Back to Journals » Open Access Emergency Medicine » Volume 14
Success Rate on Endotracheal Intubation with Prone versus Kneeling Position in Mannequin Model with Limitation of Neck Movement: A Cross Over Study
Authors Tangkulpanich P ![]() , Jenpanitpong C
, Jenpanitpong C ![]() , Patchkrua J
, Patchkrua J ![]() , Silarak C, Srinaowech N
, Silarak C, Srinaowech N ![]() , Thiamdao N
, Thiamdao N ![]() , Yuksen C
, Yuksen C ![]()
Received 3 February 2022
Accepted for publication 6 April 2022
Published 19 April 2022 Volume 2022:14 Pages 177—182
DOI https://doi.org/10.2147/OAEM.S360169
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Panvilai Tangkulpanich, Chetsadakon Jenpanitpong, Jirayoot Patchkrua, Chappawit Silarak, Nattagit Srinaowech, Natthaphong Thiamdao, Chaiyaporn Yuksen
Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Chetsadakon Jenpanitpong, Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Thung Phayathai, Ratchathewi, Bangkok, 10400, Thailand, Tel +66 8 3183 1373, Fax +66 2201 2404, Email [email protected]
Purpose: Endotracheal intubation is a lifesaving procedure for airway management but is more complex when performed in patients lying on the ground and requiring cervical spine immobilization. This study aims to compare the optimal technique between prone and kneeling positions in increasing intubation success rate on these prehospital trauma patients.
Patients and Methods: This study was an experimental study on a mannequin. Paramedic students performed intubation on the supine mannequin, which was applied with a rigid cervical collar and manual in-line stabilization. The participants were randomly assigned to intubate in a prone or kneeling position as the first method, then perform another method seven days later. Study outcomes include the percentage of successful intubation, time to perform intubation successfully, and Cormack and Lehane’s classification of laryngeal view.
Results: Thirty-nine participants were enrolled in this study; 22 were male (56.41%). The mean age, weight, and height were 23.15 ± 4.75 years, 67.38 ± 17.39 kg, and 167.36 ± 8.70 cm., respectively. The percentage of successful intubation in prone (37 [94.90%]) was higher than kneeling position (35 [89.74%]), but there was no statistically significant (p-value = 0.675). Time to intubation successfully, the number of attempts, and Cormack & Lehane’s laryngeal view classification were not significantly different between prone and kneeling groups (p-value = 0.808, 0.814, and 0.948, respectively).
Conclusion: Intubation with the prone or kneeling position on a mannequin, lying on the ground with cervical spine immobilization, has no statistical difference. Both intubation approaches appear to be effective in successful and rapid intubation, proper glottic visualization and low attempts.
Keywords: endotracheal intubation, airway management, prone position, kneeling position, advanced trauma life support care
Introduction
Injuries are the leading cause of global mortality and disability, whether intended or unintended.1 Classically, the distribution of death among injured patients was classified into three periods: immediate, early, and late death based on the causes and time interval since the injury to death.2 Immediate death occurs seconds to minutes after the injury due to severe central nervous system injury that is a nonsurvivable injury, whereas early death occurs minutes to several hours due to threatened airway and inability to control hemorrhage. Late death occurs several days or weeks later, resulting from trauma complications such as multiple organ dysfunctions.3 Nowadays, the trend of death in traumatic injury patients has changed to bimodal distribution resulting from the development of the trauma care system. However, immediate or early death numbers were not different from the classic trimodal distribution.4 Failure of airway maintenance and impaired pulmonary ventilation increase the likelihood of death, especially in the severely injured patient. Thus, airway management is prioritized for trauma care.5 There are several techniques to maintain a patient’s airway, initially by airway maneuvers, simple adjunctive devices, supraglottic devices (SGD), or endotracheal intubation (ETI).6
ETI is the gold standard for airway management in emergencies situations which aims to supplement oxygenation, support ventilation, and prevent airway aspiration. Direct laryngoscopy (DL) using Macintosh laryngoscope is a conventional method for performing ETI. In some conditions, DL could be challenging from both anatomic and physiologic difficulties, which leads to a higher chance of failed intubation and worsening outcome.7,8
Firstly, an optimal laryngoscopic view can be achieved by positioning the patients in a sniffing position that allows the oral, pharyngeal, and laryngeal axis to align with the vocal cords. Because of sniffing position causes neck flexion with upper cervical extension, it is contraindicated in traumatic injury patients.9,10 Thus, the provider’s position, which enhances optimal laryngoscopic view, is an essential factor that may increase the rate of successful intubation.
