Back to Journals » Clinical Ophthalmology » Volume 20
Subconjunctival Triamcinolone Acetonide Injection Compared with Dexamethasone Ophthalmic Insert for Inflammation Prophylaxis After Cataract Surgery: A Comparative Clinical Study
Authors Gannamaneni K, Reddy K ![]() , Shapiro JN, Levine H
, Shapiro JN, Levine H ![]() , Verkade AJ, Armenti ST, Hood CT, Mian SI
, Verkade AJ, Armenti ST, Hood CT, Mian SI
Received 30 August 2025
Accepted for publication 18 December 2025
Published 21 January 2026 Volume 2026:20 564202
DOI https://doi.org/10.2147/OPTH.S564202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kartik Gannamaneni,1,* Karthik Reddy,1,* Jeremy N Shapiro,2 Harry Levine,1 Angela J Verkade,1 Stephen T Armenti,3 Christopher T Hood,1 Shahzad I Mian1
1Department of Ophthalmology and Visual Sciences, University of Michigan, Ann Arbor, MI, USA; 2Department of Ophthalmology, Johns Hopkins University, Baltimore, MD, USA; 3Department of Ophthalmology, University of Pennsylvania, Philadelphia, PA, USA
*These authors contributed equally to this work
Correspondence: Shahzad I Mian, Department of Ophthalmology and Visual Sciences, University of Michigan, 1000 Wall Street, Ann Arbor, MI, 48105, USA, Tel +1 734-764-6468, Email [email protected]
Purpose: To determine differences in efficacy and outcomes during the first post-operative month (POM1) between intracanicular dexamethasone implant (DII) and subconjunctival triamcinolone injection (STAI) for prophylaxis of rebound iritis or cystoid macular edema (CME) in patients undergoing cataract surgery.
Design: This was a retrospective, comparative cohort study of standard phacoemulsification with posterior-chamber intraocular lens placement between January 2020 and July 2023.
Methods: Patients in the DII group received a 0.4 mg insert intraoperatively, whereas those in the STAI group received 4– 6 mg of triamcinolone. Patients were excluded if they received additional anti-inflammatory treatment or a history of iritis, ocular infection, glaucoma, intraoperative posterior capsular rupture, vitreous prolapse, or retained lens fragments. Post-operative visits during POM1 were reviewed to determine the characteristics and timing of rebound iritis, CME, and changes in intraocular pressures (IOP).
Results: In total, 266 eyes from 174 patients were included in the DII group, while 103 eyes from 62 patients were included in the STAI group. Demographics, comorbidities, and pre-operative IOPs were similar between groups. Neither group experienced an increase in IOP elevation of > 10 mmHg from baseline or preoperative measurements compared to POM1. The DII group had mean time (days) to iritis that occurred sooner compared to the STAI group [DII group (12.8 days, SD: 8.3) vs STAI group (22.3 days, SD: 5.7), p < 0.05]. Overall, there was a trend toward higher rates of rebound iritis among the DII (9.0%) than among the STAI (3.9%) groups (p = 0.12).
Conclusion: In this retrospective cohort study, participants who received STAI appeared to have iritis at a later onset than those who received DII. However, post-operative complications were low, with no significant differences in the rates of rebound iritis or CME between the two groups. STAI and DII have similar clinical utility in the prophylaxis of inflammation after cataract surgery.
