Back to Journals » Patient Preference and Adherence » Volume 15
Subcutaneous Interferon Beta Therapy in Multiple Sclerosis Patients – Characterization of Injection Site Reactions and Flu-Like Symptoms in a Daily Practice Setting – Results from the Non-Interventional Study PERFECT
Authors Kukowski B, Rehberg-Weber K, Taipale K, Kowalik A, Oschmann P
Received 23 February 2021
Accepted for publication 6 May 2021
Published 24 May 2021 Volume 2021:15 Pages 1091—1100
DOI https://doi.org/10.2147/PPA.S307987
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Borries Kukowski,1 Karin Rehberg-Weber,2 Kirsi Taipale,2 Andreas Kowalik,3 Patrick Oschmann4
1Neurologische Gemeinschaftspraxis, Göttingen, Germany; 2Biogen GmbH, Munich, Germany; 3Praxis Dr. Kowalik, Stuttgart, Germany; 4Klinik für Neurologie, Klinikum Bayreuth GmbH, Bayreuth, Germany
Correspondence: Borries Kukowski
Neurologische Gemeinschaftspraxis, Groner-Tor-Straße 3, Göttingen, 37073, Germany
Tel +49 551 46069
Fax +49 551 55172
Email [email protected]
Purpose: The purpose of this study was to assess the prevalence of injection site reactions (ISR) and flu-like symptoms (FLS) during treatment with subcutaneous (SC) interferon (IFN) beta therapies and to document measures to mitigate and prevent ISR and FLS.
Patients and Methods: The cross-sectional post-authorization safety study PERFECT was conducted from 11/2017 to 7/2019 in neurology practices in Germany. Adult patients with relapsing-remitting multiple sclerosis (MS) receiving SC IFN beta for ≥ 3 months were eligible. The primary endpoints were patient-reported prevalence of ISR and FLS. Additional endpoints reported by patients, MS nurses, and neurologists included type, frequency, duration, time of occurrence, and management of ISR and FLS.
Results: In total, 603 patients (median age 45 years [range 36– 53], 74% female) were included in the analysis. Time since MS diagnosis was > 5 years in most patients. The majority had received none (64%) or 1 (22%) prior therapy. Current MS therapy in 36%, 32%, and 30% of patients was IFN beta-1b, IFN beta-1a, and peginterferon beta-1a, respectively. ISR and FLS under current therapy were reported by 84% and 68% of patients, respectively. ISR developed within 5 days after injection (84%) and lasted for 2– 14 days (53%) in most patients. The most frequent patient-reported symptom was erythema (39%). ISR resolved or abated with systemic treatments or topical ointments. Most frequent preventive measures included alternating injection sites (58%). Occurrence of ISR rarely resulted in treatment interruption (5%). FLS occurred predominantly up to 6 h after injection (40%) and lasted < 12 h (26%). The most frequent patient-reported symptoms were fatigue (15%) and aching limbs (15%). Assessments by physicians and MS nurses differed from patient-reported results.
Conclusion: Although ISR were experienced by the majority of patients, they rarely resulted in treatment interruption. In this real-world setting, ISR and FLS management was in line with published expert recommendations.
Keywords: peginterferon beta-1a, post-authorization safety study, real-world, erythema, disease-modifying therapy
Introduction
Interferon beta (IFN beta) therapies are well-established disease-modifying treatments for patients with relapsing multiple sclerosis (RMS). Almost 25 years of experience is available on the use of IFN beta treatment to treat multiple sclerosis (MS),1,2 and their safety and efficacy in MS therapy have been studied extensively. All five IFN beta preparations available feature a well-characterized efficacy and safety profile, but differ in structure, formulation, dose as well as frequency and route of administration.3 The most recently available IFN beta, peginterferon beta-1a, was developed as a modern pegylated version of the native protein IFN beta-1a with improved pharmacological properties to provide an interferon with increased biological activity, higher exposure, decreased renal clearance and longer elimination half-life.4–6 Based on results from the randomized placebo-controlled Phase 3 ADVANCE trial,7 peginterferon beta-1a was EMA approved in July 2014 and has been available in Germany since September 2014. By reducing the frequency of administration to bi-weekly SC injections, peginterferon beta-1a therapy achieved a high level of adherence in a real-world setting.8
The safety profile of peginterferon beta-1a is similar to that of the non-pegylated interferons, with the most common adverse events being mild-to-moderate injection site reactions (ISR) and flu-like symptoms (FLS).7,9 Recurring side effects such as ISR and FLS have important implications for quality of life and adherence and thus affect treatment outcomes.10−13 On therapy with peginterferon beta-1a, the FLS duration per injection was shown to be slightly longer than with non-pegylated IFN beta therapy, but the cumulative duration was significantly decreased.14
Currently, there is only limited information on the actual cause of skin reactions associated with SC injection of interferon therapies, and in particular on the effectiveness and implementation of recommended mitigation strategies in real life. Skin biopsies indicated that non-pegylated IFN beta may trigger inflammatory skin reactions through local chemokine induction followed by rapid movement of immune cells to the injection site.15 A better understanding of the adverse events of subcutaneously injected interferon beta, including the symptoms, pattern and duration of side effects, as well as mitigation strategies of patients in daily real life, is essential for developing effective strategies to improve adherence and persistence and to reduce the rate of treatment discontinuations. Therefore the cross-sectional study PERFECT as a single-time-point evaluation was conducted to analyze prevalence, severity, duration, and management of ISR and FLS in patients with relapsing-remitting MS (RRMS) receiving SC peginterferon beta-1a, SC interferon beta 1a, or SC interferon beta-1b. In addition, the perspectives of physicians, MS nurses and patients with regard to the frequency, duration, time to onset, and impact of ISR and FLS were analyzed. Another important aim was to learn more about the prevention and treatment of those side effects and their impact on patient’s daily activities.