Secondly, in traumatic injury patients, in-line stabilization (ILS) should be performed manually or mechanically while initiating airway intervention. This effort helps limit the cervical range of motion and reduce the risk of spinal cord injury, which may result in deterioration of neurological outcome.11 However, ILS increases intubation failure rate at 30 seconds and worsens glottic visualization during direct laryngoscopy.12
Manual ILS is a common practice instead of applying a semi-rigid cervical collar or fully immobilization by using a long backboard and head immobilizers. Manual ILS alone allows wider mouth opening that improves the success rate of intubation.13,14 However, although manual ILS seems more suitable than other immobilization techniques, greater forces were applied to get the best laryngeal view. The greater force applied during direct laryngoscopy results in more significant pressure transmitted to the cervical spine.15 Moreover, emergency medical personnel usually encounter trauma patients lying down on the ground where the incidence occurred. To intubate a patient lying in the supine position is more difficult, especially in a patient who requires spinal immobilization. This factor causes inappropriate laryngoscopic view, which leads to failed intubation and severe complications.16,17
This study compares the optimal technique between prone and kneeling positions in increasing intubation success rate when manual ILS is performed on a mannequin lying supine on the ground.
Materials and Methods
Study Design
This study was a mannequin-based experimental with a cross-over design. The study was conducted at the Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University in Thailand, between July and September 2018. The Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital approved the study to conduct an experimental study (Ethics code: MURA2018/98). The study obtained the participants’ written consent regarding human rights related to research involving the Helsinki Declaration subjects.
Eligible criteria of participants were the 3rd and 4th-year paramedic students who completely participated in the adult airway management course. The course was consisted of 1-hour didactic lecture and 2-hours hands-on workshop provided by emergency physicians. Participants who did not complete procedures according to an experimental protocol were excluded.
After enrollment, the study protocol was introduced to each participant by research assistants. Then, participants were assigned randomly to intubate in a prone or kneeling position as the first method, then perform another method seven days later to provide enough length for the washout period. Random allocation was done using a sequentially opaque sealed envelope (SNOSE) with block-of-four randomization to manipulate each experimental group to a 1:1 ratio.
Setting
Resusci Anne® Advanced SkillTrainer (Laerdal Medical Corporation, Stavanger, Norway) was placed supine on the floor in the simulation room. The mannequin was applied with a semi-rigid cervical collar and maintained manual in-line stabilization by one of the research assistants to limit the cervical range of motion. Participants performed intubation with either prone or kneeling position (Figure 1) by using conventional laryngoscope with Macintosh curved blade size three and 7.5-mm internal diameter endotracheal tube which tracheal stylet was inserted. The mannequin was placed in the same position through the study period, and the equipment was checked before performing each experimental procedure.
 |
Figure 1 Intubation methods. (A) Prone position. (B) Kneeling position. Note: The people in the figure provided informed consent for the images to be published. |
Data Gathering and Outcome Measures
Participants’ characteristics, including age, gender, weight and height, percentage of successful intubation, time to perform intubation successfully, numbers of attempts, and Cormack and Lehane's classification of laryngeal view18 graded by participants, were recorded using a data recording form. Successful intubation was defined when the tracheal tube was placed in the mannequin’s trachea coupled with a presence of chest raising when assisted ventilation was performed with a bag-valve-mask device. The time to perform intubation successfully is defined since the laryngoscope passes through the mannequin’s front teeth to successful intubation. Moreover, successful intubation will be considered if participants can perform intubation less than or equal two attempts.
Study Size Estimation
According to Adnet F et al19 which compared the ease and speed of intubation between kneeling and left lateral decubitus position, the study found that 87% of physicians completely visualized the glottis in the left lateral decubitus (LLD) position versus 33% of the kneeling (KN) position group.