Keywords: post-operative inflammation, triamcinolone acetonide, dexamethasone, cataract surgery, macular edema
Introduction
Cataract surgery is among the most widely performed surgical procedures in the world, involving removal of the natural lens and placement of an intraocular lens.1 While largely effective and safe with limited complications, post-operative inflammation is a common phenomenon that affects patients undergoing cataract surgery.2,3 These effects may manifest as cystoid macular edema, intraocular inflammation, post-operative iritis, and increased intraoperative pressures, contributing toward poorer outcomes.2,4–7
Many solutions exist for the management of post-operative inflammation, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids.2 These medications are utilized in a spectrum of oral, intracameral, topical, and injectable formulations. However, a common phenomenon among elderly patients is difficulty with compliance and instillation of topical and drop-based formulations.8–10 Some studies estimate <50% adherence to topical prednisolone.11 Additionally, the topical route has known issues with penetration due to complex eye physiology and medication usage patterns, leading to reduced efficacy despite compliance with topical regimens.12,13
Current solutions to ensure the continual penetration of anti-inflammatory agents, regardless of patient compliance, include intracameral and injectable formulations.9 These agents may be injected or placed post-operatively to provide continuous dosing of these medications and have been associated with decreased or similar levels of inflammation to topical methods with similar rates of post-operative complications.14–17
Among options for dropless management of post-operative inflammation, dexamethasone intracanalicular insert (DII) and subconjunctival triamcinolone injection (STAI) have been found to be efficacious for inflammation management in several studies. Walters et al first identified the efficacy of single dose DII for reducing post-operative ocular pain and decreases in anterior chamber flare compared to placebo vehicle depot after cataract surgery.18 There is a wide variance in the rates of rebound iritis (3–11%) with use of intracanalicular inserts.15,17,19,20 Selected studies have reported superiority or non-inferiority of DII compared to common topical formulations.15,21 One study did find a trend that was non-significant (p = 0.50) toward higher rates of rebound inflammation among eyes that received DII (9.2%) compared to eyes that received steroid drops (6.9%), but sample size was limited (n = 131).19 STAI has had similar or superior efficacy in inflammation reduction compared to topical formulations in other studies. One prospective study found decreased retinal thickness (+1.2 in dexamethasone drops versus −9.2 in STAI, p = 0.031) and lower aqueous flare (3.3 in dexamethasone drops versus −0.02 in STAI, p = 0.021) among patients receiving STAI.22
Identification and utilization of effective drugs for inflammation is critical for enhanced patient safety and reduction of postoperative intraocular pressure (IOP) spikes. To date, however, few studies have directly compared the efficacy of management in dropless cataract surgery, such as intracanalicular dexamethasone, to subconjunctival triamcinolone injection with regard to post-operative prophylaxis of inflammation in patients undergoing cataract surgery. This study aimed to compare DII with STAI for prophylaxis of post-operative inflammation after uncomplicated cataract surgery. We hypothesized that STAI provides comparable or superior prophylaxis against post-operative inflammation compared with DII.
Methods
This study adhered to the Declaration of Helsinki and followed the STROBE guidelines after obtaining approval from the University of Michigan’s Institutional Review Board (HUM00236867). This retrospective, comparative effectiveness study included patients who underwent cataract surgery with phacoemulsification and placement of intraocular lens (IOL) between January 2020 and July 2023. All procedures were performed by one of five surgeons (SM, CH, AK, LP, JB, and AV). A retrospective chart review was conducted to consecutively collect data regarding participant demographics, medical and surgical histories, perioperative medications, and comorbidities. This study was approved by the University of Michigan Institutional Review Board (IRB) [HUM00272654]. The requirement for patient informed consent was waived by the IRB because this study utilized a retrospective design involving the review of existing medical records, posed minimal risk to the subjects, and obtaining consent was not required. All patient data were kept confidential, and all distinct identifiers were removed prior to analysis to ensure anonymity. The study was conducted in strict compliance with the ethical standards of the Declaration of Helsinki.
The DII group included individuals who had a 0.4 mg dexamethasone ophthalmic insert (Ocular Therapeutix, United States, 2021) placed in either the lower or upper canaliculus intraoperatively after wound closure. The STAI group consisted of participants who received 4–6 mg triamcinolone acetonide (TA; Kenalog [Bristol-Myers-Squibb, United States]) in the subconjunctival space 4–6 mm inferior to the inferior limbus. Variance in dosing was due to surgeon preference and/or clinical reasoning. All patients received intraoperative intracameral cefuroxime 1 mg/0.1 mL or moxifloxacin 0.5 mg/0.1 mL and were advised to use preservative-free artificial tears as needed postoperatively.
Exclusion criteria included a history of ocular infection, uveitis, glaucoma, and intraoperative complications such as posterior capsular rupture, vitreous prolapse, retained lens fragments, or cataract surgery in conjunction with other procedures (eg, corneal transplant). Individuals were also excluded if they received any anti-inflammatory medications (eg, NSAID drops) in addition to either DII or STAI at any point between the surgery and final follow-up. Finally, individuals were excluded if the DII or STAI was placed, but additional corticosteroid drops were added to the post-operative regimen on or before post-operative day 3. This was to avoid potential confounding of combined treatment effects with dual anti-inflammatory therapy.
Follow-up intervals and outcome measures were abstracted from routine clinical records using standardized post hoc definitions applied uniformly across all patients. Follow-up occurred on post-operative day 1 (POD1), 1-week follow-up via telephone visit (POW1), and 1-month follow-up (POM1). The 1-month follow-up in the clinic was defined as follow-up between 21 and 56 days due to scheduling variations. Individuals with POM1 outside the interval or those who did not visit the window were excluded from the study. Baseline preoperative intraocular pressure (IOP) and IOP at the POM1 visit were measured in each eye using rebound tonometry (iCare, Icare Finland Oy). All visits for each post-operative eye between the date of surgery and POM1 were reviewed for the presence of examination findings consistent with rebound iritis, which was a trace or more anterior chamber cell necessitating the addition of supplemental topical anti-inflammatory medication between post-operative day 3 and the POM1 visit.