Materials and Methods
Study Design and Patients
This multicenter non-interventional, cross-sectional, open-label voluntary post-authorization safety study (PASS) (EU PAS reg no EUPAS21013) was conducted at 54 sites across Germany from November 2017 to September 2019. The study design was reviewed and approved by the Ethics Committee of the Medical Association Lower Saxony, Germany (ref no. Bo/18/2017), and is consistent with the ethical standards included in the Declaration of Helsinki of 1964 and its later amendments.
Adult patients with RRMS, who had been stable on SC interferon beta treatment (IFN beta-1a, IFN beta-1b or peginterferon beta-1a) for at least 3 months were eligible for inclusion. Switching between SC interferon beta treatments within the 3-month period was allowed. Patients were excluded from the observation if they had any contraindications to SC interferon beta according to the German summary of product characteristics (SmPC), or if they received treatment with glatiramer acetate or intramuscular (IM) interferon beta. All patients were required to provide their written informed consent prior to enrolment.
Study Procedure and Endpoints
All patients were treated with their current SC interferon beta medication according to the SmPC and were managed according to clinical practice. On a single visit (at a single point of time), patients completed a standardized paper questionnaire. The completed questionnaire was stored in a sealed envelope to keep physicians and MS nurses blinded in order to enable them to answer the same questions independently of the patient and each other in an electronic case report form (eCRF). Additionally, the physician and MS nurse both documented the patient’s baseline characteristics into the eCRF.
The two primary endpoints were the number and proportion of patients with at least one patient-reported ISR and the number and proportion of patients with at least one patient-reported FLS. Secondary endpoints were the number and proportion of patients with at least one MS nurse-reported ISR/FLS and the number and proportion of patients with at least one physician-reported ISR/FLS. Additional secondary endpoints assessed by patients, MS nurses and physicians, respectively, included type and frequency of ISR/FLS assessed on a 5-point Likert scale (almost always, often, sometimes, rarely, never), duration of ISR/FLS (pre-defined periods: few minutes, up to 2 h, up to 1 d, 2–3 d, 4–6 d, 7–14 d, >2 weeks), usual time of occurrence of ISR/FLS (pre-defined periods: immediately, within 1 d, on the next day, after 2–5 d, after >5 d), interference of ISR/FLS with patient’s daily activities assessed by a visual analogue scale ranging from ‘0ʹ (not at all) to ‘10ʹ (extremely), number and proportion of patients taking treatment/actions to relieve the ISR/FLS, and number and proportion of patients with at least one self-administered treatment/action resulting in resolution or relief of ISR/FLS. Safety assessments included the documentation of serious adverse events.
Statistical Analysis
All documented data were analyzed by descriptive statistics using SAS® Version 9.3 (SAS Institute Inc., Cary, NC, USA). For continuous variables, statistic parameters including arithmetic mean, standard deviation and range were calculated. Frequency distributions for discrete variables were provided as percentage in relation to the total sample. No data imputation was performed. Due to the exploratory nature of the study and absence of formal hypothesis-testing, no formal sample size calculation was carried out. Subgroup analyses were performed with respect to patient’s previous and current MS therapy.
Results
In total, 626 patients provided informed consent. Of those, 23 patients were excluded from the analysis set for the following reasons: the informed consent form was signed after completion of the questionnaire (N=14), incorrect inclusion (N=5), no questionnaire available (N=2), and questionnaire completed prior to start of therapy (N=2). In addition to the 603 patients included in the analysis set, 545 physicians and 599 nurses completed questionnaires; for 541 cases, completed questionnaires were available from all involved functions (patients, physicians and MS nurses) (Figure 1). Baseline demographics including current treatment are summarized in Table 1. Patients, physicians and MS nurses correspondingly documented that the application of injections was mostly performed via autoinjector/pen (patients 68.7%, physicians 72.8%, MS nurses 75.0%). Nearly all patients received a training for injections.
