Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Subtype-Specific Response to Fractional-Mode Q-Switched Ruby Laser in Melasma: A Prospective Single-Blind Clinical Study Using Clinical and Noninvasive Imaging Assessments
Authors Wang Y, Li Z, Wen Z, Liu J, Li Z
Received 22 March 2026
Accepted for publication 28 May 2026
Published 4 June 2026 Volume 2026:19 611230
DOI https://doi.org/10.2147/CCID.S611230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Yulan Wang, Zongxiang Li, Zhichao Wen, Jia Liu, Zhenhang Li
Department of Dermatology, The Second Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, People’s Republic of China
Correspondence: Yulan Wang, Email [email protected]
Objective: Melasma is a chronic relapsing facial hyperpigmentation disorder with pigmentary and vascular heterogeneity. This study compared responses of pigmentary melasma (M), characterized predominantly by brown hyperpigmented macules or patches with non-dominant vascularity, and pigmentary–vascular melasma (M+V), characterized by pigmentation with persistent erythema or telangiectatic vascular features, to fractional-mode 694 nm Q-switched ruby laser.
Methods: In this prospective, single-center, single-blind clinical study with assessor-blinded outcome evaluation, 100 women with facial melasma were classified at baseline as M (n = 50) or M+V (n = 50) by clinical examination and dermoscopy. All received three laser sessions at 4-week intervals. Outcomes included MASI, VISIA brown spots, ultraviolet spots, red areas, dermoscopic vascular scores, responder status, patient-reported improvement, satisfaction, and adverse events.
Results: Ninety patients completed week 12 assessment (M, n = 42; M+V, n = 48). Week 12 MASI percentage reduction was 71.1% ± 13.5% in M versus 51.2% ± 12.3% in M+V (P < 0.001), and ≥ 50% MASI improvement occurred in 95.2% versus 56.3% of patients, respectively (P < 0.001). M showed larger reductions in VISIA brown and ultraviolet spots. Red-area scores decreased in both groups, but between-subtype longitudinal reduction was not significant. MASI improvement correlated with VISIA brown (r = 0.502) and ultraviolet spots (r = 0.390), but not red areas. In multivariable analysis, M subtype independently predicted greater week 12 MASI improvement. Treatment was generally well tolerated.
Conclusion: Fractional-mode 694 nm Q-switched ruby laser improved both subtypes, but pigmentary melasma showed a more favorable response. Baseline clinicodermoscopic subtype classification and multimodal assessment may support individualized laser treatment and response evaluation. Infographic on melasma study with assessments, treatment and key findings for 100 women.The infographic presents a study on 100 women with facial melasma, divided into two subtypes: M (pigmentary melasma, n=50) and M+V (pigmentary-vascular melasma, n=50). Treatment involved a fractional-mode 694 nm Q-switched ruby laser over 3 sessions every 4 weeks, with assessments at week 12. Assessments included Clinical: MASI, VISIA: brown spots, ultraviolet spots, red areas, Dermoscopy: vascular quantity/morphology and patient-reported improvement and satisfaction. Key findings: Week 12 MASI reduction was 71.1 percent ± 13.5 percent for M and 51.2 percent ± 12.3 percent for M+V. ≥ 50 percent MASI improvement was 95.2 percent for M and 56.3 percent for M+V. Greater reduction in VISIA brown and ultraviolet spots in M. Red areas decreased in both subtypes; between-subtype longitudinal difference not significant. M subtype independently predicted greater week 12 MASI improvement. Treatment was generally well tolerated in both subtypes.
Keywords: melasma, laser therapy, lasers, solid-state, dermoscopy, treatment outcome, prospective studies
Introduction
Melasma is a common acquired disorder of facial hyperpigmentation that is clinically characterized by symmetric brown to gray-brown macules and patches, most often involving the cheeks, forehead, upper lip, and chin.1,2 Although it is benign in a strictly medical sense, melasma is often persistent, relapse-prone, and cosmetically distressing, which makes it a frequent source of treatment dissatisfaction in daily dermatologic practice.3–5 Its psychosocial burden should not be underestimated. Earlier work established the Melasma Quality of Life scale as a disease-specific instrument for affected women, and later evidence confirmed that melasma can exert a substantial negative impact on emotional well-being, social life, and treatment-related expectations.6–8 In this sense, melasma remains a clinically important condition not only because of its prevalence, but also because of the difficulty of achieving stable and meaningful improvement.
One major reason for this therapeutic challenge is that melasma is no longer understood as a purely epidermal pigmentary disorder. In addition to ultraviolet exposure and hormonal influences, contemporary research has emphasized the role of basement membrane alteration, solar elastosis, dermal remodeling, fibroblast senescence, mast-cell activity, and vascular proliferation in the pathogenesis of melasma.1,3,9,10 This broader model helps explain why patients with apparently similar pigmentation may respond differently to the same treatment. In particular, the vascular component has attracted increasing attention, because lesions with greater erythematous or telangiectatic features may reflect a more complex dermal microenvironment that is less readily reversed by pigment-directed therapy alone.9,11,12 A phenotype-oriented approach may therefore be more informative than treating melasma as a single homogeneous condition.
Current management of melasma is usually multimodal and individualized. Strict photoprotection remains a fundamental component of treatment, because ultraviolet and visible-light exposure can aggravate pigmentation and contribute to recurrence. Commonly used medical therapies include topical depigmenting agents, such as hydroquinone-containing regimens, retinoids, azelaic acid, and other pigment-modulating agents, while tranexamic acid may be considered in selected patients. Chemical peels and laser- or light-based devices are generally used as adjunctive or procedural options, particularly in patients with incomplete response to topical therapy or those seeking more visible improvement. Nevertheless, treatment selection must consider disease chronicity, Fitzpatrick skin type, vascular or dermal involvement, recurrence risk, and the possibility of post-inflammatory hyperpigmentation.2,4,5,13 Laser and light-based therapies have attracted increasing interest in melasma, but outcomes remain variable and recurrence is common, particularly when procedural treatment is applied without adequate attention to subtype heterogeneity and maintenance therapy.2,4,5,14 Fractional-mode 694 nm Q-switched ruby laser was selected for the present protocol for several reasons. The 694 nm ruby wavelength has strong melanin absorption, making it biologically relevant for pigment-directed treatment, while fractional delivery creates a microbeam treatment pattern that may reduce confluent epidermal thermal injury compared with non-fractional exposure. Previous clinical studies have reported improvement of melasma severity using fractional Q-switched ruby laser under carefully selected parameters.15,16 In this study, the modality was therefore used as a reproducible pigment-directed procedural model to examine whether baseline clinicodermoscopic subtype, especially the presence of a vascular component, is associated with different trajectories of clinical and imaging response. This question is clinically relevant, because a pigment-predominant lesion and a pigmentary–vascular lesion may not be expected to show identical improvement after the same pigment-targeted laser protocol.
Another unresolved issue is how treatment response should be assessed. MASI remains the most widely used clinical severity index in melasma research, but it cannot fully capture the multidimensional biological changes that occur during treatment.17 Noninvasive imaging techniques may therefore provide important complementary information. VISIA allows objective quantification of pigment-related and vascular-related facial features, whereas dermoscopy offers direct visualization of pigment distribution and superficial vascular structures.12,18–21 These tools are especially relevant when the clinical goal is not simply to document lightening, but also to understand why some patients improve more than others and why residual disease may persist despite apparently favorable clinical change. A combined assessment strategy may therefore be particularly useful in studies seeking to identify subtype-specific treatment responses.
Against this background, the present study was designed to compare the response of pigmentary melasma and pigmentary–vascular melasma to fractional-mode 694 nm Q-switched ruby laser treatment in a prospective cohort. Using MASI together with VISIA and dermoscopic assessment, we sought to determine whether subtype influences clinical improvement, whether pigmentary and vascular imaging domains show different patterns of change, and whether multimodal assessment can provide a more informative picture of treatment response than clinical scoring alone. The central contribution of this study is therefore not only to evaluate the efficacy of a specific laser protocol, but also to clarify how baseline clinicodermoscopic subtype relates to subsequent therapeutic outcome.
Materials and Methods
Study Design and Setting
This study was designed as a prospective, single-center, single-blind, non-randomized clinical study. Consecutive patients with facial melasma who were scheduled to receive fractional-mode 694 nm Q-switched ruby laser treatment at a tertiary dermatology center in China were screened for eligibility between January 2024 and June 2025. All participants received the same laser protocol, and the comparison groups were defined by baseline clinicodermoscopic subtype rather than by random assignment to different interventions. Therefore, the study should be interpreted as a non-randomized interventional clinical study rather than as a randomized clinical trial.
The manuscript was reviewed against relevant CONSORT items for transparent reporting of interventional clinical studies. Items related to random sequence generation, allocation concealment, and randomized treatment allocation were not applicable because patients were not randomized to treatment arms. Relevant reporting items concerning eligibility criteria, participant flow, intervention details, outcome definitions, assessment schedule, adverse-event monitoring, and statistical analysis were checked and clarified where appropriate.
