and often associated with hypothyroidism, has been linked to ovarian dysfunction, menstrual irregularities, and impaired ovulation, and is associated with an increased risk of infertility (odds ratio ~1.4–1.6).5 When both conditions are present, reproductive impairment may be more pronounced In women with PCOS, the coexistence of Hashimoto thyroiditis has been linked to lower anti-Müllerian hormone levels compared to PCOS alone (eg., ~5.4 ± 3.1 vs. 7.1 ± 3.8 ng/mL; p < 0.05), suggesting a possible adverse effect on ovarian reserve and possibly on treatment response.6 Both disorders are characterized by chronic systemic inflammation, which leads to increased oxidative stress.7 Women with these disorders have an increased risk of remaining childless despite extensive fertility treatments. This underscores the need for strategies that also take these immunological factors of reproductive dysfunction into account. Extracorporeal therapeutic apheresis, traditionally used to reduce lipoprotein levels in patients with familial hypercholesterolemia and elevated lipoprotein(a), can also modulate inflammatory pathways. Beyond its lipid-lowering effects, it exerts systemic effects, including the reduction of circulating pro-inflammatory and oxidized plasma components, which in turn has been associated with reductions in markers of oxidative stress.8–10 At the same time, improvements in microcirculation and endothelial function have been reported, as reflected by clinically relevant improvements in walking distance and regression of ischemic tissue lesions, alongside reductions in fibrinogen and inflammatory and endothelial activation markers such as hs-CRP (~67% reduction), sVCAM-1 (~37% reduction), and sE-selectin (~24% reduction), which collectively indicate changes consistent with improved blood rheology and reduced endothelial activation.11 Together, these effects may reflect a systemic milieu characterized by lower inflammatory and oxidative burden. Available exploratory data suggest a possible short-term temporal association between extracorporeal apheresis and changes in reproductive outcomes, with some observations suggesting short-term changes within the first months after treatment. This observation remains preliminary and has not been confirmed in controlled studies.12
Case Presentation
A 33-year-old female dentist presented to a fertility clinic with her partner in August 2023. She had been trying unsuccessfully to conceive since 2020. Her medical history included PCOS, diagnosed in 2011 when her menstrual cycle was irregular to amenorrheic. In addition, she had been diagnosed with Hashimoto thyroiditis in 2022 after developing new, persistent swallowing difficulties. At the time of diagnosis, her anti-thyroid peroxidase (anti-TPO) antibodies were significantly elevated at 917 IU/mL (Reference: <34 IU/mL) (Table 1). Thyroid function was stabilized with levothyroxine (25 μg, once daily).
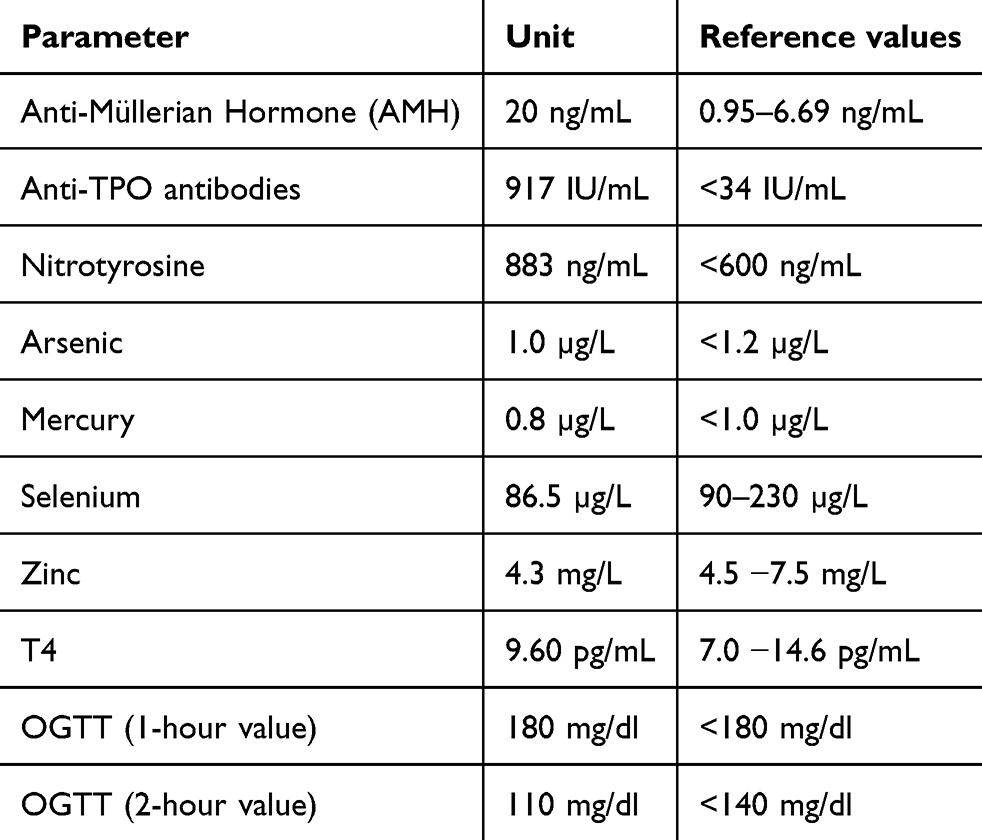 |