Following commands for comparing two proportions with a power of 0.8, the significance level of 0.05, a 1:1 ratio of sample, and a two-sided test suggested a minimum study sample size of 19 for each study group. The sample size was calculated using STATA software version 14.0 (StataCorp, College Station, TX, USA).
Statistical Analysis
Statistical analyses were performed by STATA software version 14.0. Categorical variables are presented as numbers and percentages (%), whereas numerical variables are presented as mean ± standard deviation (SD) or median and interquartile range (IQR), as appropriate. Chi-square or Exact probability test was used to compare independent categorical variables. The Student’s t-test was used for the parametric variable to compare two independent numerical variables, while the Wilcoxon rank-sum test was used for non-parametric variables. All results were considered to be significant at the p-value <0.05.
Results
Forty paramedic students were enrolled in the study, and one was excluded due to incomplete experimental procedures. Data from 39 participants were analyzed. The majority was male (56.41%), while the mean age, weight, and height were 23.15 (± 4.75) years, 67.38 (± 17.39) kg, and 167.36 (± 8.70) cm., respectively.
The percentage of successful intubation was higher in the prone group (37 [94.90%]) than in the kneeling group (35 [89.74%]), but there was no statistically significant (p-value = 0.675). The median time to intubate successfully in both groups was 14 seconds (p-value = 0.808). At the same time, the procedure was almost completed by the first intubation attempt (84.62% in the prone group and 82.05 in the kneeling group, p-value = 0.814). Both prone and kneeling positions mainly provide the laryngoscopic view Grade I of Cormack & Lehane's classification, 53.85%, and 51.28%, respectively, with no statistically significant (p-value = 0.948) as shown in Table 1.
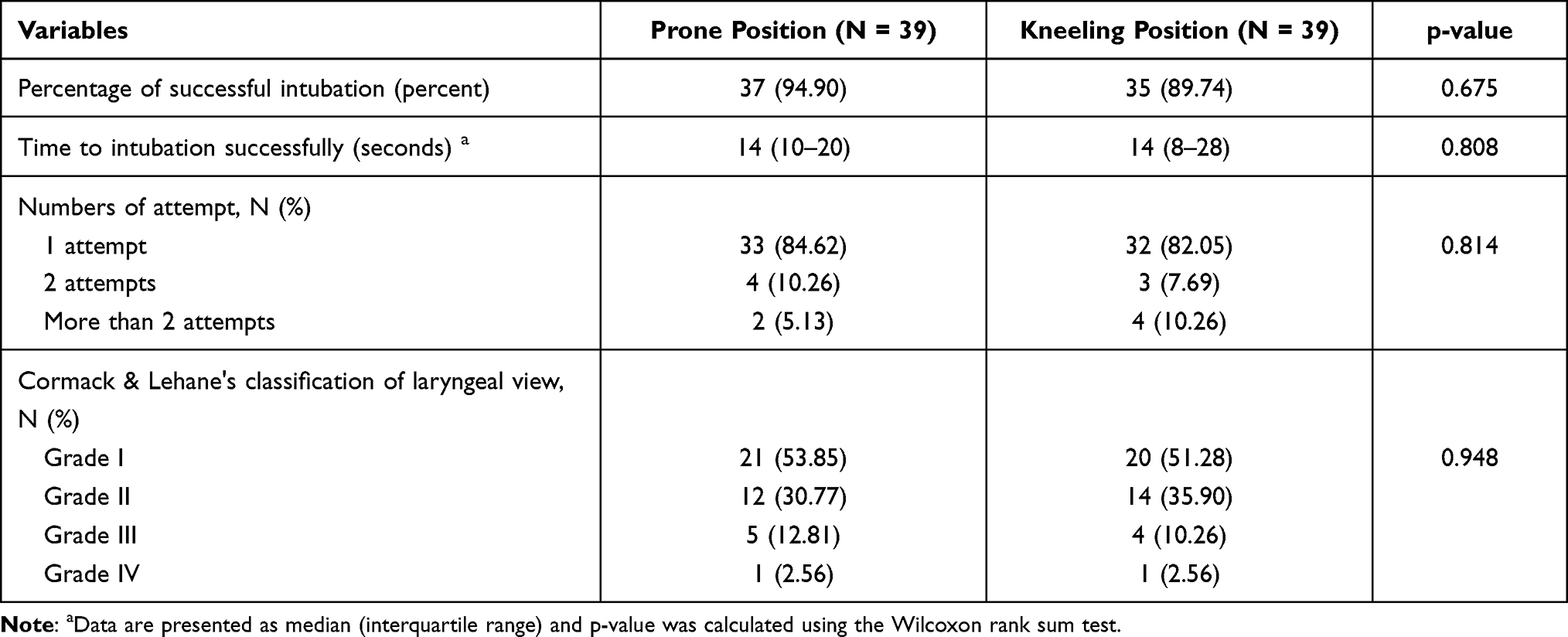 |
Table 1 Comparison of Intubation Characteristics Between Prone and Kneeling Position |
Discussion
In this experimental study which simulated trauma patients who required spinal immobilization and lying supine on the ground, the percentage of successful intubation was not significantly different between prone and kneeling positions. Both approaches appear to be very effective, with a more than 90% success rate in this setting. Additionally, the performance of successful intubation, ie, intubation time, number of attempts, and optimal laryngoscopic view (grade I of Cormack & Lehane's classification), were not significantly different between the two studies groups.
The influence of operator position on intubation performance found in our study is different from a previous study conducted by Adnet et al, which aimed to evaluate the influence of operator body position during emergency intubation of patients lying on the ground.19 The study’s results demonstrate that the incidence of laryngoscopic difficulty (defined as Cormack grade III or IV) was lower in the left lateral decubitus (LLD) group than in the kneeling (KN) group (11.1% vs 26.9%; p-value <0.001). The number of attempts required for successful intubation was lower in the LLD group than in the KN group (Median 1, IQR [1–1] vs Median 1, IQR [1–2], p-value <0.001).