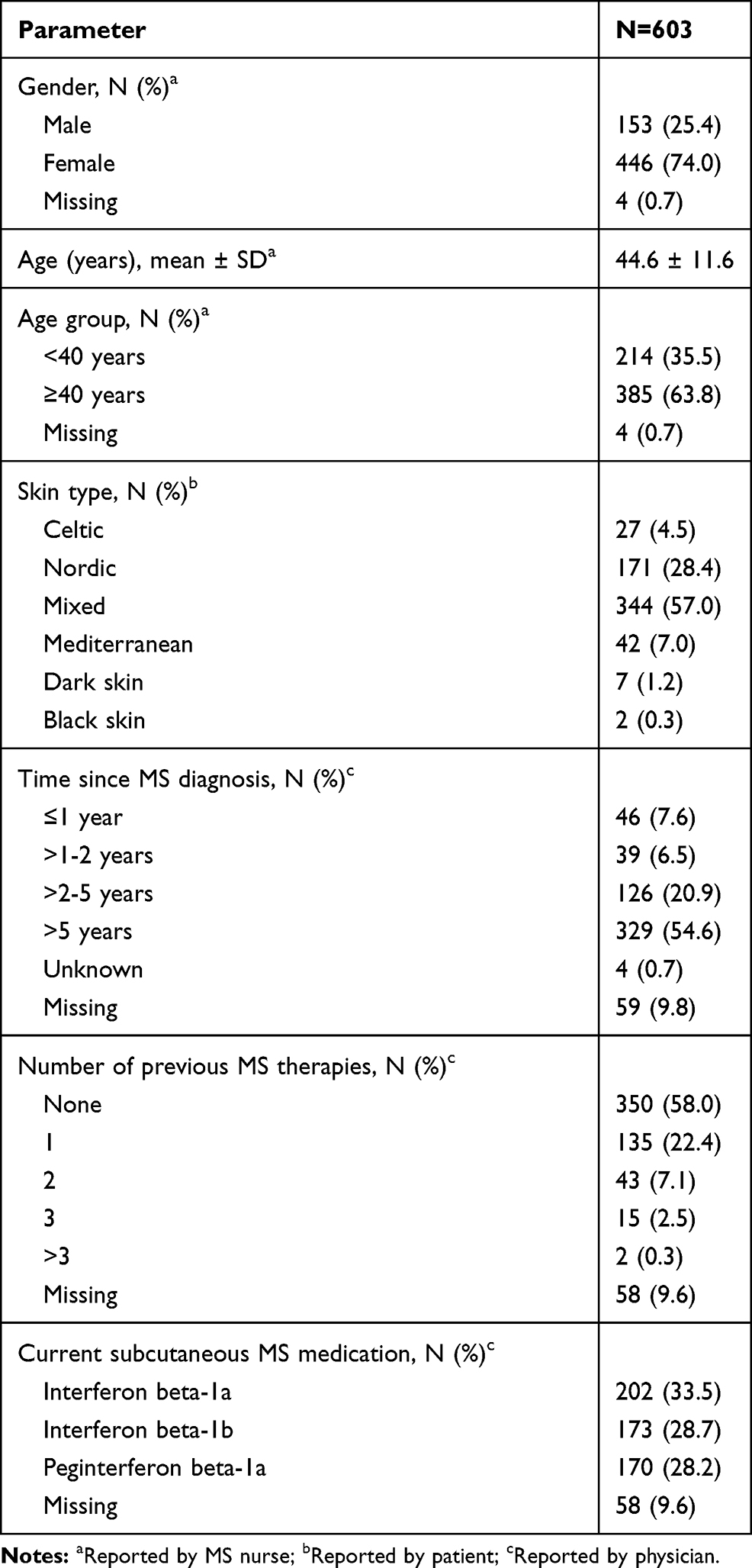 |
Table 1 Baseline Demographics |
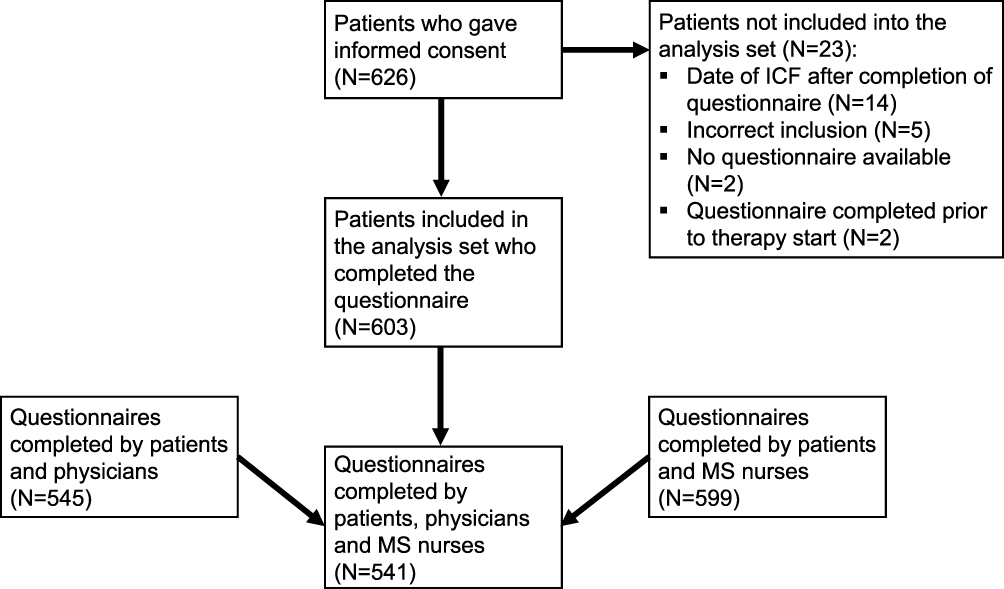 |
Figure 1 Patient disposition. Abbreviations: ICF, informed consent form; MS, multiple sclerosis. |
Prevalence of ISR and FLS
Under their current SC interferon beta therapy, 83.7% of patients experienced at least one ISR. In comparison, 65.8% of MS nurses and 56.1% of physicians reported patients experiencing at least one ISR under current therapy. ISR occurred across all skin types (Celtic, Nordic, mixed, Mediterranean, dark skin, black skin). Among pretreated patients, those who had ISR under their previous MS therapy (N=122) were with 91.8% numerically more likely to experience ISR also under their current therapy than patients who had no occurrence of ISR under previous therapy (N=69) (71.0%). The leading symptom of ISR was erythema, which was experienced ‘almost always’ by 38.5% of patients and documented by 31.2% of MS nurses and 28.1% of physicians (Figure 2). ISR lasted predominantly for 2 to 14 days (2–3 days: 18.4% patients, 20.9% physicians, 22.8% MS nurses; 7–14 days: 18.7% patients, 14.1% physicians, 19.3% MS nurses) (Figure 3). The most common time of onset of ISR was documented as “within one day after the injection” by 32.5% of patients, 39.6% of MS nurses, and 40.8% of physicians (Figure 4).