Table 1 Clinical Parameters of the Patient |
Initial treatment for infertility consisted of six cycles of off-label letrozole therapy (2.5 mg), ovulation induction with chorionic gonadotropin alfa (Ovitrelle 250 mcg), and concomitant administration of vaginal progesterone suppositories (Cyclogest 400 mg). The patient was monitored with blood tests and ultrasound. Despite adequate follicular maturation, pregnancy did not occur.
The therapy was intensified and the patient was now treated with controlled ovarian stimulation using follitropin alfa (Ovaleap 150 IU) injections and additional ovulation induction with chorionic gonadotropin alfa (Ovitrelle 250 mcg) and vaginal progesterone suppositories (Cyclogest 400 mg) over six further cycles, also without successful pregnancy.
The couple was then given detailed information about the possibilities of in vitro fertilization (IVF) / intracytoplasmic sperm injection (ICSI) treatment. During the initial stimulation phase with follitropin alfa (Ovaleap 150 IU) and human chorionic gonadotropin (HCG) (Brectavid 5000 IU), grade II ovarian hyperstimulation syndrome (OHSS) occurred, requiring one week of inpatient treatment. Twenty-six oocytes were retrieved, 13 of which were successfully cryopreserved at the pronucleus stage. They were later thawed, fertilized, and cultured, resulting in three blastocysts per transfer.
After a regeneration phase of about three months, three consecutive transfers of high-quality, 4- to 5-day-old blastocysts were performed in stimulated cycles with estradiol (Estrifam 1 mg) and vaginal progesterone suppositories (Cyclogest 400 mg). Despite optimal endometrial thickness and high embryo quality, all three transfers failed to result in pregnancy, thereby meeting the clinical criteria for recurrent implantation failure (RIF). Further laboratory tests in preparation for extracorporeal therapeutic apheresis revealed evidence of increased oxidative stress and continued active Hashimoto thyroiditis. Toxic metals were also determined in the blood as the patient works as a dentist; arsenic levels of 1.0 µg/L (SI: 13.3 nmol/L) (reference range < 1.2 µg/L (SI: < 16.0 nmol/L)) and mercury levels of 0.8 µg/L (SI: 4.0 nmol/L (reference range < 1.0 µg/L (SI: < 5.0 nmol/L)) were interpreted as borderline (Table 1).
Diagnostic Assessment
The anti-Müllerian hormone (AMH) level was 20 ng/mL (SI: 143 pmol/L) (reference range women 30–34 years 0.95–6.69 ng/mL (SI: 6.8–47.8 pmol/L)), indicating a pronounced ovarian reserve in the context of PCOS (Table 1). Other hormone levels were within the normal range. The gynecological examination and transvaginal ultrasound at the fertility clinic showed enlarged ovaries on both sides with a typical “string of pearls” configuration and no structural uterine abnormalities. Hashimoto thyroiditis, confirmed by sonography, with severely elevated anti-TPO antibodies was successfully converted to a euthyroid metabolic state under L-thyroxine therapy.