As in LLD position which is lying on the ground position for the providers, the providers’ heads are close to the ground, which allows the providers’ visual axis to be aligned with the patient tracheal axis. Thus, the proper glottic visualization is associated with successful intubation, rapid time to intubate, and lower numbers of attempts.20,21
Although the prone position is not entirely different from the left lateral decubitus position, there are some differences between our study and the study conducted by Adnet F et al. Our study was conducted in a mannequin model, which simulated trauma patients who require spinal immobilization. In contrast, Adnet F et al conducted the study among non-traumatically ill patients who do not contraindicate to sniffing position. Moreover, our study participants are paramedic students who have less experience in performing intubation, whereas the other study participants are anesthetists or emergency physicians who have higher experience. These result in different findings between the two studies.
There were some limitations in this study. First, this was an experimental study on mannequins. Thus, the study results may not directly apply to the actual clinical situation. Second, the intubation was performed in an isolated simulation room which is different from the prehospital environment. Third, grading the laryngoscopic view by participants may be subjective and causes measurement bias. A previous study found that Cormack & Lehane's grading by paramedics exhibits poor intra- and interrater reliabilities. Therefore, the percentage of glottic opening (POGO) should be used in further study instead of a more reliable classification system.22 Fourth, participants in our study were paramedic students who have less experience in performing emergency intubation impacted the study results. Finally, this study was completed with small amounts of sample sizes. Thus it might be insufficient statistical power to find out any differences.
Conclusion
Intubation with the prone or kneeling position on a mannequin, lying on the ground with cervical spine immobilization, has no statistical difference. Both intubation approaches appear to be effective in successful and rapid intubation, proper glottic visualization, and low attempts.
Acknowledgment
We would like to thank Ms. Dangfun Promkhum, from National Institute for Emergency Medicine (NIEM), for editing the draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
2. Trunkey DD. Trauma. Accidental and intentional injuries account for more years of life lost in the U.S. than cancer and heart disease. Among the prescribed remedies are improved preventive efforts, speedier surgery and further research. Sci Am. 1983;249(2):28–35.
