Back to Journals » International Medical Case Reports Journal » Volume 19
Successful Management of Infected Widely Dehisced Wound Using Progressive Tension Sutures: Case Report
Authors Asrat K, Fikadu T, Tesfai B ![]() , Mekonen S, Frezgi O
, Mekonen S, Frezgi O ![]()
Received 20 November 2025
Accepted for publication 10 February 2026
Published 19 February 2026 Volume 2026:19 583069
DOI https://doi.org/10.2147/IMCRJ.S583069
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Kibreab Asrat,1,2 Tekeste Fikadu,3 Berhe Tesfai,1,2 Salem Mekonen,1,2 Okbu Frezgi1,2
1Department of Obstetrics and Gynaecology, Orotta National Referral Maternity Hospital, Ministry of Health, Asmara, Eritrea; 2Department of Obstetrics and Gynaecology, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 3Department of Surgery, Orotta College of Medicine and Health Sciences, Asmara, Eritrea
Correspondence: Okbu Frezgi, Email [email protected]
Background: Surgical wound dehiscence is a life-threatening postoperative complication mainly related to a failure of wound healing that leads to psychosocial stress in patients and their caregivers. Here, we report a successful management of widely dehisced wound using progressive tension sutures in low-resources setting.
Case Report: A 35-year-old grand multipara woman underwent caesarean section for fetal distress. On postoperative day five, she developed a surgical site infection and the wound dehisced. After two failed attempts of dehisced wound closure she was referred to our hospital. The midline widely dehisced wound was dirty but all her investigative studies were within normal range, except for hypoalbuminemia. She was successfully treated with wound dressing, broad-spectrum antibiotics, and progressive approximation of wound edges using tension sutures, without the application of a Mesh.
Conclusion: After full wound bed granulation, a progressive approximation of wound edges using tension sutures at an interval of two to three weeks could increase the success of widely dehisced surgical wound closure without applying Mesh in resource-limited areas.
Keywords: surgical wound dehiscence, surgical site infection, hospital stays, tension sutures
Introduction
Surgical wound dehiscence (SWD) is the separation of the margins of a closed surgical incision in skin, with or without exposure or protrusion of underlying tissue, organs, or implants.1 Broadly, SWD could be a partial or total separation of previously approximated wound edges due to failure of wound healing.2–4 In partial dehiscence, only the superficial layers or part of the tissue layers reopen, but in complete wound dehiscence, all layers of the wound thickness are separated.5,6 If the intestine protrudes through the separated wound, the term evisceration (burst abdomen) is used.4 The dehisced incision may or may not be associated with clinical signs and symptoms of infection. Depending on the presence of infection and depth of separation, SWD has four grades (Table 1). In the majority of patients, SWD occurs between the fifth and 14th postoperative day.3,4,7,8 SWD is rare, with a frequency of 0.06% and 7%. Nonetheless, the reported mortality rate reaches as high as 45%.3,6–9
 |
Table 1 Sandy Classification System of the World Union of Wound Healing Societies (WUWHS, 2018) |
The major risk factors for SWD include post-operative wound infection, older age, hypoproteinemia, emergency surgery, duration of surgery, obesity (BMI exceeding 30), chronic obstructive pulmonary disease (COPD), smoking, diabetes, malnutrition, radiation, and poor perfusion.1,4,6,9,10 Hematoma or seroma at the incision site, described in 2–5% of women after CS, has been known to act as a predisposing factor to wound infection and subsequently to wound dehiscence.8 Abnormal wound healing, untying of the suture knots, and mechanical stress can also lead to SWD.6,10–12 Various surgical interventions are used to address SWD, some of which include tension suturing, Mesh repair, Bogota bag, and vacuum-assisted closure.3 Here, we report a case of complete wound dehiscence successfully managed by progressive approximation of widely separated wound edges by tension sutures.
Case Report
A 35-year-old Para-VII Eritrean woman was referred to Orotta National Referral Teaching Hospital as a case of intractable wound dehiscence. She was a postpartum patient on day 30 who delivered by caesarean section for a prolonged second stage and fetal distress. The membrane ruptured during the active phase of labor and was meconium-stained. On postoperative day 5, the patient developed a surgical site infection, complicating wound dehiscence. Consequently, the patient had a fever and occasional diarrhea that subsided after five days of broad-spectrum antibiotic treatment. Following two failed attempts at dehisced wound closure at an interval of one week, the patient was referred to Orotta National Referral Hospital for further treatment.
On arrival at our hospital, she was chronically ill-looking and emaciated with normal vital signs. She had pink conjunctivae and nonicteric sclera. The abdomen was moderately distended with a longitudinal midline incision below the umbilicus. The size of the wound bed was 20 cm by 18 cm, and protruding abdominal contents through the dehisced wound, but covered by the peritoneum (Figure 1a). On vaginal examination, the cervical os was closed, without discharge or bleeding. Transabdominal ultrasound revealed an empty uterus without any collection of intra-abdominal fluid or abscess. The complete blood count, liver function test, and renal function test were all within normal range. But the serum albumin was low (hypoalbuminemia). Under general anesthesia, thorough debridement was done; the patient was started on broad-spectrum antibiotics, followed by daily wound dressing with normal saline. Eventually, the wound slowly started to granulate (Figure 1b).