The patient had lived exclusively in large cities since childhood and was therefore chronically exposed to increased air pollution and environmental stress. Due to her profession as a dentist, chronic exposure to heavy metals, especially mercury vapors during amalgam removal, was also suspected. Laboratory tests showed significantly elevated nitrotyrosine concentrations of 883 ng/ mL (SI: 3.89 µmol/L) (reference range <600 ng/mL (SI: <2.64 µmol/L)), indicating pronounced oxidative and nitrosative stress, as well as reduced selenium and zinc levels, indicating reduced antioxidant capacity (Table 1).
Treatment
Given the repeated implantation failure despite favorable embryo quality and adequate endometrial preparation, together with persistent autoimmune activation and increased oxidative stress markers, extracorporeal therapeutic apheresis was considered an individualized experimental therapeutic approach after exhaustion of established reproductive treatment options. The treatment was carried out in an INUSpheresis® practice using the INUS-30 system and the TKM-58 filter. The duration of each therapy session was approximately three hours. The therapy was carried out on two days, with a one-day break in between. Two large-lumen peripheral venous accesses were established for each treatment. The accesses were established without any problems. A 0.4 µm filter was inserted on the first day and a 0.2 µm filter on the second day of treatment. Heparin was used for anticoagulation. This was followed by an individualized vitamin B and C infusion. There were no acute side effects. The eluate showed a dark orange color with numerous streaks in both runs (Figure 1). A detailed laboratory analysis of the eluate was refused by the patient. Before and after apheresis, the patient continued her professional activities as a dentist without interruption; there was no interruption except on the day of embryo transfer.
 |
Figure 1 Extracorporeal therapeutic apheresis eluate. First blood was drawn from a large vein and processed through an INUS-30 system. Then a porous membrane was used to separate blood cells from plasma. The plasma was processed through a TKM-58 filter for removal of different blood components. The remaining blood components were reinfused into the patient through a second venous access. The components removed from the plasma are contained in the eluate. |
Outcome and Follow-Up
Approximately four weeks after apheresis, another embryo transfer was performed in an artificially constructed cycle with estradiol (Estrifam 1 mg) and vaginal progesterone suppositories (Cyclogest 400 mg). The pregnancy test was positive. In the 7th week of pregnancy, an intact intrauterine pregnancy with fetal heart action was confirmed sonographically. The course of the pregnancy was without complications; the fetal development corresponded to the gestational age and the thyroid values were stable on L-thyroxine. The thyroid values and autoantibodies were determined in the gynecologist’s practice and were within the normal range.
The subsequent pregnancy proceeded without complications. During the pregnancy, the OGTT showed minimal abnormalities (1-hour value at the borderline, 2-hour value normal); in consultation with the diabetologists, no therapy was given (Table 1). At 41 weeks of gestation, a spontaneous vaginal delivery was achieved with epidural analgesia support. After five years of involuntary childlessness, the patient delivered a healthy female infant weighing 4.5 kg.
Patient Perspective and Ethical Considerations
The patient described the prolonged infertility course and repeated treatment failures as emotionally highly burdensome. After multiple unsuccessful evidence-based fertility treatments, she perceived extracorporeal therapeutic apheresis as a final individualized therapeutic attempt and expressed a strong desire to proceed despite the experimental nature of the intervention. Following detailed counseling regarding the limited clinical evidence, potential risks, and uncertain benefit of the procedure, informed consent for treatment and publication was obtained. From a clinical perspective, the intervention was considered only after established reproductive treatment options had been exhausted, including repeated transfers of high- quality blastocysts with adequate endometrial preparation. Given the persistent autoimmune activation, increased oxidative stress markers, and the absence of major structural reproductive abnormalities, extracorporeal therapeutic apheresis was regarded as a proportionate individualized therapeutic approach in this specific clinical context.