The severity of rebound iritis was defined on a scale of 0 to 4. The trace cell corresponds to a value of 0.5, the 1+ cell corresponds to a value of 1, the 2+ cell corresponds to a value of 2, the 3+ cell corresponds to a value of 3, and the 4+ cell corresponds to a value of 4. At the POM1 visit, any patient with suboptimal post-operative vision (best-corrected visual acuity [BCVA] worse than 20/20) not explained by another ocular comorbidity underwent optical coherence tomography (OCT) imaging to evaluate cystoid macular edema (CME). CME was defined as the development of macular thickening due to fluid accumulation, as evidenced by OCT.
The use of STAI for cataract surgery began at our institution in 2020, while the use of DII for cataract surgery at our institution began in mid-2021 and was determined via shared decision-making between the physicians (SM, CH, AK, LP, JB) and the patient.
Statistical analyses were performed using the SPSS statistical package (version 28.0; IBM Corp). The data were assessed for normality using visual inspection of Q-Q plots and showed no evidence of departure from a normal distribution. Independent two-tailed Student’s t-test, Chi-square, and Fischer’s exact tests were used, as appropriate, to compare variables of interest between groups. A p-value less than .05 was considered statistically significant. Post-hoc power analysis indicated 100% power to detect a significant difference at an alpha of 0.05 in our outcome of interest.
Results
A total of 369 eyes from 236 patients met the inclusion criteria. A total of 266 eyes of 174 patients were included in the DII group, and 103 eyes of 62 patients were included in the STAI group. The DII group’s mean age (SD) was 73.2 (8.3) compared to the mean age (SD) of 68.8 (9.2) in the STAI group (p = 0.13). Statistically significant differences were not observed between the two groups with regard to demographic, comorbidity, and ocular characteristics. All the demographic data and comorbidities of the included patients are shown in Table 1.
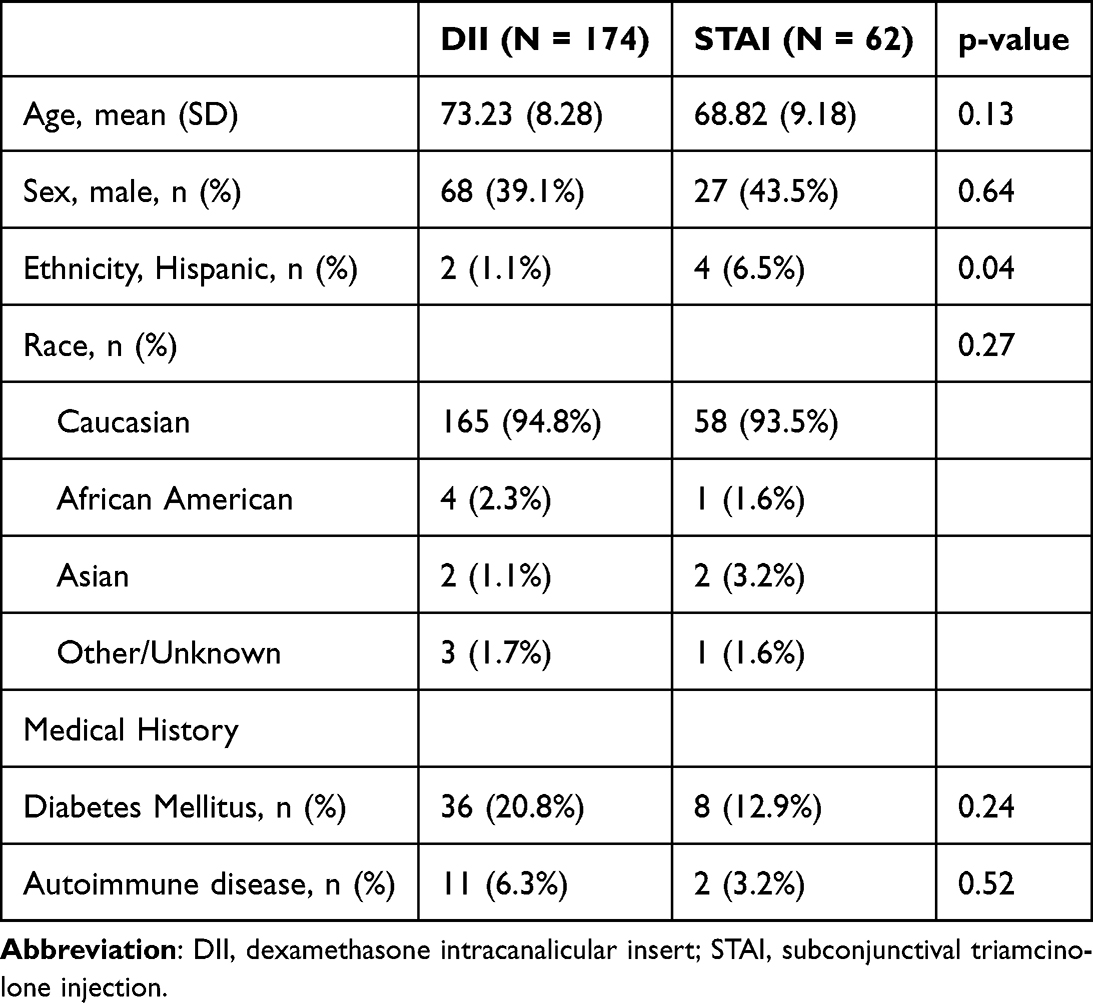 |
Table 1 Demographic, Medical History, and Ocular Characteristics of Patients Receiving Either Dexamethasone Intracanalicular Insert (DII) or Subconjunctival Triamcinolone (STAI) Post-Operatively After Cataract Surgery |