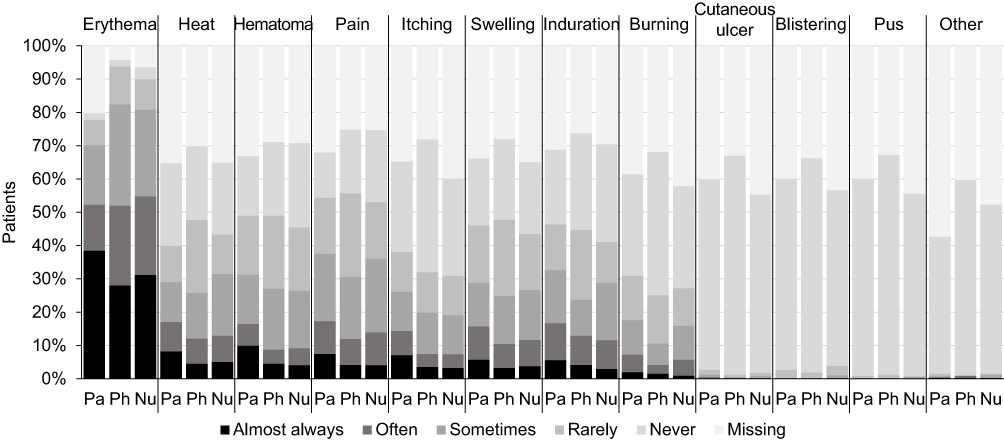 |
Figure 2 Frequency of ISR as reported by patients, physicians and MS nurses. Abbreviations Pa, patients (N=603); Ph, Physicians (N=545); Nu, MS nurses (N=599). |
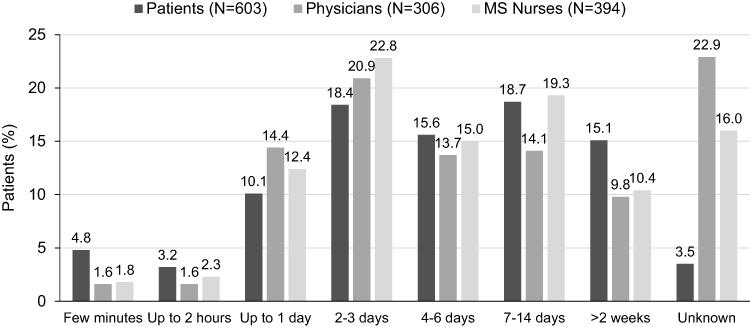 |
Figure 3 Duration of ISR as reported by patient, physician and MS nurse. |
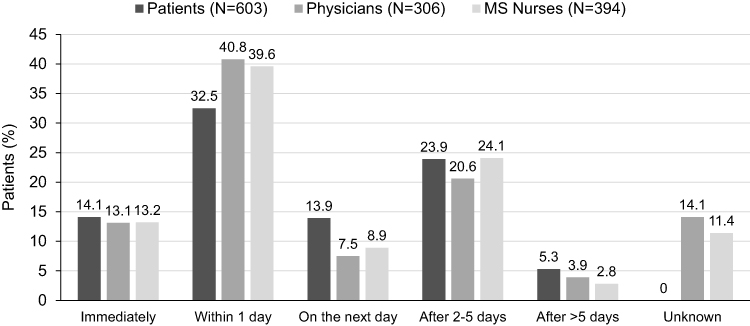 |
Figure 4 Time of occurrence of ISR after the injection. |
Under their current SC interferon therapy, 67.5% of patients reported at least one FLS. 50.8% of MS nurses and 47.9% of physicians reported at least one FLS. FLS occurred predominantly after 2 to 6 h after injection (30.3% reported by patients, 31.8% reported by physicians, 36.2% reported by MS nurses) and lasted 12 h or less (39.1% reported by patients, 48.7% reported by physicians, 50.5% reported by MS nurses). The most frequently reported FLS symptoms were aching limbs, headache, fatigue and weakness (Figure 5). No serious adverse events occurred during the study.
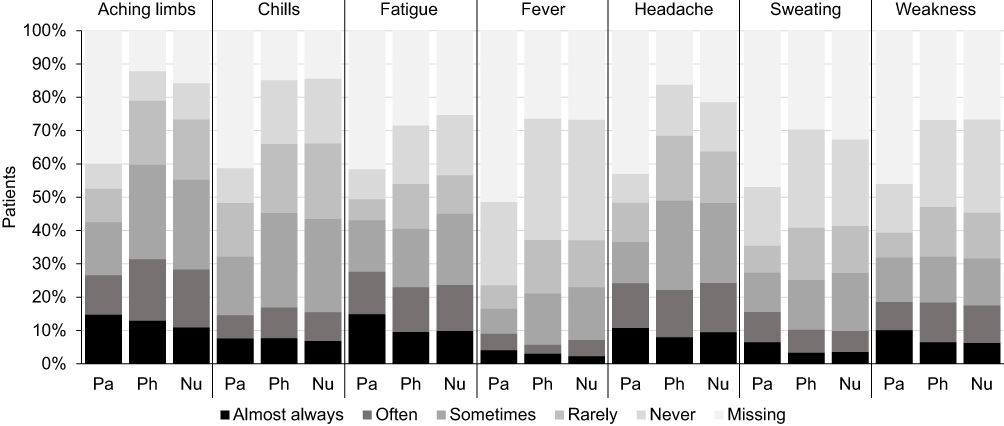 |
Figure 5 Frequency of FLS as reported by patients, physicians and MS nurses. Abbreviations: Pa, patients (N=603); Ph, Physicians (N=545); Nu, MS nurses (N=599). |
Interference of ISR and FLS with Daily Activities
Mean (±SD) interference of ISR with daily activities was 2.0 ± 2.3 reported by patients, 2.7 ± 2.2 reported by MS nurses, and 2.6 ± 2.3 reported by physicians (Figure 6). Mean (±SD) interference of FLS on daily activities was 4.5 ± 2.8 reported by patients, 4.4 ± 2.3 reported by physicians, and 4.2 ± 2.5 reported by MS nurses (Figure 6).