Discussion
This case highlights the multifactorial nature of the patient’s infertility. The established diagnoses of PCOS and Hashimoto thyroiditis may contribute to a broader systemic dysregulation that could also affect local perfusion and microcirculation. Both conditions are characterized by chronic, low- grade inflammation and increased oxidative stress.7 It is therefore conceivable that the cumulative systemic burden, further exacerbated by occupational exposure to environmental toxins such as mercury vapor during amalgam removal, may have adversely affected endometrial receptivity despite adequate reproductive treatment and multiple transfers of high-quality embryos.13,14 In this case, elevated nitrotyrosine concentrations together with reduced selenium and zinc levels suggested increased oxidative stress and reduced antioxidant reserve.15
Successful implantation occurred in close temporal relation to the extracorporeal therapeutic apheresis performed. The rationale of this systemic therapeutic approach is supported by parallels to other chronic inflammatory syndromes in which persistent inflammation, endothelial dysfunction, and oxidative stress play a central role. For example, we and others have previously shown that extracorporeal apheresis may have a potential therapeutic option in chronic post-COVID-19 syndrome and chronic fatigue syndrome, diseases also characterized by persistent systemic inflammation, endothelial dysfunction, and metabolic dysregulation by reducing pro-inflammatory cytokines (eg., IL-6, TNF-α, and CRP), autoantibodies, and oxidized lipids, thereby potentially contributing to improved immunometabolic balance.16–22
In this case, extracorporeal therapeutic apheresis may have contributed through several complementary mechanisms: first, by reducing pathogenic autoantibodies and the associated inflammatory cascades in the context of Hashimoto thyroiditis; second, by removing pro- inflammatory and oxidized lipids related to PCOS-associated metabolic stress; and third, by possibly reducing circulating levels of heavy metals as recently shown.18
This latter aspect is especially pertinent in the present case, given the patient’s occupation as a dentist, as reproductive risks have been associated with occupational exposure to dental practice agents. For example, exposure to nitrous oxide has been linked to reduced fertility and an increased risk of spontaneous abortion.23 In addition, heavy metals, including mercury from amalgam exposure, have been associated with impaired reproductive function by disrupting hormonal balance, damaging gametes, and impairing reproductive function in both females and males, thereby contributing to reduced fertility and adverse pregnancy outcomes.24,25
The systemic relief achieved by extracorporeal apheresis may have contributed to improved endothelial function and endometrial microcirculation, which could have supported implantation. The clinical relevance of these mechanisms is supported by previous studies, such as the work by Dubinskaya et al, who reported a significant improvement in immunological parameters and an increased pregnancy rate after plasmapheresis in patients with treatment-resistant infertility and endometriosis. In women with endometriosis-associated infertility and NAT2 polymorphisms, pregnancy rates during follow-up were reported to be up to 6.5-fold higher after therapeutic plasmapheresis, while early pregnancy loss occurred four times less frequently compared with controls. Although these findings are not directly transferable to the present case, they support the hypothesis that systemic inflammatory and oxidative mechanisms may influence reproductive outcomes.12 Another study by Muller et al reported three women with recurrent IVF failure and detectable anti-hCG antibodies who were treated with a combined immunomodulatory regimen consisting of membrane plasmapheresis, low-dose corticosteroids, and intravenous immunoglobulins before/around IVF. All three subsequently achieved pregnancy and live birth without major adverse events. The study suggests that apheresis may be a useful adjunct in highly selected cases of suspected autoimmune infertility.26 Furthermore, apheresis, plasmapheresis, and immunoadsorption have been shown to significantly improve live birth rates and reduce pregnancy loss in women with refractory autoimmune conditions27,28. Nevertheless, causality between extracorporeal therapeutic apheresis and successful implantation cannot be inferred from a single case report. Spontaneous pregnancy after repeated embryo transfer cannot be excluded. Furthermore, serial laboratory measurements before and after treatment were limited, and no eluate analysis was available.
Against this background, apheresis appears to be a potentially useful systemic therapeutic approach for complex or immunologically mediated fertility disorders.29 Furthermore, this approach may be relevant in patients with increased exposure to environmental or occupational toxins, such as those working in dental practice settings.30 Rather than acting solely on local endometrial mechanisms, extracorporeal therapeutic apheresis may contribute to a more favorable balance between oxidative stress, immune activity, and microcirculatory function.
In conclusion, this case underscores the temporal association between targeted systemic therapeutic interventions and successful pregnancy, emphasizing the importance of integrating both immunological and environmental factors into the management of complex infertility. The findings highlight the potential value of personalized approaches when addressing the multifactorial challenges of infertility, while also acknowledging the need for larger, controlled studies to validate these observations.
Data Sharing Statement
Data sharing does not apply to this article as no datasets were generated or analyzed during the current study.
Ethics Approval
This case report did not require institutional review board approval. Informed consent for publication of de-identified clinical information was obtained from the patient.
