Back to Journals » International Medical Case Reports Journal » Volume 19
Successful Immune Checkpoint Inhibitor Rechallenge After Sintilimab-Induced Pancreatitis: A Case Report
Authors Shi H, Ye L ![]() , Mo Q, Li R, Yu Y
, Mo Q, Li R, Yu Y
Received 28 April 2025
Accepted for publication 10 January 2026
Published 3 March 2026 Volume 2026:19 531904
DOI https://doi.org/10.2147/IMCRJ.S531904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Thomas E Hutson
Hao Shi,* Lin Ye,* Qinrong Mo, Renjian Li, Yaqun Yu
Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital of Guilin Medical University, Guilin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yaqun Yu, Department of Hepatobiliary and Pancreatic Surgery, The First Affiliated Hospital of Guilin Medical University, No. 15 Lequn Road, Xiufeng District, Guilin, Guangxi Zhuang Autonomous Region, 541000, People’s Republic of China, Tel +86 15807739295, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is the fourth most prevalent and the second most lethal cancer in China. Immune checkpoint inhibitors (ICIs) have dramatically improved treatment outcomes for advanced HCC. However, ICIs can also cause immune-related adverse events (irAEs), including the rare occurrence of ICI-related pancreatitis (ICIPI). After successful treatment of ICI-related pancreatitis, further research is needed to determine whether continuation of ICI therapy is appropriate for the patient. Currently, the clinical feasibility of resuming ICI therapy following complete resolution of ICIPI has not been definitively established. We report A 28-year-old patient diagnosed as unresectable HCC was treated with sintinilab, a programmed cell death-1 (PD-1) inhibitor, but he started appearing abdominal pain and was diagnosed with ICIPI. Following complete resolution of pancreatitis, immunotherapy was resumed with an alternative PD-1 inhibitor, tislelizumab. Ultimately achieving tumor partial response. ICIPI is a rare clinical event, and there is no unified management approach. In this case, after immune re-challenge, it not only prevented recurrence of immune ICIPI but also sustained a durable tumor partial response throughout the longitudinal follow-up period. This provides a practical treatment strategy for managing ICI-related adverse events in clinical practice.
Keywords: hepatocellular carcinoma, immune checkpoint inhibitors, immune-related adverse events, pancreatitis, case report
Introduction
Hepatocellular carcinoma (HCC) is the fourth most prevalent and the second most lethal cancer in China.1 Due to the high incidence of HBV in China, the number of HCC patients in China is significantly higher than in other nations.2–4 Moreover, the lack of clinical symptoms in the early stages of HCC often leads to a diagnosis at an advanced stage. Approximately 60–70% of patients present with locally advanced or metastatic disease at diagnosis,5 meaning that over half of the patients lose the opportunity for surgical intervention and must choose appropriate treatment options from interventional therapy, targeted therapy, immunotherapy, and radiation therapy.6 Recently years, the emergence of combination therapies involving interventional treatment, immune checkpoint inhibitors (ICIs), and targeted therapies has greatly improved the prognosis and treatment outcomes for HCC.7,8
Transarterial chemoembolization (TACE) is a minimally invasive locoregional therapy widely used for treating intermediate-stage HCC. It involves the intra-arterial delivery of chemotherapeutic agents followed by embolization to induce tumor ischemia and necrosis. TACE is considered the standard treatment for unresectable HCC when surgical options are not feasible. However, its efficacy remains limited in advanced HCC, necessitating combination strategies with systemic therapies.
Immune checkpoint inhibitors, such as programmed cell death 1 (PD-1) inhibitors, programmed cell death 1 ligand 1 (PD-L1) inhibitors, and cytotoxic T-lymphocyte-associated antigen 4 inhibitors, have revolutionized cancer therapy and have become the standard treatment for advanced HCC in recent years.9,10 Sintilimab and tislelizumab are both PD-1 inhibitors that have demonstrated efficacy in HCC treatment in clinical trials. While ICIs activate the immune system to target tumor cells, they can also disrupt the body’s normal immune response, leading to immune-related adverse events (irAEs).11 As the use of immunotherapy continues to rise, clinicians are increasingly faced with the challenge of managing uncommon but serious irAEs, with immune checkpoint inhibitor-induced pancreatitis (ICIPI) being one of the rarer manifestations in clinical practice. Although treatment guidelines suggest discontinuing immunotherapy in the event of severe irAEs, the decision is not straightforward, as stopping therapy can potentially compromise the therapeutic benefit. The dilemma of whether to discontinue treatment or continue with adjustments remains a subject of ongoing clinical debate.