There were no significant differences between the DII and STAI groups with regard to a prior ocular history of surgical care, eye disease, or changes in IOP. The mean (SD) IOP at baseline was 15.0 (4.2) for the DII group and 14.8 (2.6) for the STAI group (p = 0.86). The mean IOP was lower in both DII (12.6) and STAI (13.11) groups at POM1, but there remained no significant difference between groups (p = 0.2). Neither group experienced increased IOP elevation of >10 mmHg from baseline or preoperative measurement compared to POM1 (Table 2).
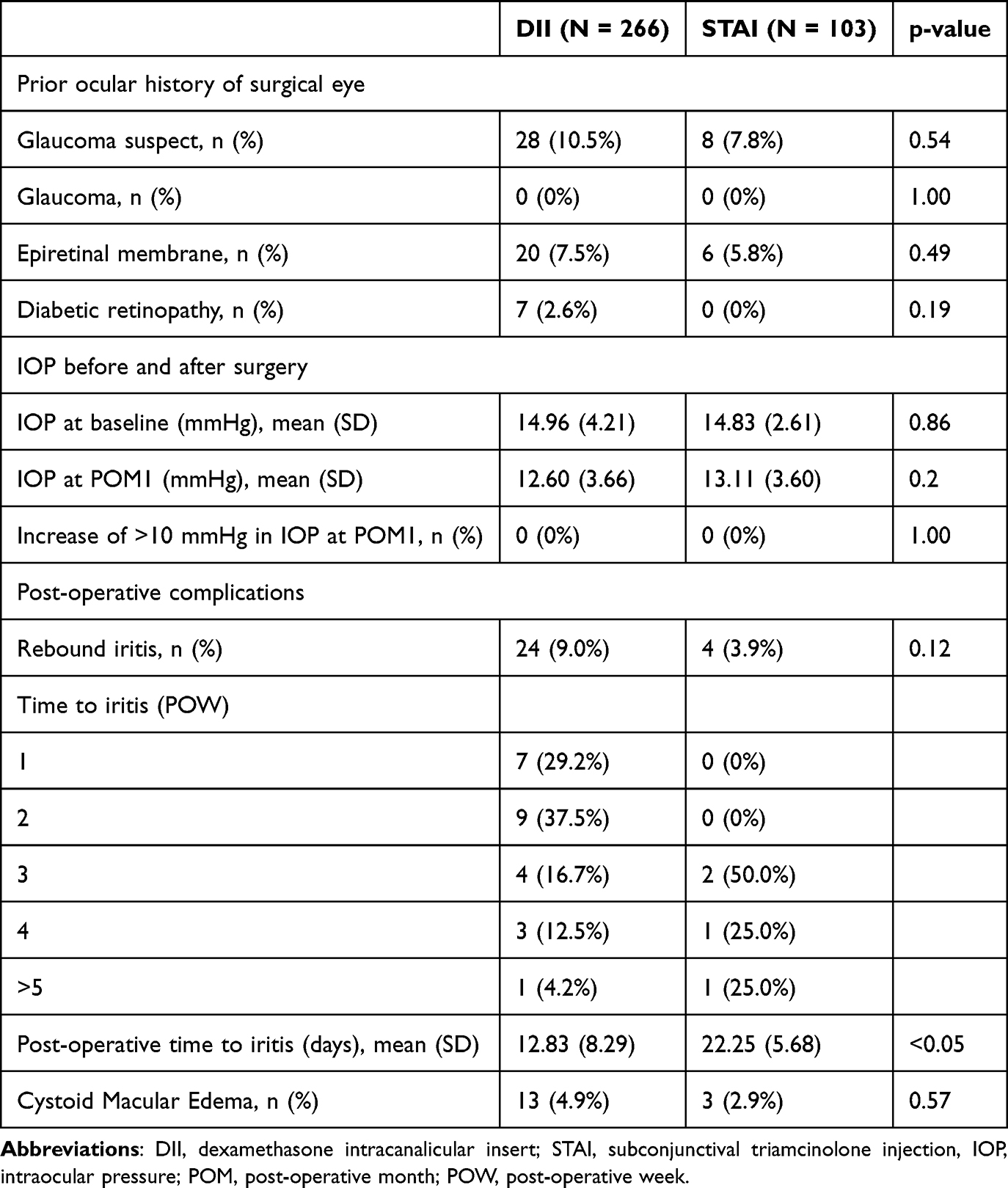 |
Table 2 Baseline Characteristics and Outcomes of Eyes Receiving Either Dexamethasone Intracanalicular Insert (DII) or Subconjunctival Triamcinolone (STAI) Post-Operatively After Cataract Surgery |
The DII group had a significantly shorter mean post-operative time (days) to iritis than the STAI group [DII group (12.8 days, SD: 8.3) compared to STAI group (22.3 days, SD: 5.7), p < 0.05]. Notably, there was a trend toward higher rates of rebound iritis in the DII (9.0%) compared with the STAI (3.9%) groups; however, this did not reach statistical significance (p = 0.12). The majority of those who experienced rebound iritis in the DII group occurred in weeks 1 and 2 (16 patients, 66.7%), whereas none of the patients in the STAI group experienced rebound iritis in the first two post-operative weeks (Table 2).
Discussion
In this single-institution, retrospective study, 369 eyes that previously underwent cataract surgery and post-operatively received either DII or STAI for inflammation prophylaxis in dropless cataract surgery were analyzed. To our knowledge, this is the first study to directly compare DII and STAI for prophylaxis of inflammation in dropless cataract surgery. As a shift is made towards dropless cataract surgery to improve patient compliance and drug penetration,12,20,23 it is important for surgeons to know which among the options for prophylaxis in dropless cataract surgery are most efficacious for their patients. This is the largest known study to compare inflammatory prophylaxis in dropless cataract surgery.24