The study was considered single-blind because the investigators who performed clinical, VISIA, and dermoscopic outcome assessments were not involved in administering the laser treatment. All participants received the same laser modality and were classified at baseline into a pigmentary subtype group and a pigmentary–vascular subtype group before longitudinal outcome assessment. The treatment course consisted of three laser sessions performed at 4-week intervals. Clinical and imaging evaluations were carried out at four prespecified time points, namely baseline, 4 weeks after the first treatment, 4 weeks after the second treatment, and 4 weeks after the third treatment. The final visit therefore represented the primary endpoint assessment at week 12.
Participants
Female patients aged 18 to 55 years were eligible if they met all of the following criteria: a clinical diagnosis of facial melasma confirmed by two board-certified dermatologists; disease duration of at least 6 months; Fitzpatrick skin phototypes III or IV; bilateral facial involvement suitable for standardized photography and imaging; and willingness to refrain from other melasma-directed procedures or medications during the study period. Because hormonal fluctuation is a recognized contributor to melasma severity and treatment response, only non-pregnant and non-lactating women with stable menstrual or hormonal status during the study period were included. Patients were excluded if they had received any laser, intense pulsed light, radiofrequency, chemical peel, or microneedling treatment to the face within the previous 6 months; used topical hydroquinone, retinoids, azelaic acid, corticosteroids, or tranexamic acid on the face within 8 weeks before enrolment; used oral tranexamic acid or systemic photosensitizing medication within 3 months; had active dermatitis, rosacea flare, bacterial or viral infection, or open wounds on the face; had a history of hypertrophic scarring or keloid formation; had vitiligo, ochronosis, or another facial pigmentary disorder that could confound outcome evaluation; or had any uncontrolled endocrine or systemic disease considered by the investigators to interfere with study participation. Eligible participants were enrolled consecutively after written informed consent had been obtained. During the study period, participants were asked to maintain their usual daily skin care routine except for the restrictions specified in the treatment protocol.
Melasma Subtype Classification
Baseline subtype classification was established before the first laser session on the basis of clinical examination and dermoscopic vascular features only. VISIA parameters were not used for subtype assignment and were analyzed solely as longitudinal outcome measures. Dermoscopy is useful for estimating melanin depth, identifying mixed melasma, and detecting vascular structures that may carry therapeutic relevance.12,18 In addition, increased vascularity has been demonstrated histologically and instrumentally in melasma lesions, supporting the clinical importance of a vascular component.9 Studies of vascular-targeted adjunctive therapy have further suggested that visibly widened capillaries on dermoscopy may be associated with a distinct treatment response pattern.11 Patients were classified as having pigmentary melasma, hereafter referred to as the M subtype, when the lesions were predominantly characterized by symmetric brown to dark-brown macules or patches without a clinically dominant erythematous background and when dermoscopy showed absent, mild, or non-dominant vascular structures. Patients were classified as having pigmentary–vascular melasma, hereafter referred to as the M+V subtype, when the pigmentary lesions were accompanied by a persistent erythematous background or telangiectatic appearance on clinical examination and when dermoscopy showed clearly increased vascular structures considered to represent a relevant vascular component. Subtype classification was therefore based on the overall clinicodermoscopic predominance of pigmentary versus pigmentary–vascular features rather than on any VISIA-derived parameter or a single isolated dermoscopic sign. Subtype assignment was performed independently by two board-certified dermatologists who were unaware of the later outcome assessments. In cases of disagreement, a third senior dermatologist reviewed the clinical photographs and dermoscopic images, and the final subtype was assigned by consensus.
Treatment Protocol
All participants were treated with a 694 nm Q-switched ruby laser equipped with a fractional handpiece. The fractional delivery system generated a microbeam array covering a 7.1×7.1 mm field with 196 microspots of approximately 300 μ m diameter and a coverage density of 27.7%, which is consistent with previously published fractional Q-switched ruby laser systems used in melasma.15,16 The pulse duration was 40 ns. The prespecified laser intervention parameters are summarized in Table 1.
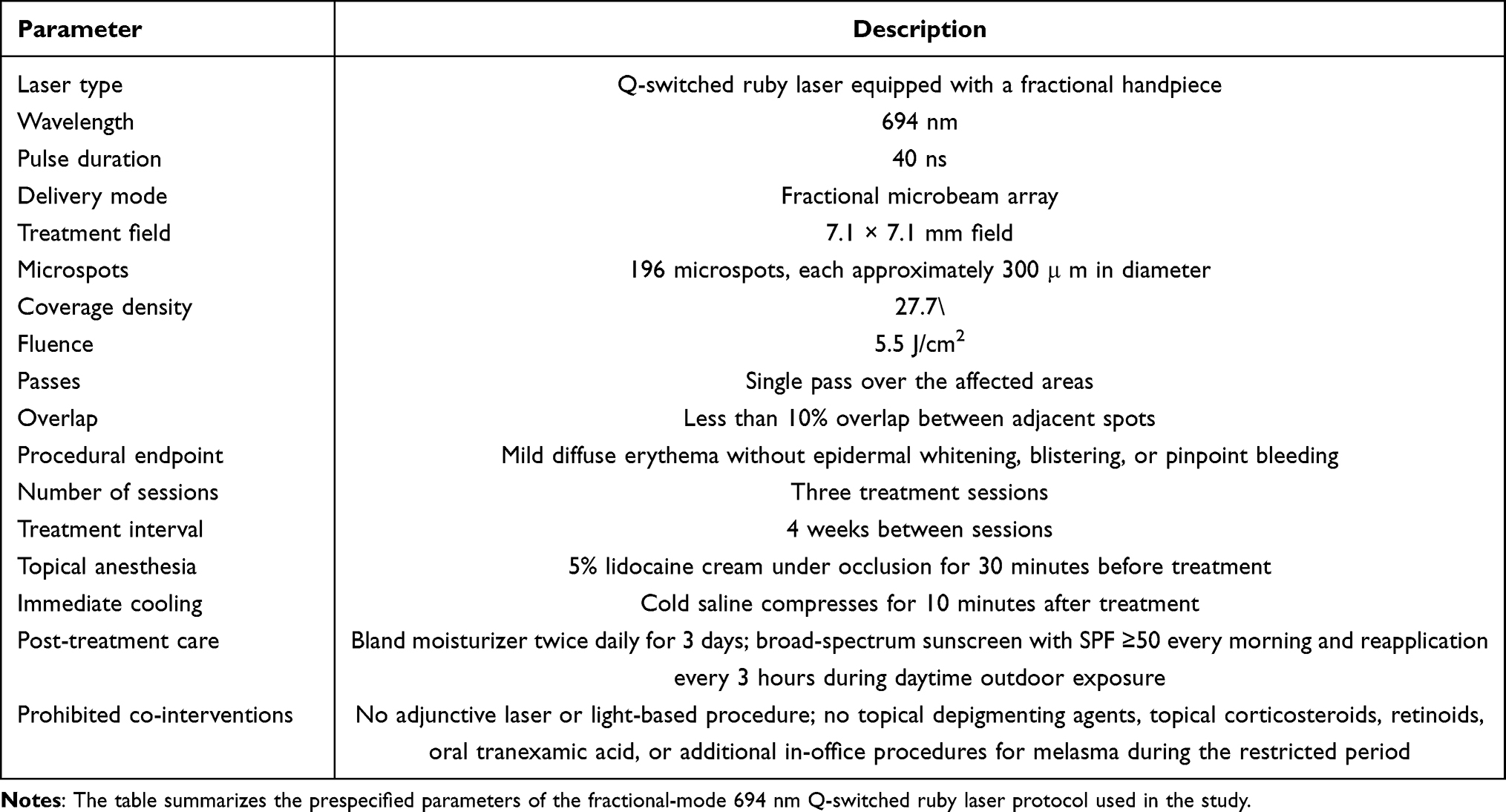 |
Table 1 Laser Intervention Parameters |
After facial cleansing, a topical anesthetic cream containing 5% lidocaine was applied under occlusion for 30 minutes and then removed completely. Protective eyewear was used for both the patient and the operator throughout the procedure. Each treatment was delivered at a fluence of 5.5 J/cm2 with a single pass over the affected areas and less than 10% overlap between adjacent spots. The procedural endpoint was mild diffuse erythema without epidermal whitening, blistering, or pinpoint bleeding. No adjunctive laser or light-based procedure was allowed during the study period. Immediately after treatment, cold saline compresses were applied for 10 minutes. All participants were instructed to use a bland moisturizer twice daily for 3 days and a broad-spectrum sunscreen with a sun protection factor of at least 50 every morning, with reapplication every 3 hours during daytime outdoor exposure. The use of topical depigmenting agents, topical corticosteroids, retinoids, oral tranexamic acid, and any additional in-office procedures for melasma was prohibited from 8 weeks before enrolment until completion of the final follow-up visit.