The pathogenesis of pancreatitis involves pancreatic duct obstruction, lysosomal dysfunction, inflammatory responses, and bile acid toxicity, with clinical features including upper abdominal pain radiating to the back, vomiting, persistent abdominal distension, and fever. The pathophysiology of ICIPI remains unclear but may be related to excessive T-cell activation attacking pancreatic cells.12
We describe a patient who developed ICIPI after multiple cycles of sintilimab, leading to acute pancreatitis and a temporary discontinuation of treatment. Despite the resolution of pancreatitis, immunotherapy was resumed after careful consideration, with a change to Tislelizumab. This case provides clinical evidence supporting the resumption of immunotherapy under close monitoring following the resolution of irAEs, thereby contributing to the clinical understanding of immune rechallenge, and provides valuable insight into the current clinical management of patients undergoing immune rechallenge and the management of ICI-related immune adverse events.
Case Presentation
A 28-year-old male with a 10-year history of chronic hepatitis B virus (HBV) infection, maintained on entecavir (Baraclude®) (0.5 mg/day), was diagnosed with a liver mass during routine surveillance at baseline (Day 0). The patient presented with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 and Child-Pugh class A liver function. Diagnostic workup revealed elevated alpha-fetoprotein (AFP) levels of 1129 ng/mL and protein induced by vitamin K absence-II (PIVKA-II) levels of 26771mAU/mL, with well-controlled HBV (HBV DNA <100 IU/mL). CT imaging showed a large right hepatic mass. The patient was diagnosed with hepatocellular carcinoma (HCC), classified as Barcelona Clinic Liver Cancer (BCLC) stage B. Surgical resection was initially contraindicated due to an elevated indocyanine green retention rate at 15 minutes (ICG R15) of 19.1% and an insufficient future liver remnant volume (remnant-to-standard liver volume ratio: 41.7%). The patient subsequently underwent conventional transarterial chemoembolization (c-TACE) followed by combination therapy with bevacizumab biosimilar (BYVASDA®) (95mg every 3 weeks) and sintilimab (TYVYT®) (200mg every 3 weeks). No other significant medical history.
Following the fourth cycle of sintilimab (approximately 12 weeks after treatment initiation, cumulative dose of 800 mg), the patient developed acute epigastric pain. The pain was continuous and severe (NRS pain score 7/10), radiating to the left shoulder and back, with significant exacerbation after food intake. The patient denied nausea, vomiting, or fever. Laboratory studies showed a marked elevation of serum amylase (480 U/L) and lipase (425 U/L), with mild elevation of liver enzymes (AST 85 U/L, ALT 63 U/L). Serum triglyceride and calcium levels were within normal limits.
The patient had no history of biliary diseases on previous physical examinations. Based on the characteristic abdominal pain and elevated serum amylase/lipase according to the Revised Atlanta Classification, combined with the strong temporal association with sintilimab administration, the diagnosis of immune checkpoint inhibitor-induced pancreatitis (ICIPI) was established. This diagnosis was confirmed by a multidisciplinary team (MDT) discussion, following the CTCAE 5.0 grade 3 criteria for drug-induced pancreatitis.
Upon diagnosis, the patient was promptly admitted to the Department of Hepatobiliary Surgery for comprehensive management. Sintilimab was discontinued, and treatment was initiated according to the acute pancreatitis protocol. The management strategy included complete bowel rest, intensive fluid resuscitation with a balanced crystalloid solution (initial rate 150 mL/h, adjusted based on hemodynamic parameters and urine output), and octreotide acetate (0.6 mg daily via continuous intravenous infusion for eight days). We closely monitored the patient’s vital signs, abdominal symptoms, and daily laboratory parameters. With this regimen, the patient’s clinical condition steadily improved. Serum amylase decreased to 125 U/L by Day 5 of hospitalization and normalized (62 U/L) by Day 8. Oral intake was gradually resumed on Day 4, progressing from clear liquids to a low-fat diet by Day 6. The patient was discharged on June 3, 2022, with complete resolution of symptoms. A follow-up endoscopic ultrasound approximately 2 weeks after discharge confirmed complete resolution of pancreatic inflammation.
