Back to Journals » Journal of Asthma and Allergy » Volume 13
Successful Deferasirox Rechallenge and Treating Through Reaction in a Patient with Challenge-Proven Mild Immediate Reaction: A Case Report
Authors Sompornrattanaphan M ![]() , Krikeerati T, Wongsa C, Thongngarm T
, Krikeerati T, Wongsa C, Thongngarm T ![]() , Yampayon K
, Yampayon K ![]()
Received 11 July 2020
Accepted for publication 2 October 2020
Published 30 October 2020 Volume 2020:13 Pages 557—561
DOI https://doi.org/10.2147/JAA.S271742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Mongkhon Sompornrattanaphan,1 Thanachit Krikeerati,1,2 Chamard Wongsa,1 Torpong Thongngarm,1 Kittika Yampayon3
1Division of Allergy and Clinical Immunology, Department of Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 3Adverse Drug Reaction (ADR) Unit, Pharmacy Department, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Kittika Yampayon
Adverse Drug Reaction (ADR) Unit, Pharmacy Department, Siriraj Hospital, Mahidol University, 2 Wanglang Road, Bangkok Noi, Bangkok 10700, Thailand
Tel +66 81 488 6887
Fax +66 2 419 7376
Email [email protected]
Abstract: This is the first report of successful deferasirox administration, using graded challenge and treating through, in a patient with mild immediate hypersensitivity reaction. Beginning with drug graded challenges could indicate the eliciting dose and reaction severity which are important for the management plan in the next step. This approach could be a safe shortcut in a stable patient with a mild reaction and a long avoidance period.
Keywords: deferasirox, drug allergy, rechallenge, desensitization, hypersensitivity, iron overload, iron chelating agents, thalassemia, premedication
Introduction
There are three iron-chelating agents for patients with transfusion-dependent thalassemia, including deferoxamine (DFO), deferiprone (DFP), and deferasirox (DFX). There is a significant variation in the recommendations for iron chelation therapy.1–3 DFX dose of 30–40 mg/kg/day could reduce serum ferritin level, liver iron concentration (LIC), and achieved negative iron balance in transfusion-dependent thalassemia. DFX is well tolerated in most patients. Longer-term extension studies have confirmed the efficacy and safety of DFX.4
The most common adverse events consist of gastrointestinal disturbances, skin rash, nonprogressive increases in serum creatinine, and elevations in liver enzyme levels. DFX is known to cause a maculopapular eruption in up to 10% of the patients. There were reports regarding successful DFX desensitization for delayed-type drug hypersensitivity reactions (DHR), including maculopapular eruption and erythema multiforme.5,6 Those protocols took several days to achieve the target dose. There have been no reports on a challenge-proven immediate hypersensitivity reaction. Therefore, we report a case of challenge-proven immediate hypersensitivity reaction and successful DFX graded challenge with treating through the reaction.
Case Presentation
A 50-year-old woman with β-thalassemia/Hb E and secondary hemochromatosis due to blood transfusion since the age of eight. She was initially prescribed oral DFP for the treatment of iron overload, but she developed DFP-induced agranulocytosis, leading to drug discontinuation. After 2 months, her white blood cell count returned to normal range. DFX was prescribed as an alternative for iron chelation in May 2006. Three hours after taking 1000 mg of DFX, she had a generalized pruritic rash and swollen eyelids. The hematologist discontinued the drug and prescribed H1-antihistamine with prednisolone, 20 mg/day, for 3 days. The rash was completely resolved without hyperpigmentation within 1 day. Subcutaneous injection of DFO was then used as the single iron-chelating agent from the years 2006 to 2019. However, the serum ferritin level was still excessive, ranging from 1300 to 2000 ng/mL. Magnetic resonance imaging revealed T2* heart = 48.6 ms which is within the normal range (normal Cardiac T2* >25 ms; In case of iron overload, mild = 20–25 ms, moderate = 10–20 ms, and severe ≤10 ms). She had liver iron concentration (LIC) of 35.1 mg of elemental iron/g dw, which indicated severe liver iron overload (LIC ≤ 3 = normal, 3–7 = mild, 7–15 = moderate, and >15 = severe iron overload). She had persistent transaminitis (ALT, ranging 80–90 μg/L and AST, ranging 100–150 μg/L), and a mean liver stiffness value of 7.7 kilopascals indicated by fibroscan. Left and right ventricular ejection fractions were 69.4% and 59.4%, respectively. No valvular heart diseases were demonstrated.