Funding
Funding was provided by Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) Project Number 522201563 – IRTG 3019/1.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. WHO fact sheet on infertility. Global Reproductive Health. 2021;6(1):e52–7. doi:10.1097/grh.0000000000000052
2. Deswal R, Narwal V, Dang A, Pundir CS. The prevalence of polycystic ovary syndrome: a brief systematic review. J Human Reproduct Sci. 2020;13(4):261–271. doi:10.4103/jhrs.JHRS_95_18
3. Kahn LG, Hipwell AE, Charifson M, Ling R, Cajachagua-Torres KN, Ghassabian A. Maternal polycystic ovarian syndrome and offspring psychopathology and neurodevelopment. Hum Reprod. 2025;40(7):1257–1265. doi:10.1093/humrep/deaf079
4. Teede H, Deeks A, Moran L. Polycystic ovary syndrome: a complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010;8(1):41. doi:10.1186/1741-7015-8-41
5. Orouji Jokar T, Fourman LT, Lee H, Mentzinger K, Fazeli PK. Higher TSH levels within the normal range are associated with unexplained infertility. J Clin Endocrinol Metab. 2018;103(2):632–639. doi:10.1210/jc.2017-02120
6. Serin AN, Birge Ö, Uysal A, Gorar S, Tekeli F. Hashimoto’s thyroiditis worsens ovaries in polycystic ovary syndrome patients compared to Anti-Müllerian hormone levels. BMC Endocr Disord. 2021;21(1):44. doi:10.1186/s12902-021-00706-9
7. Batog G, Doloto A, Bak E, et al. The interplay of oxidative stress and immune dysfunction in Hashimoto’s thyroiditis and polycystic ovary syndrome: a comprehensive review. Front Immunol. 2023;14:1211231. doi:10.3389/fimmu.2023.1211231
8. Kopprasch S, Bornstein SR, Bergmann S, Graessler J, Hohenstein B, Julius U. Long-term follow-up of circulating oxidative stress markers in patients undergoing lipoprotein apheresis by Direct Adsorption of Lipids (DALI). Atheroscler Suppl. 2017;30:115–121. doi:10.1016/j.atherosclerosissup.2017.05.029
9. Mickiewicz A, Kreft E, Kuchta A, et al. The impact of lipoprotein apheresis on oxidative stress biomarkers and high-density lipoprotein subfractions. Oxid Med Cell Longev. 2020;2020:9709542. doi:10.1155/2020/9709542
10. Walther R, Singh B, Yin X, et al. Proteomic Profiling of Age-Related Proteins Following Extracorporeal Apheresis. Horm Metab Res. 2025;57(11):626–631. doi:10.1055/a-2563-1187
11. Rotella S, Gesualdo L, Fiorentino M. Heparin-mediated extracorporeal low-density lipoprotein precipitation apheresis for treating peripheral arterial disease in patients with chronic kidney disease. J Clin Med. 2024;13(4):1121. doi:10.3390/jcm13041121
12. Dubinskaya E, Lapteva N, Lukyanova Y. The use of plasmapheresis in treatment of patients with infertility, peritoneal endometriosis and Nat2 gene polymorphism. EUREKA. 2016;2(2):3–10. doi:10.21303/2504-5679.2016.00087
13. Al-Saleh I, Coskun S, Mashhour A, et al. Exposure to heavy metals (lead, cadmium and mercury) and its effect on the outcome of in-vitro fertilization treatment. Int J Hyg Environ Health. 2008;211(5–6):560–579. doi:10.1016/j.ijheh.2007.09.005
14. Escalante E, Semenova Y, Peana M, Bjorklund G. The impact of mercury from dental amalgams on pregnancy and childhood: a health and risk assessment evaluation. Curr Med Chem. 2025;32:7193–7212. doi:10.2174/0109298673334663250101101006
15. Grieger JA, Grzeskowiak LE, Wilson RL, et al. Maternal selenium, copper and zinc concentrations in early pregnancy, and the association with fertility. Nutrients. 2019;11(7):1609. doi:10.3390/nu11071609
16. Achleitner M, Steenblock C, Danhardt J, et al. Clinical improvement of Long-COVID is associated with reduction in autoantibodies, lipids, and inflammation following therapeutic apheresis. Mol Psychiatry. 2023;28(7):2872–2877. doi:10.1038/s41380-023-02084-1