Following the resolution of pancreatitis, it was crucial to resume immunotherapy due to the ongoing need for treatment of the patient’s HCC. Despite the temporary interruption caused by the immune-related adverse event, the patient had achieved partial response (PR) under the RECIST criteria by immune therapy, as evidenced by a favorable outcome after five months of c-TACE combined with targeted therapy. This remarkable tumor response supported the decision to continue immunotherapy. Approximately 3 weeks after resolution of pancreatitis, given the patient’s previous response to the PD-1 inhibitor, it was decided to adjust the immunotherapy to the PD-1 inhibitor tislelizumab (TEVIMBRA®) (200 mg/3 weeks) while continuing bevacizumab biosimilar (95 mg/3 weeks) therapy.
During the first three cycles of immunotherapy resumption, the patient’s serum amylase levels were regularly monitored and found to be within normal limits, suggesting that pancreatitis did not recur. After completing 19 cycles of combination therapy with Tislelizumab and bevacizumab biosimilar (BYVASDA®), the patient continued on Tislelizumab as monotherapy, despite the lack of proof of evidence of efficacy.
The laboratory test parameters changes are shown in Figures 1 and 2 presents the serial changes in CT images observed during the patient’s treatment regimen. The patient has remained alive since the resumption of immunotherapy, with an overall survival (OS) of 36 months. No new lesions or metastases were observed on CT imaging, and the HCC, as assessed by CT under the RECIST criteria, has continued to show partial response.
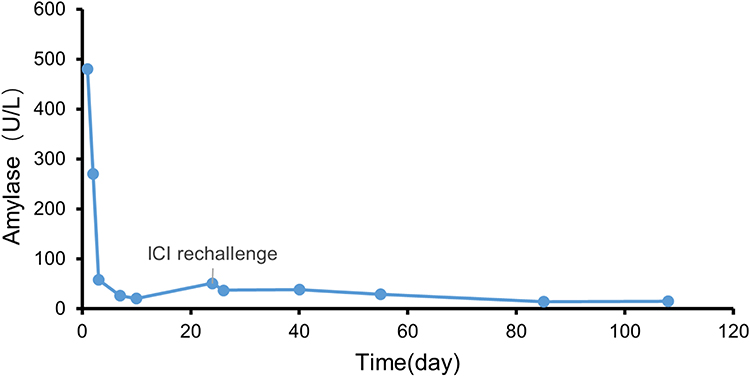 |
Figure 1 Timeline of laboratory parameters during treatment. The X-axis represents days from treatment initiation, with key clinical events marked. The patient demonstrated a favorable response to pancreatitis management during hospitalization, with no recurrence observed following immunotherapy rechallenge. An inset panel shows the detailed changes during the acute pancreatitis phase. |
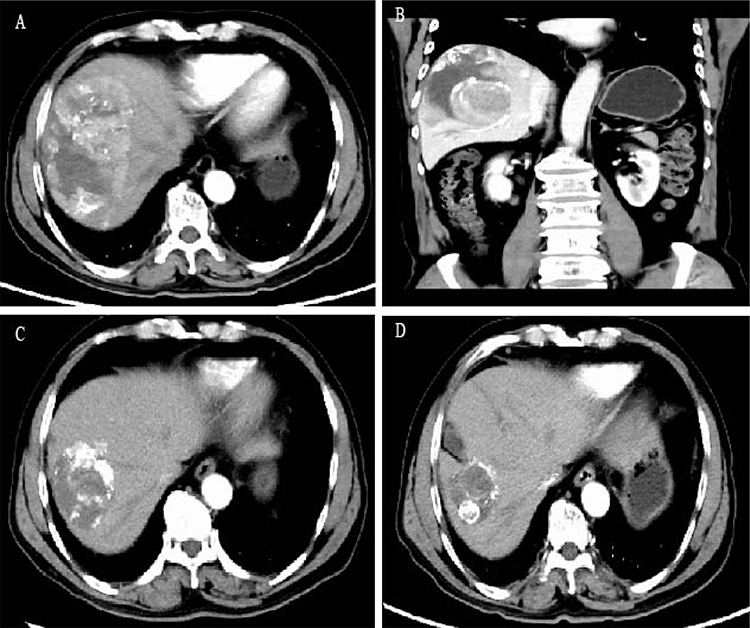 |
Figure 2 Serial CT images of HCC at matched anatomical levels. (A) Initial diagnosis of HCC showing the primary lesion. (B) Same anatomical level as (A), showing initial tumor characteristics. (C) CT imaging during presentation with abdominal pain and elevated lipase, demonstrating diffuse pancreatic enlargement with peripancreatic inflammatory changes consistent with acute pancreatitis, with stable hepatic lesion. (D) Same anatomical level, twenty-four months after tislelizumab immunotherapy rechallenge, demonstrating sustained partial response. |
Discussion
In China, hepatocellular carcinoma (HCC) is predominantly diagnosed at advanced stages, precluding surgical intervention. Current consensus guidelines advocate for integrated therapeutic protocols combining locoregional and systemic modalities. The concurrent application of TACE with targeted therapy and ICI has been increasingly recognized by multidisciplinary tumor boards as a strategy to potentiate therapeutic response and improve survival endpoints.13 TACE is a minimally invasive locoregional therapy widely used for treating intermediate-stage HCC. It involves the intra-arterial delivery of chemotherapeutic agents followed by embolization to induce tumor ischemia and necrosis. TACE is considered the standard treatment for unresectable HCC. However, its efficacy remains limited in advanced HCC, necessitating combination strategies with systemic therapies such as ICI and targeted agents. ICIs are a class of immunotherapies that enhance the body’s antitumor response by blocking inhibitory pathways in T cells, thereby restoring their ability to recognize and attack cancer cells. TACE standalone use may leave residual cancer cells, potentially causing recurrence. Targeted therapies, such as bevacizumab biosimilar, inhibit tumor angiogenesis and proliferation, addressing pathways that TACE alone might not affect.