The patient was referred to allergy consultation due to the need for DFX use in April 2020. As DFX in solution form was not available, we initially performed DFX skin prick test (SPT) by dissolving 500-mg tablet of DFX in 25 mL of 0.9% saline at room temperature for 20 minutes, giving a 20 mg/mL concentration. The SPT result was negative.
The overall timeline is summarized in Figure 1. We performed DFX graded challenge to confirm the diagnosis and indicated the eliciting dose under close monitoring (Table 1). DFX challenge started with 1 mg, followed by 10 mg, 100 mg, 250 mg, 250 mg with escalation at every 1-hour interval. Generalized pruritic papular rash (Ring and Messmer grade 1) occurred at the cumulative dose of 611 mg (Figure 2). We treated the reaction with intravenous chlorpheniramine and started bilastine 20 mg twice daily for premedication purposes. After the rash was resolved, we restarted the graded challenge on the next day, starting with 250 mg, followed by 500 mg, and 250 mg. A cumulative dose of 1000 mg/day of DFX was achieved without a breakthrough reaction. Because the elimination half-life of DFX was 8–16 hours,7 the patient then was advised to take the drug 500 mg twice daily to ensure DFX remained in the body at all times to cover the medication interval as well as to reduced plasma drug level fluctuations and gastrointestinal side effects.8,9 Bilastine was discontinued 1 week later.
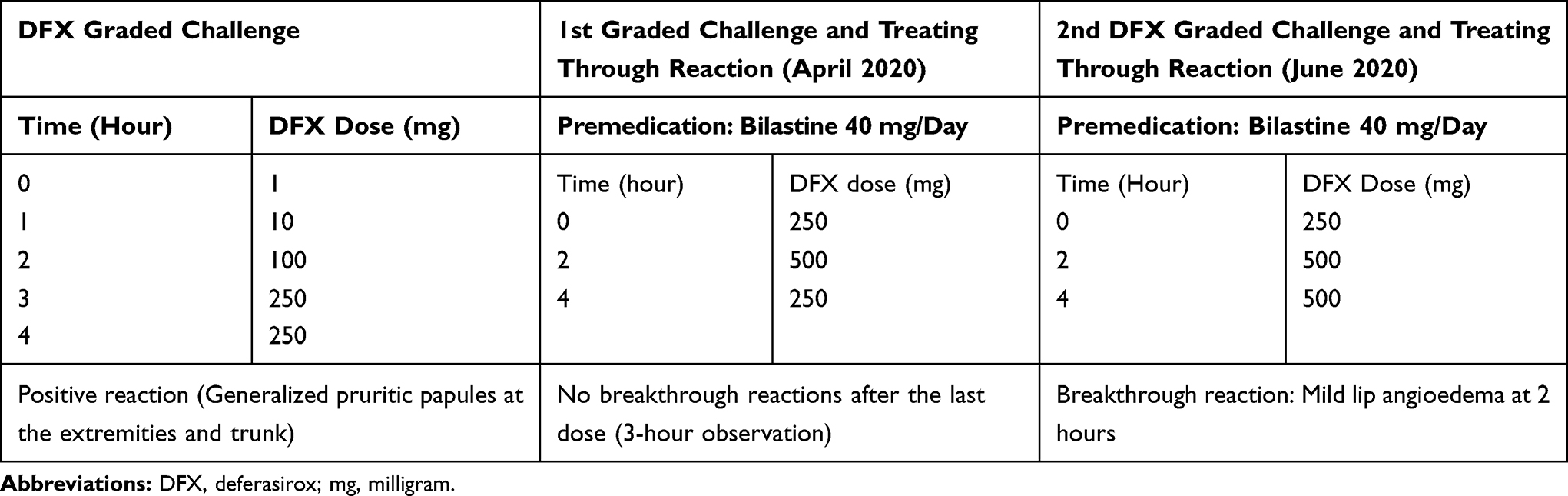 |
Table 1 DFX Graded Challenge and Treating Through Protocol in Our Case |
 |
Figure 1 The timeline of the case report. |
 |
Figure 2 Positive DFX challenge: a few discrete ill-defined erythematous macules on the right arm. |
Two months later, she was admitted to a local hospital due to acute gastroenteritis with acute hemolysis. The physician discontinued DFX during the investigation. Red cell transfusion was administered. She was discharged without taking DFX for 1 week. An allergist was consulted for repeating DFX desensitization. A hematologist requested increasing the dose of DFX to 1250 mg. We premedicated with bilastine 20 mg 1 day before desensitization and continued twice daily. DFX desensitization was performed, starting with 250 mg, followed by 500 mg, and 500 mg. She developed mild lip angioedema 45 minutes after the last dose (Figure 3), which spontaneously resolved the next day without increasing the dose of antihistamine. She then continued a combination of iron-chelating agents which included 1250 mg/day of DFX, and subcutaneous DFO 3000 mg/day, 4 times/week. She has finally achieved a