Clinical and Noninvasive Imaging Assessments
All assessments were performed at baseline and at each follow-up visit by trained investigators who were not involved in laser delivery. This separation between treatment administration and outcome evaluation constituted the single-blind, assessor-blinded design of the study. Standardized digital photographs were obtained with the same camera, lighting conditions, patient positioning, and room setting at all visits.
MASI Assessment
Melasma severity was evaluated using the original Melasma Area and Severity Index. This score was first described by Kimbrough-Green et al and later shown to have acceptable reliability and validity in melasma research.17,22 The forehead, right malar region, left malar region, and chin were assessed separately. For each region, the area of involvement A, darkness D, and homogeneity H were graded, and the total MASI was calculated as

Possible total scores ranged from 0 to 48, with higher scores indicating more severe disease.
Two dermatologists independently scored standardized clinical photographs at each visit. The mean of the two ratings was used for analysis. If the absolute difference between the two total MASI scores exceeded 10% of their mean, the images were reviewed jointly and a consensus score was assigned.
VISIA Assessment
Facial imaging was performed with the VISIA complexion analysis system under standardized conditions. Objective digital analysis of facial pigmentation and erythema has become increasingly useful in dermatologic research, and VISIA-derived brown and red lesion metrics have shown meaningful correlations with clinical and instrumental measures of pigmentary and vascular change.19–21 Before each imaging session, participants removed make-up and sunscreen, washed the face with a gentle cleanser, and rested for 20 minutes in a temperature-controlled room maintained at 21 ± 1 ° C and relative humidity of 45% to 55%. Frontal, left oblique, and right oblique images were captured at each visit. The preplanned VISIA variables were brown spots, ultraviolet spots, and red areas. For each domain, the primary analytic value was the mean absolute score across the three facial views. Percentile values were recorded but were treated as descriptive rather than inferential variables because they are partly reference-database dependent.
Dermoscopic Assessment
Polarized digital dermoscopy was performed at 10× magnification on both malar areas and on the forehead when clinically involved. Dermoscopy was used because it allows simultaneous visualization of pigmentary structures and superficial vascular changes and has been shown to be informative both for melasma classification and for treatment monitoring.11,12,18 At each visit, vascular quantity and vascular morphology were evaluated using prespecified semiquantitative scales. Vascular quantity was scored as 0 for no increase, 1 for slight increase, 2 for obvious increase, and 3 for marked increase. Vascular morphology was categorized as 0 for faint red patches or simple linear vessels, 1 for linear or arborizing vessels, and 2 for reticular vessels. After review of the frontal and bilateral images, one visit-level score for each domain was assigned according to the highest vascular finding observed in any involved facial area. Two dermatologists evaluated the dermoscopic images independently, and disagreements were resolved by consensus.
Outcomes
The primary endpoint was the change in total MASI from baseline to the third follow-up visit at week 12, defined as

A larger positive value therefore represented greater clinical improvement. The secondary endpoints were longitudinal changes in total MASI at the intermediate follow-up visits; longitudinal changes in the VISIA brown spots, ultraviolet spots, and red areas scores; longitudinal changes in dermoscopic vascular quantity and morphology scores; the change from baseline to week 12 in MASI, VISIA variables, and dermoscopic semiquantitative scores; the proportion of patients achieving at least 30% and at least 50% improvement in MASI at week 12; patient-reported improvement in pigmentation at week 12; patient satisfaction at week 12 measured on a 4-point Likert scale ranging from 1 for not satisfied to 4 for very satisfied; and the frequency of treatment-related adverse events. For all change analyses, change from baseline to week 12 was defined as baseline value minus week 12 value so that positive values indicated improvement.
Safety Assessment
Safety was evaluated after each treatment session and at every follow-up visit. The prespecified adverse events were transient erythema lasting more than 48 hours, edema, crusting, blistering, post-inflammatory hyperpigmentation, hypopigmentation, acneiform eruption, and rebound worsening of melasma. Each event was graded as mild if it resolved spontaneously without treatment interruption, moderate if topical treatment or an unscheduled visit was required, and severe if the event led to withdrawal from treatment or caused persistent sequelae beyond the final follow-up visit.
Ethical Considerations
The study protocol was reviewed and approved by the local institutional ethics committee before recruitment began. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.23 All participants provided written informed consent for study participation and separate written consent for the use of their clinical, dermoscopic, and VISIA images for research and publication purposes.
Sample Size Consideration and Statistical Analysis
Sample size was calculated on the basis of the primary endpoint, namely the between-subtype difference in ΔMASI at week 12. Based on pilot data from our center, we assumed a mean difference of 2.5 MASI points between the M and M+V groups with a common standard deviation of 4.2 points. At a two-sided significance level of 0.05 and 80% power, 45 participants were required per group. Allowing for an anticipated attrition rate of approximately 10%, the target sample size was set at 100 patients. All analyses were prespecified and performed using R version 4.3.2. Continuous variables are presented as mean ± standard deviation, and categorical variables as counts and percentages. Baseline between-group comparisons were performed using Welch’s t-test for continuous variables and Fisher’s exact test for categorical variables.
The primary longitudinal analysis used a linear mixed-effects model with total MASI as the dependent variable, visit and subtype as fixed effects, and a visit-by-subtype interaction term, with participant-specific random intercepts to account for repeated measurements. Estimated marginal means with standard errors were obtained from the fitted model, and post hoc contrasts were used to estimate between-group differences at each visit and within-group changes from baseline to week 12. The same modeling framework was applied to repeated VISIA outcomes, dermoscopic vascular quantity, and dermoscopic morphology treated as a repeated semiquantitative score. For presentation, change from baseline to week 12 was defined as baseline minus week 12 so that positive values indicated improvement. Change-score analyses, responder analyses, week 12 patient-reported improvement, week 12 satisfaction, and week 12 categorical dermoscopic comparisons were restricted to participants with both baseline and week 12 data available. Pearson correlation coefficients were used to examine associations between ΔMASI and changes in VISIA or dermoscopic measures. Multivariable linear regression was performed to identify independent predictors of week 12 MASI improvement, with ΔMASI as the dependent variable and subtype, age, disease duration, baseline MASI, Fitzpatrick skin type, previous topical treatment, previous device-based treatment, and photoprotection adherence entered as covariates. Treatment-emergent adverse events were summarized at the participant level across the study period. Week 12 categorical outcomes and adverse-event rates were compared using Fisher’s exact test. All tests were two-sided, and a p value below 0.05 was considered statistically significant.
Results
Patient Screening, Enrollment, Follow-Up, and Analysis Population
A total of 125 patients were assessed for eligibility, and 100 eligible patients were enrolled and received the first laser treatment. Based on baseline clinical and dermoscopic findings, 50 patients were classified as the M subtype and 50 as the M+V subtype. By week 12, 90 patients had complete baseline and final follow-up data and were included in the complete-case analyses, including 42 patients in the M group and 48 patients in the M+V group. The detailed participant flow is summarized in Figure 1.
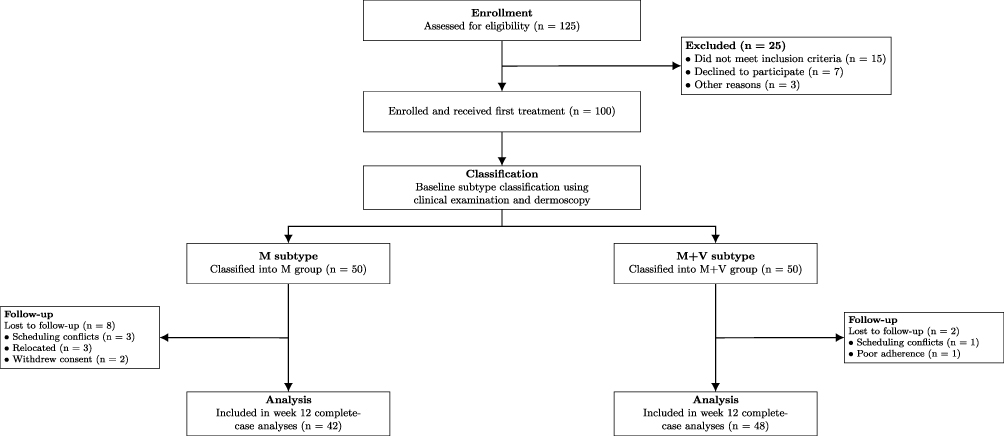 |
Figure 1 Flow diagram of patient screening, enrollment, baseline subtype classification, follow-up, and inclusion in the week 12 complete-case analyses. |
Baseline Characteristics
The baseline characteristics of the study population are summarized in Table 2. At baseline, 100 patients were included, with 50 classified as the M subtype and 50 as the M+V subtype. The two groups were comparable in age, disease duration, previous topical treatment, previous device-based treatment, and hormone-related history. However, the M+V subtype showed a more complex baseline phenotype. Fitzpatrick skin type IV was more common in the M+V group than in the M group (80.0% vs 46.0%, P < 0.001), and self-reported aggravation after sun exposure was also more frequent (88.0% vs 66.0%, P = 0.016). Baseline MASI was higher in the M+V subtype than in the M subtype (19.5 ± 3.2 vs 16.4 ± 3.8, P < 0.001). The M+V subtype also had higher VISIA brown spots, ultraviolet spots, and red-area scores, together with higher dermoscopic vascular quantity and morphology scores, indicating greater pigmentary and vascular burden at study entry.