The patient, possessing a strong educational background, actively engaged in the decision-making process. Given the urgency of disease progression, a thorough multidisciplinary evaluation determined that TACE combined with targeted and immunotherapy provided an optimal balance of efficacy and safety. This treatment strategy adhered to evidence-based guidelines while respecting the patient’s informed choice. We implemented a combination therapeutic approach in accordance with Chinese guidelines for unresectable HCC. Concurrent with TACE treatment, systemic therapy was initiated utilizing sintilimab plus bevacizumab biosimilar. The Phase 2–3 ORIENT-32 study has demonstrated that the combination of PD-1 inhibitor sintilimab with VEGF antibody bevacizumab biosimilar significantly improved overall survival and progression-free survival in Chinese patients with advanced HCC.14 Accumulating clinical evidence suggests that the triple combination of TACE with a PD-1 inhibitor plus VEGF antibody demonstrates positive and definitive efficacy with manageable adverse events.15,16
Prior to the onset of immune-related adverse events, the patient exhibited a highly favorable response to treatment, demonstrating significant tumor regression under the RECIST criteria. Following the initiation of c-TACE in combination with sintilimab (200 mg/3 weeks) and bevacizumab biosimilar (95 mg/3 weeks), the patient’s AFP levels markedly declined from an initial 1129 ng/mL, indicating effective tumor control. Radiological assessments showed progressive tumor shrinkage on contrast-enhanced CT, consistent with a partial response. The patient maintained stable liver function (Child-Pugh class A) and an Eastern Cooperative Oncology Group (ECOG) performance status of 0. This comprehensive evidence confirmed the initial success of the multimodal treatment strategy prior to the development of ICIPI. Following the fourth cycle of immunotherapy, the patient developed pancreatitis. The pancreatitis (CTCAE 5.0 grade 3) in the patient was considered to be attributable to ICI treatment, based on the following factors: The AE occurred after the use of sintilimab, indicating a temporal association; there have been previous reports of pancreatitis with ICIs, which are recognized as known drug-related side effects. The bevacizumab biosimilar is not associated with reported pancreatitis.17,18 Therefore, bevacizumab biosimilar (BYVASDA®)-related causes were ruled out. Additionally, the patient had no other medications, such as NSAIDs or PPIs, that could explain the condition. After discontinuation of ICI therapy and initiation of supportive treatment, the patient’s abdominal pain improved immediately without any further deterioration, meeting the criterion of dechallenge in AE assessment. After the diagnosis of pancreatitis, we managed the patient according to mild pancreatitis treatment protocols. With supportive care, the patient’s pancreatitis-related symptoms resolved and laboratory parameters improved.