3. Meislin H, Criss EA, Judkins D, et al. Fatal trauma: the modal distribution of time to death is a function of patient demographics and regional resources. J Trauma. 1997;43(3):433–440.
4. Gunst M, Ghaemmaghami V, Gruszecki A, Urban J, Frankel H, Shafi S. Changing epidemiology of trauma deaths leads to a bimodal distribution. Proc. 2010;23(4):349–354.
5. Eastridge BJ, Mabry RL, Seguin P, et al. Death on the battlefield (2001-2011): implications for the future of combat casualty care. J Trauma Acute Care Surg. 2012;73(6 Suppl 5):S431–437.
6. Pitteloud JC, Goulesque B. Airway and Ventilation. In: McSwain N, Salomone J, editors. PHTLS: Prehospital Trauma Life Support.
7. Carney N, Totten AM, Cheney T, et al. Prehospital Airway Management: a Systematic Review. Prehosp Emerg Care. 2021;1:1–12.
8. Sanguanwit P, Yuksen C, Laowattana N. Direct Versus Video Laryngoscopy in Emergency Intubation: a Randomized Control Trial Study. Bull Emerg Trauma. 2021;9(3):118–124.
9. Akhtar M, Ali Z, Hassan N, et al. Comparing the Sniffing Position with Simple Head Extension for Glottis Visualization and Difficulty in Intubation during Direct Laryngoscopy. Anesth Essays Res. 2017;11(3):762–766.
10. Butler KH, Clyne B. Management of the difficult airway: alternative airway techniques and adjuncts. Emerg Med Clin North Am. 2003;21(2):259–289.
11. Lennarson PJ, Smith DW, Sawin PD, Todd MM, Sato Y, Traynelis VC. Cervical spinal motion during intubation: efficacy of stabilization maneuvers in the setting of complete segmental instability. J Neurosurg. 2001;94(2 Suppl):265–270.
12. Thiboutot F, Nicole PC, Trépanier CA, Turgeon AF, Lessard MR. Effect of manual in-line stabilization of the cervical spine in adults on the rate of difficult orotracheal intubation by direct laryngoscopy: a randomized controlled trial. Can J Anaesth. 2009;56(6):412–418.
13. Heath KJ. The effect of laryngoscopy of different cervical spine immobilisation techniques. Anaesthesia. 1994;49(10):843–845.
14. Tienpratarn W, Yuksen C, Aramvanitch K, et al. Success Rate of Endotracheal Intubation Using Inline Stabilization with and without Cervical Hard Collar; a Comparative Study. Arch Acad Emerg Med. 2020;8(1):e81.
15. Santoni BG, Hindman BJ, Puttlitz CM, et al. Manual in-line stabilization increases pressures applied by the laryngoscope blade during direct laryngoscopy and orotracheal intubation. Anesthesiology. 2009;110(1):24–31.
16. Gaither JB, Stolz U, Ennis J, Moiser J, Sakles JC. Association Between Difficult Airway Predictors and Failed Prehosptial Endotracheal Intubation. Air Med J. 2015;34(6):343–347.
17. Garza AG, Gratton MC, McElroy J, Lindholm D, Coontz D. Environmental factors encountered during out-of-hospital intubation attempts. Prehosp Emerg Care. 2008;12(3):286–289.
18. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984;39(11):1105–1111.
19. Adnet F, Cydulka RK, Lapandry C. Emergency tracheal intubation of patients lying supine on the ground: influence of operator body position. Can J Anaesth. 1998;45(3):266–269.
20. Tremblay MH, Williams S, Robitaille A, Drolet P. Poor visualization during direct laryngoscopy and high upper lip bite test score are predictors of difficult intubation with the GlideScope videolaryngoscope. Anesth Analg. 2008;106(5):1495–1500.
21. Adnet F, Lapostolle F, Borron SW, Hennequin B, Leclercq G, Fleury M. Optimization of glottic exposure during intubation of a patient lying supine on the ground. Am J Emerg Med. 1997;15(6):555–557.
22. O’Shea JK, Pinchalk ME, Wang HE. Reliability of paramedic ratings of laryngoscopic views during endotracheal intubation. Prehosp Emerg Care. 2005;9(2):167–171.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.