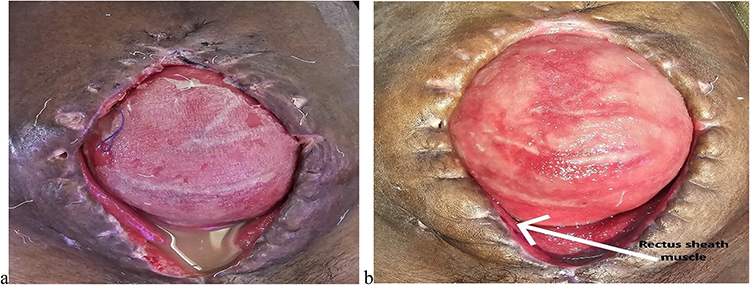 |
Figure 1 (a) Dirty wound with purulent discharge and widely separated wound edges upon hospital admission. (b) Clean wound with some granulation tissue after a week of dressing and antibiotic treatment, and the arrow shows the separated edge of the rectus sheath muscle. |
With the dressing and wound healing, the wound contracture began to approximate the wound edges (Figure 2a). Progressive approximation of the wound edges using tension sutures was performed at an interval of three weeks under spinal anesthesia (Figure 2b). The through-and-through retention sutures with Vicryl number 2 passing through a sterile intravenous set (tube) were placed at a distance of 2 cm from the skin through all layers of the wound to strengthen the tension (Figure 2b). After 3 weeks, the tension sutures were removed, and the wound base decreased to a width of 3 centimeters.
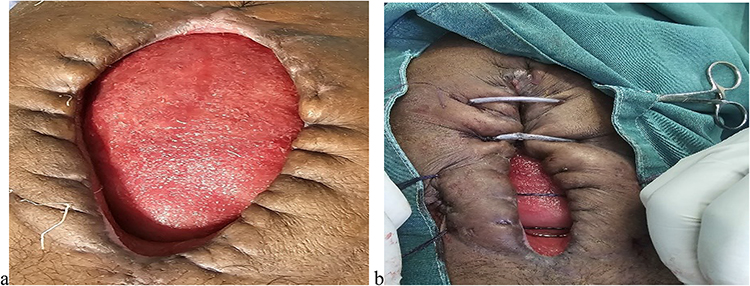 |
Figure 2 (a) After 2 weeks of wound dressing, wound contracture started to approximate the wound edges. (b) Further approximation of wound edges using tension sutures. |
Finally, after the removal of the tension sutures, the patient was taken to the operating room for the third time, and the ragged and scarred wound edges were debrided, and the closure was left to heal by third intention. Another set of tension sutures was placed at two sites to be removed after two weeks (Figure 3a–c).
 |
Figure 3 (a) Removal of ragged and scarred wound edge with closure by tertiary intention. (b) Tension sutures at two sites during tertiary intention, and (c) finally, the successfully treated wound. |
Discussion
Surgical wound dehiscence is a serious postoperative complication where management poses a clinical challenge.3 Surgical wound dehiscence occurs when the wound does not gain sufficient strength to withstand the strains placed on it.3,6 It is less common (0.1% to 0.7%) in gynecologic abdominal procedures. SWD incurs high healthcare expenditures due to increased rates of reoperations and extended hospital stay.6,10,13 SWD also contributes significantly to dissatisfaction and related psychosocial stress in patients and their caregivers. In our case, the length of hospital stay could have been reduced if the wound breakdown had been recognized early, and the two initial trials of closure had been deferred. Unfortunately, it was identified when full-blown purulent discharge developed.
The risk factors and causes of SWD are similar to the causes of SSI.10 Good knowledge of the risk factors is of paramount significance for the prevention of wound dehiscence using prophylaxis.9 Factors such as excessive wound tension, choice of suturing material, and quality of tissue influence the risk of dehiscence.13 In our case, prolonged labour, the materials used in their first trial, and wound tension might have predisposed her to the recurrent wound dehiscence. Proper selection of suture material is critical in preventing wound dehiscence. If a suture has too little initial tensile strength or it is absorbed too quickly before the wound regains enough strength to resist normal stress.4 A surgeon’s expertise and surgical techniques also play a key role in preventing wound dehiscence.1,3 For high-risk groups, an interrupted far-far, near-near mass closure technique is preferred.4 In our patient, the initial surgery was performed in another hospital. Thus, we have no knowledge of the sutures used. During our progressive wound closure, we used the number 2 Vicryl tension sutures.