At this stage, our primary concern shifted to whether to resume ICI therapy following the onset of irAEs, particularly in patients who had demonstrated a significant antitumor response. The occurrence of irAEs suggests a robust immune activation, potentially enhancing the therapeutic efficacy of ICIs for the patient.19,20 To our knowledge, no studies have definitively established the clinical benefits of re-challenging ICIs in patients with advanced HCC. Although current clinical guidelines recommend the immediate discontinuation of ICIs upon the occurrence of grade 3 or higher irAEs, these recommendations are largely based on expert consensus rather than robust evidence. Furthermore, multiple studies have suggested that immunotherapy re-challenge may be a viable strategy in selected patients, while others propose that the incidence of irAEs may not significantly differ before and after switching to an alternative ICI.21,22
Regarding the safety of ICI rechallenge specifically after ICIPI, the available literature remains limited. The rationale for switching between different ICIs within the same class (eg, from sintilimab to tislelizumab, both PD-1 inhibitors) is based on the hypothesis that individual ICIs may have different immunogenicity profiles, binding characteristics, and associated adverse event patterns. Studies on same-class ICI switches after other types of irAEs, such as immune-related hepatitis and colitis, have demonstrated that rechallenge with an alternative ICI can be successful in selected patients with close monitoring. However, it should be noted that recurrence of the same irAE or development of new irAEs remains a risk, emphasizing the importance of careful patient selection and vigilant monitoring.
Following thorough communication with the patient and once the irAE had improved to grade 1, a comprehensive evaluation was conducted, including serial serum amylase measurements and radiological assessments confirming stable amylase levels over a 14-day period and complete resolution of pancreatic inflammation on CT imaging. After multidisciplinary team consultation involving clinical pharmacology and gastroenterology specialists, ICI re-challenge was approved with tislelizumab, which has demonstrated a superior response rate and a more favorable safety profile compared to sorafenib in clinical trials.23 The patient subsequently completed seven additional cycles of immunotherapy with continued monitoring of pancreatic markers, achieving successful treatment completion without recurrence of pancreatic complications. The patient has completed ICI therapy with closely monitored, with no evidence of radiographic tumor progression or recurrence of irAEs observed to date.
ICIPI is a rare gastrointestinal adverse event triggered by ICIs. A meta-analysis has shown that the incidence rates of all-grade pancreatitis, amylase elevation, and lipase elevation related to ICIs are 0.68%, 2.53%, and 2.80%, respectively.24 The exact mechanism of ICIPI remains unclear. ICIs may induce non-specific inflammatory responses, leading to excessive T cell activation and mediating immune responses.25 Some studies suggest that during the occurrence of IrAEs, there is a significant increase in CD8+ and CD4+ T cells, which subsequently decrease with steroid treatment. Known risk factors for ICI-PI include combination therapy with ICIs, melanoma, age under 65 years, and a history of pancreatitis.26
Pancreatitis typically presents as severe upper abdominal pain, nausea, vomiting, fever, jaundice, and dyspepsia, along with elevated pancreatic enzyme levels. Approximately 15% of ICIPI experience long-term adverse events, such as recurrent acute pancreatitis, chronic pancreatitis, and pancreatic insufficiency. Therefore, early control and treatment of pancreatitis are crucial, not only to restore the patient’s cancer treatment but also to reduce potential long-term complications.27 Currently, the treatment for ICIPI is primarily supportive, aimed at alleviating the pancreatic burden and relieving symptoms. Common treatments include fasting, fluid resuscitation, and pain management. Existing studies suggest that although ICIPI closely resembles autoimmune pancreatitis (AIP), steroids do not show significant advantages in the treatment of ICI-related pancreatitis.28 A search of PubMed has not found any reported fatalities due to ICIPI, and most patients recover to grade 1 within 50 days after treatment.29,30