17. Bornstein SR, Voit-Bak K, Rosenthal P, et al. Extracorporeal apheresis therapy for Alzheimer disease—targeting lipids, stress, and inflammation. Mol Psychiatry. 2020;25(2):275–282. doi:10.1038/s41380-019-0542-x
18. Castillo-Aleman YM, Villegas-Valverde CA, Al-Karam M, et al. Double filtration plasmapheresis for environmental toxin removal: a case series of patients with hyperlipoproteinemia(a). J Clin Apher. 2025;40(5):e70060. doi:10.1002/jca.70060
19. Korth J, Steenblock C, Walther R, Barbir M, Husung M, Velthof A. A single-center pilot study of therapeutic apheresis in patients with severe post-COVID syndrome. Horm Metab Res. 2024;56(12):869–874. doi:10.1055/a-2445-8593
20. Pressler H, Machule M-L, Ufer F, et al. IA-PACS-CFS: a double-blinded, randomized, sham-controlled, exploratory trial of immunoadsorption in patients with chronic fatigue syndrome (CFS) including patients with post-acute COVID-19 CFS (PACS-CFS). Trials. 2024;25(1):172. doi:10.1186/s13063-024-07982-5
21. Steenblock C, Walther R, Kok Y, et al. Single-center study of therapeutic apheresis in 24 male Patients from the MENA region: reduction of lipids, inflammatory markers, autoantibodies, and implications for fatigue, genetics, and aging. Horm Metab Res. 2025;57(11):646–652. doi:10.2174/0109298673334663250101101006
22. Stein E, Heindrich C, Wittke K, et al. Efficacy of repeated immunoadsorption in patients with post-COVID myalgic encephalomyelitis/chronic fatigue syndrome and elevated β2-adrenergic receptor autoantibodies: a prospective cohort study. Lancet Reg Health Eur. 2025;49:101161. doi:10.1016/j.lanepe.2024.101161
23. Olfert SM. Reproductive outcomes among dental personnel: a review of selected exposures. J Can Dent Assoc. 2006;72(9):821–825.
24. Marconi G, Di Resta C, Naclerio A, Banfi G, Tomaiuolo R. Heavy metals and human reproductive toxicity: mechanisms, pregnancy outcomes, and mitigation strategies. Reprod Toxicol. 2026;139:109104. doi:10.1016/j.reprotox.2025.109104
25. Picard G, Prakash T, Labreche F, Gravel S. Occupational exposures to chemicals in dentistry: a scoping review. J Occup Environ Hyg. 2025;22(12):970–986. doi:10.1055/a-2678-7739
26. Muller V, Ob’edkova K, Krikheli I, et al. Successful pregnancy outcome in women with recurrent ivf failure and anti-hcg autoimmunity: a report of three cases. Case Reports Immunol. 2016;2016:4391537. doi:10.1080/15459624.2025.2540834
27. He L, Sims C. Impact of Antiphospholipid syndrome on reproductive outcomes: current insights and management approaches. Semin Reprod Med. 2024;42(3):197–208. doi:10.1055/s-0044-1790225
28. Ruffatti A, Favaro M, Hoxha A, et al. Apheresis and intravenous immunoglobulins used in addition to conventional therapy to treat high-risk pregnant antiphospholipid antibody syndrome patients. A prospective study. J Reprod Immunol. 2016;115:14–19. doi:10.1016/j.jri.2016.03.004
29. Connelly-Smith L, Alquist CR, Aqui NA, et al. Guidelines on the use of therapeutic apheresis in clinical practice - evidence-based approach from the writing committee of the american society for apheresis: the ninth special issue. J Clin Apher. 2023;38(2):77–278. doi:10.1002/jca.22043
30. Guan D, Sun W, Gao M, Chen Z, Ma X. Immunologic insights in recurrent spontaneous abortion: molecular mechanisms and therapeutic interventions. Biomed Pharmacother. 2024;177:117082. doi:10.1016/j.biopha.2024.117082
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lipidomics Reveals Common Mechanisms in Polycystic Ovarian Syndrome, Recurrent Spontaneous Abortion, and Infertility: A Genetic-Based Analysis
Tao A, Wu T, Han X, Niu D, Feng X
International Journal of Women's Health 2025, 17:1055-1065
Published Date: 13 April 2025