Our retrospective study identified that among those who experienced iritis, DII patients tended to experience it in the first two weeks, whereas those in the STAI group only experienced iritis after three weeks. There are some theoretical clinical advantages to this. The delay in iritis with STAI may provide a quieter early recovery with less disruption of wound healing and IOP control, fewer urgent early visits, better adherence, and the ability to target surveillance at 3 to 4 weeks when patients may be more comfortable. Notably, however, there was no significant difference in the rate of occurrence of rebound iritis between the groups, despite the time to post-operative iritis being significantly longer in the STAI group. The trend towards earlier timing of post-operative iritis in the DII group in our study may also be due to the underlying pharmacokinetics and mechanisms of these agents. The DII is designed for sustained, low-dose release targeting the ocular surface.25 However, subconjunctival triamcinolone depot may potentially provide more prolonged release and greater tissue penetration.20,26 This may be due to the hydrophobic and diffusive nature of STAI, which may persist up to 8 weeks in ocular tissues and binds ocular pigment, possibly yielding more prolonged exposure; however, further anterior-segment-specific studies are needed to confirm this definitively.20,27–29 This may also help explain the trend towards lower rates of rebound iritis in the STAI group compared to the DII group and potentially contribute to the lower rates and later presentation of post-operative iritis observed in the STAI group. Another factor may be due to DII’s risk of falling out of the canaliculus in the treatment window, with Phase III trials reporting that 9.6% of patients did not retain the insert for 30 days.25
The established rate of clinical cystoid macular edema after uncomplicated cataract surgery is between 0.8 and 3%.30,31 Broadly, both DII and STAI have rates of cystoid macular edema largely consistent with the literature. While only 2.9% of individuals who received STAI had cystoid macular edema, which was lower than that in the DII group, the low sample size limits the broader benefit for either prophylaxis option. The higher rate observed in the DII group (4.9%) compared to established levels may be due to the exclusion of patients placed on any topical NSAID prophylaxis, the standard preventative measure of cystoid macular edema.30 Still, cross-cohort comparison may suggest that STAI tends toward lower rates of cystoid macular edema; however, no significant association existed, and the number of cases was small in both groups.