Immune-related adverse events, while dangerous, are not entirely unpredictable In recent years, researchers have gradually uncovered several biomarkers and clinical features associated with IrAE occurrence, among which hematological parameters have received wide attention as potential predictors. For instance, absolute lymphocyte count (ALC ≥2.6 k/ul), absolute monocyte count (AMC >0.29 k/uL), and absolute eosinophil count (AEC >125k/μL) have been shown to be associated with the risk of developing irAEs at treatment initiation.31,32 In this case, the patient’s blood test approximately 5 weeks prior to the onset of pancreatitis showed an elevated ALC (4.8 k/ul) without a clear trigger, but the clinicians did not take note of it. Gut microbiota may also play a role in ICI-related pancreatitis. Patients with ICIPI show an increase in the abundance of Firmicutes and Bacteroidetes, which is associated with more severe clinical manifestations.33
This case report has several unique aspects: it is the first to describe an HCC patient who developed PD-1 inhibitor-associated ICI-P and was successfully treated with a different PD-1 inhibitor. Through this treatment approach, the ICI therapy not only maintained efficacy uncompromised by irAEs but also achieved prolonged progression-free survival with no subsequent irAEs recurrence observed throughout the clinical monitoring period. This successful experience suggests that, in carefully selected patients, even in the presence of severe gastrointestinal immune-related adverse events, switching to a different type of PD-1 inhibitor for re-challenge may be a safe and feasible therapeutic option. This is particularly significant for patients who lack other treatment options and are responsive to immunotherapy. However, as this is a single case report and the patient in this case had a generally good status (ECOG PS score 0, Child-Pugh grade A), no definitive conclusions can be drawn, and more safety data are needed to further validate this strategy.
Based on the treatment experience in this case, we recommend that during PD-1 inhibitor therapy, clinicians should maintain a high level of vigilance for pancreatitis-related symptoms and monitor indicators that may suggest the onset of irAEs. Patients should also receive education on potential adverse reactions to facilitate early identification and intervention fo any immune-related adverse events. Additionally, a multidisciplinary approach should be established to promptly assess and manage any potential complications.
Conclusion
Although PD-1 inhibitors demonstrate significant antitumor efficacy in HCC, the management of irAEs remains a clinical challenge. This study, through a case of severe immune-related pancreatitis, demonstrates that selective PD-1 inhibitor rechallenge following thorough clinical evaluation and symptom resolution can effectively suppress tumor progression and significantly prolong overall survival, highlighting dual clinical benefits in disease control and survival improvement. Implementation of this strategy requires precise patient stratification, attention to baseline immune-related biomarkers (eg, ALC/AMC) that may predict irAE risk, and multidisciplinary collaborative decision-making for individualized interventions. While the role of dynamic monitoring of these biomarkers during treatment warrants further investigation, our case provides observational evidence supporting its potential utility. Particularly for immunotherapy-responsive patients experiencing severe irAEs, ICI therapy reintroduction may sustain long-term survival benefits while ensuring safety. Future research should prioritize larger clinical cohorts to validate the generalizability of this approach and establish standardized rechallenge protocols, thereby advancing evidence-based optimization of immunotherapy in HCC management.
Abbreviations
HCC, Hepatocellular carcinoma; irAEs, Immune-related adverse events; ICIPI, Immune checkpoint inhibitor-induced pancreatitis; ICIs, Immune checkpoint inhibitors; PD-1, Programmed cell death 1; PD-L1, Programmed cell death 1 ligand 1; TACE, Transarterial chemoembolization; HBV, Hepatitis B virus; AFP, Alpha-fetoprotein; PIVKA-II, Protein induced by vitamin K absence-II; CT, Computed tomography; MRCP, Magnetic resonance cholangiopancreatography; BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Cooperative Oncology Group; MDT, Multidisciplinary team; CTCAE, Common Terminology Criteria for Adverse Events; PR, Partial response; OS, Overall survival; RECIST, Response Evaluation Criteria in Solid Tumors; ALC, Absolute lymphocyte count; AMC, Absolute monocyte count; AEC, Absolute eosinophil count; VEGF, Vascular endothelial growth factor; AIP, Autoimmune pancreatitis; NRS, Numeric Rating Scale; ICG R15, Indocyanine green retention rate at 15 minutes.