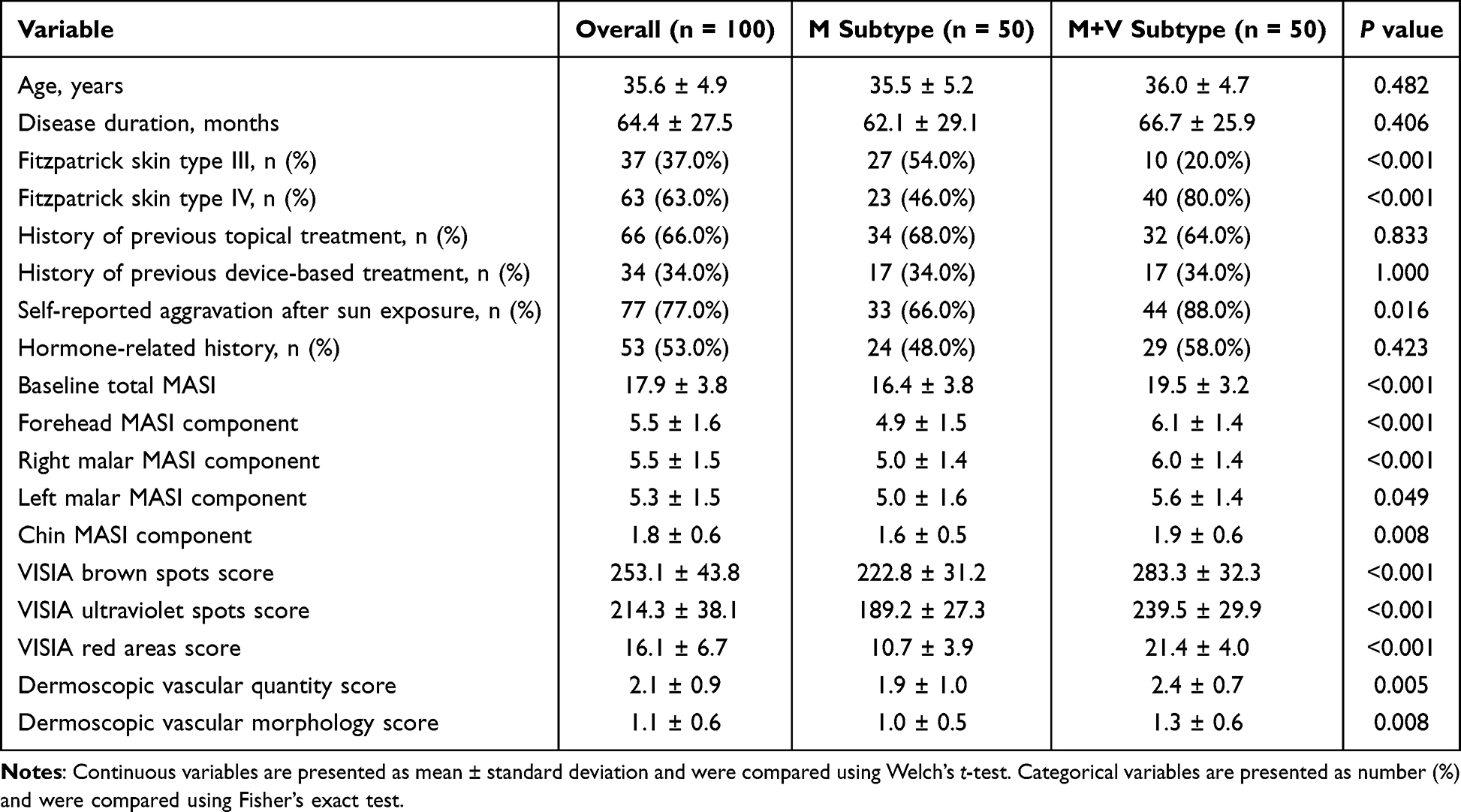 |
Table 2 Baseline Characteristics of the Study Population |
Primary Outcome: Changes in MASI
Total MASI declined progressively in both subtypes, but the magnitude and temporal pattern of improvement differed between groups (Table 3). The visit-by-subtype interaction was statistically significant (P < 0.001), indicating that longitudinal clinical response was modified by baseline subtype. At week 12, the model-estimated MASI was lower in the M subtype than in the M+V subtype (4.90 ± 0.48 vs 9.62 ± 0.46), with a significant adjusted between-group difference. Complete-case change analyses confirmed a more favorable response in the M subtype. The mean ΔMASI was 11.5 ± 2.8 in the M subtype and 10.0 ± 2.7 in the M+V subtype (P = 0.012). The percentage reduction in MASI was also greater in the M subtype than in the M+V subtype (71.1% ± 13.5% vs 51.2% ± 12.3%, P < 0.001). Although at least 30% improvement was achieved by most patients in both groups, at least 50% improvement was substantially more frequent in the M subtype than in the M+V subtype (95.2% vs 56.3%, P < 0.001).
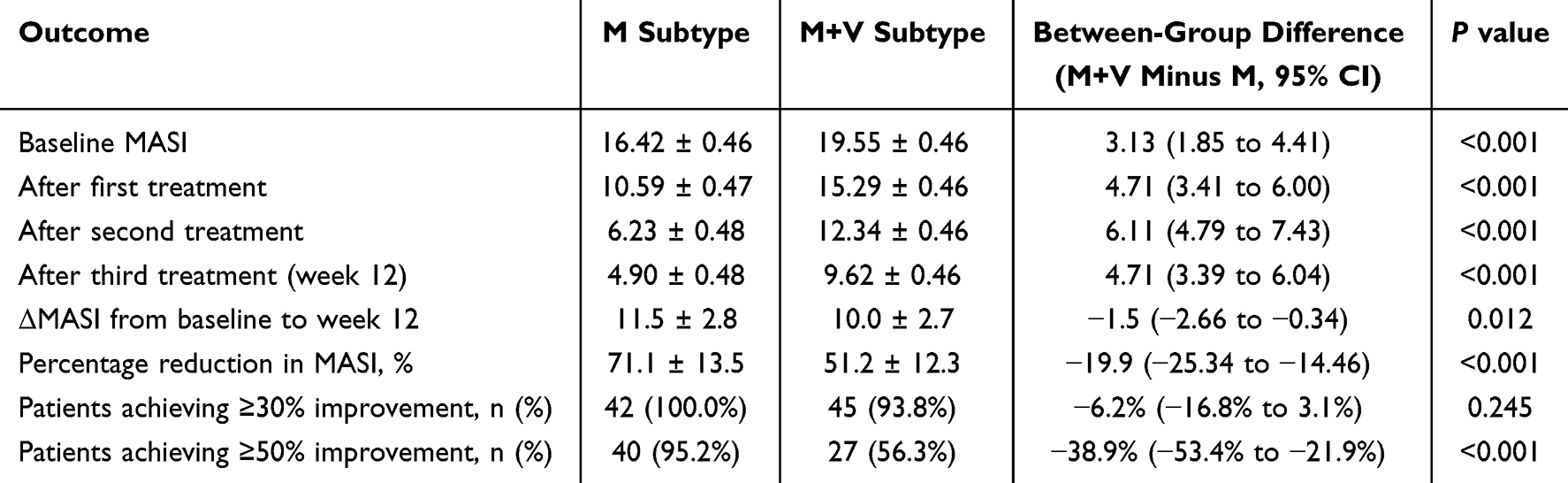 |
Table 3 Longitudinal Changes in MASI by Melasma Subtype |
VISIA Findings
Longitudinal VISIA findings are summarized in Table 4. Pigment-related VISIA domains improved in both subtypes, but reductions in brown spots and ultraviolet spots were greater in the M subtype. For brown spots, week 12 scores remained higher in the M+V subtype than in the M subtype (141.0 ± 4.2 vs 68.0 ± 4.3, P < 0.001), and the baseline-to-week 12 reduction was significantly greater in the M subtype. Ultraviolet spots showed a similar pattern, with lower week 12 scores and a greater reduction in the M subtype than in the M+V subtype. By contrast, red-area scores decreased in both groups but did not show a significant between-subtype difference in longitudinal reduction. Red-area scores remained higher in the M+V subtype at week 12, but the baseline-to-week 12 decrease was not significantly different between groups. Overall, the VISIA results suggest that subtype-specific differences were more evident in pigment-associated imaging domains than in the vascular red-area domain.