Currently, many effective options exist for the prophylaxis of post-operative inflammation after cataract surgery.9,30 The evidence continues to suggest that topical formulations remain limited in their real-world efficacy due to issues with adherence and pharmacokinetic challenges.13 As such, dropless cataract surgery methods with STAI or DII may gain greater market share and utilization within practices globally. Options such as DII have continued to have high rates of efficacy in clinical outcomes among other studies, including ours. Additionally, real-world patient and staff experience shows >90% rates of satisfaction with the use of DII compared to topical formulations.32,33 Similarly, STAI has been in practice for post-operative prophylaxis and has been as safe and efficacious as similar topical solutions. While both options provide adequate benefits for the prophylaxis of inflammation after cataract surgery, our study identified a significantly faster onset of post-operative iritis with DII, potentially related to the underlying pharmaceutical mechanisms or issues due to drug delivery. This may indicate that STAI may be somewhat more consistent in early inflammatory reduction, especially given that no patients in the STAI group experienced iritis before three weeks post-operatively. The increased availability and penetration of the subconjunctival formulation may also explain the trend toward lower rates of cystoid macular edema in the STAI group.
Clinically, the DII group’s earlier iritis onset (approximately 9.5-day difference) and the numerically higher rebound rate (9.0% vs 3.9%) mirror recent evidence that dexamethasone intracanalicular inserts have more rebound iritis than steroids after cataract surgery.17 These patterns suggest STAI may provide more durable postoperative control when minimizing early iritis and rebound is a priority, with the caveat that the rebound difference here was not statistically significant. However, further work needs to be done to better define thresholds for optimal clinical decision-making between these two options.
Our study has some limitations. This was a retrospective cohort study and could not prove causal relationships between treatment and outcome, and may be susceptible to information bias. Excluding participants who required topical steroids potentially removed higher-risk cases or those with higher inflammation, biasing incidence and severity estimates, and partially limiting external validity to real-world settings where rescue therapy may be more common. If rescue use differed between DII and STAI cases, this exclusion could also introduce differential selection bias for between-group comparisons. Because this was a retrospective chart review without standardized documentation of DII retention, we could not reliably assess canalicular fallout, which may have led to under-ascertainment of retention failures as a potential outcome or contributing factor. Additionally, there was a wide definition of the follow-up schedule for POM1 (21–56 days) due to the retrospective nature of our study, which may introduce variability in our outcomes of interest. The unequal group sizes (266 in the DII group compared to 103 eyes in the STAI group) may reduce statistical power and precision, especially in the smaller cohort, and increase susceptibility to baseline imbalances that limit group comparability. Certain surgeons (JB and SM) preferentially used the DII, whereas other surgeons (AV) nearly exclusively used the STAI, which may further bias our results. Our study also consisted of predominantly white males, potentially limiting external validity and generalizability, especially given the associations with higher rates of rebound iritis among certain minority groups.31 Additionally, given the increased healthcare costs associated with DII,32 portions of our study population may have greater levels of affluence or ability to afford care. The mean Medicare-allowed charge for a dexamethasone intracanalicular insert implant in the United States is $538.49 (SD, $63.79) per eye.32 By contrast, a standalone subconjunctival injection of triamcinolone acetonide costs only $4.01 per eye.33 Although dexamethasone intracanalicular insert affords improved patient convenience and workflow efficiencies,17 its higher upfront cost and limited coverage under government programs constrain accessibility for uninsured and publicly insured patients. Regardless, evidence suggests that options for inflammation prophylaxis in dropless cataract surgery may offer potential cost benefits compared with topical options.34
Despite these limitations, this is the largest study to compare options for methods of inflammation prophylaxis in dropless cataract surgery.24 Furthermore, this is the first study to compare the two options for dropless cataract surgery that are increasingly utilized nationally and globally. Our data suggest that DII and STAI are largely similar in efficacy in terms of pre- and post-operative IOP, without significant differences in rebound iritis or cystoid macular edema; however, STAI had a significantly longer post-operative time to iritis than DII. Given the rates of complications in this study, although largely similar to established rates, clinicians should still individualize the clinical management of each patient’s unique risk factors and history. Longitudinal prospective studies and larger randomized clinical trials should be conducted to better identify superior options among other modalities of dropless cataract surgery, factoring comparisons of patient satisfaction and cost analyses of each option.
Abbreviations
POMI, first post-operative month; DII, intracanicular dexamethasone implant; STAI, subconjunctival triamcinolone injection; CME, cystoid macular edema; IOP, intraocular pressure; NSAIDs, non-steroidal anti-inflammatory drugs; IOL, intraocular lens; TA, triamcinolone acetonide; POD1, post-operative day 1; POW1, post-operative week 1; BCVA, Best Corrected Visual Acuity; SD, Standard deviation.
Data Sharing Statement
Available upon reasonable request to corresponding author.
Funding
Work on this project was in part supported by an unrestricted grant from Research to Prevent Blindness to the University of Michigan Department of Ophthalmology and Visual Sciences and the University of Pennsylvania Department of Ophthalmology.