Ethical Approval
Ethical approval was not needed, the confidentiality of participants’ information was kept secret and was used only for this publication without patients’ identification.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Acknowledgment
We thank the patient and her family for their cooperation and consent. We acknowledge the nursing staff and allied health professionals who contributed to the care of this patient.
Funding
This work was funded by Guilin Science Research and Technology Development Project (No. 20230135-1-3).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–8. doi:10.3322/caac.21834
2. Chen J, Jia J, Zhuang H, et al. Assessing pricing and affordability of HBV treatment in Asia-Pacific region: a barrier to elimination. Hepatol Int. 2025;19:349–357. doi:10.1007/s12072-024-10744-9
3. Sarin SK, Kumar M, Eslam M, et al. Liver diseases in the Asia-Pacific region: a lancet gastroenterology & hepatology commission. Lancet Gastroenterol Hepatol. 2020;5(2):167–228. doi:10.1016/S2468-1253(19)30342-5
4. Xu Y, Xia C, Li H, et al. Survey of hepatitis B virus infection for liver cancer screening in China: a population-based, cross-sectional study. Chin Med J. 2024;137(12):1414–1420. doi:10.1097/CM9.0000000000003171
5. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
6. Bureau of Medical Administration, National Health Commission of the People’s Republic of China. [Standardization for diagnosis and treatment of hepatocellular carcinoma (2022 edition)]. Zhonghua Gan Zang Bing Za Zhi. 2022;30(4):367–388. doi:10.3760/cma.j.cn501113-20220413-00193
7. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
8. Damaskos C, Garmpis N, Dimitroulis D, et al. Targeted therapies for hepatocellular carcinoma treatment: a new era ahead-a systematic review. Int J Mol Sci. 2022;23(22):14117. doi:10.3390/ijms232214117
9. Postow MA, Callahan MK, Wolchok JD. Immune checkpoint blockade in cancer therapy. J Clin Oncol. 2015;33(17):1974–1982. doi:10.1200/JCO.2014.59.4358
10. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1(8):EVIDoa2100070. doi:10.1056/EVIDoa2100070
11. Barron CC, Stefanova I, Cha Y, et al. Chronic immune-related adverse events in patients with cancer receiving immune checkpoint inhibitors: a systematic review. J Immunother Cancer. 2023;11(8):e006500. doi:10.1136/jitc-2022-006500
12. Kramer S, van Hee K, Blokzijl H, van der Heide F, Visschedijk MC. Immune checkpoint inhibitor-related pancreatitis: a case series, review of the literature and an expert opinion. J Immunother. 2023;46(7):271–275. doi:10.1097/CJI.0000000000000472
13. National Clinical Research Center for Infectious Diseases; Society of Hepatology, Beijing Medical Association; Translational Medicine Branch, China Association of Gerontology and Geriatrics. [Expert consensus on precise diagnosis and management of primary hepatocellular carcinoma in advanced stage (2023 version)]. Zhonghua Gan Zang Bing Za Zhi. 2023;31(9):910–920. doi:10.3760/cma.j.cn501113-20230717-00006
14. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2–3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
15. Wang L, Lin L, Zhou W. Efficacy and safety of transarterial chemoembolization combined with lenvatinib and PD-1 inhibitor in the treatment of advanced hepatocellular carcinoma: a meta-analysis. Pharmacol Ther. 2024;257:108634. doi:10.1016/j.pharmthera.2024.108634
16. Cai M, Huang W, Huang J, et al. Transarterial chemoembolization combined with lenvatinib plus PD-1 inhibitor for advanced hepatocellular carcinoma: a retrospective cohort study. Front Immunol. 2022;13:848387. doi:10.3389/fimmu.2022.848387
17. Shord SS, Bressler LR, Tierney LA, Cuellar S, George A. Understanding and managing the possible adverse effects associated with bevacizumab. Am J Health Syst Pharm. 2009;66(11). doi:10.2146/ajhp080455