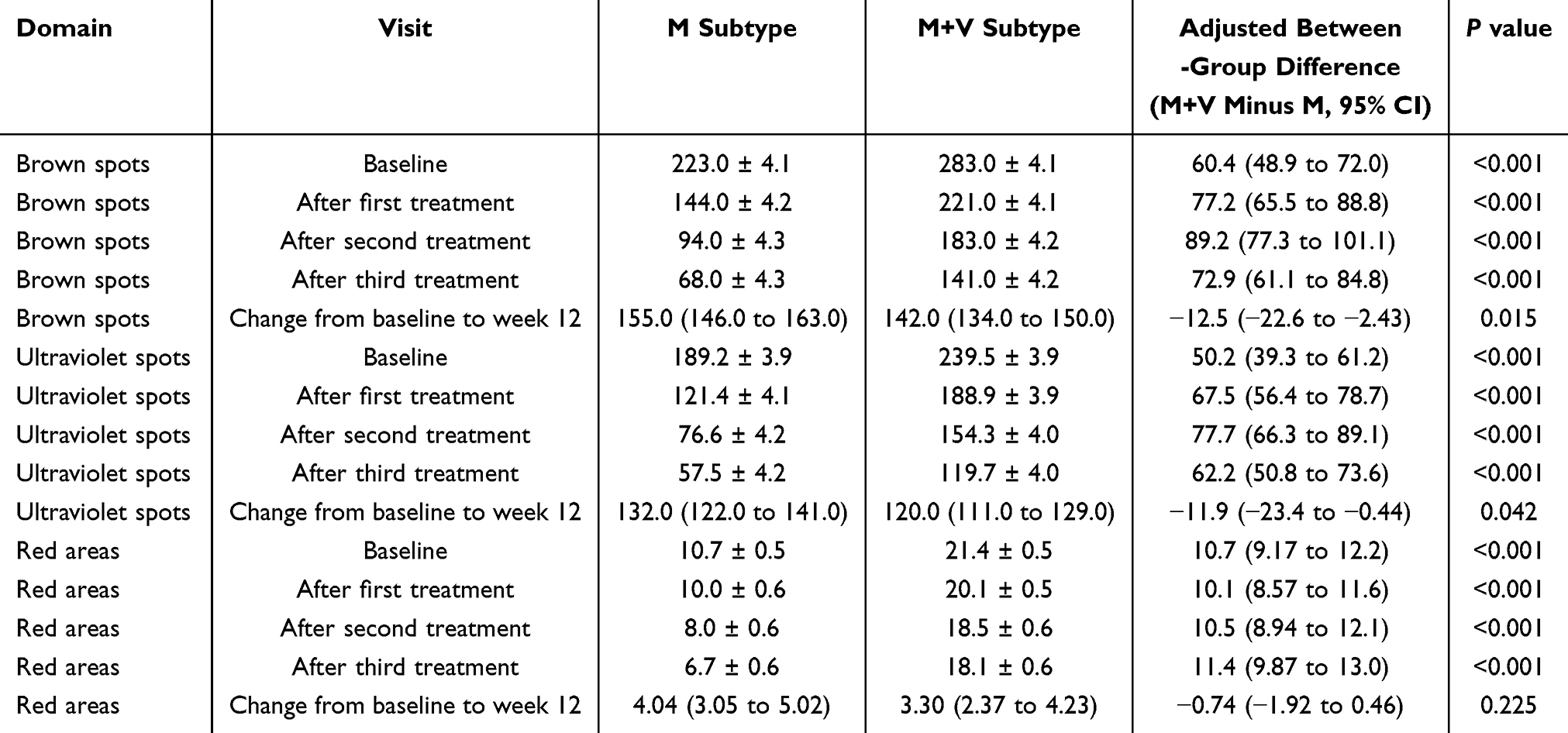 |
Table 4 Longitudinal VISIA Findings by Melasma Subtype |
Dermoscopic Findings
Dermoscopic vascular findings during follow-up are summarized in Table 5. Vascular quantity decreased during treatment in both subtypes, but the reduction was greater in the M subtype. At week 12, the estimated vascular quantity score remained higher in the M+V subtype than in the M subtype (2.08 ± 0.12 vs 0.80 ± 0.13, P < 0.001). The reduction from baseline to week 12 was also larger in the M subtype than in the M+V subtype, supporting a subtype-specific vascular response. Dermoscopic morphology showed a similar direction but a weaker longitudinal subtype effect. At week 12, faint red patches or simple linear vessels were more common in the M subtype, whereas reticular vessels remained more frequent in the M+V subtype (35.4% vs 2.4%, P < 0.001). Representative dermoscopic images further illustrate these subtype-specific patterns: the M subtype showed a clearer attenuation of pigmentary and vascular prominence by week 12, whereas the M+V subtype retained a more evident vascular background despite improvement in pigmentation (Figure 2).
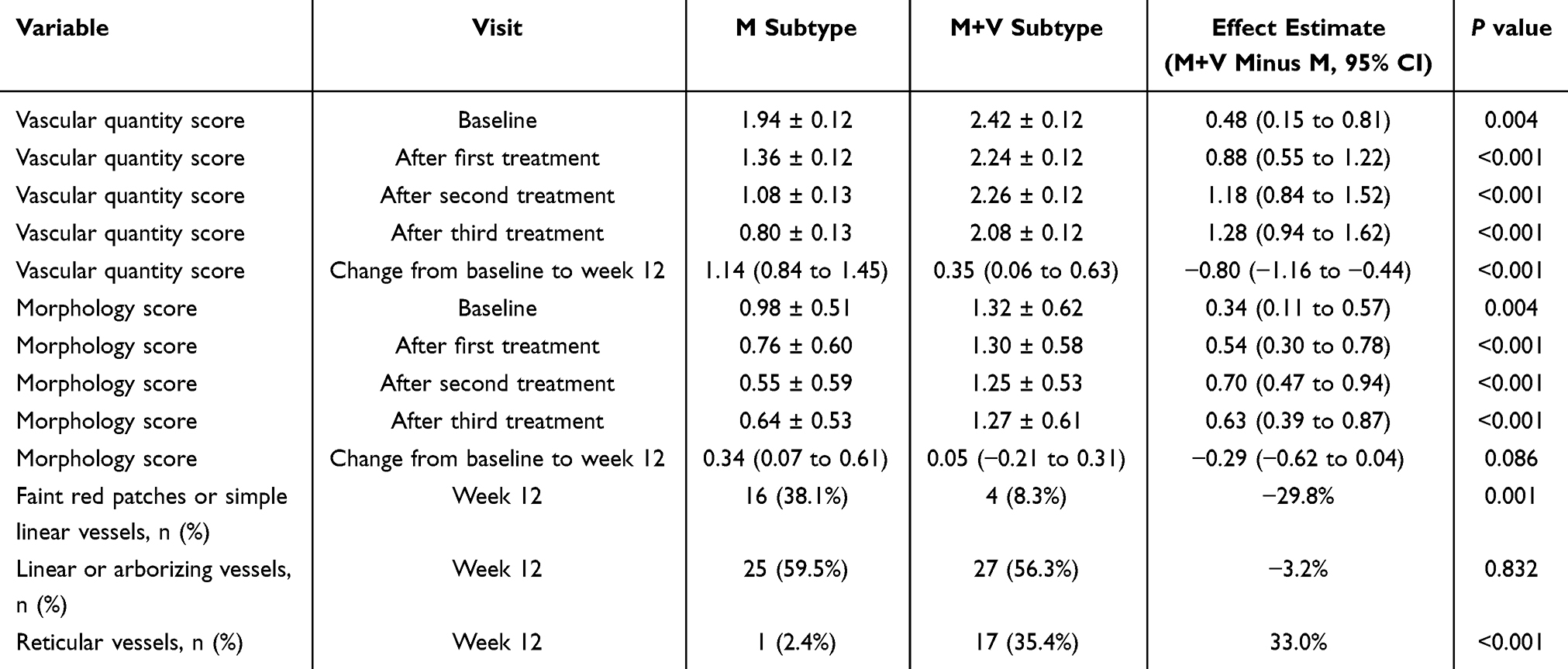 |
Table 5 Dermoscopic Vascular Findings During Follow-up |
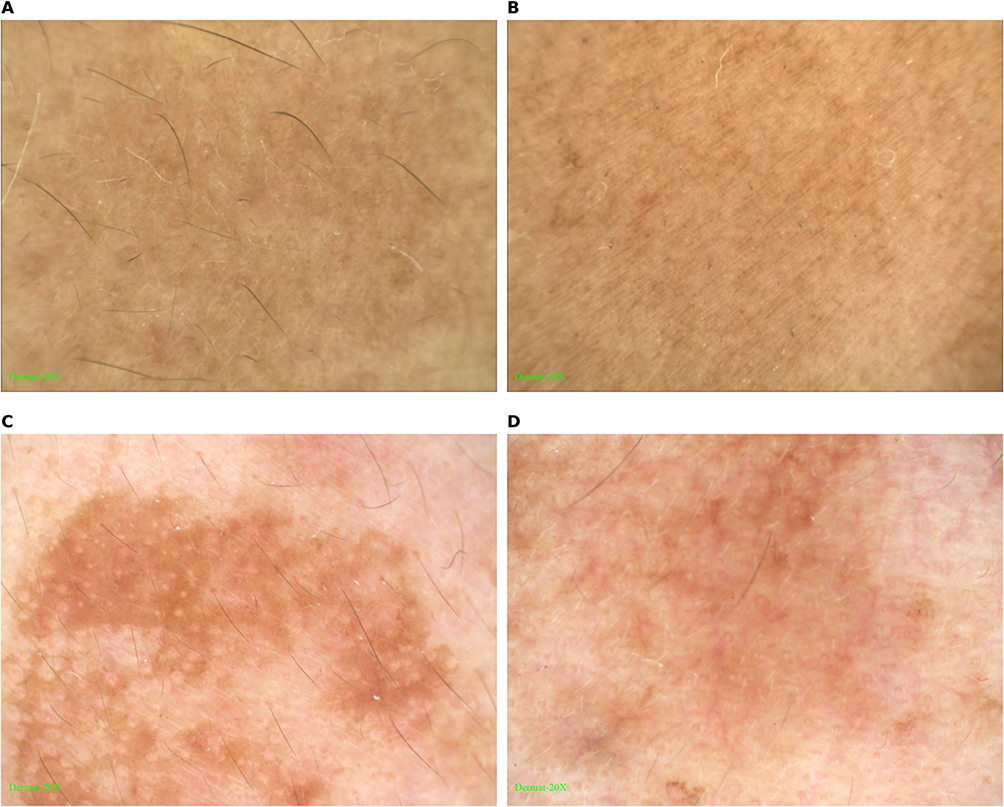 |
Figure 2 Representative dermoscopic images of the M and M+V subtypes at baseline and week 12. (A and B) show the M subtype at baseline and week 12, respectively. (C and D) show the M+V subtype at baseline and week 12, respectively. |
Safety and Patient Satisfaction
Safety and patient-reported outcomes are summarized in Table 6. Treatment was generally well tolerated in both subtypes, and no severe adverse events were recorded. Overall adverse events occurred in 18.0% of patients in the M subtype and 30.0% in the M+V subtype, without a statistically significant between-group difference. Transient erythema lasting more