desensitized state as she could discontinue antihistamine and continued DFX without any significant breakthrough reactions for the next 2 months. However, she developed a single episode of mild eyelid angioedema without visual disturbance after missing the DFX for 1 day. The reaction was resolved after taking oral bilastine 20 mg/day for 3 days. At a 3-month follow-up visit in September 2020, her ferritin level was decreased to 601 ng/mL. The liver enzymes were improved from baseline (ALT 44 μg/L and AST 56 μg/L). The serum creatinine was 0.64 mg/dL. No significant impairment of the patient’s hearing and vision during the 3-month follow-up. The patient has been continuing on DFX until now (September 2020).
 |
Figure 3 Lip angioedema during the second DFX graded challenge and treating through with H1-antihistamine. |
Discussion
This is the first report of challenge-proven DFX-induced immediate hypersensitivity reaction. There is a tendency for the drug-specific IgE level to decline over time and the observation of tolerance developing in patients with IgE-mediated reactions.10,11 Therefore, we initially performed a graded challenge to confirm the diagnosis as some patients might develop natural tolerance after a long avoidance period. This approach could indicate the eliciting dose and the appropriate interval for designing a graded challenge/desensitization protocol. A general published desensitization protocol begins with a 1/10,000 dose, which would sometimes take a longer time to reach the target dose.
We observed that the majority of patients who underwent chemotherapy desensitization usually elicited breakthrough reactions in the terminal step at high doses.12 This implied that the eliciting dose threshold of each patient was varied. We believed that graded challenge/desensitization could be individually tailor-made and might not necessarily start at a very low dose in all cases, especially those with mild reaction and long avoidance period since the last reaction. Our patient had a high eliciting dose, >50% of therapeutic dose, demonstrated by the first graded challenge and the reaction was non-anaphylaxis. She had no risk of severe reactions, such as decompensated cardiopulmonary diseases or taking antihypertensive medications. Treating through the reaction with H1-antihistamine during graded challenges could be an alternative option in such a case. As she had recurrent reactions from DFX reexposure after short discontinuation, this was compatible with the traditional definition of desensitization, the temporary induction of tolerance.