18. Taugourdeau-Raymond S, Rouby F, Default A, Jean-Pastor MJ. Bevacizumab-induced serious side-effects: a review of the French pharmacovigilance database. Eur J Clin Pharmacol. 2012;68(7):1103–1107. doi:10.1007/s00228-012-1232-7
19. Lai K-C, Chen Y-H, Hung Y-P, Chiang N-J, Chen M-H, Chen S-C. Efficacy and safety of durvalumab rechallenge in advanced hepatocellular carcinoma patients refractory to prior anti-PD-1 therapy. Hepatol Int. 2024;18(6):1804–1814. doi:10.1007/s12072-024-10728-9
20. Ramos-Casals M, Brahmer JR, Callahan MK, et al. Immune-related adverse events of checkpoint inhibitors. Nat Rev Dis Primers. 2020;6(1):38. doi:10.1038/s41572-020-0160-6
21. Dolladille C, Ederhy S, Sassier M, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer. JAMA Oncol. 2020;6(6):865–871. doi:10.1001/jamaoncol.2020.0726
22. Pollack MH, Betof A, Dearden H, et al. Safety of resuming anti-PD-1 in patients with immune-related adverse events (irAEs) during combined anti-CTLA-4 and anti-PD1 in metastatic melanoma. Ann Oncol. 2018;29(1):250–255. doi:10.1093/annonc/mdx642
23. Qin S, Kudo M, Meyer T, et al. Tislelizumab vs sorafenib as first-line treatment for unresectable hepatocellular carcinoma: a phase 3 randomized clinical trial. JAMA Oncol. 2023;9(12):1651–1659. doi:10.1001/jamaoncol.2023.4003
24. Zhao Z, Zhang W, Pang L, Zeng L, Liu S, Liu J. Pancreatic adverse events of immune checkpoint inhibitors therapy for solid cancer patients: a systematic review and meta-analysis. Front Immunol. 2023;14:1166299. doi:10.3389/fimmu.2023.1166299
25. Ramos-Casals M, Lambotte O, Kostine M, et al. THU0628 immune-related adverse events induced by cancer immunotherapies. Big data analysis of 13,051 cases (Immunocancer International Registry). Ann Rheumatic Dis. 2019;78:607–608. doi:10.1136/annrheumdis-2019-eular.2707
26. Reck M, Wehler T, Orlandi F, et al. Safety and patient-reported outcomes of atezolizumab plus chemotherapy with or without bevacizumab versus bevacizumab plus chemotherapy in non-small-cell lung cancer. J Clin Oncol. 2020;38(22):2530–2542. doi:10.1200/JCO.19.03158
27. George J, Bajaj D, Sankaramangalam K, et al. Incidence of pancreatitis with the use of immune checkpoint inhibitors (ICI) in advanced cancers: a systematic review and meta-analysis. Pancreatology. 2019;19(4):587–594. doi:10.1016/j.pan.2019.04.015
28. Abu-Sbeih H, Tang T, Lu Y, et al. Clinical characteristics and outcomes of immune checkpoint inhibitor-induced pancreatic injury. J Immunother Cancer. 2019;7(1):31. doi:10.1186/s40425-019-0502-7
29. Brahmer JR, Abu-Sbeih H, Ascierto PA, et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2021;9(6):e002435. doi:10.1136/jitc-2021-002435
30. Fujiwara Y, Horita N, Namkoong H, Galsky MD. The effect of adding immune checkpoint inhibitors on the risk of pneumonitis for solid tumours: a meta-analysis of Phase III randomised controlled trials. Eur J Cancer. 2021;150:168–178. doi:10.1016/j.ejca.2021.03.012
31. Michailidou D, Khaki AR, Morelli MP, Diamantopoulos L, Singh N, Grivas P. Association of blood biomarkers and autoimmunity with immune related adverse events in patients with cancer treated with immune checkpoint inhibitors. Sci Rep. 2021;11(1):9029. doi:10.1038/s41598-021-88307-3
32. Nakamura Y, Tanaka R, Maruyama H, et al. Correlation between blood cell count and outcome of melanoma patients treated with anti-PD-1 antibodies. Jpn J Clin Oncol. 2019;49(5):431–437. doi:10.1093/jjco/hyy201
33. Tan B, Chen M-J, Guo Q, et al. Clinical-radiological characteristics and intestinal microbiota in patients with pancreatic immune-related adverse events. Thorac Cancer. 2021;12(12):1814–1823. doi:10.1111/1759-7714.13990
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.