Low transverse incisions are 30 times stronger than midline incisions; they are also less painful, and result in less interference with postoperative respirations compared to mid-longitudinal line incisions.4 In our patient, the mid-longitudinal line incision was preferred, for fast entry for fetal distress, a decision which predisposed her to recurrent wound dehiscence. The key factors that must be considered are the timely identification of risk factors, early detection of the signs and symptoms of SWD, accurate assessment and categorization of the type of wound dehiscence, and, more importantly, prompt management.1,3 Primary SWD closure is the most common practice, unless there is no significant tissue tension. Furthermore, it is better suited for patients whose wound dehiscence is due purely to technical failure.3 In our case, the two previous attempted closures possibly failed due to incomplete tissue granulation and surgical techniques in the approximation of the edges of the wound.
Thorough wound cleaning was done to remove foreign bodies, devitalized and dead tissue, and bacteria. Complete removal of necrotic tissue minimizes bacterial burden. Debridement also removes migrated leukocytes that have phagocytized the bacteria.12 Supportive measures such as nutritional support, regular ambulation with control of infection, speed up the recovery.3 In our case, wound debridement was done once with normal saline, and wound dressing was done daily to avoid disruption of the wound response.
The use of prophylactic antibiotics can reduce the risk of infection and subsequent dehiscence.1,5,9 Emergency laparotomies have an increased risk of delayed healing, mainly due to increased contamination and inadequate preparation for surgery.1,9 In our case, the surgery was performed after a prolonged second stage of labor and fetal distress. Poor quality of wound closure, leading to inadequate tissue perfusion and thus tissue ischemia, can hinder wound healing and contribute to wound dehiscence.13 Proper postoperative wound care with appropriate wound dressing, prophylactic antibiotics, and vigilant monitoring of the surgical site are of utmost importance in preventing wound dehiscence.
Conclusion
Complete wound debridement, followed by progressive approximation of wound edges using tension sutures at the interval of two to three weeks, increases the success rate of dehisced surgical wound closure without using a Mesh in resources limited areas.
Data Sharing Statement
All available information is included in the paper.
Ethical Approval
The Ministry of Health ethical clearance committee does not require ethical approval for reporting case reports or case series.
Consent Form
Written informed consent was obtained from the patient to share her case details and any accompanying images published globally.
Acknowledgment
The authors sincerely acknowledge the patient’s willingness and consent to share her unidentified information worldwide.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Morgan-Jones R, Downie F, Dowsett C, et al. Prevention, Identification and Management of Surgical Wound Dehiscence (SWD). London: Wounds UK; 2023. www.wounds-uk.com.
2. Magro M. Reducing Surgical Site infections post-caesarean section. Int J Women’s Health. 2023;15:1811–5. doi:10.2147/IJWH.S431868
3. Abeysinghe AHMGB, Senarathne R, Wimalasena GADNB. Successful management of abdominal wound dehiscence with bogota bag, vacuum-assisted closure combined with tension sutures. J Sur Cas Rep and Img. 2021;4(7):1.
4. Rock JA, Jones HW, Te Linde RW, Wilkins LW, eds. Te Linde’s Operative Gynecology.
5. Choden N, Dorji N, Dem D, Lhaden K. Post-Cesarean Severe Sepsis and Uterine Wound Disruption Presenting as Abdominal Wound Abscess and Peritonitis: A Case Report. Vol. 10. SAGE Open Medical Case Reports; 2022:1–4.
6. Saxena G, Rai A. A study of abdominal wound dehiscence in adults-etiology and its management. Ann Int Med Den Res. 2017;3(6):SG40. doi:10.21276/aimdr.2017.3.6.SG6
7. El-Agwany EA. Conservative management of infected postpartum uterine dehiscence after cesarean section. J Med Ultrasound. 2018;26(1):59–61. doi:10.4103/JMU.JMU_5_18
8. Landy KA. Surgical site infections after cesarean delivery: epidemiology, prevention and treatment. Maternal Health Neonatol Perinatol. 2017;3(12).
9. Sreedhara DA, Bhat PR. Management of abdominal wound dehiscence at a tertiary care hospital. Int J Surg Sci. 2020;4(1):280–282. doi:10.33545/surgery.2020.v4.i1e.348
10. Kurniawan RH, Atmantika NP, Harzif AK, et al. Surgical wound dehiscence treatment. Indones J Obstet Gynecol Clin North Am. 2023;11(2).
11. Head B, Dursley J, Griffiths S. Clinical guidance on the management of wounds Sirona’s care and health. 2024.
12. Cosmin Repciuc C, Toma CG, Ober CA, et al. Management of surgical wound dehiscence by oxygen-ozone therapy in a FIV-positive cat – a case report. Acta Vet BRNO. 2020;89:189–194.
13. Itzel Juárez Campuzano T, López JDS, Bravo VHM, et al. Risk factors and management of wound dehiscence in abdominal surgery. Int J Med Sci Clin Res Stud. 2023;3(11):2767–8342.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.