Disclosure
Dr. Shahzad Mian is a research investigator for KOWA and has received up-to-date royalties for work unrelated to the content of this manuscript. The other authors report no potential conflicts of interest that could influence this work, including consulting, royalties, and research support.
References
1. McGhee CN, Zhang J, Patel DV. A perspective of contemporary cataract surgery: the most common surgical procedure in the world. J Roy Soc New Zeal. 2020;50(2):245–8. doi:10.1080/03036758.2020.1714673
2. Donnenfeld ED. Current trends in postsurgical management of ocular inflammation following cataract surgery. Expert Rev Ophthalmol. 2015;10(1):23–31. doi:10.1586/17469899.2015.996548
3. El-Harazi SM, Feldman RM. Control of intra-ocular inflammation associated with cataract surgery. Curr Opin Ophthalmol. 2001;12(1):4–8. doi:10.1097/00055735-200102000-00002
4. Gulkilik G, Kocabora S, Taşkapılı M, Engin G. Cystoid macular edema after phacoemulsification: risk factors and effect on visual acuity. Can J Ophthalmol. 2006;41(6):699–703. doi:10.3129/i06-062
5. Hoffman RS, Braga‐Mele R, Donaldson K, et al. Cataract surgery and nonsteroidal antiinflammatory drugs. J Cataract Refract Surg. 2016;42:1368–1379. doi:10.1016/j.jcrs.2016.06.006
6. Mohammadpour M, Jafarinasab MR, Javadi MA. Outcomes of acute postoperative inflammation after cataract surgery. Eur J Ophthalmol. 2007;17:20–28. doi:10.1177/112067210701700104
7. Pleyer U, Ursell PG, Rama P. Intraocular pressure effects of common topical steroids for post-cataract inflammation: are they all the same? Ophthalmol Ther. 2013;2:55–72. doi:10.1007/s40123-013-0020-5
8. Donnelly D. Instilling eyedrops: difficulties experienced by patients following cataract surgery. J Adv Nurs. 1987;12(2):235–243. doi:10.1111/j.1365-2648.1987.tb01327.x
9. Lindstrom RL, Galloway MS, Grzybowski A, Liegner JT. Dropless cataract surgery: an overview. Curr Pharm Des. 2017;23(4):558–564. doi:10.2174/1381612822666161129150628
10. Matossian C. Noncompliance with prescribed eyedrop regimens among patients undergoing cataract surgery—prevalence, consequences, and solutions. US Ophthalmic Rev. 2020;13(1):18. doi:10.17925/USOR.2020.13.1.18
11. Hermann MM, Üstündag C, Diestelhorst M. Electronic compliance monitoring of topical treatment after ophthalmic surgery. Intl Ophthalmol. 2010;30:385–390. doi:10.1007/s10792-010-9362-3
12. Gaudana R, Ananthula HK, Parenky A, Mitra AK. Ocular drug delivery. AAPS J. 2010;12:348–360. doi:10.1208/s12248-010-9183-3
13. Chrai SS, Makoid MC, Eriksen SP, Robinson JR. Drop size and initial dosing frequency problems of topically applied ophthalmic drugs. J Pharmaceut Sci. 1974;63(3):333–338. doi:10.1002/jps.2600630304
14. Assil KK, Greenwood M, Gibson A, Vantipalli S, Metzinger J, Goldstein MH. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction. Curr Opin Ophthalmol. 2020.