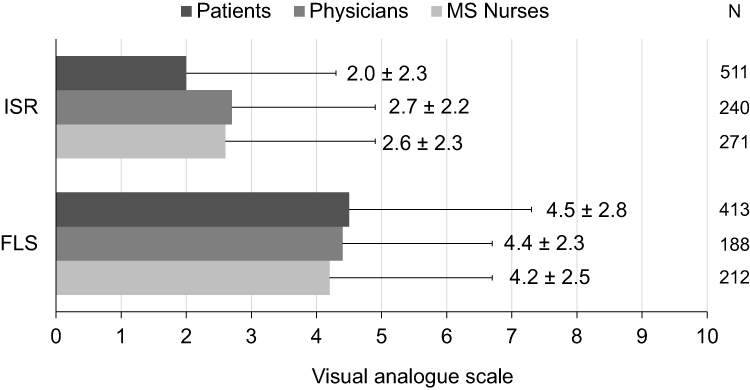 |
Figure 6 Mean (±SD) interference of ISR and FLS with patients’ daily activities assessed on a visual analogue scale ranging from ‘0ʹ (not at all) to ‘10ʹ (extremely) as reported by patients, physicians and MS nurses. |
Management of ISR and FLS
Within the first 3 months of treatment 4.3% of patients consulted a physician due to ISR compared to 2.5% within the last 3 months of treatment. Among patients, 33.0% (172/522) reported actions to relieve ISR and 22.3% of MS nurses (88/394) and 17.0% of physicians (52/306) reported that patients performed actions to relieve ISR. Treatment to mitigate ISR included local topical treatments, including pharmaceuticals (eg, dimetindene, bamipine, heparin ointment, hydrocorticoid or steroid ointments), and natural remedies (eg, cold brewed black tea compresses, ointments of arnica, marmot, hametum). Other measures such as cross-taping, leaving the needle longer in the injection site, homeopathic cell salts, or a mosquito bite stamp were used (Figure 7). ISR symptoms resolved with self-administered systemic treatments or topical ointments, as reported by 4.3% of patients (26/603), 13.6% of MS nurses (12/88) and 13.5% of physicians (7/52). Relief of ISR symptoms with self-administered systemic treatments or topical ointments was reported by 21.1% of patients (127/603), 67.0% of MS nurses (59/88) and 84.6% of physicians (44/52).
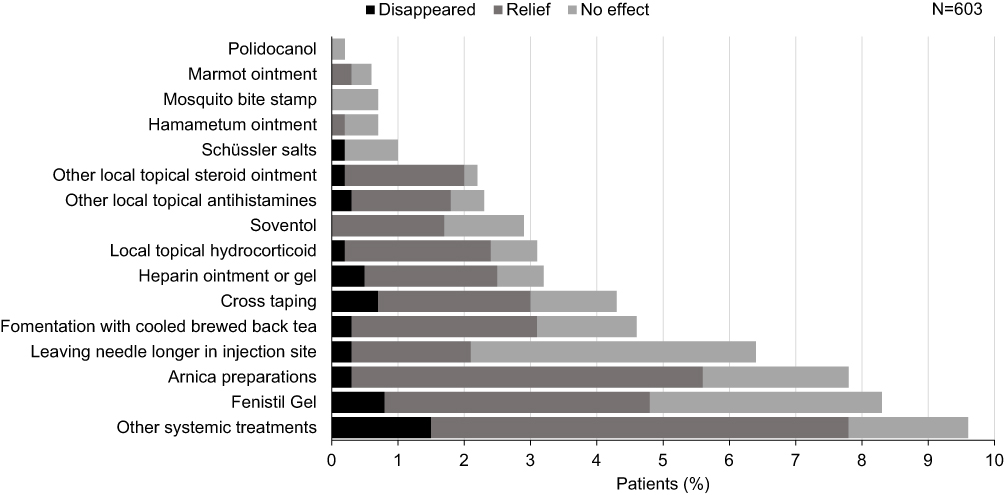 |
Figure 7 Actions performed to relieve ISR as reported by the patients. |
Precautions to prevent ISR were performed by 64.1% of patients (379/591). In contrast, only 22.9% of physicians (125/545) and 30.9% of MS nurses (185/599) reported that patients performed such precautions. The most frequently reported preventive measures used by patients included alternating injection sites (57.9%), followed by “allowing the injection solution to reach room temperature before injecting” (40.6%), “disinfecting the injection site before injecting” (39.6%), “taking plenty of time for each injection” (35.3%), and “cooling the injection site after injecting” (19.4%). These measures and frequency of use were in accordance with the assessments provided by physicians and MS nurses.