than 48 hours was the most common adverse event. Post-inflammatory hyperpigmentation was numerically more frequent in the M+V subtype than in the M subtype, but the difference was not statistically significant. No cases of blistering, hypopigmentation, or acneiform eruption were observed. Patient-reported outcomes at week 12 were more favorable in the M subtype. Marked improvement was reported by 59.5% of patients in the M subtype but only 10.4% of patients in the M+V subtype, and the overall distribution of self-reported improvement differed significantly between groups (P < 0.001). Satisfaction ratings showed a similar pattern, with very satisfied responses reported by 61.9% of patients in the M subtype compared with 16.7% in the M+V subtype (P < 0.001 for the overall distribution).
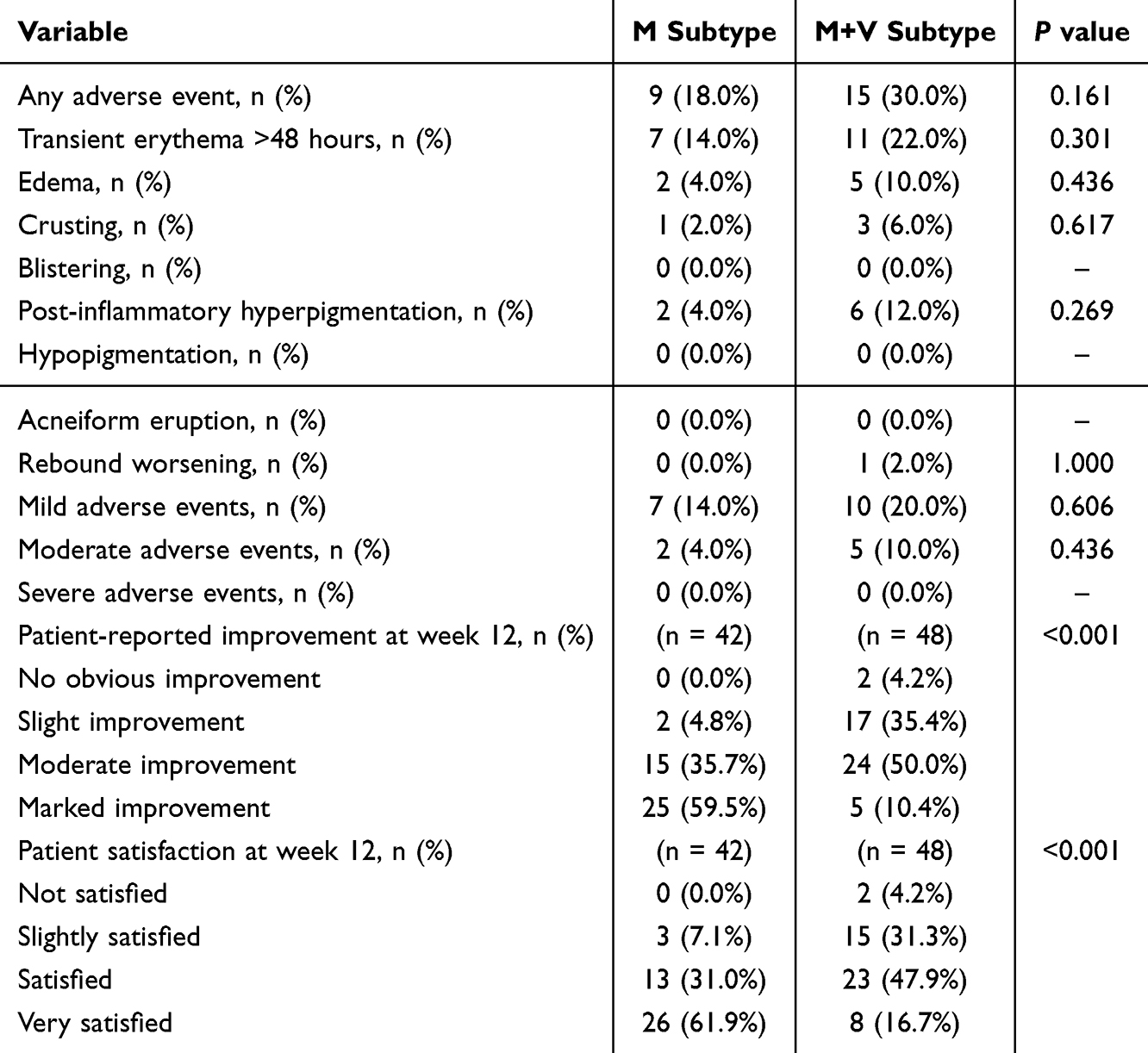 |
Table 6 Adverse Events and Patient Satisfaction |
Correlation and Multivariable Analyses
Correlation and multivariable regression results are summarized in Table 7. Improvement in MASI was moderately associated with reductions in pigment-related VISIA parameters. Specifically, ΔMASI was correlated with reductions in VISIA brown spots (Pearson r = 0.502, P < 0.001) and ultraviolet spots (Pearson r = 0.390, P < 0.001), but not with changes in VISIA red areas (Pearson r = 0.026, P = 0.807). The change in dermoscopic vascular quantity was also not significantly correlated with the change in VISIA red areas. In the multivariable model adjusted for age, disease duration, baseline MASI, Fitzpatrick skin type, previous topical treatment, previous device-based treatment, and photoprotection adherence, subtype remained an independent predictor of week 12 MASI improvement. Compared with the M+V subtype, the M subtype was associated with greater MASI reduction (adjusted coefficient, 2.863; 95% CI, 1.697 to 4.028; P < 0.001). Baseline MASI was also independently associated with greater improvement.