Conclusion
In conclusion, we report the first case of challenge-proven immediate hypersensitivity reaction to DFX and performed graded challenge with treating through the reactions using H1-antihistamine. The patient finally developed tolerance to the drug as the patient could discontinue H1-antihistamine. We provide a new perspective that “not all individuals with immediate reaction require desensitization starting at a very low dose with multiple steps”. However, the decision should be based on the patient’s status, history of index reaction, the eliciting dose, and the patient’s informed consent.
Ethical Approval
The institutional approval was not applicable (case report).
Consent for Publication
Written informed consent for publication was obtained from the patient. The patient was informed that de-identified data would be used in scientific research and publications.
Acknowledgment
We acknowledge the contributions of Ms Orathai Theankeaw and Ms Aree Jameekornrak Taweechue for the research assistance. We also thank Dr Anthony Tan for editing the English language in the manuscript.
Authorship
All authors made a significant contribution to the work reported, whether that is in the conception, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare no personal, professional, or other conflicts of interest.
References
1. Musallam KM, Angastiniotis M, Eleftheriou A, Porter JB. Cross-talk between available guidelines for the management of patients with beta-thalassemia major. Acta Haematol. 2013;130(2):64–73. doi:10.1159/000345734
2. Huang V, Luini C, El-Ali A, Kessabi S. Iron chelation therapy: a review of the literature on the issues and importance of adherence to treatment in iron overload. Blood. 2015;126(23):4748. doi:10.1182/blood.V126.23.4748.4748
3. Kontoghiorghe CN, Kontoghiorghes GJ. Efficacy and safety of iron-chelation therapy with deferoxamine, deferiprone, and deferasirox for the treatment of iron-loaded patients with non-transfusion-dependent thalassemia syndromes. Drug Des Devel Ther. 2016;10:465–481. doi:10.2147/DDDT.S79458
4. Chaudhary P, Pullarkat V. Deferasirox: appraisal of safety and efficacy in long-term therapy. J Blood Med. 2013;4:101–110.
5. Bruner KE, White KM. Deferasirox desensitization. J Allergy Clin Immunol Pract. 2016;4(1):171–172. doi:10.1016/j.jaip.2015.09.007
6. Davies GI, Davies D, Charles S, Barnes SL, Bowden D. Successful desensitization to deferasirox in a paediatric patient with beta-thalassaemia major. Pediatr Allergy Immunol. 2017;28(2):199–201. doi:10.1111/pai.12677
7. Tanaka C. Clinical pharmacology of deferasirox. Clin Pharmacokinet. 2014;53(8):679–694. doi:10.1007/s40262-014-0151-4
8. Lu MY, Wang N, Wu WH, et al. Simultaneous determination of plasma deferasirox and deferasirox-iron complex using an HPLC-UV system and pharmacokinetics of deferasirox in patients with beta-thalassemia major: once-daily versus twice-daily administration. Clin Ther. 2015;37(8):1751–1760. doi:10.1016/j.clinthera.2015.05.506
9. Chang HH, Lu MY, Liao YM, et al. Improved efficacy and tolerability of oral deferasirox by twice-daily dosing for patients with transfusion-dependent beta-thalassemia. Pediatr Blood Cancer. 2011;56(3):420–424. doi:10.1002/pbc.22826
10. Isik P, Yarali N, Bay A, Ozmen S, Tunc B. Type-I hypersensitivity reaction secondary to deferasirox intake. Int J Hematol Oncol. 2010;20:42–44.
11. Blanca M, Torres MJ, Garcia JJ, et al. Natural evolution of skin test sensitivity in patients allergic to beta-lactam antibiotics. J Allergy Clin Immunol. 1999;103(5):918–924. doi:10.1016/S0091-6749(99)70439-2
12. Kang Y, Kwon OY, Jung H, et al. Breakthrough reactions during rapid drug desensitization: clinical outcome and risk factors. Ann Allergy Asthma Immunol. 2019;123(1):48–56 e41. doi:10.1016/j.anai.2019.05.007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.