Treatment interruptions due to ISR within the last 3 months occurred only for 4.8% of patients; of those, n=11 patients missed only one injection, n=5 missed 2, n=3 missed 3, and n=7 missed >3 injections.
Actions to relieve FLS were performed by 76.0% of patients (351/462); 73.7% of MS nurses (224/304) and 72.4% of physicians (189/261) reported that patients performed actions to relieve FLS. The resolution of FLS symptoms with self-administered treatment/action such as use of analgesics (eg, ibuprofen or paracetamol) or change of injection time from the morning to the evening, was reported by 27.0% of patients (163/603), 36.2% of MS nurses (81/224) and 33.3% of physicians (63/189). The most frequently patient-reported measures to achieve resolution of FLS were ibuprofen (133/603) and paracetamol (36/603). Relief of FLS with self-administered treatment/action was reported by 35.0% of patients (211/603), 68.3% of nurses (153/224) and 70.4% of physicians (133/189). The most frequently patient-reported measure to achieve relief of FLS was ibuprofen (147/603), followed by “increase drinking per day” (49/603) and paracetamol (47/603).
Discussion
The present study provided a cross-sectional overview of the ISR and FLS prevalence in patients on SC interferon beta therapy as reported from three different perspectives – patients, physicians and MS nurses. The majority of patients experienced at least one ISR and/or FLS under current SC interferon beta therapy. The occurrence of ISR and FLS was reported at numerically lower rates by MS nurses and physicians compared to the data provided by patients. An inconsistency between patient-reported cutaneous adverse events and the prevalence reported by treating neurologists has been previously observed, indicating that skin reactions seem to be underrecognized by neurologists.10 MS nurses on the other hand appeared better informed about the occurrence of ISR and FLS than physicians. The reason for the observed discrepancy is unclear and warrants further investigation. Possibly patients are more reluctant to report adverse events to the neurologist, whereas they are more inclined to report them to the MS nurse. Other reasons could be that physicians are in a hurry. The occurrence of ISR was not associated with any particular skin type.
The rate of FLS for peginterferon beta-1a versus placebo after one year reported in the pivotal phase 3 ADVANCE trial (47%) was markedly lower than in the present study, in particular compared to the patient-reported rate (77%).
Consistent with observations from the ALLOW study,16 mean interference of ISR with patients’ daily activities was assessed as low by all three groups. Duration and interference of ISR and FLS with patients’ daily activities were slightly overestimated by nurses and physicians compared to the data provided by patients. The VAS applied here for assessing interference with daily activities is a generic, ie, not disease-specific, instrument commonly used to assess health status and is, for example, part of the EuroQol-5D (EQ-5D) health questionnaire,17,18 but the horizontal VAS used in the PERFECT study differs from that of the EQ-5D (vertical, scaled line). A 100-mm horizontal VAS had been used in MS patients for the assessment of injection pain of a novel glatiramer acetate formulation19 and a novel SC IFN beta-1a injection device20 as well as magnitude of discomfort of an IM IFN beta-1a formulation.21
Adverse events such as ISR and FLS are often reported as reasons for poor patient adherence to the treatment regimens.13,22 Although the rate of treatment interruptions due to ISR within the previous 3 months was low (4.8%), it is important to observe prevention and mitigation strategies in order to promote treatment persistence. In 2019, experts from an interdisciplinary Board of German and Austrian neurologists and dermatologists published recommendations for ISR management in daily clinical care.23 Prevention strategies included warming the interferon solution to room temperature before injection, usage of an aseptic injection technique, and rotation of the subcutaneous injection site at each injection. Mitigation strategies involved cold brewed black-tea compresses, topical treatment with 5% polidocanol, and topical corticosteroids, as well as refrigerated lotions, creams and ointments.23 Most of these recommendations were implemented by the patients in our study. Despite the broad range of reported mitigation strategies, however, the majority of patients did not perform any actions to relieve ISR. Among those applying self-administered treatments, ISR rarely resolved, but relief was achieved in approximately three-quarters of patients. Generally, a less frequent prevalence of ISRs with interferon beta-1a IM than with SC administration has been reported in prior studies.3,24 Consequently, IM administration may offer patients an additional peginterferon beta-1a treatment option. A recent Phase 1 study established the bioequivalence of IM compared to SC administration of peginterferon beta-1a and indicated a numerically lower prevalence of ISR with IM than with SC administration, thus supporting the consideration of IM injection as an alternative route of administration for peginterferon beta-1a in patients with RMS or RRMS.25
Strategies applied to ease FLS were in line with previously published recommendations and included analgesic use, dose titration, and consideration of the timing of administration so that FLS occur during sleep.26 MS nurses were generally more aware of the patient’s discomfort and actions to relieve or prevent symptoms than physicians. Overall, a numerically higher percentage of patients reported success of the measures applied to prevent and relieve FLS than with ISR. In line with two previous Delphi analyses,16,22 the results reinforce expectation setting and tolerability management to reduce the impact of ISR and FLS on patient experience.
This study was not designed as a head-to-head comparison between different SC interferon beta formulations, but to provide a general overview of the scope and management of ISR and FLS during treatment with SC injectable interferons. The benefits and increase in satisfaction of switching from non-pegylated interferon to peginterferon beta-1a have already been addressed in the ALLOW study and the Italian PLATINUM study.14,27,28 However, contrary to the longitudinal design of the ALLOW study, which reported the cumulative duration of FLS, the cross-sectional design of our study provides rather a snapshot in time and results may be subject to recall bias.