15. Lu AQ, Rizk M, O’rourke T, et al. Safety and efficacy of topical vs intracanalicular corticosteroids for the prevention of postoperative inflammation after cataract surgery. J Cataract Refract Surg. 2022;48(11):1242–1247. doi:10.1097/j.jcrs.0000000000000963
16. Tan DT, Chee S-P, Lim L, Lim AS. Randomized clinical trial of a new dexamethasone delivery system (Surodex) for treatment of post-cataract surgery inflammation. Ophthalmology. 1999;106(2):223–231. doi:10.1016/S0161-6420(99)90060-X
17. Shapiro JN, Armenti ST, Levine H, Hood CT, Mian SI. Dexamethasone intracanalicular insert versus standard topical steroids for the prophylaxis of inflammation after cataract surgery. Am J Ophthalmol. 2024;268:174–180. doi:10.1016/j.ajo.2024.07.030
18. Walters T, Bafna S, Vold S, et al. Efficacy and safety of sustained release dexamethasone for the treatment of ocular pain and inflammation after cataract surgery: results from two Phase 3 studies. J Clin Exp Ophthalmol. 2016;7(4):572. doi:10.4172/2155-9570.1000572
19. Singhal R, Luo A, O’Rourke T, Scott IU, Pantanelli SM. Transzonular triamcinolone–moxifloxacin versus topical drops for the prophylaxis of postoperative inflammation after cataract surgery. J Ocul Pharmacol Ther. 2019;35(10):565–570. doi:10.1089/jop.2019.0097
20. Shorstein NH, McCabe SE, Alavi M, Kwan ML, Chandra NS. Triamcinolone acetonide subconjunctival injection as stand-alone inflammation prophylaxis after phacoemulsification cataract surgery. Ophthalmology. 2024;131(10):1145–1156. doi:10.1016/j.ophtha.2024.03.025
21. Fram N, Alsetri H, Shiler O, Paterno PJ, Cabang J. Retrospective study of a sustained-release intracanalicular dexamethasone insert for treatment of ocular inflammation after cataract and corneal surgery. Clin Ophthalmol. 2022;16:4065. doi:10.2147/OPTH.S386702
22. Lindholm JM, Taipale C, Ylinen P, Tuuminen R. Perioperative subconjunctival triamcinolone acetonide injection for prevention of inflammation and macular oedema after cataract surgery. Acta Ophthalmologica. 2020;98(1):36–42. doi:10.1111/aos.14175
23. Assil KK, Greenwood MD, Gibson A, Vantipalli S, Metzinger JL, Goldstein MH. Dropless cataract surgery: modernizing perioperative medical therapy to improve outcomes and patient satisfaction. Curr Opin Ophthalmol. 2021;32:S1–S12.
24. Güngör SG, Bulam B, Akman A, Çolak M. Comparison of intracameral dexamethasone and intracameral triamcinolone acetonide injection at the end of phacoemulsification surgery. Indian J Ophthalmol. 2014;62(8):861–864. doi:10.4103/0301-4738.141045
25. Lee A, Blair HA. Dexamethasone intracanalicular insert: a review in treating post-surgical ocular pain and inflammation. Drugs. 2020;80(11):1101–1108. doi:10.1007/s40265-020-01344-6
26. Beer PM, Bakri SJ, Singh RJ, Liu W, Peters GB III, Miller M. Intraocular concentration and pharmacokinetics of triamcinolone acetonide after a single intravitreal injection. Ophthalmology. 2003;110(4):681–686. doi:10.1016/S0161-6420(02)01969-3
27. Du W, Sun S, Xu Y, et al. The effect of ocular pigmentation on transscleral delivery of triamcinolone acetonide. J Ocul Pharmacol Ther. 2013;29(7):633–638. doi:10.1089/jop.2012.0226
28. Mora P, Eperon S, Felt-Baeyens O, et al. Trans-scleral diffusion of triamcinolone acetonide. Curr Eye Res. 2005;30(5):355–361. doi:10.1080/02713680590934094
29. Kovacs K, Wagley S, Quirk MT, et al. Pharmacokinetic study of vitreous and serum concentrations of triamcinolone acetonide after posterior sub-tenon’s injection. Am J Ophthalmol. 2012;153(5):939–948. doi:10.1016/j.ajo.2011.10.021
30. Miller KM, Oetting TA, Tweeten JP, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2022;129(1):P1–P126. doi:10.1016/j.ophtha.2021.10.006
31. Iftikhar M, Dun C, Schein OD, Lum F, Woreta F. Cystoid macular edema after cataract surgery in the United States: IRIS® Registry (Intelligent Research in Sight) analysis. Ophthalmology. 2023;130(10):1005–1014. doi:10.1016/j.ophtha.2023.06.001
32. Nijm L, Matossian C, Rhee MK, et al. Early real-world patient and staff experience with an intracanalicular dexamethasone insert. Clin Ophthalmol. 2024;Volume 18:1391–1401. doi:10.2147/OPTH.S448973
33. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (Dextenza™): results of a qualitative survey</sup>. Patient Prefer Adher. 2017;Volume 11:487–494. doi:10.2147/PPA.S126283
34. Massa S, Smits DJ, Nguyen AT, et al. Cost analysis of dropless cataract surgery prophylaxis with intracameral antibiotics and subconjunctival steroids. J Cataract Refract Surg. 2024;50(12):1215–1223. doi:10.1097/j.jcrs.0000000000001526
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Intravitreal Injection of Conbercept Combined with Dexamethasone for Macular Edema Following Central Retinal Vein Occlusion
Wu P, Zhang P, Xu J, Ma W, Li L, Xu H
Clinical Ophthalmology 2024, 18:1851-1860
Published Date: 26 June 2024
Efficacy and Safety of Ranibizumab Combined with Dexamethasone Intravitreal Implant Sequential Therapy for Macular Edema Secondary to Non-Ischemic Retinal Vein Occlusion
Gao L, Cai X, Dang Y
Drug Design, Development and Therapy 2026, 20:604539
Published Date: 30 March 2026