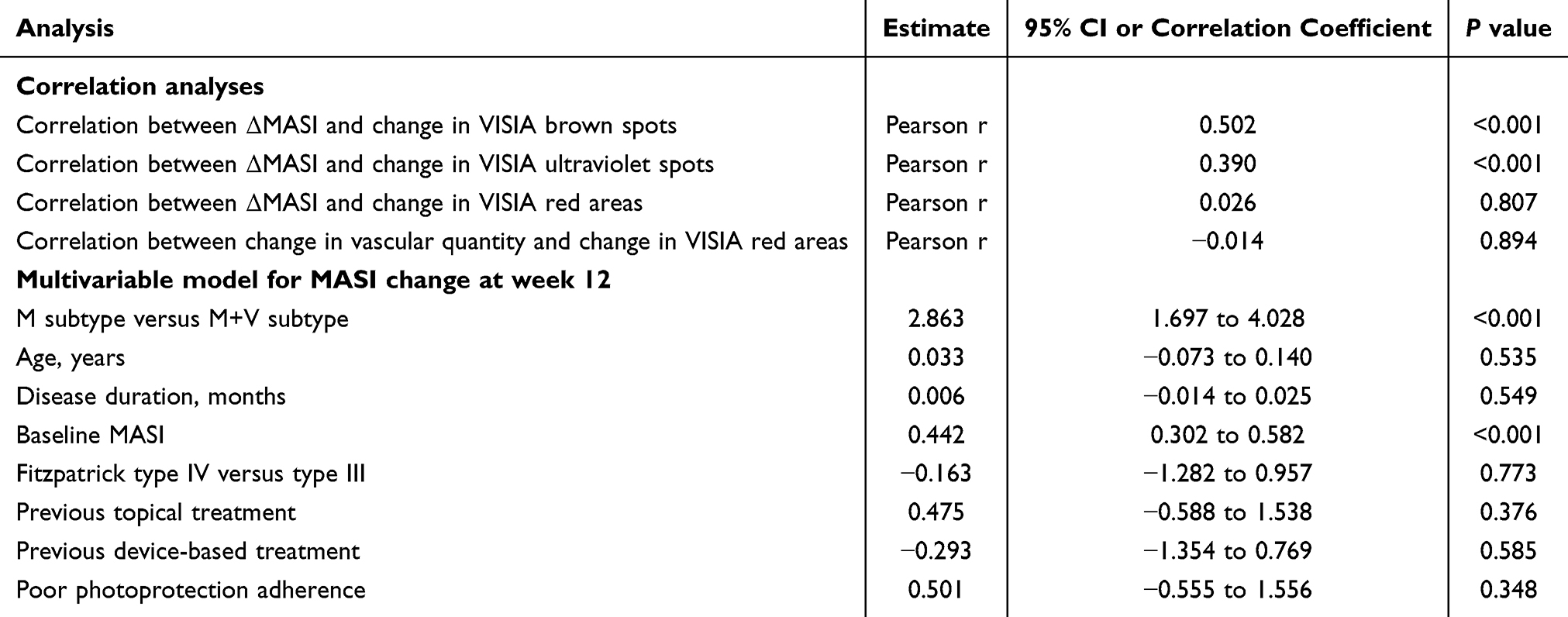 |
Table 7 Correlation and Multivariable Analyses |
These analyses suggest that the superior response observed in the M subtype was not fully explained by demographic characteristics or treatment-history variables included in the adjusted model. The correlation analyses further indicate that clinical improvement was more closely linked to reductions in pigment-related imaging features than to vascular-related changes. Thus, the key result-level signal was a divergence between pigment-responsive clinical lightening and persistent vascular features, particularly in the M+V subtype. This pattern supports the view that mixed pigmentary–vascular melasma represents a more challenging therapeutic phenotype and may require subtype-aware management beyond pigment clearance alone.
Discussion
Principal Findings
The present study showed that fractional-mode 694 nm Q-switched ruby laser improved melasma in both subtypes, but the magnitude and pattern of response were not uniform. Compared with the M+V subtype, the M subtype showed greater improvement in MASI, larger reductions in VISIA brown and ultraviolet spots, a more pronounced decline in dermoscopic vascular quantity, and substantially higher patient-reported improvement and satisfaction at week 12. By contrast, the M+V subtype entered treatment with a heavier pigmentary and vascular burden and, although it also improved, retained more residual disease at the final evaluation. The novelty of these findings lies in demonstrating, within the same laser protocol, that baseline clinicodermoscopic subtype was linked not only to clinical response but also to divergent pigmentary and vascular imaging trajectories. In the adjusted model, subtype remained independently associated with week 12 MASI improvement, supporting the view that melasma subtype is a clinically meaningful determinant of treatment response rather than a purely descriptive label.
Interpretation of Subtype-Specific Responses
These findings are consistent with the current understanding of melasma as a multifactorial disorder that extends beyond epidermal hypermelanosis alone. In addition to ultraviolet exposure and hormonal influences, previous and recent work has emphasized the importance of basement membrane disruption, solar elastosis, fibroblast senescence, mast-cell activity, vascular proliferation, oxidative stress, and upper dermal remodeling in melasma pathogenesis.1,3,9,10,24,25 Espósito et al further reported epidermal, basement membrane zone, upper dermal alterations and Wnt pathway activation in melasma compared with adjacent and retroauricular skin, supporting an integrated epidermal–dermal model of disease persistence.26 Within this framework, the less favorable response observed in the M+V subtype is biologically plausible. A phenotype with a more prominent vascular background may reflect broader dermal involvement, inflammatory activity, and a more persistent hypermelanogenic microenvironment, which may not be fully reversed by a predominantly pigment-targeted laser strategy.
This mechanism is particularly relevant when a pigment-directed intervention is used as monotherapy. Fractional-mode Q-switched ruby laser can reduce melanin-related clinical and imaging burden, but it may have limited ability to normalize vascular reactivity, dermal inflammation, matrix remodeling, or photoaging-associated changes that contribute to mixed melasma. This interpretation is consistent with our findings that MASI improvement was closely associated with reductions in VISIA brown and ultraviolet spots, whereas VISIA red areas and dermoscopic vascular findings showed weaker or more persistent change. Recent discussion of photobiomodulation and other noninvasive light-based strategies also suggests that future melasma management may need to consider not only melanogenesis but also inflammation, oxidative stress, vascular activity, and tissue repair pathways.27 Therefore, the M+V subtype may represent a more treatment-resistant phenotype in which pigment clearance alone is insufficient, and broader subtype-adapted approaches may be required.
The observed efficacy of fractional Q-switched ruby laser in both subtypes is in line with previous reports showing that ruby laser treatment can reduce melasma severity when delivered in fractional or carefully selected low-damage settings.15,16 However, prior procedural studies have generally focused on overall treatment efficacy rather than subtype-specific response. Our results extend that literature by showing that the same device protocol may yield substantially different outcomes according to the baseline clinicodermoscopic phenotype. This distinction is clinically important because recent treatment reviews have emphasized that procedural efficacy in melasma should be interpreted within the broader context of disease heterogeneity, relapse tendency, and the need for maintenance-oriented care.4,5,13
Clinical Value of Multimodal Assessment
An important contribution of this study is that clinical improvement and noninvasive imaging did not behave identically across all domains. VISIA brown and ultraviolet spots closely paralleled the clinical response, whereas VISIA red areas showed persistent between-group separation and much weaker association with MASI improvement. The correlation analyses reinforced this pattern: improvement in MASI was associated with reductions in VISIA brown and ultraviolet features, but not with change in VISIA red areas. This suggests that, under the present treatment protocol, clinical lightening was driven mainly by reduction in pigmentary burden rather than by equivalent normalization of the vascular component. This interpretation is consistent with the mechanism of a pigment-directed Q-switched laser and supports the practical value of combining clinical scoring with objective imaging, since a single metric may underrepresent biologically relevant residual disease.19–21
The dermoscopic findings further strengthened this interpretation. Dermoscopy has increasingly been recognized as a useful bedside tool for distinguishing melasma patterns and for monitoring treatment-related change.12,18 In our study, the M subtype showed a greater decline in vascular quantity and a shift toward less complex vascular morphology, whereas the M+V subtype more often retained reticular vessels and a higher residual vascular burden at week 12. In this sense, dermoscopy helped bridge the gap between the clinical phenotype and the imaging phenotype. It also explained why some patients appeared clearly improved clinically but still retained a vascular signature that may be relevant to persistence of disease activity.
Clinical Implications
From a therapeutic perspective, these results support a subtype-adapted treatment approach. For pigment-predominant melasma, fractional Q-switched ruby laser appears capable of achieving substantial lightening with favorable patient satisfaction. For pigmentary–vascular melasma, the more limited reduction in vascular parameters suggests that pigment clearance alone may be insufficient. This has practical relevance because vascular-targeted adjunctive strategies have previously been proposed for selected patients with clinically or dermoscopically evident vascular involvement.4,5,11 Our findings do not indicate that ruby laser is ineffective in the M+V subtype; rather, they suggest that this subgroup may benefit from a broader treatment plan in which pigment reduction is combined with attention to the vascular and photoaging-associated components of disease.
The present findings also have implications for follow-up and outcome assessment. In daily practice, treatment success in melasma is often judged mainly by visual improvement or by a single summary score. Our results suggest that this may be insufficient, especially in patients with mixed pigmentary–vascular features. A patient may show substantial MASI reduction and still retain a clinically meaningful vascular background on dermoscopy or VISIA red-area analysis. Conversely, the closer alignment between MASI and pigment-related VISIA domains indicates that brown and ultraviolet spot metrics may be particularly useful for tracking response in pigment-predominant disease. A multimodal framework combining MASI, VISIA, and dermoscopy therefore appears better suited to melasma than any single endpoint alone, because it captures different biological layers of response and helps distinguish true subtype-specific improvement from residual mixed-pattern activity.
In summary, the present study supports three clinically relevant conclusions. First, melasma subtype influences response to fractional Q-switched ruby laser, with better overall outcomes in pigment-predominant disease. Second, the vascular component remains relevant not only at baseline but also during follow-up, because residual vascular burden is more likely to persist in the M+V subtype. Third, integrating clinical scores with VISIA and dermoscopic assessment provides a more informative picture of treatment response than relying on one modality alone. Together, these findings favor a more individualized approach to melasma management in which clinicodermoscopic subtype classification helps guide both procedural choice and post-treatment evaluation.