The study is limited by its non-interventional cross-sectional design which simultaneously assesses exposure and outcome, and therefore does not provide evidence of a temporal relationship between exposure and outcome. Yet, this study design has advantages in terms of patient heterogeneity as it collects data in a real-world setting. Another limitation was the incomplete data set, which is a common issue in non-interventional studies. Furthermore, the questionnaire used was not validated as a tool for measuring patient-reported outcomes. Cross comparison of data from different functions (patient, physician, MS nurse) has to be assessed with caution, as all results are based on descriptive statistics only. No statistical tests were conducted to verify how far comparable answers of two or more functions were in accordance. Approximately 10% of physicians did not complete the questionnaire and possible site effects have not been investigated. For the survey of patient-reported data, a paper questionnaire was used, therefore inconsistent data for all analyses may be expected. The electronic questionnaire used by MS nurses and physicians was constructed with filters enabling skipping over non-applicable questions for a particular patient. As these filters were not applicable in the paper questionnaire, patients may have answered non-applicable questions, resulting in inconsistencies of data, which were not evaluated. There is no gold standard to differentiate whether the data provided by one respondent (eg, patient) is more valid than data from another (eg, physician). Nevertheless, it might be expected that patients were more aware of their own physical condition and measures to relieve and prevent discomfort, whereas physicians and MS nurses might have been better informed about previous medication, duration of treatment and injection schemes. The strength of this study was the collection of data from three different groups of respondents, thus providing a comprehensive overview of the occurrence, impact and management strategies of ISR and FLS from the distinct perspectives of patients, MS nurses and physicians.
Conclusion
Although ISR and FLS were experienced by the majority of patients in this real-world setting, they rarely resulted in treatment interruption, and interference with daily activities was low. In this real-world setting, ISR and FLS management was in line with published expert recommendations. However, the study uncovered an obvious need to better educate patients as only a little more than half of them applied the most simple and important strategies such as rotating injection sites. The differences in assessments observed between patients, physicians and MS nurses may indicate a need in real-world settings to improve communication between the three functions in order to align perspectives.
Acknowledgments
This study is funded by Biogen GmbH, München, Germany. The sponsor was involved in the conceptualisation and supervision of this study. We thank Dr Petra Jöstingmeyer (med:unit GmbH, Cologne, Germany) who provided medical writing services. Biogen GmbH provided funding for medical writing support in the development of this article. The authors had full editorial control of the manuscript and provided their final approval.
Disclosure
BK reports personal fees from Biogen, during the conduct of the study. KRW and KT are employees of Biogen. PO received honoraria as a speaker from Bayer Vital, Novartis, Roche and Teva; for trial activities from AB Science, Bayer Vital, Biogen, Bionorica, Deutschland GmbH, Roche, Merck Serono, Sanofi/Genzyme, Novartis, Teva and received grants for congress trips and participation from Bayer Vital. The authors report no other conflicts of interest in this work.
References
1. Hegen H, Auer M, Deisenhammer F. Pharmacokinetic considerations in the treatment of multiple sclerosis with interferon-β. Expert Opin Drug Metab Toxicol. 2015;11(12):1803–1819. doi:10.1517/17425255.2015.1094055
2. O’Connor PW, Oh J. Disease-modifying agents in multiple sclerosis. Handb Clin Neurol. 2014;122:465–501.
3. Limmroth V, Putzki N, Kachuck NJ. The interferon beta therapies for treatment of relapsing-remitting multiple sclerosis: are they equally efficacious? A comparative review of open-label studies evaluating the efficacy, safety, or dosing of different interferon beta formulations alone or in combination. Ther Adv Neurol Disord. 2011;4(5):281–296. doi:10.1177/1756285611413825
4. Bailon P, Won CY. PEG-modified biopharmaceuticals. Expert Opin Drug Deliv. 2009;6(1):1–16. doi:10.1517/17425240802650568
5. Baker DP, Pepinsky RB, Brickelmaier M, et al. PEGylated interferon beta-1a: meeting an unmet medical need in the treatment of relapsing multiple sclerosis. J Interferon Cytokine Res. 2010;30(10):777–785. doi:10.1089/jir.2010.0092
6. Hu X, Miller L, Richman S, et al. A novel PEGylated interferon beta-1a for multiple sclerosis: safety, pharmacology, and biology. J Clin Pharmacol. 2012;52(6):798–808. doi:10.1177/0091270011407068
7. Calabresi PA, Kieseier BC, Arnold DL, et al. Pegylated interferon beta-1a for relapsing-remitting multiple sclerosis (ADVANCE): a randomised, phase 3, double-blind study. Lancet Neurol. 2014;13(7):657–665. doi:10.1016/S1474-4422(14)70068-7
8. Menge T, Rehberg-Weber K, Taipale K, Nastos I, Jauß M. Peginterferon beta-1a was associated with high adherence and satisfaction in patients with multiple sclerosis in a German real-world study. Ther Adv Neurol Disord. 2021;14:17562864211000461. doi:10.1177/17562864211000461
9. Newsome SD, Scott TF, Arnold DL, et al. Long-term outcomes of peginterferon beta-1a in multiple sclerosis: results from the ADVANCE extension study, ATTAIN. Ther Adv Neurol Disord. 2018;11:1756286418791143. doi:10.1177/1756286418791143
10. Balak DM, Hengstman GJ, Hajdarbegovic E, van den Brule RJ, Hupperts RM, Thio HB. Prevalence of cutaneous adverse events associated with long-term disease-modifying therapy and their impact on health-related quality of life in patients with multiple sclerosis: a cross-sectional study. BMC Neurol. 2013;13:146. doi:10.1186/1471-2377-13-146
11. Beer K, Müller M, Hew-Winzeler AM, et al. The prevalence of injection-site reactions with disease-modifying therapies and their effect on adherence in patients with multiple sclerosis: an observational study. BMC Neurol. 2011;11:144. doi:10.1186/1471-2377-11-144
12. Devonshire V, Lapierre Y, Macdonell R, et al. The Global Adherence Project (GAP): a multicenter observational study on adherence to disease-modifying therapies in patients with relapsing-remitting multiple sclerosis. Eur J Neurol. 2011;18(1):69–77. doi:10.1111/j.1468-1331.2010.03110.x
13. Moccia M, Palladino R, Russo C, et al. How many injections did you miss last month? A simple question to predict interferon β-1a adherence in multiple sclerosis. Expert Opin Drug Deliv. 2015;12(12):1829–1835. doi:10.1517/17425247.2015.1078789
14. Naismith RT, Hendin B, Wray S, et al. Patients transitioning from non-pegylated to pegylated interferon beta-1a have a low risk of new flu-like symptoms: ALLOW phase 3b trial results. Mult Scler J Exp Transl Clin. 2019;5(1):2055217318822148.
15. Buttmann M, Goebeler M, Toksoy A, et al. Subcutaneous interferon-beta injections in patients with multiple sclerosis initiate inflammatory skin reactions by local chemokine induction. J Neuroimmunol. 2005;168(1–2):175–182. doi:10.1016/j.jneuroim.2005.07.011
16. Hendin B, Huang D, Wray S, et al. Subcutaneous peginterferon beta-1a injection-site reaction experience and mitigation: delphi analysis of the ALLOW study. Neurodegener Dis Manag. 2017;7(1):39–47. doi:10.2217/nmt-2016-0032
17. Hinz A, Klaiberg A, Brähler E, König HH. [The Quality of Life Questionnaire EQ-5D: modelling and norm values for the general population]. Psychother Psychosom Med Psychol. 2006;56(2):42–48. doi:10.1055/s-2005-867061
18. Kersten P, Küçükdeveci AA, Tennant A. The use of the Visual Analogue Scale (VAS) in rehabilitation outcomes. J Rehabil Med. 2012;44(7):609–610. doi:10.2340/16501977-0999
19. Anderson G, Meyer D, Herrman CE, et al. Tolerability and safety of novel half milliliter formulation of glatiramer acetate for subcutaneous injection: an open-label, multicenter, randomized comparative study. J Neurol. 2010;257(11):1917–1923. doi:10.1007/s00415-010-5779-x
20. Jaber A, Bozzato GB, Vedrine L, Prais WA, Berube J, Laurent PE. A novel needle for subcutaneous injection of interferon beta-1a: effect on pain in volunteers and satisfaction in patients with multiple sclerosis. BMC Neurol. 2008;8:38. doi:10.1186/1471-2377-8-38
21. Kleinschnitz C, Niemczyk G, Rehberg-Weber K, Wernsdörfer C. Interferon Beta-1a (AVONEX®) as a Treatment Option for Untreated Patients with Multiple Sclerosis (AXIOM): a prospective, observational study. Int J Mol Sci. 2015;16(7):15271–15286. doi:10.3390/ijms160715271
22. Halper J, Centonze D, Newsome SD, et al. Management strategies for flu-like symptoms and injection-site reactions associated with peginterferon Beta-1a: obtaining recommendations using the delphi technique. Int J MS Care. 2016;18(4):211–218. doi:10.7224/1537-2073.2015-042
23. Kolb-Mäurer A, Sunderkötter C, Kukowski B, Meuth SG. An update on peginterferon beta-1a management in multiple sclerosis: results from an interdisciplinary Board of German and Austrian Neurologists and dermatologists. BMC Neurol. 2019;19(1):130. doi:10.1186/s12883-019-1354-y
24. Balak DM, Hengstman GJ, Çakmak A, Thio HB. Cutaneous adverse events associated with disease-modifying treatment in multiple sclerosis: a systematic review. Mult Scler. 2012;18(12):1705–1717. doi:10.1177/1352458512438239
25. Zhao Y, Chen K, Ramia N, et al. Bioequivalence of intramuscular and subcutaneous peginterferon beta-1a: results of a Phase I, open-label crossover study in healthy volunteers. Ther Adv Neurol Disord. 2021;14:1756286420975227. doi:10.1177/1756286420975227
26. Filipi ML, Beavin J, Brillante RT, et al. Nurses’ perspective on approaches to limit flu-like symptoms during interferon therapy for multiple sclerosis. Int J MS Care. 2014;16(1):55–60. doi:10.7224/1537-2073.2013-006
27. Hendin B, Naismith RT, Wray SE, et al. Treatment satisfaction significantly improves in patients with multiple sclerosis switching from interferon beta therapy to peginterferon beta-1a every 2 weeks. Patient Prefer Adherence. 2018;12:1289–1297. doi:10.2147/PPA.S157317
28. Centonze D, Fantozzi R, Buttari F, et al. Peg-IFN beta-1a pre-filled pen (Plegridy®) improves satisfaction in patients with relapsing-remitting multiple sclerosis who were dissatisfied with other subcutaneous interferons.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.