Conclusion
In conclusion, fractional-mode 694 nm Q-switched ruby laser improved melasma in both pigmentary and pigmentary–vascular subtypes, but the magnitude and pattern of response differed according to baseline clinicodermoscopic phenotype. The pigmentary subtype showed greater improvement in MASI, larger reductions in VISIA brown and ultraviolet spots, a more pronounced decline in dermoscopic vascular quantity, and more favorable patient-reported outcomes at week 12. By contrast, the pigmentary–vascular subtype retained a heavier residual pigmentary and vascular burden after treatment, despite showing measurable clinical benefit. These findings support the practical value of baseline subtype classification and multimodal assessment for guiding laser-based treatment and interpreting therapeutic response in melasma.
The main strengths of this study include its prospective design, standardized fractional-mode 694 nm Q-switched ruby laser protocol, assessor-blinded clinical and imaging evaluation, and integrated assessment using MASI, VISIA, dermoscopy, patient-reported outcomes, safety monitoring, and multivariable analysis. Several limitations should also be acknowledged. This was a single-center, non-randomized clinical study that included only women with Fitzpatrick skin types III–IV, and the follow-up period was limited to 12 weeks after treatment. In addition, the study did not include a no-treatment or active-comparator group, and histologic or molecular markers of vascular activity, inflammation, oxidative stress, and dermal remodeling were not assessed.
Future multicenter controlled studies with longer follow-up are needed to confirm the durability of subtype-specific responses and to determine whether multimodal imaging can predict relapse or guide maintenance therapy. Further research should also explore combination regimens for pigmentary–vascular melasma, in which pigment-directed laser treatment is integrated with strategies targeting vascular, inflammatory, photodamage-related, and barrier-repair components. Such work may help refine individualized treatment algorithms for different melasma subtypes and improve long-term clinical outcomes.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy considerations but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of The Second Affiliated Hospital of Guilin Medical University (Approval No. QWJW-2024012). Informed consent was obtained from all participants before inclusion in the study. All study procedures were performed in accordance with the Declaration of Helsinki.
Acknowledgments
The authors sincerely thank all participants for their involvement in this study. The authors also acknowledge the support of the clinical staff of The Second Affiliated Hospital of Guilin Medical University in treatment delivery, data collection, and follow-up.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the project “Application and Efficacy Evaluation of Noninvasive Skin Imaging Technology in Q-Switched Ruby Fractional Laser Treatment of Melasma” (No. Z-C20240925).
Disclosure
The authors declare that they have no competing interests.
References
1. Passeron T, Picardo M. Melasma, a photoaging disorder. Pigm Cell Melanoma Res. 2018;31(4):461–16. doi:10.1111/pcmr.12684
2. Jo JY, Chae SJ, Ryu HJ. Update on melasma treatments. Ann Dermatol. 2024;36(3):125–134. doi:10.5021/ad.23.133
3. Passeron T. Melasma pathogenesis and influencing factors: an overview of the latest research. J Eur Acad Dermatol Venereol. 2013;27(Suppl 1):5–6. doi:10.1111/jdv.12049
4. Cassiano DP, Espósito ACC, da Silva CN, et al. Update on melasma-part II: treatment. Dermatol Ther. 2022;12(9):1989–2012. doi:10.1007/s13555-022-00780-4
5. Gan C, Rodrigues M. An update on new and existing treatments for the management of melasma. Am J Clin Dermatol. 2024;25(5):717–733. doi:10.1007/s40257-024-00863-2
6. Balkrishnan R, McMichael AJ, Camacho FT, et al. Development and validation of a health-related quality of life instrument for women with melasma. Br J Dermatol. 2003;149(3):572–577. doi:10.1046/j.1365-2133.2003.05419.x
7. Zhu Y, Zeng X, Ying J, Cai Y, Qiu Y, Xiang W. Evaluating the quality of life among melasma patients using the MELASQoL scale: a systematic review and meta-analysis. PLoS One. 2022;17(1):e0262833. doi:10.1371/journal.pone.0262833
8. Anderson L, Rodrigues M. Quality of life in a cohort of melasma patients in Australia. Australas J Dermatol. 2019;60(2):160–162. doi:10.1111/ajd.12969
9. Kim EH, Kim YC, Lee ES, Kang HY. The vascular characteristics of melasma. J Dermatol Sci. 2007;46(2):111–116. doi:10.1016/j.jdermsci.2007.01.009
10. Espósito ACC, Cassiano DP, da Silva CN, et al. Update on melasma-part I: pathogenesis. Dermatol Ther. 2022;12(9):1967–1988. doi:10.1007/s13555-022-00779-x
11. Kong SH, Suh HS, Choi YS. Treatment of melasma with pulsed-dye laser and 1,064-nm Q-switched Nd:YAG laser: a split-face study. Ann Dermatol. 2018;30(1):1–7. doi:10.5021/ad.2018.30.1.1
12. de Abreu L, Ramos-e Silva M, Quintella LP, et al. Dermoscopic classification of melasma: concordance study and correlation with the melanophages count. J Cosmet Dermatol. 2022;21(11):5887–5894. doi:10.1111/jocd.15145
13. Desai SR, Alexis AF, Elbuluk N, et al. Best practices in the treatment of melasma with a focus on patients with skin of color. J Am Acad Dermatol. 2024;90(2):269–279. doi:10.1016/j.jaad.2023.07.1045
14. Jiryis B, Toledano O, Avitan-Hersh E, Khamaysi Z. Management of melasma: laser and other therapies-review study. J Clin Med. 2024;13(5):1468. doi:10.3390/jcm13051468
15. Jang WS, Lee CK, Kim BJ, Kim MN. Efficacy of 694-nm Q-switched ruby fractional laser treatment of melasma in female Korean patients. Dermatol Surg. 2011;37(8):1133–1140. doi:10.1111/j.1524-4725.2011.02018.x
16. Hilton S, Heise H, Buhren BA, Schrumpf H, Bölke E, Gerber PA. Treatment of melasma in Caucasian patients using a novel 694-nm Q-switched ruby fractional laser. Eur J Med Res. 2013;18(1):43. doi:10.1186/2047-783X-18-43
17. Pandya AG, Hynan LS, Bhore R, et al. Reliability assessment and validation of the Melasma Area and Severity Index (MASI) and a new modified MASI scoring method. J Am Acad Dermatol. 2011;64(1):78–83. doi:10.1016/j.jaad.2009.10.051
18. Abdel Hay R, Mohammed FN, Sayed KS, Abd El Fattah NA, Ibrahim S. Dermoscopy as a useful tool for evaluating melasma and assessing the response to 1064-nm Q-switched Nd:YAG laser. Dermatol Ther. 2020;33(4):e13629. doi:10.1111/dth.13629
19. Zawodny P, Stój E, Kulig P, Skonieczna-żydecka K, Sieńko J. VISIA skin analysis system as a tool to evaluate the reduction of pigmented skin and vascular lesions using the 532 nm laser. Clin Cosmet Invest Dermatol. 2022;15:2187–2195. doi:10.2147/CCID.S380388
20. Zuo Y, Li A, He H, Wan R, Li Y, Li L. Assessment of features in facial hyperpigmentation: comparison study between VISIA and CSKIN. Skin Res Technol. 2022;28(6):846–850. doi:10.1111/srt.13216
21. Ma L, Huang X, Qiu Y, He Y. Analysis of facial redness by comparing VISIA and YLGTD. Skin Res Technol. 2023;29(7):e13356. doi:10.1111/srt.13356
22. Kimbrough-Green CK, Griffiths CEM, Finkel LJ, et al. Topical retinoic acid (tretinoin) for melasma in Black patients: a vehicle-controlled clinical trial. Arch Dermatol. 1994;130(6):727–733. doi:10.1001/archderm.1994.01690060057005
23. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
24. Kwon SH, Na JI, Choi JY, Park KC. Melasma: updates and perspectives. Exp Dermatol. 2019;28(6):704–708. doi:10.1111/exd.13844
25. Phansuk K, Vachiramon V, Jurairattanaporn N, Chanprapaph K, Rattananukrom T. Dermal pathology in melasma: an update review. Clin Cosmet Invest Dermatol. 2022;15:11–19. doi:10.2147/CCID.S343332
26. Espósito ACC, Brianezi G, de Souza NP, Miot LDB, Miot HA. Exploratory study of epidermis, basement membrane zone, upper dermis alterations and Wnt pathway activation in melasma compared to adjacent and retroauricular skin. Ann Dermatol. 2020;32(2):101–108. doi:10.5021/ad.2020.32.2.101
27. Galache TR, Sena MM, Tassinary JAF, Pavani C. Photobiomodulation for melasma treatment: integrative review and state of the art. Photodermatol Photoimmunol Photomed. 2024;40(1):e12935. doi:10.1111/phpp.12935
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.